
Abstract
To examine sex-stratified differences in peer violence trends between early to late adolescence and examine the role of gender norm perceptions on these trends. A 5-year, five-wave linked panel cohort of a purposive sample of adolescents (n = 1,551) from Kinshasa, Democratic Republic of Congo (DRC) was used. During Wave 1 in 2017, out-of-school and in-school adolescents aged 10 to 14 years were selected from two urban communes. Peer violence was operationalized as no violence, victimization only, perpetration only, and victimization and perpetration overlap. A weighted multinomial logistic regression was conducted to determine the role of gender norm perceptions on peer violence experiences. Between 2017 and 2022, there was a reduction in peer violence experiences for both males and females driven by lower victimization (males: 0.8, 95% CI [0.8, 0.9]); females: 0.8 [0.7, 0.8]) and victimization and perpetration overlap (males: 0.9 [0.8, 0.96]; females: 0.7 [0.7, 0.8]) relative to one wave prior. A one-unit increase in sexual double standard (SDS) mean score increased risk of victimization and perpetration overlap for females (RRR: 1.3 [1.1, 1.6]). Peer violence has predominantly been assessed among males without understanding patterns among females. By creating a unique variable that captures victimization and/or perpetration, we unpack both commonalities and differences by sex in peer violence. More unequal perceptions of SDS increased relative risk of peer violence victim and perpetration overlap among females. Additionally, ACEs and alcohol emerged as risk factors for peer violence experiences. Family-based programs combined with gender transformative interventions and policies to address alcohol misuse among adolescents could mitigate peer violence experiences.
Keywords
Introduction
Although peer violence and bullying encompass a broad spectrum of aggressive behavior (e.g., reactive, instrumental, relational, verbal, physical, sexual or cyber), they differ in scope (Finkelhor et al., 2012; Kretschmer, 2016). Peer violence is a broader construct that may be singular or repeated, with or without power hierarchies (Finkelhor et al., 2012). Bullying, by contrast, is a repeated and intentional behavior, with a clear power differential, and intent to cause harm (Kretschmer, 2016). Peer violence can manifest in various forms, including physical, verbal, social, or sexual violence (Karmaliani et al., 2017), and can be either direct or indirect in nature. Although peer violence can occur at any age, it is most prevalent during adolescence, with a noticeable increase in early adolescence followed by a decrease or stabilization in later years (Moffitt, 1993, 2017; Troop-Gordon, 2017). A recent study involving school-aged children (ages 12–15 years) across 29 countries and multiple rounds revealed an overall prevalence of 39.4% in the past 6 months for peer violence victimization (Smith et al., 2023). However, the rates varied significantly by region: peer violence increased in 6 countries, decreased in 13, and remained stable in 10 (Smith et al., 2023). The impact of peer violence is far-reaching, with consequences for mental health, substance use, future violent behavior, and delinquency (Moore et al., 2017; Sabri et al., 2013; Turanovic & Siennick, 2022).
Both biological and social factors affect vulnerability to peer violence (Maksimovic & Dimitrijevic, 2020; Troop-Gordon, 2017). One particularly relevant variable is sex and gender. Sex is a biological characteristic based on genitalia, hormones and chromosomes that categorizes a person as male, female, or intersex (Gender Equity Unit, 2024); gender is the social construction of sex based on expectations and characteristics prescribed by society on appropriate behavior, roles and norms (Gender Equity Unit, 2024). Gender is not limited to the three categories outlined within sex (Gender Equity Unit, 2024). A study conducted among 11 to 15-year-old students across 46 countries (not including DRC) found that males had significantly higher odds of perpetrating and being victims of traditional bullying and engaging in cyberbullying in comparison to females (Cosma et al., 2022). After controlling for the gender inequality index, countries that were more gender unequal showed greater traditional perpetration and victimization of males in comparison to females. In more gender-equal countries, females had a higher risk of experiencing cyberbullying (Cosma et al., 2022).
Gender roles and norms are also an expression of power systems that intersect to drive peer violence during adolescence (Beckwith et al., 2022; Ramaiya, Choiriyyah, et al., 2021; Ramaiya, Zimmerman, et al., 2021). In the Democratic Republic of Congo (DRC) and other countries, cross-sectional studies from the Global Early Adolescent Study (GEAS) have shown that gender norms prescribing masculine and feminine roles significantly shape adolescents’ experiences of peer violence, often creating gender disparities (Ramaiya, Choiriyyah, et al., 2021; Ramaiya, Zimmerman, et al., 2021). Masculine norms encourage behaviors such as aggression, dominance, and emotional detachment, which are linked to the increased perpetration of violence (Fine et al., 2021, 2023; Mmari et al., 2018). For example, males are often socialized to value physical aggression and control, behaviors that are strongly associated with higher rates of bullying (Nansel et al., 2001). In contrast, feminine norms tend to emphasize passivity, dependency, and emotional sensitivity, which can restrict girls’ mobility and independence, increasing their vulnerability to victimization (Thornberg & Jungert, 2014).
Moreover, the acceptance of gender inequitable attitudes, where males are expected to dominate and females to be submissive, can normalize violence, limiting the willingness to seek help or access services (Juvonen & Graham, 2014; Murphy et al., 2021). For instance, males may avoid seeking help due to the stigma surrounding vulnerability and help-seeking behaviors, reinforcing a cycle of violence. Similarly, females who challenge traditional gender roles may experience further bullying or social exclusion, which complicates their ability to seek support or escape abusive situations (Juvonen & Graham, 2014).
Violence within the DRC is pervasive, driven by the political conflicts since 1996 and poverty, with 74% of the population living on less than $2.10 per day (UNdata, 2019; World Bank Group, 2024). Interpersonal violence, defined as the “intentional use of physical force or power against other persons by an individual or small group of individuals” (Mercy et al., 2017), is the third leading cause of mortality and morbidity among males 10 to 19-years-old in the region (Ross et al., 2021). Notably, exposure to violence varies by gender with males disproportionately affected by physical violence (49.7% vs. 36.5%) and witnessing community violence (55.0% vs. 9.0%), while females experience higher rates of sexual violence (16.0% vs. 8.0%; Amene et al., 2024). Baseline analysis of the GEAS in Kinshasa, DRC, showed that 40% of males and 33% of females experienced peer violence victimization and/or perpetration in the past 6 months (Ramaiya, Zimmerman, et al., 2021). Males, in particular, had a higher likelihood of experiencing the overlap of victimization and perpetration and witnessing peer bullying (Fine et al., 2022; Ramaiya, Zimmerman, et al., 2021). Recent surveys show that almost 50% of women experience physical, emotional, and sexual violence, with girls reporting a significantly higher prevalence of experiencing sexual violence (Amene et al., 2024; UNFPA, 2024). A recently published paper examined peer violence trajectories using latent class analysis during early adolescence in China, DRC, and Indonesia from ages 12 to 15 years. The study found five classes in DRC including low peer violence (most frequent), peaks in the middle, declining violence, increasing violence and consistently high violence (Ramaiya et al., 2025). The peaks in the middle, declining violence, and increasing violence showed age-based transitions with the “peaks in the middle” class showing low peer violence when adolescents were 11 to 13 years, followed by higher experiences at 14 to 15 years and thereafter a reduction at 16 to 17 years. The “declining violence” and “increasing violence” classes showed a decrease or increase in peer violence experiences between 11 and 17 years, respectively (Ramaiya et al., 2025). Similarly, a latent transition analysis of Chinese adolescents (N = 1,261) spanning Grades 5 to 8 identified three subgroups: aggressive–victims, victims, and uninvolved (Zheng et al., 2024). Notably, the transition from primary to middle school (Grades 6 to 7) represented a critical window for change, with aggressive–victims and victims more likely to transition to the uninvolved group during this period compared to transitions within the same educational phase. Males were at higher risk of belonging and staying in involved groups, which increased their risk of internalizing and externalizing behaviors during middle school (Zheng et al., 2024).
Despite this evidence, there are still gaps within the literature, with limited studies examining peer violence transitions between no violence and victimization only/perpetration only or overlap of victimization/perpetration during adolescence in a resource-limited settings from early to late adolescence. Current literature focuses more on adverse childhood experiences (ACEs) and how they shape long-term outcomes in adulthood related to general well-being, intimate partner violence, and social mobility (Haczkewicz et al., 2024). Secondly, there are limited studies that understand factors related to peer violence trends in humanitarian settings. Major challenges and hardships such as displacement, overcrowding, and gender-based violence are heightened during humanitarian emergencies, and the impacts of the latter during the entirety of adolescence are an area of high consideration for potential interventions (Rubenstein & Stark, 2017). Thirdly, the lack of sex-stratified differences, as well as understanding the role of gender norms between males and females in peer violence trends, warrants further research. The longitudinal study between gender norms and peer violence trajectories found that unequal sexual double standard (SDS) was associated with higher probability of being the declining violence class relative to no violence class in DRC. However, this study didn’t provide the nuances on changes in peer violence categories over time as well as differentiation by sex (Ramaiya et al., 2025).
To fill these gaps, we will use the GEAS five-wave linked Kinshasa, DRC cohort to answer the following questions:
Understand sex differences in peer violence trends between early to late adolescence.
Examine the role of gender norm perceptions among sexes in shaping peer violence trends.
We hypothesize that males versus females are more likely to experience victimization and perpetration overlap, and more unequal gender norm perceptions exacerbate peer violence experiences for males and females.
Methods
Study Setting and Data Source
Kinshasa is one of the fastest-growing cities in the world, with 22% of its population consisting of adolescents and 21.6% of 6 to 11-year-old children considered out of school (INS, 2018). Kinshasa was the first country to launch the GEAS survey in 2017, which was conducted over five annual data collection rounds (waves) between 2017 and 2022. Adolescents in Kinshasa were also part of a gender transformative intervention known as Growing Up Great (GUG!), which addressed conventional norms by building knowledge regarding sexual reproductive health, gender norms, violence and conflict resolution, communication/decision-making, and alcohol and drugs. The intervention also prioritized positive attitudes and skills, and self-efficacy (Mmari et al., 2023). The intervention was conducted with in- and out-of-school adolescents, including teachers, community organizations, headmasters, and peers (Mmari et al., 2023).
We used the GEAS’ longest-running cohort in Kinshasa, DRC, as our dataset. The GEAS explores the role of gender socialization on health outcomes among adolescents living in under-resourced urban settings across 11 countries using quantitative surveys (Global Early Adolescent Study, 2021). Surveys elicit data on socio-demographic characteristics, family, peer, community, and school factors across all five waves. For this manuscript, we selected variables that were associated with peer violence and gender norms such as sex, age, household wealth index, household composition, school status, puberty attainment, participation in the gender transformative intervention, agency, alcohol use, tobacco use, parental monitoring and closeness, ACEs, peer composition, spending time with peers, neighborhood safety, neighborhood social cohesion, gender norms (SDS, gender stereotypical traits [GST]), and peer violence experiences.
Study Sampling
During Wave 1 (W1), all adolescents were between 10 and 14 years from two urban communes of Kinshasa. The recruitment and sampling were purposive based on age, whether they lived in an under-resourced urban commune/s, and whether they attended school at the time of the W1 interview (Mmari et al., 2021). Across all five waves, most of the survey was administered by an interviewer through computer-assisted personal interviews in Lingala or French. The study sought consent from parents and assent from minors. Anonymity was maintained through deidentified data and consent procedures. The study received ethical approval from the Johns Hopkins Bloomberg School of Public Health and secondary approval from the Kinshasa School of Public Health (ESP/CE/023/2017).
Data & Analytical Sample
During W1 in 2017, 2,842 adolescents aged 10 to 14 years were enrolled including 2016 in-school (IS) adolescents and 826 out-of-school (OOS) adolescents. After five waves of annual follow-up (completed in 2022), 58.4% (n = 1,661) were retained in the sample. Loss to follow-up was significantly higher if W1 adolescents were in the lowest tertile for wealth, living in a single/no parent household, being OOS, and not being part of the GUG! intervention (Supplemental Appendix 1).
A total of 110 participants were excluded from the analytical sample because they had a missing peer violence value. Our final analytical sample, therefore, included 1,551 participants (93.4% of W1–W5 sample) who provided all data between W1 and W5 and did not have any peer violence observations missing at any point in time. Factors associated with loss to follow-up, after excluding the additional 110 participants, were the same as above (Supplemental Appendix 1). We, thereafter, calculated inverse probability weights to address selection bias (Infante-Rivard & Cusson, 2018).
Measures
Sex: Sex was our moderating variable and operationalized based on whether the adolescent identified as a boy or girl during W1.
Gender norm perceptions: Gender norms perceptions were our main independent variables measured using two scales which have previously shown to be associated with peer violence in baseline analysis (Beckwith et al., 2022; Ramaiya, Choiriyyah, et al., 2021; Ramaiya, Zimmerman, et al., 2021): GST and SDS (Moreau et al., 2019, 2021). GST and SDS are validated on seven- and six-item scales, respectively, among adolescents (Moreau et al., 2019, 2021). The responses for these scales vary on a five-point Likert scale from “disagree a lot” to “agree a lot” (Moreau et al., 2019, 2021). GST measures perceptions of gender traits that believe males are tough and females are weak; SDS measures the extent to which unequal perceptions of romantic relationships are held for males and females (Moreau et al., 2019). The scores for GST and SDS were summarized into a continuous score ranging from 1 to 5, with higher scores indicating more unequal gender norms. The GST and SDS mean scores were calculated based on available item responses, which excluded “don’t know/refuse to answer.” The GST and SDS scales have adequate internal reliability through Cronbach’s Alpha across all five waves (.57 to .63 for GST and .74 to .80 for SDS). We used SDS and GST from W1 given non-significant changes in gender norms over time (Supplemental Appendix 2).
Peer violence: Peer violence was our main dependent variable. The variables measured peer violence in the past 6 months across the five waves. Questions explored: (1) verbal bullying perpetration (“Have you bullied or threatened another boy or girl for any reason?”); (2) verbal bullying victimization (“Have you been teased or called names by someone?”); (3) physical bullying perpetration (“Have you slapped, hit or otherwise physically hurt another boy or girl in a way that they did not want?”); and (4) physical bullying victimization (“During the last 6 months, have you ever been slapped, hit or otherwise physically hurt by a boy or girl in a way that you did not want?”). The responses were “no; yes, by a girl; yes, by a boy; yes, by both boys and girls.” Given the unequal distribution in responses, each question was made dichotomous based on whether the adolescent experienced or perpetrated a form of peer violence (Beckwith et al., 2022; Ramaiya, Choiriyyah, et al., 2021; Ramaiya, Zimmerman, et al., 2021). A composite measure was created for each of the five waves, denoting the following categories: (1) No peer violence experience; (2) peer violence victimization only; (3) peer violence perpetration only; and (4) peer violence victimization and perpetration overlap.
Adjustment Variables: Supplemental Appendix 3 presents the list of all variables and their operationalizations based on W1 correlates with peer violence experiences in DRC (Beckwith et al., 2022; Ramaiya, Zimmerman, et al., 2021). These variables include sex, age, household wealth index, household composition, school status, intervention participation, puberty, agency – freedom of movement (ability to move in their community without supervision), agency – voice (ability to express their needs and what they think), agency – decision-making (ability to make daily decisions), alcohol use, tobacco use, parental monitoring and awareness, parental closeness, ACEs, peer sex composition, time spent with friends, neighborhood safety and social cohesion. Most measures were collected at each wave; however ACEs were collected at W1 and W5 only, and household wealth index and household composition were collected from parents during W1 only and from adolescents from W3 onwards. All adjustment variables were observations from W1. All covariates were categorized except the agency scales. Mean scores were calculated for the different agency scales based on available item responses, which excluded “don’t know/refuse to answer.”
Analyses
All analyses were stratified by sex to examine the role of gender in peer violence trends over five waves. Once we had our analytical sample, we conducted univariate analysis of the complete cases by sex to examine sample characteristics and determine differences between males and females. Thereafter, we conducted simple imputation for variables that had <5% missing with the most frequent response or mean. For variables that had 5% or more missing, we created a valid “missing category” for the individual. We then reshaped the wide dataset into a long format and used the “xtmlogit” command to determine the factors associated with changes in peer violence experiences over time for both sexes in unadjusted (Supplemental Appendix 4) and adjusted regressions (Supplemental Appendix 5) without inclusion of weights.
Next, due to loss to follow-up between W1 and W5, we calculated inverse probability weights using wealth tertile, household composition, school status, and intervention exposure (factors associated with loss to follow-up) to reduce selection bias due to attrition. Similar to the complete case analysis (without weights), we converted the wide dataset into a long dataset and used the “xtmlogit” to conduct bivariate and multinomial regression analyses with weights [pweight=ipw].
We reported relative risk ratios (RRR) as well as 95% confidence intervals (95% CIs) based on the weighted multinomial regression results. A sensitivity analysis compared the complete case sample without weights to the weighted results. All associations should be interpreted as the relative risk of being a part of the peer violence category versus no peer violence category.
Results
Table 1 shows the sample characteristics during W1 of the W1 to W5 linked sample (n = 1,551). Overall, there was an equal distribution by sex, with males comprising 50.7% and females comprising of 49.3% of the sample. Specifically, more than 60% of the adolescents were between 10 and 12 years during W1, 34.8% were in the highest tertile for wealth, 72.5% lived in a two-parent household, 75.0% were in school, 61.1% had achieved puberty, and 56.5% were part of the GUG! intervention. For agency, the mean for freedom of movement was lowest at 1.4 (SD: 0.6), followed by voice at 2.3 (SD: 0.7), and decision-making at 2.7 (SD: 0.9). The Lifetime history of alcohol and tobacco use was 8.0% and 5.1%, respectively. In the individual and household factors, there were significant differences between both sexes, with males more likely to be in the lowest tertile for wealth (males: 34.7% vs. females: 25.9%, p = .001); report greater freedom of movement (males: 1.5 [SD: 0.7] vs. females: 1.3 [SD: 0.6], p < .001), greater voice (males: 2.4 [SD: 0.7] vs. females: 2.3 [SD: 0.7], p = .002), and ever use alcohol (males: 10.8% vs. females: 5.1%, p < .001). Females were more likely to be in school (females: 77.4% vs. males: 72.7%, p = .03) and enter puberty during the W1 survey (females: 73.5% vs. males: 49.1%, p < .001).
W1 Sample Characteristics of W1 to W5 Linked Sample Without Peer Violence Missing (n = 1,551).
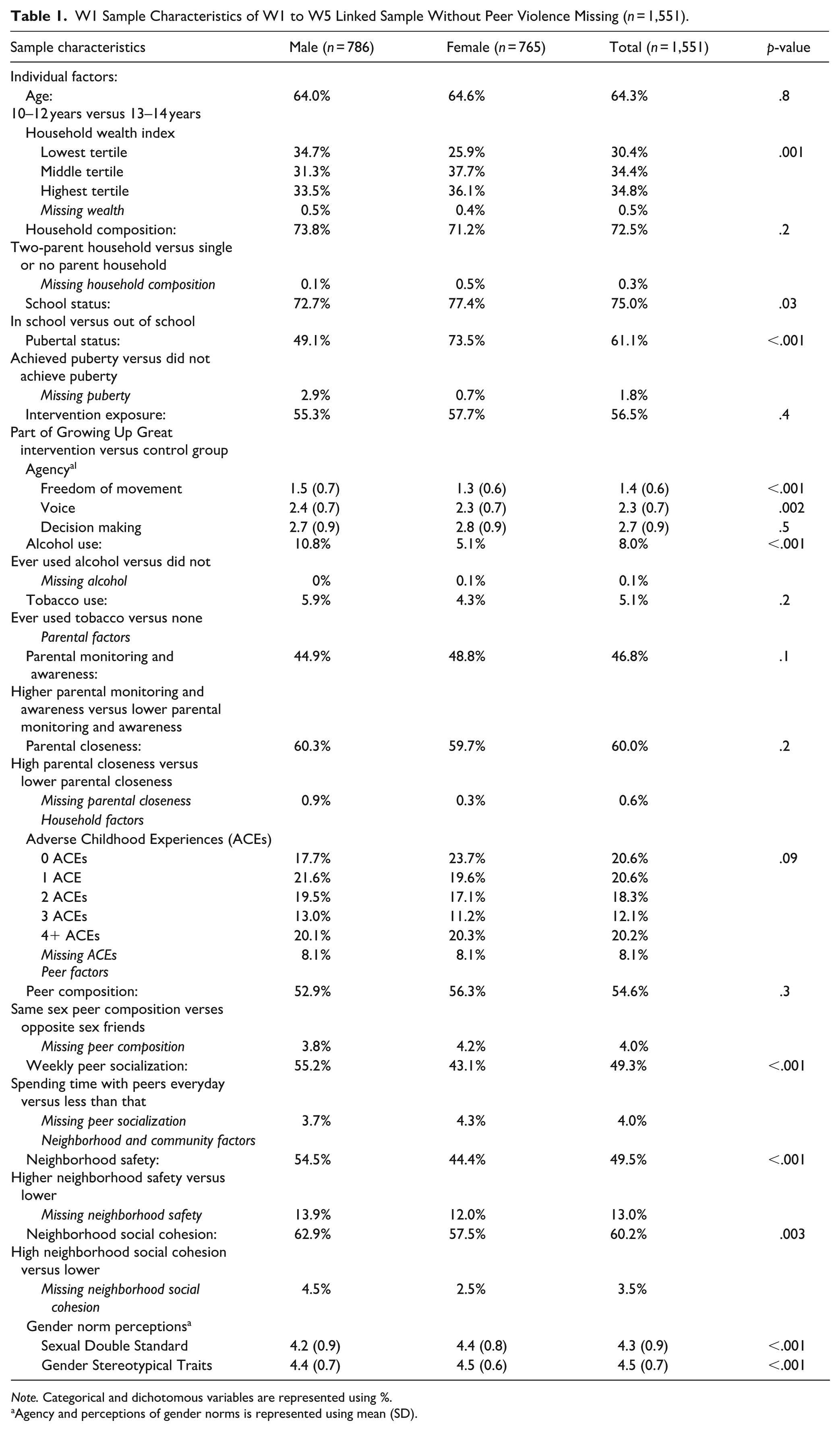
Note. Categorical and dichotomous variables are represented using %.
Agency and perceptions of gender norms is represented using mean (SD).
Among parental factors, 46.8% of adolescents reported high parental monitoring and awareness, and 60.0% reported high parental closeness. Household factors included ACEs with 20.2% of the adolescents reporting 4 or more ACEs. In terms of peer factors, 54.6% of adolescents reported having same-sex peers, and 49.3% reported socializing with peers daily. Males were more likely to report socializing with peers daily in comparison to females (55.2% vs. 43.1%, respectively, p < .001).
Neighborhood and community factors included neighborhood safety, neighborhood social cohesion, and gender norm perceptions. All these factors were significantly different by sex. Higher neighborhood safety and social cohesion were reported by 49.5% and 60.2% of adolescents, respectively. These proportions were significantly higher for males in comparison to females (Neighborhood safety: 54.5% vs. 44.4%, p < .001; neighborhood social cohesion: 62.9% vs. 57.5%, p = .003). The mean scores for gender norm perceptions, measured by SDS and GST, were 4.3 (SD: 0.9) and 4.5 (SD: 0.7), respectively, with females consistently exhibiting more unequal gender norm perceptions compared to males (SDS mean score for females versus males: 4.4 [SD: 0.7] vs. 4.2 [SD: 0.9], GST mean score for females versus males: 4.5 [SD: 0.6] vs. 4.4 [SD: 0.8]).
Figure 1 shows the sex-stratified peer violence experiences over the five waves. Over time, there is a significant reduction in peer violence victimization only (p < .001) and peer violence victimization and perpetration overlap (p < .001) among both sexes, which drove the significant increase in no peer violence experiences (Males: 41.4% to 54.1%; Females: 53.7% to 70.6%). Supplemental Appendix 6 shows the proportions across time for each peer violence category by sex.

Sex-stratified peer violence experiences over five waves (n = 1,151).
Table 2 shows the bivariate regression among both sexes. We see that RRR for peer violence victimization only and peer violence victimization and perpetration overlap versus no peer violence across all three models, was statistically significant for both sexes in the current survey wave relative to one wave prior. Additionally, a one-point increase in the SDS mean score among females was associated with a 40% increase (RRR: 1.4, 95% CI [1.2, 1.7]; p ≤ .001) in the risk of peer violence victimization and perpetration overlap.
Bivariate Relationship Between Time, Gender Norms, and Peer Violence by Sex.
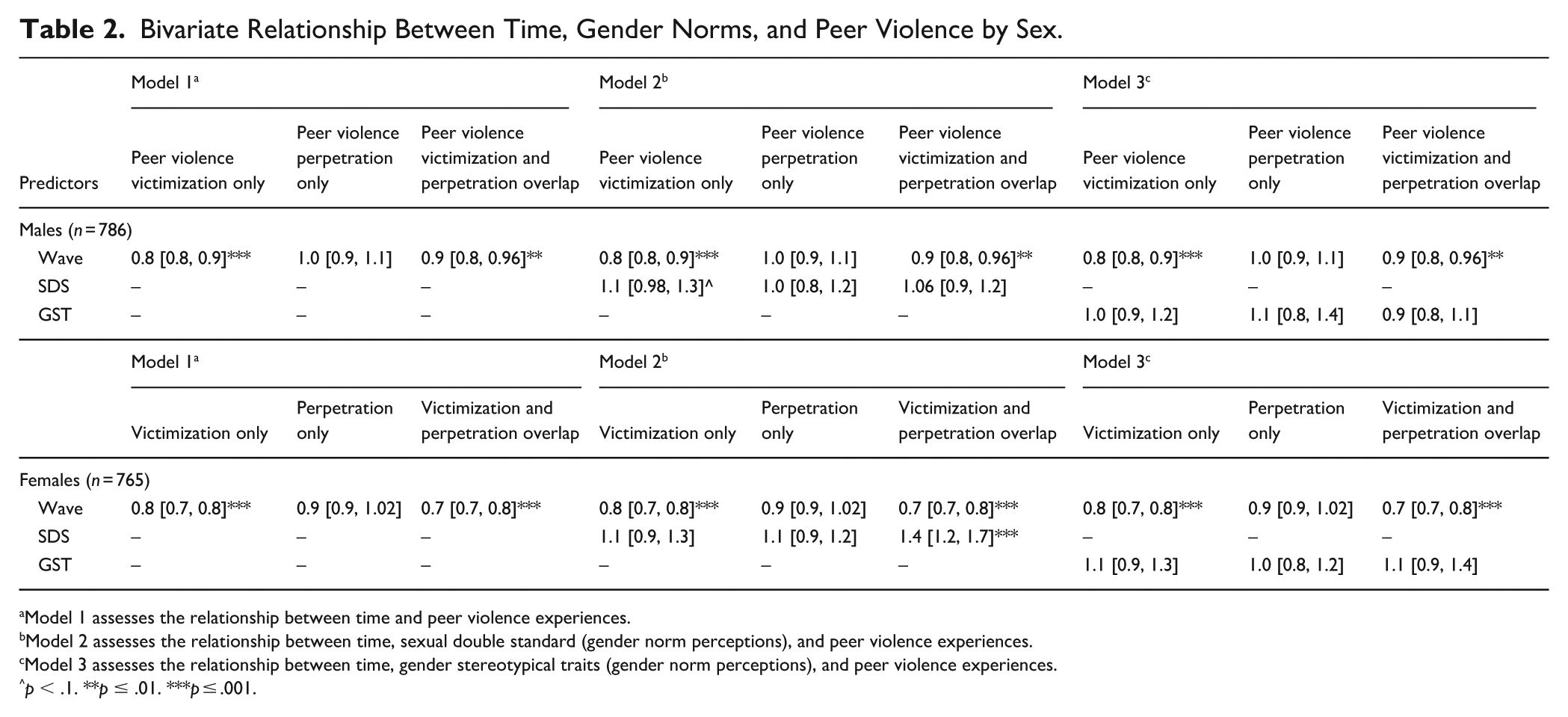
Model 1 assesses the relationship between time and peer violence experiences.
Model 2 assesses the relationship between time, sexual double standard (gender norm perceptions), and peer violence experiences.
Model 3 assesses the relationship between time, gender stereotypical traits (gender norm perceptions), and peer violence experiences.
p < .1. **p ≤ .01. ***p ≤ .001.
Table 3 presents the weighted multinomial logistic regression results, highlighting significant risk factors for peer violence among both sexes. Among males, after controlling for all other covariates, RRR for peer violence victimization only and peer violence victimization and perpetration overlap versus no peer violence, was 0.8 (95% CI [0.8, 0.9]; p ≤ .001) and 0.9 ([0.8, 0.96]; p ≤ .01), respectively, for the current survey wave relative to one wave prior. In the unweighted analysis (Supplemental Appendix 5), the RRR for peer violence victimization only versus no peer violence significantly increased for a one-point increase in SDS mean score (RRR: 1.2 [1.01, 1.3]). However, after applying weights, the association became borderline (p ≤ .1), with the RRR slightly reduced to 1.1 ([0.97, 1.3]; p < .1). Other factors associated with higher peer violence experiences versus no peer violence included having greater freedom of movement, ever drinking alcohol and experiencing 3+ ACEs (Supplemental Appendix 7).
Sex-Stratified Weighted Multinomial Logistic Regression, Assessing the Relationship Between Time, Gender Norms, and Peer Violence Using No Peer Violence Group as Reference. a
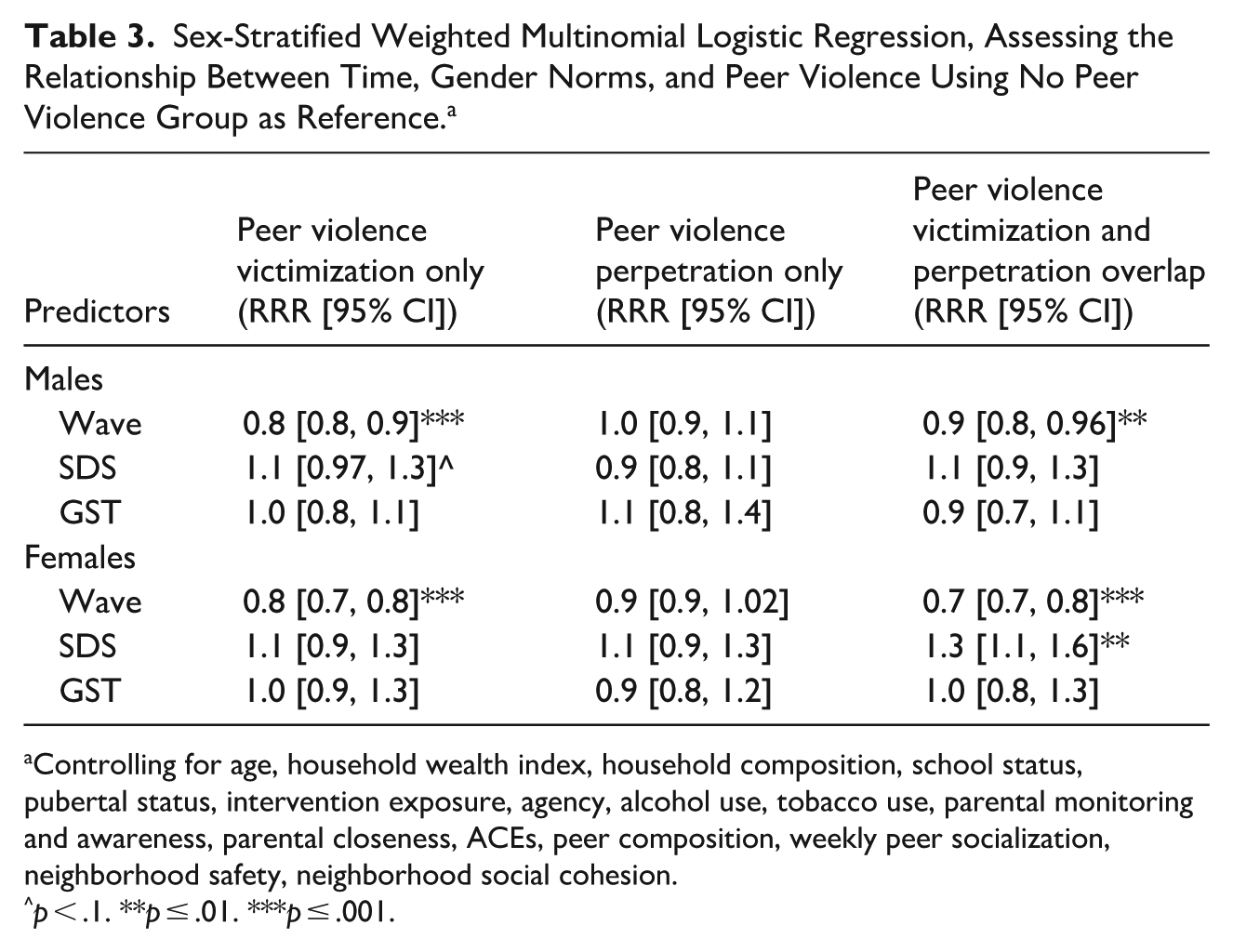
Controlling for age, household wealth index, household composition, school status, pubertal status, intervention exposure, agency, alcohol use, tobacco use, parental monitoring and awareness, parental closeness, ACEs, peer composition, weekly peer socialization, neighborhood safety, neighborhood social cohesion.
p < .1. **p ≤ .01. ***p ≤ .001.
Among females, RRR for peer violence victimization only and peer violence victimization and perpetration overlap versus no violence was 0.8 (95% CI [0.7, 0.8]; p ≤ .001) and 0.7 ([0.7, 0.8]; p ≤ .001), respectively, for the current wave relative to one wave prior (Table 3). For SDS, a one-point increase in the SDS mean score was associated with a 30% increase (RRR: 1.3 [1.1, 1.6]; p ≤ .01) in the risk of peer violence victimization and perpetration overlap. Other risk factors associated with peer violence experiences versus no peer violence included having attained puberty, ever drinking alcohol and having 2+ ACEs (Supplemental Appendix 8). Promotive factors include older age and high parental closeness (Supplemental Appendix 8).
Discussion
The aim of this study was to assess the role of gender norm perceptions in understanding peer violence trends between early to late adolescence by sex among under-resourced urban participants in Kinshasa, DRC. Specifically, we conducted sex-specific analyses to understand differences in trends and examined the role of gender norm perceptions using the SDS and GST scales (Moreau et al., 2021) on peer violence experiences. Over time, from 2017 to 2022, there was a reduction in peer violence experiences for both sexes, driven by decreased prevalence of peer violence victimization only and peer violence victimization and perpetration overlap. However, no change was seen in peer violence perpetration. Although unequal SDS increased risk of peer violence victimization and perpetration overlap among females, GST did not show any association with peer violence. Our study was designed to examine gender as a power system in shaping peer violence, our findings also revealed that ACEs and alcohol use intersected with gender to predict violence trajectories. This highlights the complex interplay between gender norms and other psychosocial factors in adolescent violence experiences for males and females.
SDS is a gender norm scale that rewards males for sexual progressions but sanctions females (Moreau et al., 2019). This study showed that more unequal perceptions of SDS are associated with peer violence victimization and perpetration overlap for females and is likely to be related to peer violence victimization among males. A GEAS paper assessing peer violence trajectories using Latent Class Analysis across three waves in three countries, including DRC, found that SDS increased the likelihood of being in the declining violence versus low violence category, suggesting cross-sectional associations instead of longer-term associations (Ramaiya et al., 2025). However, in this study, we see unequal SDS differentially relates to types of peer violence, with associations differing for males and females. There is an indication from literature within the United States that SDS is influenced by peer and societal norms with higher numbers of sexual partners associated with negative peer acceptance among girls but positive acceptance among boys (Dunn et al., 2014). Peer violence is a function of peer acceptance with lower peer acceptance associated with bullying victimization; therefore, girls who don’t conform to the norm are at increased risk of peer rejection through victimization and/or perpetration (Dunn et al., 2014). This gendered difference demonstrates that although peer violence disproportionally affects males (Corboz et al., 2018; Karmaliani et al., 2017; Ramaiya, Zimmerman, et al., 2021), SDS in particular is harmful for females in predicting peer violence experiences.
ACEs are adverse events experienced during childhood that affect lifelong health and well-being (Dube, 2019; Taillieu et al., 2019; Vig et al., 2019; Wekerle et al., 2019). Our study showed a significantly increased risk for peer violence experiences as the number of ACEs increased for both sexes. ACEs have consistently demonstrated associations with peer violence outcomes in both high- and low-income settings, including past GEAS studies (Beckwith et al., 2022; Blum et al., 2019; Ramaiya, Choiriyyah, et al., 2021; Ramaiya, Zimmerman, et al., 2021). Exposure to ACEs increases toxic stress through biological and behavioral changes affecting the neurobiological composition of the brain, which predicts future ill health (Claypool & Moore de Peralta, 2021; Shonkoff et al., 2012). Preventing and addressing childhood adversity by partnering with families and communities is critical to addressing peer violence.
The complex association between alcohol use and peer violence is particularly striking. Males were more likely to report alcohol use, which is consistent with global trends where male adolescents have higher odds of drinking alcohol and engaging in risky behaviors (Leung et al., 2019). For both sexes, alcohol use was linked to higher rates of peer violence victimization and perpetration overlap, suggesting that substance use may act as both a coping mechanism and a facilitator of aggression in peer interactions (Choo et al., 2014; Fine et al., 2022).
Implications for the Future
The results of this study have research and programmatic implications due to the different factors that affect peer violence experiences among adolescent males and females. In addition to the above factors observed for both sexes, other factors differ; having supportive neighborhoods and communities, promoting positive behaviors such as playing sports, mentorship, street outreach, and creating after-school programs could reduce peer violence among males (Centers for Disease Control and Prevention, 2021; Kia-Keating et al., 2017; Ohmer, 2016). Our study found parental closeness to be a promotive factor against peer violence victimization and perpetration overlap among females, highlighting the critical role that families play in mitigating peer violence. Family-based interventions that foster positive communication, emotional support, and active involvement in adolescents’ lives could serve as effective strategies to reduce peer violence. Unequal perceptions of SDS were also associated (significant and borderline) with increased peer violence experiences for both sexes. Gender transformative programs that address harmful SDS within peer and community networks are essential to reducing peer violence experiences and the cycle of violence across different environments (Centers for Disease Control and Prevention, 2021). Research implications stress the need to take a multifaceted approach to gender when examining health outcomes, especially peer violence. This study shows how various factors, such as freedom of movement, puberty, parental closeness, and age, differ and the importance of stratifying analyses by sex. Future research should also consider diverse gender identities as an important construct in understanding peer violence.
Limitations
Although this study is unique in its design and conceptualization of peer violence, it has limitations. As a longitudinal cohort, there was loss to follow-up, which introduced selection bias; however, we reduced this bias by applying inverse probability weights. The GEAS sample was among under-resourced urban adolescents in Kinshasa, DRC, limiting generalizability to all adolescents. Additionally, these analyses did not take into consideration gender-diverse individuals, which affects the extent to which we can extrapolate these results to the sexual and gender minority population. Peer violence, our main outcome variable, was measured within the past 6 months and did not measure frequency and dosage to determine if the behavior was repetitive. Additionally, the GST scale demonstrated low internal consistency (Cronbach’s alpha = .57 to .63), which may have attenuated associations between GST and peer violence outcomes. Violence usually occurs within different realms; not analyzing intimate partner violence, cyberbullying, and community violence could affect the understanding of violence. Lastly, all these associations were based on quantitative data, without further qualitative exploration on how and why factors between males and females differed. Qualitative research that explores the lived experiences of adolescents could help triangulate the findings of this study and provide deeper insights into how gender norms are internalized and acted upon in situations where peer violence occurs.
Conclusion
This study analyzed the role of sex and gender on peer violence trends in Kinshasa, DRC. Historically, peer violence has predominantly been assessed among males without inclusion of females. By exploring peer violence experiences over time through a unique variable, we are able to examine differences and similarities by sex over time. More unequal perceptions of SDS increased risk of peer violence victim and perpetration overlap among females and peer violence victimization only for males. ACEs and alcohol were risk factors for both sexes. Family-based programs combined with gender transformative interventions addressing SDS and alcohol use could prevent or mitigate peer violence experiences.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605261421619 – Supplemental material for Assessing the Role of Sex and Gender Norms in Peer Violence Trends During Adolescence: A Longitudinal Study From Kinshasa, Democratic Republic of Congo
Supplemental material, sj-docx-1-jiv-10.1177_08862605261421619 for Assessing the Role of Sex and Gender Norms in Peer Violence Trends During Adolescence: A Longitudinal Study From Kinshasa, Democratic Republic of Congo by Astha Ramaiya, Gayatri Malhotra, Aimée Lulebo, Eric Mafuta, Hanna George, Sabrina Page, Bushra Sabri, Mahboubeh Shirzad and Mengmeng Li in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We would like to acknowledge the program staff from Kinshasa School of Public Health, Democratic Republic of Congo, who worked through all obstacles to follow up with participants over 5 years. We would also like to acknowledge the Global Early Adolescent Study Hopkins Coordinating Center for supporting this work throughout the 5 years. Additionally, Saifuddin Ahmed played a critical role in determining the analysis plan for this paper. Finally, we would like to give our greatest appreciation to our participants who agreed to be in this study and providing us with their insights.
Ethical Considerations
The study received ethical approval from the Johns Hopkins Bloomberg School of Public Health and secondary approval from the Kinshasa School of Public Health (ESP/CE/023/2017).
Consent to Participate
The study sought written consent from parents and assent from minors to participate in the study.
Consent to Publication
Within the informed consent and assent; participants were also asked if the data could be used for dissemination, including publication without identifying individual participants.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: The data collection was funded by Oak Foundation [OCAY-17-649], Packard Foundation [2019-69311], United States Agency for International Development [AID-OAA-A-15-00042] and Bill and Melinda Gates Foundation [INV-009194]. The first author received salary support from Johns Hopkins University Faculty Innovation Fund to dedicate some of her time to conceptualize, analyze, and write this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.