
Abstract
Intimate partner violence (IPV), is one of the most significant sources of psychological distress for women globally, yet mental health remains chronically underserved within IPV service provision, particularly for racialized survivors. This mixed methods study explores how racialized immigrant and nonimmigrant women in Ontario, Canada, experience the psychological impact of IPV and whether their mental health needs were addressed through available services. Drawing on 107 in-depth interviews, the study employs an intersectional, trauma-informed, and culturally responsive feminist methodology. Findings show that survivors primarily sought help not to stop the violence itself but to cope with the accumulating mental health consequences of long-term emotional abuse, coercion, and distress. Many described their emotional pain through culturally rooted idioms, such as “mental block” or “spiritual drowning,” which were often misunderstood or dismissed in Western clinical models. Women reported a severe shortage of licensed mental health providers, culturally responsive therapy, and trauma-informed treatment within IPV agencies. In the absence of appropriate care, women relied on self-guided coping strategies, spiritual practices, and informal supports. This research documents a significant institutional failure to integrate trauma-informed and culturally grounded mental health care into Ontario’s IPV response system. It contributes to IPV scholarship by centering racialized survivor voices and offering recommendations for embedding culturally safe, trauma-responsive mental health support within shelters and social service agencies.
Keywords
Introduction
Intimate partner violence (IPV) is one of the most emotionally harrowing public health and human rights crises globally, with well-documented associations to long-term psychological harm, including post-traumatic stress, depression, and suicidality (Al-Alosi, 2020; Aversa, 2022; Cavalcanti Pereira Lima, 2024; Dillon et al., 2013; George et al., 2022; World Health Organization [WHO], 2021).In Canada, regrettably, racialized women are facing disproportionately higher rates of IPV (Chan, 2020; Holliday et al., 2020; 2021; Tasbiha & Zaidi, 2025), with some communities experiencing significantly greater levels of harm than the national average (Statistics Canada, 2021). In Canada, 44% of women report experiencing some form of IPV since age 15, with higher rates among immigrants and refugees, particularly those facing insecure legal status, language barriers, and social isolation (Guruge et al., 2012; OCASI, 2020; Statistics Canada, 2021). Statistics Canada’s 2025 report on IPV states that the true scope of IPV due to “underreporting” and barriers to disclosure are linked to fear, dependency, and psychological distress among survivors.
In this paper, “racialized women” refers to women whose social locations are shaped by systemic and structural marginalization based on race, ethnicity, and cultural identity within the Canadian context (Ontario Human Rights Commission, 2005; Statistics Canada, 2021; Hankivsky, 2012; Galabuzi, 2006). While overall reported rates among racialized women appear lower than the general population, this often reflects barriers to disclosure such as fear, stigma, language obstacles, and mistrust of formal systems (Ammar & Zaidi, 2019; Mohamed, 2023; OCASI, 2020). This pattern is reinforced by national data, where Cotter (2021) found that while immigrant and visible minority women report lower rates of IPV than nonimmigrant women, including both racialized and non-racialized Canadian-born women, these figures likely reflect significant underreporting due to cultural stigma, institutional mistrust, and fear of repercussions. Within specific communities, including Black, Arab, and Latin American women, experiences of emotional, physical, and psychological abuse are alarmingly common (Statistics Canada, 2021). These women frequently navigate layers of discrimination, cultural pressure, and limited access to supportive services, which compound the trauma of abuse (Dasgupta, 2022; Guruge et al., 2015). Despite seeking safety and healing, many are met with systems that fail to recognize or respond adequately to their lived realities, leaving their emotional needs unmet and their voices marginalized (Aversa, 2022; Cavalcanti Pereira Lima, 2024). The challenges faced by racialized women in reporting and recovering from IPV reveal urgent gaps in Canada’s approach to violence prevention and mental health care (Tasbiha & Zaidi, 2025).
Despite the severity of IPV-related trauma with racialized women, culturally institutional responses to mental health in Canada remain inadequate. Most IPV services continue to prioritize housing and legal aid, while culturally responsive trauma-informed mental health care is underfunded or absent and, at times, goes unrecognized. IPV agencies often lack licensed professionals, with many relying on caseworkers untrained in psychological care (Ahmadzai, 2015; George et al., 2022). Racialized women survivors arrive at these services with profound psychological needs only to encounter structural deficits and systemic indifferences (Alaggia et al., 2017; Couture-Carron et al., 2022). This, compounded with their IPV survivorship, becomes challenging. What becomes especially challenging is the emotional toll of navigating trauma while simultaneously confronting language barriers, fears related to immigration status, cultural stigma, and institutional mistrust, factors that significantly complicate survivors’ ability to access timely and culturally aligned mental health care (Centre of Excellence for Research on Migration and Integration, 2026).
Racialized women survivors of IPV often face a range of systemic barriers that impede access to effective mental health care. These include language isolation, cultural stigma, racism, and insecure immigration status, which collectively constrain help-seeking pathways (Crenshaw, 1991; Guruge et al., 2010). Such intersecting challenges complicate the process of seeking support. Many survivors report that emotional distress, rather than physical violence, was their primary motivation for accessing services (Harper, 2022). However, these services are frequently misaligned with their lived realities and cultural identities, resulting in a compounded burden: the trauma of IPV and the trauma of unsupported or culturally inappropriate recovery (Dasgupta & Melvin, 2024; Ammar & Zaidi 2019). These disparities in care are well-documented and underscore persistent inequities in access to trauma-informed mental health services, particularly among racialized and immigrant women survivors (Barrett et al., 2020; Hyman et al., 2009). In response to these systemic gaps and inequities, this study is guided by the following five research objectives:
To explore how racialized women describe their reasons for seeking support from IPV agencies, with particular attention to how mental health distress figures into their help-seeking journeys.
To understand the psychological and psychosomatic experiences articulated by immigrant and nonimmigrant racialized women as they navigate intimate partner violence.
To examine survivors’ perceptions of the cultural relevance, emotional safety, and overall appropriateness of the mental health support offered within IPV agencies.
To interpret how intersecting factors, such as immigration histories, linguistic barriers, racialization, and cultural identity, shape survivors’ pathways to healing and recovery.
To generate survivor-informed recommendations for strengthening trauma-informed, culturally grounded mental health supports within Canada’s IPV service system.
In this study, immigrant women include both recent newcomers and long-term immigrants, while nonimmigrant women refer to Canadian-born racialized participants. These groups are not interchangeable: Not all racialized women are immigrants, and not all immigrant women are racialized. Distinguishing between these groups allows for a more nuanced interpretation of how migration histories, cultural norms, and racialization uniquely shape mental health experiences after IPV. These objectives are interpretive rather than statistical; they focus on how survivors experience, perceive, and navigate mental health needs in relation to IPV, rather than attempting to measure prevalence or generate population-level causal inferences. These analyses refer to how survivors described these phenomena, not numerical measurement of population-level patterns.
To guide this analysis, the study integrates an intersectional lens with trauma-informed care (TIC) to interpret how structural inequalities and trauma histories shape survivors’ mental health experiences. This exploratory research examines how the intersecting spaces of race, gender, immigration status, and language intensify the psychological trauma of IPV and compound it with systemic neglect in recovery (Broaddus, 2020; Dasgupta & Melvin, 2024). Both these social explanations act as a theoretical lens to analyze how systems of immigration, racialization, and gendered service provision intersect to shape survivors’ experiences with IPV and mental health, as well as work as an intervention model promote safety, empowerment, and cultural relevance for racialized women.
Centering on racialized survivors’ voices, this study challenges Eurocentric service models that treat mental health as peripheral and instead argues for culturally competent care embedded within IPV agencies (Ammar & Zaidi, 2019). This study calls for a reimagining of IPV services where trauma recovery is not outsourced or secondary but a core integrated practice. As rates of IPV and related mental health distress continue to rise in Canada (CAMH, 2023; Statistics Canada, 2025), this research contributes a timely and policy-relevant intervention into gender-based violence and health equity debates, advocating for intersectional survivor-led and structurally responsive care systems (Aversa, 2022; Cavalcanti Pereira Lima, 2024).
Literature Review
IPV has been long recognized to be among the primary causes of adverse mental health consequences in women, including depression, anxiety, post-traumatic stress disorder (PTSD), suicidality, and psychosomatic symptoms (Dillon et al., 2013; Thomas et al., 2008). For racialized women in Canada, IPV effects are exacerbated by structural barriers such as racism, linguistic marginalization, immigration, and cultural stigmatization that all effect survivors’ access to resources and trauma (Ammar & Zaidi, 2019; Couture-Carron, et al., 2022; OCASI, 2020; Tasbiha & Zaidi, 2025). Despite the obvious intersection between IPV and mental health, service models in Canada fail to integrate trauma-informed and culturally sensitive mental health services into IPV support systems (Ammar & Zaidi, 2019; Tasbiha & Zaidi, 2025).
IPV, Mental Health, and Racialized Immigrant Women in Canada
The Psychological Aftermath of IPV: An Ongoing Crisis
The emotional and psychological effects of intimate partner violence are increasingly recognized not only as personal trauma but as a pressing public health issue shaped by social determinants, structural inequalities, and institutional barriers (Kanter & Hassija, 2026; Public Health Agency of Canada, 2023; Statistics Canada, 2025; World Health Organization, 2021; World Health Organization, 2023). For racialized immigrant women, this trauma is compounded by the erasure of cultural worldviews from mainstream service models (Guruge et al., 2012). Survivors frequently experience a “disintegration of self” (Thomas et al., 2008), a state where prolonged abuse erodes identity, agency, and the capacity to seek help. This condition is worsened by fear of stigma, cultural misalignment, and revictimization by Eurocentric mental health systems (Aversa, 2022; Dasgupta, 2022). Canadian studies repeatedly document elevated rates of PTSD, depression, anxiety, and psychosomatic symptoms in immigrant women IPV survivors (Anitha, 2023; Okeke-Ihejirika, et. al., 2020).
Despite growing awareness, Canadian IPV agencies remain underprepared to address these mental health impacts. Survivors reported that housing and legal services were prioritized, while psychological support was underfunded or delivered by generalist staff with limited cultural or clinical training (Cavalcanti Pereira Lima, 2024). These systemic failures disproportionately affect racialized women, particularly those facing multiple forms migration-related uprooting, loss of social networks, and cultural dislocation, as well as marginalization. The need for trauma-informed and culturally responsive care is now widely recognized in the scholarly literature (Beilke, 2024; Dasgupta, 2022). Such care must move beyond superficial multiculturalism to restructure service delivery around safety, empowerment, and survivor-defined healing.
Ignoring these shifts, as scholars argue, risks replicating patterns of control within IPV services themselves (Ammar & Zaidi, 2019; Tasbiha & Zaidi, 2025). In summary, the psychological aftermath of IPV for immigrant women is layered and long-term, rooted in both personal abuse and structural neglect. Survivors require not only safety but also culturally congruent mental health care to support lasting healing. These elevated rates indicate that racialized and immigrant survivors may require mental health supports that are culturally attuned and trauma-specific, yet such services remain scarce within mainstream IPV agencies, a gap this study investigates qualitatively.
Service Barriers & Systemic Gaps in Mental Health Services
Despite growing awareness of IPV’s psychological effects, a broad spectrum of evidence now highlights a persistent lack of mental health infrastructure within Canadian IPV services, particularly for racialized immigrant women (Ammar & Zaidi, 2019; Tasbiha & Zaidi, 2025). IPV survivor organizations tend to prioritize crisis intervention, housing, and legal assistance, while mental health services are often underfunded or treated as secondary. Even when such services are nominally available, they are typically delivered by generalist caseworkers rather than licensed mental health professionals, and they rarely address survivors’ linguistic, racial, or cultural needs (Cavalcanti Pereira Lima, 2024). Chan (2020), in Hiding in Plain Sight: Immigrant Women and Domestic Violence, further emphasizes that immigrant women are not only at heightened risk of abuse but are also systematically underserved by mainstream IPV services that fail to reflect their psychosocial and cultural realities.
Racialized women navigating Canada’s IPV systems, as noted by Alaggia et al., (2017) and OCASI (2020), often encounter “one-size-fits-all” interventions that reinforce the very marginalization they are trying to escape. For example, shelters may lack interpretation services, culturally competent staff, or trauma-informed psychological care. The lack of professional mental health services is particularly harmful for racialized immigrant women, especially refugees or those with precarious legal status, who are more likely to experience layered trauma resulting not only from IPV but also from prior displacement, war, and migration-related stressors (Ammar & Zaidi, 2019; Cavalcanti Pereira Lima, 2024; Couture-Carron et al., 2022; Tasbiha & Zaidi, 2025).
Sanhueza-Morales et al. (2025) echo these concerns, reporting that immigrant and ethnic minority survivors, along with community organization workers, identify institutional rigidity and cultural misalignment as persistent barriers to accessing IPV services. Similarly, George et al. (2022), in their analysis of 15 Ontario Family Law case files, found that service fragmentation fails to address survivors’ intersecting vulnerabilities, such as cultural isolation, economic precarity, and legal instability. They simply argue for a coordinated, interdisciplinary, and culturally informed “one-stop” model to more effectively address domestic violence as coercive control and to provide holistic support for both survivors and their children. Together, these overlapping barriers contribute to a deeper mental health burden for racialized immigrant women and underscore the urgent need for integrated, trauma-informed, and culturally responsive care (Beilke, 2024).
The Call for Trauma-Informed and Culturally (TIC) Responsive Care
Culturally responsive and TIC practices are increasingly recognized as essential for improving outcomes among diverse populations (McEvoy et al., 2024). Scholars such as Beilke (2024) and Dasgupta (2022) similarly emphasize the growing consensus that integrating such approaches into IPV services is not only a critical policy imperative but also an ethical responsibility and mandate. Trauma-informed practices recognize the long-term emotional and social consequences of violence and emphasize survivor safety, voice, and choice (Beilke, 2024; Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). Culturally responsive care acknowledges the specific cultural, racial, and linguistic needs of survivors, ensuring that support is not only accessible but also meaningfully responsive to their lived realities and healing trajectories (Guruge et al., 2015). Critelli and Yalim (2021), drawing from research in a mid-sized U.S. city, emphasize that improving access to IPV services for immigrant and refugee women requires integrating trauma-informed practices that are culturally relevant and responsive to settlement-related stressors. Similarly, Mengo et al. (2024), in their qualitative study with adolescent girls and adult refugee women survivors, found that survivors’ knowledge, perceptions, and lived experiences shaped whether and how they accessed domestic violence services, with cultural stigma, service invisibility, and fear of institutional judgment emerging as persistent barriers.
In the Canadian context, culturally responsive care involves more than multicultural “add-ons” to existing systems. It requires system change in the design, delivery, and evaluation of services. Ammar & Zaidi 2019) argue that IPV services must be reimagined with community-based, intersectional, and immigrant-led approaches that recognize racialized women as experts in their own recovery and not as passive victims. Tasbiha and Zaidi (2025) also argue that ignoring this shift risks continuing the same control and neglect patterns survivors are subjected to in abusive relationships. Comparably, a national scoping review by Okeke-Ihejirika et al. (2020) highlights how immigrant women in Canada face distinct barriers to IPV disclosure and support, including cultural stigma, institutional misalignment, and a lack of intersectional policy responses.
Relevance to the Current Study
In combination, this review of the literature displays racialized women carry a double load in matters related to IPV: the psychological pain of IPV and structural failure to meet their mental health needs. While education regarding IPV is growing in Canada, institutional absence of trauma-informed, culturally grounded mental health services remains a persistent deficit. This study fills this void by hearing the authentic narratives of racialized women themselves, prioritizing their concerns, frustrations, and suggestions on creating and reforming services that impact mental health. This work contributes and is an extension to the growing body of literature, which asserts that healing needs to be just, culturally framed, and survivor led.
To address the distinction raised in the literature between the nature and intensity of challenges, this study conceptualizes racialized survivors’ experiences as shaped by both. Structural factors such as immigration precarity, language barriers, and racialization alter the nature of the obstacles survivors face, while the cumulative layering of trauma from IPV, migration stress, and socioeconomic instability increases the intensity of psychological need. The qualitative design allows these dimensions to emerge directly from survivors’ narratives.
Theory
This study draws on two complementary frameworks: intersectionality and TIC to examine how racialized women navigate IPV and the failures of mental health systems to support their healing. Together, these frameworks illuminate both the roots of survivors’ marginalization and the necessary principles for creating safe, responsive services (Cardenas, 2023; Crenshaw, 1991; Wathen & Mantler, 2022).
Understanding Interlocking Oppressions: An Intersectional Approach
Intersectionality, as developed by Crenshaw (1991), explains how systems of oppression, such as racism, sexism, xenophobia, and class inequality, interact to shape the lived realities of racialized women. Rather than referring to the stacking of individual identities, intersectionality highlights how structural forces converge to produce specific forms of vulnerability for survivors navigating IPV and mental health systems. Instead of considering race, gender, and immigration status as isolated sources of disadvantage, intersectionality highlights and emphasizes how these identities come together to produce specific forms of vulnerability for racialized women survivors of IPV. For example, a woman’s experience of violence and her ability to access mental health care may be shaped simultaneously by cultural stigma, language isolation, racial discrimination, and legal precarity (Bruckert & Law, 2018;Cardenas, 2023; Crenshaw, 1991; Kelly, 2011; Mackey, et al., 2025). Intersectionality, here, refers to the combined effects of racism, xenophobia, and patriarchy that interact in the lived experiences of racialized women, shaping both their vulnerability to IPV and their exclusion from responsive care (Aversa, 2022). This framework allows for a more nuanced understanding of how trauma is experienced and how systemic gaps in services disproportionately affect racialized women in IPV situations.
By underscoring how overlapping identities shape survivor experiences, intersectionality exposes the structural nature of trauma and reveals how mental health systems consistently fail racialized women by overlooking these compounded vulnerabilities (Ammar & Zaidi, 2019; Collins, 2020; Crenshaw, 1991 ). It reframes IPV not as an isolated or individual issue, but as a systemic problem rooted in broader institutional and governmental neglect of those situated at the intersections of multiple forms of oppression (Aversa, 2022; Guruge et al., 2010; Thomas et al., 2008).
Trauma-Informed Care
Recognizing the widespread influence of trauma on individuals and communities, TIC functions as both a philosophical orientation and a practical framework for service delivery (Merlo & Bratina, 2022; SAMHSA, 2014; Wathen & Mantler, 2022). TIC challenges conventional, clinical-only views of trauma by emphasizing that trauma is also a psychosocial and relational experience, one that affects survivors’ emotional regulation, physical health, trust in others, and interactions with public systems (Kulkarni, 2019; Ponic et al., 2016).
Grounded in a set of core principles, TIC encourages organizations to create environments that embody:
safety, trustworthiness, and transparency;
peer support and mutual collaboration;
empowerment, voice, and choice; and
cultural, historical, and gender responsiveness.
In the context of IPV and racialized women, TIC acknowledges that survivors often face compounding trauma, not only from physical abuse but also from emotional manipulation, financial control, cultural silencing, and systemic marginalization (Moore et al., 2025; Warshaw et al., 2013). This layered trauma can manifest as PTSD, anxiety, depression, or disassociation, and alienation.
Notably, TIC warns that when services are dehumanizing, culturally irrelevant, or delivered by unqualified or nondiverse professionals, they can become sites of retraumatization (Halloran et al., 2025; Little, 2024). This concern is particularly acute for racialized immigrant women, who, as demonstrated in this study, encounter significant mental health burdens related to IPV yet face structural barriers in accessing support. These include the absence of licensed mental health professionals, lack of cultural competency, and inadequate language interpretation services (Ammar & Zaidi, 2019; Guruge et al., 2012). TIC, therefore, is not simply about understanding trauma but about actively resisting practices that compound it, especially in healthcare and social service systems that engage with survivors from diverse cultural and migratory backgrounds.
An Intersectional Trauma-Informed Framework
Intersectionality and TIC emerge from different philosophical approaches, critical race feminist theory and clinical social service practice, but collectively they provide a powerful lens for understanding and addressing the experiences of racialized women survivors of IPV. Intersectionality explains how overlapping systems of oppression such as racism, sexism, and precarious immigration status shape vulnerability and limit access to care (Collins & Bilge, 2020; Crenshaw, 1991; Hankivsky, 2012). In contrast, TIC focuses on how support services can respond to trauma in ways that are emotionally safe, culturally sensitive, and empowering (Bowen & Murshid, 2016; SAMHSA, 2014, Sweeney & Taggart, 2018). Together, intersectionality and TIC allow for a holistic analysis of IPV as both a personal and structural crisis. Intersectionality makes visible the compounded vulnerabilities faced by racialized women, while TIC offers a model for healing that centers safety, cultural responsiveness, and survivor agency.
The power of this research is that it eloquently draws on both approaches to examine not only the voices of racialized women IPV survivors but also extends itself to the structural gaps in mental health services available to them. The persistent lack of culturally grounded and trauma-informed mental health support within Canada’s IPV sector reveals a deeper pattern of systemic neglect and disregard that disproportionately impacts racialized immigrant and nonimmigrant women (Cavalcanti Pereira Lima, 2024; Guruge et al., 2012; Mohamed, 2023). Although the psychological impacts of IPV are well established for women, survivors from immigrant backgrounds face intensified harm when services fail to align with their cultural values, lived experiences, or trauma histories (Dillon et al., 2013; WHO, 2021). A more collaborative approach is needed in how mental health care is designed and delivered (Ahmed et al., 2024; Dasgupta, 2022). This research calls for a new care model that centers survivors as agents of change, advancing healing, justice, and culturally grounded support systems.
Methodology
Sampling and Recruitment
This study analyzed 107 qualitative interviews conducted with racialized women survivors of IPV in the GTA. Because of the reported challenge in accessing IPV survivors (Cullen, 2023; Erez & Ammar, 2003; Hellmuth et al., 2013), a larger sample and more diverse sample was not feasible. Participants were recruited using non-probability purposive sampling through 1 to 2 community-based women’s counseling agency and/or shelters located in the Greater Toronto Area. Staff informed eligible women about the study, and those who expressed interest contacted the researcher directly via email or phone for confidentiality purposes. Because recruitment relied on agency-based pathways rather than population-based sampling, findings were not generalizable and should be understood as contextual to this sample. Frontline workers distributed flyers and provided general information to clients. No organization provided participant names or pressured clients to participate. This recruitment strategy was intentionally designed to reach diverse racialized survivors currently accessing community support while preserving ethical independence in selection. Eligibility criteria included the following: (1) identifying as a racialized immigrant or Canadian-born racialized woman, (2) having experienced IPV within the past 10 years, and (3) being over the age of 18. No restrictions were placed on immigration category, relationship duration, or type of abuse experienced, to ensure diversity of lived experiences.
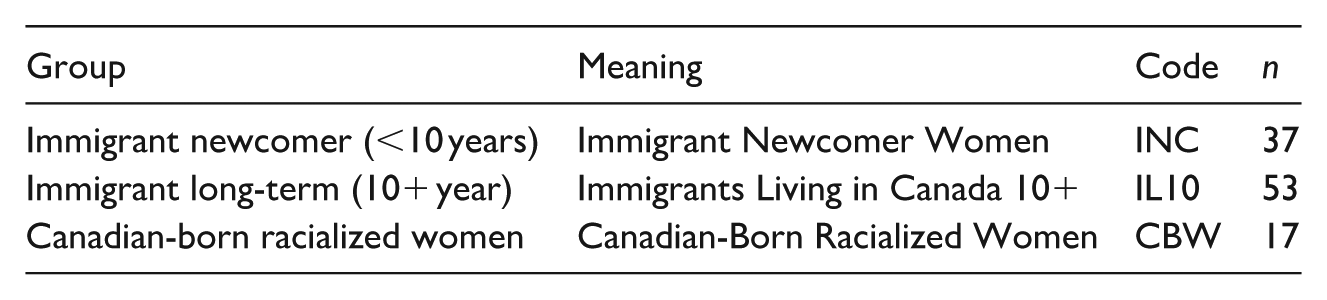
The three relevant groups were as follows:
Immigrant Newcomer Women (INC): Immigrants in Canada for 10 years or less.
Immigrants Living in Canada 10+ Years (IL10): Immigrants in Canada for more than 10 years.
Canadian-Born Racialized Women (CBVM): Canadian-born racial minority women who reported having experienced IPV.
These three groups were selected to capture a range of immigrant and racialized women’s experiences with IPV and mental health services. Immigrant Newcomer Women (INC) represent recent arrivals who may face acute challenges such as language barriers, legal precarity, and limited knowledge of available services. Immigrants Living in Canada for 10+ Years (IL 10) provide insights into how long-term settlement shapes access to care, acculturation, and evolving service needs. Canadian-Born Racialized Women (CBVM) allow for the comparison of experiences not shaped by recent immigration but still influenced by systemic racism and cultural marginalization. Together, these groups offer a comparative framework to examine how length of time in Canada, migration status, and racial identity intersect to shape survivors’ access to and experiences with mental health and IPV services. This sample reflects survivors who were currently engaged with support agencies and therefore does not represent all racialized women experiencing IPV, including those who do not or cannot access services.
Participants came from a range of countries, some of which included the following: Pakistan, India, Jamaica, Sri Lanka, Syria, Afghanistan, Barbados, China, and Guyana. While equal group quotas were not required, the group categorizations also guided recruitment efforts and data analysis. Interviews took place either in private rooms at the community partner site or in secure locations selected by the participants, like their place of residence. This was done to ensure comfort and confidentiality. Most importantly, participants felt safe at the community partner site. Participants received an honorarium of $35 as a small token of appreciation for their time and participation. Below is a table of key demographic characteristics of the sample by each group.
Research Design and Data Collection
A mixed-methods approach that included both the quantitative and qualitative methodologies was adopted, with a heavy focus on qualitative methods. Because the research sought to examine meaning-making, lived experience, and trauma processes, qualitative methods were the most appropriate for capturing emotional and culturally grounded dimensions of IPV. Closed- and open-ended question were employed to establish the richness of IPV experiences for racialized immigrant and Canadian-born women. At the end of each interview, a survey was given to establish statistical trends and relationships among the groups of participants. Because this study employed a non-probabilistic or non-randomized purposive qualitative design, its goal is not statistical or econometric generalizability but analytic generalizability, where the aim is to develop conceptual insight into how racialized survivors describe mental health needs and service barriers. The quantitative component was strictly restricted to descriptive anlayses to assess trends of the data and were included only to contextualize demographic patterns; no inferential statistical claims were made for this data; nor any generalizations from a sample to population.
Data Analysis: Qualitative & Quantitative Analyses
All face-to-face audio-recorded interviews were transcribed verbatim and analyzed using NVivo to facilitate systematic coding and thematic exploration of the qualitative data. Any quantitative data were analyzed using SPSS. Data were discussed together with community partners, and findings of key significance were reported to participants through different means. The quantitative component played a limited but supportive role by providing demographic context that informed the qualitative interpretation. This study employed a primarily qualitative approach. There were three central themes, which emerged from the data: (1.) Mental health as a key reason for service use; (2.) Long-term emotional consequences of IPV; and (3.) Lack of professional, culturally responsive mental health care. The analytic goal is to capture depth and complexity in survivors’ accounts, particularly culturally grounded idioms of distress, help-seeking motivations, and perceived institutional responses, elements that cannot be adequately examined through quantitative modeling alone. The coding was as follows for each racialized group of women:
Ethical Considerations
Prior to data collection, the research was officially approved by the University’s Research Ethics Board. Informed consent was maintained for all participants, who were assured confidentiality and anonymity. Written and verbal consent was obtained. For non-English speakers, interpreters or translated consent forms were provided. Most interviews were conducted in English with language support available. Participants were free to withdraw from the study at any point without losing their honorarium. Pseudonyms were used to ensure anonymity.
Researcher Reflexivity and Positionality
As researchers, we recognize our own positionalities and the influence of cultural familiarity and distance in interpreting participants’ narratives. While this proximity enabled trust-building, it also required reflexive awareness to avoid over-identifying or imposing meaning (Corlett & Mavin, 2018; Couture et al., 2012; Holmes, 2020). This research was conducted by a researcher whose participants shared insider status as racialized women and long-standing community-based practice in IPV and anti-oppressive service delivery in Ontario. These social locations collectively informed a research positionality that emphasized cultural empathy, relational trust, and epistemic justice. Interview participants habitually offered very personal narratives of abuse, trauma, and mental health suffering with emotional openness that was most likely made possible through shared linguistic, cultural, or gendered location.
However, insider status is neither simple nor risk-free. While shared identity may enhance rapport, it may also conceal difference. The researcher was cautious not to assume homogeneity of immigrant women’s experiences or over-identify with narratives of resilience and suffering. Reflexive journaling, peer debriefing, and methodological transparency were integrated into the research process to compensate for positional power, bias possibility, and emotional entanglement (Couture et al., 2012).
Furthermore, our intersectional positionality required a reflexive awareness of knowledge production itself, how academic inquiry can reproduce extractive logics, even in good-faith community partnerships. As such, survivors’ voices were not distilled into data points but were approached as narrative testimony and situated knowledge with the power to critique and reimagine institutional systems. Participants were consulted on the language and interpretation of the study, and preliminary findings were shared with community stakeholders for confirmation and response (Holmes, 2020).
Findings
This section presents key findings from interviews with racialized women survivors of IPV in Ontario. Guided by an intersectional and trauma-informed framework, the analysis examines women’s mental health needs, barriers to care, and institutional responses to IPV-related trauma. Participants described profound psychological distress, unmet needs, and significant gaps in support systems. The sample included 37 INC (less than 10 years in Canada), 53 long-term immigrant women (10+ years in Canada), and 17 Canadian-born racialized women. Most participants were mothers, the majority had some post-secondary education, and many lived below the poverty line. Indicators such as language proficiency, income, and home ownership varied significantly by immigration history, highlighting the structural disadvantages that shaped women’s experiences with IPV and access to mental health services (Table 1).
Sample Profile Table for Immigrant and Nonimmigrant Racialized IPV Survivors.
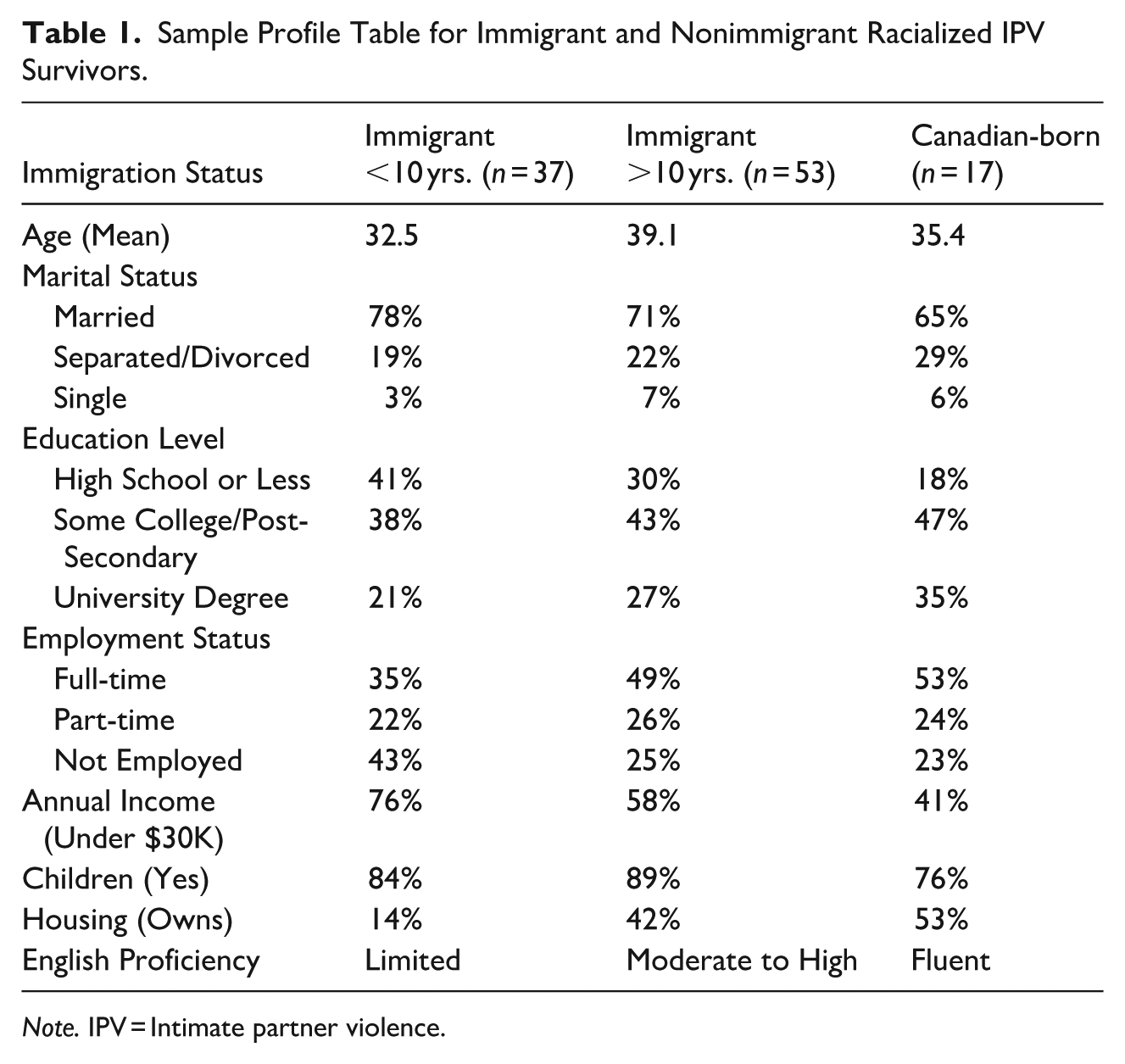
Note. IPV = Intimate partner violence.
Prevalence and Patterns of Psychological Abuse
Across all groups, participants reported experiencing multiple forms of IPV, including psychological, physical, and sexual violence, with psychological abuse emerging as the most pervasive and damaging. Co-occurrence of all three forms was reported by 70% of newcomers, 81% of long-term immigrants, and 94% of Canadian-born racialized women. These figures describe this sample alone and were not intended as population estimates.
Importantly, women interpreted psychological abuse through different cultural and social lenses. Newcomer women often described emotional abuse through culturally embedded notions of honor, shame, and spiritual distress. Canadian-born racialized women, by contrast, framed their experiences in terms of racial gaslighting and societal invalidation. Long-term immigrants frequently discussed emotional suppression and institutional neglect. These differences illustrate how immigration history shapes both the meaning and impact of psychological harm.
Recent immigrants described the most compounded trauma due to precarious immigration status, language barriers, and unfamiliarity with Canadian services. Their distress was often expressed through culturally specific idioms that were misunderstood within Western clinical contexts. Long-term immigrants spoke of enduring emotional erosion after years of navigating oppressive relational dynamics. Canadian-born racialized women frequently reported psychological manipulation that mirrored societal stereotypes portraying racialized women as irrational or “crazy.” These quantitative patterns function solely as contextual markers to situate the qualitative findings and do not support econometric inference (Table 2).
Measures of Psychological Abuse Reported “Very Often.”
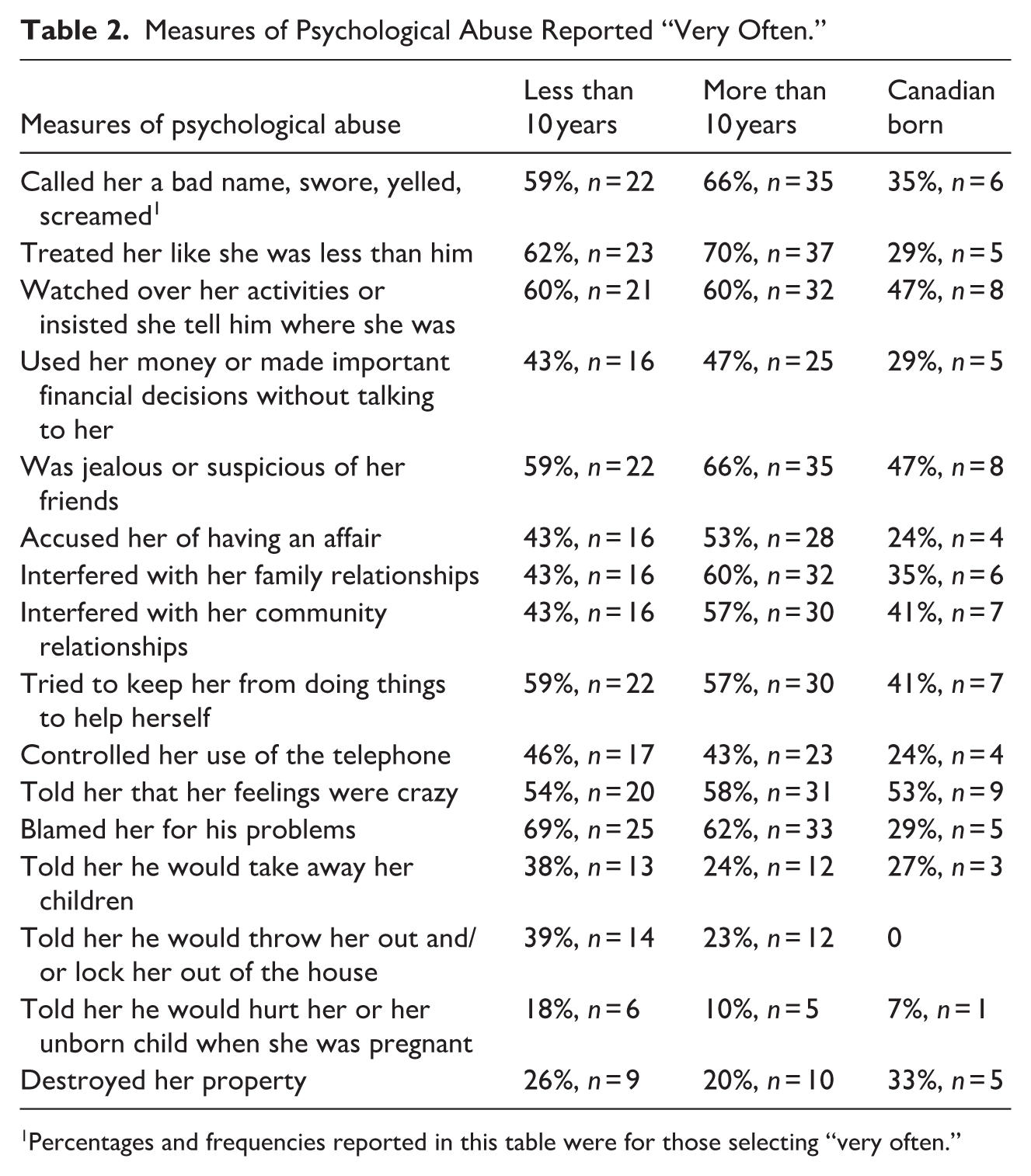
Percentages and frequencies reported in this table were for those selecting “very often.”
The analysis revealed three interconnected themes that together illustrate how racialized survivors understood, experienced, and sought support for the mental health impacts of IPV. These themes trace a progression, from the initial crisis that prompted help-seeking, to the long-term emotional and physical consequences of abuse, to the systemic failures that left these needs unmet within Ontario’s IPV service landscape. These themes were evident in 57 of the 107 interviews (53%), indicating that more than half of the participants explicitly linked their IPV experiences to unmet mental health needs and barriers to care.
Theme #1: Mental Health as the Primary Reason for Seeking Help
This important theme highlights that for many racialized women, psychological distress, not physical violence, was the primary catalyst for seeking assistance. Emotional collapse, suicidal thoughts, and overwhelming stress were consistently identified as the breaking points that pushed survivors into IPV services. Many women sought IPV services not due to immediate physical danger but because their mental health collapsed under the strain of emotional abuse, isolation, and chronic stress.
As one Canadian-born racialized participant reflected:
Everything that went wrong; money, kids, the house; was somehow my fault. It made me believe I was failing as a wife and mother.
Her narrative demonstrates how emotional abuse targets core identities and contributes to psychological decline, making mental health deterioration the tipping point for seeking help.
A long-term immigrant woman distinguished between physical harm:
The bruises go away, but the inside is there.
Her words underscore how emotional pain lasts far longer than physical injuries, a pattern that appeared across groups.
A newcomer woman described reaching a life-threatening state:
I was not mentally there and was suicidal.
Her statement reflects the intersection of migration stress and IPV, both of which contributed to severe psychological overload.
Many survivors described trauma as deeply embodied:
PTSD . . . couldn’t eat, stressed.
Such somatic symptoms, insomnia, appetite loss, chronic tension, were common markers of emotional collapse.
Another participant explained what ultimately prompted her to leave:
I went to the shelter not because he hit me, I could survive that, but because I thought I was going to lose my mind.
This finding overturns the common belief that physical violence is what drives women to seek help. For many survivors in this study, it was the emotional collapse, not the bruises, that felt most urgent and terrifying. Taken together, the narratives show that declining mental health, including suicidal thoughts, overwhelming emotional strain, and physical symptoms of distress, was the main reason women across all groups sought support. These patterns illustrate how their mental health needs were shaped by the combined effects of gendered abuse, racialization, migration pressures, and broader structural barriers. Across groups, mental health distress functioned as both a consequence of abuse and an early warning system indicating the limits of survivability. Women described psychological collapse not merely as an outcome of IPV but as a turning point that prompted help-seeking. This positions mental health as a central mechanism through which racialized survivors interpret risk, safety, and recovery, a notable finding. While deteriorating mental health brought many survivors into the IPV system, the emotional consequences of abuse did not end there. The second theme explores how psychological and psychosomatic distress persisted long after women left their abusive partners.
Theme #2: Long-Term Emotional and Psychosomatic Consequences of IPV
This theme captures the enduring emotional and physical impacts of IPV, including PTSD symptoms, depression, anxiety, and chronic stress. These long-term consequences were intensified by immigration pressures, financial insecurity, and ongoing racialized and gendered marginalization. Across all three groups, newcomer immigrants (INC), long-term immigrants (IL10), and Canadian-born racialized women (CBW), participants described enduring emotional and physical consequences that persisted long after separation from their abusive partners. These consequences were not isolated events but part of a cumulative pattern of trauma shaped by IPV, migration stress, financial strain, and social exclusion. Many women described developing new or worsening mental health conditions directly linked to abuse. One newcomer participant explained:
I developed this eating disorder.
This narrative highlights a common pattern: emotional trauma manifesting through the body. Eating difficulties, chronic stress, and stomach pain were frequently cited as somatic markers of psychological overwhelm. For others, the trauma was triggered by memories of specific abusive incidents:
My partner locked me in the room from the outside; I get and continue to get claustrophobic attacks.
Her ongoing claustrophobia shows how the body “remembers” trauma even after physical danger has passed.
Many newcomers described trauma as layered with migration hardships:
I felt like I was drowning, not just from the abuse, but from everything like immigration; no money; no family. Just me and my pain.
This quote reflects the compounding effect of IPV and settlement stress, aligning with Table 3‘s identification of “migration pressure and isolation” as key contextual contributors for INC participants. Long-term immigrants described chronic hypervigilance, demonstrating how prolonged emotional abuse becomes internalized:
I was living on eggshells and continuously monitoring my heart rate.
Distinctions in IPV and Mental Health Experiences Across Racialized Women by Immigration Status: A Theoretical Analysis.
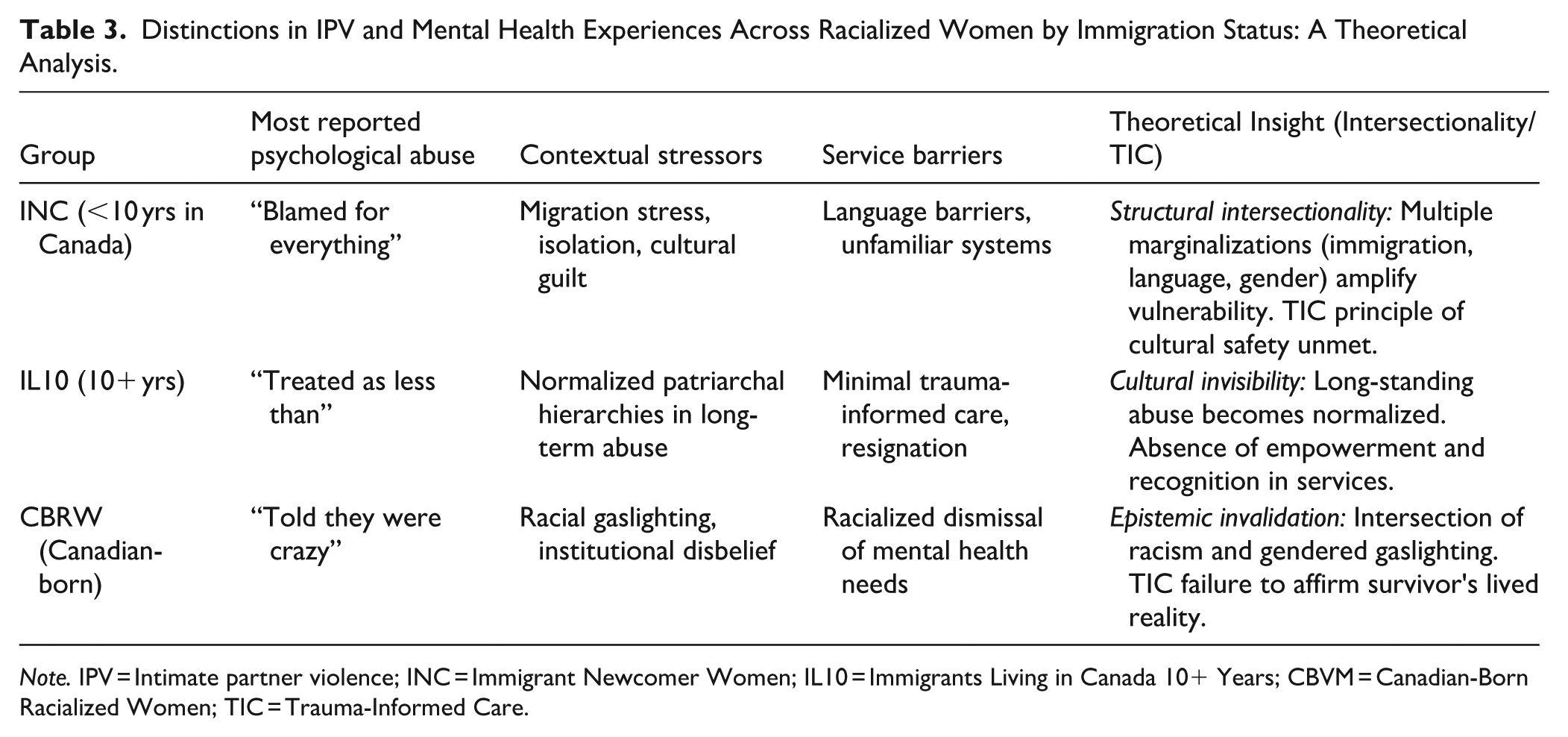
Note. IPV = Intimate partner violence; INC = Immigrant Newcomer Women; IL10 = Immigrants Living in Canada 10+ Years; CBVM = Canadian-Born Racialized Women; TIC = Trauma-Informed Care.
This bodily vigilance illustrates the long-lasting physiological imprint of psychological abuse.
Women across groups also reported severe psychological distress:
I feel suicidal and depressed and mentally ill.
These long-term consequences were often described as intrusive, persistent, and difficult to treat. Anxiety, insomnia, nightmares, panic attacks, loss of appetite, and feelings of suffocation appeared repeatedly across interviews. Overall, these accounts reveal that IPV produces chronic, layered, and embodied forms of trauma. Survivors lived with symptoms long after leaving the relationship, and these symptoms intersected with structural inequities such as poverty, immigration precarity, and racialization. The persistence and severity of these impacts highlight the need for long-term, trauma-informed, and culturally grounded mental health responses. The persistence of these symptoms raises a critical question: Why were survivors’ mental health needs not adequately met when they sought help? The third theme addresses this gap by examining the systemic limits of mental health support within IPV agencies.
Theme #3: Lack of Professional and Culturally Responsive Mental Health Care
This theme highlights survivors’ widespread reports of inadequate, nonclinical, and culturally unresponsive mental health support. Women described receiving physical safety but not the trauma-informed, culturally grounded emotional care they urgently needed. Across all three groups, women emphasized that while IPV agencies provided basic safety, such as shelter beds, food, and emergency support, they did not provide the trauma-informed and culturally grounded mental health care that survivors urgently needed. The absence of licensed mental health professionals, combined with limited cultural competence, left many participants feeling unseen, unheard, and emotionally abandoned.
A long-term immigrant woman described this gap clearly:
There was no psychologist to help with emotional mental aspects of my life, [the director] is the director but not a mental health specialist.
Her statement reflects a widespread sentiment: Agencies were staffed by well-intentioned workers but lacked the clinical expertise necessary to support women experiencing acute trauma, PTSD, or cultural distress. Others echoed similar concerns about staff training:
More knowledgeable counsellor, staff not trained.
Mental health services were inadequate.
These comments point to systemic issues, structural underfunding, lack of specialization, and insufficient mental health personnel, that limited agencies’ ability to respond to women’s psychological needs.
Several women reported never seeing a mental health professional at all:
I did not see any mental health professionals and I think organizations like this should have them.
We need professional women that deal with mental health and well-being.
These reflections highlight the unmet expectation that IPV supports should include trauma-informed clinicians, particularly given the emotional severity of survivors’ experiences. Participants also described feeling culturally misunderstood. For newcomer women especially, the interaction between migration stress and emotional trauma required culturally sensitive approaches that agencies did not provide:
These agencies did not understand my cultural needs.
Language barriers, differing expressions of distress, and culturally rooted notions of shame, honor, and spiritual suffering were often overlooked or misinterpreted.
Canadian-born racialized women described a different but related problem: Staff lacked training in the specific traumas tied to racism, racial identity, and stereotypes. One participant explained:
The staff were kind, but they weren’t trained to deal with my culture’s trauma.
Her experience suggests that even when staff were compassionate, their lack of cultural literacy resulted in emotional invalidation.
Other participants described feeling emotionally neglected in shelters:
They gave me food and a bed, but no one asked why I was crying every night.
This quote captures a recurring theme: Agencies met women’s immediate physical needs but overlooked the psychological dimensions of abuse, leaving survivors to navigate their emotional suffering alone.
Several women stopped trying to communicate their trauma after repeated misunderstandings:
I stopped trying to explain how I felt. They didn’t understand when I said it felt like my soul was drowning.
This statement, “my soul was drowning,” reflects how profound the emotional suffering was and how deeply women felt the disconnect between their lived experience and the services available to them. Together, these narratives reveal a systemic mismatch between what survivors needed and what agencies were equipped to provide. While shelters offered safety, they lacked trained mental health professionals, culturally responsive care, and the trauma-informed expertise necessary to support complex psychological recovery. This gap left many women feeling unheard, unsupported, and forced to cope with the emotional aftermath of IPV on their own. Theme #3 directly illustrates how the core TIC principles, safety, trust, collaboration, empowerment, and cultural responsiveness, were inconsistently implemented. Women repeatedly reported that while physical safety was provided, emotional and cultural safeties were largely unmet.
Distinguishing newcomer, long-term immigrant, and Canadian-born racialized women is analytically important because each group occupies a different structural position within Canada’s immigration regime, labor market, and racial hierarchy. These positions shape how psychological abuse is experienced, interpreted, and responded to. Across the sample, immigration history, racialization, and social location interacted in patterned ways, producing distinct forms of emotional and psychological harm among INC (less than 10 years in Canada), Long-Term Immigrant Women (10 or more years in Canada), and Canadian-Born Racialized Women.
Newcomer women most often described being blamed for “everything,” a pattern tied to intensified patriarchal expectations, migration-related stress, and economic precarity. Long-term immigrants frequently articulated experiences of being “treated as less than,” reflecting chronic emotional degradation normalized over years of relationship entrenchment and systemic misrecognition. Canadian-born racialized women more commonly reported being told they were “crazy,” a form of racialized gaslighting that echoes broader societal narratives that pathologize women of color and undermine their credibility.
These patterns were embedded within distinct structural and contextual pressures. For newcomers, psychological abuse intersected with migration stress, linguistic barriers, and social isolation. Long-term immigrants described emotional suppression shaped by long-standing patriarchal norms and institutional neglect. Canadian-born racialized women emphasized racial gaslighting, disbelief, and the cumulative effects of navigating racialized gender stereotypes. Service barriers also differed across groups: Newcomers faced language and access constraints; long-term immigrants commonly reported resignation to inconsistent or low-quality care; and Canadian-born women described racialized invalidation within service encounters. These variations illustrate how intersectional positioning structures both the production and consequences of trauma, and how TIC principles remain unevenly implemented across the sector.
Overall, the findings demonstrate that mental health needs were central to the IPV trajectories of racialized women. For many, emotional deterioration, rather than physical injury, was the primary catalyst for seeking help. Anxiety, depression, post-traumatic stress, dissociation, and suicidal ideation often persisted long after the abusive relationship ended, reflecting the sustained psychological toll of IPV. Yet, participants consistently reported inadequate access to licensed, trauma-informed, and culturally responsive mental health supports. The nature and severity of psychological abuse, the meaning attributed to distress, and the pathways to help-seeking all varied by immigration history, cultural context, and structural inequities.
In summary, the three themes collectively reveal a continuum of unmet mental health needs shaped by gendered violence, racialization, migration histories, and structural exclusion. They highlight significant gaps in Ontario’s IPV response system and underscore the critical need for trauma-informed and culturally safe mental health care.
Finally, although this qualitative study did not control for age differences between groups, it is important to acknowledge that variations in IPV severity and psychological harm may be partially influenced by age and life-course stage. Future research should examine age as a potentially meaningful factor shaping IPV experiences and mental health needs among diverse groups of racialized women.
Discussion & Conclusion
This study contributes to the literature on IPV by offering a critical, intersectional, and trauma-informed analysis of the mental health needs and service experiences of immigrant, long-term immigrant, and Canadian-born racialized women in Ontario. Drawing on qualitative data from IPV survivors, the study reveals the central role of mental health concerns as a primary motivator for help-seeking. The findings disclose that many immigrant and racialized women viewed mental health care, rather than physical safety, as their primary motivation for seeking help, yet described encountering a system unprepared to recognize or respond to their emotional needs. These findings challenge dominant assumptions that treat psychological harm as secondary to physical violence and emphasize the need for integrated services that address emotional well-being. This study does not assume that all racialized or immigrant survivors have identical needs, nor does it claim population-level causal links. Rather, the findings demonstrate that structural contexts, such as migration status, racialization, language isolation, and economic precarity, shape survivor experiences in patterned ways. These contextual differences alter both the type of mental health challenges faced and the cumulative burden of trauma, reinforcing the need for tailored, culturally grounded interventions.
Findings affirm and extend prior research showing that racialized and immigrant women face structural barriers to culturally appropriate care (Guruge, Thomson et al., 2015; Nyikavaranda, et al., 2023; Olukotun, et al., 2025; Warshaw et al., 2013). Emotional and psychological abuse might be less visible than physical violence, but it has clear and lasting effects on mental health and overall well-being. These include increased risks of depression, anxiety, trauma-related distress, and long-term social and psychological damage (Dokkedahl et al., 2019; Lortkipanidze et al., 2025; Muchemwa et al., 2025; Smith et al., 2025; Yick, 2008).This study adds to the field by coupling intersectionality theory (Crenshaw, 1991) with the TIC framework (SAMHSA, 2014), offering a dual lens that critically examines how trauma is produced through structural inequality and how institutions fail to address it. By positioning psychological trauma as a primary driver of service use, this research highlights how identities, such as race, immigration status, and cultural background, shape both IPV experiences and service encounters. This approach offers a more integrated understanding of trauma in the Canadian context and calls for culturally grounded, survivor-led reforms.
Commonalities and distinctions were observed across participant groups. Mental health was a shared priority, but the nature of emotional abuse varied: Recent immigrants described isolation and blame compounded by language and legal fears; long-term immigrants highlighted normalized emotional degradation within patriarchal norms; and Canadian-born racialized women most often reported gaslighting tied to societal stereotypes. Despite these variations, all groups encountered a fragmented, culturally misaligned system that failed to meet their mental health needs. These findings align with past research documenting group-specific barriers experienced by immigrant and racialized women (Ahmad et al., 2009; Ahmed et al., 2024; Warshaw et al., 2013) and are further supported by recent studies showing that immigrant and minority survivors continue to face structural, cultural, and institutional barriers to accessing support, offering a novel comparative lens by examining these dynamics together (Flores et al., 2025; Sanhueza-Morales et al., 2025; Tastsoglou, 2025).
TIC allowed for a critical assessment of whether IPV services met survivors’ emotional needs. While legal and housing supports were noted, participants consistently reported a lack of trauma-specific care, licensed mental health professionals, and culturally responsive counseling. Fears of retraumatization, especially in the context of surveillance technologies, further complicated help-seeking. This systemic neglect of psychological healing amounts to structural retraumatization, driven by funding models that prioritize crisis management over emotional recovery. Culturally responsive feminist frameworks deepened the understanding of trauma expression. Participants described distress using idiomatic or culturally embedded language, such as spiritual suffering or mental blocks, which are often illegible within Western paradigms. This contributes to diagnostic oversight and marginalization, reinforcing Eurocentric models of care that exclude racialized expressions of pain.
This study offers four contributions to Canadian IPV scholarship:
It identifies mental health as a central motivator, not a byproduct, of IPV service use.
It critiques the failure of agencies to provide trauma-informed, culturally competent mental health support.
It illustrates how racialized women express trauma through culturally rooted idioms, contributing to decolonial health research.
It advocates for intersectional, culturally responsive reforms in Ontario’s IPV service systems.
Ultimately, this research reveals a critical mental health gap in IPV service provision. Structural neglect, cultural erasure, and institutional racism compound survivors’ trauma, particularly for racialized women. Legal and safety resources, though necessary, are insufficient without robust, culturally grounded mental health supports. This includes multilingual services, peer-led interventions, and survivor-informed programming. These reforms and improvements are widely supported in the literature (Cavalcanti Pereira Lima, 2024; Chan, 2020; Critelli & Yalim, 2021; George et al., 2022; Kanter & Hassija, 2026; McEvoy et al., 2024; Mengo et al., 2024; Sanhueza-Morales et al., 2025).
This research does not come without limitations; thus, it is important to recognize and acknowledge them. This study is based on a small, non-random sample of racialized immigrant women in Ontario and does not claim generalizability across all newcomer communities or regions. The data reflect self-reported experiences, which may be shaped by social or cultural silences around IPV. Furthermore, while the qualitative approach provides depth and nuance, it limits statistical comparisons and broader demographic analysis.
Future studies should incorporate longitudinal or mixed-method designs to examine mental health outcomes across diverse immigrant contexts. Additionally, research should explore the impact of surveillance technologies, such as police body-worn cameras, on survivors’ willingness to seek help. As Couture-Carron and Saulnier (2026) note, many participants expressed fear that recorded footage could be weaponized against them, deterring future disclosures. Similar patterns have been observed in research on technology-facilitated abuse, where survivors report fear of digital monitoring, evidentiary misuse, and loss of control, all of which can influence decisions about reporting and help-seeking (Brookfield, 2024; Dragiewicz et al., 2018; Woodlock, 2017). Emerging scholarship further suggests that surveillance can generate psychological distress, mistrust, and behavioural withdrawal among vulnerable populations, underscoring the need for deeper examination of the psychological and legal implications of institutional surveillance within IPV response systems. This highlights the need for further inquiry into the psychological toll and legal implications of institutional surveillance in IPV response systems. Another future direction includes studying the perspectives of service providers to understand how structural constraints, training gaps, and institutional biases shape the delivery of trauma-informed, culturally responsive care. This could help identify points of disconnect between survivor needs and agency practices. Finally, future research should evaluate the long-term impacts of recent policy reforms on the accessibility and quality of mental health services within IPV agencies, particularly those aimed at racialized and immigrant populations. Such studies could help assess whether intersectional and trauma-informed principles are being meaningfully implemented or remain tokenistic. Also, because the sample was recruited through community IPV and settlement agencies, the findings reflect the experiences, narratives, and story-telling of survivors engaged with support systems and are not intended to represent all racialized women in Ontario. Instead, the study provides theoretically transferable insights about the current barriers and gaps commonly encountered by racialized survivors in these unfavorable IPV situations.
By articulating how survivors link their emotional and/or psychological suffering to structural barriers within Canada’s IPV support systems, this study contributes conceptual clarity to understanding the relationship between racialization, migration, and mental health in ways that complement and extend quantitative and policy-oriented research. This research was indeed a labor of love and contributes to the important field of IPV by demonstrating that mental health distress is not only a consequence of IPV but a major driver of help-seeking among racialized survivors. It further shows how immigration history and racialization shape the meaning of psychological abuse and the accessibility of appropriate mental health support.
Footnotes
Acknowledgements
The author gratefully acknowledges the contributions of co-investigators involved in the broader SSHRC-funded project from which the dataset for this study was derived. Thank you to the graduate students who assisted me with this.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Social Sciences and Humanities Research Council of Canada (SSHRC) through a Partnership Development Grant awarded to the author.
Declaration of Conflicting Interests
The author declared no potential conflicts of interests with respect to the authorship and/or publication of this article.