
Abstract
Gambling severity has been linked to various social and health-related harms, including intimate partner violence (IPV). This study uses nationally representative health survey data from Finland (n = 28,153; collected in 2022 and 2023) to examine the associations between gambling severity and self-reported victimization from physical and psychological violence perpetrated by spouse. Gambling severity is assessed using the Problem Gambling Severity Index (PGSI). The analyses control for sex, age, family structure, socioeconomic status, mental health, and substance use. The data were analyzed using complex samples logistic regression. Any form of violence experiences was more commonly reported by women, younger respondents, and past-year gamblers. Women reported experiencing all forms of violence more frequently than men, with experiences of psychological violence being more prevalent than physical violence. Psychological violence perpetrated by family members was the most common type reported. The prevalence of violent experiences increased with higher gambling severity. In the logistic regression models, physical violence perpetrated by spouse was more likely to be reported by women, younger respondents, those with hazardous alcohol use, suicidal ideation, and PGSI scores of eight or more. Experiences of psychological violence perpetrated by spouse were more likely among women, younger age groups, those with one or two children younger than 18 years in the household, harmful alcohol use, and psychological distress. Respondents with higher PGSI scores were more likely to have experienced psychological violence, and even those who gambled at a non-problem level were more likely to report experiencing psychological violence. These findings underscore the importance of addressing gambling, mental health, and violence together in prevention and support services.
Introduction
Intimate partner violence (IPV) is a major public health and human rights concern with substantial social and economic consequences (Clarke, 2011; Scott-Storey et al., 2023). Despite growing recognition of gambling-related harm, its intersection with IPV is insufficiently understood. Consistent with the World Health Organization (WHO, 2021), IPV refers to physical, sexual, and psychological harm—including aggression, coercion, and controlling behaviors—within current or former intimate relationships. For clarity, we distinguish IPV from broader domestic violence: while domestic violence encompasses harm within the family more generally, IPV specifically involves violence between intimate partners and is the focus of this study. In this article, “experiencing violence” refers specifically to being a victim or survivor of violence perpetrated by another person, rather than the use or perpetration of violence.
Problem gambling (PG) has been consistently associated with increased IPV risk for both perpetrators and victims (Afifi et al., 2010; N. Dowling et al., 2016; Roberts et al., 2018, 2020). Previous research indicates that problem gambling may increase the likelihood of perpetrating violence and having convictions on violent crimes (Adolphe et al., 2019). In the Finnish context, gambling problems have also been identified as one of the background factors in some family homicides, as shown in recent analyses of mental state examinations of offenders (Ellilä et al., 2025). The present study, however, focuses on the risk of people experiencing gambling-related harm being victims of violence, examining their self-reported victimization.
The relationship between gambling and IPV victimization is complex and bidirectional. Gambling problems can lead to emotional distress, shame, and anxiety, which in turn may increase the risk of coercive control, emotional abuse, and financial harm in intimate relationships (Banks & Waters, 2023). According to Hing et al. (2016, 2024), women are particularly vulnerable to victimization by a partner with a gambling problem. Conversely, IPV and relationship conflict may contribute to the development of gambling problems, as individuals may use gambling as an escape or coping mechanism (Hing, Mainey, et al., 2023). Despite this, IPV often goes unreported also in gambling contexts due to stigma and perceptions that such violence is not criminal (Banks & Waters, 2023; Hing et al., 2024).
In one study, 63% of individuals with PG reported IPV victimization experiences (Korman et al., 2008). The severity of a partner’s gambling behavior is a strong predictor of IPV victimization (Liao, 2008; Muelleman et al., 2002), and nationally representative studies from the United States and the United Kingdom have reinforced this association (Afifi et al., 2010; Roberts et al., 2018, 2020). Help-seekers for gambling-related issues also report higher rates of family violence than the general population (Palmer du Preez et al., 2018).
Sex differences in gambling-related IPV are well documented. Research indicates that problem gambling increases IPV perpetration in both men and women, but victimization risk appears higher for women (Roberts et al., 2018). Men with gambling problems are more likely to engage in physical or verbal IPV, whereas women show lower perpetration rates (Suomi et al., 2013). Despite these findings, most studies focus on women in heterosexual relationships, with limited attention to male victims (Scott-Storey et al., 2023). Because IPV is a gendered phenomenon, understanding men’s experiences requires attention to masculinity, gender norms, and stigma. A recent review emphasized the need for gender- and age-sensitive research on gambling and IPV (Hing et al., 2016).
Family systems and cultural norms also influence the dynamics of IPV. Family can serve either as a protective buffer or as a source of escalation, while cultural attitudes that normalize violence against women or reinforce rigid gender roles can increase the risk of IPV, particularly when help-seeking is stigmatized (Hing et al., 2023; Tur-Prats, 2021).
Problem gambling frequently co-occurs with other IPV risk factors such as mental health problems and substance use. Gambling is commonly comorbid with depression, hazardous alcohol use, and other psychiatric conditions (Hing et al., 2016; Loo et al., 2019; Lorains et al., 2011), which in turn increases IPV risk (McManus et al., 2022, 2023). For instance, alcohol use disorder elevates the likelihood of IPV in relationships affected by gambling problems (Brasfield et al., 2012), and individuals with histories of substance use and violent behavior are more likely to report gambling-related issues than those without such a history. Similarly, individuals with both substance use and violent behavior are more likely to report gambling issues than their counterparts without involvement in violence (Cunningham-Williams et al., 2007). While some studies found no significant differences in alcohol use between violent and non-violent problem gamblers (Lavis et al., 2015), the broader evidence suggests that gambling-related harms, particularly when combined with other mental health challenges, are associated with IPV (N. A. Dowling et al., 2025a).
Socioeconomic disadvantage further amplifies these risks. Lower education and limited employment opportunities increase vulnerability to both problem gambling and IPV (Hing et al., 2016; Weitzman, 2018). Poverty, unemployment, and residence in deprived neighborhoods also heighten IPV risk (Lucero et al., 2016). Financial instability can lead to household conflict, economic coercion, and control, particularly when household income is diverted to gambling (Hing et al., 2024; Järvinen-Tassopoulos, 2020; Suomi et al., 2013). Children in such households are also affected, facing increased risks of direct or indirect abuse and long-term behavioral and emotional difficulties (Jofre-Bonet et al., 2025). When gambling-related stress affects the household, frustration may be displaced onto children, reinforcing cycles of violence (Hing et al., 2024; Suomi et al., 2013).
Social isolation and perceived exclusion (Eckhardt et al., 2022) are additional factors linking gambling and IPV. Individuals with low social inclusion often experience a lack of control over their lives, diminished support networks, and reduced meaningful engagement in society (Isola et al., 2021) contributing to psychological distress and maladaptive coping behaviors, such as gambling (Hing et al., 2016). While gambling may initially provide a sense of escape or control, it often escalates financial and relational problems, further increasing the risk of interpersonal violence.
In Finland, IPV remains a significant public health concern, with the majority of victims being women. The domestic violence experienced by women tends to be more prolonged and occurs more repeatedly than the domestic violence experienced by men (Siltala et al., 2022). According to the Statistics Finland’s data, 12,300 victims of domestic and IPV offenses were reported to the authorities in 2023, 76% of whom were adults and 25% minors (under 18 years; percentages do not sum to 100% due to rounding). Notably, IPV perpetrated by spouses grew by 11% from 2022 (Statistics Finland, 2024). It should be noted, however, that IPV is widely underreported in many settings, and that gender differences exist in how violence is experienced (Follingstad & Rogers, 2013). Cultural attitudes, stigma, and fear often prevent victims from reporting incidents to authorities, and these same factors make IPV difficult to capture reliably in surveys (Cullen, 2023). Consequently, official statistics in Finland reflect only the cases that reach the attention of authorities (Statistics Finland, 2024) and therefore underestimate the true prevalence of IPV.
Despite growing evidence on the co-occurrence of gambling problems and IPV, several important gaps remain. Most research has focused on women in heterosexual relationships, with limited attention to male victims or to gendered experiences shaped by social roles, norms, and power relations that may affect individuals across different relationship types. Additionally, few studies have simultaneously examined gambling severity alongside a broad range of demographic, socioeconomic, mental health, substance use, and social factors that may contribute to IPV risk. This lack of comprehensive, multi-factorial research limits our understanding of which individuals experiencing gambling harm are most vulnerable to IPV and how intersecting risk factors interact. To address these gaps, the present study investigates (a) whether individuals with more severe gambling problems report higher levels of IPV and (b) how IPV experiences are associated with age, sex, education, income level, the presence of children under 18 in the household, gambling severity, mental distress, hazardous alcohol use, social inclusion, and suicidal ideation. By integrating these factors in a single analysis, this study provides a more nuanced understanding of the relationship between gambling harm and IPV in Finland.
Data and Methods
This study used data from the population-based Healthy Finland survey, which was conducted by the Finnish Institute for Health and Welfare between September 2022 and February 2023 (Sääsjärvi et al., 2025). This survey examines various aspects of health, well-being, and service use within the Finnish population. A nationally representative sample of 61,000 permanent Finnish residents aged 20 and older was selected using stratified random sampling. The survey was available in both paper and online formats in Finnish, Swedish, English, and Russian. A total of 28,154 individuals responded, yielding a response rate of 46.3%. The data were weighted according to age, sex, marital status, education level, first language, and area of residence. Further details on the dataset can be found elsewhere (Koskela et al., 2023; Sääsjärvi et al., 2025).
Measures
To address the study’s aims, measures capturing IPV, sociodemographic characteristics, well-being indicators, and gambling severity were included. Together, these measures allow us to examine how gambling-related harm intersects with psychosocial distress, relationship dynamics, and broader social inclusion.
IPV was assessed with a set of behaviorally specific items to capture both physical and psychological forms of violence. Measures concerning physical or psychological IPV were based on the questions: “Has anyone behaved violently toward you during the past 12 months?” The questions included the following: threatened to physically harm you in person, over the phone, or online; prevented you from moving; grabbed you, shoved, pushed, or slapped you; hit you with a fist or an object, kicked, strangled, suffocated, burned, or used a weapon to hurt you; called you names to belittle or humiliate you; tried to limit or has limited your contact with others (e.g., your family, relatives, or friends). The response options were as follows: no one, current or former spouse or partner, another family member or relative, and another acquaintance. The survey item used the term “spouse,” although the intended construct corresponds to the broader category of intimate partners. The survey did not allow differentiation between married and non-married partners, separated versus divorced partners, or whether former partners had re-partnered. While the degree of intimacy may differ for current versus former spouses, both are treated as intimate partner relationships in this study.
Sociodemographic Factors
Sociodemographic variables were included to contextualize the sample and to account for structural factors known to shape both well-being and gambling behaviors. Education was measured by the total years of schooling and categorized into three levels: low, medium, and high. The cut-off points were determined separately for different age and sex groups.
Household income was assessed with the question: “What was your household income last year (before tax)?” Response options included the following: under €15,000; €15,001 to €35,000; €35,001 to €55,000; €55,001 to €75,000; and over €75,001. For analysis, the last two categories were combined into a single group: “over €55,001.” In Finland in 2023, the median disposable household income was approximately €35,738 (Statistics Finland, 2025). Thus, our income categories roughly cover below-average (under €15,000), low-to-middle (€15,001–€35,000), and above-average (over €55,001) household incomes relative to national norms at that time.
Family status was defined by combining information on household size and the number of children under 18. The variable was categorized into three groups: single-person households, couples, and families with children.
Sociodemographic factors had no missing values for sex, age, or family status, while missing data were minimal for education (2.2%) and household income (2.5%).
Factors of Well-Being
Indicators of well-being were included to capture the broader health and psychosocial context in which gambling and IPV may co-occur. Given that alcohol use is closely linked to both gambling harm and relationship strain, hazardous drinking was evaluated using the modified three-item Alcohol Use Disorder Identification Test (AUDIT-C; Bush et al., 1998), which assesses drinking frequency, quantity, and binge drinking. The total score ranges from 0 to 12. The thresholds for excessive alcohol use are set at ≥6 for men aged 20 to 64, ≥5 for women aged 20 to 64, and ≥4 for individuals aged 65 and older (Finnish Medical Society Duodecim & Finnish Association for Addiction Medicine, 2017; Seppä, 2010). This measure had 4.3% missing data.
To capture the possible effects of IPV and gambling on psychological welfare, severe psychological distress was measured using the five-item Mental Health Inventory (MHI-5; Berwick et al., 1991), which evaluates emotional well-being (nervousness, blues, jollity, calmness, and happiness) over the past four weeks on a six-point scale (1 = all the time, 6 = not at all). Total scores for the MHI-5 were obtained by summing the individual item scores (range: 4–30), which were then transformed to a scale from 1 to 100. Severe psychological distress was defined as a score 52 or below (Viertiö et al., 2021). Missing data for this measure accounted for 4.6%.
Because gambling harm and IPV have been linked to elevated suicidality, we also assessed past-year suicidal ideation. Suicidal ideation was assessed with the question: “Have you had suicidal thoughts in the past 12 months?” with response options of “yes” or “no.” This measure had 2.3% missing data.
Social inclusion reflects individuals’ sense of belonging and agency, and low social inclusion has been associated with both mental health problems and gambling harm. The experience of social inclusion was measured using the Experiences of Social Inclusion Scale (ESIS; Leemann et al., 2022). The ESIS consists of 10 statements that assess the experience of meaningfulness, belief in one’s ability to act, and the perceived quality of social interaction. Each statement is rated on a scale from 1 to 5. The total score of the scale is calculated by summing the scores of the statements, resulting in a total score between 10 and 50. This score is then converted to a scale ranging from 0 to 100. A higher score indicates a stronger experience of social inclusion. In accordance with Leemann et al. (2022), a cutoff of 50 points was used to determine low social inclusion. Cronbach’s alpha for the scale was .907, indicating high internal reliability.
Past-year gambling severity was assessed using the Problem Gambling Severity Index (PGSI), which includes nine self-reporting questions (Ferris & Wynne, 2001). The PGSI items have a four-point scale: 0 = never, 1 = sometimes, 2 = most of the time, and 3 = almost always. The total scores ranging from 0 to 27 were calculated, and the following five categories were classified: non-gambling, non-problem gambling (score of 0), low-risk (score 1–2), moderate-risk (score 3–7), and problem gambling (score ≥8). The non-gambling category included individuals who responded “not at all” to the question: “Think about the past 12 months, how often did you gamble?” This measure had a missing data rate of 4.9%.
Statistical Analyses
Descriptive statistics were used to summarize sample characteristics. Differences in categorical variables were assessed using χ² test. To examine associations among experiences of partner violence (psychological and physical), sociodemographic characteristics, psychosocial indicators, and gambling severity, we employed complex samples logistic regression to account for the stratified sampling design and apply appropriate weighting. Separate models were specified for psychological violence and physical violence (Williams et al., 2012; WHO, 2012), with the presence of such experiences coded as the dependent variable and absence of violence used as the reference category. For example, items such as threats, insults, and controlling behaviors are classified as psychological, while items involving hitting, slapping, or restricting movement (e.g., “prevented you from moving”) are classified as physical. Model estimates are reported as odds ratios (ORs) with 95% confidence intervals (CIs). Analyses were weighted by age, sex, marital status, education level, first language, and area of residence. All statistical analyses were conducted using IBM SPSS Statistics (version 29.0.2.0, Armonk, NY: IBM Corp).
Ethics
The research permits required were obtained for the Healthy Finland survey (Sääsjärvi et al., 2025). Written information about the study and the voluntary nature of participation was provided to all potential participants. Completion of the questionnaire was considered as an indication of informed consent. The ethics committee of the Finnish Institute for Health and Welfare approved the research protocol (THL/72/6.02.01/2022). The results of this study are presented in a way that the participants cannot be identified: no combinations of variables or descriptive details are reported that could permit identification of individual participants. Categories with fewer than five observations are not reported to further protect participant confidentiality.
Results
Higher PGSI categories were more prevalent among male respondents, individuals aged under 60 years, those who were single or divorced/separated, respondents with lower household income, fewer years of education, hazardous alcohol use, psychological distress, suicidal ideation, and low social inclusion (Table 1). Overall, these patterns indicate that elevated gambling severity tended to cluster with various psychosocial vulnerabilities.
PGSI Categories by Demographic Characteristics (%).
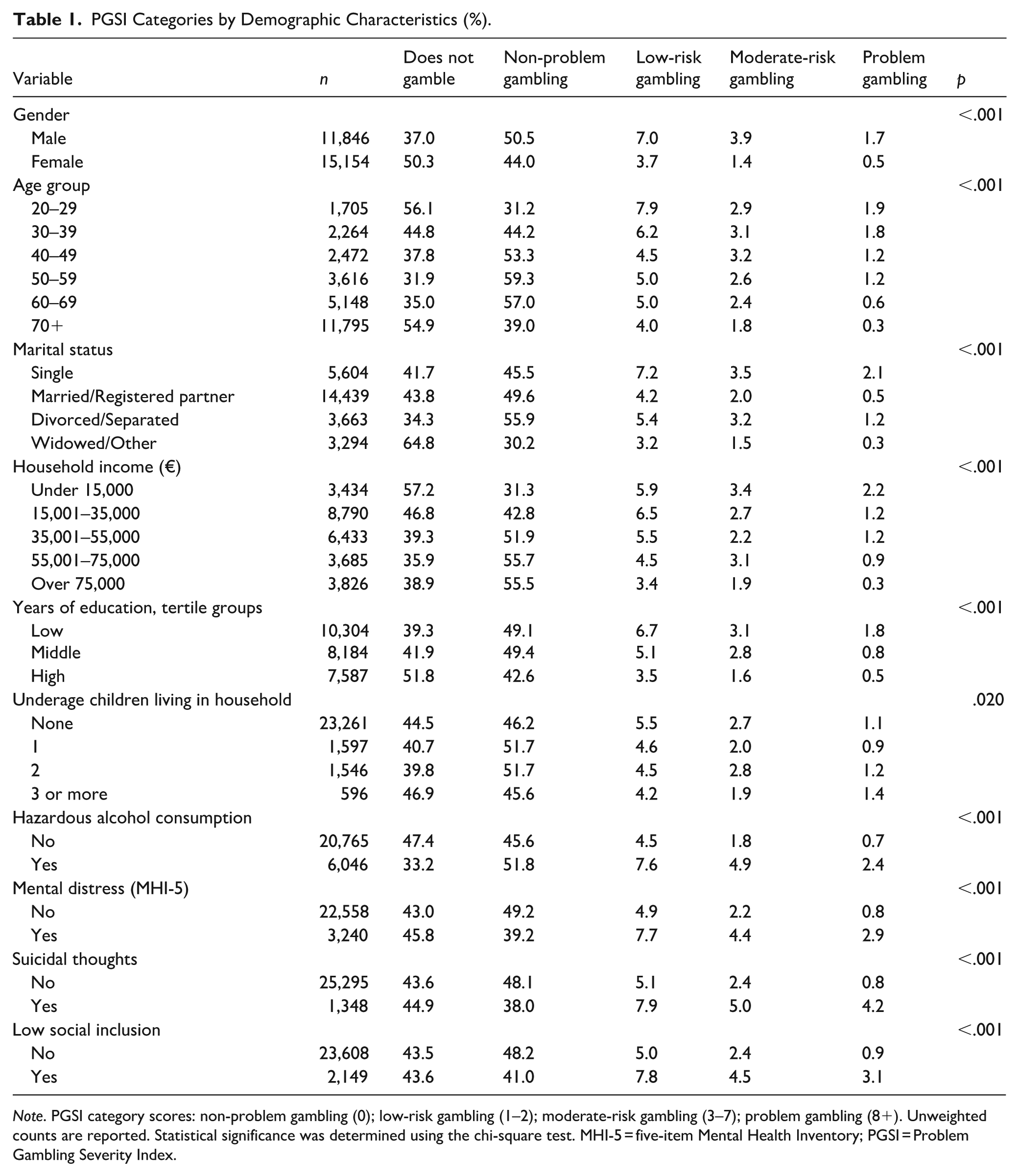
Note. PGSI category scores: non-problem gambling (0); low-risk gambling (1–2); moderate-risk gambling (3–7); problem gambling (8+). Unweighted counts are reported. Statistical significance was determined using the chi-square test. MHI-5 = five-item Mental Health Inventory; PGSI = Problem Gambling Severity Index.
Experiencing any form of violence was more common among females than males and more common among younger age groups (Table 2). The prevalence of experiencing violence was higher among individuals who had gambled in the past 12 months. This trend was consistent across all examined forms of violence.
Experiences of Violence by Gender, Age Group, and Past-Year Gambling Activity (%).
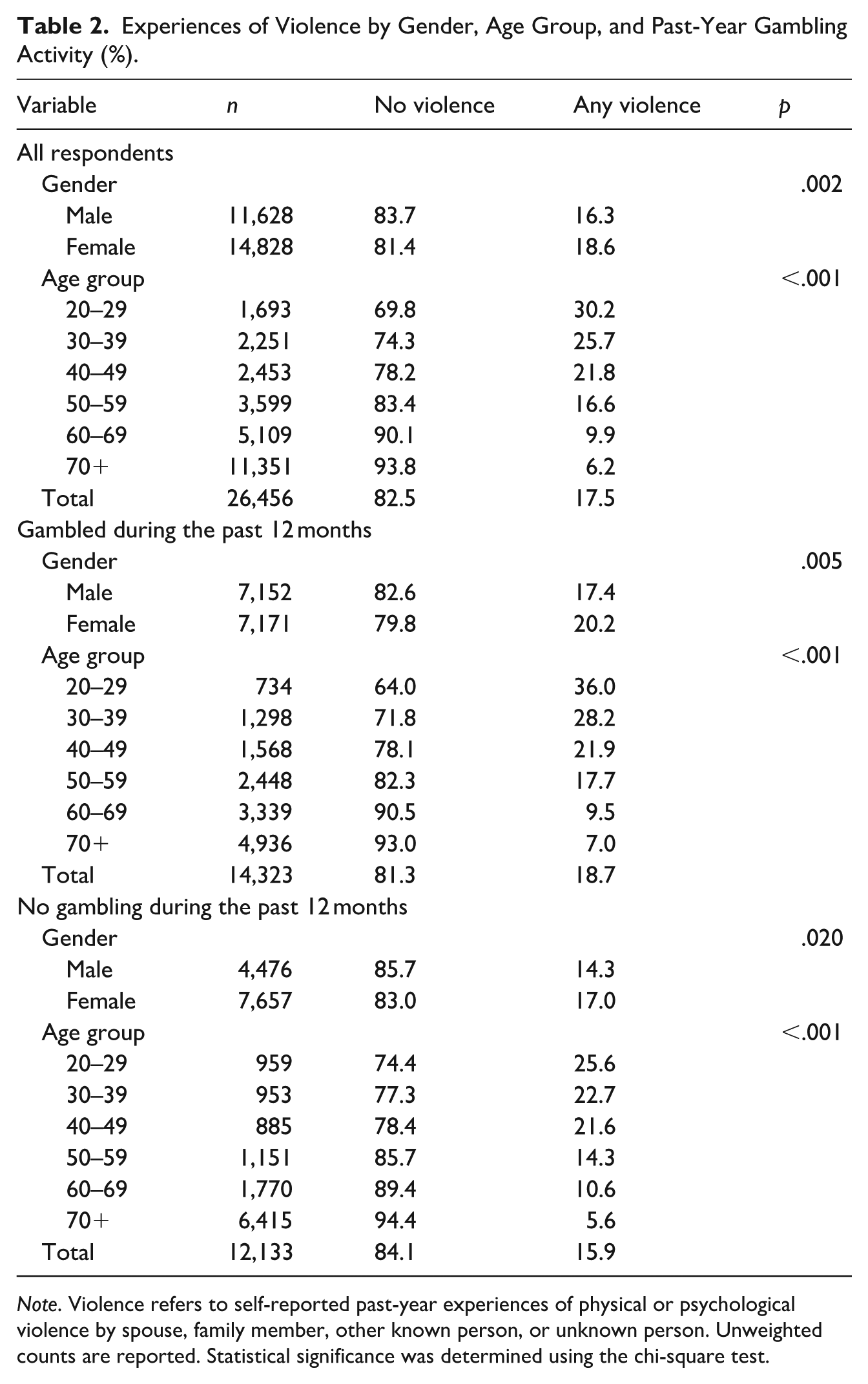
Note. Violence refers to self-reported past-year experiences of physical or psychological violence by spouse, family member, other known person, or unknown person. Unweighted counts are reported. Statistical significance was determined using the chi-square test.
Females experienced violence more commonly than males across all categories of violence and perpetrators (Table 3). Similar patterns were observed across PGSI groups, with all forms of violence being more common in higher PGSI score groups.
Individuals Reporting Violence (%) Experiences by PGSI Category and Gender.
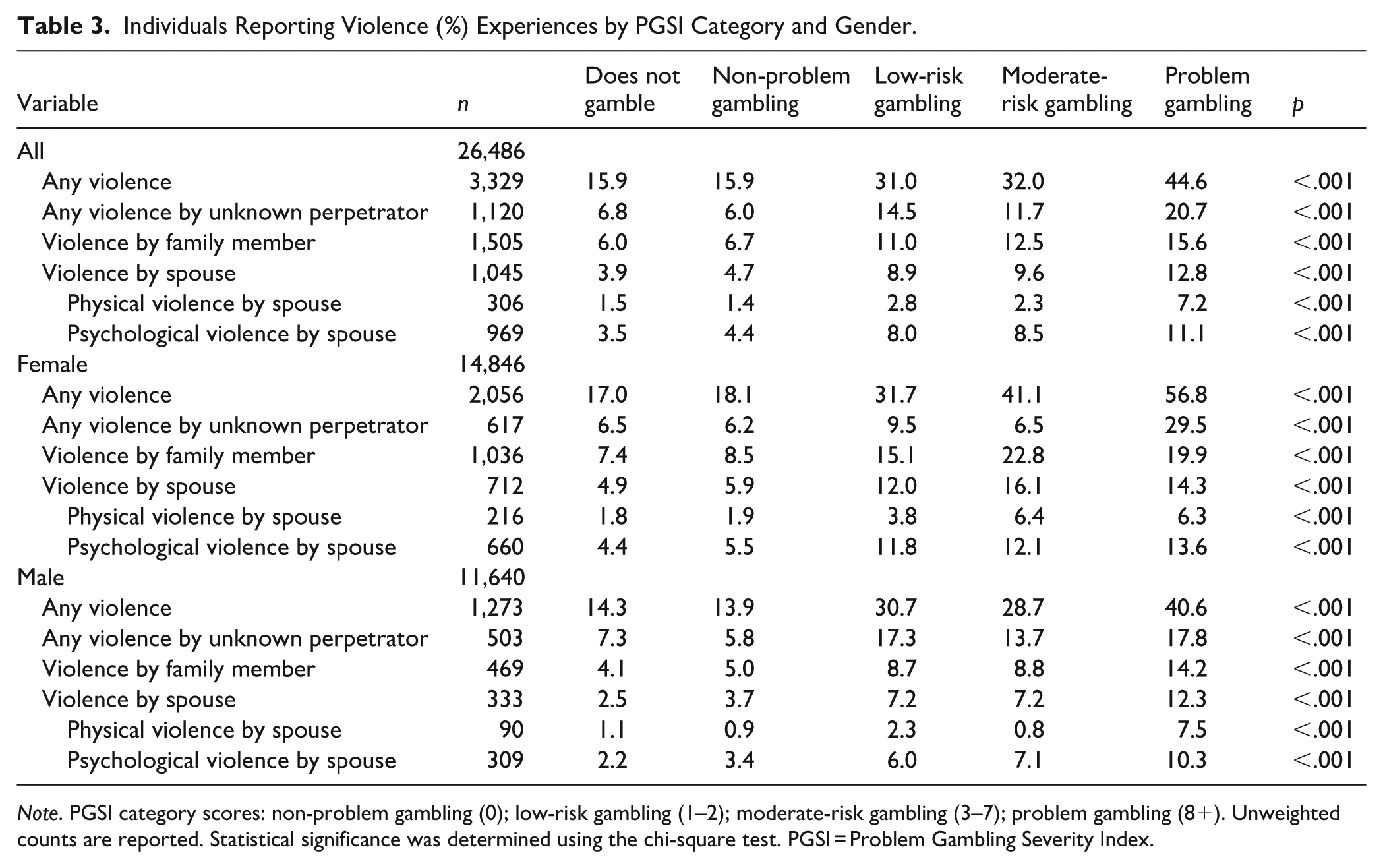
Note. PGSI category scores: non-problem gambling (0); low-risk gambling (1–2); moderate-risk gambling (3–7); problem gambling (8+). Unweighted counts are reported. Statistical significance was determined using the chi-square test. PGSI = Problem Gambling Severity Index.
Violence by family members was the most common subtype. Psychological violence was more prevalent than physical violence. However, when observed by perpetrator, compared to females, males especially among the higher PGSI categories experienced physical violence more often by an unknown perpetrator.
In complex sample logistic regression models, females were more likely than males to report experiences of physical violence by a spouse (OR 2.01, 95% CI [1.46, 3.03]), as were all younger age groups except those aged 60 to 69 years, compared with individuals aged 70 years or older. Individuals reporting hazardous alcohol use had increased odds of reporting spousal physical violence compared with those without such use (OR 1.99, 95% CI [1.42, 2.79]), as did respondents with suicidal thoughts compared with those without (OR 2.23, 95% CI [1.44, 3.46]). Problem gamblers were more likely to report spousal physical violence than non-gamblers (OR 2.82, 95% CI [1.16, 6.88]). Together, these findings highlight that both behavioral and mental health factors contributed independently to heightened risk.
Females were also more likely than males to report psychological violence (OR 1.90, 95% CI [1.55, 2.33]), and all younger age groups except those aged 60 to 69 years had increased odds compared with individuals aged 70 years or older. Respondents with one (OR 1.43, 95% CI [1.06, 1.93]) or two (OR 1.68, 95% CI [1.18, 2.39]) children younger than 18 years in the household were more likely to report psychological violence than those with no children. Hazardous drinking (OR 1.49, 95% CI [1.21, 1.84]) and psychological distress (OR 1.38, 95% CI [1.01, 1.90]) were both associated with increased odds of reporting psychological violence. Compared with non-gamblers, all PGSI groups had higher odds of reporting psychological violence by a spouse. The likelihood of psychological violence increased steadily among respondents scoring at least one point on the PGSI (Tables 4 and 5).
Tests of Model Effects.
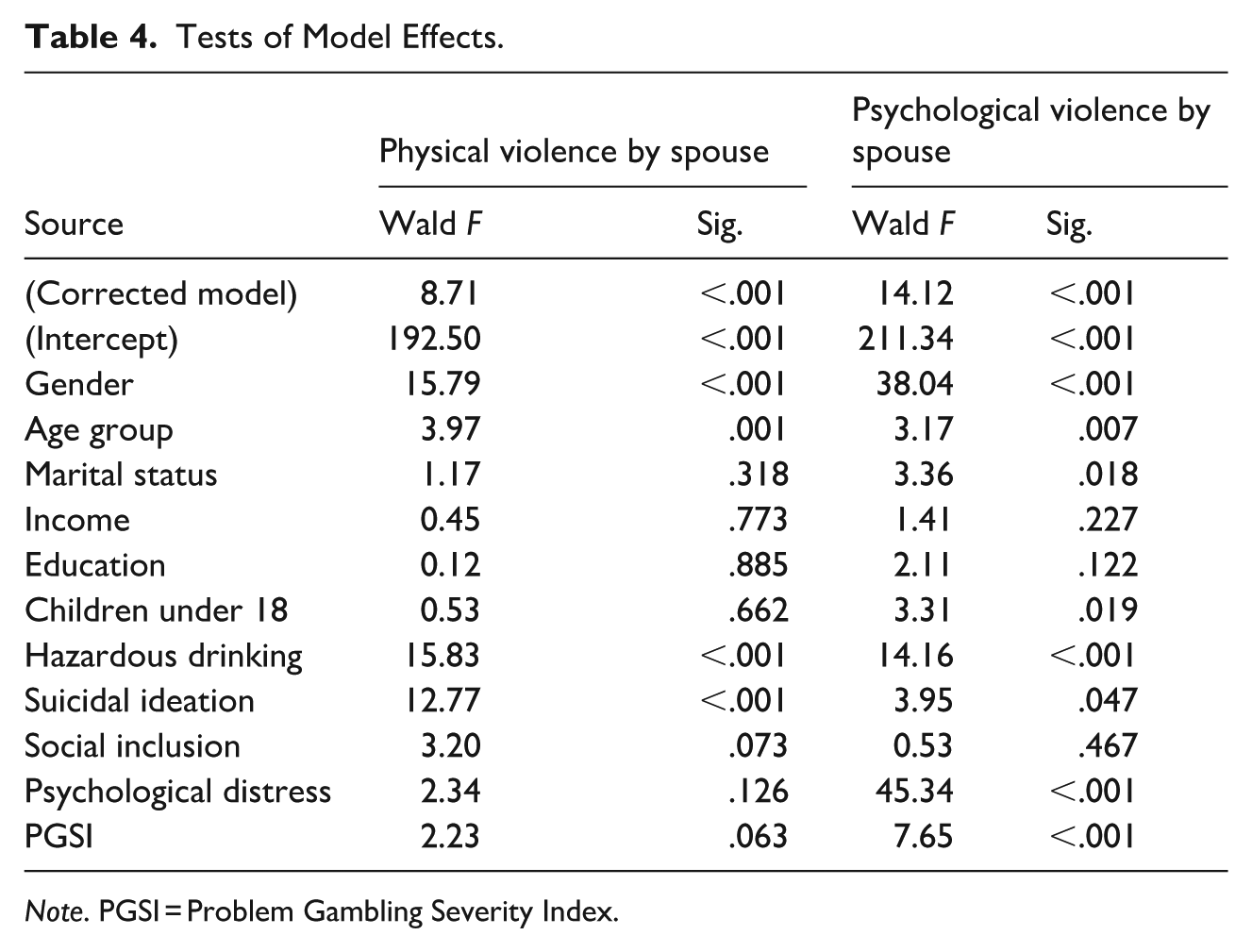
Note. PGSI = Problem Gambling Severity Index.
Complex Sample Logistic Regression Models With Odds Ratios.

Note. OR = odds ratio; PGSI = Problem Gambling Severity Index.
Discussion
This study aimed to examine (a) whether individuals with greater gambling severity experience higher levels of IPV and (b) whether associations exist among problem gambling (PG), IPV experiences and age, sex, education, income, mental distress, hazardous alcohol use, social inclusion, and suicidal ideation.
Our results demonstrate a clear link between gambling severity, as measured by the PGSI, and experiences of violence perpetrated by spouse. Higher PGSI scores were associated with increased likelihood of both physical and psychological IPV. Psychological IPV was reported across all levels of gambling involvement, including among non-problem gamblers, indicating a pattern that extends beyond those with gambling problems. Individuals scoring 8 or more were significantly more likely to report physical IPV. These findings align with prior research identifying gambling as both a consequence and contributing factor to IPV (Browne et al., 2016; N. A. Dowling et al., 2025a; Hing et al., 2016; Hing, O’Mullan, et al., 2023).
Mechanisms and Risk Pathways?
Although our data do not allow conclusions about causal relationships, gambling may serve as a maladaptive coping strategy in relationships where one partner uses violence, especially among trauma survivors seeking escapism (Suomi et al., 2013). More harm from IPV is found under conditions of gambling-induced financial strain, emotional distress, family disruption, and interpersonal conflict (Hing et al., 2016; Hing, Mainey, et al., 2023; Hing, O’Mullan, et al., 2023; Holdsworth et al., 2013; Patford, 2009; Saugeres et al., 2012). Financial hardship, such as debt and depleted family resources, is a common consequence of PG and a driver of household stress that can trigger IPV. While low income did not directly predict IPV, it was linked to higher PGSI scores. The emotional toll of financial insecurity, including shame, guilt, and helplessness, may compound mental health challenges and increase vulnerability to both PG and IPV.
Gender Differences and Cultural Factors
Women were significantly more likely to report all forms of IPV, especially partner violence (Hing et al., 2016, 2023). Men, in contrast, reported slightly more physical violence experiences by unknown perpetrators. Gendered help-seeking patterns may be influenced by social norms, with women feeling responsible for home life (Clarke, 2011), while younger women may be more likely to report abuse (Piispa, 2004). The role of gambling in IPV may be underrecognized, particularly as women’s gambling often carries greater stigma and deviates more from gendered norms than men’s (Palmer du Preez et al., 2021), potentially influencing both disclosure and service engagement (Baxter et al., 2015).
Alcohol Use, Mental Health, and Co-Occurring Problems
In Finland, IPV is often included under broader violence categories and associated with alcohol-related harm (Clarke, 2011), yet little is known about IPV among individuals with gambling problems (cf. J. Järvinen-Tassopoulos, 2016). Hazardous alcohol use was more common among those with problem gambling and consistently predicted both physical and psychological IPV. Substance abuse is a well-established driver of IPV, particularly among men (Afifi et al., 2010; N. Dowling et al., 2016). Gender-specific interventions may be needed, such as alcohol treatment programs for men and integrated care for women. N. Dowling et al. (2016) also found that controlling for mental disorders weakened the link between PG and IPV, highlighting the central role of psychological vulnerability.
Psychological distress was strongly associated with psychological IPV. Individuals reporting suicidal ideation were also more likely to experience physical violence, pointing to the need for integrated mental health and crisis support in PG and IPV services.
Social Exclusion and Family Context
Problem gambling was more common among respondents with low social inclusion, although this did not directly correlate with IPV in our data. Still, prior research links social exclusion to loneliness, poor decisions, and harmful relationships (Hing et al., 2016; Suomi et al., 2013). Strengthening social bonds and reducing stigma may help prevent both IPV and PG.
Family dynamics also matter: having one or two children younger than 18 years was associated with increased psychological violence, compared to living alone or being separated/divorced or having more than three children younger than 18 living in the household. This suggests the need to assess also caregiving stress when treating co-occurring PG and IPV.
IPV remains under-identified in Finnish services, with only 10% to 20% of serious IPV cases reported to police (Siltala et al., 2022). Although not a separate crime in Finland’s Criminal Code, IPV is treated differently than stranger violence (Fagerlund et al., 2022). Finland’s ratification of the Istanbul Convention in 2015 extended also protection to male and boy victims, but it is likely that many groups such as socially disadvantaged men, for example, remain outside service scopes.
Societal Framing of Violence and Gambling
Violence is culturally constructed and context-dependent (Hearn, 1998; Piispa, 2003). Hearn (1998) recommends the term “men’s violence” to reflect broader power structures. According to our findings, the prevalence of psychological IPV was 18.6% among women and 16.3% among men. Although these percentages are relatively close, the impacts, contexts, and patterns of IPV can differ substantially by gender. Therefore, while it is important not to overlook male victims, the gendered dynamics and consequences of IPV must still be acknowledged. Norms around violence and masculinity also shape reporting and service use. Finland’s high IPV rates may stem from deeper socio-cultural factors, including historical narratives that valorize aggression (Matikainen, 2015; Rantala, 2011). While such narratives risk stereotyping men as perpetrators, they might also obscure male victimization, especially in public or even domestic settings (Clarke, 2011). Many marginalized men grow up in environments where aggression is normalized as survival rather than celebrated cultural behavior (Fleming et al., 2015).
Gambling and violence permeate everyday Finnish life to some extent. Gambling is accessible in supermarkets, gas stations, and online. IPV, too, cuts across social domains: work, relationships, and leisure (Hearn, 1998). In situations involving partner violence, the secrecy of gambling can deepen, compounding isolation and stress. In social settings where both behaviors are normalized, gambling and IPV may reinforce one another.
Implications
This study has important implications for clinical practice, policy, and research. The demonstrated link between gambling severity and IPV underscores the need for systematic cross-screening in both gambling and IPV services. Routine inquiry about gambling in IPV assessments, and vice versa, could enable earlier detection and more comprehensive intervention strategies.
Integrated, multidisciplinary services are essential. These should combine trauma-informed care, substance use support, mental health treatment, and violence prevention. Mental health providers must be trained to recognize the co-occurrence of PG, IPV, suicidal ideation, and psychological distress. Although services for gambling problems, IPV, and suicide prevention in Finland already involve elements of multidisciplinary collaboration, existing evidence indicates that practice is uneven and that substantial gaps in professional competence remain. Heiskanen et al. (2021) report that while most municipalities offer treatment for gambling problems and collaborate with other services (e.g., mental health, social work, debt counseling, and child protection), visibility of services is limited and 90% of municipalities identify a need for further professional training. Similarly, national initiatives have strengthened suicide-prevention skills (Partonen et al., 2023) and are expanding systematic IPV-related training across welfare regions (Finnish Institute for Health and Welfare [THL] project 2025–2027), yet these programs do not guarantee that all frontline providers consistently recognize or assess the co-occurrence of problem gambling, IPV, suicidal ideation, and psychological distress. A further indication of uneven practice is that the national Current Care Guidelines for Suicide Prevention (Current Care Guideline, 2023b) do not address problem gambling, while the newer Current Care Guideline for Problem Gambling (Current Care Guideline, 2023a) includes suicide-risk assessment and screening. This inconsistency suggests that sectors vary in how fully they recognize and respond to the interconnected risks of gambling-related harm and suicidality. Consequently, our findings highlight a persistent need to better integrate screening and cross-sector competencies. Rather than assuming that multidisciplinary services are already “essential,” the study underscores an empirical rationale for testing structured, integrated models, such as controlled comparisons between standard care and enhanced care with targeted PG, IPV, or suicide-risk screening to determine whether more coordinated approaches improve outcomes. In addition, The Stress–Strain–Information–Coping–Support model highlights the need to support affected family members by addressing their psychological burdens (van Beek et al., 2024).
Age- and gender-specific outreach should be prioritized, especially for young adults and women, and include interventions targeting trauma, alcohol misuse, and emotional regulation. While financial strain did not independently predict IPV in our models, its close link to gambling severity supports the inclusion of financial counseling and debt relief services in both treatment pathways. Similarly, social inclusion was linked to gambling but not IPV, suggesting that community-based efforts to reduce stigma and foster belonging could help buffer against maladaptive coping behaviors, such as excessive gambling or aggression.
From a public health perspective, it is crucial to addressing the overlapping harms of financial stress, emotional distress, and interpersonal violence. These shared risk factors should inform preventive screening and early intervention efforts across sectors. Integrating IPV screening into gambling services could help identify high-risk individuals earlier (Davis & Lee, 2021; Suomi et al., 2013). Public awareness campaigns should highlight the connections between gambling and IPV while also challenging stigma and gendered barriers to help-seeking (Overstreet & Quinn, 2013). Male victims, in particular, may fear disbelief or shame, and gender-neutral or male-specific services remain limited (Machado et al., 2024). Without tailored care (N. A. Dowling et al. 2025b), protective systems risk remaining symbolic.
The social and economic burden of IPV spans criminal justice, health, housing, and social services (Clarke, 2011; Jofre-Bonet, Rossello-Roig & Serra-Sastre, 2024). IPV victims rely on these systems at significantly higher rates than the general population (Siltala et al., 2022), and financial dependency often necessitates social and child protection support for safe exits from abusive situations (Hing et al., 2024; H. Järvinen-Tassopoulos, 2020). Policies should address structural determinants, e.g., housing instability, income inequality, and limited access to care, and foster intersectoral strategies that reduce harm and promote resilience.
Finally, research must advance by collecting longitudinal data to clarify gendered and social pathways linking PG and IPV. Evidence-based, gender-sensitive interventions remain a priority for both prevention and treatment.
Strengths and Limitations
The strengths of this study are noteworthy. It utilized data from the large, nationally representative Healthy Finland survey (n = 28,153), which includes a wide range of questions related to health, well-being, and service use among Finnish adults. However, several limitations should also be acknowledged. As with many population-based surveys, the Healthy Finland survey was affected by non-response, which may limit the generalizability of the results. The participation rate was low among men aged 20 to 39 years (21.9%), which is particularly relevant given the high prevalence of gambling problems in this subgroup (Sääsjärvi et al., 2025; THL, 2024). Additionally, individuals with the lowest education level participated less actively than those with higher education (Sääsjärvi et al., 2025). Since low education is associated with an increased risk of experiencing IPV (Weitzman, 2018), this type of non-response may introduce bias into survey findings on IPV experiences. Furthermore, individuals living in violent circumstances may be underrepresented in such surveys, potentially due to stigma, fear of disclosure, and concerns about personal safety (Bonevski et al., 2014; Follingstad & Rogers, 2013). To mitigate non-response bias, the survey applied weighting adjustments based on register data available for the entire sample. Specifically, inverse probability weighting methods were used to generate weights, a technique shown to be effective in correcting for non-response in the Finnish population (Härkänen et al., 2014; Koskela et al., 2023).
Conclusion
Problem gambling has been associated with an increased risk of both perpetrating and experiencing IPV. This study examined the relationship between gambling severity and self-reported experiences of physical and psychological IPV. Our findings indicate that individuals with gambling problems are significantly more likely to have experienced physical violence from a partner, and that the risk of psychological violence increases progressively with gambling severity. Notably, even those who engage in gambling at non-problematic levels showed a higher likelihood of reporting psychological IPV compared to non-gamblers. The evidence supports a comprehensive and nuanced approach to prevention and intervention. Screening for gambling problems in IPV context, and vice versa, could improve early detection and enable more effective, trauma-informed care. Tailoring these interventions to the specific needs of different gender and age groups, and addressing underlying psychological and social vulnerabilities, will enhance their effectiveness. Improving social inclusion through community support and education, addressing financial vulnerability, and continuing research into these interconnected phenomena are essential for mitigating the risks and promoting the well-being of individuals affected by both problem gambling and IPV.
Footnotes
Ethical Considerations
The study was conducted in accordance with the ethical standards of the Declaration of Helsinki. The ethics committee of the Finnish Institute for Health and Welfare approved the research protocol (THL/72/6.02.01/2022).
Consent to Participate
Potential participants were provided with written information about the study and the principles of voluntary participation. The results of the study are presented in such a way that the respondents cannot be identified on the basis of the results. Filling in the questionnaire was considered as providing consent.
Author Contributions
KL was responsible for study conception and design, data analysis, and drafting the original manuscript and tables. TG wrote the data description. KL, TG, JJ-T, TL, and SC conducted literature searches and summarized prior research. KL, TG, JJ-T, TL, and SC interpreted the results and contributed to writing. All the authors reviewed and edited the manuscript for important intellectual content and approved the final version for publication.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: the Ministry of Social Affairs and Health, Helsinki, Finland, funded the study (appropriation under section 52 of the Lotteries Act).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Data Availability Statement
The data supporting this article are not publicly available due to confidentiality concerns that could risk participant privacy. However, access to the data may be granted to collaborators upon reasonable request and under a collaboration agreement (Sääsjärvi et al., 2025).