
Abstract
Remuneration in health care is a contested topic, with various pay systems rewarding equal services unequally. This study investigates the motives of 17 panel doctors in Austria and identifies dysfunctionalities in remuneration systems that do not guarantee optimal, outcome-oriented treatment. Using Vroom’s expectancy theory of motivation (1964), we analyse the behavioural motivation of doctors, considering both individual and environmental factors. We identify four types of panel doctors – profit maximisers, prestige seekers, altruists and system-compliant types – and explore how remuneration impacts their choices and outcome expectations. Our findings show that doctors’ motivations, shaped by their goals (e.g., quality assurance or leisure time), affect their performance. Regional context factors further inform the design of an outcome-oriented pay system. The study concludes with practical implications for health service providers and highlights future research directions.
Introduction
For many years, visits to doctors’ offices made us think about the effects remuneration can have on the motivation of medical doctors and consequently on the quality of care they provide. A visit to a privately-run joint practice specialised in ultrasound treatments helped to understand how strongly remuneration of doctors is connected to patients’ health care. According to the medical assistant, a treatment for both legs had to be performed on separate days because conducting the examination on both legs in one visit could not be billed to health insurance. This led to the second leg being examined by another doctor the following day. The initially highly motivated attending physician began expressing frustration over cost-cutting measures affecting doctors, showing clear signs of irritation and a noticeable decline in attentiveness compared to the second examination conducted by a colleague the following day. This prompted the question of how the apparent loss of remuneration impacts a doctor’s motivation and the quality of patient’s care.
The effects of remuneration on employee motivation have been widely discussed in literature (e.g., Cerasoli et al., 2014; Chapman & Kelliher, 2011; Gerhart & Fang, 2015; Lawler, 1971; Rynes et al., 2004; Shawn, 2011). The choice of remuneration as a human resource practice is not always based on an organisational strategy, but can depend on context factors (Wright & McMahan, 1992). We observe this with remuneration in the exceptional role of panel doctors who are ‘doctors within a given area available for consultation by patients insured under a national health insurance system’ and where state health insurances frame the remuneration system. Panel doctors are formally self-employed and work under standard contracts with health insurance bodies, often acting as independent contractors like ‘quasi-employees’. This interplay with remuneration as a context factor is of interest as it investigates into how doctors as ‘dependent employees’ respond to external incentives aiming at optimal performance.
The financial feasibility of health care and an extension of primary care are major concerns of social states but several scholars question the increase in attractiveness for doctors and concomitant positive effects on the quantity and quality of care (e.g., Davidson et al., 2015; Davies & Macfarlane, 2010; Kötter et al., 2011).
We address a motivational problem of panel doctors by questioning how remuneration systems can entice doctors to provide optimal service and simultaneously guarantee optimal health care. Remuneration systems allow either outcome- or performance-oriented medical service. Outcome-orientated care focuses on achieving optimal health results without over- or undertreatment of patients, aligning with both the panel doctor’s and health insurance’s objectives. In contrast, performance-based care focuses on the number of services provided according to the insurance’s service catalogue, potentially leading to over- and undertreatment of patients to maintain affordability. We aim to explore how these two motivational drivers, influenced by remuneration, impact health care delivery.
The research question guiding this study is: How does remuneration impact the medical treatment of patients, and how does this relate to the individual motives of panel doctors? Despite existing research on medical remuneration systems, the specific impact of financial incentives on panel doctors and the quality of health care remains underexplored. We address this research gap by examining the role remuneration plays in motivating panel doctors and how it influences health care quality.
We use Vroom’s Expectancy Theory of Motivation (1964) to analyse how remuneration impacts the motivation and behaviour of panel doctors. Vroom’s framework, which focuses on how individuals make choices based on expected rewards, provides a useful lens for understanding how panel doctors navigate the system of health insurance while trying to meet both societal demands and personal goals. Based on interviews with 17 panel doctors from various medical fields we suggest a typology of four panel doctors: those motivated by maximising profit, gaining professional recognition, behaving altruistically and complying with the system. This typology helps us identify the potential dysfunctions within health care systems driven by financial incentives.
The case of remuneration systems and motives of panel doctors is of interest for two major reasons. First, remuneration systems vary significantly across countries, including Austria, where health insurance payments include fee-for-service, capitation, and a small share of performance-based components. A theoretical analysis of financial incentives and the motivation of panel doctors can identify potential dysfunctions and suggest ways to modernise medical remuneration systems. Second, primary care focuses on the strong connection between doctors and patients, particularly in the context of chronic illness and should not aim at a pursuit of profit. Understanding how performance-based remuneration affects doctors’ behaviour can reveal why some might prioritise financial incentives over altruistic motives in patient care. Our findings highlight the critical role of remuneration in scheduling appointments, billing practices, and how certain services are delegated to locum doctors. In cases where remuneration is viewed as the primary motivator, it shapes the panel doctor’s performance behaviour and the provision of all further services.
In the following, we describe the specific context of Austria as the setting for our study, review existing literature on the relationship between motives and remuneration in medical professions, and introduce Vroom’s expectancy theory as the theoretical framework. We then present the empirical findings of our qualitative study with panel doctors in Austria, discuss the implications for health care quality and offer suggestions for improving remuneration systems based on these insights. Our contribution to the literature includes a nuanced understanding of panel doctors’ motives and a new form of panel doctors as system-compliant types.
The Case of Austria – Health Care System and Panel Doctors
As of December 2023, 50.631 doctors were in employment in Austria (ÖAK, 2023). Thereof, 8.300 were panel doctors, compared to 11.548 doctors of choice (Arthofer, 2024; Ärztestatistik, 2023). Whereas panel doctors are typically tied to specific health insurance networks, doctors of choice refer to the patient’s ability to choose any doctor freely without such restrictions, although the cost might be higher. Importantly, a doctor in Austria cannot be both a panel doctor and a doctor of choice at the same time, which creates a structural division in the health care system. This separation directly affects remuneration systems, as panel doctors operate within standardised, collectively negotiated payment schemes, while doctors of choice are reimbursed on a fee-for-service basis, often with higher out-of-pocket payments for patients. Since the health care reform in 2013 financial feasibility and primary care have become a crucial point in Austria’s health care agenda (HVB SV, 2018). In contrast to the strengthening of primary care Austria suffers from an increasing shortage of doctors, attributed to succession problems and bureaucracy (ÖAK, 2021) as well as unappealing remuneration (ÄKNÖ, 2019). As a consequence, health economists highlight dysfunctional effects of remuneration regarding overuse and shortage in medical supply (Czypionka et al., 2015; Janus, 2014). Based on international experience and theoretical findings Czypionka et al. (2011) conclude that the Austrian remuneration system with a mixture of fee-for-service, flat-rate payments and pay-for-performance has potential for improvement and claim a stronger focus on processes and putting services in relation to effort in order to eliminate distortive incentives. In fact, Austrian doctors are socialised in monetary incentives (Dragosits & Scheuringer, 2016; Kaiser et al., 2015) which bears the danger of over- or undertreatment of patients and raises the question of effectiveness.
Although Austria has a strong focus on a fee-for-service system with payments for separately listed individual services, a study by Jung (2016) shows that 75% of the total turnover in medical services is generated by flat-rate payments. The fee structure of the Federation of Austrian Social Insurance Institutions includes a relative low number of flat-rate items, still those are the ones most frequently billed, e.g., a capitation fee per registered patient. As a further shortcoming, the current remuneration system does not take a different rating of panel doctor’s individual goals into consideration. This leads to an ongoing debate about appropriate remuneration for panel doctors.
An essential characteristic of the Austrian health care system is a statutory compulsory health insurance with open access for all population groups to all levels of medical care (panel doctors, doctors of choice and hospitals). Holders of the statutory health insurance have free choice between medical service providers. Remuneration arrangements are determined on national level. Panel doctors have contracts with the Austrian state health insurance (Österreichische Krankenversicherung) whereby the amount of a doctor’s medical fee claims for provided medical services covered by state health insurance depends on the current official scales of fees for services along with supplemental agreements. Patients do not have to pay their doctors directly. An e-card serves as valid proof of a person’s insurance and acts as a voucher for payment of treatment. This is in contrast to doctors of choice where patients are free to choose their doctors but must pay for treatment up front. As long as a treatment is scientifically recognised, 80% of the treatment costs the health insurance would have paid a panel doctor can be reimbursed. Doctors of choice set their own fees freely which are generally higher than the rates paid to panel doctors, resulting in patients paying more out of their own pocket (City of Vienna, 2021). The system of panel doctors and doctors of choice can lead to a two-class medical system where patients change from panel doctors to doctors of choice as long as they can afford in order to get optimal medical care. The relationship between financial incentives and health care service quality has gained renewed attention, particularly in light of the VUG 2024 (Vereinbarungsumsetzungsgesetz) collective amendment. This recent health care reform initiative by the Austrian government emphasises primary health care expansion, team-based care, and remuneration restructuring (Schoenherr, 2024) and aims to address historical remuneration-related challenges like unequal pay, insufficient service coverage, and bureaucratic complexities.
Motives and Remuneration Systems in the Literature
Health care generally aims at social welfare, firmly positioned in the Hippocratic oath taken by doctors. Research underscores the relationship between financial incentives and motivation among health care professionals (Karaferis et al., 2022; Zhang et al., 2023). Recent studies further reinforce the importance of aligning financial incentives with health care quality, as health care professionals seek optimal combinations of intrinsic and extrinsic motivations (Karaferis et al., 2022; Aggarwal et al., 2025). Remuneration systems therefore function not only as tools for cost control but also as strategic levers for influencing provider behaviour and promoting desired health system outcomes (Heider & Mang, 2020) Czypionka et al. (2011) and Janus (2014) attempt in their literature reviews to theoretically explain an optimal compensation for medical performance. From an economical point of view a remuneration system is preferable which enables a demand-oriented and cost minimal health care provision of all citizens (Schulenberg, 1981; Thiemeyer, 1986). However, scholars address various motives in professional practice: altruism, recognition and profit maximisation. We therefore review literature according to the linkage between doctors’ motives and different remuneration systems and their impact on medical care.
Altruistic Motives and Remuneration
Several scholars address altruism and its interplay with remuneration in health care (e.g., Arrow, 1963; Ellis & McGuire, 1986; Jack, 2005). Arrow (1963) highlights the role of asymmetric information and specific aspects in health care industry to be considered in remuneration systems. Based on the assumption that a doctor as a medical service provider has more information on the health condition than a patient, the doctor’s interest in the patient’s benefit leads to more altruistic than profit maximising behaviour. Similarly, Ellis and McGuire (1986) argue an information advantage of doctors vis-à-vis patients in principal-agent-relationships where doctors are motivated by both altruism and profit. A patient who lacks information about the necessary range of treatment relies on the doctor’s recommendations, as the doctor has access to all of the patient’s health information. Ellis and McGuire (1986) address full reimbursement for rendered services, flat-rate payment and mixed forms of compensation which is considered most efficient. The authors further show that flat-rate payment works for doctors who are able to balance altruism and profit maximisation. A mixed form of compensation offers incentives for a socially efficient treatment if reimbursement is adjusted to the doctor’s level of altruism. The less altruistic the agent the higher the need for reimbursement. The model of Jack (2005) investigates into altruistic doctors who choose contracts with flat-rate payments and non-altruistic doctors who chose reimbursement of costs to show how a specially designed contract can lead to a self-selected move into different contractual relationships. As flat-rate payments can restrict altruistic doctors in their altruism, they tend to change to a contract with reimbursement of costs. Doctors with low levels of altruism prefer flat-rate payments because it allows them to minimise their costs of treatment. Jack (2005) sees the solution in annuity payments for highly altruistic doctors to compensate for flat-rate payments. Recent research has refined and empirically grounded these earlier models. For instance, Oxholm et al. (2024) confirm that both financial incentives and altruistic motivations jointly shape medical decision-making, particularly in contexts where long-term patient outcomes are at stake. Their findings underscore the complexity of motivation in health care and support the idea that neither pure altruism nor financial incentives alone suffice to explain clinical behaviour. Zhang et al. (2023) build on this by demonstrating that mixed remuneration models can mitigate the inherent trade-off between profit and patient benefit, fostering an environment where altruistic behaviour is both encouraged and sustainable. However, other studies highlight the risks of poorly calibrated remuneration systems. Kavas et al. (2025), examining pay-for-performance schemes, show that performance metrics can shift doctors’ attention from patient-centred care to target compliance, increasing workloads and contributing to burnout. Their findings suggest that excessive reliance on extrinsic motivators may erode intrinsic values such as altruism and professional commitment. Similarly, Kreindler and Stolee (2015) argue that altruistic doctors are less responsive to financial incentives and more committed to patient welfare regardless of remuneration. They argue that mixed or hybrid payment systems could align doctors’ intrinsic motivations with external incentives to achieve optimal care. This concern is echoed by Coleman and Joiner (2021), who critique volume-based remuneration schemes for undermining intrinsic motivators and professionalism. They advocate for models rewarding clinical value, encompassing quality and cost, thereby aligning financial incentives with patient-centred care and preserving altruistic values. These studies provide a nuanced view of how altruistic motives and remuneration systems interact in health care, particularly the ways in which compensation structures can either support or undermine doctors’ intrinsic motivations to prioritise patient well-being.
Recognition Motives and Remuneration
In contrast, another group of scholars focuses on recognition motives in health care (e.g., Deci, 1971, 1975; Newhouse, 1970). Recognition in this context refers to professional status, peer respect, and opportunities for advancement, all of which can act as powerful non-monetary drivers of performance. Newhouse (1970) argues that recognition and prestige are granted by the volume and average quality of treatments provided in a hospital. As hospitals are subject to budget restrictions, there is a trade-off between quality and quantity of treatments. The aspiration for prestige results in high quality service for only a few patients. A reimbursement of expenses by a third party amplifies this effect as it eases budget restrictions and causes a cadillac only effect – a socially inefficient distortion towards excessive quality. Newhouse (1970) concludes that service providers should be reimbursed as little as possible as full reimbursement leads to treatments above a socially efficient level. In this context Deci (1975) emphasises the importance of recognition for professional doctors and questions whether motivation is driven by professional recognition and status (obligation-based recognition) or the task of treating and curing itself (enjoyment-based recognition). Both forms of motivation influence the perception of work and the embedded work context. A recent investigation by Chang, Saggar et al. (2023) shows that recognition in the form of professional development opportunities, rather than monetary incentives alone, enhances a doctor’s satisfaction and reduces burnout. This aligns with earlier findings by Deci (1975) but reflects the changing context in which modern health care professionals operate. Aggarwal et al. (2025) further analyse how health care organisations design compensation frameworks that address both financial incentives and recognition. Their work focuses on the balance between intrinsic and extrinsic motivation and how recognition of professional achievements can be embedded into remuneration systems. They argue that performance frameworks must be holistic, blending monetary rewards with recognition and growth opportunities, and account not only for monetary incentives but also for mechanisms that validate professional achievement, such as peer-reviewed evaluations or career advancement pathways. Expanding on this research, Li et al. (2025) discuss the importance of designing performance-related pay schemes to enhance performance without undermining intrinsic motivation in health care. These studies highlight how recognition plays a key role in health care professionals’ motivation and how remuneration systems are evolving to reflect these non-financial incentives.
Profit Motives and Remuneration
A third group of scholars explains remuneration in health care based on profit maximisation motives of doctors (e.g., Allen & Gertler, 1991; Davies & Macfarlane, 2010; Eggleston, 2005; Ellis, 1998; Gravelle, 1999). Central to this perspective is the assumption that doctors, like other economic agents, respond to financial incentives in ways that may not always align with socially optimal outcomes. Davies and Macfarlane (2010) evidence an alteration of treatment plans and a rejection of risk patients in order to optimise remuneration. The potential for quality discrimination under flat-rate payments is also explored by Allen and Gertler (1991), who argue that doctors control the level of care provided and may preferentially offer higher-quality services to ‘cheaper’ patients - those who require fewer resources - while minimising care for more complex, costly cases. Their findings illustrate a direct link between payment structure and clinical decision-making, reinforcing the argument that financial incentives can distort medical judgement. In response to these challenges, several scholars have proposed hybrid models to balance efficiency and equity. While Ellis and McGuire (1986) advocate for mixed payment systems that blend fee-for-service and capitation to align doctor and patient interests, Ma (1994) further refines this approach by introducing cost barriers. In his model, doctors receive mixed payments up to a certain cost threshold, but above the cost barrier full compensation to guarantee treatment of highly cost-intensive patients. Gravelle’s study (1999) addresses profit orientation by focusing on competition among service providers with capitation fees for each registered patient, irrespective of an actual treatment (list system). In case of free price competition for health services there will be an inefficient level of quality and number of privately managed doctor’s offices which results in a trade-off in the number of service providers and quality or vice versa. Gravelle (1999) therefore suggests a combination of a capitation fee to regulate market entry and a flat-rate payment per patient to guarantee quality which has to be part of public regulation to create a higher-level of social welfare. Eggleston (2005) highlights the influence of performance-based criteria on remuneration. Pay-for-performance creates incentives for service providers to treat patients with regard to specific criteria which can be monitored. In order to avoid distortions in remuneration Eggleston (2005) suggests a partially performance-based system in terms of supplemental payments for measurable components in combination with flat-rate payments for unverifiable indicators. In line with these arguments, a recent systematic literature review by Wagenschieber & Blunck (2024) further confirms that mixed models that incorporate both capitation and performance-based incentives improve care quality and cost efficiency by mitigating the adverse effects of pure fee-for-service models. Their empirical findings suggest that well-calibrated incentive structures are key to sustaining high-quality health care delivery in resource-constrained environments. Adding to this discourse, Iserson et al. (2024) explore the challenges faced by emergency doctors in balancing patient care with profit maximisation, emphasising the ethical dilemmas in profit-driven health care settings. They highlight the moral strain that arises when doctors are forced to navigate between patient needs and institutional financial goals, particularly in high-stakes settings like emergency departments. Their study illustrates the human cost of profit-oriented models, where financial imperatives can conflict with professional ethics and patient advocacy. These studies underscore the impact of profit-driven remuneration systems on health care practice and provider behaviour, examining how financial incentives influence medical decision-making, patient care, and the overall quality of the health care system.
Remuneration Systems and Their Effects on Medical Care
There is modest empirical evidence for the impact of fee-for-service and flat-rate payment on medical care with much of the existing research concentrated in the field of dentistry. Studies have predominantly addressed pay-for-performance systems, reflecting a broader interest in how financial incentives affect health care provision. Brosig-Koch et al. (2024), for instance, investigate the effects of performance-based financial incentives on doctors’ service provision and quality of care. They explore how variations in doctors’ profit orientation and patient care motivations influence their responsiveness to financial incentives, underscoring the complexity of designing effective remuneration systems. Davidson et al. (2015) show for the dental care in Sweden that a change from individual fee-for-service to more aggregated payments leads to an increase in simple and a decrease of complex treatments. In contrast, Norway’s introduction of a capitation fee as flat-rate compensation shows no deterioration in the treatment of patients (Grytten et al., 2013). A change of contracts with the UK Nationals Health Service (NHS) and the removal of fee-for-service items illustrates for the UK that complex treatments were no longer offered to patients (Davies & Macfarlane, 2010). Listl and Chalkley (2014) show for Scotland, how fee-for-service payments according to the number of registered patients can lead to an increase in service and how control examinations can be effectively expanded by additional incentives. Recent studies have also questioned the broader effectiveness of pay-for-performance models. For example, Jamili et al. (2023) highlight in a descriptive-comparative analysis the limitations of pay-for-performance models in health care, particularly regarding the measurement of quality in primary care. Their findings emphasise limitations in the operationalisation of quality indicators, echoing Brosig-Koch et al.’s (2024) argument about the importance of accounting for heterogeneous provider motivations. Together, these studies suggest that while pay-for-performance models aim to improve health care quality, challenges persist in designing effective programmes that accurately measure performance and achieve desired outcomes.
There is no empirical support of long-term effects pay-for-performance has on the quality of medical care. In short and medium-term negative impacts on doctors’ motivation are possible. For an exhaustive overview see Chenot (2017), who analyses the effects of pay-for-performance in combination with quality objectives in dental care.
The main advantages of pay-for-performance lie in the optimisation of the quality of treatment, a prevention of care below the acceptable level, more transparency in health care and cost optimisation (Dragosits, 2016; Veith et al., 2012). On the other hand, selection effects such as cherry picking of patients, gaming with financially rewarded tasks being preferred and non-rewarded tasks being neglected, significant measurement results caused by the complexity in health, and finally the acceptance by doctors (bureaucratic overheads and decrease in intrinsic motivation) pose serious threats (Dragosits, 2016). According to Voinea-Griffin et al. (2010) pay-for-performance can only be successful under specific conditions, namely better information of parties involved, an increase in the number of evidence-based clinical guidelines and the development of valid criteria for evidence-based performance measurement. For Germany, Ankowitsch et al. (2014) see the challenge of pay-for-performance systems in the definition of process indicators for prospective and preventive medical care. In this context Kötter et al. (2011) analyse quality indicators as a foundation for the German health system. Following an evaluation study of the NHS, concerns regarding adverse effect and a decline in the quality of care of pay-for-performance systems appear to be justified for primary care.
Already in the 1970ies Glaser (1970) shows in an international comparison a disillusioning outcome for the effectiveness of monetary incentives with none working perfectly but still being used depending on the respective context. Also, Krauth et al. (2013) show that monetary incentives in health systems aim at an increase in efficiency and quality but only work to a limited extent. A literature review by Glassmann (2009) highlights that remuneration systems have to take different treatment options into account, depending on efficacy and safety. For example, an integrated remuneration for the treatment of diabetic patients in the Netherlands indicates an improvement in medical care, and the distribution and delegation of tasks (Mohnen et al., 2013).
Recent literature highlights innovations in health care remuneration systems. Pay-for-performance models have evolved with more nuanced structures that reduce gaming and ensure quality outcomes (Brosig-Koch et al., 2024; Li & Evans, 2022). Furthermore, pay-for-performance models have increasingly integrated holistic care metrics to prevent overemphasis on isolated measures like process adherence. Similarly, mixed payment systems combining capitation and outcome-based incentives have shown promise in enhancing service quality (Wagenschieber & Blunck, 2024). Austria’s recent framework reflects these trends, trying to integrate flexible capitation payments while retaining essential pay-for-performance features to balance cost and quality. This trend reflects a broader shift towards value-based care and the importance of patient outcomes over short-term efficiency.
In sum, three main drivers of behaviour – altruism, recognition and profit – and different remuneration systems play a decisive role for doctors in the pursuit of their personal goals. Most authors suggest a mixed remuneration system to avoid distortions in the provision of medical care and to guarantee a maximum of social welfare. However, research so far does not sufficiently shed light on the interplay of a panel doctor’s motivation and remuneration in the contractual dependency with a state health insurance – in particular how remuneration can affect the achievement of panel doctors’ outcome expectations.
Hence, the mainly economics-based literature goes too short as motivation of doctors is explained solely as a rational individual decision, without taking account of the organisational setting doctors are embedded in. Although scholars attempt to theoretically explain the underlying coherencies of doctors’ behavioural actions, they do not sufficiently pay attention to the organisational perspective with remuneration being a decisive factor for the motivation of panel doctors. In the following we investigate this topic under the lens of Vroom’s (1964) expectancy theory which helps us to balance out such a deficiency.
Theoretical Background
We adopted Vroom’s (1964) expectancy theory because this well-established theory explains the linkage between motivation and individual outcome expectations as well as organisational goals. It is one of the most commonly used theories of motivation in the workplace (e.g., Chiang & Jang, 2008; Heneman & Schwab, 1972; Mitchell & Biglan, 1971). Recent studies explicitly propose the theory to analyse factors which influence the level of motivation, such as e.g., job tenure (Estes & Polnick, 2012), motivation determinants such as responsibility and control over the job, challenging work tasks, use of skills and abilities or feelings of accomplishment and personal growth (Beiu & Davidescu, 2018; Suciu et al., 2013), the social environment (Lloyd & Mertens, 2018) or the psychological climate in project management (Purvis et al., 2015). Apart from the workplace and organisational studies recent fields of application of the expectancy theory can be found in e.g., industrial relations (Vansteenkiste et al., 2005), tourism and environmental research (Kiatkawsin & Han, 2017), building and energy markets (Baumhof et al., 2017) or child psychology (Kim et al., 2017). In broader health care contexts, the extended application of expectancy theory highlights, that perceived rewards significantly impact health care providers’ motivation (De Simone, 2015). Complementary findings by Jones et al. (2022) or Stockkamp et al. (2023) further highlight the enduring significance of intrinsic motivators, including job autonomy and professional recognition. Austria’s policy now acknowledges such factors by embedding professional development incentives into its remuneration model. Although expectancy theory has received substantial support, main limitations are a lack of necessary theoretical classification of the major constructs valence and expectancy and the ambiguousness of instrumentality which makes it difficult to operationalise (Wabba & House, 1974). Furthermore, the complexity of the expectancy theory with many variables represents a challenge for testing and analysing motivation and might portray a too idealistic picture as most individuals do not clearly perceive the suggested effort-performance and performance-reward linkages (Parijat & Bagga, 2014).
Still, the expectancy theory is powerful as apart from the main concepts of valence (attractiveness), expectancy (ability to achieve goals), and instrumentality (to achieve other outcomes) Vroom’s model allows us to incorporate other factors such as remuneration. Vroom’s model comprises cognitive variables that reflect individual differences in work motivation and incorporates relationships between the efforts people put into work, the performance they achieve from that effort, and the rewards people achieve from their effort and performance. People have behavioural choices and are motivated if they believe that their effort will lead to good performance which will then result in desired rewards. Behaviour is a result of conscious choice based on an individual’s expectancy calculations. Therefore, people choose among alternatives which help to optimise their personal outcomes (Lunenburg, 2011; Vroom, 1964). The three main components effort, (task) performance and rewards helped as a theoretical perspective for our analysis where individual outcome expectations connect to societal performance expectations.
In Vroom’s model outcome expectations play the key role in motivating behaviour. Outcome expectations involve personal beliefs about the consequences or outcomes of performing particular behaviour. Inspired by social cognitive career theory (Lent et al., 1994) this includes beliefs about extrinsic rewards for successful behaviour, self-directed consequences such as pride in oneself for mastering a challenging task, and outcomes derived from task performance, as e.g., absorption in the task itself. Already Kantas (1997, p. 261) shows in his study on career-related decision making how Vroom’s model was commonly employed for outcome expectations, including status-recognition, interest, and money as major outcomes.
While we focus on outcome expectations to provide an explanation for panel doctors’ behavioural motivation to provide service and quality of medical care, we also investigate into the role of the factor remuneration. Lloyd and Mertens (2018) highlight the need to expand the expectancy theory and specifically focus on the interaction of the social environment within the organisation as well as across sectors. Including this aspect, we suggest that apart from outcome expectations different forms of remuneration impact the motivation to provide health services. In addition to different forms of remuneration we are open to more findings impacting the behaviour of panel doctors, such es regional representation or panel doctors’ value systems, etc., which can affect the organisation of doctor offices and the flow of patients.
Figure 1 depicts our model and shows that panel doctors have in general two choices. Outcome-oriented medical service aims at the results to be achieved which leads to an optimal provision of medical care in accordance with the goals of the health system. Although we are open to a variety of outcome expectations, in this case we expect rewards driven by altruistic motives to be the most important for a panel doctor. Performance-oriented medical service follows the formal requirements of the state health insurances as listed in the service catalogue. This does not always result in an optimal provision of care as service catalogues are based on financial feasibility of the health care system. Here, we expect panel doctors to be open to a variety of individual goals. We must emphasise that Figure 1 illustrates only the causal relationships and does not show the specific effects of each alternative. As such, it is clear that alternative one does not contribute to maximising income, while alternative two is much more effective in achieving this goal. However, the situation is exactly the opposite when it comes to patient benefit. With either an outcome- or performance-oriented effort in providing medical service a panel doctor shows a certain performance (expectancy) ideally compliant with the expectations of the health system. The performance of the panel doctor then leads to attainment (instrumentality) of a desirable reward. Expectancy is the degree to which panel doctors believe that their abilities will lead them to goal achievement which, in our model is negligible, as all panel doctors have a high professional qualification. Instrumentality is the perception that a given performance leads to an anticipated reward. We assume the instrumentalities – in how a panel doctor fulfils the goals of the health system in order to achieve individual outcome expectations – to be connected to remuneration. A remuneration system can impact the panel doctor’s choice among alternatives and consequently the fulfilment of outcome expectations. Based on these interrelationships we postulate that panel doctors strive for an outcome- or performance-oriented treatment of patients if the remuneration system guarantees the achievement of individual goals. Linking expectancy theory to remuneration for panel doctors.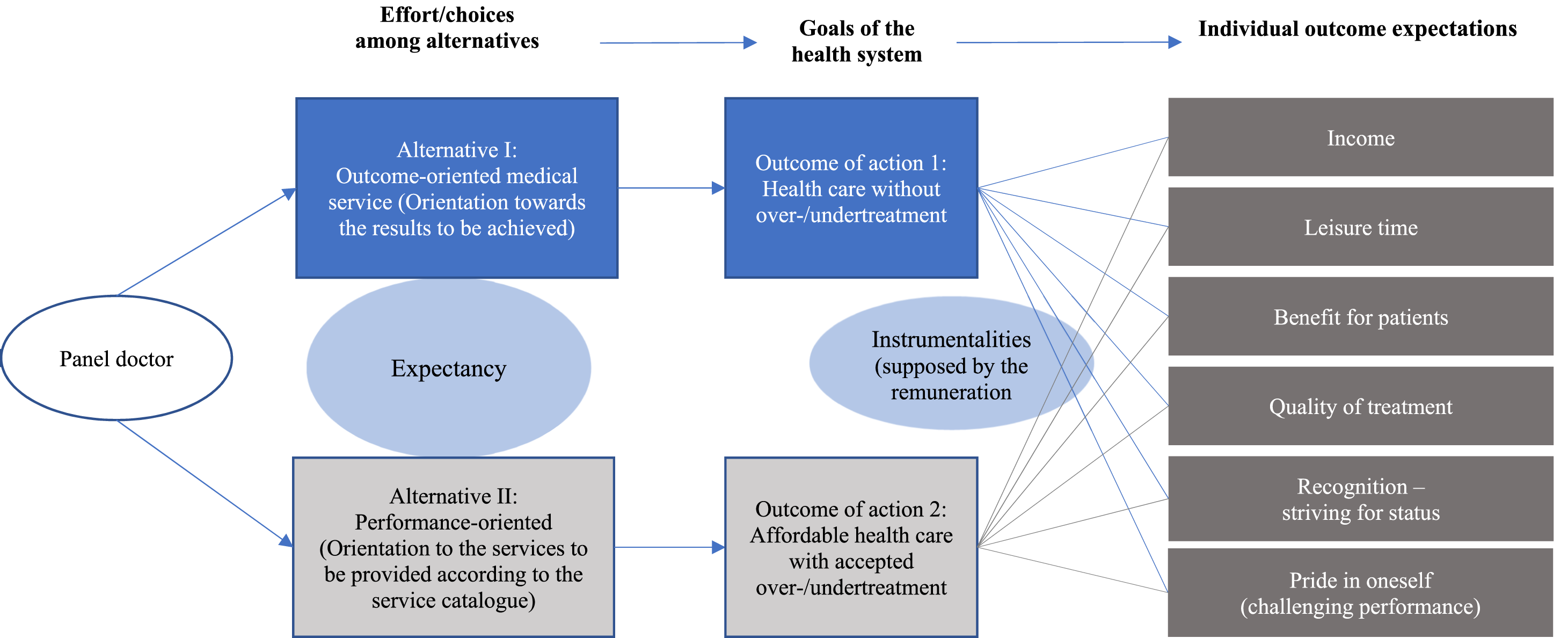
Although Vroom’s theory focuses on manager-employee relationships and a comparison with a conventional employment relationship is controversial among panel doctors, the situation between the state health insurance on the superordinate level and panel doctors is similar. Both managers in organisations and the state health insurance body must explain to their subordinates what they must do to be rewarded. External structures and internal perceptions can shape professional behaviour and outcomes (Shortland & Perkins, 2024). The way remuneration is designed for panel doctors can be seen as an incentive structure similar to executive compensation. If doctors are rewarded based on performance (e.g., number of patients seen or patient outcomes), their motivation and service quality may be influenced, much like how executives may be motivated by bonuses or stock options tied to company performance. Hence, remuneration systems provided by the state health insurance can influence the individual choices of panel doctors in the treatment of patients and similarly affect social welfare.
We therefore consider Vroom’s theory suitable for our explorative study to analyse the impact of the current remuneration system on panel doctors’ motivation to provide service and fulfil societal objectives, as well as to derive implications for a possible redesign of the current remuneration system of panel doctors. Thus, Vroom’s theory serves as a framework for our model and empirical analysis.
Methodology
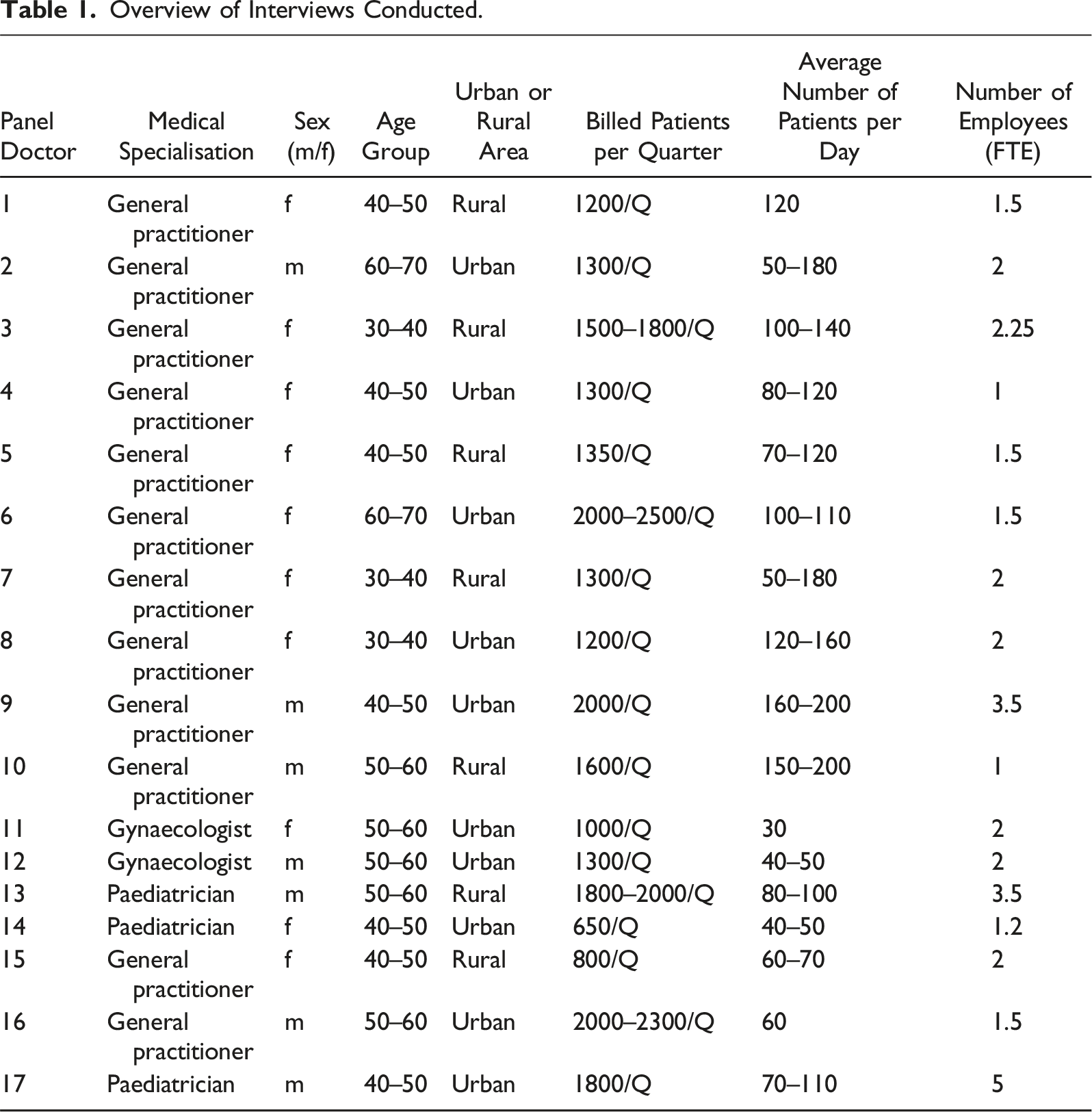
Overview of Interviews Conducted.
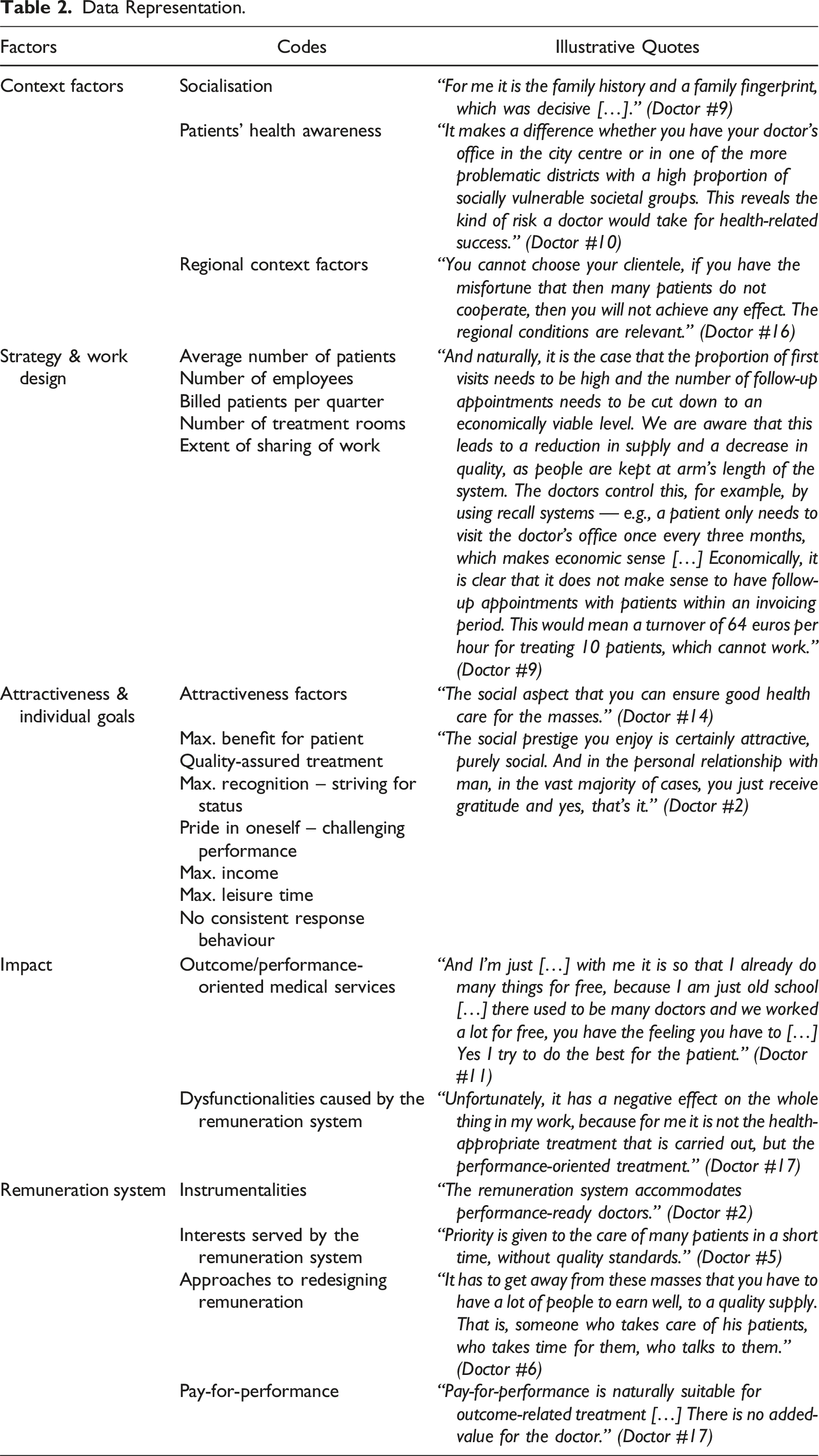
Data Representation.
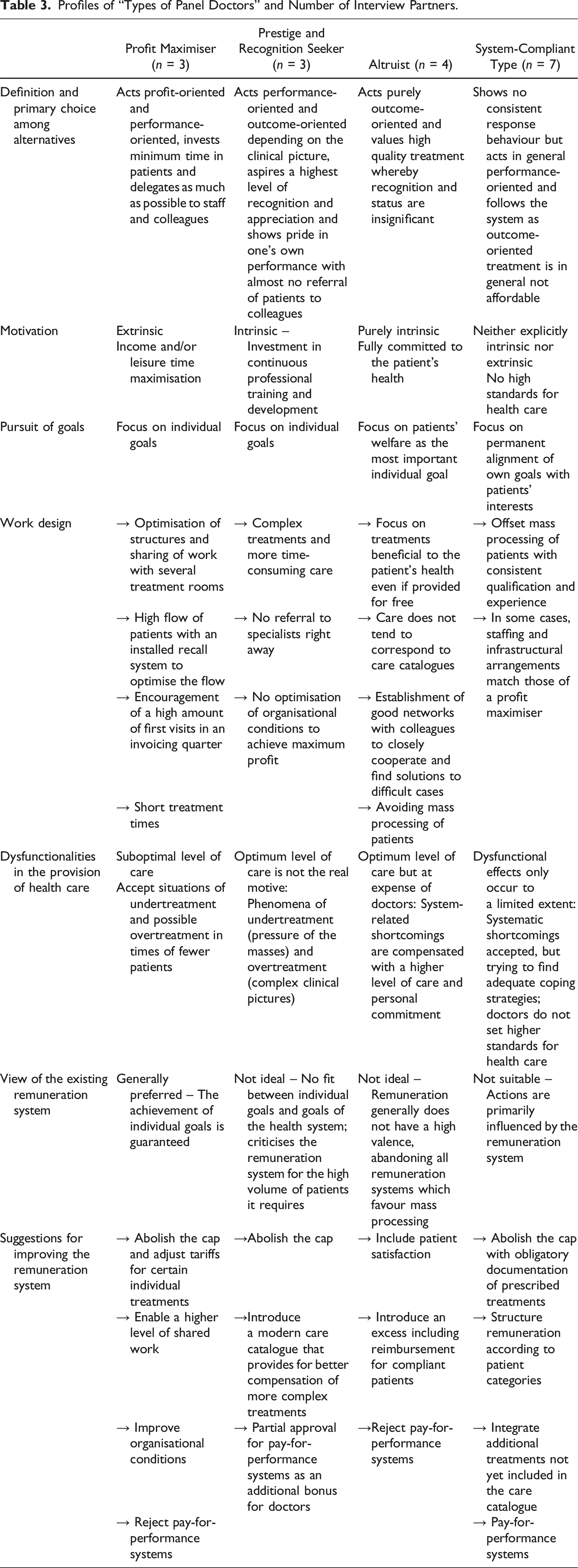
Profiles of “Types of Panel Doctors” and Number of Interview Partners.
Findings
Context Factors, Work Design, Motives and Medical Types
The results of our qualitative interviews demonstrate the various ways in which context factors influence a panel doctor’s treatment behaviour. Despite the existence of a standard remuneration system for panel doctors – which constitutes the relevant context factor in our study – they display very different behaviours. Besides the remuneration system, it can be concluded from the interviews that socialisation, patients’ health awareness and regional context factors also have a significant impact. As Doctor #6 impressively recounts for socialisation: “I was three and a half years old when I contracted measles. I come from a very poor family. And the general practitioner who came more or less attacked me with his tweezers. […] He said, and I quote: I’m not touching such a pitiful being.” “And back then I thought to myself: I can do better than that. And from the age of four onwards, I knew that I wanted to become a doctor and that people should not be classified according to what they have but treated like human beings. And this motivation has remained with me to this day, and it drives me to continue to work with enthusiasm, although I am close to retirement age.”
On the other hand, patients’ health awareness also has a strong impact on panel doctors’ behaviour and their estimation of their self-efficacy. As such, individual doctors focus their treatment methods on awareness, knowing where the patients stand in terms of this, and at the same time they reject any kind of acceptance of responsibility for successful treatment. To this end, Doctor #10 states: “It makes a difference whether you have your doctor’s office in the city centre or in one of the more problematic districts with a high proportion of socially vulnerable societal groups. This reveals the kind of risk a doctor would take for health-related success.”
Depending on the local conditions in the area surrounding a panel doctor’s office, there is a naturally diverse patient base. Regional context factors are the reason why there are different behaviours in the ‘steering’ of the flow of patients as well as in the quality and scope of treatment. For example, doctor’s offices in urban regions usually have a large patient base to tend to. As time is the limiting factor, inter-organisational measures (e.g., several treatment rooms, better sharing of work between the doctor and the surgery’s assistant) are taken so that as many patients can be treated as possible.
When there are large numbers of patients, however, the quality of treatment is inevitably reduced to the minimum level required. Allen and Gertler (1991) highlight this in combination with flat-rate payments for more expensive treatments. At the same time, individual doctors control the number of first visits (as they receive above-average remuneration for these) in combination with a reduction in the number of follow-up appointments so that the result is a profitable economic situation with more billed patients per quarter. Finally, even when there are comparable context factors (regional requirements, remuneration systems, etc.), various treatment strategies, both in qualitative and quantitative terms, can be observed. Thus, it is apparent that panel doctors deal with the fact of over- or undertreatment differently based on collective professional experience (professional socialisation). In our interview sample, we see panel doctors who accept this state of affairs and take it to be a fact which cannot be changed, while at the same time we also see doctors who refuse to accept these conditions and attempt to solve this issue by means of appropriate (usually unpaid) efforts.
From the interviews, we conclude that panel doctors select completely different treatment strategies with and for their patients, despite comparable context factors. These include all conceivable dimensions of quantity and quality when it comes to medical treatments – from processing the masses and referring patients to a specialist as quickly as possible, to overtreating patients by means of close supervision. Experience gained in the course of professional socialisation leads to manifested assumptions in panel doctors as to the outcomes associated with particular types of behaviours. Some panel doctors report that they already know what they have earned at the end of every day. On the contrary, others explain that multimorbid patients often require long treatment processes which they also see as being particularly challenging. The responses suggest that diverse individual motives lead to varying treatment qualities, based on different strategies. We systemised the answers in line with the underlying individual motives of their preferred behaviours and allocated them to four basic types. The differentiation between these types of panel doctors can be seen in the following Figure 2. Medical types of panel doctors.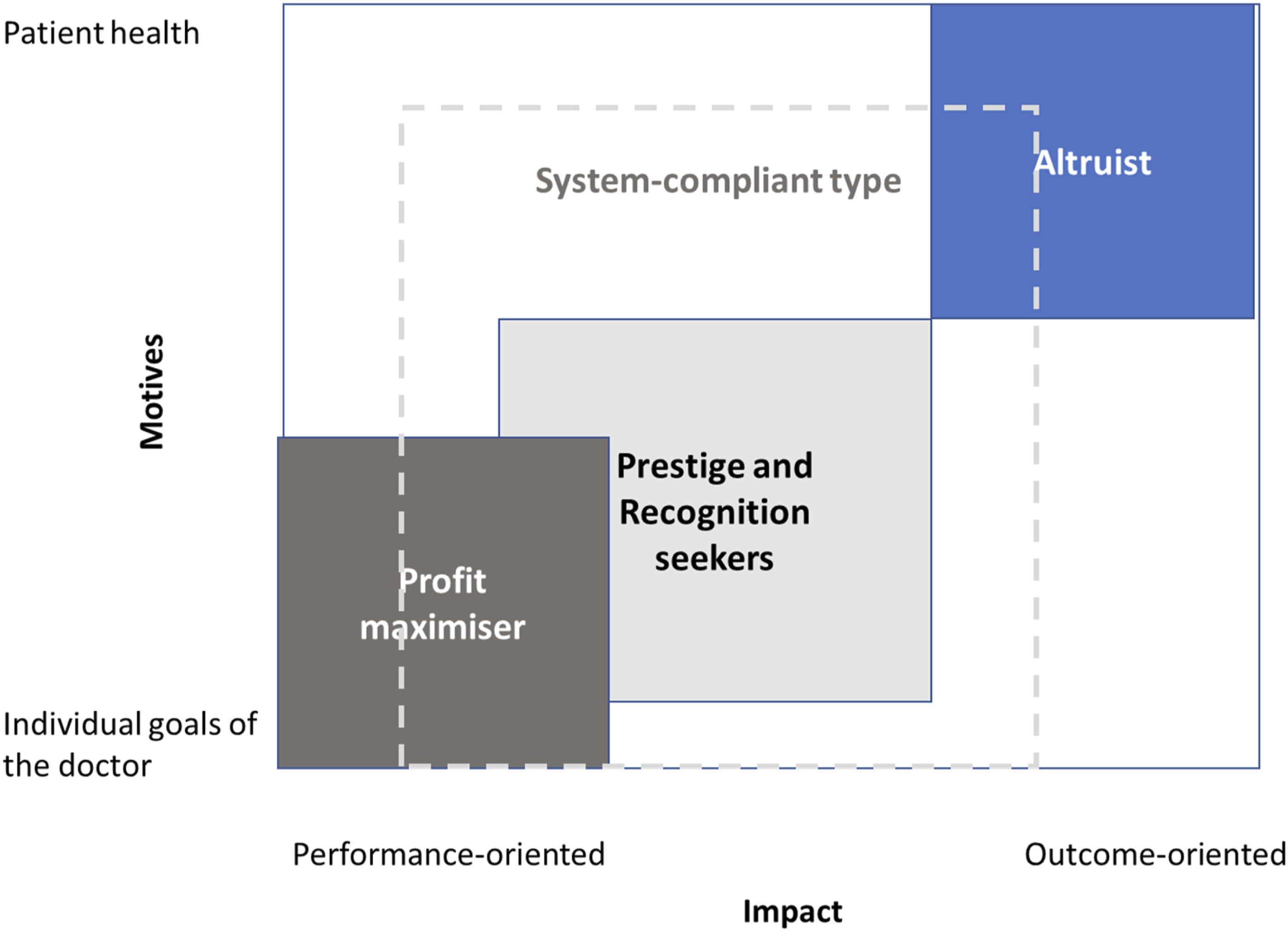
Below, we describe the four types of panel doctors based on Vroom’s theoretical model. In each case, we consider the impact in terms of preferred alternative action (i.e., whether a panel doctor allocated to a certain type is motivated rather towards performance-oriented or outcome-oriented treatment) and the associated dysfunctionalities in health care, as well as the impact on the individual achievement of goals on the basis of the instrumentalities assumed. Moreover, we discuss the implications for redesigning the remuneration system from the perspective of the individual doctor types. Table 3 gives an overview of the four types of panel doctors with the main characteristics. Since our findings are grounded in recurring patterns observed across all doctors, our goal is to highlight specific nuances and experiences rather than generalise too broadly. We believe that focusing on the words of a single doctor can provide a more in-depth and illustrative understanding of a category, offering greater insight than summarising multiple perspectives. Therefore, we present primarily one doctor’s experience to serve as a representative example of each categorisation.
The Profit Maximiser
The profit-maximising doctor generally acts in a performance-oriented manner and is therefore extrinsically motivated. Panel doctors who primarily structure their work to satisfy their individual needs are subsumed under the profit-maximising type. Here, we discuss two forms: (a) consistent focus on income maximisation, and (b) directing their own actions towards achieving as much leisure time as possible. This is reflected in different strategies for action which concern both the type of individual treatment as well as the way in which the organisational environment is structured. Typical strategies for action include ensuring a high flow of patients, whereby the time invested in each patient is minimised to the greatest degree possible according to the motto: the shorter the appointment, the greater the economic benefit. The number of first visits in an invoicing quarter is typically controlled through a recall system to optimise patient flow and improve the return rate from an economic perspective. Patients who contact a doctor frequently within an invoicing period do not pay off economically. Doctor #9 explains: “And, naturally, it is the case that the proportion of first visits needs to be high and the number of follow-up appointments needs to be cut down to an economically viable level. […] Economically, it is clear that it does not make sense to have follow-up appointments with patients within an invoicing period. This would mean a turnover of 64 euros per hour for treating 10 patients, which cannot work.”
Profit-oriented doctors know exactly how much they have earned at the end of a working day. The infrastructural and staff requirements are tailored to cope with the heavy flow of patients. This is evident in the existence of several treatment rooms to prepare patients or provide them with basic care, so that the doctor can move from room to room in short intervals and only needs to carry out basic medical treatments. The sharing of work in the care of patients has been optimised so that anything which does not necessarily need to be done by the doctor is done by another member of staff. More complex patients who need closer, more regular supervision tend to be referred to a specialist, as they require more time per appointment and also need follow-up appointments at shorter intervals. Additional care, which is not covered by the health insurance tariff, is invoiced separately. All in all, these doctors are highly performance-oriented and are also prepared to exchange leisure time for money (depending on the valence of their individual goals). In the interviews, we observed that panel doctors corresponding to this type purposefully used terms such es business model, scaling, or strategy in their answers.
Profit maximisers accept that there will always be sub-optimal situations in the provision of care. In the knowledge that the high number of patients required per day leads to very short treatment times and that there is thus a tendency towards undertreatment, they still act almost only in accordance with their own motives. Times of fewer patients (which are fundamentally avoided) might lead to overtreatment, which means that unnecessary treatment is given to maximise profits.
Having a high number of patients in a short period of time is decisive for this type of panel doctor, both from the perspective of a strong focus on leisure time and profit maximisation. As such, from their point of view the existing remuneration system guarantees the achievement of individual goals. Knowing that the existing remuneration system supports this logic and there is positive instrumentality, these panel doctors are motivated by the performance-oriented option. Caps or limits on the number of specific examinations/treatments per invoicing period reduce the otherwise highly positive link between the existing remuneration system for ensuring health goals and the individual goal of profit maximisation. As a logical consequence, suggestions for improving and amending the remuneration system made by profit-oriented doctors are directed towards abolishing the cap and adjusting the tariffs for certain individual treatments. These are accompanied by recommendations concerning improvements to organisational conditions, such as enabling a higher level of shared work or employing doctors at their own offices. On this topic, Doctor #9 explains: “Time systems scare doctors more than the devil fears holy water! Time is the limiting factor, although quality can also suffer. For better scalability it would make sense if work could be shared (i.e., if certain treatments could be given by a third party under instruction) and the cap (degression rates/limits) was removed at the same time.”
Moreover, this type of panel doctor generally rejects pay-for-performance remuneration approaches, as the risk is shifted to the sphere of the doctor. Being primarily driven by financial incentives, this group adapts strategies to maximise income while minimising service time.
Prestige and Recognition Seeker
A recognition-oriented individual’s fundamental motivation is expressed in different ways. This type of panel doctor is principally motivated by performance-oriented action. In few cases, such as those concerning a complex clinical picture, prestige and recognition seekers are motivated to choose outcome-oriented treatment, whereby their motivation for selecting this action serves, in turn, to satisfy their individual needs. Doctor #2 explains: “Erm, an important factor which […] should not be overlooked is the feeling of self-empowerment. You are in the position of being able to do something. Based, namely, on the scientific grounds you work on. And you see the success which results from your actions. This is good feedback which is usually quite positive.”
As we noted previously, these types of panel doctors are intrinsically motivated when confronted with particularly challenging tasks. Due to this specific provision of care, they receive corresponding appreciation from their patients. Based on the interviews, we can conclude that recognition and appreciation are generally important to these doctors. For most patients, these types of panel doctors behave in a similar way to profit maximisers and therefore tend to be performance-oriented. Their exclusive orientation towards their own needs is something they have in common.
Actions performed reveal a preference for carrying out complex treatments. In contrast to profit maximisers, they are prepared to administer more time-consuming care at the expense of achieving other goals. Doctor #2 explains: “I consider what can I do at my level as a primary provider of care for a large number of people, what can I do to ensure that the person concerned receives the best, easily accessible medical care possible close to his or her home. If I do this responsibly, I know, on the one hand, where my boundaries are, when I will make a referral. When I plainly and simply just don’t know the way out, or something gets too much for me, then I will always refer the patient.”
Patients with complex clinical pictures are thus not referred to specialists right away; this only happens if improvements to health cannot be achieved. At the same time, these panel doctors are willing to invest significant time in their own development and view continuous professional training as essential. With regard to concrete treatment results, the effects are similar to those of profit-oriented doctors. Knowing the required number of patients to run an economically successful doctor’s office, they act similarly to profit maximisers in their basic structure. The organisational conditions are usually not optimised to achieve maximum profit, as pure extrinsic motivation cannot be assumed.
The phenomena of over- and undertreatment are displayed in prestige and recognition-oriented doctors. There is a particular threat of overtreatment in complex cases. With the majority of patients, the ‘pressure of the masses’ is perceived and situations involving undertreatment are accepted. The optimum effect of treatment is not the real motive, rather the solution of complex tasks which can result in situations of optimum care.
Pride in one’s own performance and the highest possible level of recognition are the core individual goals pursued by this type of panel doctor. The interviews reveal that the existing remuneration system does not support an optimum fit between the goals of the health system and individual goals. In contrast to the profit maximiser, this type of panel doctor criticises the remuneration system for the high volume of patients it requires. This type therefore expresses particular demand for a modern care catalogue in the hope that it provides for better compensation for more complex treatments. At the same time, they demand remuneration models which generally aim towards remuneration based upon the clinical picture. Due to the many similarities to profit maximisers in strategies for action, identified structural recommendations are similar in nature: adjusting individual care remuneration, adjusting the care catalogue, and abolishing the cap. Pay-for-performance remuneration models are not generally rejected, however they are limited to certain clinical pictures and interpreted as an additional bonus for doctors. In sum, prestige seekers are motivated by professional recognition, they are more likely to pursue complex cases requiring high expertise.
The Altruist
The altruist is committed to one, single goal: the patient’s health. He or she values high quality treatment and is motivated to act in an exclusively outcome-oriented manner, whereby this motivation is purely of intrinsic nature. All necessary steps are taken which are beneficial to the patient’s health, regardless of whether they receive remuneration for these steps or not. Doctor #6 explains: “I’m not bothered. Even if I don’t get paid for it, I do it. I belong to a special species; I have no idea what I earn, so please don’t ask me, I don’t know. […] Greed is a terrible disease present in all of us. And when we see sums and think about money, we forget about goodwill. I work without thinking about whether I will get paid for what I am doing or not. If I get paid, that’s nice. If I don’t get paid, it doesn’t matter.”
Doing everything is secondary to the welfare of the patient and, as such, patients’ welfare is selected as the most important individual goal with the highest valence. These panel doctors do not focus on the remuneration linked to the care they provide; they only know whether they have actually earned anything at the end of an invoicing period. Appreciation, recognition and status are insignificant for this type, as Doctor #6 mentions: “I don’t care about status.”
While providing treatment, the altruist always tries to achieve an optimum level of care. At the same time, the altruist is driven by concerns that too little is being done for the patients and that other doctors do not pay attention to providing an optimum level of care. The care they give does not tend to correspond to the care catalogues and many treatments are provided for free. Altruists usually have a good network of colleagues with whom they are in close cooperation to find solutions to difficult cases. In any case, the altruist tries to avoid situations involving undertreatment, but does not carry out treatments if they are not strictly necessary. If treatment is provided in accordance with the care catalogue, the altruist constantly feels too little care being administered. System-related shortcomings are compensated by the altruist with a higher level of care, usually provided for free. From a public health perspective, an optimum level of care has been achieved. This is, however, at the expense of individual doctors.
The remuneration system does not provide compensation for the difference between system goals and individual goals, as remuneration generally does not have a high valence for altruistic types. Altruists therefore advocate high-quality care, which means abandoning all remuneration systems which favour ‘mass processing’. They demand the inclusion of patient satisfaction as well as the introduction of an excess including reimbursement for compliant patients. Despite the impact-orientation strived for in pay-for-performance remuneration systems, they are strictly rejected by altruists. Doctor #6 explains: “Well, that is a catastrophic system. What do I do with the poor person? I give him tons of medication just so I get my money? No, thank you. Certainly not. He won’t take it anyway. And if he doesn’t take it, what am I supposed to do with him then? Should I crack the whip and say: “You simply must take it so that I get my money!” No, definitely not.”
In sum, altruists are focused on patient welfare, this group often disregards financial rewards, sometimes compromising their economic stability.
The System-Compliant Type
System-compliant doctors are motivated in different ways, as they do not show consistent response behaviour. Generally, these panel doctors act in a performance-oriented manner (not health-oriented, but performance-appropriate treatment), as this complies with the basic logic of the remuneration system. The interviews revealed that patient goals and panel doctors’ individual goals were on par with one another, and it was not possible to identify priorities. System-compliant doctors permanently try to align their own goals with patients’ interests. At the same time, these panel doctors accept the systematic shortcomings, e.g., a high patient flow, but still try to find adequate coping strategies so that dysfunctional effects only occur to a limited extent. They try to offset the mass processing of patient flows with consistent qualification and experience. However, they accept conditions involving over- or undertreatment by providing more care than necessary, for example in quieter times.
The interviews revealed that some of the system-compliant doctors assume that health care services, particularly those ensuring regional and easy access to health care, are available to everyone. They do not set higher standards for health care. With regard to their selected strategies for action, we see the different facets of the other three types of panel doctors mirrored in system-compliant doctors. Upon close analysis, we deduce numerous ‘system mutations’ with different valences for individual goals. Doctor #17 provides here an example by confirming that two of his individual goals, the health of the patient and high-quality care, are his most important goals. Yet, at the same time we see that his remaining staffing and infrastructural arrangements match those of a profit maximiser. He also explains that the existing remuneration system is neither suitable for achieving patients’ goals nor his own goals: “Treatments often have nothing to do with the care of the patient and sometimes you have to carry out treatments to get the money, even though you would have only needed to carry out half of the treatments from the perspective of optimum care.”
As such, overtreatment is accepted and is consciously carried out to achieve the individual goal. Or Doctor #1 who states his priority goals as being his patients’ health, attractive remuneration, and challenging work. This statement basically addresses all three different types of panel doctors. From a motivational perspective, we can deduce that system-compliant doctors are neither explicitly extrinsically nor intrinsically motivated. There are several panel doctors who are allocated to this type because their actions are primarily influenced by the remuneration system, and they take a stand as ‘followers’ in the system. At the same time, we see panel doctors who want to provide treatment in a more outcome-oriented manner but cannot ‘afford’ due to financial conditions. Precisely for this ‘mutation’ of system-compliant doctors, the restructuring of the remuneration system is the greatest chance. Design recommendations from the interviews for amendments to the existing remuneration system focus on the following: structuring of remuneration according to patient categories (disease patterns), integration of additional treatments which are not yet included in the care catalogue, and the removal of the cap with obligatory documentation of the treatments prescribed. In sum, system-compliant doctors balance system requirements and patient needs, adapting pragmatically to institutional constraints.
Discussion
This study aimed to examine the motivation of panel doctors in deciding between outcome- and performance-oriented medical service, specifically focusing on how remuneration affects their behavioural decisions. The attractiveness of individual goals certainly depends on the type, and the same applies to both extrinsic and intrinsic motivation. We found that the impact of remuneration on the individual goals of panel doctors varies depending on their type – whether profit maximiser, prestige and recognition seeker, altruist, or system-compliant – along with other contextual factors such as the doctor’s professional socialisation, the patient’s health awareness, and regional specifics. These factors reveal various dysfunctions in the medical treatment of patients. Therefore, the types described also highlight the challenges in designing a new remuneration system. There is only a partial alignment between the individual goals of panel doctors and the objectives of the public health system. As a result, the current remuneration system does not ensure ‘good’ quality health care. Interestingly, out of the 17 panel doctors interviewed, only one expressed a positive attitude towards the existing remuneration system. The remaining 16 panel doctors criticised the system, highlighting its shortcomings from the perspectives of the health system, the patients, and the doctors themselves. Additionally, their recommendations for system improvements varied significantly, depending on their motivations. Based on our empirical findings, several theoretical and practical implications can be derived.
Theoretical Implications
Our empirically grounded analysis of panel doctors’ motives reveals a new system-compliant type which has not yet been discussed in literature. Thus, we provide a more nuanced understanding of different motives in health care and contribute to the discussion of performance-based identity (Walker & Caprar, 2020), which helps better explain how individuals relate to their performance at work. For example, Shaw and Gupta (2015) find that extrinsic incentives strongly correlate with performance, a point also explored by Davies and Macfarlane (2010), who suggest that system-designed rewards can induce specific treatment behaviours. Vengberg et al. (2021) further highlight how fee-for-service payments might lead to behaviours like up-coding and skimming healthier patients, which could strain relationships with insurers. Contrary to previous studies (e.g., Arrow, 1963; Ellis & McGuire, 1986), we do not observe any altruists who are also profit-oriented. This contrasts with Ellis and McGuire’s (1986) finding, which suggested that altruism and profit maximisation could be present in the same doctor, motivated by varying financial compensation models. We clearly see that the prevailing basic motivation shapes action. Thus, for altruists, for example, the existing remuneration system has no influence on their actions. This confirms the results of Zhang et al. (2023), who highlighted that more altruistically motivated doctors are unaffected by financial rewards. Even if a panel doctor’s preferred motivation significantly controls their behaviour, overlaps can be observed between the prestige and recognition seeker and profit maximiser types. As such, recognition was occasionally important to panel doctors categorised as profit maximisers, supporting the conclusions drawn by Deci (1975), who argues that professional recognition can play a substantial role in motivating profit-driven doctors.
From a systems perspective, both individual motives of agents and the societal goals of health care must be considered in the optimal design of a remuneration system. This echoes the findings by Levine and Drossman (2022) in their study of U.S. health care systems, where a misalignment of health care providers’ goals with patient outcomes led to inefficiencies. A key shortcoming of the current remuneration system is its failure to consider the individual motives of panel doctors, as not everyone acts as an altruist. This aligns with recent work by Aggarwal et al. (2025), who emphasise the necessity of understanding diverse doctor’s motivations in remuneration design. Therefore, these complex interrelations – particularly the potential mismatch between the goals of state health insurance bodies, which are responsible for doctors’ compensation, and the personal motives driving panel doctors’ actions – can only be understood through a systems analysis that integrates both macro and micro perspectives on goals and motives in health care. In addition, we believe that our typology can serve as an example for analysing motivation in other professional fields. Using the example of panel doctors, we also provide empirical support for Vroom’s theory, which is based on optimisation choice criteria, as proposed by Wabba and House (1974).
Practical Implications
We create awareness for practitioners concerning the type they correspond to. Self-reflecting and comparing with other types might help panel doctors to uncover a possible wrongdoing in their day-to-day actions which might no longer be aligned to their professional ethos. The importance of self-reflection and understanding one’s motivational drivers is consistent with studies by Veith et al. (2012), who argue that personal motivation must be considered for achieving optimal health care outcomes. Highlighting contextual motivational influences helps to better comprehend motivated workplace behaviour (Merriman, 2017). Based on our results, state health insurance bodies and medical associations can gain a better understanding of the various motives influencing panel doctors’ behaviour. Our empirical evidence can guide future suggestions for remuneration systems, helping to optimise the combination of different elements of compensation, particularly through mixed remuneration models, as suggested in our literature review. These models, as discussed by Brosig-Koch et al., 2024, combine performance-based pay with capitation systems to provide flexibility while still aligning doctor behaviour with health system objectives. There is a need to consider the removal of caps, re-working the care catalogue and not implementing a full pay-for-performance system as often discussed for medical professions. Integrating performance-linked pay with flexible capitation models, regular review of pay structures and transparent evaluation criteria could mitigate adverse effects such as overtreatment or patient neglect, as outlined in research by Dragosits (2016). The existing remuneration regulations are an expression of a pronounced culture of mistrust in the contracting parties’ relationships. This is a concern shared by Karlsson et al. (2022), who highlight the inefficiency of a remuneration system that builds mistrust between health professionals and insurers. Caps, not in terms of the number of partial services provided but in terms of the patients treated, could already bring relevant improvements. In any case, the pay-for-performance model, discussed as a sustainable approach, would need to be designed more as an additional motivational tool for both doctors and patients. With a corresponding redesign of the remuneration system, we expect positive short-term effects, particularly for system-compliant panel doctors. Comparative analyses reveal parallels with health care systems in the U.S., U.K., and Scandinavia. For example, the introduction of value-based care in the U.S. led to improved patient outcomes but required costly administrative oversight (McKinsey, 2022). Austria’s recent health care amendment demonstrates an innovative approach by aligning remuneration with team-based care, professional development, and primary care expansion. Professional development incentives in terms of recognising and rewarding continuous education could foster innovation and skill enhancement among panel doctors. Tailored incentive models would allow to differentiate incentive structures based on doctor typologies (profit maximisers, altruists, etc.,) and thereby help to align individual goals with systemic health care objectives. Finally, we see a need for administrative simplification. Streamlining administrative processes related to pay-for-performance can reduce bureaucratic burdens and improve service delivery efficiency, a challenge highlighted by Feng et al. (2024).
The panel doctors surveyed often expressed the opinion that Austrian health care has a much greater focus on low-threshold access to health services than high-quality care for all. The ‘mass processing’ described, which is accompanied by enormous time pressure when it comes to treatment, often leads to undertreatment (lack of high-quality care). Panel doctors complain about this situation, yet point out its absolute necessity for reasons of economic efficiency. This mirrors findings by Almehwari et al. (2024) emphasising the importance of focusing on the provision of quality service, collaboration, and tailored solutions as low-cost structures may undermine quality. As a result, panel doctors are gradually losing importance in health care and, in turn, the system with doctors of choice becomes more and more relevant. In the medical specialist disciplines gynaecology and paediatrics, this has already led to a shortage of panel doctors in the Austrian health system and, as such, regional health care can only be maintained by a system with doctors of choice. To ensure high-quality care, financially better-off patients switch to the elective doctor system. Our results show that, from the panel doctors’ point of view, the remuneration system is largely responsible for the shortcomings outlined. Therefore, the contracting parties must make every effort to fundamentally reform the remuneration system and not just discuss annual inflation adjustments.
Limitations and Suggestions for Future Research
While our findings link the context factor remuneration to panel doctors’ individual motives, we acknowledge that our study has several limitations. First, we recognise that a larger sample population of panel doctors with a larger number of medical specialisations may result in different representations among the identified medical types. As panel doctors work under special contracts with the national health insurances, our findings are not generalisable to all medical professions or health systems. Thus, further research should examine other groups of doctors and take the case of Austria as an example for countries with similar heterogenous structures. As we conducted focused qualitative interviews, no new themes or insights were emerging after 17 interviews. Therefore, we considered to have sufficient depth and breadth for analysis with our sample size. Our data is still relevant as till now there were no major changes in neither doctor’s behaviours nor the health system. As both unfold gradually our data can still offer valuable insights into foundational shifts between remuneration and quality of health care. Second, as interviewees may want to show their best behaviour, we cannot fully exclude a slight tendency towards socially desirable answers. We created an atmosphere of trust during the interviews and tried to take countermeasures by including paraphrases and negations in the interview questions. Guaranteeing strict confidence in the collection and handling of data made us feel comfortable that interviewees were by all means frank in their answers. Third, it would make sense for further work to include the perspective of health insurance institutions. The types of panel doctors outlined in this research and their corresponding treatment behaviours could be analysed in detail based on panel doctors’ billing data. Fourth, we insinuate that health systems always aim at outcome-oriented performance. We are aware that this follows a simplified perspective as state health insurances must consider both a demand-oriented and cost-minimal provision of health care. However, financial feasibility might not always allow a desired outcome-oriented provision of care for patients. Fifth, our study did not consider the effect of patients’ increasing access to medical information online on doctors’ remuneration and the quality of care. The availability of online resources and its impact on patient behaviour and expectations, as well as on doctor-patient interactions, was outside the scope of the research. Future studies could explore how patients’ access to medical knowledge influences remuneration models and whether it leads to a redefinition of quality care standards, particularly in terms of communication and patient satisfaction. Additionally, it would be valuable to investigate how doctors adapt their treatment approaches and their time management in response to more informed patients. Finally, although we are aware that Vroom’s expectancy theory links motivation to an increase in productivity at the organisational level, we encourage scholars to follow a systems approach linking individual and societal goals, as shown in the case of panel doctors and national health systems.
Conclusion
The relationship between remuneration and health care quality remains a pressing concern. Similar to our introductory story our study confirms that the remuneration system significantly influences the medical treatment of patients, depending on the type of panel doctor and their motivation. The current remuneration system results in a range of dysfunctionalities, including mass processing and medical over- or undertreatment, which not only harms individual patients but also creates long-term problems in the health care system, such as doctor shortages in the panel doctor segment. Our analysis affirms that remuneration systems play a crucial role in shaping panel doctors’ motivations and service quality. Tailoring these systems to align with both individual and organisational goals is essential for improving health care outcomes.
The solutions we propose for a revised remuneration system depend on recognising the distinct goals of different types of panel doctors, which makes a one-size-fits-all approach difficult to implement in practice. Our findings suggest that relying on a single form of remuneration will not address the varying motivations of the identified panel doctor types. Instead, a combination of different remuneration forms should be implemented. The redesign should aim to align the individual goals of panel doctors with the broader goals of the public health system. While any new remuneration system will likely incur additional costs, focusing on improving care quality will ultimately benefit the system. Austria’s health care reform can offer a progressive blueprint, balancing economic incentives with service quality. Tailored compensation strategies that align with individual and organisational goals are crucial for achieving sustainable health care improvements.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.