
Abstract
Purpose:
To evaluate the effectiveness of an individually tailored intervention for improvement in lifestyle behavior, health indicators, and prevention and reduction of overweight among construction workers.
Design:
Randomized controlled trial.
Setting:
Various blue-collar departments of a large construction company in the Netherlands.
Participants:
Blue-collar workers randomized to an intervention (n = 162) or a control group (n = 152).
Intervention:
The intervention group received individual coaching sessions, tailored information, and materials to improve lifestyle behavior during a 6-month period, and the control group received usual care.
Measures:
Body weight, body mass index (BMI), waist circumference, physical activity (PA) levels, dietary behavior, blood pressure, and blood cholesterol were assessed.
Analysis:
Effectiveness of the intervention on outcome measures at 6- and 12-month follow-up was assessed by using linear and logistic regression models adjusting for baseline levels.
Results:
After 6 months, a statistically significant intervention effect was found on body weight (B = −1.06, P = .010), BMI (B = −0.32, P = .010), and waist circumference (B = −1.38, P = .032). At 6 months, the percentage of those meeting public health guidelines for PA increased significantly in the intervention group compared to the control group (B = 2.06, P = .032), and for sugar-sweetened beverages, an intervention effect was found at 6 months as well (B = −2.82, P = .003). At 12 months, for weight-related outcomes, these differences were slightly smaller and no longer statistically significant. The intervention was not effective on the total amount of moderate to vigorous PA and other dietary and health outcomes.
Conclusion:
Intervention participants showed positive changes in vigorous PA and intake of sugar-sweetened beverages compared to controls, as well as effects on weight-related outcomes at 6 months. Long-term effects were still promising but not statistically significant.
Introduction
The worldwide increased prevalence of overweight and obesity is associated with considerable negative impact on health. Excess body weight is associated with increased mortality 1 and adverse health outcomes. 2 The predominant health issues associated with overweight and obesity include type 2 diabetes, cardiovascular disease (CVD), cancer, and musculoskeletal disorders. 3,4 The economic burden of overweight is substantial and is expected to increase. 5 In the Netherlands, annual overweight-related health-care costs are estimated at US$635 million, while indirect costs, reflecting the value of lost productivity resulting from work absence and disability, are projected to be about US$2.5 billion. 6,7
In general, even after adjustment for sociodemographic factors, the prevalence of overweight and obesity in manual laborers within the construction industry is higher than in the general adult population. 8 -10 These blue-collar (or construction) workers have an increased risk of sick leave, disability, and decreased productivity resulting from (a combination of) risk factors such as obesity, high physical workload, 11 and musculoskeletal symptoms. 12 -14
This increased prevalence of overweight justifies occupational and sector-specific preventive strategies 6 for construction workers. Among workers with a high physical work demand, preventing and reducing excessive body weight might be a strategy to increase or preserve work ability, 12 decrease sick leave, 11 and reduce musculoskeletal symptoms by lowering the relative load on the musculoskeletal system.
Evidence for the effectiveness of worksite physical activity (PA) and dietary behavior interventions on weight outcomes was found in several systematic reviews and a recent meta-analysis. 15,16 These publications did not include effective interventions specifically designed for blue-collar workers in the construction industry. A lifestyle program aimed at improving the health of construction workers with a high risk of CVD showed promising effects of lifestyle counseling on weight-related outcomes. 17 However, this lifestyle program aimed at a high risk group. The World Health Organization has recommended that prevention of overweight and obesity should target adults, even while body mass index (BMI) is still within an acceptable range. 18 Therefore, a population approach might be the most appropriate prevention strategy in a population with a relatively high prevalence of unhealthy weight.
The aim of the present study was to evaluate the effectiveness of an individually tailored intervention, “VIP in construction,” among blue-collar construction workers on body weight–related measures (ie, body weight, BMI, and waist circumference), blood pressure, and cholesterol. The VIP in construction intervention consists of personal health coaching, information, and tools to support changes in PA and dietary behavior. In addition, to gain insight into which behavioral changes may have led to the effects on these outcomes, PA and dietary intake were evaluated.
Methods
Trial Design
The effectiveness of the program was measured by performing a randomized controlled trial (RCT). Participants were measured at baseline, at 6 months, and at 12 months. Written informed consent was obtained from participants before enrollment in the study. Consenting participants were randomized to the intervention or control group after the baseline measurement. The control group received care as usual and was only contacted for the baseline and follow-up measurements. Care as usual consisted only of a noncompulsory periodic health screening (PHS), whereas the intervention group received a lifestyle intervention tailored to the PHS outcomes. The study design and procedures have been approved by the Medical Ethics Committee of the VU University Medical Center, and the trial has been registered in the Netherlands Trial Register (NTR): NTR2095.
Participants
The research population consisted of consenting blue-collar workers of a construction company who attended the PHS. In the Netherlands, collective labor agreement workers in this sector are entitled to these health screenings. The PHS is conducted by occupational physicians (OPs) and assistants from occupational health services. In the participating company, over 80% of the workers participate in the PHS. The population consisted of workers in various construction trades such as carpenters, bricklayers, road workers, crane operators, and factory workers. The exclusion criterion was being on sick leave for >4 weeks at baseline. Sickness absence data were collected over a 2-year period, starting 12 months prior to baseline. In total, 327 workers were recruited over a 15-month period (March 2010 to June 2011), and 314 of those were randomized to an intervention (n = 162) or a control group (n = 152; Figure 1).
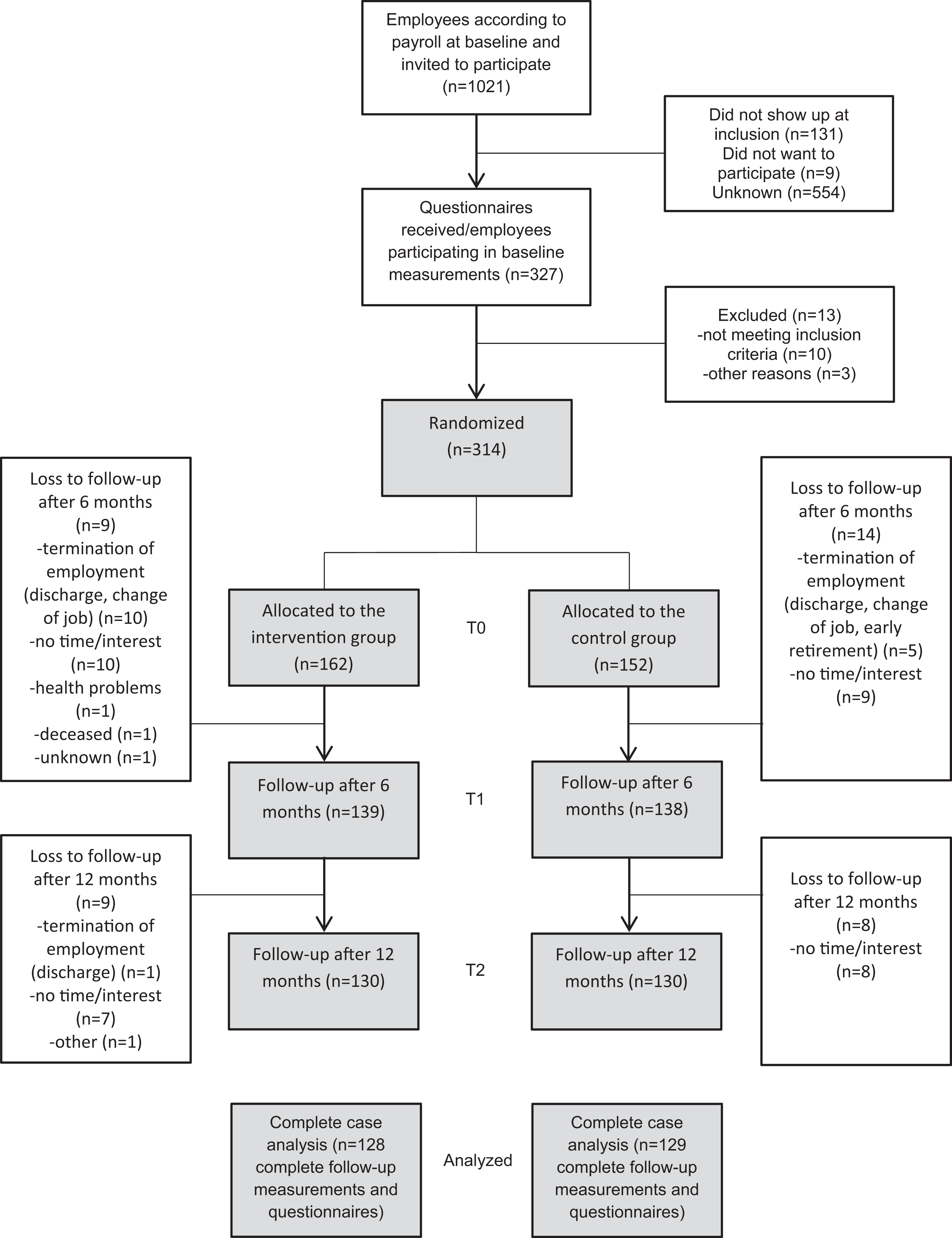
Flowchart of the study participants.
Randomization and Blinding
After baseline measurements, the participants were randomly assigned to either the intervention or the control group by a computer-generated list using SPSS (version 15). The randomization was prepared and performed by an independent researcher (ie, the research assistant). After randomization, workers assigned to the control group received general information on the follow-up measurements. In the trial, data collectors and data analysts were blinded for allocation. Although participants were not informed of their allocation, participants and intervention providers could not be blinded.
Intervention
The intervention program aimed at the prevention and reduction of overweight and musculoskeletal disorders and was developed and implemented by applying the Intervention Mapping protocol. 19,20 This protocol guides the systematic and evidence-based planning and development of health promotion programs with a strong emphasis on stakeholder involvement. This process resulted in the “VIP in construction” program, a tailored program including personal health coaching, information, and tools to support changes in PA and dietary behavior. The program was offered at the worksite during working hours. According to the study protocol, the intervention commenced within 2 weeks after the baseline measurements delivered by study-trained health professionals (personal health coaches) during initial face-to-face and follow-up telephone health coaching sessions, consisting of a minimum of 2 and a maximum of 4 sessions. During the coaching sessions, participants received personalized feedback on their health screening and current lifestyle behavior, received training instruction, and were supported in self-monitoring of behavior, goal setting, and evaluation. Participants also received personal energy plan forms to record their goals and action plans, forms they could also use during the follow-up health coaching sessions. The intervention was tailored to the participant’s weight status (BMI and waist circumference), PA level, and stage of change. The intervention program focused on improving PA levels and healthy dietary behavior and in addition to the coaching sessions consisted of tailored information, training instruction for core stability and strengthening exercises, and the VIP in construction toolbox (overview of the company health-promoting facilities, waist circumference–measuring tape, pedometer, BMI calculator, calorie guide, recipes, and knowledge tests).
Outcome Measures
Questionnaire and physiological measurement data were collected from 2009 until 2012 at baseline before the randomization (n = 314), 6 months after baseline, following the intervention (n = 277), and 12-month follow-up after baseline (n = 261). The periodical health screening provided baseline data and was performed by the OP or assistant. Follow-up measurements at 6 and 12 months were performed by study-trained research assistants. To ensure standardization of measurements, OPs and assistants were provided with measurement protocols.
Body weight and BMI
Body weight was measured using a digital weight scale. Body weight and height were measured with the participants standing without shoes and heavy outer garments. Data on body weight and height were used to calculate BMI (kg/m2).
Waist circumference
Waist circumference was measured as midway between the lower rib margin and the iliac crest with participants in standing position at the end of expiration. 21 To standardize waist circumference measurement, OPs and assistants were provided with a Seca 201 waist circumference measure (Seca, Hamburg, Germany) and measurement protocol.
Blood pressure
At follow-up, systolic and diastolic blood pressures (mm Hg) were measured twice with a fully automated blood pressure monitor (type: OMRON M6, Omron Healthcare, Japan). The mean value of the 2 measurements was computed.
Blood cholesterol (total cholesterol)
Total cholesterol (TC; mmol/L) was measured with nonfasting finger stick samples analyzed on a Cholestech LDX desktop analyzer (Cholestech, Hayward, California). This analyzer has been validated for lipid measurements in clinical practice. 22
Physical activity
To measure PA, the validated Short Questionnaire to ASsess Health Enhancing-Physical Activity (SQUASH) was applied, which is generally considered a fairly reliable and valid questionnaire (r Spearman: .58 and .45, respectively). 23 The SQUASH measures duration, frequency, and intensity of different domains of PA (active work transportation, occupational PA, household activities, and leisure time activities). For the leisure time domain, activities were subdivided into age-dependent intensity categories, by the metabolic equivalents derived from the compendium of physical activities. 24 Since the VIP in construction intervention was aimed at improving leisure time moderate and vigorous physical activities (MVPAs), the outcome measure for this study was total minutes per week for moderate to vigorous activities in leisure time including sports activities, walking, cycling, doing odd jobs, and gardening. Additionally, the frequency of vigorous activities was assessed by the number of days per week that vigorous-intensity leisure time activities were performed for at least 20 minutes. This measure relates to international PA guidelines 25 as well as to the Dutch guidelines. 26 To apply to the public health guideline for vigorous PA (Fitnorm), vigorous-intensity aerobic PA should be performed for a minimum of 20 minutes on 3 days each week. This was assessed with the question “How many times a week, in leisure time, do you engage in strenuous sports or physical activities, that last long enough to make you sweat, with a minimum of 20 minutes?”
Dietary intake
Number of beverages as well as consumption of energy-dense snacks, fruit, and vegetables were assessed using questions as applied in the Health under Construction study for workers in the construction industry at risk of CVD. 27 In these questions, in line with the Short Questionnaire for Measuring Fruit and Vegetable intake, average weekly intake and daily portions of several food groups during a usual week during the past month are indicated.
Alcohol consumption was assessed by asking participants to report their average consumption of beer, wine, and/or spirits in days per week and number of consumptions a day. Total consumption was converted to number of standard drinks, containing approximately 10 g of alcohol. Sugar-sweetened beverages (SSBs) are defined as soft drinks, energy drinks, fruit juice, and coffee or tea with added sugar. Snack intake was defined as the sum of sweet (ie, chocolate bar) and cold and warm salty snacks (ie, handful of crisps) eaten outside regular meals. Fruit was assessed by intake of pieces a day, and vegetable intake was determined for heated and raw vegetables in number of tablespoons. The effectiveness evaluation of the intervention on musculoskeletal disorders has been described in a separate publication. 28
Potential Confounders and Effect Modifiers
Data on potential confounders and effect modifiers were assessed by a questionnaire including age, smoking (yes/no), education (low = elementary school, medium = secondary education, and high = college/university), and marital status (married/cohabitating and single/divorced/widowed).
Statistical Methods
Randomization was checked for differences in baseline values between the intervention and control groups, using independent t test for continuous variables and Pearson χ2 tests for categorical and dichotomous variables. The sample size calculation has been described elsewhere. 19
The effectiveness of the lifestyle intervention was assessed using a regression analysis with the outcome measures at 6- and 12-month follow-up as the dependent variables and adjusting for the baseline levels of the outcome measure. Both crude and adjusted analyses were performed. Linear and logistic regression analyses were performed using SPSS version 20.0 (SPSS Inc, Chicago, Illinois). According to the intention-to-treat principle, all available data of the participants, regardless of whether or not they actually received the complete intervention, were used for data analysis. The analysis was conducted with all available data of the respondents at the time of follow-up (complete cases). Within-group analyses were conducted using paired t tests. For all analyses, a 2-tailed significance level of <.05 was considered statistically significant. Regression models, with unstandardized regression coefficients (B) for linear models and odds ratios (ORs) for logistic models, were presented as crude (model I) and adjusted full models (model II).
Results
Between March 2010 and June 2011, 314 participants were enrolled in the study. Figure 1 presents the CONSORT flowchart of the participants throughout the trial. A total of 162 workers were assigned to the intervention group and 152 to the control group; 83% of the workers remained in the study during the 12-month follow-up.
Baseline and Confounding
Baseline characteristics of the 2 study groups are presented in Table 1. All participants were male, reflecting the predominantly male worker population. Of the total study population, 70% were overweight and 22.7% obese. No statistically significant baseline differences between the intervention and control groups were found for outcome measures or potential confounders.
Baseline Characteristics of the Total Study Population and by Group Allocation.
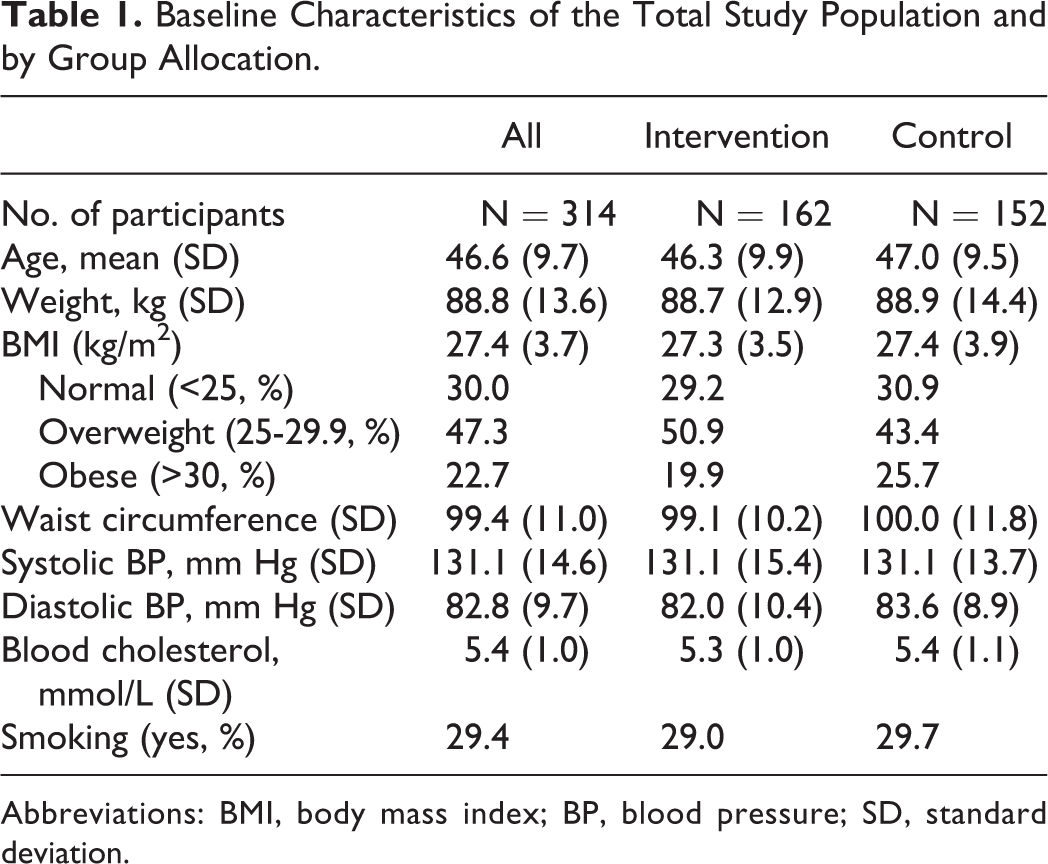
Abbreviations: BMI, body mass index; BP, blood pressure; SD, standard deviation.
Physiological Outcomes
Table 2 presents the mean (SD) for body weight, BMI, and waist circumference at baseline, 6-month, and 12-month follow-up for the intervention and control groups, as well as the results of the linear regression analysis. At 6 months, there was a significant intervention effect on body weight (B = −1.06, 95% CI: −1.87 to −0.26), BMI (B = −0.32, 95% CI: −0.57 to −0.08), and waist circumference (B = −1.38, 95% CI: −2.63 −0.1; Table 2). Directly following the intervention period, body weight and BMI increased in the control group, while it did not change significantly in the intervention group. Waist circumference decreased at 6 and 12 months of follow-up for the intervention participants. At 12 months, analyses within groups (paired t tests) showed that the decrease in waist circumference in the intervention group and the increase in body weight and BMI in the control group compared to baseline values were still significant. However, the effects for body weight and BMI in the between-group analyses were not statistically significant (P = .053 and P = .057, respectively) and even further from statistically significant for waist circumference (P = .187). Baseline weight status was not found to be an effect modifier in the adjusted model. However, this may be due to the low number of participants in subgroups, while modest effect differences were found in BMI subgroups (Table 3). No significant intervention effects in diastolic or systolic blood pressure or TC levels were found (Table 4).
Data on Primary Outcome Measures for Complete Cases at Baseline (Mean, SD) at 6- and 12-Month Follow-Up in the Intervention and Control Groups.a,b,c
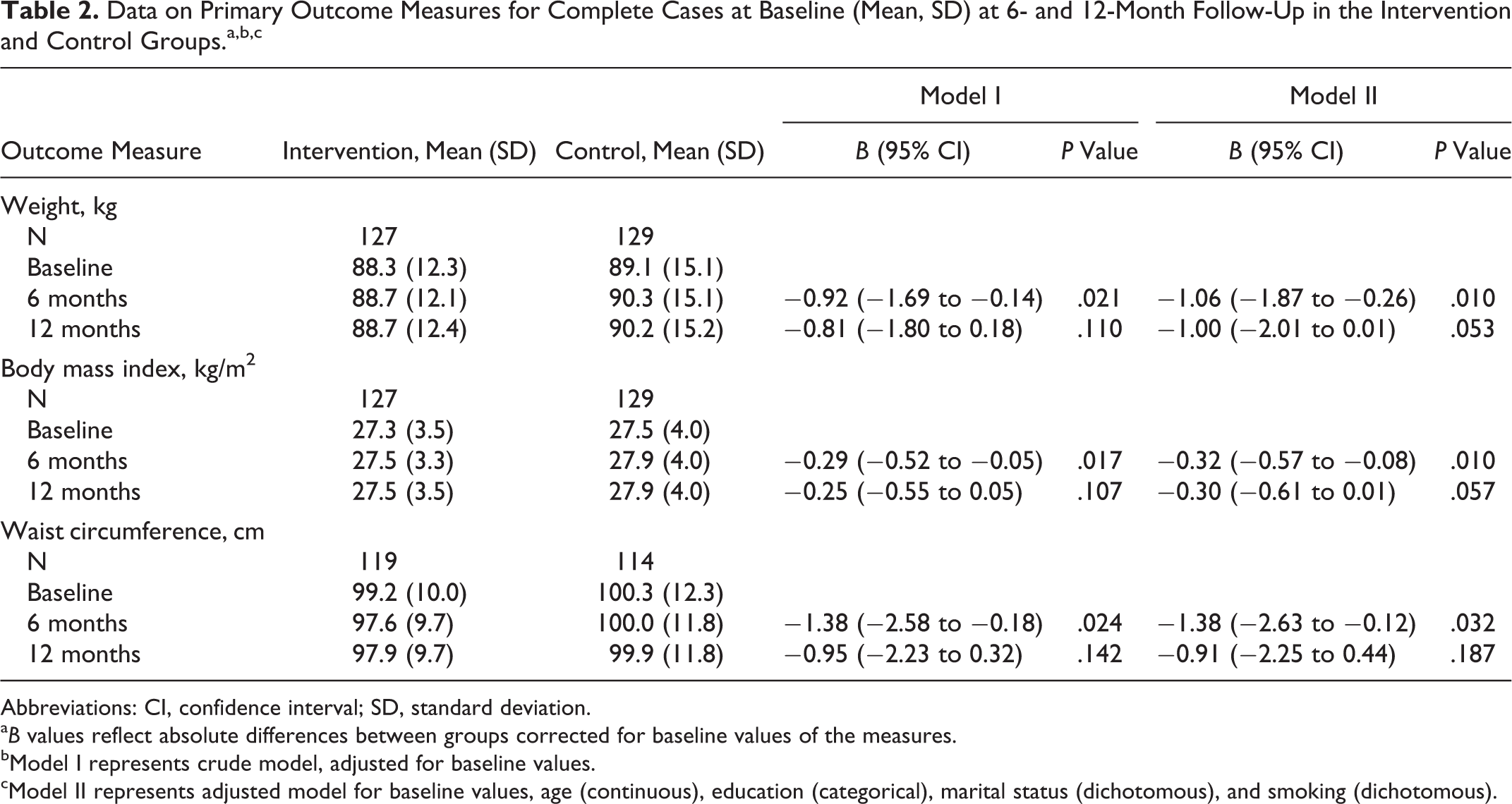
Abbreviations: CI, confidence interval; SD, standard deviation.
a B values reflect absolute differences between groups corrected for baseline values of the measures.
bModel I represents crude model, adjusted for baseline values.
cModel II represents adjusted model for baseline values, age (continuous), education (categorical), marital status (dichotomous), and smoking (dichotomous).
Baseline Data and Estimated Effects of the Intervention on Blood Pressure (BP) and Cholesterol.a,b,c
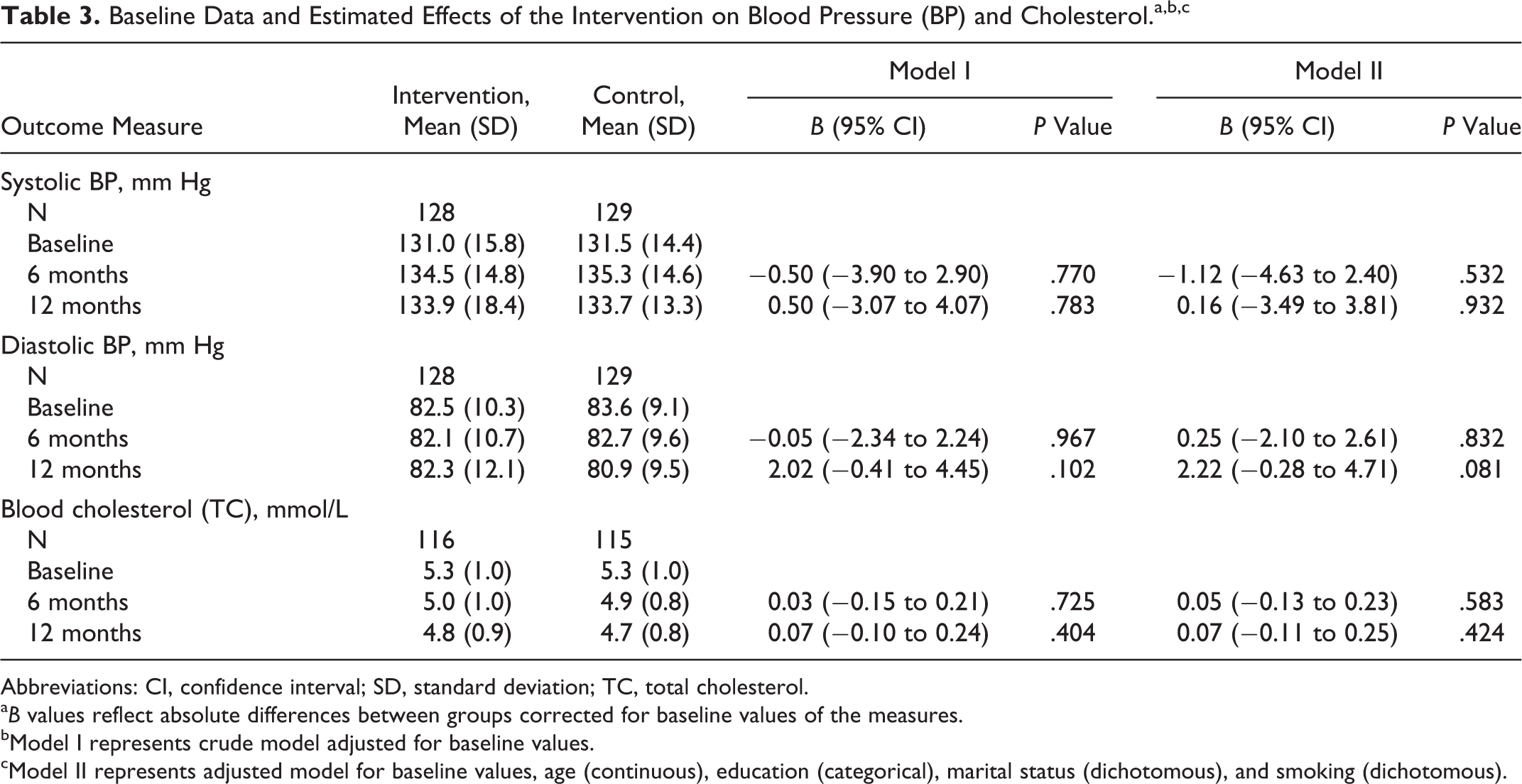
Abbreviations: CI, confidence interval; SD, standard deviation; TC, total cholesterol.
a B values reflect absolute differences between groups corrected for baseline values of the measures.
bModel I represents crude model adjusted for baseline values.
cModel II represents adjusted model for baseline values, age (continuous), education (categorical), marital status (dichotomous), and smoking (dichotomous).
Differences in Minutes Per Week Spent on At Least Moderate Intensity of Physical Activity, Meeting the Public Health Guideline for Vigorous Physical Activity, and Dietary Intake Between Intervention and Control Groups at 6- and 12-Month Follow-Up, Corrected for Baseline Values.a,b
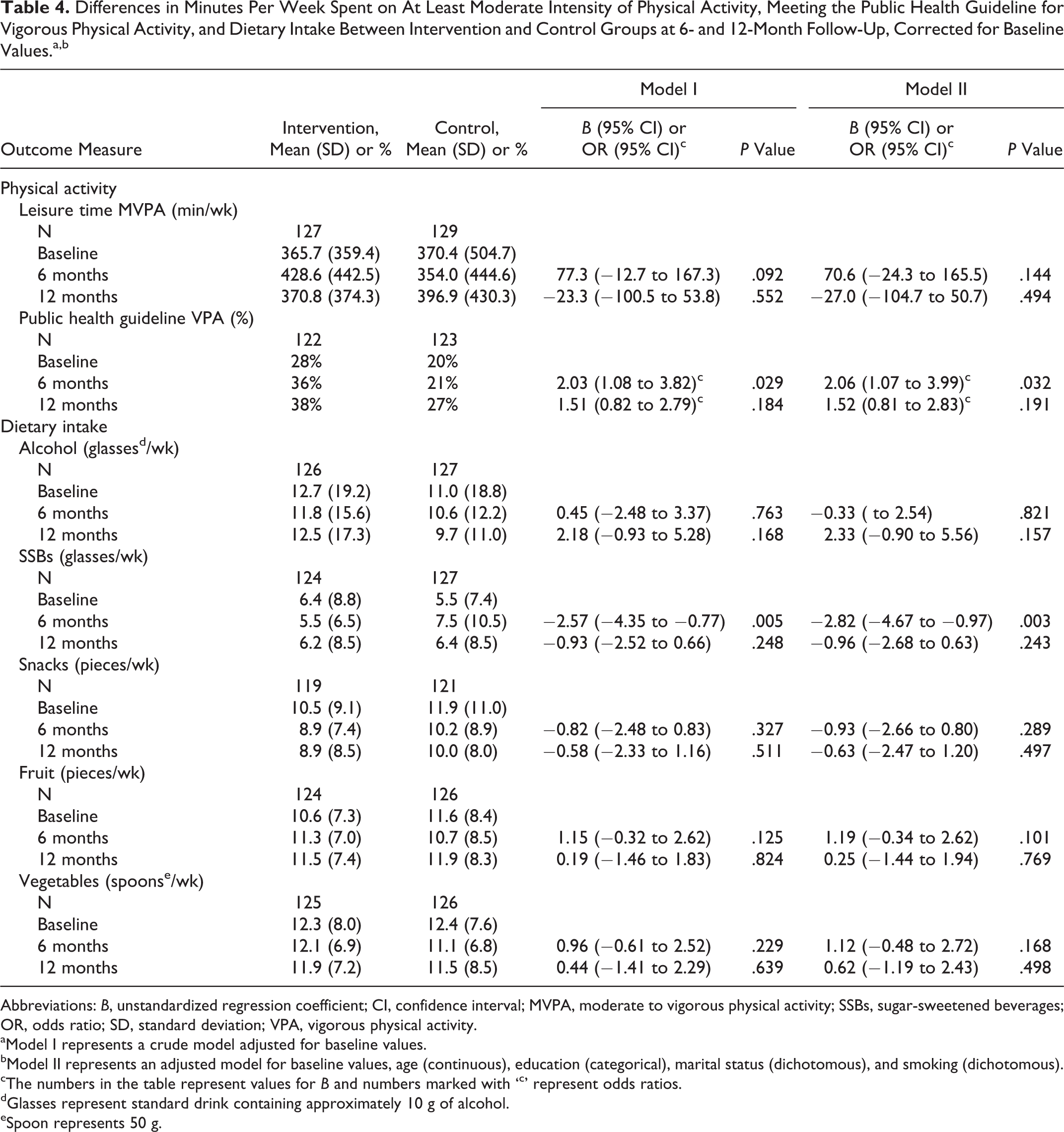
Abbreviations: B, unstandardized regression coefficient; CI, confidence interval; MVPA, moderate to vigorous physical activity; SSBs, sugar-sweetened beverages; OR, odds ratio; SD, standard deviation; VPA, vigorous physical activity.
aModel I represents a crude model adjusted for baseline values.
bModel II represents an adjusted model for baseline values, age (continuous), education (categorical), marital status (dichotomous), and smoking (dichotomous).
cThe numbers in the table represent values for B and numbers marked with ‘c’ represent odds ratios.
dGlasses represent standard drink containing approximately 10 g of alcohol.
eSpoon represents 50 g.
Physical Activity
No intervention effects were found on leisure time MVPA (Table 4). At 6 months, the intervention group participants increased their leisure time MVPA, but no significant intervention effect was found (B = 70.6, 95% CI: −24.3 to 165.5). At 6 months after baseline, there was a significant intervention effect on meeting the public health guideline of vigorous PA (OR = 2.06, 95% CI: 1.07 to 3.99). Participants in the intervention group meeting the guideline increased from 28% to 36%. After 12 months, there was no significant difference between the intervention and control groups.
Dietary Intake
A statistically significant intervention effect on intake of SSBs was found after 6 months (Table 5). Participants in the intervention group decreased their intake with 1 glass per week, while control group participants increased their intake (B = −2.82, 95% CI: −4.67 to −0.97). At 12 months after baseline, no effect was found on SSBs (B = −0.96, 95% CI: −2.68 to 0.63). No significant short-term or long-term intervention effects were found for any of the other dietary outcome measures.
Body Weight (kg) by Subgroups of BMI (Normal Weight, Overweight, and Obese) for Complete Cases at Baseline (Mean, SD) at 6- and 12-Month Follow-Up in the Intervention and Control Groups.
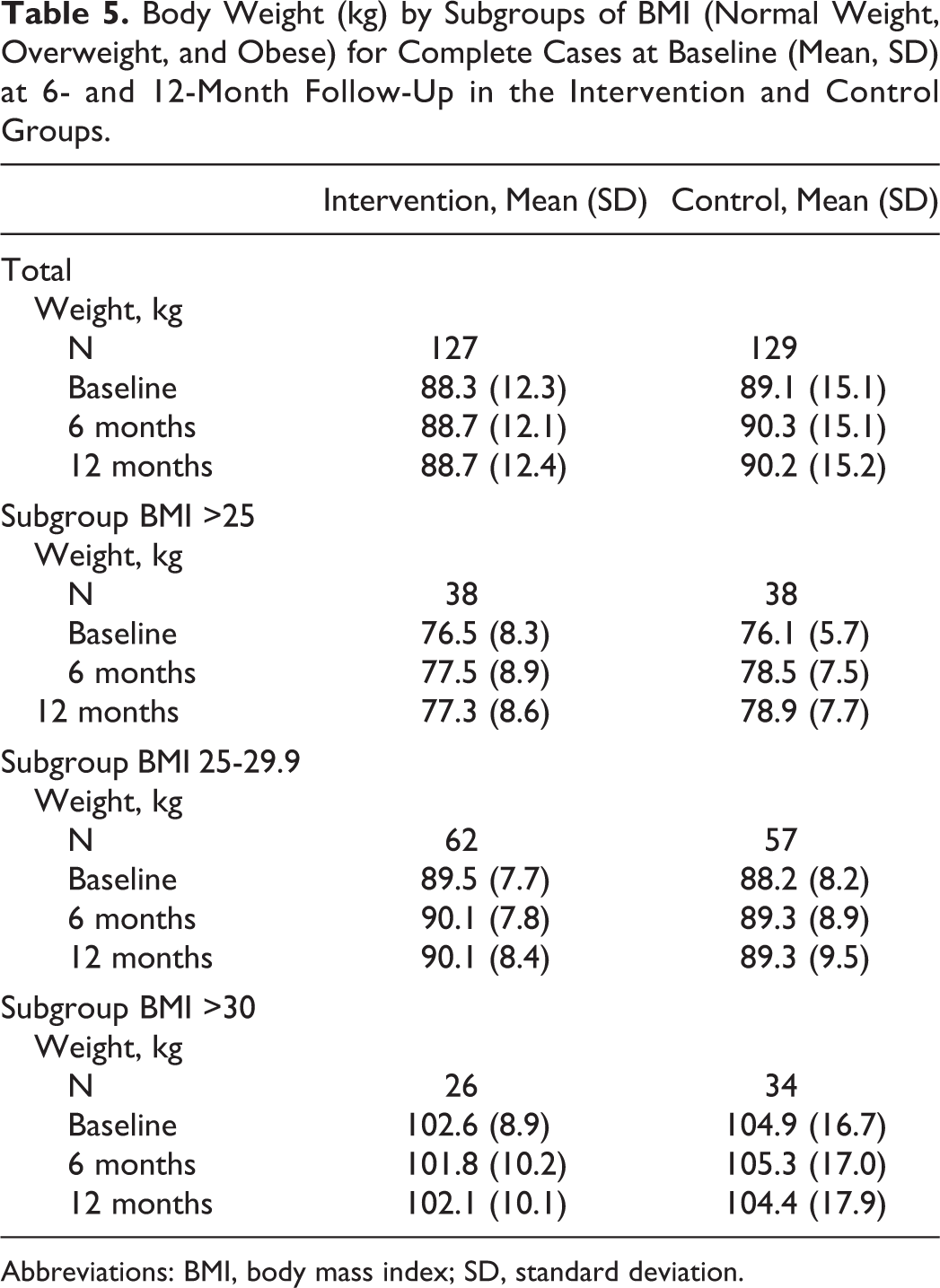
Abbreviations: BMI, body mass index; SD, standard deviation.
Discussion
Overall, the VIP in construction intervention positively impacted the intake of SSBs and the percentage of those meeting public health guidelines for vigorous-intensity PA and resulted in short-term favorable body weight–related outcomes when compared to usual care. Our results indicate no effectiveness of the intervention in modifying blood pressure or cholesterol levels in construction workers.
After the intervention period, although intervention participants showed significant positive changes in PA and dietary behavior measures, these effects did not translate into body weight loss. Although changes in mean body weight and BMI were negligible across the intervention period for the intervention group, the control group participants gained weight at 6 months, which resulted in an intervention effect on body weight and BMI. Furthermore, the intervention group participants showed a decrease in waist circumference, which resulted in a significant intervention effect on waist circumference at 6 months as well. At 12-month follow-up, differences were slightly smaller and no longer statistically significant.
Some worksite intervention studies have shown long-term effects on diet and PA behavior, 29,30 while in blue-collar worker populations, studies targeting PA and/or diet showed mixed results on body weight and BMI. 31 -34
Weight-Related Outcomes
From the perspective of many worksite health promotion programs, and the trend in increasing body weight in the control group in the present study, preventing weight gain may be a positive and a realistic outcome. The net effects on body weight as found in our study are modest compared to other worksite interventions that report outcomes ranging from −1.2 to −1.3 kg and from −0.3 to 0.5 kg/m2 for BMI. 15,35 An explanation for our modest results might be that participation in this worksite health promotion trial was not restricted to workers with overweight. The intervention targeted workers both with current overweight or risk of future overweight due to other lifestyle behaviors (eg, diet, PA, alcohol). In contrast, other weight loss interventions only include participants with overweight or obesity, and consequently weight loss results are likely to be larger. Therefore, our results on body weight are not directly comparable to those in the literature. Still, the lack of more impressive weight loss results in this study raises questions about the relevance of the effects in practice. Clinically relevant weight loss is associated with an improvement in the clinical risk of adverse health problems. 36 Although often weight loss of 5% has been indicated as clinically relevant, even smaller reductions in weight have been shown to result in clinically meaningful reductions in important CVD risk factors and in risk of diabetes. 37,38 This indicates that very small reductions in body weight could be considered relevant. Prevention of body weight gain may not appear clinically meaningful. However, given the importance of primary prevention and the difficulty of losing weight and maintaining weight loss long term, this should be considered with regard to weight gain that typically occurs in adults with obesity-related health problems. To date, very few studies have evaluated the effectiveness of these prevention programs and their effect on health. 39
The goal of the intervention was to improve lifestyle behaviors that would be easy to implement and could be maintained over time. These types of interventions can be incorporated into or linked to routine health screening, which potentially increases reach as well as the likelihood of implementation. It is important to emphasize that the intervention was not designed to maximize short-term weight loss. The lack of overall weight loss in the intervention group could be attributed to intervention intensity. In other studies where weight loss has been a primary outcome, more intensive approaches have typically been more effective than those with less contact. 40,41 However, such intensive approaches have a number of limitations. High-intensity programs are not only more expensive but also likely to appeal only to a small percentage of those who would benefit because of the level of commitment required. In the present study, even though the coaching sessions mostly took place during working hours and at the workplace, some participants indicated lack of time as a reason not to participate or did not complete all contacts. 42
It has been suggested that waist circumference is more sensitive to changes in energy balance than is BMI. 43 -45 In the present study, the overall effect on waist circumference was not accompanied by reduction in body weight. Although reductions in central obesity are larger when accompanied by weight loss, increases in PA have been associated with significant reductions in waist circumference, despite small or no changes in body weight. 46 The BMI reflects lean tissues as well as body fat. The PA provides metabolic adaptations that are associated with reductions in abdominal fat and increases in fat-free mass (skeletal muscle mass) as well as metabolic efficiency of muscle. 47,48 Since a substantial percentage of the study participants had a baseline waist circumference representing a health risk (>102 cm), the effect on waist circumference is considered relevant. Even more so because this specific group of workers has a high prevalence of musculoskeletal disorders, which are found to be associated with central obesity. 28,49
Physical Activity and Dietary Behavior
Both changes in intake of SSBs and PA could have contributed to the effects on weight-related outcomes. The intervention showed a positive effect on meeting the public guidelines for vigorous PA. However, no intervention effects were found for leisure time MVPA. This is in line with the study of Groeneveld et al 50 who suggested that lack of effect may be related to average high levels of baseline PA at work for construction workers. Furthermore, the SQUASH questionnaire was not designed to measure energy expenditure and changes over time but to give an indication of habitual PA level. 23 It has been suggested that high-intensity activity measures might be more reliable, presumably because these activities are easier to recall. As a result, responsiveness in measures of more intensive levels of PA could be higher. The intervention effect on decreased intake of SSBs could have contributed to the effect on weight-related outcomes. Intakes of SSBs have been found to significantly contribute to increased caloric intake and higher body weight. 51,52
Although short-term postintervention effects were found, comparable to other weight loss or weight gain prevention studies, 53,54 maintaining health behavior changes and effects on weight-related measures remains difficult. In general, this might be a result of relapse (not maintaining behavior change) in the intervention participants. A decrease in between-group differences could also be the result of changes in favor of the control group participants. The measurements conducted for the evaluation of the study effectiveness itself may have motivated control participants to improve health-related behavior. In addition, contamination between the intervention group participants and the controls could not be completely ruled out. Contamination of the control group was expected to be minimal, since personal coaching was only available for the intervention participants. However, behavior change in colleagues, especially dietary behavior at work, could have influenced control participants. This could partly explain the decreased contrast in outcome measures between the 2 groups at 12-month follow-up.
Strengths and Limitations
A main strength of the present study is that it was designed as an RCT. Randomization was performed at the level of the individual, which reduces the probability of confounding factors resulting from baseline differences between the intervention and control participants. Another strength was that the intervention was tailored to the individual worker, which might be especially important in a heterogeneous group of workers (eg, ranging from crane operators to bricklayers) and when intervening on complex behaviors.
Several methodological limitations deserve attention as well. Diet and PA were measured by self-report. Therefore, social desirability may have resulted in an overestimation of fruit and vegetable intake and underestimation of snack, alcohol, and SSBs intake, particularly in the intervention group participants. 55 Further, we did not use validated food frequency questionnaires. The dietary intake questionnaire used was tested for face validity by experts on nutrition and lifestyle change and comprehensibility by construction workers. Accurate assessment of actual behavior, and using more objective measures without imposing a large burden on respondents (especially in occupational groups where illiteracy is present), remains challenging.
Recommendations for Future Research and Practice
Future studies should include objective measures of PA. Accurate assessment of total PA levels (leisure time as well as work related) will improve the ability to give tailored advice. It will also enable better assessment of possible effect modification by strenuousness of work-related PA in intervention effectiveness. The latter might hold especially true for construction workers—as in our study—a population in which activity is part of their daily job routine.
Further, worksite health promotion research should aim to identify interventions to achieve sustained energy balance-related behavioral change. There is still little evidence from trials on effective long-term strategies. From observational studies, it is suggested that, for example, continued intervention contacts (face-to-face or by e-mail) 56 or continued self-monitoring of weight 57 lead to sustained effects on body weight–related outcomes. Complementary intervention components at company level, for example, strategies to enhance social support by colleagues and supervisors, might also reinforce sustained effects. 58 Also our program, although it appeared feasible for blue-collar workers with a relatively low-intensity intervention, only showed promising short-term effects. The program needs to be adapted to improve long-term effectiveness before implementation in the current setting or a broader one can be recommended.
Conclusion
The results of this study indicate that a relatively low-intensity worksite intervention has the potential to improve the intake of SSBs at 6 months and the percentage of those meeting public health guidelines for vigorous-intensity PA in blue-collar construction workers and to contribute to the prevention of body weight gain. Further research is needed to improve long-term effectiveness, and insight into effectiveness might be increased if more objective measures of PA and diet are used.
So What? Implications for Health Promotion Practitioners and Researchers
What is already known on this topic?
In the literature, evidence is found for the effectiveness of worksite physical activity and dietary behavior interventions on weight outcomes. The prevalence of overweight and obesity in blue-collar construction workers is higher than in the general adult population; however, no effective weight management programs have been found targeted at this specific occupational group.
What does this article add?
The effectiveness of a newly developed targeted and tailored intervention is assessed in a randomized controlled trial. The relatively low-intensity lifestyle intervention appeared feasible for blue-collar workers with promising short-term effects.
What are the implications for health promotion practice or research?
Before implementation can be recommended, the program needs to be adapted to improve long-term effectiveness. It is recommended that for successful weight management, further worksite health promotion research aims at identifying methods to achieve long-term sustainable impact.
Footnotes
Author’s Note
LV was involved in the design, protocol, and data collection of the study, and she drafted the manuscript. All authors contributed to the manuscript by reading and correcting draft versions. All authors approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is part of the research programme “Vitality in Practice,” which is financed by Fonds Nuts Ohra (Nuts Ohra Foundation).