
Abstract
Women who experience intimate partner violence (IPV; versus those who have not) are less likely to engage in treatment and more likely to encounter barriers to treatment. There is inadequate research regarding the effects of substance use, mental health symptoms, and IPV severity on mental health and substance use treatment utilization and barriers to treatment utilization among women who experience IPV. The goal of the present study was to describe substance use and mental health treatment utilization and to examine the extent to which substance use disorder (SUD), mental health symptoms, and IPV severity influence treatment utilization and barriers to treatment utilization among women experiencing IPV. Participants were 275 adult women experiencing IPV and who used any amount of alcohol or drugs in the past three months recruited from the community. A total of 54.5% of women engaged in treatment for substance use and/or mental health in the past 30 days. Receiving substance use treatment was associated with greater odds of having a SUD (OR = 2.30, p = .01). Receiving mental health treatment was associated with greater post-traumatic stress disorder (PTSD; b = 5.04, p = .002) and depressive symptom severity (b = 6.45, p < .001). Receiving combined substance use and mental health treatment was associated with more severe PTSD symptoms (b = 5.32, p = .03) and IPV-related injury (b = 5.14, p = .04). PTSD symptom severity was correlated with confidentiality concerns (r = .40, p = .02), and depressive symptom severity was correlated with attitudinal barriers (r = .40, p = .02). Psychological IPV severity was associated with attitudinal (r = .45, p = .01) and partner-related barriers (r = .35, p = .04). Utilizing treatment is associated with greater mental health severity, suggesting that either greater mental health symptom severity is associated with women seeking treatment and/or that treatment is not effectively reducing symptoms. Results highlight the importance of assessing psychological IPV and mental health symptoms to understand for whom barriers to treatment utilization are most relevant.
Introduction
Intimate partner violence (IPV), which refers to physical, sexual, and/or psychological abuse from a romantic or intimate partner, is a significant public health concern. One in two women in the United States experiences IPV in their lifetime (Leemis et al., 2022), and IPV is associated with negative outcomes, including substance use concerns and mental health symptoms (Cafferky et al., 2018; Khalifeh et al., 2016; Makaroun et al., 2020; Sullivan et al., 2009). Women who experience IPV tend to underutilize available substance use and mental health treatment options and encounter numerous barriers when seeking services (Rodriguez et al., 2009; Simmons et al., 2015). While it is well-established that substance use, mental health symptoms, and IPV severity influence one another, there is inadequate research regarding the rates at which women who experience IPV access treatment, and the effects of substance use, mental health symptoms, and IPV severity on substance use and mental health treatment utilization (Pallatino et al., 2021). To address this gap, the goal of the present study was to describe substance use and mental health treatment utilization and to examine the extent to which substance use disorder (SUD), mental health symptoms, and IPV severity influence treatment utilization and barriers to treatment utilization among women experiencing IPV.
Women who experience IPV (compared to those who don’t experience IPV) are at increased risk for SUD and mental health symptoms. They have a greater likelihood of using alcohol and/or drugs (i.e., 90.1% have used alcohol and 82.1% have used drugs; Sullivan et al., 2009) or developing a SUD compared to women who never experienced IPV. In a 2024 nationally representative sample, 33% of adults diagnosed with a mental health disorder had a co-occurring SUD (Substance Abuse and Mental Health Services Administration, 2025). Globally, post-traumatic stress disorder (PTSD) and depression are the most common and prevalent mental health sequelae associated with experiencing IPV compared to women who have never experienced IPV (Johnson et al., 2020; Lagdon et al., 2014; Spencer et al., 2019). Women who experience IPV are at a three to five times increased risk for PTSD and major depressive disorder (Beydoun et al., 2012; Golding, 1999; Spencer et al., 2019) relative to women who have not experienced IPV. While there is limited research examining the rate at which substance use, mental health, and IPV co-occur, post-traumatic stress related to IPV experiences has been found to influence substance use (Sullivan et al., 2009). Furthermore, among women with a co-occurring substance use and mental health disorder in substance use treatment, 59% reported experiencing IPV in their lifetime upon admission (Lipsky et al., 2010). Despite these heightened rates of substance use and mental health concerns, treatments tend to be underutilized among women who experience IPV.
Rates of treatment utilization by women who experience IPV vary, likely due to the low rates at which IPV is disclosed to professionals and inconsistency in how agencies record requests for treatment and history of IPV (Satyen et al., 2019). In the United States, 23% of adults received any kind of mental health treatment, 6.7% of adults received substance use care, and 14.5% of individuals diagnosed with both SUD and a mental health disorder received concurrent treatment in 2024 (Substance Abuse and Mental Health Services Administration, 2025). U.S. women who experience IPV report seeking treatment for substance use or mental health significantly more frequently than women who never experienced IPV (Makaroun et al., 2020), however, rates of substance use and mental health treatment utilization decrease over time after women stop experiencing IPV (Bonomi et al., 2009). Furthermore, among women who experience IPV, more severe physical abuse is associated with greater likelihood of using mental health resources (Sabri et al., 2013). However, experiencing IPV also more than doubles women’s odds of reporting unmet need for mental health treatment (i.e., 19% of women who experience IPV report needing but not receiving mental health treatment compared to 8% of women who never experienced IPV; Lipsky & Caetano, 2007) and experiencing IPV has shown to interfere with the completion of substance use treatment and recovery from SUDs (Ogden et al., 2022). Current IPV victimization is associated with 25% decreased odds of completing substance use treatment (Lipsky et al., 2010). Moreover, individuals who had (versus had not) experienced IPV were 40% less likely to remain abstinent from substances at a 12-month follow-up assessment (Reed et al., 2015). Treatments that concurrently address substance use and mental health concerns for women experiencing IPV have been found to be effective for women who experience IPV; yet little is known about rates at which women engage in such treatments. Engaging in co-occurring trauma and substance use treatment has been found to reduce substance use more substantially for women who have (versus have not) experienced IPV (Fowler & Faulkner, 2011), and these effects have been found to last over time and to be associated with increased self-confidence among women who experience IPV (Bennett & O’Brien, 2007). The higher rates of co-occurring substance use and mental health disorders among women who experience IPV address the need to develop interventions and treatment options that address the specific occurrence of disorders (Weaver et al., 2015). These findings highlight the influence of IPV on substance use and/or mental health treatment utilization.
While seeking substance use and mental health treatment, women who experience IPV encounter several barriers (Overstreet & Quinn, 2013; Phillips et al., 2021; Simmons et al., 2015). In other populations, barriers to treatment have been characterized as attitudinal, structural, and confidentiality concerns (Haeny et al., 2021; Priester et al., 2016; Verissimo & Grella, 2017). Attitudinal barriers are individual beliefs and feelings, and concerns about the opinions of others, which can include experiencing stigma around seeking treatment for substance use and mental health concerns. Structural barriers are logistical or practical restrictions, which can include not being able to afford treatment or not having transportation. Confidentiality concerns include worries that personal information (e.g., information between the individual and treatment provider) will not be kept private (Haeny et al., 2021; Verissimo & Grella, 2017). Despite these barriers having been examined in other populations (e.g., individuals who use substances), a significant limitation of the literature is that they have not been examined among women who experience IPV, regardless of the significant barriers they encounter when seeking substance use or mental health treatment (Robinson et al., 2021). Additional barriers unique to women who experience IPV are related to their partner. These may include fear of the partner’s reactions or anticipating controlling behaviors (Phillips et al., 2021), such as partners using IPV survivors’ mental health diagnoses to threaten or harm them in legal cases or restricting their ability to make use of treatment (Simmons et al., 2015). Understanding barriers to treatment utilization among women who experience IPV can inform efforts to reduce those barriers and therefore, increase rates of utilization.
It is well-established that women who experience IPV have high rates of co-occurring substance use and mental health disorders (Cyrus et al., 2021; Spencer et al., 2019), and that substance use, mental health symptoms (e.g., PTSD and depression), and IPV severity influence one another. However, there is inadequate research regarding the rates at which women who experience IPV access substance use and mental health treatment. Additionally, there is insufficient literature regarding the effects of substance use, mental health symptoms, and IPV severity on mental health and substance use treatment utilization (Pallatino et al., 2021) and barriers to treatment utilization among women who experience IPV. To address these gaps, the purpose of this study is to describe substance use and mental health treatment utilization and barriers to substance use and mental health treatment among women who experience IPV, and to examine the extent to which SUD (i.e., DSM-IV-TR alcohol or drug abuse or dependence), mental health symptoms, and IPV severity influence women’s substance use and mental health treatment utilization and barriers to utilizing substance use and mental health treatment.
Methods
Participants
These data were collected from 275 adult women from a larger study aiming to examine the daily dynamics of PTSD symptoms, sexual risk behavior, and substance use among women experiencing IPV (Sullivan et al., 2020). Recruitment materials were posted in the community in English and Spanish in: (1) community buildings (e.g., grocery stores, libraries, pizza shops, targeting specific neighborhoods and community health clinics that represented diverse racial/ethnic groups); (2) city buses; and (3) websites (e.g., Craigslist, Facebook). Participants had experienced physical IPV by their male romantic partner in the past 3 months and had used any amount of alcohol or drugs during that time. Additional eligibility criteria included: (1) ongoing contact with their partner (saw partner a minimum of twice a week and did not exceed 2 weeks without contact during the past month); (2) English or Spanish speaking, (3) identify as Black, White, or Latina race/ethnicity (because the parent study was stratified to allow for tests of moderation). Exclusion criteria were psychiatric instability based on self-reported inpatient psychiatric hospitalization in the past year (due to concerns regarding management of acute risk) or residence in a shelter or group living environment (because such living environments may place limitations on the use of alcohol or drugs, relevant to primary aims of the parent study). Seven women were removed from the sample due to inconsistency between screening criteria and information reported at baseline. Thus, the final sample comprised 275 participants. Eligibility was determined via a phone screen based on women’s self-report. Participant demographic characteristics are summarized in Table 1.
Descriptive Information on Demographics and Study Variables of Interest.
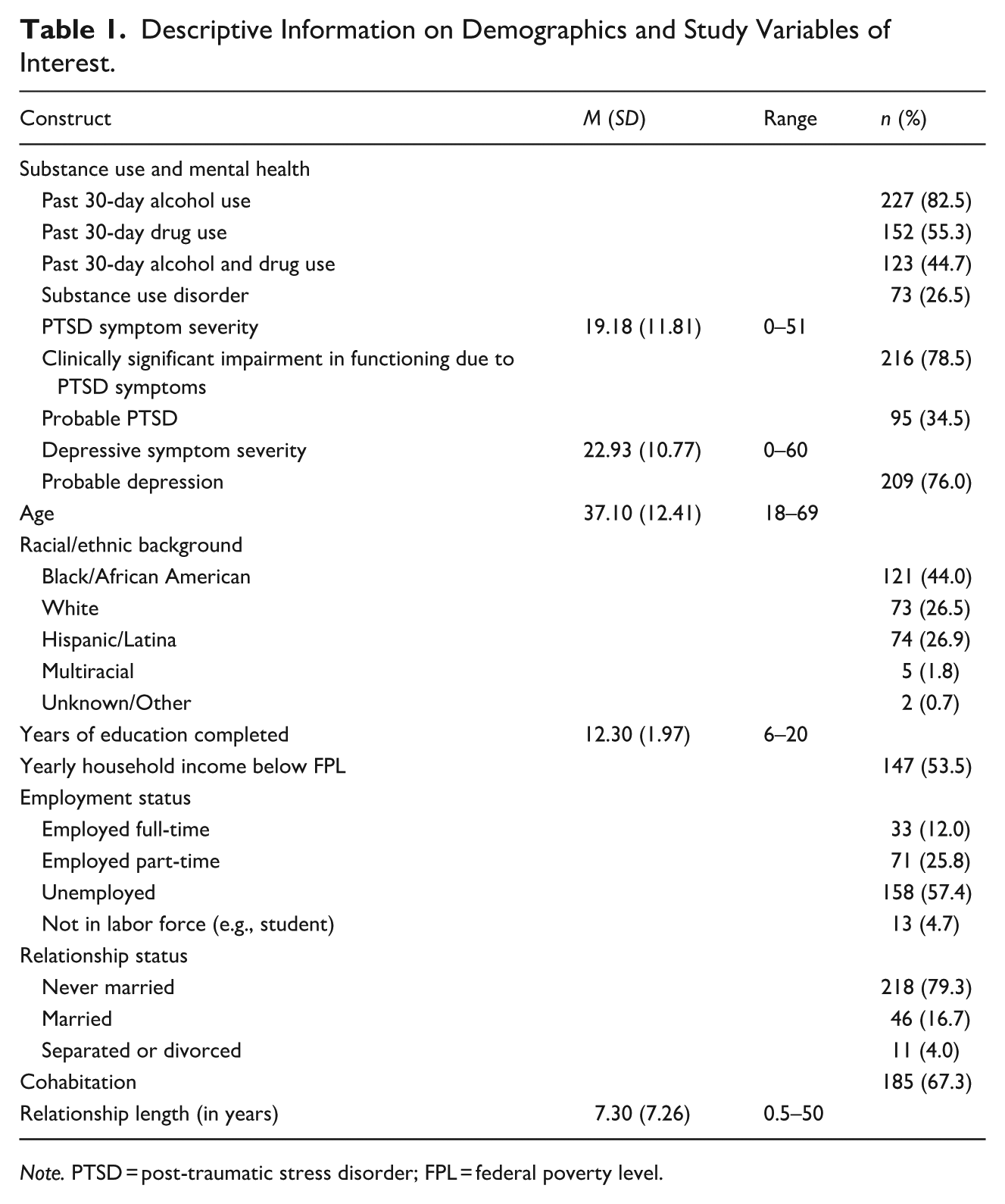
Note. PTSD = post-traumatic stress disorder; FPL = federal poverty level.
Procedure
Participants completed (1) a baseline interview, (2) 30 days of four times daily data collection, and (3) a follow-up interview. The current study uses only data collected during the baseline interview. The baseline interview was administered by a trained female research assistant or postdoctoral fellow in a private office. Informed consent was obtained, and the interview was administered in either English or Spanish using computer-assisted self-report measures. Women were compensated up to $325 for the baseline interview, daily data collection, follow-up interview, and bonus payments. A resource brochure distributed at the end of the interview provided information on services in the area including IPV victimization support, mental health, substance use, employment, housing, financial assistance, etc. The research assistant offered support with referrals and also offered to complete a safety plan unique to the participant’s situation at the end of the baseline interview.
Measures
Substance Abuse/Dependence
The Structured Clinical Interview for DSM-IV (SCID-I; First et al., 2016) was used to establish current DSM-IV-TR alcohol abuse and/or dependence and drug abuse and/or dependence diagnosis. The SCID-I is a semi-structured assessment for psychiatric disorders. The interview was administered by research assistants or postdoctoral fellows trained by the principal investigator. All data were reviewed by a doctoral-level clinical psychologist, and diagnoses were further discussed in meetings. For the purpose of the present study, we refer to alcohol abuse and/or dependence and drug abuse and/or dependence as SUD.
PTSD Symptom Severity
The Post Traumatic Stress Diagnostic Scale (PDS; Foa et al., 1997) measures DSM-IV-TR PTSD symptom severity. The PDS assessed past 30-day PTSD symptoms related to IPV victimization by a current male partner. Symptom severity items assess the frequency of each symptom on a 4-point scale ranging from 0 (not at all, or only one time) to 3 (5 or more times a week, or almost always). Items are summed to create a total symptom severity score, with higher scores indicating more severe symptoms (Cronbach’s α = .92). Probable PTSD was determined based on endorsement of at least one Criterion A event (i.e., participants were instructed to consider IPV as the referent traumatic event), endorsement of at least one re-experiencing symptom, three avoidance/numbing symptoms, two hyperarousal symptoms, symptom duration of at least 1 month, and impairment in at least two areas of functioning, in line with DSM-IV-TR diagnostic rules (American Psychiatric Association, 2000).
Depressive Symptom Severity
The Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) is a 20-item scale that measures depressive symptom severity. Items assessed how often participants have experienced symptoms in the past 30 days on a 4-point scale ranging from 0 (rarely or none of the time) to 4 (most or all of the time [on average, 5–7 days a week]). Items were summed to create a total score, with higher scores indicating more severe symptoms, and a cutoff score of 16 (Lewinsohn et al., 1997) or greater indicating probable depression (Cronbach’s α = .78).
Intimate Partner Violence
Psychological IPV
The Psychological Maltreatment of Women Inventory (PMWI-S; Tolman, 1999) is a 14-item scale that assesses psychological victimization from an intimate partner. The PMWI-S assesses dominance/isolation (7 items that assessed the power, control, and isolation) and emotional/verbal (7 items that assessed verbal abuse) victimization in the past 30 days on a 5-point scale ranging from 1 (never) to 5 (very frequently). Items were summed to create a total score, with higher scores indicating more severe psychological victimization (Cronbach’s α = .91).
Physical IPV and Injury
The Revised Conflict Tactics Scale (CTS-2; Straus et al., 1996) assessed physical assault (12 items that assessed physical victimization by a partner) and injury (6 items that assessed physical injuries that required medical attention) by their intimate partner in the past 30 days. Consistent with scoring recommendations by Straus et al. (2003), responses that were a range were recorded to the midpoint (0 = never or not in the past year, 1 = once, 2 = twice, 4 = 3–5 times, 8 = 6–10 times, 15 = 11–20 times, 25 = more than 20 times). Items were summed to create total subscale scores, with higher scores indicating more severe victimization and injury (Cronbach’s α = .92) and IPV-related injury (Cronbach’s α = .74).
Sexual IPV
The Sexual Experiences Survey (SES; Koss & Oros, 1982) is a 13-item scale that assesses women’s experiences of sexual victimization. Items were modified to assess sexual victimization by an intimate partner, as the original SES was designed to assess women’s experiences by any man (Weiss et al., 2017). Responses were modified to match the CTS-2 response options and scoring systems. Items were summed to create a total score, with higher scores indicating experiencing more severe victimization (Cronbach’s α = .92).
Treatment Utilization
Types of substance use and mental health treatment received in the past 30 days were assessed using 15 questions from the National Survey on Drug Use and Health (NSDUH; U.S. Department of Health and Human Services, 2008). Types of treatment included detoxification, meetings (e.g., Narcotics Anonymous or Alcoholics Anonymous), self-help groups or services for alcohol or drug use, individual outpatient treatment, and group outpatient treatment. Participants indicated whether they engaged in treatment to address mental health, substance use, or both simultaneously. Responses across items were collapsed to create two variables. The first represents whether participants accessed any mental health or substance use treatment (0 = no treatment, 1 = any mental health or substance use treatment). The second represents whether treatment was received to address mental health and/or substance use (0 = no treatment, 1 = treatment for mental health, 2 = treatment for substance use, and 3 = treatment for both mental health and substance use (i.e., simultaneous treatment).
Barriers to Treatment
Barriers to utilizing substance use and mental health treatment were assessed using 24 questions (12 regarding substance use, 12 regarding mental health). Participants were asked whether there has been a time in the past 30 days that they have needed treatment for substance use and/or mental health but did not engage in it (see Supplemental Material). If they answered affirmatively, they were administered questions regarding the following barriers: attitudinal (3 items; e.g., “getting help might cause negative opinion of you”), structural (4 items; e.g., “you couldn’t afford the cost”), partner-related (4 items; e.g., “your partner would think you are having an affair”), and confidentiality (1 item; i.e., “concerned information might not be kept confidential”), consistent with previous literature (Haeny et al., 2021). Questions assessing attitudinal, structural, and confidentiality barriers were drawn from the NSDUH (U.S. Department of Health and Human Services, 2008). Questions assessing partner barriers were developed specifically for this study based on extant research and the PI’s over 20 years of clinical and research experience with women who experience IPV in various IPV, substance use, and mental health settings. Items assessed participants’ agreement that each item represents a barrier to treatment on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). Items were summed to create a total subscale score, with higher scores indicating greater experiences of attitudinal (Cronbach’s α = .70), structural (Cronbach’s α = .81), partner (Cronbach’s α = .89), and confidentiality barriers to utilizing substance use and/or mental health treatment.
Demographic and Relationship Characteristics
Participants self-reported age, race and ethnicity, education, yearly household income, employment status, cohabitation with partner, and relationship length. Yearly income was converted into a dichotomous variable reflecting whether the participant’s yearly income fell above (coded as 0) or below (coded as 1) the federal poverty level based on the year of data collection and number of people supported by that income.
Data Analysis Plan
Frequencies and percentages were used to describe categorical variables. Means and standard deviations were used to describe continuous variables. Regression analyses were used to examine the association between treatment utilization and likelihood of having a SUD diagnosis (i.e., logistic regression) and between treatment utilization and mental health symptom severity and IPV severity (i.e., linear regression). Pearson product–moment correlations between two continuous variables and point-biserial correlations between continuous and categorical variables were used to examine the associations between barriers to treatment utilization and SUD, mental health symptom severity, and IPV severity (Figure 1).
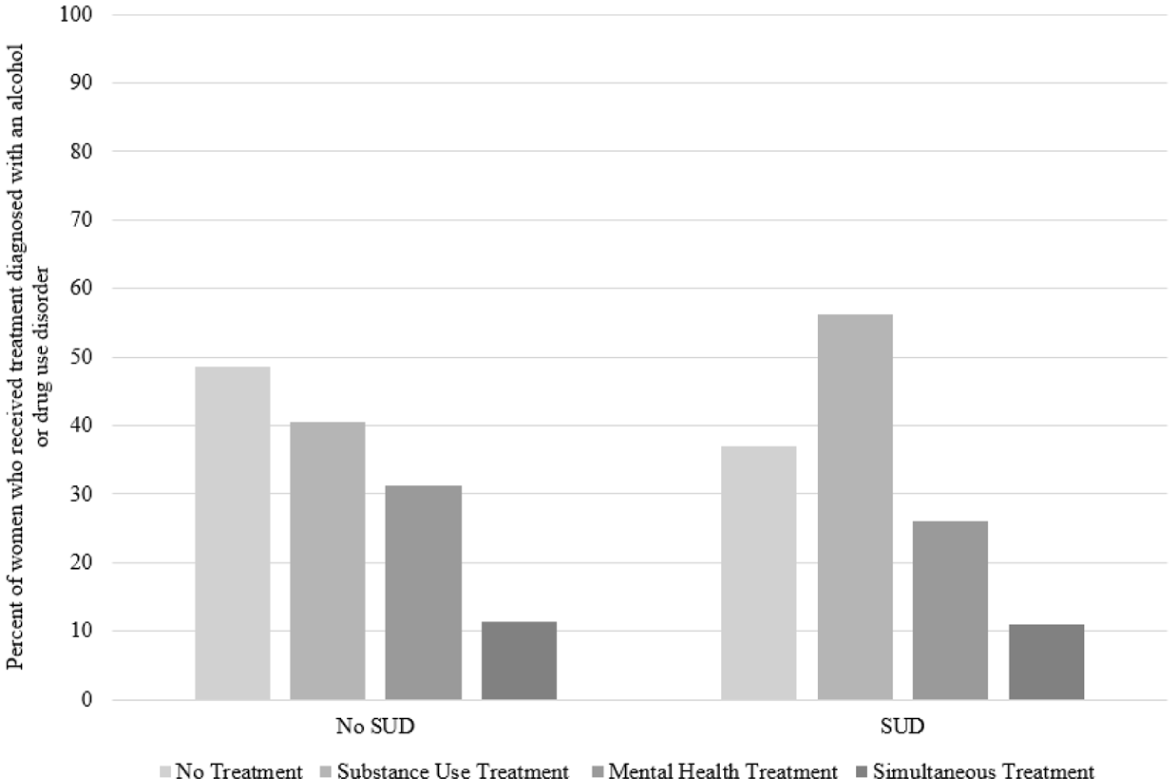
Percentage of participants with probable SUD diagnosis by substance use and/or mental health treatment utilization.
Results
Of the total sample, 82.5% (n = 227) used alcohol, 55.3% (n = 152) used drugs and 44.7% (n = 123) used both alcohol and drugs in the past 30 days. According to the SCID-I, 26.5% (n = 73) met criteria for a SUD. Based on applying DSM-IV-TR diagnostic rules to PDS items (American Psychiatric Association, 2000; Foa et al., 1997), 34.5% (n = 95) reported probable PTSD and regardless of probable PTSD diagnosis, 78.5% (n = 216) of individuals who experienced clinically significant impairment in functioning due to symptoms. Based on a cutoff score of 16 or greater on the CES-D (Lewinsohn et al., 1997; Radloff, 1977), 76.0% (n = 209) reported probable depression. Further descriptive statistics are presented in Table 1.
Treatment Utilization
In total, 54.5% (n = 150) of women engaged in treatment for substance use and/or mental health symptoms; 44.7% (n = 123) engaged in substance use treatment, 29.8% (n = 82) engaged in mental health treatment, and 11.3% (n = 31) of women engaged in simultaneous treatment for both substance use and mental health symptoms; of note, women could report engaging in multiple types of treatment and treatment groups are not mutually exclusive. See Table 2 for utilization of each treatment type.
Types of Substance Use, and Mental Health Treatment Engaged in and Barriers to Treatment Utilization.
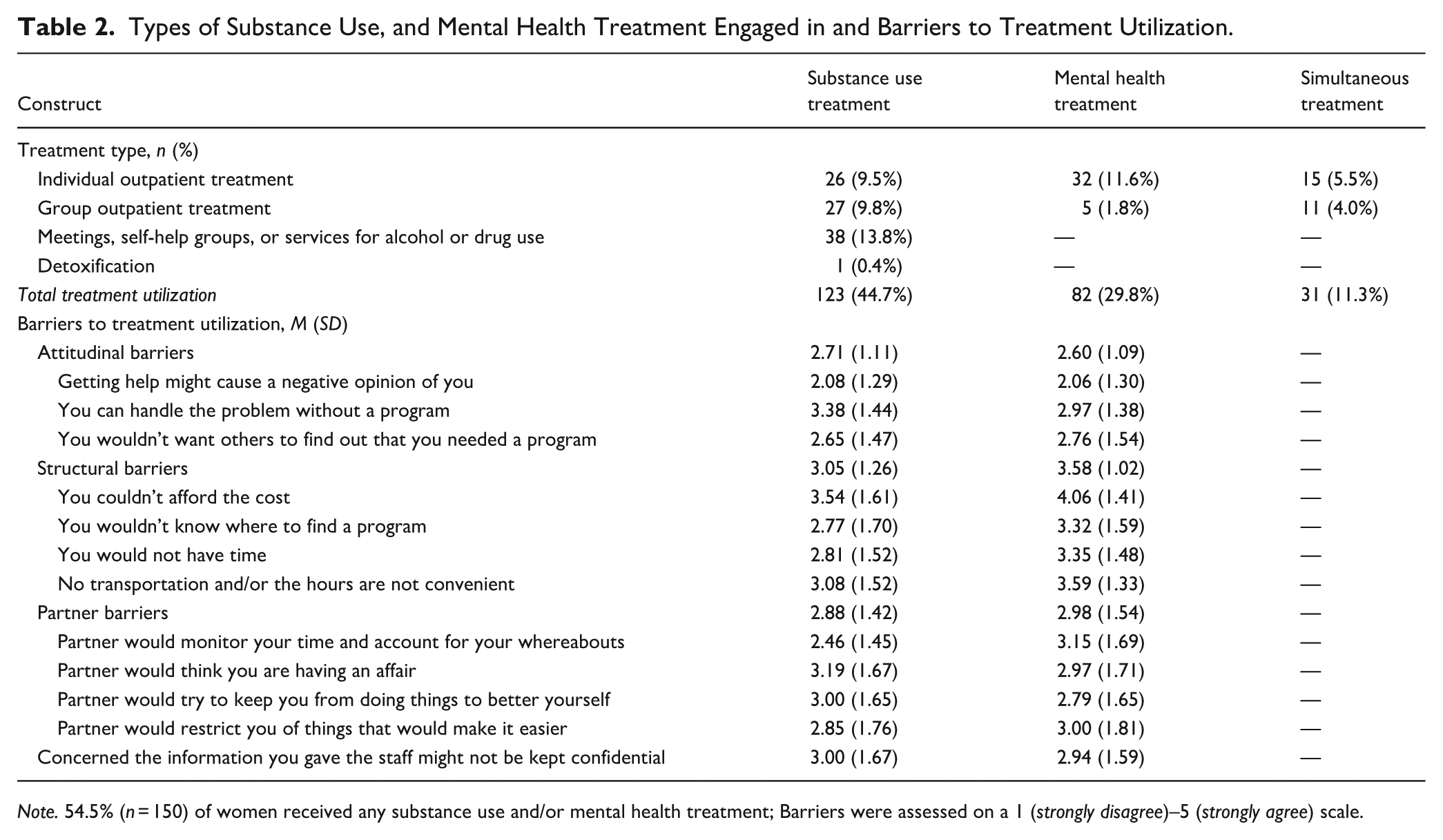
Note. 54.5% (n = 150) of women received any substance use and/or mental health treatment; Barriers were assessed on a 1 (strongly disagree)–5 (strongly agree) scale.
See Table 3 for regression results. Results of logistic regression analyses examining the association between treatment utilization and SUD revealed that engaging in substance use treatment was associated with significantly greater odds of having a SUD (OR = 2.30, p = .01, 95% CI [1.27, 4.17]). Results of linear regression analyses examining the association between treatment utilization and mental health symptom and IPV severity revealed that engaging in mental health treatment (b = 5.04, SE = 1.61, p = .002, 95% CI [1.87, 8.21]) and simultaneous treatment (b = 5.32, SE = 2.39, p = .03, 95% CI [0.62, 10.02]) were associated with significantly greater PTSD symptom severity. Engaging in mental health treatment was associated with significantly greater depressive symptom severity (b = 6.45, SE = 1.45, p < .001, 95% CI [3.60, 9.30]). Finally, engaging in simultaneous treatment was associated with more severe IPV-related injury (b = 5.14, SE = 2.43, p = .04, 95% CI [0.36, 9.91]; Figure 2).
Regression Analyses Examining the Effect of Treatment Utilization on the Likelihood of SUD, Mental Health Symptom Severity, and IPV Severity.
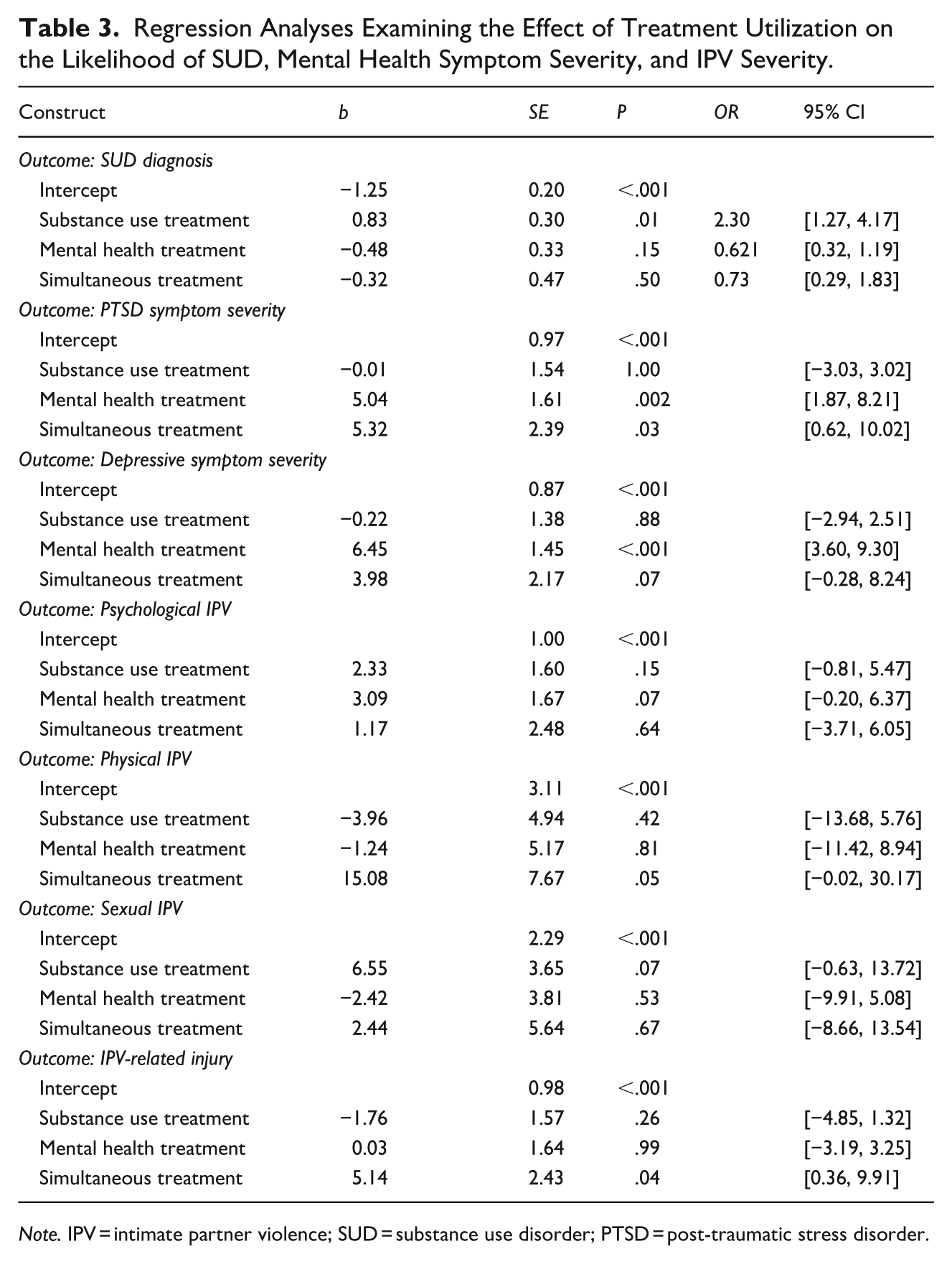
Note. IPV = intimate partner violence; SUD = substance use disorder; PTSD = post-traumatic stress disorder.
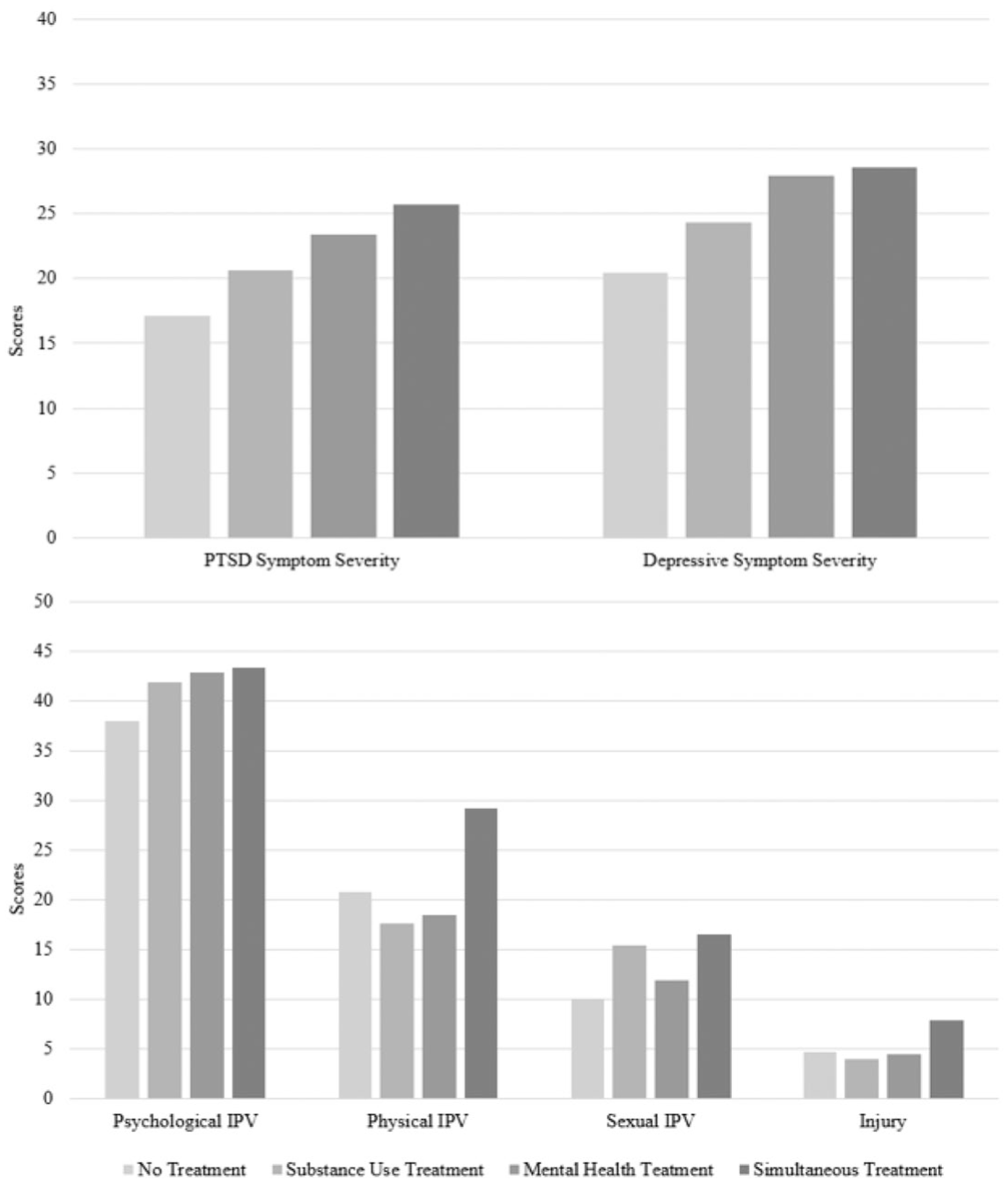
Mean mental health symptom and IPV severity scores by substance use and/or mental health treatment utilization.
Barriers to Treatment
In total, 23.3% (n = 64) of women reported that they needed treatment for a SUD and/or mental health in the preceding 30 days but did not utilize it. Of these, 35.9% (n = 23) had a SUD, 40.6% (n = 26) had a probable PTSD diagnosis, and 92.2% (n = 59) had probable depression. See Table 4 for bivariate correlations between barriers and SUD diagnosis, mental health symptom severity, and IPV severity. PTSD symptom severity was significantly positively correlated with the barrier of concerns about confidentiality (r = .40, p = .02). Depressive symptom severity was significantly positively correlated with attitudinal barriers (r = .39, p = .03). Psychological IPV severity was significantly positively correlated with attitudinal barriers (r = .45, p = .008) and partner-related barriers (r = .35, p = .04). There were no significant correlations between barriers to receiving substance use treatment and SUD diagnosis, mental health symptom severity, or IPV severity.
Bivariate Correlations Between SUD, Mental Health Symptoms, IPV Severity, and Treatment Barriers.
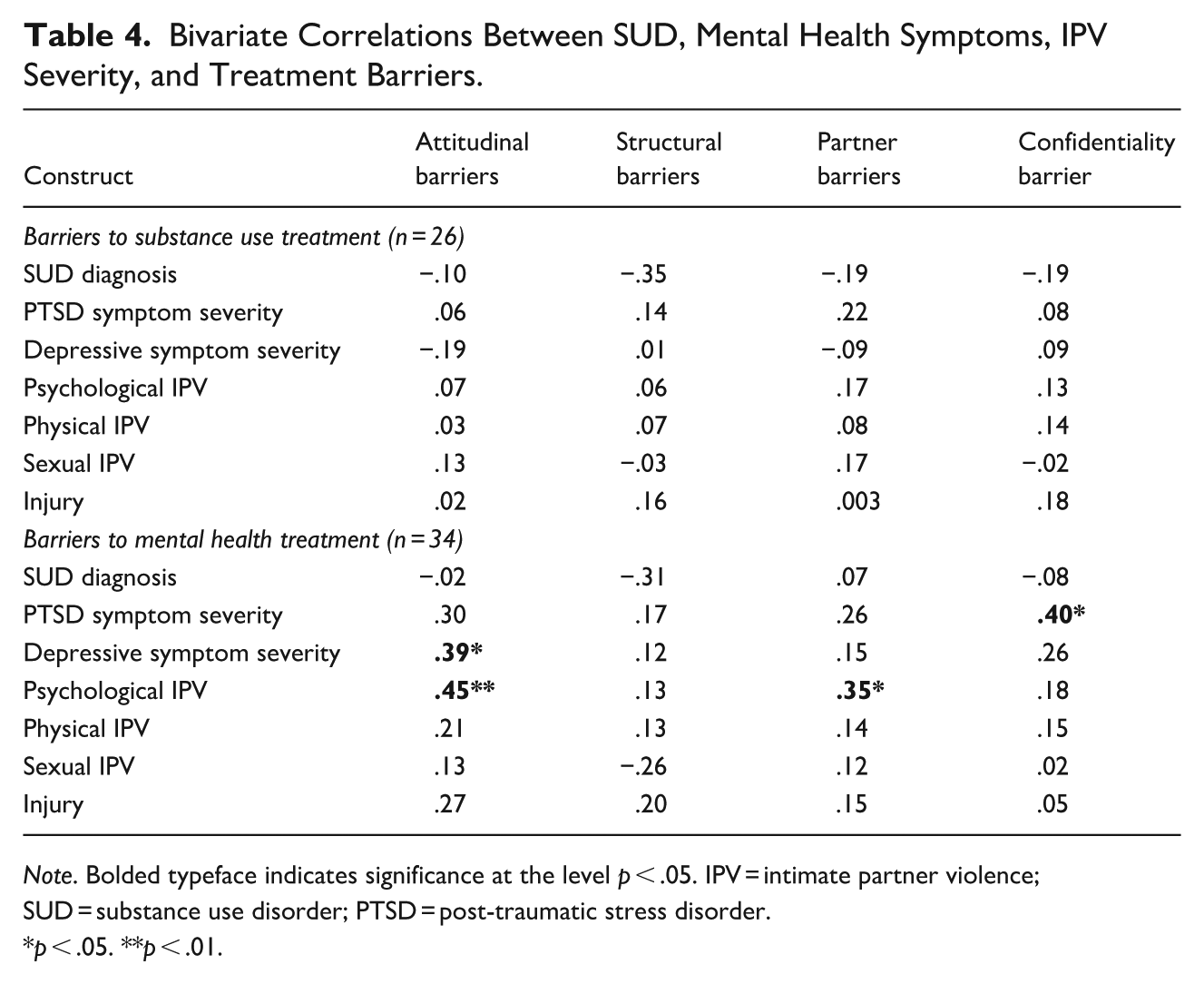
Note. Bolded typeface indicates significance at the level p < .05. IPV = intimate partner violence; SUD = substance use disorder; PTSD = post-traumatic stress disorder.
p < .05. **p < .01.
Discussion
The goal of the present study was to describe substance use and mental health treatment utilization and to examine the extent to which SUD, mental health symptoms, and IPV severity influence treatment utilization and barriers to treatment utilization among women experiencing IPV. First, more than half of the participants engaged in substance use and/or mental health treatment in the preceding month. This finding adds to the existing literature highlighting varied rates of treatment utilization among women who experience IPV (Makaroun et al., 2020). Next, we found that those who engaged in substance use treatment, but not those who engaged in mental health or simultaneous treatment, were at greater odds of having a SUD. Similarly, receiving mental health or simultaneous treatment was associated with greater PTSD symptom severity, and mental health treatment was associated with greater depressive symptom severity. Given the cross-sectional nature of these data, we are not able to delineate the direction of these associations. On one hand, it may be that those who meet criteria for a SUD diagnosis or who experience more severe PTSD and depressive symptoms are more likely to seek out or be referred for treatment. On the other hand, these findings may suggest that treatment is not effectively helping to reduce symptoms or may not be fully meeting the needs of women experiencing IPV. Alternatively, it is important to note that IPV and mental health symptom severity may interact and dynamically influence one another—previous meta-analytic reviews have reported bidirectional associations between IPV and mental health, most notably depressive symptoms (Bacchus et al., 2018). Further research focusing on symptom change over the time and over the course of treatment specifically among women experiencing IPV is needed to understand the experience of women with PTSD symptoms who use substances and are seeking treatment (Myers et al., 2015) and to better understand if substance use treatment is effective for this population (Hien et al., 2004). Finally, receiving simultaneous substance use and mental health treatment was associated with greater IPV-related injury. Further research is needed to understand these findings.
Next, with respect to barriers to treatment utilization, about one-quarter of our sample reported recently needing substance use and/or mental health treatment but not receiving it. Of note, this subsample had high rates of SUD diagnosis and probable PTSD and depression, bolstering their self-perceived need for treatment. This finding may reflect difficulty of seeking treatment when experiencing symptoms of depression and awareness of what PTSD symptoms are. This rate of non-treatment receipt is relatively higher than those reported in previous literature (Lipsky & Caetano, 2007), which may reflect differences in sample characteristics. For instance, Lipsky and Caetano (2007) made use of national epidemiologic data, whereas women were recruited from the community for participation in the present study; previous work has found that community-recruited samples tend to report more frequent and more severe IPV relative to large epidemiologic or population-based studies (Langhinrichsen-Rohling et al., 2012). Among barriers to receiving substance use or mental health treatment, structural barriers (e.g., inability to afford treatment, not having health insurance) were the most frequently endorsed. Of note, over half of our sample was unemployed and had a yearly household income that was below the federal poverty line (i.e., 53.5%), and the majority of participants are from minoritized racial and ethnic groups (i.e., Black and Latina). Previous work has found that socioeconomic status is an important social determinant of health care (Stepanikova & Oates, 2017) and that members of minoritized racial and ethnic groups report greater structural barriers to receiving medical care relative to White individuals (Caraballo et al., 2022). These disparities likely reflect forms of structural racism and other group-specific challenges (e.g., fear related to applying for government assistance if family members do not have legal citizenship, which therefore influences the ability to afford treatment; Sue & Sue, 2016). Further work is needed to address specific practical barriers to make treatment more accessible.
Significant correlations were found between barriers to receiving mental health treatment and mental health and IPV severity. First, PTSD symptom severity was correlated with concerns about confidentiality. This finding may be due to negative alterations in cognitions related to trust that are common in PTSD, as posited by the cognitive model of PTSD and models of complex PTSD (Bell et al., 2019; Ehlers & Clark, 2000; Laddis, 2019). Next, depressive symptom severity was correlated with attitudinal barriers (e.g., thinking it would go away on its own or that you are strong enough to handle it by yourself). This finding adds to existing literature that highlight women’s perception of needing to be strong enough to overcome their depression themselves, and therefore, not seeking treatment (Caplan & Whittemore, 2013). Furthermore, our sample had a relatively larger proportion of Latina women, who have been found to be more likely to express concerns regarding feeling embarrassed for family members or friends to learn they are experiencing symptoms of a mental health disorder, which can negatively influence their likelihood of seeking treatment (Sue & Sue, 2016). Finally, psychological IPV severity was positively correlated with attitudinal barriers and partner-related barriers. The positive association between psychological IPV and partner-related barriers may reflect that these partner-related barriers are themselves forms of psychological IPV (i.e., preventing women from doing things to better themselves). These results also may reflect the “invisible” nature of psychological IPV relative to physical and sexual IPV, the latter of which can cause physical pain and injury (Arriaga & Schkeryantz, 2015). It is important to note that issues related to gender, power, and hegemonic masculinity are likely inextricably linked to experiences of IPV (Connell, 2016; Krivoshchekov et al., 2023; Mahmood, 2020) and subsequently, their influence on treatment utilization. “Gender transformative” approaches, which emphasize transforming gender roles, reducing harmful gender role stereotypes, and promoting gender-equitable relations to address IPV have begun to be implemented with promising results (World Health Organization, 2007); their expansion may be important to promote women’s treatment utilization and, therefore, well-being. We found no significant correlations between barriers to receiving substance use treatment and SUD diagnosis, mental health, or IPV severity. These results suggest that barriers to receiving substance use treatment do not depend upon SUD diagnosis, mental health symptom severity, and IPV severity, perhaps due to the high degree of stigma experienced by individuals in substance use treatment (Crapanzano et al., 2019; Zwick et al., 2020). Results highlight the importance of assessing psychological IPV and mental health symptoms to understand for whom barriers to treatment utilization are most relevant. In addition, it is critical for future research to identify ways to serve culturally diverse populations to increase treatment utilization and decrease barriers to accessing treatment (Cokley, 2006).
Limitations
While the present study provides important insight, findings should be considered in the context of the following limitations. First, women who had been hospitalized or living in a group home during the past year were excluded; thus, findings do not represent treatment utilization and barriers for women who may be experiencing more severe substance use and mental health symptoms. Future research should address the rate of inpatient treatment utilization to better understand barriers that women may encounter when seeking treatment. Further, these findings may not generalize to other individuals who experience IPV, such as men or individuals in same sex romantic relationships. Second, other forms of treatment women may have utilized (e.g., prescribed medication for SUD) were not assessed. This restricts our understanding to psychosocial treatments only. Third, treatment utilization was focused on substance use and mental health resources and services, and therefore, did not reflect other support women may have received (e.g., from domestic violence service providers). Future research should expand the types of services assessed. Fourth, we did not collect information on the effectiveness of treatments, and therefore, are unable to determine whether engagement in treatment was associated with symptom reduction. Future research should examine the extent to which SUD, mental health symptom severity, and IPV severity influence treatment outcomes for this population. Fifth, only participants who endorsed needing treatment but not receiving it had the opportunity to answer questions related to barriers, leading to a small sample size for bivariate analyses and does not represent barriers that may have been experienced by women who did access treatment that could have influenced treatment retention or efficacy. Lastly, it is important to note that women who experience IPV likely face unique barriers to treatment that were not captured in the present study (e.g., stigma related to experiencing IPV, fear of retaliation if their partner accesses their treatment records; Wright et al., 2022) and may have underreported barriers to treatment utilization. Future research could employ qualitative methods to better understand the abundance of barriers specific to women who experience IPV so that strategies can be identified to mitigate those unique barriers.
Conclusions
Findings provide important insights regarding substance use and mental health treatment utilization and barriers to treatment. Findings demonstrate that there are high rates of treatment utilization among women who experience IPV, and mental health and psychological IPV symptom severity are correlated with barriers to utilizing treatment. Future research is needed to examine treatment effectiveness to further understand the varying rates of treatment among women who experience IPV, and to understand for whom barriers are most relevant in order to increase treatment utilization. In addition, this will allow for a better understanding of symptom severity and whether treatment is reducing those symptoms. Furthermore, clinical providers may benefit from screening for psychological IPV and mental health conditions to identify individuals who may be most in need of additional orientation to treatment to reduce attitudinal and confidentiality-related barriers.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605261429549 – Supplemental material for The Influence of Substance Use, Mental Health Symptoms, and Intimate Partner Violence (IPV) Severity on Treatment Utilization Among Women Who Experience IPV
Supplemental material, sj-docx-1-jiv-10.1177_08862605261429549 for The Influence of Substance Use, Mental Health Symptoms, and Intimate Partner Violence (IPV) Severity on Treatment Utilization Among Women Who Experience IPV by Alexis R. Alfano, Melissa R. Schick and Tami P. Sullivan in Journal of Interpersonal Violence
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by National Institute on Drug Abuse grant R01DA031275. Work by the second author was supported by the National Institute on Drug Abuse grant T32DA019426.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.