
Abstract
This study applied network analysis to examine the internal structure of Adverse Childhood Experiences (ACEs) and to develop a network-derived structural framework for prevention and intervention. Using nationally representative data (N = 4,008), we estimated the sex-stratified networks of the 13 ACE domains. Results revealed clustered structures and bridging mechanisms that linked distinct ACE domains. Emotional abuse and witnessing domestic violence consistently emerged as sex-invariant anchors with high centrality and bridging influence. In addition, we identified sex-differentiated cascade pathways, which we term “abuse-driven cascading victimization” in men and “neglect-driven cascading victimization” in women, as well as a shared “psychosocial risk environment” community that reflected common vulnerabilities across sexes. Building on these findings, we developed a structural framework of the ACE model comprising three strata: Public Awareness, Implicit Awareness, and the Social Unconscious, capturing gradients of visibility and clinical detectability. Refined through expert consultation, the model underscores how covert adversities function as gateways to broader ACE networks and clarifies leverage points for screening, targeted prevention, and multisystem coordination. By integrating network metrics with a structural framework, this approach advances beyond cumulative scores or latent class models, and offers an actionable framework for early detection, differentiated intervention, and policy innovation in child maltreatment prevention.
Introduction
Adverse Childhood Experiences (ACEs) encompass a broad set of highly stressful and potentially traumatic events occurring before the age of 18 years, including abuse, neglect, and household dysfunction (World Health Organization [WHO], 2018). Since the seminal collaboration between the U.S. Centers for Disease Control and Prevention and Kaiser Permanente in the 1990s, Felitti et al. (1998) provided an operational foundation, largely centered on intra-familial adversities, that catalyzed a large, multidisciplinary literature spanning social work, sociology, psychology, and medicine. The construct itself has broadened beyond the original 10 items: the WHO ACE-IQ (International Questionnaire) incorporates peer, community, and collective violence to capture co-occurring harm outside the family system (World Health Organization [WHO], 2020). This expansion highlights that ACEs, although heterogeneous in their occurrence across multiple contexts, tend to cluster in systematic patterns, thereby underscoring the importance of investigating their internal structure rather than relying exclusively on cumulative counts. ACEs are both prevalent and consequential.
Evidence indicates that a majority of individuals report at least one of the ACE exposures, with graded associations with proximal psychosocial outcomes such as anxiety, depression, and emotion-regulation difficulties, as well as distal sequelae across the life course, including medical comorbidity and increased premature mortality. Recent systematic evidence further demonstrates robust links between ACE exposure and adult multimorbidity, suggesting that cumulative and co-occurring adversities contribute to a broad burden of chronic disease (Senaratne et al., 2024). In addition, prospective cohort studies have shown that ACE exposure is associated with an elevated risk of premature mortality extending into mid-adulthood (Brown et al., 2009; Yu et al., 2022). Notably, Carlson et al. (2020) reported that up to 97% of the population had encountered at least one form of adversity, underscoring the pervasiveness of these experiences. Taken together, this body of evidence positions ACEs as a central public health priority for prevention and early intervention (WHO, 2020).
Although ACEs have been actively investigated across diverse disciplines, two enduring limitations continue to constrain the translational value of the literature. Conceptually, many studies treat adversities as isolated exposures, even though they typically co-occur and are embedded in interdependent social systems (J. Kim et al., 2025). Fragmented, single-domain approaches risk reductionism by overestimating the salience of highly visible adversities while under-detecting less salient but consequential ones, thereby obscuring the full topology of risk (de Vries et al., 2022; C. Lee et al., 2023). Analytically, linear methods, such as cumulative ACE counts or latent class analysis, either assume homogeneous impacts across domains or rely on unobserved classes that do not directly index the heterogeneous influence of specific adversities (C. Lee et al., 2023).
Network analysis provides a principled alternative for representing ACEs as interconnected systems rather than independent risk factors. In this framework, adversity types are modeled as nodes connected by partial associations/partial correlations (edges), allowing investigators to (a) visualize interdependence, (b) detect clusters (“communities”) that tend to co-occur, and (c) identify high-influence nodes via centrality metrics that may serve as leverage points for prevention (de Vries et al., 2022; C. Lee et al., 2023). Bridge metrics further indicate which adversities connect otherwise separate clusters, potentially propagating risk across domains (Borsboom & Cramer, 2013; M. Kim & Choi, 2020).
Parallel developments in psychiatry underscore the utility of network approaches that capture comorbidity patterns that cut across traditional DSM-5 boundaries and illuminate transdiagnostic processes (Price et al., 2019). Accordingly, beyond psychiatric symptom comorbidity, network methods have migrated to social phenomena with contagion-like, co-occurring dynamics, such as poly-victimization following violence exposure and the cumulative layering of adversity, where dependencies among events are central. de Vries et al. (2022) provide a representative illustration: they model ACE indicators as a conditional-dependence network (e.g., EBICglasso GGM), use community detection to delineate clusters of co-occurring harms, and apply centrality/bridge metrics to identify leverage points for prevention and early intervention. They further argue that conventional approaches, such as using sum scores, latent class models, and single-adversity designs, cannot recover direct relations among adversities and, therefore, advocate network models to estimate conditional associations.
Despite these methodological advances, significant limitations remain in how network approaches have been applied within the ACE literature. Most studies continue to estimate pooled models that implicitly assume structural equivalence across sexes (de Vries et al., 2022; C. Lee et al., 2023), reflecting a broader tendency to treat sex primarily as a covariate or outcome modifier rather than as a dimension along which the internal organization of adversities themselves may differ. However, given extensive evidence that males and females differ not only in the prevalence of specific adversities but also in exposure contexts, developmental timing, and pathways linking adversity to later psychosocial outcomes, this assumption may overlook the broader context of ACEs. Such differences imply that the co-occurrence, clustering, and bridging of ACE domains may follow sex-specific structural patterns rather than a single unified architecture. When network models are estimated in aggregated samples, these structural differences may be obscured, yielding centrality and bridge estimates that reflect an average of heterogeneous processes, thereby under-identifying sex-specific leverage points for prevention and intervention. In parallel, even recent network-based applications have tended to prioritize ACE-outcome associations or population-level surveillance rather than the internal structure of ACEs per se. For example, network and variable-centered models have been used to link ACE exposure to cardiovascular disease and obesity (C. Lee et al., 2023), Internet addiction (Wang et al., 2024), and inflammatory phenotypes (O’Shields et al., 2023). While valuable for etiologic hypothesis building and policy targeting, these approaches are not designed to recover within-person conditional dependencies among ACE domains or to identify bridge nodes that transmit risk across clusters.
Building on these gaps, the present study is designed to propose a structural framework for ACEs by applying network analysis to estimate conditional dependencies among individual adversity domains and examine influential and bridging adversities within the ACE system. We estimated sex-stratified ACE networks to assess the shared and distinct patterns of co-occurrence, expected influence, and bridging across domains. To enhance translational relevance, this study organizes network-analytic findings into a structural framework that positions adversities along gradients of social visibility and clinical detectability, distinguishing adversities that are publicly recognized, indirectly inferred, or under-detected in practice settings. By mapping the network structure onto service-relevant dimensions, this approach shows how screening, early intervention, and multi-sector coordination may be prioritized within detection and response systems.
Therefore, this study aims to (i) examine sex-invariant structural anchors and sex-differentiated cascade pathways within ACE networks, (ii) inform targeted prevention strategies by focusing on adversities with high expected and bridge influence, and (iii) support cross-system coordination by aligning detection efforts with the social salience and detectability of harms. In doing so, this study seeks to move beyond cumulative ACE scores and latent class approaches, offering a structurally informed and practice-relevant perspective for public health prevention, intervention, and policy development.
Current Study
Our aims were threefold. First, we estimated and visualized sex-stratified networks of 13 ACE domains in a nationally representative adult sample and summarized the co-occurrence using community detection. Second, we identified expected influence (EI) nodes that disproportionately activate the system and bridge expected influence (BEI) nodes that connect communities using case-dropping bootstrap diagnostics to assess stability (Epskamp et al., 2018). A priori, we anticipated that emotional abuse and witnessing domestic violence would emerge as sex-invariant anchors with high central and/or bridge influence. We further expected sex-differentiated clustering, with abuse-driven cascading victimization—centered on physical and emotional abuse and their links to other victimization domains (e.g., peer/school violence and sexual abuse)—to be more salient among men, and neglect-driven cascading victimization—centered on emotional and physical neglect and their links to relational/sexual victimization—to be more salient among women, consistent with the differences in guardianship loss and victimization contexts observed in prior work. All the ACE domains assessed in this study (including household challenges, such as household substance use, household mental illness, family member incarceration, and community/collective violence exposure) were included in the sex-stratified network estimation. Next, we incorporated expert consultation to develop a structural framework for ACEs grounded in the network results. This framework organizes adversities by their relative visibility and clinical detectability and links them to practical intervention points across family, school, community, and system levels.
Methods
Data
We used nationally representative data from South Korea collected by the Korea Institute for Health and Social Affairs (KIHASA) in 2017. The target population comprised married adults aged 19 to 59 years who had at least one child under the age of 18 years. Data were collected through structured, in-person household surveys administered by trained interviewers. Stratified random sampling was used to ensure proportional representation by region, sex, and age. All the procedures were approved by the Institutional Review Board, and informed consent was obtained from all the participants (Ryu et al., 2017). As there were no missing values, the final analytic sample comprised the full dataset (N = 4,008).
Measures
ACEs were measured using a modified version of the Adverse Childhood Experiences International Questionnaire (ACE-IQ; WHO, 2018) adapted to the South Korean context by Ryu et al. (2017). The 30-item scale categorizes childhood adversity into 13 domains: physical abuse, emotional abuse, physical neglect, emotional neglect, household alcohol/drug abuse, household mental illness, household incarceration, parental separation or death, witnessing domestic violence, sexual abuse, peer violence, community violence, and collective violence. Community violence refers to witnessing violent crimes within one’s neighborhood, whereas collective violence includes assaults by police or military personnel and violence related to robbery or organized crime. All the items were retrospectively self-reported before age 18 and coded as binary variables (1 = experienced at least once, 0 = not experienced). The scale demonstrated acceptable reliability in this study (Cronbach’s α = .75). Because the ACE-IQ is designed as a retrospective self-report instrument administered at a single time point, inter-rater reliability indices (e.g., Kappa) and test–retest reliability (ICC) could not be estimated within the present dataset. However, prior validation studies of the Korean-adapted ACE-IQ have reported acceptable reliability and construct validity (Ryu et al., 2017).
Analysis
Descriptive and Correlation Analyses
Descriptive analyses were conducted to examine the sociodemographic characteristics of the participants and the prevalence of childhood adversities. Frequency distributions were calculated for categorical variables, whereas means and standard deviations were reported for continuous measures. To assess sex differences, chi-square tests were performed for categorical variables, and independent sample t-tests were applied for continuous variables. This allowed us to identify potential sex-based differences in exposure to adversities and levels of psychological symptoms. Sociodemographic variables included both continuous and categorical measures. Continuous variables included age (years), duration of marriage (years), and monthly household income. Household income was reported in units of 10,000 Korean won (KRW); for ease of interpretation, an average value of 425.33 corresponds to approximately 4.25 million KRW per month (approximately USD 3,200 based on the 2017 average exchange rate). Categorical variables included educational attainment (high school or below, associate’s degree or below, bachelor’s degree and above), and receipt of public assistance (yes/no).
In addition, we examined the interrelationships among the 13 domains of ACEs. Because ACE indicators were dichotomous (experienced vs. not experienced), we estimated tetrachoric correlations to capture the association between the underlying latent continuous variables that give rise to the observed binary outcomes. Tetrachoric correlation coefficients (ρ values) were computed for all pairwise combinations of ACE domains. This method provides more appropriate estimates of the association between dichotomous adversity indicators than Pearson correlations, as it assumes that the binary categories reflect thresholds on underlying normally distributed variables.
Network Estimation and Visualization
Network analyses were performed using the R software (version 4.2.2; R Core Team, 2022). We estimated the network structure of childhood adversities by employing a Graphical Gaussian Model (GGM), a widely used method for constructing partial correlation networks in psychopathology and adversity research (Epskamp et al., 2018). To produce a sparse and interpretable network, we applied the graphical Least Absolute Shrinkage and Selection Operator (gLASSO) in combination with the Extended Bayesian Information Criterion model selection procedure. This approach balances model complexity and fit, pruning spurious connections while retaining meaningful edges. The estimation and visualization were conducted using the qgraph package (version 1.6.7). In the resulting undirected weighted network, nodes represented each ACE domain and edges reflected the partial correlation coefficients between pairs of adversities, controlling for all other variables. Visualization was implemented using the Fruchterman-Reingold algorithm to optimize the spatial configuration of nodes such that strongly connected variables were positioned more closely together.
Community Detection, Expected Influence, and Bridge Centrality
To examine the structural organization of ACEs, we first performed community detection analyses to identify groups of adversities that were more strongly interconnected with one another than the rest of the networks. Community detection was carried out using the igraph package (Csardi & Nepusz, 2006). Specifically, we applied the information-map algorithm (Rosvall & Bergstrom, 2008) to identify clusters of nodes and subsequently used the Walktrap algorithm (Pons & Latapy, 2005) to evaluate the robustness of the resulting community structure. Communities in this context represent clusters of ACE domains that frequently co-occur, providing insight into the latent structure of adversity exposure.
Following community detection, we evaluated the relative importance of individual ACE domains by calculating EI. EI is a centrality index that considers the sum of all edge weights connected to a node, thereby capturing the extent to which a specific adversity contributes to the activation of the overall network (Robinaugh et al., 2016). Because this index incorporates both positive and negative edge weights, it provides a more accurate estimation of node influence than traditional centrality indices. We further computed the BEI to identify adversities that acted as connectors between distinct communities. Bridge nodes are particularly relevant because they may facilitate the spread of risk across separate domains of adversity. The BEI was calculated by summing only the edge weights that linked a node in one community to nodes in another community, thereby isolating adversities that serve as cross-community bridges. To ensure the robustness of the EI and BEI estimates, we implemented a case-dropping bootstrap procedure using the bootnet package (Epskamp et al., 2018). The correlation stability (CS) coefficient was calculated to evaluate the stability of centrality estimates, with values above .25 indicating minimally acceptable stability and values above .50 regarded as preferable.
Expert Consultation for Interpretive Validation
After computing the network analysis, we conducted expert consultation to enhance the interpretive credibility of the findings and to inform the development of the proposed structural framework of ACEs. Given that network analysis often yields complex structures, such as clusters of adversities or highly central nodes, interpretation requires domain-specific insights to ensure clinical, policy, and practice relevance. We convened a panel of five experts with extensive experience in childhood adversity research, clinical mental health practice, and child welfare policy, including academic researchers, policy specialists, and frontline practitioners. Two rounds of online expert consultation were conducted using a focus-group interview format. Experts were presented with network analysis outputs (e.g., centrality indices and community structures) and invited to provide feedback on (a) the substantive interpretation of identified clusters, (b) the clinical and policy relevance of central and bridging adversities, and (c) the applicability of the network structure to prevention and intervention contexts. Importantly, these consultations were not analyzed as independent qualitative data and did not generate standalone qualitative results. Rather, the expert input served as an interpretive bridge between the quantitative network findings and the formulation of the proposed structural framework, supporting theoretical coherence and practical plausibility without altering the statistical results.
Results
Descriptive Statistics of Demographic Characteristics by Sex
Table 1 presents the sociodemographic characteristics of the participants and the prevalence of ACEs by sex. Overall, significant sex differences were observed across the variables of interest. Men were older on average than women (41.68 years, SD = 6.30 vs. 40.12 years, SD = 6.10; t = 7.98, p < .001). Educational attainment also differed significantly, with women reporting lower levels of education more frequently than men (χ2 = 96.11, p < .001). No sex difference was observed in monthly household income; however, receipt of public assistance was more common among women (2.6%) than among men (1.6%; χ2 = 3.91, p < .001). With respect to ACEs, the overall ACE score was significantly higher among men (M = 3.14, SD = 2.43) than among women (M = 2.57, SD = 2.29; t = 7.65, p < .001). The most prevalent adversity for both groups was exposure to collective violence (men 54.7%, women 44.7%), followed by witnessing domestic violence (men 50.0%, women 44.0%) and emotional abuse. The least prevalent ACE was household incarceration (men 0.3%, women 0.1%), followed by household chronic depression (men 1.3%, women 1.2%), with no significant sex differences observed in the latter.
Descriptive Statistics of Demographic Characteristics by Sex.
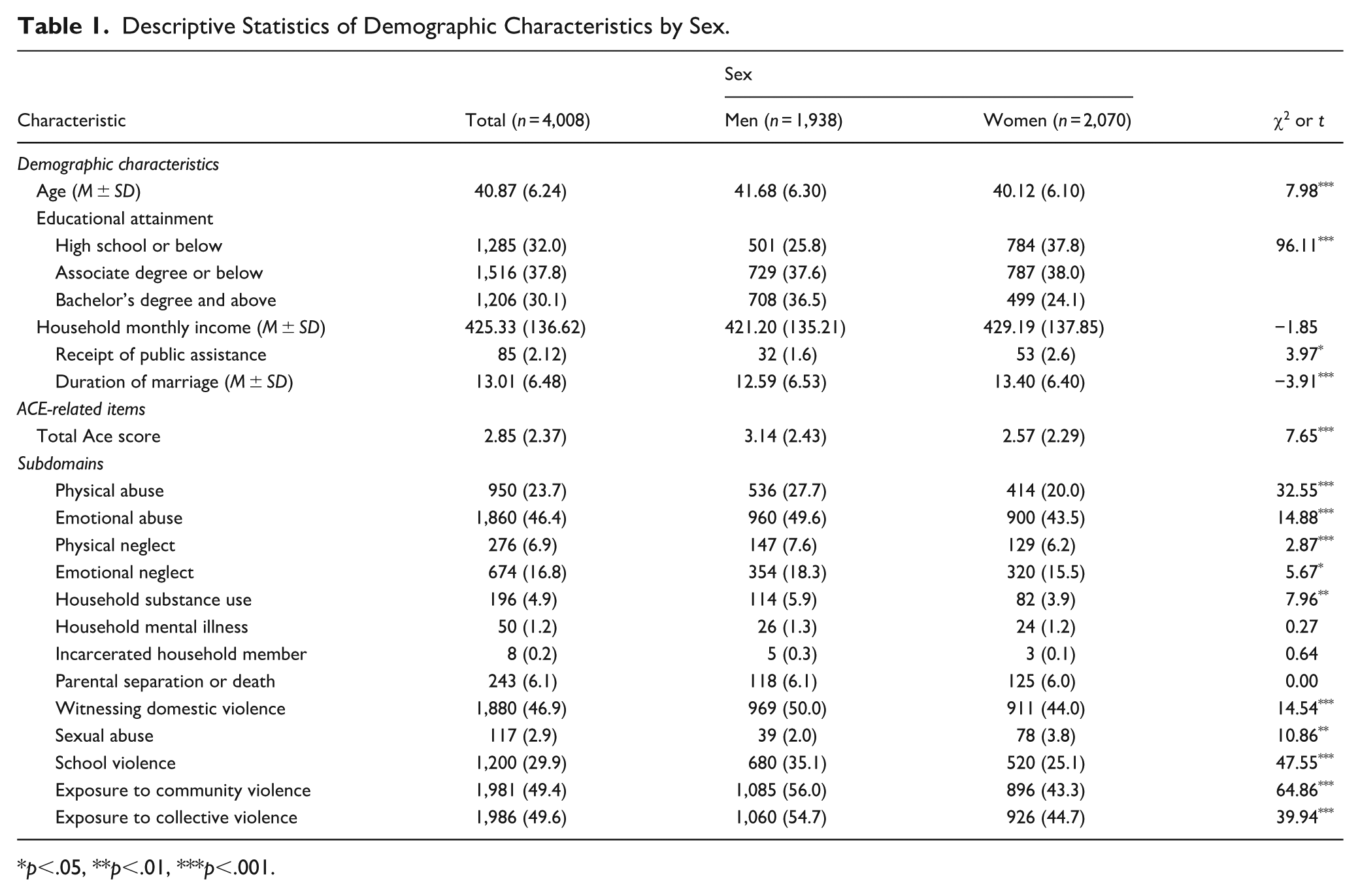
p<.05, **p<.01, ***p<.001.
Correlation Analysis of Binary ACE Variables by Sex
The results of the tetrachoric correlation analyses of the binary ACE variables are shown in Figure 1. Overall, both men and women exhibited positive correlations with most adversities. For men, the strongest associations were between emotional abuse and witnessing domestic violence (ρ = .91), followed by physical–emotional abuse (ρ = .84), and physical abuse–witnessing domestic violence (ρ = .75). Negative coefficients (ρ = –1.00) for rare domains, such as household incarceration, likely reflect sparse data rather than substantive relationships. For women, the strongest correlations involved emotional abuse and witnessing domestic violence (ρ = .92), mirroring the male pattern. However, women generally showed stronger correlations between sexual abuse and other ACE domains, suggesting sex-specific clustering around this adversity.
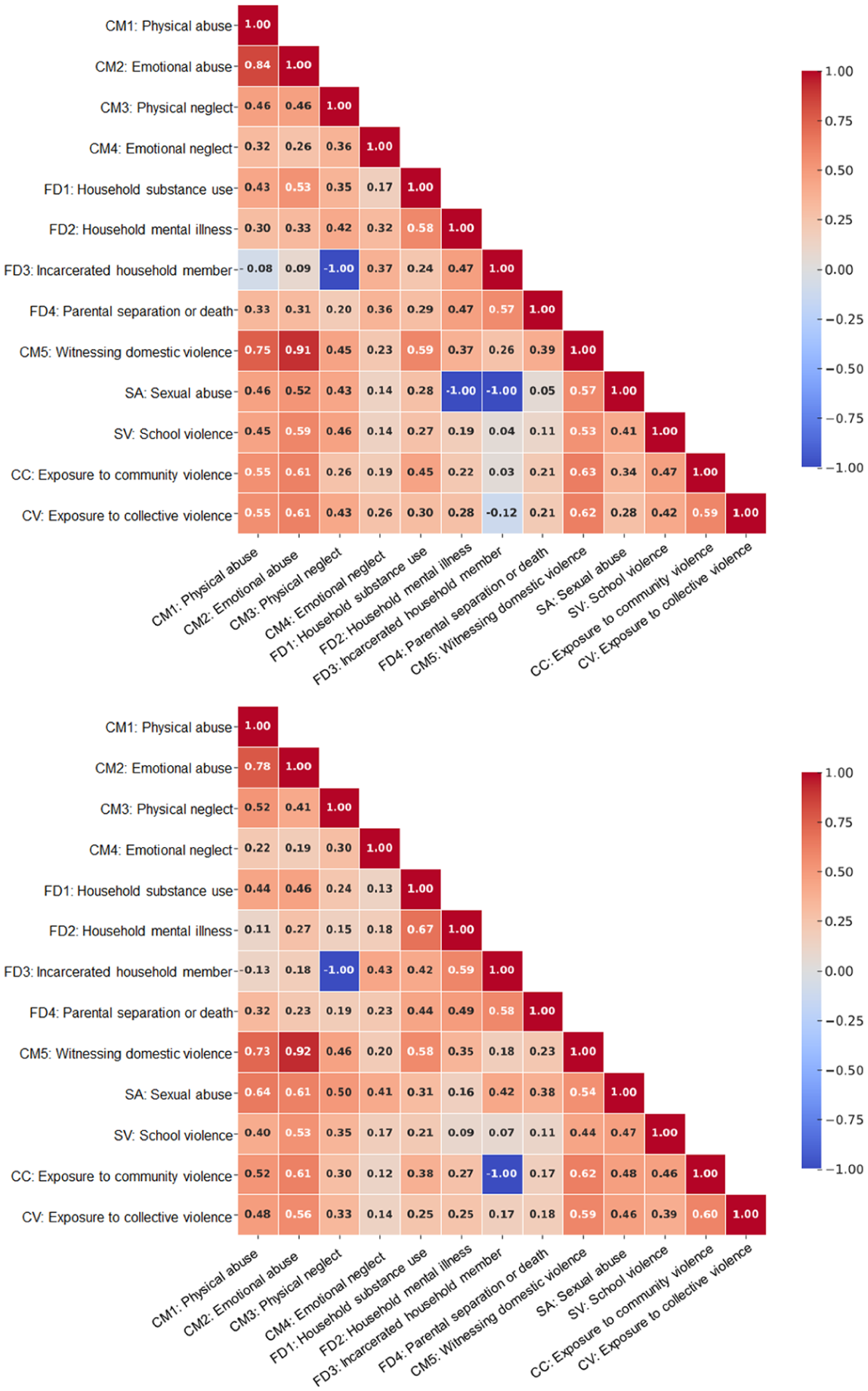
Heatmaps depicting intercorrelations across subdomains of adverse childhood experiences for men (top) and women (bottom).
Network Analysis Results
Central and Bridge ACE by Sex
The CS coefficients for the estimated networks were 0.75 for both men and women, indicating acceptable stability of the network structure (Epskamp et al., 2018). Table 2 summarizes the communities, EI, and BEI values. Overall, the most central and bridging adversities were highly consistent across the sexes. For men, the network comprised 13 nodes with a density of 0.57 (45/78). The most influential adversity, based on EI, was emotional abuse (CM2; EI = 43.7), followed by witnessing domestic violence (CM5; EI = 40.4), and physical abuse (CM1; EI = 35.8). This indicates that these adversities functioned as central nodes driving the activation of the entire ACE network. Regarding bridging effects, BEI analyses identified witnessing domestic violence (CM5; BEI = 21.2) as the most important connector across communities. The strongest edge was observed between emotional abuse (CM2) and witnessing domestic violence (CM5). For women, the network density was somewhat lower at 0.42 (33/78). The EI results closely mirrored those of men, with emotional abuse (CM2; EI = 48.9) emerging as the central node, followed by witnessing domestic violence (CM5; EI = 48.6) and physical abuse (CM1; EI = 40.5). However, the BEI results differed slightly: the most influential bridge node was emotional abuse (CM2; BEI = 25.2), followed by witnessing domestic violence (CM5; BEI = 22.1).
Network Analysis Outcomes Derived from Community Detection Algorithms.
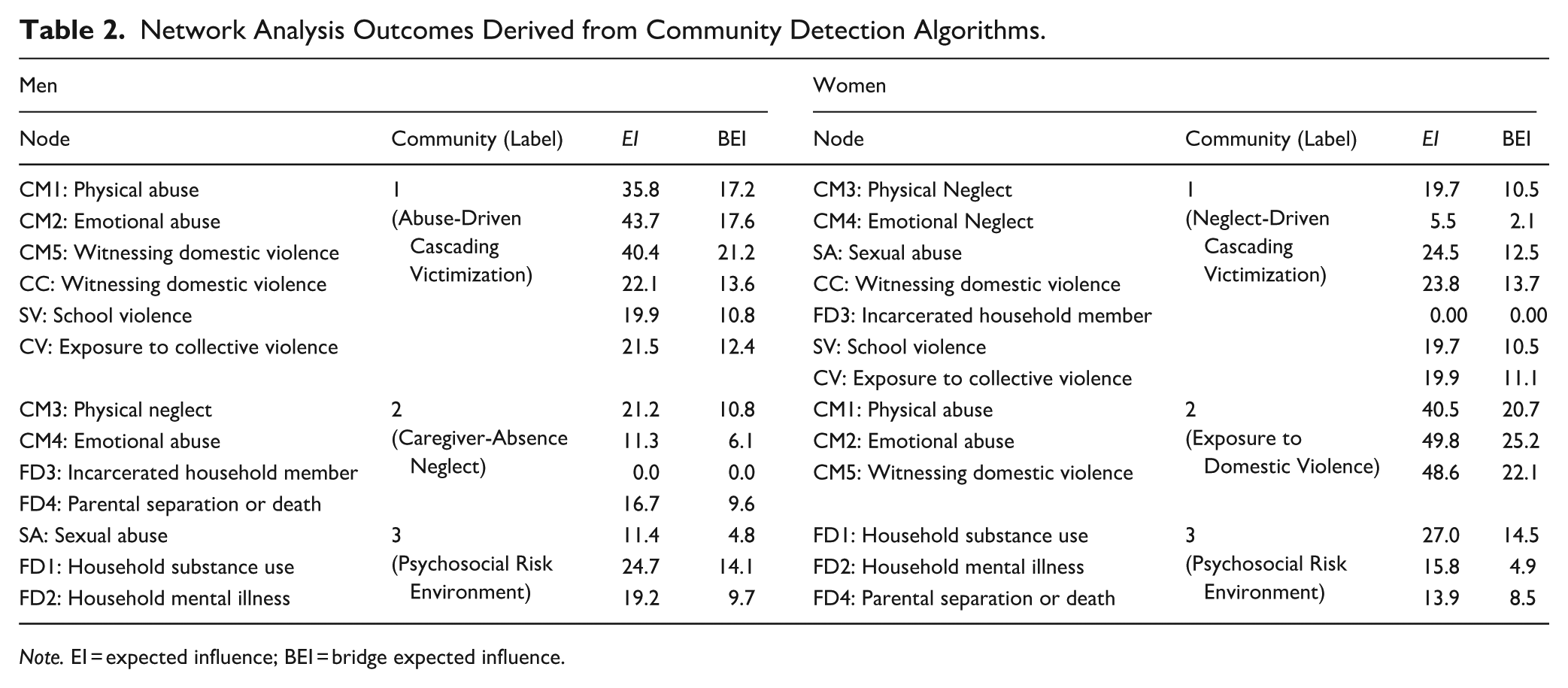
Note. EI = expected influence; BEI = bridge expected influence.
Community Detection by Sex
Community detection using the Walktrap algorithm revealed both common and sex-specific clustering patterns. For men, the largest cluster combined physical and emotional abuse, witnessing domestic violence, and community, school, and collective violence, labeled Abuse-Driven Cascading Victimization. For women, the corresponding cluster included neglect (physical, emotional); sexual abuse; witnessing domestic violence; and community, school, and collective violence, thus termed Neglect-Driven Cascading Victimization. A second cluster among men comprised physical and emotional neglect, household incarceration, and parental separation or death (Absentee Neglect), whereas, for women, it included physical and emotional abuse with witnessing domestic violence (Exposure to Domestic Violence). Finally, both sexes shared a cluster that reflected family-level psychosocial risks. For men, this involved household substance use, mental illness, and sexual abuse, while, for women, it included substance use, mental illness, and parental separation or death. This cluster was labeled Psychosocial Risk Environment, given its enduring family-based vulnerabilities (Figure 2).

Network analysis diagrams illustrating associations among adverse childhood experience subdomains in men (top) and women (bottom).
Proposed Structural Framework ACEs
Based on network analysis, we developed a sex-differentiated structural framework that organizes childhood adversities according to their patterns of interconnection and detectability within the network. Rather than assuming a cumulative or homogeneous structure, adversities were reorganized along gradients of social visibility and clinical detectability, yielding three analytically distinct strata: Public Awareness, Implicit Awareness, and the Social Unconscious. Importantly, these terms are used here as heuristic descriptors of social visibility and clinical detectability and not as adaptations of psychoanalytic or intrapsychic constructs. These strata do not refer to individual psychological processes or levels of consciousness, but rather to differences in how adversities are recognized, inferred, and documented within social, institutional, and service contexts.
Public Awareness corresponds to adversities that are relatively visible and socially recognized as public issues (e.g., physical abuse, school violence, witnessing domestic violence), whereas Implicit Awareness represents adversities that are socially acknowledged yet less readily detected (e.g., neglect, parental separation). Finally, the Social Unconscious encompasses hidden but fundamental risk conditions within the family environment (e.g., household substance use, household mental illness, incarceration), which exert profound effects on children’s development, yet remain systematically under-detected and insufficiently addressed in routine screening, prevention, and intervention systems. Although the detrimental developmental consequences of ACEs are widely acknowledged by global health authorities, these family-level adversities are often less visible, less likely to be disclosed, and less likely to trigger timely intervention because of stigma, normalization within families, and institutional detection thresholds.
Sex-specific distinctions have also emerged. Among men, the model emphasized “Abuse-Driven Cascading Victimization,” at the surface, reflecting the centrality of abuse-related adversities and their role in spreading across multiple domains. In contrast, for women, the most salient surface cluster was “Neglect-Driven Cascading Victimization,” highlighting the role of neglect and sexual abuse in shaping vulnerability. Furthermore, men’s “Caregiver-Absence Neglect” cluster suggests that family disruption (e.g., incarceration, parental separation) is embedded in their structural risk, while women’s “Exposure to Domestic Violence” cluster indicates a stronger integration of abuse and witnessing violence as co-occurring experiences. Despite these differences, both sexes shared a “Psychosocial Risk Environment,” in the deeper, unconscious layer, illustrating the pervasive yet under-recognized influence of adverse family environments on childhood development (Figure 3).
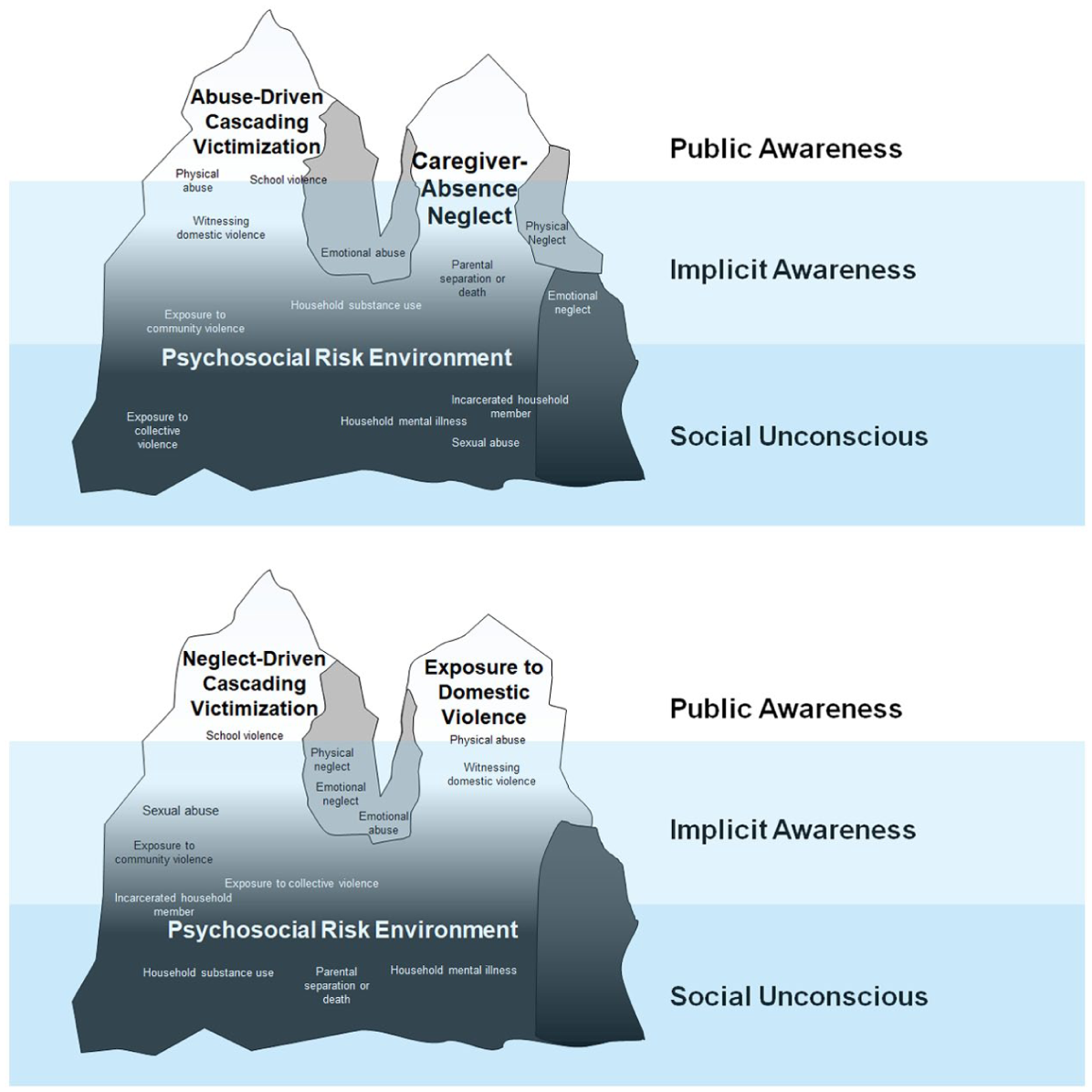
Structural framework of adverse childhood experiences in men (top) and women (bottom).
Discussion
This study applied network analysis to ACEs and proposed a structural framework that advanced the conventional cumulative risk framework. While prior research has often treated ACEs as an additive index, our findings suggest that adversities are interrelated, with specific domains functioning as central nodes that bridge multiple forms of maltreatment and household dysfunction. To interpret these structural layers, we situated the observed ACE network within three societal strata: public awareness, implicit awareness, and the social unconscious.
Importantly, these terms were used as heuristic strata to describe gradients in the social visibility and clinical detectability of the ACE domains. These are not intended to invoke psychoanalytic constructs or individual-level intrapsychic structures; rather, they denote how adversities differ in whether they are publicly recognizable, indirectly inferable through practice and screening, or systematically under-detected due to relational, cultural, and institutional barriers. This visibility-based organization is intended to be a practice heuristic rather than a diagnostic taxonomy. This highlights that adversities differ not only in severity but also in how they are detected, disclosed, and documented factors that shape feasible screening strategies and engagement pathways. Accordingly, intervention planning may benefit from pairing symptom-driven entry points with structured inquiry into less visible adversities that are likely to remain unreported.
Situating this framework within the broader ACE literature, ecological and developmental frameworks have been instrumental in elucidating the multilevel contexts in which childhood adversities arise and exert long-term effects, emphasizing interactions among individual, family, community, and societal systems. Similarly, epigenetic and neurobiological models have advanced our understanding of how early adversity becomes biologically embedded, shaping stress physiology and health trajectories across the life course. However, these approaches primarily emphasize cumulative exposure and etiological pathways rather than structural interrelationships among specific adversities, as they co-occur in contemporary social contexts. In contrast, the present study applies a network-analytic perspective to empirically model how ACE domains cluster and bridge one another with sex-specific patterns. By further organizing these structures along gradients of social visibility and clinical detectability, our framework incorporates sociocultural and institutional processes that shape the recognition and disclosure of adversity. This approach complements existing theories by providing a practice-oriented structural map that highlights leverage points for screening and early intervention.
Importantly, the proposed framework is not confined to a single intervention level. Rather, it is designed to inform intervention planning across all three strata, each corresponding to distinct points of entry within the prevention and care systems. Interventions at the Public Awareness level primarily involve identification, reporting, and immediate protection; those at the Implicit Awareness level emphasize targeted screening, trauma-informed assessment, and relational or school-based support; and interventions addressing the Social Unconscious necessarily operate at structural and family system levels, including caregiver treatment, social policy, and service coordination for chronic household risks. In this way, the framework provides a multilevel intervention map that aligns network-identified adversity structures with differentiated strategies across prevention, early detection, and sustained support, rather than confining intervention to a single domain of visibility.
Three Main Structures of the Proposed Model
Public Awareness includes adversities widely recognized as social problems, such as physical abuse and school violence. These adversities are visible and easily identified by teachers, neighbors, or peers. Prior studies highlight their detectability and public sensitivity toward physical abuse and school violence (Glouchkow et al., 2023; Ho et al., 2017). These adversities have public consensus on their harmfulness and protective mechanisms. However, awareness does not ensure accurate detection or effective protection (Ho et al., 2017). The assumption that awareness and mandatory reporting improve child protection reveals a paradox in child welfare policies. Glouchkow et al. (2023) found teachers’ detection rates for physical abuse were low (58% detection and 27% reporting), highlighting the gap between visibility and identification. Analyses of Universal Mandatory Reporting (UMR) policies, requiring all citizens to report suspected maltreatment, indicate unintended consequences. Ho et al. (2017) reported UMR states had lower rates of confirmed physical abuse (11.9%) than non-UMR states (13.9%). Although UMR increased reports, particularly from non-professionals, the confirmation rate was lower (6.6% vs. 12.0%). This pattern underscores a reporting fallacy: the belief that greater visibility automatically enhances child safety (Raz, 2020). Increased reporting may overwhelm child protection systems with unsubstantiated cases, diverting resources from children in need. Evidence suggests expanded mandatory reporting disproportionately affects marginalized families, including those experiencing poverty, parental mental illness, and incarceration (Haskins, 2015; Ho et al., 2017; Raz, 2020). Thus, even within the Public Awareness stratum, visibility operates through socially stratified lenses, complicating the assumption that recognition translates into protection.
Second, Implicit Awareness refers to adversities that are less visible and rarely acknowledged by the public; however, they exert substantial psychological and developmental consequences closely linked to overt adversities in the Public Awareness stratum. This category includes witnessing domestic violence, emotional abuse, and exposure to community or collective violence, which are forms of indirect victimization consistently associated with developmental risks (Burgos-Benavides et al., 2025). Such exposure erodes children’s sense of safety, compromises stress-response systems, and heightens vulnerability to internalizing and externalizing psychopathology. Covert emotional abuse illustrates this complexity. Through manipulation tactics like gaslighting, emotional withholding, and undermining of self-worth, victims experience depression, anxiety, and somatic symptoms without visible markers, making detection challenging (Parkinson et al., 2024). This invisibility leads others to misattribute reactions to the victim’s presumed hypersensitivity or vulnerability, reinforcing stigmatizing narratives and exposing survivors to secondary victimization (Anda et al., 2006; McLaughlin & Lambert, 2017). Similarly, witnessing domestic violence shows this pattern: children exposed to interparental aggression develop anxiety, PTSD symptoms, regressive behaviors, or peer conflicts that are difficult to trace to the underlying adversity (Burgos-Benavides et al., 2025; Jedd et al., 2015).
Neurobiological disruptions caused by early covert adversities further amplify vulnerability to overt victimization. Deficits in emotion regulation, such as poor emotional understanding, heightened reactivity, and difficulty modulating affect, undermine a child’s ability to navigate interpersonal conflicts safely, increasing the likelihood of peer victimization, school-based aggression, or exposure to community violence (J. Kim & Cicchetti, 2010; Nesin et al., 2025). In turn, these overt incidents further exacerbate emotional dysregulation, creating a feedback loop in which covert and overt adversities reinforce one another in a spiral rather than a simple continuum.
This dynamic interplay underscores the necessity for integrated interventions that address both the concealed impact of Implicit Awareness and the more visible risks of Public Awareness, preventing cumulative escalation. However, a systematic assessment of implicit adversities remains a critical gap. Thus, beyond retrospective self-report, practice settings may benefit from brief, structured modules that triangulate (a) child emotion-regulation indicators (e.g., heightened emotional reactivity, difficulties in soothing or recovery from distress), (b) relational signals (e.g., coercive control, chronic invalidation), and (c) collateral information from schools and caregivers, implemented within trauma-informed interviewing protocols that minimize re-traumatization and under-disclosure. Future measurement work should evaluate whether incorporating such multi-informant, behaviorally anchored screening improves the detection of implicit adversities and strengthens the linkage to early support across healthcare, education, and child welfare systems.
Finally, the Social Unconscious encompasses adversities deeply rooted in family dynamics and broader social environments that often remain unnoticed or insufficiently acknowledged at the societal level. This refers to adversities that are systematically under-detected or rarely disclosed in routine assessment contexts, despite their substantial developmental impact. Chronic psychosocial risks, such as household substance use, family member incarceration, and household mental illness, fall into this category, exerting substantial and enduring influence on children’s developmental trajectories despite their relative invisibility (Anda et al., 2006; Haskins, 2015; Turney & Olsen, 2019). Due to their detection challenges, these conditions are often overlooked in prevention policy, yet they serve as a root layer of the ACEs, amplifying vulnerability across other strata. For example, household substance use illustrates how chronic family-level dysfunction normalizes maladaptive coping strategies and disrupts neurobehavioral dysregulation. Prior research has demonstrated a graded dose–response relationship between exposure to household substance use and later health risk in adulthood, mediated through disruptions in stress-response systems and prefrontal-limbic circuitry (Manhica et al., 2024; Sinha, 2024). Children raised in such environments exhibit heightened amygdala reactivity to threat cues and reduced prefrontal regulation of emotion, increasing their vulnerability to impulsivity, anxiety, and substance use disorders (Turney & Olsen, 2019). These neural adaptations are rarely observable to outsiders and seldom reported, reinforcing the invisibility of Social Unconscious adversities. Additionally, family member incarceration destabilizes the psychosocial–developmental environment through stigma, economic strain, with downstream effects on Hypothalamic–Pituitary–Adrenal (HPA) axis functioning, all of which heighten risk for both internalizing and externalizing psychopathology (Haskins, 2015). Household mental illness further exposes children to inconsistent emotional availability, fostering schemas of insecurity and mistrust that shape long-term social and emotional regulation.
Taken together, the Social Unconscious comprises conditions that largely evade observation, yet exert profound and enduring effects across neural, emotional, and relational domains. Advancing ACE models, therefore, requires moving beyond surface detection toward systemic, family-centered assessments that integrate neurobiological and ecological indicators. Addressing these hidden adversities also demands preventive, structural interventions, such as caregiver treatment, decarceration policies, and accessible mental health services targeting root conditions, rather than only overt manifestations of harm.
Common Issues Across Sex: Emotional Abuse and Witnessing Domestic Violence
A key finding of our network analysis was the central and bridging role of emotional abuse and witnessing domestic violence in both sexes. While prior studies have consistently identified these adversities as severe risk factors, our findings extend this literature by demonstrating their structural function in linking otherwise disparate ACE domains, thereby illustrating how covert adversities operate as gateways into broader ACE networks. Even indirect forms of violence exposure undermine children’s self-concepts through persistent parental rejection, negative evaluations, and withdrawal of affection, which, in turn, foster pervasive emotional dysregulation characterized by emotional instability, hypervigilance, and maladaptive coping (Colley et al., 2024; J. Kim & Cicchetti, 2010).
These structural findings also have implications for how ACE exposure is interpreted in clinical and research settings. Rather than relying solely on a cumulative ACE score, a network-informed approach suggests supplementing sum scores with attention to (a) “anchor” adversities that are consistently central across sexes (e.g., emotional abuse and witnessing domestic violence) and (b) “bridge” adversities that connect otherwise distinct clusters and may facilitate risk propagation. Practically, this can be operationalized as a brief interpretive addendum to standard scoring, flagging the presence of high-influence or bridging adversities, and documenting the dominant configuration (e.g., abuse-dominant vs. neglect-dominant profiles). Such a supplement does not replace cumulative scoring, but provides a clinically actionable nuance by prioritizing follow-up assessment and case formulation around adversities most likely to organize broader co-occurrence patterns.
These central roles can be explained by two mechanisms. Neurodevelopmental evidence elucidates that emotional abuse chronically overactivates the amygdala and impairs medial prefrontal cortex modulation, producing entrenched hypervigilance to negative social signals and diminished capacity for top-down affect control (Peverill et al., 2019). Neural dysregulation fosters heightened threat sensitivity, predisposing children to internalizing disorders and amplifying their risk of peer rejection and victimization (Jedd et al., 2015; J. Kim & Cicchetti, 2010). Because these outcomes fall within overt adversities captured in the Public Awareness strata, emotional abuse functions as a bridge linking covert adversities with overt ACEs. Social cognitive mechanisms show that children exposed to interparental violence develop early maladaptive schemas, particularly punitiveness and mistrust/abuse, which reshape their cognitive-emotional processing of social situations (McLaughlin & Lambert, 2017). The Punitiveness schema reflects internalization of harsh parental figures, leading children to believe violence is the primary response when others fail expectations, while the Mistrust/Abuse schema creates hypervigilance for social threats (Pilkington et al., 2021). These frameworks manifest in social-information processing biases, including hostile attribution, exaggerated threat appraisal, and positive evaluation of violent solutions to conflict.
These findings highlight the need for early targeted intervention that disrupts the bridging mechanisms of covert adversities. Family-based therapies that enhance emotion regulation (e.g., dialectical behavior therapy for adolescents), alongside trauma-focused cognitive-behavioral interventions, can restore adaptive coping and reducing susceptibility to subsequent ACEs. In addition, integrating routine screening for subtle emotional maltreatment and violence exposure into pediatric and school settings may facilitate earlier identification and support, thereby curbing the network propagation of ACEs.
Sex Differences in ACE Patterns: Abuse-Driven Versus Neglect-Driven Adversities
Our results suggest that sex-differentiated ACE trajectories reflect developmental cascade processes across neural, relational, and ecological levels. For men, the predominant “abuse-driven sequential victimization” pathway appears to originate in repeated physical and emotional abuse that sensitizes threat circuitry (heightened amygdala reactivity, HPA hyperarousal) and weakens prefrontal inhibitory control, thereby increasing impulsivity and aggression in peer and community contexts (Jedd et al., 2015). This aligns with evidence that cumulative victimization strongly predicts externalizing psychopathology and is especially common among male populations.
In contrast, women more often follow a “neglect-driven cascading victimization” pathway, characterized by caregiver absence or parental loss (separation, incarceration) that erodes protective monitoring, supervision, and diminishes routine guardianship. This absence significantly heightens situational vulnerability to sexual and relational victimization that erodes protective monitoring and heightens vulnerability to sexual and relational victimization. This process reflects routine activity theory, as diminished guardianship increases exposure to risky contexts. Neglect compromises attachment security and emotion regulation, thereby propelling women toward high-risk relational contexts and exploitative dynamics. Neuroendocrine studies indicate that women with a history of neglect exhibit altered oxytocin functioning, impaired trust, and heightened susceptibility to coercion (Müller et al., 2019). However, neglect showed a different pattern in men. While boys who abused boys tended toward externalizing behaviors, neglected boys were more prone to internalized difficulties such as social withdrawal, often linked to caregiver absence due to incarceration, separation, or death.
Taken together, these sex-specific mechanisms help elucidate why clusters of abuse often precipitate externalizing cascades in men, whereas clusters of neglect are more often implicated in sexual victimization among women and emotional withdrawal among men. From a clinical standpoint, these pathways suggest different assessment priorities and entry points for intervention: abuse-driven patterns may warrant early formulation focused on threat reactivity, impulsivity/externalizing risk, and trauma-related cognitions, whereas neglect-driven patterns may require prioritizing attachment insecurity, relational vulnerability, and exploitation risk, alongside internalizing distress. Policy and practice should, therefore, tailor intervention to these distinct trajectories. For boys exposed to abuse, integrating trauma-focused cognitive-behavioral therapy with executive function training and aggression regulation modules can mitigate the escalation of risk trajectories (Hoogsteder et al., 2022; A. H. Lee & Brown, 2022). For neglected girls, attachment-based mentoring and empowerment interventions should be complemented by physical safety barriers (e.g., low-barrier shelters and safe-harbor protections) to disrupt pathways toward exploitation (Godoy et al., 2025). For neglected boys, early interventions that build emotional literacy and relational competence and provide stigma-free counseling may prevent internalized distress. At the policy level, surveillance systems must move beyond visible abuse to address the hidden neglect and psychosocial risks that accumulate before detection.
Importantly, the proposed framework can be situated within the classical prevention continuum of primary, secondary, and tertiary interventions. Drawing on Gershoff et al. (2017), adversities located within the Public Awareness stratum align with primary (universal) prevention efforts, such as school-based social–emotional learning and parenting programs that reduce harsh discipline and promote early protective factors. The Implicit Awareness stratum corresponds to secondary (selective) prevention, where targeted screening and trauma-informed interventions (e.g., mentoring, attachment-based, or trauma-focused therapies) are directed toward youth exhibiting early signs of risk or relational vulnerability. Finally, adversities embedded within the Social Unconscious map onto tertiary (indicated) prevention require intensive, coordinated responses addressing chronic household risks, including caregiver treatment, mental health services, and cross-system care coordination. By aligning network-identified structures with the prevention continuum, the framework clarifies how ACE-informed interventions may operate across all levels of care, rather than being confined to visible or symptomatic forms of adversity.
Limitations and Future Research Directions
This study had several limitations. First, ACEs were reported retrospectively in adulthood, raising concerns about recall bias, social desirability, and misclassification, particularly for household incarceration. The cross-sectional design and network models preclude causal inference; centrality indices quantify structural importance but do not identify intervention points. Future work should use longitudinal designs to clarify sequencing and test whether altering central nodes reduces risk. Second, measurement choices limit interpretation. ACE domains were dichotomized, sacrificing information on severity, frequency, and timing. Future research should incorporate graded exposure indices and compare network findings to binary estimators and mixed graphical models with sensitivity checks. Third, community detection results are algorithm-dependent. We used information-map detection with robustness checks, but results vary by algorithm. Although bootstrap analyses showed acceptable stability (CS = 0.75), small rank differences warrant caution. Future research should use consensus clustering across algorithms and report confidence intervals for centrality findings. Fourth, external validity is limited by the sampling frame and period of data collection. The target population comprised married adults aged 19 to 59 with at least one minor child in South Korea. In addition, data were collected in 2017, and subsequent social and policy changes (e.g., pandemic-related stressors and shifts in reporting practices) may have altered ACE patterns and detectability. Thus, replication in diverse and cross-cultural samples is a critical next step in this line of research. The organization, visibility, and social interpretation of ACEs are shaped by cultural norms, welfare systems, family structures, and reporting practices, all of which may influence both the co-occurrence patterns of ACEs and their position within network structures. Accordingly, the structural features identified in the present study may vary in salience across sociocultural contexts. Future research should examine whether the network architecture and sex-differentiated pathways observed in this Korean sample are replicated in other cultural settings, including low- and middle-income countries and societies with different child welfare and mental health infrastructures. Comparative network analyses across countries may help distinguish culturally invariant structural features from context-specific configurations, thereby refining the generalizability and applicability of network-informed prevention and intervention strategies.
Conclusion
This study highlights that childhood adversities operate as interrelated manifestations of violence rather than discrete risks. Emotional abuse and witnessing domestic violence emerged as common anchors across sexes, functioning as structural gateways that disseminate risk into broader ACE networks. Distinct cascade patterns further highlight sex-specific vulnerabilities: abuse-driven trajectories in men escalate externalizing violence, and neglect-driven trajectories in women heighten susceptibility to sexual and relational victimization. By translating these findings into a topographic model, we clarify how visible, covert, and hidden adversities interact within systems of violence and reveal concrete leverage points for prevention. These findings underscore the necessity for intervention strategies that disrupt covert violence early, integrate sex-specific pathways of risk, and strengthen multi-sector coordination across family, school, and community contexts. Future research should extend this model both longitudinally and cross-culturally to enhance preventive and intervention efforts aimed at disrupting the cycles of interpersonal violence.
Footnotes
Acknowledgements
We would like to express our deepest gratitude to Prof. Jae Yop Kim and Prof. Soyean Lee for their invaluable guidance and support throughout this research.
Ethical Considerations
The national representative data used in this study were obtained from KIHASA in 2017, conducted in the study of Understanding Connections among Abuse and Violence in the Life Course with explicit permission under the data use agreement. The data was downloaded and utilized strictly per the guidelines and regulations set forth by the Ministry of Health and Welfare of the Republic of Korea. Data were anonymized prior to analysis to ensure the privacy and confidentiality of the individuals involved. The survey was conducted by the principles of the Declaration of Helsinki. All the participants were provided with detailed information regarding the purpose of the study, the procedures involved, and any potential risks or benefits. Informed consent was obtained from all the participants prior to their enrollment in the original study. Participants were assured that their participation was voluntary, that they could withdraw from the study at any time without penalty, and that their data would be kept confidential and used solely for research purposes.
Author Contributions
Joonbeom Kim: Conceptualization, Formal Analysis, Funding Acquisition, Methodology, Software, Visualization, Supervision, Writing—Original Draft, Writing—Review & Editing.
Sumin Son: Conceptualization, Data Curation, Investigation, Project Administration, Resources, Validation, Writing—Original Draft.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2023S1A5B5A17086517). The funder had no role in the study design; the collection, analysis, or interpretation of the data; writing of the manuscript; or the decision to submit the article for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used DeepL to provide the first translation from Korean to English and improve the readability of the manuscript. After using these tools, the authors reviewed and edited the content as necessary and take full responsibility for the content of the publication.