
Abstract
While minimum standards for Domestic Abuse Perpetrator Programs (DAPP) are beginning to reflect the need for neurodiversity-affirmative provision, the intersection of neurodivergence and domestic abuse remains poorly understood, as are the implications for DAPP provision. This paper draws on semi-structured interviews with neurodivergent and neurotypical domestic abuse perpetrator program practitioners from Australia, the Netherlands, the United States and the United Kingdom who had adapted how they worked to be more inclusive of Autistic men and those with lived experience of Attention Deficit Hyperactivity Disorder (ADHD). The aims of this study are two-fold. Firstly, it explores DAPP practitioners’ understandings of neurodivergent (Autistic and ADHD) men’s violence, coercion and control towards their partners. Secondly, it details how DAPP practitioners had adapted their practice to make it more inclusive of neurodivergent men. Although a small sample, new insights were revealed about how practitioners understood the intersection of neurodivergence and domestic abuse, and how their views shaped how they work with neurodivergent men within DAPP provision. While practitioners stressed that Autism and ADHD do not cause domestic abuse, a major finding was that Autistic and/or ADHD men may exert control not only as a form of abuse, but also as a coping strategy to manage anxiety, (dys)regulation, and to provide structure in a disabling and unpredictable, neurotypical world. Other insights included the need to suspend (neurotypical) assumptions about how their neurodivergent men experience, perceive and relate to the world and the relationships they encounter within it so that they can engage them on a more meaningful level. Practitioners also offered up reflections and concerns when working with victim-survivors within integrated partner support services. Practice implications and future research are discussed.
Introduction
Domestic Abuse Perpetrator Programs (DAPPs) originated in North America approximately four decades ago, most notably within the framework of the Duluth Model. Conceived as part of a broader Coordinated Community Response, the Duluth Model positioned DAPPs as one component within a systemic approach to addressing abuse (Pence & Paymar, 1993). These programs were primarily designed to confront men’s violence, typically through curricula informed by feminist perspectives that challenge belief systems underpinning violence against women. Over time, DAPPs have been adopted internationally, evolving in their theoretical orientations and increasingly recognising the importance of tailoring interventions to the diverse communities they serve (Andrews et al., 2021; Barnes & Donovan, 2016; Satyen et al., 2022). Despite these developments, there has been limited exploration of how DAPPs might better respond to the needs of neurodivergent (e.g. men – such as those who are Autistic and/or have Attention Deficit Hyperactivity Disorder (ADHD)) – who have used violence against their partners. Furthermore, the intersection of neurodivergence and domestic abuse remains insufficiently understood, as it has historically been framed through a pathologising medical model (Renehan, 2024b).
This paper begins to address a significant gap in both conceptual understanding and empirical knowledge by drawing on the diverse experiences and perspectives of DAPP practitioners from five countries across the Global North and Southern hemispheres. It emphasises that the intersection of domestic abuse and neurodivergence, and DAPP provision, must be understood through a Neurodiversity lens. In doing so, this paper rejects pathologising narratives surrounding neurodivergence and the violence perpetrated by neurodivergent men. It also advocates for neurodiversity-affirmative provision – one that recognises and responds to the differences, strengths, and barriers many neurodivergent individuals encounter when accessing mainstream interventions not designed with their needs in mind (Chapman & Botha, 2022). It begins by contextualising the discussion with a brief overview of widely accepted principles for safe and effective DAPP interventions. It then explores why these principles must be adapted to reflect the experiences of Autistic and/or ADHD neurodivergent men. Following a description of the study’s methodology, the findings are presented across four overarching themes, capturing practitioners’ insights into key aspects of DAPP delivery. The paper concludes by introducing the concept of Coercive Structural Control, differentiating between and examining the intersection of coercive control – intended to subjugate one’s partner – and the act of controlling one’s environment (structural control) – a strategy for managing (neurodivergent) (dys)regulation. In doing so, it advances our understanding of how neurodivergence intersects with domestic abuse, and what this means for supporting neurodivergent men in addressing their use of violence in ways that are inclusive, safe and effective. Research implications and future directions are also discussed.
Core Principles for Delivering Safe and Effective DAPP
Standards establish minimum requirements to ensure that DAPPs are delivered safely and effectively. They provide guidance for practitioners and commissioners on key aspects such as the program’s theoretical orientations (based on evidence), duration, practitioner training and evaluation of outcomes. However, not all countries have developed formal program standards, and amongst those that have, there is considerable variation in governance, scope and alignment with national frameworks. For example, in England and Wales, DAPPs operating within both the voluntary and criminal justice sectors are governed and accredited by their respective umbrella organisations (see Ministry of Justice and His Majesty’s Prison and Probation Service, 2022; Respect, 2022). However, the recently published UK Home Office Standards (2023) have expanded minimum requirements to include help-seeking, early response and multi-agency case management for community-based perpetrator interventions. In Australia and the United States, individual states have developed their own program standards (see Richards et al., 2022 for a review of standards in the United States). However, in Australia, the Council of Australian Governments (2015) National Outcome Standards for Perpetrator Interventions extend beyond program delivery to include policing, child protection, corrections and community-based services. In contrast, the Netherlands does not have specific national standards governing the commissioning or implementation of DAPPs. However, the Working with Perpetrators European Network’s (WWP EN, 2023) European Standards for Perpetrator Programmes have been developed with flexibility to accommodate the legal and policy contexts of various European member states.
Despite these differences, minimum standards for DAPPs do broadly coalesce around some key principles. Victim safety (including children) is paramount. It is well established that programs that operate alongside integrated partner support for victim-survivors not only enhance safety but provide increased space for action (Kelly & Westmarland, 2015). DAPP provision should also be located within a wider coordinated community response, with referral pathways and/or combined interventions consistent with men’s additional needs (e.g. mental health, substances) that support engagement in behavioural change work (Bhavsar et al., 2023; Gadd et al., 2019; Meyer et al., 2022). DAPPs should also be based on sound evidence, though there continues to be much ambiguity about “what works” (Kelly & Westmarland, 2015). Nonetheless, what we do know is that regardless of sex, sexual orientation, gender, ethnic or racialised identities (Barnes & Donovan, 2016; Gangoli et al., 2024; Walklate et al., 2022) programs should seek to address the “foundation of seeking power and control [that] applies across all communities” (Home Office, 2023). Addressing coercive control is a core aspect of DAPPs – not least because of the fear and power imbalances it is designed to induce and exploit (Stark, 2007). Providers must, therefore, be cognisant of and be able to respond how this pattern of behaviour manifests and intersects across diverse relationships.
Practitioners must also be cognisant of the shame many men experience about what they have done, how this plays out within the (often fraught) dynamics of group-based interventions, and be attuned to the complexities of the lives of the men who present in front of them (Gadd & Jefferson, 2007; Hughes, 2024; Morran, 2011). Indeed, when practitioners are not given the time, supervision and skills needed to develop a trusting relationship with men who use violence (commonly referred to as a “therapeutic alliance”), interventions can “risk doing more harm than good” (Renehan & Gadd, 2024, p. 1175). Thus, a core principle of programs is that practitioners are highly skilled and equally well supported, for their own wellbeing as much as that of those whose lives they seek to transform (Morran, 2008; Renehan, 2021). There has, however, been little consideration of the lives and domestic abuse perpetration of Autistic and/or ADHD neurodivergent men, or how their experiences may play out within the dynamics of DAPP delivery.
Neurodiversity, Neurodivergence and Domestic Abuse
The concept of neurodiversity emerged in the 1990s from Autistic advocacy communities and has since gained global recognition (Botha et al., 2024). It challenges the dehumanising and stigmatising diagnostic lens embedded in the (bio)medical model (Botha, 2021), reframing neurological differences as natural variations in human cognition – akin to biodiversity (Singer, 2017). Rooted in the social model of disability, which shifts the focus from individual impairment to societal barriers (Oliver, 1996), the neurodiversity paradigm goes further by rejecting normative assumptions about what constitutes a typical brain (Chapman, 2020). It advocates pride in difference and calls for the empowerment and inclusion of neurodivergent individuals.
Neurodivergence refers to variations in neurocognitive processing and embodied experience that diverge from neurotypical norms (Walker, 2021). It includes, but is not limited to, Autism and ADHD, which often co-occur and intersect. Neurodivergent individuals typically have “spiky profiles” (Pearson & Rose, 2023) – marked by strengths in some areas and support needs in others such as sensory, executive function, communication and regulation. These needs fluctuate depending on context and environment. Disabling environments can lead to dysregulation, including shutdown or meltdown (e.g. fight, flight or freeze responses) triggered by sensory overload, communication barriers and masking (Corbyn & Aldred, 2025; Pearson & Rose, 2023). Such responses are often interpreted as individual disorder and deficit. However, Milton (2012) frames this as a “double empathy problem,” where mutual misunderstanding occurs between neurodivergent and neurotypical people. Despite Milton’s insights, neurodivergent people continue to navigate discriminatory systems and perceptions, often baring the burden of fitting in through (both conscious and unconscious) coping strategies designed to manage overwhelm, dysregulation and unmet needs, and to survive environments not built with their needs in mind (Pearson & Rose, 2023).
To date, research on neurodivergence and crime has been dominated by forensic psychiatry and psychology which frame neurodivergent differences as dysfunction (see Hofvander, et al., 2023). In the context of domestic abuse, these fields typically focus on the prevalence, severity, and nature of violence perpetrated by neurodivergent men compared to neurotypical counterparts (N. Buitelaar et al., 2020; Wymbs et al., 2017; Yu et al., 2019). This framing overlooks that most neurodivergent individuals are not violent towards their partners and the gendered dimensions of domestic abuse. Intervention studies similarly adopt a diagnostic lens, examining whether ADHD treatments – such as medication or psychoeducation – reduce reoffending (N. J. Buitelaar et al., 2021) while program outcomes (e.g. attrition, recidivism, program engagement) are frequently attributed to individual deficits (Romero-Martínez et al., 2023) rather than critically assessing how program design and delivery may be disabling.
In contrast, this paper adopts an affirmation model of Neurodiversity – which emerged from disability studies (Swain & French, 2000) – celebrating differences while still acknowledging personal struggles. It begins from the position that neurodivergence does not cause domestic abuse but should be understood as one aspect of a person’s intersecting identities and lived experience (Renehan, 2024b). To effectively reduce men’s violence against women, this paper argues that all aspects of DAPP provision (e.g. the therapeutic alliance, group dynamics, coercive control) must be re-examined. It begins from the premise that mainstream programs can be disabling for neurodivergent participants – who are mislabelled as challenging and non-compliant when forced to conform to curricula that ignore their learning differences and lived realities (Renehan & Fitz-Gibbon, 2022). The aim of this study is, therefore, two-fold. Firstly, it aims to explore DAPP practitioners’ understandings of neurodivergent (Autistic and ADHD) men’s violence, coercion and control towards their partners. Secondly, it aims to detail how DAPP practitioners adapted their practice to make it more inclusive of neurodivergent men.
Methodology
This paper draws on the findings from a larger study which was funded via as Economic and Social Research Council Postdoctoral Fellowship. The wider study included a systematic international literature search on DAPPs and neurodiversity, 12 semi-structured interviews with DAPP practitioners from 5 countries, and a mapping services survey distributed across the United Kingdom and Australia (Renehan & Fitz-Gibbon, 2022). Ethical approval was received by Durham and Monash Universities’ respective Research Ethics Committee (the latter for the purposes of the mapping services element) which included gaining participant informed consent (verbally recorded or written) and anonymisation. All the participants who participated in the interview component were provided with a draft of the findings, some of whom provided feedback and/or proposed edits that were incorporated into the final report prior to publication.
The current paper draws solely on the interview component of the wider study (safeguarded data is available from the UK Data Service). This included 8 single and 2 joint semi-structured interviews, 12 DAPP practitioners in total. Participants were recruited via a social media post and the author’s established networks. Practitioners with experience of delivering DAPPs that had tailored their practice to be more responsive to neurodivergent men were invited to get in touch for an interview. Participants (five male, seven female) were all white. Eight were neurotypical (NT) and three were neurodivergent (ND) (one Autistic and two ADHD), and two others volunteered that their children were neurodivergent. Participants came from five different countries, seven from the United Kingdom (England and Northern Ireland), three from Australia (NSW and Victoria), one from the Netherlands and another from the United States. As such, practitioners offered varied perspectives on cross-cultural differences within their respective frameworks (e.g. training, qualifications, multi-agency working, forensic and/criminal justice, and community-based settings).
The practitioners’ qualifications ranged from Diplomas to Doctoral level, including in Disability Studies, Child and Family Studies, Clinical Social Work, Clinical Psychology, Psychiatry, Social Sciences, Counselling and Cognitive Science. All the interview participants had professional experience providing perpetrator programs and/or therapeutic services to men who had perpetrated abuse- or domestic abuse-related stalking. Two participants specifically provided DAPP and/or counselling/psychotherapy specifically to neurodivergent people who had used violence towards their partners. One provided consultancy and training as well as delivering programs for other providers. DAPP practitioners also provided parallel sessions, support, risk assessment and management which centred victim-survivors. The referral routes across these programs consisted of court mandated men, self-referrals, or a combination of both with services either provided exclusively in remote settings and one to one, or a combination of both group work and one to one, in person and online sessions. All the practitioners had adapted their programs and/or service in some way to be more responsive to (non-learning disabled) Autistic and/or ADHD men – though mostly unilaterally within the confines of their respective organisations. Interviews were conducted and recorded on Microsoft Teams or Zoom, that lasted from 30 to 120 min, and were transcribed and anonymised at the point of transcription.
The data were analysed and coded using a reflexive thematic analysis, assisted by NVIVO software (Braun & Clarke, 2006, 2021). Reflexive thematic analysis requires that the researcher is attentive to and transparent about their own positionality in the data coding process and identification of themes. That is, it is not a value-free process but one that reflects on the researchers’ own epistemological investments, feminist or otherwise (Rutter et al., 2023). The codes and subsequent themes generated were guided by my own invested positionality, as a relational, psychoanalytically informed feminist researcher (Benjamin, 2004) – simultaneously concerned with men’s violence against women and the relational aspects of engaging them in change – and situated within the neurodiversity paradigm. During the initial coding process, the researcher identified 36 different codes which – through an iterative process of refamiliarisation, interrogating my own assumptions and informal peer review that offered up reflective questions – were reduced to four superordinate and four subordinate themes (Table 1). As an ally to the neurodivergent community, this paper was reviewed by neurodivergent colleagues to avoid harmful, stigmatising language, and epistemic injustices. Nevertheless, both neurotypical and neurodivergent participants did sometimes use medical language that, in the interests of transparency, has not been changed in their quotations.
Findings by Theme.
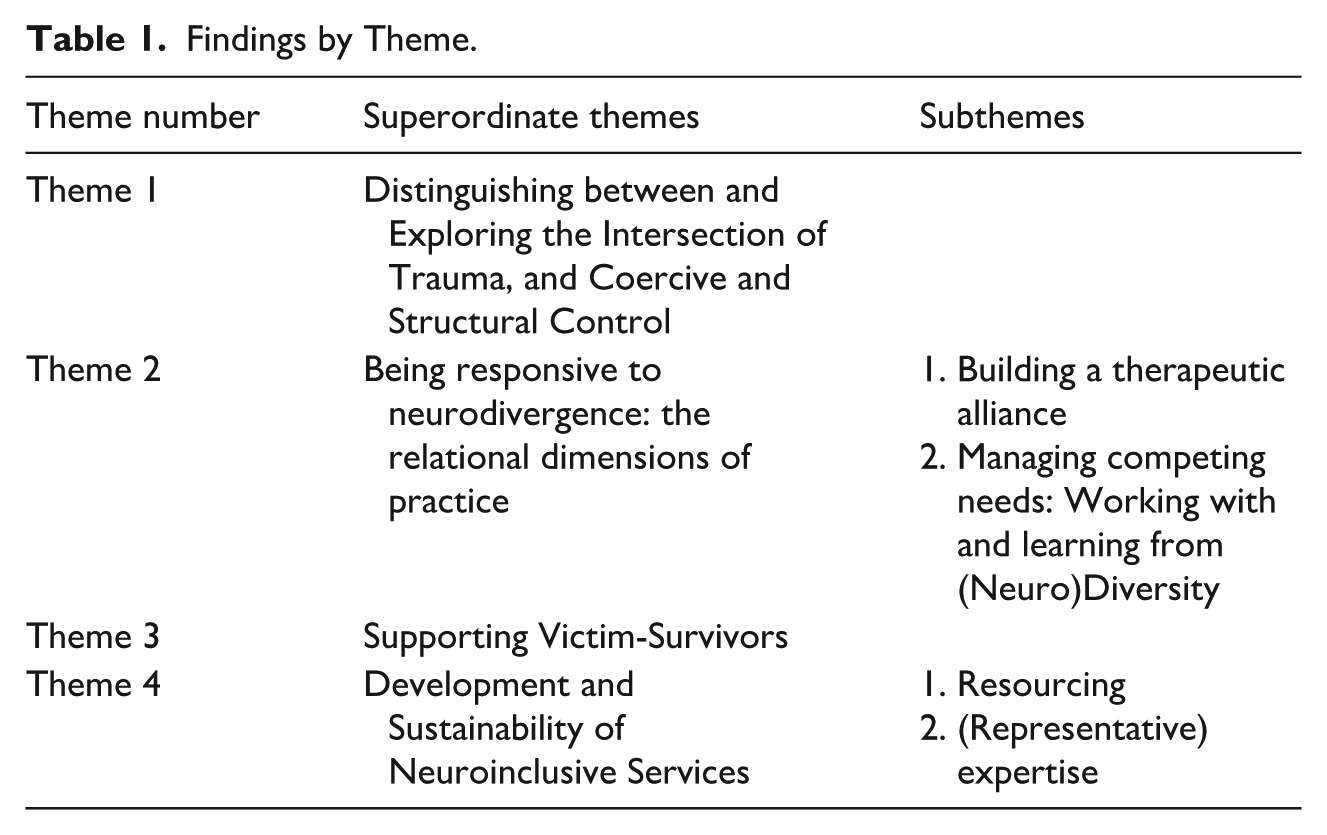
In what follows, the experiences and perspectives of DAPP practitioners are presented within the four overarching themes in Table 1. I will return to the main insights and implications for practice and research in the concluding remarks.
Findings
The first substantive theme engages with practitioners’ interpretations of neurodivergence in the context of domestic abuse, with the remaining themes drawing on practitioners’ diverse experiences and perspectives on DAPP provision and delivery, including support for victim-survivors.
Distinguishing Between and Exploring the Intersection of Trauma, and Coercive and Structural Control
In response to the interview questions posed, DAPP practitioners offered up their own interpretations of Autism and ADHD in the context of domestic abuse, specifically regarding the complexities and intersection of trauma, and coercive and structural control. All 12 were unanimous in that Autism and ADHD do not cause men to become violent towards their partners and that to suggest so was stigmatising and harmful towards neurodivergent people who “get associated with that behaviour” (ND P3, UK). There was, however, a shared understanding that being Autistic and/or ADHD shaped people’s lived experience, including of perpetration. Practitioners stated the neurodivergent men they had worked with experienced many “wounds and intersectionalities” (ND Participant 7: Victoria, Australia), including poor early care and mental health experiences, compounded by discrimination associated with being neurodivergent. As such, practitioners said it was important to be attuned to “a man’s trauma history” (NT Participant 9, UK).
There were, however, concerns that similarities in some ADHD, Autistic and trauma presentations were poorly understood amongst those who deliver programs. The implications were such that making sense of being Autistic within the context of someone’s “life trajectory” could be neglected (P6, NSW, Australia) while misunderstandings about ADHD could lead to medicalising abusive behaviours and neglecting early traumas that can lie beneath expressions of violence:
[M]y experience, most of those men there [attending DAAPs] with ADHD diagnosis, there’s also childhood neglect and trauma going on. So how much of that is a biological tendency and how much of that is the result of the childhood neglect and trauma I wouldn’t know. . . usually I think it’s probably a bit of a mix. And that’s what we’re not addressing. And I think that’s one of the problems with ADHD is that it’s sometimes used. . .as a label for dealing with some of these issues without having to really address the fact that there’s kind of trauma at the root of this. (NT Participant 1, UK)
Some practitioners stressed that a clear distinction should be made between men’s coercively controlling behaviours and the kind of control neurodivergent people exert in many aspects of their life to safely navigate a disabling world (Chapman & Bovell, 2022). Several practitioners stated that Autistic and/or ADHD men may exert control not only as a form of abuse intended to subjugate their partners (see Stark, 2007), but more distinctly as a coping strategy for managing anxiety by embedding necessary structure into their lives. Distinguishing coercive control from structural control was perceived as key to supporting neurodivergent men in identifying and addressing their abusive behaviours:
[H]ow much of that is a controlling behaviour? Knowing that someone who is on the spectrum, sometimes with ADHD, has to have a very structured, ordered, almost controlling type of behaviour to manage life in general without it spilling over and leading into full-on meltdowns, instilling behaviours. . .those are some of the challenges that we will face going forwards. (NT Participant 10:1, UK)
Practitioners’ accounts suggested a more holistic understanding of and approach to addressing men’s violence was a necessary aspect of the work they did. On the one hand, this meant helping Autistic and/or ADHD men make sense of their own identities and “neglected childhood” within a wider context of disablement and discrimination. On the other, they said it was important to hold men to account so that controlling and abusive behaviours did not get “downplayed in terms of their impact” (NT P4, UK). Therefore, it was important to help men recognise the “cut-off point” between what constituted controlling their environment and when that intention spilled over into causing harm. Dysregulation in the form Autistic “meltdowns” does not – as one Autistic practitioner pointed out – transpire into “attacking” others (ND, Participant 3, UK) nor could being neurodivergent ever be described as “causal” or a “defence” for violence and abuse (NT Participant 2, UK).
[W]e can have empathy for them. . .their hardship, for their experience, for their upbringing. . .we do not have empathy for their behaviour that they’ve chosen to use to hurt someone. And so there is a difference, and challenging the men is important. . .because we need that discomfort (ND Participant 7:2, Victoria, Australia).
This theme underscores the complexities of working with neurodivergent men who both experience and cause harm. In the following sections, practitioners’ accounts of working at this intersection are outlined, set out within the core aspects of the DAPP delivery, focusing on the relational elements of practice and adopting a neurodiversity lens.
Being Responsive to Neurodivergence: The Relational Dimensions of Practice
Program delivery matters as much – if not more – than its theoretical orientations (Hughes, 2024). This includes fostering a strong therapeutic alliance, managing diverse and competing needs, and facilitating learning that is empathetic to the mind-body diversity of participants (Corbyn & Aldred, 2025). The following two subthemes highlight what practitioners identified as key to creating inclusive environments.
Building a Therapeutic Alliance
Although therapeutic alliance is linked to sustained program engagement and improved outcomes (Dunn & Bentall, 2007; Goldsmith et al., 2015), its dynamics between neurodivergent men and practitioners – who may be neurodivergent themselves – remain underexplored. Practitioners emphasised that early identification of neurodivergent men’s needs increased “the best chance of accessing support and adaptation” (NT P4, UK); though this was complicated by the fact that many men lacked a diagnosis or awareness of their neurodivergence. For example, two practitioners noted that, if there was a known diagnosis of ADHD, medication could “really make a big difference” in “build[ing] a good relationship” and engaging men in groupwork (NT P1, UK). While medication is, of course, welcomed by some ADHD neurodivergent people, such insights must be understood within the broader context of disabling mainstream interventions (Renehan, 2024b). Building in time for curiosity, exploring neurodivergent lived experiences alongside other intersecting factors, and support needs during the assessment stage of interventions was viewed as key to developing individualised and responsive approaches:
If you’re meeting someone once, twice at the most for 20 minutes, people can you know, they’ll get missed. . .That’s. . .where I see a weakness in the programs I’ve done before. Lack of training, lack of awareness of staff, and not having time for those who might need more time. (NT P9, UK).
In building a therapeutic alliance, practitioners commonly described a delicate “balance between empathy and accountability” to build “trust, safety and rapport” while addressing harmful behaviours (NT P6, NSW, Australia). Reflecting the double empathy problem (Milton, 2012), one practitioner likened cross-neurotype communication to “having flamingos and penguins” (ND Participant 3, UK). This aligns with research showing that rapport between Autistic and non-Autistic individuals is often weaker than amongst Autistic peers (Crompton et al., 2020), suggesting potential for intersubjective breakdown (Bervoets, 2022) that can hinder the therapeutic relationship. To address this, practitioners recommended suspending assumptions about how others perceive and experience the world. Crucially, this should be a reciprocal process and not solely the labour of neurodivergent individuals. The benefits of suspending neuro-normative assumptions was summarised by one practitioner:
[I]t takes more work and effort to genuinely understand how a neurodivergent person perceives. . .how they see the world and how they experience relationships. And you have to actually park and hang up all of your perceptions and judgements and ideas about how that stuff works because they’re different to what the person in front of you might be experiencing about the world and other people. And. . .you have to listen and understand and enquire with them about what would be most helpful in managing that so that they can learn alongside their neurotypicals (NT P6, NSW, Australia).
Neurodivergent practitioners echoed this, noting that such relational work felt more intuitive. One Autistic practitioner said neurodivergent men did not need to “translate” for her, as she was attuned to their ways of relating (ND P3, UK). Drawing from her own experience of being “misunderstood,” she described how miscommunication can escalate conflict:
Autism is really alienating in terms of the communication, right? So there’s different levels of that alienation. . .I’m misunderstood a lot because the way I use words and the way I use language is different. But when I’m with a lot of clients who are coming to me, or people in the past. . .If you’re misunderstood, that leads to frustration. So I’ve seen people kick off, not at me but at other people because they’re [like] “That’s not what I said!” It was what they said but it’s not what they meant. (ND P 3 UK).
Two neurodivergent practitioners further advocated for a “whole diversity lens,” integrating “neurodiversity,” “cultural diversity,” and sexual orientation (ND P7:1, Victoria, Australia), suggesting that an intersectional approach would suspend all biased assumptions to create services that reflect people’s multiple, overlapping identities.
Managing Competing Needs: Working With and Learning From (Neuro)Diversity
Most practitioners interviewed worked with mixed neurotype groups and emphasised the importance of attuning to diverse and competing needs to create inclusive learning environments. There was broad agreement that how programs were delivered mattered more than what was delivered, to accommodate different “way[s] of learning” (NT Participant 10, UK). This, in their view, required skilled facilitators who understood how to adapt “whatever [theoretical] model” was being used and to “deliver it effectively” (ND Participant, P7: Victoria, Australia). One practitioner stressed the importance of how facilitators “hold [their] space,” suggesting practitioners need to be aware of how their own presence can be (dys)regulating. They highlighted the need to monitor group members’ “body language” for signs of disengagement, such as distraction or “dozing off.” Another expressed concern that even with neurodiversity training, many facilitators lacked the ability to “provide and adapt that piece [of information] in the moment” (NT P8, US) to meet varied learning needs and strengths. One practitioner summarised this challenge:
[W]e’ve got that lens all the time. . .[W]e actually adjust on the fly, recognising, picking up; but that means that each facilitator or pair of facilitators is actually dealing with it differently, based of their experiences. . .Because of my experience, being neurodivergent, I can flip and my own personal way of doing things, so it means that we’re not necessarily having a way of supporting all, it’s very much who’s there, how they respond to who’s working with them (ND P7:1, Victoria, Australia)
Their colleague echoed this, describing how lived experience and practice informed a flexible, moment-to-moment approach that avoided assumptions about neurodivergent people:
[I]n terms of reflective practice and debriefing, we are trying to discuss [with other practitioners] what we’re picking up on and what we’re noticing with our co-facilitator. But. . .I don’t think I know a clear way of how I would teach someone to pick up on these things. Like I can talk about. . .picking up on cues and body language and different ways of adjusting your style of working and different examples or modes of delivery and all of that. But. . .it’s not a one-size, you can’t just pick one way of working [or] say. . .this will suit this cohort. . .or. . .another, we’re having to do it on a needs basis, or as we come across these people. (ND P7:2, Victoria, Australia).
While some practitioners felt neurodivergent individuals might benefit more from individual work due to differences in learning pace, communication and sensory processing, there was consensus that mixed neurotype groups – with appropriate adaptations – could benefit all. This, however, depended on having highly skilled facilitators. Neurodivergent participants could offer valuable insights, as one practitioner explained:
It’s such a burden and a gift, I think, for neurodivergent people because they actually often don’t realise, like they think they’re being a nuisance or disrupting a process or whatever, or certainly sometimes that’s the feedback that they get if people are defensive and not open to their contributions. But if people are open to their contributions, what they bring is an opportunity for people to think differently about things that have been thought about in the same way for an incredibly long time, and I love that. I feel like that is, you know, that’s where change happens, when people have an opportunity to think differently about something, it presents an opportunity. And I really enjoy and value how neurodivergent clients can do that. (NT P6, NSW, Australia).
Facilitators, practitioners said, also need to be attuned to the emotional dynamics involved in DAPPs and should avoid expecting neurodivergent clients to simply “fit in” with mainstream programs (NT P8, The Netherlands). This included understanding and responding to hyper/hypo sensitivities to emotional content, embodied reactions and coping strategies for those “feeling incredibly anxious” (NT P6, NSW, Australia). Given the emotional intensity of such programs, identifying, understanding and supporting neurodivergent peoples’ embodied experiences were viewed as essential for effective facilitation of mixed neurotype groups.
Supporting Victim-Survivors
Another substantive theme was consideration for victim-survivors, including integrated support and wider responses. Victim safety is central to any domestic abuse perpetrator intervention (Home Office, 2023). Several practitioners highlighted that there was added complexity when the victim-survivor’s partner was neurodivergent, noting several implications for integrated support services. One practitioner asserted that “when you have an Autistic perpetrator in your hands then actually it’s about their [victim-survivor] acceptance of what changes can be made” (NT P10:1, UK). Drawing distinctions between coercive behaviours and neurodivergent presentations, another practitioner similarly highlighted that ADHD-related behaviours such as to “postpone” or “forget things” could be misinterpreted by partners, taken “personally” or perceived as a “criticism” (NT P5, The Netherlands). Thus, several practitioners expressed that practitioners delivering integrated partner support should help victim-survivors to understand what DAPPs can realistically achieve. As one practitioner explained:
I think psychoeducation is very important, and it’s very important that the partner understands it as well, so there are no expectations which the patients [sic] cannot fulfil. Because. . .a lot of problems with couples, in which one is Autistic, it’s about this: that the partner wants a lot of things, and the other one is not able to respond. (NT P5, The Netherlands)
Other practitioners interviewed, however, were concerned and put a “question mark” over who should deliver psychoeducation to partners, given limited understanding of how neurodivergence intersects with domestic abuse (NT P10:2, UK). They stressed that working with partners in cross-neurotype relationships required skills equal to those used with neurodivergent men. Without this expertise, there was a concern that integrated partner support could be “more detrimental for the survivor” by “feeding into any assumptions about minimisation, denial and blame” and “where the cause of the behaviour lies”:
I can very easily see how talking about somebody’s diagnosis or presentation could actually really encourage survivors to further remove the accountability and the blame for where that behaviour is coming from the perpetrator. That may encourage people to stay in relationships whereas otherwise they wouldn’t necessarily have done. Or to make excuses or to continue to blame themselves for triggering behaviours, because actually it’s not their fault, it’s their diagnosis. (NT P10:2).
In this context, it was emphasised that no single agency holds all necessary expertise, and there was a shared vision that emerged around multi-agency cooperation and collaboration. In other words, a coordinated community response (NT P10:2, UK). This included working in tandem with sectors with expertise, or providing co-located/integrated services that could combine expertise in working with those who harm, victim-survivors and advocacy with neurodivergent people. One practitioner noted a UK initiative that made a “big difference” by offering one-to-one case management for high-risk, repeat offenders with complex needs which included (at times) reaching out to “specialist” services (NT P1, UK), though they stressed that such communication was not routine. Practitioners working within co-located and/or integrated services advocated for “phased” or individualised interventions (e.g. therapy, addiction support, diagnosis pathways, domestic abuse and post-separation stalking interventions) alongside psychoeducation about neurodivergence, recognising the interrelated nature of these issues (NT P2, UK ;NT P4, UK; NT P5, The Netherlands). One practitioner also stressed the importance of children’s services remaining involved throughout the intervention, rather than closing cases once the person causing harm was referred to behavioural change (NT P10:2, UK).
Development and Sustainability of Neuroinclusive Services
The final theme highlights the need for high-quality, neurodiversity-informed services amidst a climate of precarious funding.
Resourcing
Practitioners noted that delivering DAPPs was increasingly difficult due to limited funding, with resources described as “scant” (NT P9, UK). Justifying neurodiversity-affirmative provision required evidence, but “poor data” made it hard to argue for resources and capacity in competitive funding environments (NT P2, UK). One practitioner working exclusively with neurodivergent men explained the challenge of defending higher service fees compared to “traditional mental health and behaviour agencies” (NT P8, US). Their commitment to best practice often meant waiving fees:
It’s very complicated too because we’ll get phone [calls] and say, “Why are you so expensive? I could just send them to so-and-so, you know, and they’re half your cost,” which is an exaggeration, but, “They’re half your cost,” and our response is, “Well, that’s not best practice, is it?” Right? To send them to a provider without the speciality just because they’re a lower fee’d agency. And so it is – it’s difficult at times because there’s also barriers above us in other systems saying, “You need to keep your budget down. . .” (NT P8, US)
UK practitioners echoed concerns about time and costs, especially when working with some neurodivergent men whose progress through programs could be slower due to differences in learning and processing needs:
[I]t takes time. And so my challenge will be speaking to my manager, you know, all the time is, “why is this taking a long time?”. . . it is going to be part of a service question, “why is it this person isn’t shifting through the programme as quickly as we’d want to?” And that may be something that’s spoken about higher up in meetings when we’re going for things like funding. We know why because these people take time to develop those skills. And actually, we have to go over things quite a lot of the time to make sure that one, I’ve understood that they actually know where we’re coming from, and that actually we are making that difference. (NT P10:1, UK).
Despite a “growing emphasis on perpetrator programs,” practitioners stressed that the domestic abuse sector struggled to attract professionals into “incredibly skilled and incredibly intensive roles” due to chronic underfunding:
And I don’t think that the payment for that is commensurate with what is needed. And I think unless there’s really some movement on that, it poses a risk. (NT P10:2, UK).
This underscores the importance of not only what and how interventions are delivered, but who delivers them and takes us to the final subtheme.
(Representative) Expertise
Working with men who use violence was seen as highly skilled work. Practitioners expressed concern that staff often lacked adequate training to “engage with troubled and difficult clients who are causing harm,” let alone more “specialised stuff” around neurodiversity (NT P1, UK). One noted that UK criminal justice programs were often delivered by “trainee forensic psychologists or assistants,” which they felt was insufficient for working with neurodivergent men:
[T]his group is often quite complicated. You know, we discovered. . . in terms of their, their thinking, their needs, but also how it all sort of fits together. So I think the skill to be able to cope with that, and then in a dynamic group, is a huge challenge. (NT P4, UK).
Practitioners called for sector-wide training on neurodivergence, including “awareness,” “myth busting” and reflection on personal biases (NT P2, UK). One emphasised the importance of treating men as “human beings” with “respect” and “dignity” (ND P3, UK). Another stressed that attunement and relational connection were more important than technical knowledge:
I think [what] is much more important and underemphasised, if you like, in this work or in any work with humans, is use of self and attunement. Sounds really simple, but I think that’s it. I think that everything that we do, whatever skills and knowledge that we have, if we cannot manage ourselves and use ourselves in a way that is deeply attuned to the person and their experience then it doesn’t matter. You can’t take knowledge and apply it to a person if you can’t connect with them. (NT P6, NSW, Australia).
A final point is the value of recruiting neurodivergent practitioners to ensure representation and relatability, with one practitioner stating intention to create a “level playing field” (NT P9, UK). Neurodivergent practitioners relayed how they could connect with clients without needing to “translate” (ND P3, UK), offering unique insights into delivery. One practitioner described their value as being able to think outside of normative constraints:
[W]e can’t just have a one-size fits all, but it’s the importance of embedding a mindset of diversity. . . our experience of being neurodivergent. . . lets us think outside the square. . . it’s not just a black and white situation. . . our spirit and nature. . . is helping drive that change in other peoples’ philosophies. (ND P7:1, Victoria, Australia)
This quote underscores the value in exploring more inclusive recruitment strategies that encourage neurodivergent people to enter the domestic abuse sector, as they may be able to contribute lived experience skills that are not so easy to teach or learn and will be invaluable when working with neurodiverse groups (Renehan, 2024a).
Conclusions and Implications: Towards Neuro-Affirmative Provision?
While calls for neurodiversity-affirmative provision with minimum standards are emerging, research remains limited on the intersection of neurodivergence, domestic abuse and the safe, effective delivery of DAPPs. This paper sought to start that conversation, by addressing a significant gap in conceptual and empirical understanding, drawing on the diverse experiences of 12 DAPP practitioners from Australia, England, Northern Ireland, the Netherlands and the United States. It explored how practitioners understand neurodivergence in the context of domestic abuse and how this shaped their practice.
Practitioners unanimously rejected the notion that being Autistic and/or ADHD causes domestic abuse, warning that such claims risk further stigmatising neurodivergent communities. They emphasised a holistic understanding of violence used by neurodivergent men, considering childhood trauma, lifelong discrimination and adherence to harmful gender norms. Anxiety, and how it is defended against, may manifest in complex ways (Renehan, 2024b). Practitioners explained that many Autistic and/or ADHD men may exert control not only abusively but also as a coping strategy to manage anxiety, (dys)regulation and to impose structure in a neurotypical world. These accounts align with those from neurodivergent men who have used violence and coercion (Renehan, 2024b), and from non-abusive neurodivergent individuals in respect of navigating disabling environments (Chapman & Bovell, 2022).
It is at this juncture, however, that neurodivergence can overlap with coercive control. Practitioners distinguished coercive control – a pattern of domination involving isolation, degradation, exploitation and control (Stark, 2007) – from structural control, which helps neurodivergent individuals manage their environment (Pearson & Rose, 2023). However, structural control may become coercive in relationships with existing unequal power dynamics; coercive structural control extends male privileges through expectations that partners and children adapt to accommodate the needs of the person using violence.
This has clear implications for practice. Work with neurodivergent men must centre victim-survivors while recognising neurodivergent men’s fluctuating support needs. Practitioners should seek to understand their coping strategies and their impact on others, support recognition of coercive structural control, and help them to develop non-abusive coping mechanisms so that they can continue to navigate a disabling world. Neuro-affirmative provision must also adopt an Embodied Double Empathy framework that acknowledges the mind-body interaction (Corbyn & Aldred, 2025). This means shifting from deficit-based views to inclusive approaches within interventions that value the diversity of mind-body and cognition and embodied experiences. As practitioners pointed out, suspending assumptions and fostering empathy can strengthen therapeutic alliances, provide opportunities for learning “outside of the square” and create safe spaces for men to explore, acknowledge and address the harm they have caused.
Implications also extend to work with victim-survivors, revealing tensions in practitioners’ accounts. Some practitioners noted that survivors may hold neuro-normative expectations of intimacy, reciprocity or communication, or misinterpret neurodivergent presentations as personal failings that might be resolved within DAPPs. Two practitioners suggested psychoeducation for survivors, while others cautioned that, if mishandled, this could wrongly suggest coercive structural control is inherent in neurodivergence. This is not the case. However, women living under the coercion of a partner who uses abusive behaviour are harmed regardless of the underlying motive – be it male privilege, structural, mental health or substance use. Living with a neurodivergent man can further limit a women’s autonomy – adjusting routines, declining social invitations and restructuring the home to manage their partner’s dysregulation. Integrated partner support must clearly communicate that coercive structural control still constitutes abuse, upholds perpetrator accountability and avoids explanations that inadvertently risk placing blame on victim-survivors that may encourage them to remain in abusive relationships out of duty or care.
Neurodivergent-led training is, therefore, crucial to ensuring – as practitioners pointed out – this work moves beyond a “fad.” Further, DAPPs are part of a wider system, and better collaboration and cooperation will be needed with specialist services – neurodivergent-led advocacy, women’s services, mental health – to create safe, appropriate pathways of support for neurodivergent men, women and children. Moving forward, DAPPs should be co-designed in collaboration with neurodivergent people and informed by neurodivergent DAPP practitioners, whose insights are vital when working with neurodiverse groups. However, further research is needed to understand how neurodivergent DAPP practitioners experience their working environments and how employers can support neuroinclusive workplace cultures (Renehan, 2024a). While all of this, of course, must be considered within a climate of increasingly precarity and scarcity of resources, it is incumbent upon providers, commissioners and policy makers to serve a neurodiverse population of clients.
Limitations
This study is limited by interview number and representativeness. While it included diverse neurotypes, future research should engage practitioners of varied identities (e.g. ethnic and racially minoritised communities). Further research should also consider neurodiversity, domestic abuse and DAPP provision from the perspective of neurodivergent men with diverse intersecting identities, including those from Aboriginal communities. Crucially, victim-survivors’ voices were not included, representing a major gap. Future research should explore how abuse and service provision are experienced in both within- and cross-neurotype relationships, how integrated support services understand these intersections and how they can offer neurodiversity-affirmative provision that ensures safety for women and children survivors. Nevertheless, this paper offers an important starting point in a conversation about the intersection of neurodivergence, domestic abuse and developing neuroinclusive DAPPs from the perspectives of those from the North and Southern Hemisphere.
Footnotes
Acknowledgements
The author would like to thank the people who gave of their time to participate in this study, and to the authors’ Postdoctoral mentor, Prof Nicole Westmarland. The author would also like to thank Kay Aldred and Dr Amy Pearson, Dr James Rowlands, Dr Nikki Rutter and anonymous reviewers for their critical feedback. The responsibility for the argument and the accuracy and interpretation of the data lies with the author alone.
Ethical Considerations
The submitted paper for review draws on the findings from a larger study which was funded via the Economic Social and Research Council. The wider study included a systematic international literature search on Domestic Abuse Perpetrator Programs (DAPPs) and neurodiversity, semi-structured interviews with international DAPP practitioners, and a mapping services survey distributed across the United Kingdom and Australia. Ethical approval was received by Durham (United Kingdom) and Monash (Australia) Universities’ respective Research Ethics Committee (the latter for the purposes of the mapping services element).
Consent to Participate
The current paper includes only the interview component of the study. All the participants were provided with a participation information sheet, and they provided informed consent (verbally recorded or written format), inclusive of permission for published outputs and extended quotes to be used within these. All the transcripts were anonymised at the point of transcription.
Funding
The author disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by Economic Social and Research Council, Postdoctoral Fellowship [project reference ES/W005379/1].
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the authorship and/or publication of this article.