
Abstract
Purpose:
The purpose of this study was to explore gender-related factors that motivate and support men’s smoking reduction and cessation to inform effective men-centered interventions.
Approach or Design:
Focus group design using a semi-structured interview guide.
Setting:
Three communities in British Columbia, Canada.
Participants:
A total of 56 men who currently smoked and were interested in reducing or quitting or had quit.
Intervention:
N/A.
Methods:
Data collected in 6 focus group discussions were transcribed and analyzed in accord with principles of thematic qualitative methods.
Results:
We report the results across 4 interconnected themes: (1) the fight to quit takes several rounds, (2) the motivation of supportive competition, (3) challenges and benefits of connecting with smoke-free peers, and (4) playing up the physical and financial gains.
Conclusions:
Masculine-based perspectives positioned quitting alongside fighting for self-control, competing, connecting, physical prowess, and having extra cash as motivating components of programs to engage men in efforts to be smoke-free. It may be worthwhile to consider the inclusion of gain-framed and benefit-focused messaging in programs that support men’s tobacco cessation.
Purpose
Tobacco remains one of the leading preventable causes of disease and death. Mortality related to common diseases such as lung cancer, chronic obstructive pulmonary disease , heart disease, and stroke have been directly linked to cigarette smoking. However, recent research indicates that the categories of diseases linked with smoking also include infections, hypertensive heart disease, renal failure, intestinal ischemia, and other respiratory diseases. 1 Smoking cessation programs provide an important way to significantly reduce morbidity and mortality.
Smoking rates among men are notably higher than women in many countries. For example, in Canada more men currently smoke (18.4%) than women (13.9%), with the highest smoking prevalence among young adult men aged 25 to 34 years (26.6%). 2 In the United States, men are also more likely to be smokers; 20.5% of men smoke compared with 15.3% of women, and among 25- to 44-year-old men 26.8% smoke. 3
Among various subgroups of men, smoking prevalence is more than double the population average. Among men who have sex with men, 50% smoke 4 ; in nonclinical populations of men living with post-traumatic stress disorder, 34% to 61% smoke, 5 and among blue-collar occupations, such as construction, 43% of the men smoke. 6 As well, more men (18%) than women (12%) have attempted to quit smoking 4 or more times in the past year, 2 a fact confirming both the interest and challenges men experience in their quit attempts.
There is increasing evidence for the value of developing gender-specific health programs. 7 Despite this evidence, however, few men-centered smoking cessation interventions have been developed and/or formally evaluated. A review of men-specific cessation programs identified 11 studies, and only 2 of these studies reported smoking cessation treatments specifically tailored for men. 8 Smoking cessation interventions have been developed for fathers 9,10 that prescribe positive messaging to promote change, without shame and blame, by connecting to men’s positive identities, such as the desire to be healthy and strong and provide for their families. Other than Canadian-based resources for new fathers, there is a dearth of men-centered cessation programming. Masculinity as a factor influencing men’s health has been widely theorized 11 ; however, the role of masculinity in men’s smoking cessation strategies is still emerging. The following research question guided this study: What are the gender-related factors that motivate and support men’s smoking cessation and therefore might inform effective men-centered interventions?
Approach and Study Design
This research employed a social constructionist gender frame, which theorizes masculinity as a performative construct that is reproduced by social relations and social institutions. 12 Within the context of tobacco use, smoking has been theorized as a gendered cultural practice and associated with masculine behaviors that display physical invulnerability, strength, toughness, and stoicism. 13 Unlike psychological trait- or role-based theories that position gender as a static and individual-based factor, a social constructionist view holds masculinity to be context-dependant, dynamic, fluid, and plural, constituted by social relations that produce identities entwined with power and class. This approach also meshes well with health-promotion strategies that are gender-informed by the capacity to appeal to masculine identities within the specific context of men’s lives.
Focus group research was used to explore men’s attitudes, beliefs, and experiences 14,15 in relation to smoking and efforts to quit. The study took place in Canada where tobacco control policies have reduced smoking rates. The focus group sessions were held between October and November 2013 following university ethics approval.
Setting
The focus groups were held in 3 communities in British Columbia, Canada.
Participants
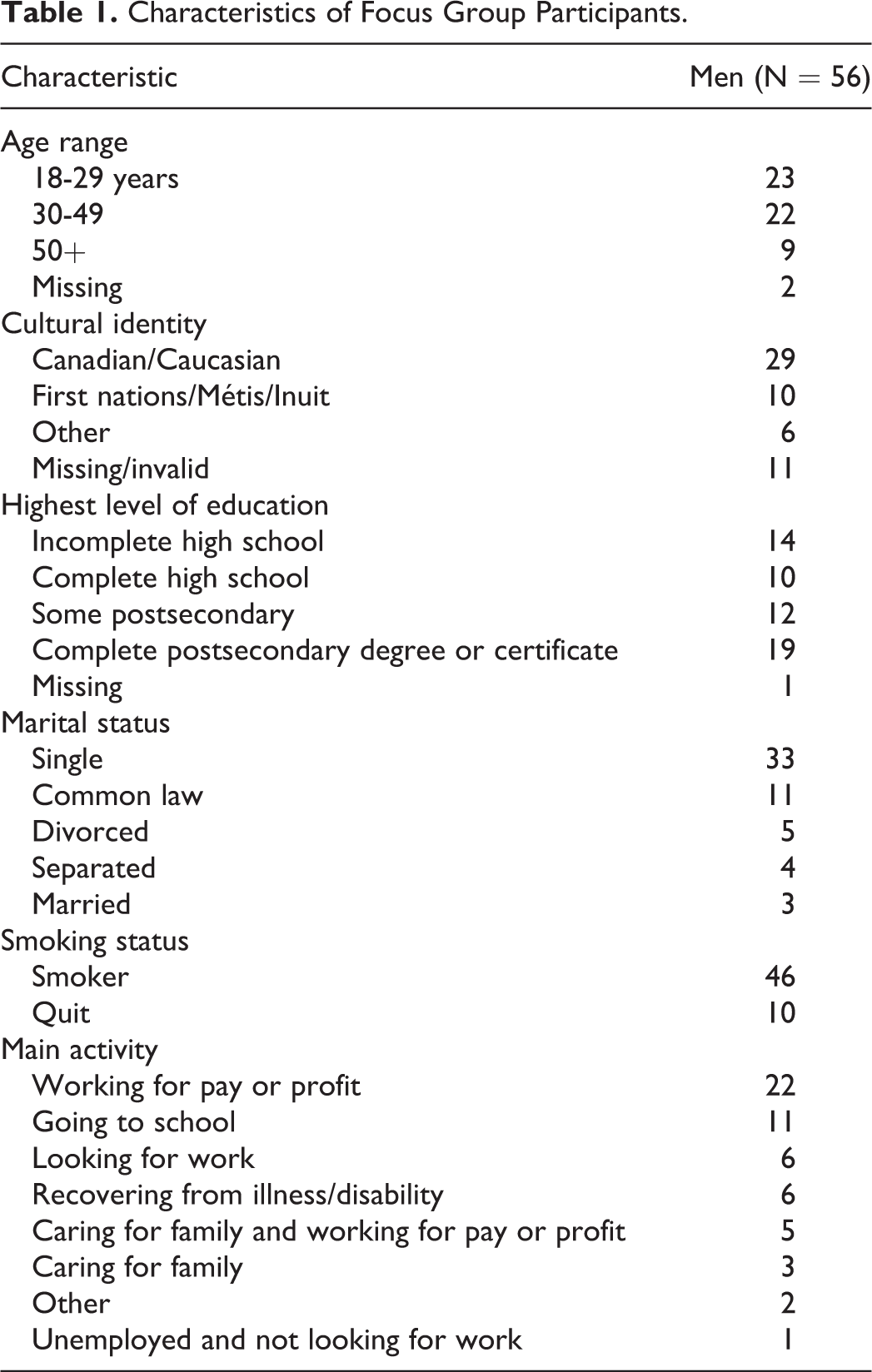
Fifty-six men were recruited from 3 locations in British Columbia, Canada, using a combination of posters and Web-based (Facebook, Kijiji, Castanet) strategies. The majority of the participants currently smoked (n = 46) and were interested in reducing or quitting; some men (n = 10) had previously quit smoking. We purposely recruited men with varied smoking histories to ensure the capture of diverse experiences and perspectives on smoking cessation efforts (see Table 1 for participant characteristics).
Characteristics of Focus Group Participants.
Method
Data Collection
Two members of the research team (G.S. and P.S.) facilitated the focus groups. The facilitators followed a comprehensive protocol to guide the group discussion. The size of each focus group ranged from 5 to 12 participants and the duration of each session was approximately 3 hours. A consultation-style approach was used to encourage discussion wherein the men participating in the groups were viewed as experts on the topic of what they do, thought, and believed. 16 Semi-structured, open-ended questions were used to stimulate dialogue, promote interaction between participants, and encourage participant self-disclosure without unduly influencing or leading responses. The facilitated discussion focused on the following topics: perceived benefits of quitting, primary motivators for changing smoking behaviors, the usefulness of various strategies to support cessation, and suggestions for designing smoking cessation resources for men. All perspectives on the topics were welcome. In addition, the discussion was interspersed with interactive activities to provide additional opportunities to share ideas and opinions. For example, participants drew pictures of their main motivators for quitting and shared preferred smoking cessation supports by writing strategies on posters. They also viewed and provided feedback on several video testimonials about reducing and quitting smoking (https://www.youtube.com/watch?v=UCoz0Y5TlXI; https://www.youtube.com/watch?v=zDHTttnIENQ). Example questions included “How helpful is it to hear from other men about their experiences reducing and quitting smoking?” “What other types of stories would be helpful to support men’s efforts to reduce and quit smoking?” and “What kinds of quit smoking supports do men most need?” All participants provided written informed consent prior to data collection and received a CDN$50 honorarium to compensate for their time and travel costs.
Analysis Strategies
The focus group sessions were audio recorded and transcribed verbatim. Thematic analysis, an approach wherein patterns in the data are identified and described to interpret and explain various aspects specific to the research topic, was employed. The process of analysis included familiarization with data, generating initial codes, allocating data segments to the codes, sorting codes to identify potential themes, reviewing themes to determine if they worked in relation to the data, and naming and refining the themes. 17 The coding framework was developed by the team and all data were independently coded by 2 of the researchers (P.S. and G.S.). The coding framework included 20 initial codes (eg, barriers to quitting; benefits of quitting; clean living; coping strategies; self-control; smoking experiences; views on addiction, health, and fitness; etc). Coded data were reviewed examining similarities and differences within and among the focus groups, and important insights were described and underpinned the development of overarching themes. Overall, the participants’ responses were fairly consistent across the groups, however, divergent views were noted when they occurred and considered in the analyses. Nine preliminary themes were identified from the initial codes and reviewed in relation to coded data extracts, as well as the entire dataset, to determine if the themes accurately reflected the data. 17 The preliminary themes included (1) connecting to peer support, (2) benefits of improved physical health—breathing and working out, (3) stories about the process of quitting and failing—building confidence, (4) technology—getting connected with positive reinforcement, (5) competition with other men, (6) community and group support—finding smoke-free friends, (7) financial savings—calculations and reinforcement, (8) nicotine replacement therapy resource information, and (9) women as motivation and support—or not. A thorough review of these themes and related data occurred in team meetings, and several themes were collapsed and named, resulting in 4 coherent, meaningful themes with identifiable distinctions. These thematic findings were further refined using collated data extracts for each theme and were theorized using a gender lens focused on masculinities and men’s health. 12 The systematic and theoretically informed approach to analysis, along with monitoring and confirming the conceptual work related to theme development, contributed to the reliability and thus rigor of the study. 18
Results
Four interconnected themes were identified: (1) the fight to quit takes several rounds, (2) the motivation of supportive competition, (3) challenge and benefits of connecting to smoke-free peers, and (4) playing up the physical and financial gains. The themes reflected the tensions around conforming to and challenging norms about smoking and cessation as masculine practices. For example, despite the language of “the fight” to quit, cold turkey quitting without smoking cessation aids (eg, nicotine replacement), a quit method associated with stoic toughness and willpower was not valorized by participants. Similarly, although the men identified competition as highly motivating, it was tempered as a “supportive” form of competition. In desiring to connect with smoke-free peers, the men challenged the autonomy and independence characteristic of traditional masculinity; they did not want to go through the quitting process independently or alone, but instead they sought connection to and mutual help with other men. And finally, the men’s insistence that the physical benefits of quitting would be motivating contradicts long-held notions that masculinity and self-care, or self-health, are mutually exclusive. Nonetheless, despite contesting hegemonic masculine codes of behavior, participants’ perceptions about the appropriateness of specific quit aids and the nature of those social connections were also scripted in line with an array of typical masculine ideals including the notion of a good fight, the enjoyment of male competition, the influence of buddies, and monetary savings. Within this context, each theme is discussed in regard to how masculine ideals worked for and against men’s cessation efforts.
The Fight to Quit Takes Several Rounds
The men said they wanted to hear about the “real” process and grind of a quit, as opposed to testimonials that narrated retrospectively a man’s success without difficulty. Personal stories about how a man succeeded in stopping cold turkey, including the professional intervention videos that participants viewed in the focus groups evoked little approval among the men. Interspersed throughout the group discussions was a dismissal of independent quitting approaches and stereotypical notions of men who quit on their own by drawing on willpower and personal strength. Hearing about a man who succeeded after making several attempts was said to represent a more realistic and compelling scenario. The presentation of uncomplicated quits belied the men’s struggles to quit by rendering their inability to action a decisive quit as a sign they could be meek, weak, and/or fraudulent in their claims about wanting to be smoke-free. Several participants talked about the need to build failure into the quit videos: P1: Find a guy who quit but maybe couldn’t quit right away. Like they had trouble and talk about what went wrong those first couple times they tried. P2: Yeah, like they failed and they quit and they failed and they quit and then they succeed. P3: Take these ideas and have three thirty second slots about the story of the guy, like ‘Oh I’m going to do it and then relapsed’ but then you know, ‘I’m getting stronger sort of thing’, you could span them out. Facilitator: So you want to see more of the struggle? Is that what you are saying? P: Yeah, well not necessarily the struggle, but I… Facilitator: Or the challenges… P: The fight [drew nods of agreement from the other participants] Yeah…because very few things in life are absolute, you are not either right or wrong, or good or bad, it’s always this constant staying above or below the line, and that should apply equally to smoking, you cut back, that’s a great thing, you didn’t manage to quit, well, you cut back, you know, or whatever.
The Motivation of Supportive Competition
Participants indicated they preferred engaging and interactive content such as quizzes and polls related to tobacco use and cessation and were keen to know how they compared to the other men who served as reference points to evaluate performance. As 1 participant confirmed, “If you want to engage men, make them compete [laughter].” Similarly, another drew parallels to health promotion focused on physical activity and healthy eating in suggesting measureable outcomes defined the competition: Like the Web site MyFitnessPal where people share their fitness goals and they have a competition to see who can lose the most weight, stuff like that, I think if you took smoking in that sense it could help, see who can quit fastest, the most effectively. P1: It wasn’t just about the competition, it was about the support, right. So having support could help too. P2: Yeah. I could second that for sure.
The competition in and of itself was enough for most participants. Indeed, some men refuted the legitimacy of tangible rewards authenticating the competition and incentivizing performance toward being smoke-free. In this respect, men refuted the need for gimmickry, internalizing the rewards as flowing from being healthier. As a participant countered, monetary rewards could be a disincentive to sustaining a quit: I just quit because I wanted to quit so why are you giving someone else money. That’s their health, that’s their life, they need to figure that out. If you’re giving someone money for something that they should do for themselves then you’ve ruined it.
A few men tempered their reliance on competition to signal personal bests as the yard stick to gauge their success. As one man said, “Whether you’re competing with someone else or yourself you’re still trying to make yourself better in a way.” Competition, in all its iterations, represented the power of men connecting with each other to establish new norms (ie, being smoke-free). Within the context of friendly competition, the actions of other men provided permission for the participants to do health (ie quit smoking). This revisionist perspective of competition, which included male comradery and personal bests, is perhaps a modification of more ruthless notions masculine competitiveness.
Challenges and Benefits of Connecting With Smoke-Free Peers
Within the group activities, men shared their ideas and experiences related to quitting, and the conversation often gravitated toward the importance of peers. Male peers with firsthand knowledge of “what it was like” to smoke and to go through smoking cessation were viewed as most helpful: Yeah because you would want to talk to someone who smokes, you don’t want to speak to someone that hasn’t smoked and is just giving you advice because you just go, “You haven’t got a clue as to what’s going on in my head right now.” I’d rather talk to someone that’s going through the same thing…I don’t want to talk to a machine or someone that doesn’t know what they are talking about. [Facilitator: So it’s gotta be peers?] Yeah it’s gotta be peers…[If] all the guys or whatever that are wanting to quit smoking, you can shoot off a [text] “I’m losing my head, this is what’s going on. Anybody have any ideas of how to get through this?”
In giving up smoking, men’s identities were challenged and it is perhaps in this context that a personal connection with familiar men became important and, as illustrated here, strongly influenced men’s views about the best forms of support for cessation. In line with this, the participants generated various types of relational support they believed would be more helpful than independent quitting supports, including a peer buddy system, joining a face-to-face group of men quitting, a group weekend immersion for men quitting, a “boot camp” for men quitting, and a residential nicotine withdrawal retreat. Online forums and phone apps were viewed as acceptable if they had the right mix of “actual people” to make them personal.
Although men recognized the value of connecting with other smoke-free men to support and motivate a quit, this was also challenging because most of the men who smoked acknowledged that they were surrounded by smokers in their social and family circles and had limited access to smoke-free friendships. Furthermore, the women in men’s lives were often smokers and as such were not positioned as smoke-free allies. While some men claimed they had relapsed because their female partners or girlfriends were smokers, others asserted that women had little power or influence over their smoking. One exchange reflects this sentiment: P1:…if you liked a girl and she didn’t like you smoking, would you change? P2: I mean you could try but no, too bad. I’ll quit eventually if it’s worth it, but I’m not gonna just not smoke because she wants me to.
Playing Up the Physical and Financial Gains
A constant refrain regarding smoking among the majority of the men was a strong desire to feel healthier; they said they wanted to breathe easier and exercise without wheezing. For example, one man said, “I cannot take a breath sometimes.” Another man described worrying about future health risks “like cancer and heart disease.” He stated, “Heart disease is in my family history, so really [its] always on my mind, [stop] smoking, breathe easier and cough less.” The men with families wanted to be healthy role models for their children.
Though the men understood the embodied changes caused by smoking, they were firm in their contention that knowledge about the negative health consequences was not enough for them to sustain a quit. Witnessing a family member with emphysema or other illnesses caused by smoking did not motivate them to quit either, because as one participant explained, men would rationalize, “I’m not as bad as that guy.” Instead they wanted information about the advantages of quitting and strategies to sustainably replace smoking with positive healthy activities: I just think that if you replace it with something positive you get to see the benefits of something positive. You know, like instead of smoking in the morning, working out, so you start to see the benefits of not just, okay I’m not smoking but I’m getting in shape. P1: Well the other thing, over a lifetime, the cigarettes that you buy and smoke ‘cause about half the money you earn almost, you know… P2: That’s crazy, eh. Facilitator: Is anyone else here concerned about cost? P3: Definitely a motivator… P4: Oh yeah. P5: It gets more expensive every day that goes by, you just try to keep up. Yeah it’s the same thing as me, it’s been 3 months or so that I’ve stopped. And you mentioned not spending the money on the cigarettes, [now I have] gym money, so I get to run and feel a bit better about myself. Yeah so you put in your body stats right, your BMI or whatever, your eating habits, and you’ve got a life expectancy. It’s like I smoke two packs a day so “guess what buddy, you’re going to die at sixty”. Okay well I quit smoking, well geez that just went up to eighty.
Conclusions
The findings from the current study reveal that cessation efforts among these men reside outside the authority of biomedical expertise and pharmacological aids. Evident is the resourcefulness of men and collective power residing in communities of practice invested in change. 20 Not to be overly optimistic, however, according to the responses of the men in this study, the things many men are known for—self-control, competing, comradery, physical prowess and having extra cash—have potential to aid men’s efforts to be smoke-free.
From a theory viewpoint, it may be that the masculinities framework used to unpack men’s health issues has a limited shelf life. Incumbent on us all is the work of describing gender and masculinity outside the confines of hegemonic masculinity in order to recognize the plurality of masculinities. For example, the findings presented here that depict masculine behaviors as potentially health-promoting can—and perhaps will—be critiqued as perpetuating destructive aspects of masculinity. Although it is not possible to generalize the findings from this qualitative study to broad populations of men or to assume these findings are reflective of masculine identities only, the men’s suggestions provide potentially useful directions for effective cessation programs for men. Recognizing that the findings of this study are influenced by gender norms and tobacco control efforts in the study setting, our findings suggest key supports that might be incorporated or pilot tested as program principles to support men’s cessation. These include the importance of authentic narratives acknowledging the fight needed to quit, friendly competitive activities that engage men in quitting, the need for relational support from men who are quitting as well as smoke-free buddies, and a desire to focus on the physical and financial benefits of quitting, rather than the risks of smoking. Central to these guiding principles is the recognition that masculine values and virtues can drive men’s behavioral change and practices related to tobacco use. 21
Online environments have been proposed as particularly appropriate for advancing men’s health because electronic resources can reflect a range of masculine voices and images and hold potential for supporting men’s preferences for self-management. 22 –24 Although online smoking cessation Web sites have the capacity to offer low cost, engaging, multicomponent resources within the context of a men-friendly Internet environment, the findings of this study indicate that current online smoking cessation resources may need to be modified to better address men’s preferences and needs. The importance of men’s preferences is a key consideration, given most individuals seeking cessation help online do not rate the Web sites they have used as particularly helpful or satisfying. 25 From the perspective of public health goals, the Internet has an enormous capacity to deliver cost-effective interventions to millions of men, and Internet-based tailored, interactive programs have proved their efficacy by delivering higher quit rates than usual care or printed materials. 26 However, if such cessation programs are to go beyond their yet modest results, perhaps Web site developers might ensure men’s identities, which are represented by markers such as age, class, ethnicity, and occupational status, are incorporated along with evidence-based strategies.
The findings also indicate we may also need to pay attention to the overall approach to messaging men about smoking cessation. As a consequence of being oversaturated by health-promotion campaigns focusing on the health risks of smoking, men in this study were largely uninterested and desensitized to these risk-reliant messages. The ineffectiveness of these loss-framed messages might also be interpreted as a reaction to challenges to masculine identities of strength, hardiness, and invincibility, as well as inadvertent support for men’s risk-taking behavior. The participants expressed a clear desire for information about the positive aspects to smoking cessation (gain framed). This finding is confirmed by other research evidence indicating that gain-framed messaging may be more effective than deficit loss-framed messaging for supporting cessation. 27 By highlighting what men stand to gain from quitting, the emphasis is taken away from the failure to perform self-health and placed on increasing self-control. Participants in the present study identified numerous suggestions of how to garner men’s attention through gain-framed messaging to empower and shift smoking-related beliefs, attitudes, and behaviors in the direction of cessation.
The degree to which these findings can be generalized are limited by the sample size and the means of recruitment. It is possible the composition of men who responded to the research opportunity held skewed views about smoking cessation. There are also limitations characteristic of all focus groups: the challenge of balancing equal participant contribution and transcription oversight that may occur due to multiple simultaneous speakers. A final limitation is related to reliability. Because 2 members of the research team coded data independently, it is possible they may have interpreted and coded the raw data differently. However, the identification of the codes involved consensus of the team, a practice that helps to ensure that the meaning of codes is the same among coders. This along with a collaborative team approach to monitoring and confirming the conceptual work related to theme development supports the rigor of this study. Finally, the theoretical reliance on a social constructionist gender frame may have obfuscated nongender factors in men’s smoking cessation.
In summary, the men in this study offered specific suggestions for the kinds of support they would find helpful to quit or reduce smoking; for the most part, these suggestions extended beyond expert biomedical approaches to cessation and emphasized how social connections among men who are focused on benefits hold more power and interest to motivate and sustain a quit. These suggestions provide a foundation for innovations in smoking cessation programs for men.
SO WHAT? Implications for Health Promotion Practitioners and Researchers
What is already known on this topic?
Gender-sensitive smoking cessation programs for men are few, despite the evidence that masculine virtues and values strongly influence tobacco use and cessation. Little is known about the kind of content men would find useful and motivating to support their desires to quit or reduce smoking.
What does this article add?
In a qualitative research study, we learned that men may be motivated by smoking cessation programs that emphasize the gains and benefits of quitting smoking, as opposed to risk-based medical messaging. This is one of the first studies to describe what men perceive to be supportive for quitting and reducing.
What are the implications for health promotion practice or research?
Men may be better engaged by smoking cessation resources that incorporate masculine-based features, such as narratives about the fight needed to quit, competitive activities, relational support from smoke-free buddies, and a focus on the physical and financial benefits of quitting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Canadian Cancer Society (Grant #701615) and conducted in collaboration with the B.C. Lung Association and QuitNow BC.