
Abstract
Although a small body of research has convincingly established the occurrence of dissociative violence, we continue to have little understanding of the forms or types of dissociative experiences identified and the context in which they occur. With this research gap in mind, we used reflexive thematic analysis of interview transcripts to understand participants’ accounts of their physical violence use toward partners, family members, friends, and associates while experiencing dissociative symptoms. Participants were 17 men and women completing community-based family violence perpetrator treatment programs or prison-based high-intensity treatment programs for violent offending. Three overarching themes and two subthemes were generated. The first theme, “Becoming overwhelmed by emotions” described participants’ experiences of intensely unpleasant emotions immediately prior to entering a dissociative state. The second theme, “Transitioning between states” was split into two subthemes (“Disconnection” and “Reconnection”) that described participants’ experiences of disconnecting from and then reconnecting to their usual way of experiencing themselves and the world around them during the violent event. The final theme, “Going to the extreme” described the extreme nature—both objectively and subjectively—of participants’ physical violence while experiencing dissociative symptoms. Taken together, our findings highlight the potential importance of taking into account dissociative phenomena as contributors to violent behavior in adult survivors of childhood trauma, and in the assessment and treatment of violent offending.
Introduction
From Robert Louis Stevenson’s The Strange Case of Dr Jekyll and Mr Hyde to Philip Zimbardo’s Stanford Prison Experiment, accounts—real or otherwise—of shocking acts of violence perpetrated by “normal” people have long fascinated the general public (Moskowitz, 2004). Perhaps of less public interest, yet of equal importance, are violent acts perpetrated by characteristically violent people that even they themselves struggle to understand. While magic potions, unspoken desires, and social conformity may help to explain the former, there is growing evidence that dissociative experiences may offer one plausible explanation for the latter (Moskowitz & Evans, 2009). In this article, we aimed to identify and analyze experiences of enacting physical violence in an apparent dissociative state, as reported by male and female perpetrators of criminal violence.
Dissociation is a controversial concept associated with a variety of ongoing scientific debates (van der Hart & Dorahy, 2022). It is defined in the DSM-5-TR as the “disruption of and/or discontinuity in the normal integration of consciousness, memory, identity, emotion, perception, body representation, motor control, and behavior” (p. 329, American Psychiatric Association, 2022). The DSM-5-TR includes five dissociative disorders that feature “positive” (e.g., depersonalization, derealization) and “negative” (e.g., amnesia) symptoms.
The concept of dissociation first emerged in the late 1800s and was again thrust into the spotlight during the 1980s when researchers began to examine responses to trauma experienced by war veterans and survivors of childhood abuse (Carlisle, 1991). So, dissociation has been etiologically linked to trauma since its earliest conceptualizations. However, dissociation is also regarded as a relatively normal experience, and there is a lack of clarity as to whether normal and pathological dissociation are distinct constructs or sit best on a continuum (Dalenberg et al., 2022).
In relation to those who perpetrate violence, dissociation has typically been viewed through a trauma response lens. It is widely recognized that those who perpetrate violence are also likely to have experienced traumatic events; often, some combination of childhood physical, sexual, and emotional abuse and neglect (Hohfeler, 2022; Nesi et al., 2020; Ternes et al., 2020). Childhood trauma exposure can indirectly contribute to adult violence perpetration through the development of maladaptive coping strategies (e.g., substance abuse), emotion regulation difficulties, and changes in social information processing (e.g., hostile attribution biases, beliefs and attitudes supportive of violence; Nesi et al., 2020; Webermann & Murphy, 2019). Some of these chronic coping strategies are now recognized as dynamic risk factors for crime and violence, and are the focus of interventions to reduce ongoing criminal involvement in adults (Fritzon et al., 2021; Polaschek, 2024).
Dissociation—another common post-traumatic symptom, and the focus of this research—has also been correlated with adult violence perpetration (Krause-Utz et al., 2023; LaMotte & Murphy, 2017; Simoneti et al., 2000; Webermann & Murphy, 2019). Dissociative violence refers to violence that occurs in association with some form of dissociative experience. Manifestations of dissociative violence can be retrospectively identified in descriptions of violent offending from earlier studies (Dutton et al., 1982; Tanay, 1969). More recent research has found that childhood exposure to trauma predicted dissociative violence toward partners, with a substantial minority of participants—22% to 36%—reporting having experienced dissociative symptoms while perpetrating violence (LaMotte & Murphy, 2017; Simoneti et al., 2000; Webermann & Murphy, 2019). Amnesia—the most commonly researched and reported dissociative symptom in relation to violence perpetration—has been reported in between 20% and 87% of violent events involving homicide, and appears to be associated with unplanned violence and high levels of emotional arousal (Moskowitz, 2004). Previous research has also found an association between violence-specific dissociation and violence severity (Mantakos, 2008; Simoneti et al., 2000), including in relation to dissociative amnesia (Porter et al., 2001). Anecdotal accounts from researchers examining gang-related violence in a prison setting (Brennan-Tupara et al., 2025), as well as our own clinical experiences of completing offending-focused assessment and treatment with incarcerated clients, suggest that dissociative violence is not limited to family contexts and may be enacted toward rival gang members, strangers, and friends or associates. Although it has been theorized that dissociation is particularly relevant to reactive violence events, one study found that the statistical association between the type of violence and peritraumatic dissociation was stronger for instrumental than reactive violence (Ternes et al., 2020).
As described above, a small body of research has strongly suggested the occurrence of dissociative violence. But as Thompson-Hollands et al. (2021) noted, there is a need for researchers to “invest effort into more basic studies” of peritraumatic dissociation (p. 670). More specific to our research, qualitative studies are now needed to better understand both the forms or types of dissociative experiences identified and the context in which they occur (LaMotte & Murphy, 2017; Webermann & Murphy, 2019). This research is important for at least three reasons: (a) to contribute event-related information to the ongoing debate about distinguishing which phenomena meet definitions for dissociation versus other states of consciousness, (b) to provide relevant evidence given the concerns about whether phenomena that might indicate dissociation might also be forms of malingering or denial, and (c) to determine whether dissociative violence may have potential treatment relevance. Therefore, the aim of the current study was to explore experiences of dissociative violence—including the intrapersonal, interpersonal, and situational circumstances in which it occurs, the nature of the violence perpetrated, and people’s understanding of their violence use within this context—in a sample of people who typically have high rates of childhood abuse victimization and relatively extensive experiences of violence perpetration.
Method
Participants
Twelve men and five women provided violent event narratives that were included in this study. At the time of their involvement in the research, participants were completing either a community-based family violence perpetrator treatment program for men or women (n = 6), or a prison-based high-intensity treatment program for men with extensive histories of violent offending and considered to be at high risk of future crime, including violence (n = 11). Community-based participants were completing the treatment program on either a self-referred (n = 4) or court-mandated (n = 2) basis. Prison-based participants were at various stages of program completion ranging from pre-program preparation to post-program maintenance. Participants ranged in age from 22 to 51 years (M = 32.82, SD = 8.34), and identified as New Zealand Māori (29%), Pasifika (12%), New Zealand European (24%), or as having multiple ethnicities (35%; e.g., New Zealand Māori/European).
Procedure
Participants were recruited by the first author between June 2017 and December 2022 into one of two independent research projects. In both projects, treatment providers initially informed potential participants of the research opportunity and invited them to attend a group information session with the author at their treatment site. Participants who remained interested in taking part in the research at the conclusion of the group information session were then invited to meet individually with the first author to further discuss the research, after which they gave formal written consent to take part.
Eight participants were part of a larger sample recruited for the first research project between June 2017 and May 2019. Participants were either completing a community-based family violence program or a prison-based violence program and were recruited based on their perpetration of family violence. In that project, participants provided a detailed description of a specific event in which they had perpetrated violence toward one or more family members (Stairmand et al., 2020a, 2020b; Stairmand et al., 2019). Of these participants, eight described experiencing one or more characteristic features of dissociation (e.g., depersonalization, derealization, or amnesia; American Psychiatric Association, 2022) while perpetrating violence during the event, and these interviews were retained for further analysis here. Given the conceptual overlap between emotion dysregulation and dissociation, interview transcripts that did not contain sufficient information to reliably distinguish between the two concepts were excluded (e.g., transcripts in which participants described experiences that could either represent emotion dysregulation or dissociation—such as emotional detachment or perceived loss of control of their behavior while experiencing heightened emotions—in the absence of other potential dissociative features; Bruno et al., 2025; Garofalo et al., 2022).
In the second project, between November and December 2022, 18 potential participants first completed the Peritraumatic Dissociative Experiences Questionnaire (PDEQ; Marmar et al., 1997) using their history of physical violence perpetration as a frame of reference. Five were excluded from the research project after completing the PDEQ, including one participant who did not endorse any PDEQ items and attended the individual meeting to “see what the research was about.” Another four endorsed at least one PDEQ item but were screened out after initial discussions revealed that the item(s) they had endorsed could be better attributed to experiences other than dissociation (e.g., alcohol-induced blackouts, enduring and non-specific memory difficulties as a result of a prior traumatic brain injury, an inability to take others’ perspectives). Consistent with the selection of interview transcripts from the first research project, potential participants were excluded if they only endorsed PDEQ item(s) that may represent emotion dysregulation in the absence of other dissociative symptoms. The remaining nine participants were invited to the interview phase, in which they were asked to describe in detail a specific violent event in which they had perpetrated physical violence while experiencing dissociative symptoms. The method used in this study required participants to have at least partial recall of the violent event so that they could describe it, but no potential participants were excluded on this basis (i.e., due to reporting they had no memory at all of the relevant violent event). Participants’ PDEQ item responses—suggesting that they had experienced dissociative symptoms while using physical violence—were used as interview prompts to assess the presence of dissociative symptoms in relation to the specific event described (e.g., “You circled that your sense of time sometimes changed when you used violence—did that happen in the event you are telling me about?”).
In both studies, semi-structured interviews were used to better understand participants’ experiences of the violent event that they described. All interviews were audio-recorded and transcribed for later analysis. Interviews ranged in length from 28 to 120 min (M = 67 min).
Measures
Peritraumatic Dissociative Experiences Questionnaire
The PDEQ (Marmar et al., 1997) was used as a screening measure and interview prompt for the second research project and was completed by potential participants prior to their commencing a semi-structured interview. The PDEQ is a 10-item self-report scale that measures the presence of a range of dissociative symptoms during traumatic events. It is a widely used measure of peritraumatic dissociation—including in a prison setting—and has adequate psychometric properties as demonstrated across a number of studies (Marmar et al., 2004; Marshall et al., 2002; Wainipitapong et al., 2025). Consistent with the intention to use the PDEQ as a screening measure, participants were asked to consider their entire history of physical violence perpetration when answering PDEQ items. Accordingly, the PDEQ Likert scale was modified from measuring the degree to which a dissociative symptom was present during a particular event (ranging from 1 = Not at all true to 5 = Extremely true) to the frequency with which participants had experienced each symptom across their history of violent behavior (ranging from 1 = Never to 5 = Always). In light of Marshall et al.’s (2002) consideration that PDEQ items may vary in how relevant and easy to understand they are (depending, e.g., on socioeconomic and ethnic backgrounds), care was taken to explain each item to participants and provide relevant examples as required, before they selected their responses. Participants endorsed an average of 8.33 out of 10 PDEQ items and typically reported that they had experienced each symptom “Sometimes” or “Very often.”
Data Analysis
Interview data were qualitatively analyzed using reflexive thematic analysis (Braun & Clarke, 2006, 2019, 2022). Reflexive thematic analysis was chosen because its flexible approach to generating rich and novel accounts of the data was a good fit with the aims of the research (Braun & Clarke, 2006, 2022). Consistent with this approach, data analysis was conducted solely by the first author. As such, it was important to consider the ways in which the author’s existing knowledge, experiences, and values influenced data collection and analysis. The first author is a registered clinical psychologist working in the prison system, has prior research experience in the family violence field, and has a professional interest in providing a trauma-informed approach to the assessment and treatment of criminal behavior. Furthermore, the author had already undertaken a separate grounded theory analysis of the first eight interviews (as part of a larger data set) for a prior research project. These aspects provided both benefits (e.g., access to participants, existing knowledge) and challenges (e.g., coding the data with “fresh eyes”), alongside underlying assumptions (e.g., that participants could provide valuable insight into their behavior) that shaped data collection and analysis.
The first author reviewed the accuracy of interview transcripts before reading and re-reading the entire data set. Each transcript was then systematically coded in Microsoft Word, with the author returning to earlier transcripts as required to add and modify codes. This iterative process was repeated over three rounds of coding. Ongoing review and refinement resulted in the initial list of 245 codes being condensed to 42 codes. Tentative code names were then printed out, reviewed alongside collated codes and interview transcripts, and physically grouped to form a thematic map. Five initial themes were eventually generated. With ongoing development, review, and refinement, these initial themes were collapsed into three overarching themes and two subthemes. The author moved recursively and flexibly through each stage of data analysis, writing and reviewing reflexive journal entries throughout the analytic process. The second author reviewed the draft analyses during later rounds of coding, offering feedback and reflective questions for consideration.
As an example of the analytic process, the earliest version of Theme 1 (“Becoming overwhelmed by emotions”) was labeled “Emotional overload” and contained revised codes such as “Current context activates trauma memory,” “Overwhelming unpleasant emotion immediately prior to violence use,” and “Perceived transgression by victim”. This theme was later labeled “Moving towards violence” with subthemes relating to existing tension in the participant-victim relationship (“Tension”) and the specific interaction and related emotional impact that had immediately preceded participants’ dissociative violence (“Trigger”). Reflective processes during analysis supported the realization that “Tension” was a general feature of interpersonal violence, rather than directly relevant to the specific instance of dissociative violence, and this subtheme was ultimately discarded. Further review and refinement of the remaining codes resulted in the final theme being generated.
Results
Characteristics of Event Narratives
For the event-based analysis, participants collectively described 19 events in which they experienced dissociative symptoms while using physical violence toward a partner (n = 8), family member (e.g., child or parent; n = 4), or friend or acquaintance (e.g., rival gang member, police officer, fellow prisoner; n = 10). Three events involved multiple victims. Fifteen participants described one event, and two participants described a second event. Five events involved participants’ reported use of a weapon (e.g., a glass or bottle, knife, metal pole, gun) and three resulted in the victim’s death.
Themes From Event Narrative Analysis
The three overarching themes and two subthemes were: “Becoming overwhelmed by emotions,” “Transitioning between states” (“Disconnection” and “Reconnection”), and “Going to the extreme” (see Figure 1). Each theme and subtheme will be discussed in turn. Participant quotes are labeled with the letter “P” or “T” according to whether they were recruited for the first (“P”) or second (“T”) research project.
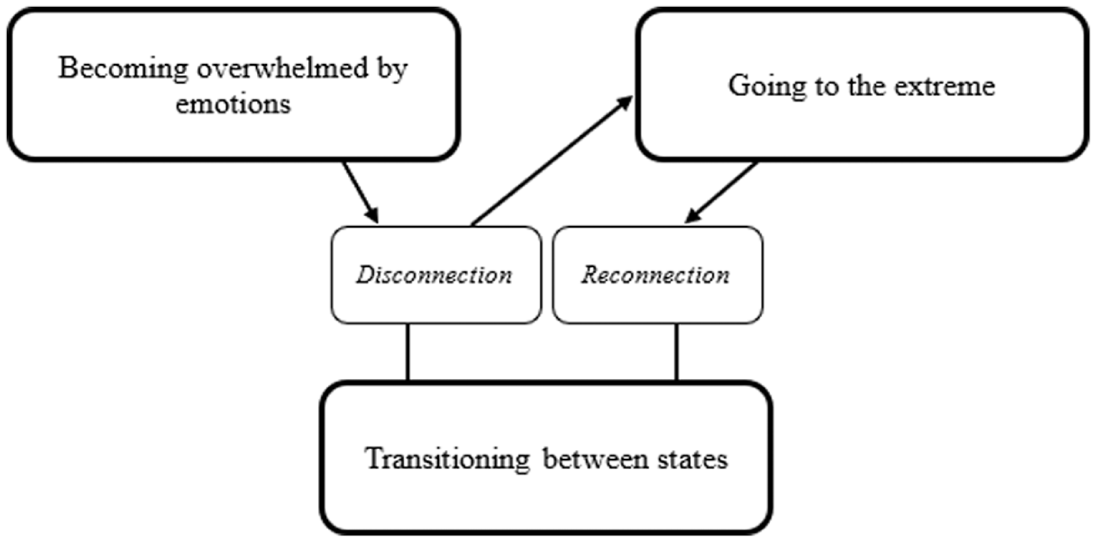
Themes and subthemes.
Theme 1: Becoming Overwhelmed by Emotions
The first theme focuses on participants’ experiences of feeling overwhelmed by intense emotions immediately prior to the onset of dissociative symptoms (see “Disconnection” in Theme 2). Participants typically reported experiencing anger and rage, but also described other unpleasant and painful emotions such as hurt, betrayal, and fear. Feelings of anger were often directed toward the victim and accompanied by a strong desire to inflict harm toward them. Some participants considered that the intensity of their emotions was unlike anything they had experienced before.
The whole world just crashed on my face you know just smacked me in the face you know, and again I’d gone back to being hurt again you know and then oh, well if I’m hurt you’re gonna hurt. (P2) I just felt so enraged like the, a rage inside it was, painful. It was so painful inside raw . . . I felt sick in my stomach and I had like a burning feeling in my chest and my hands were shaking. Like I was having anxiety. And I could feel my face red, like a fire engine red . . . I wanted to kill [victim]. I wanted to kill him. (P6) I just, I hadn’t felt this anger before. [Interviewer: “Ever, in your life?”] Nah, nah. Even like having fights with rival gang members. It was like a hot flush just came over my whole body and, everything around me went red. (P31) I freaked out. It was like everything all at once. [Interviewer: “What do you mean everything all at once?”] Feeling scared, angry, hurt, like all the emotions. (T6)
Regardless of the particular emotion experienced, participants typically linked this to a specific action by or interaction with the victim that constituted some form of perceived threat (e.g., physical, relational). This perceived threat is usually linked to participants’ trauma histories. Some participants described becoming overwhelmed by emotions after directly experiencing or hearing about abuse perpetrated by the victim that mirrored their own prior experiences of victimization. For example, one participant who had been sexually abused as a child recalled being sexually propositioned by the victim, and another reported being threatened by a fellow inmate, which he likened to bullying he had experienced as a child. Other participants described the potential or actual severing of an important attachment relationship (e.g., due to an unwanted relationship separation or death) that mirrored similar experiences of relationship separation or loss during childhood. For example, one participant who experienced forced separation from a key attachment figure during childhood reported discovering that his partner—the victim—had cheated on him. Another participant, who had witnessed the deaths of multiple key attachment figures during childhood, observed the victims shoot and kill a fellow gang member whom he considered to be his closest friend. Some participants explicitly linked their trauma histories with the accounts they gave of actions by or their interactions with the victim during the event described. On other occasions, this link was inferred by the coder during data analysis based on additional information provided by the participant (e.g., the participant likening the emotional experience to that felt during a prior traumatic event; the participant disclosing prior victimization in a separate part of the interview that they had not consciously linked—but contained obvious similarities to—the event described). Where inferences have been made, relevant information from the interview transcript is provided in square brackets alongside the quote.
I walked into [friend’s] room to find her in bed with my partner at the time [the victim] . . . I pulled back the blankets and they were both naked and my son was in the middle [the participant went on to disclose being sexually abused as a child]. (P6) [Victim] was just getting you know pushy and mentally abusive . . . I just got angry, like I just remember [prior abuser] being like that. (P13) ‘cause [victim, who had sexually propositioned the participant earlier in the evening] was up now, standing up again and he was like bigger . . . then he went “You little c**t” and he come forward . . . but [victim] looks the same as [prior abuser], the same size as [prior abuser] compared to me, yeah. Sort of, I don’t know. I feel like it was about to be that, [co-offender and I] were about to be victimized. (T3) [Son] came home and told me that he’d been threatened, to be killed . . . threats upon my family, especially children, young children, after experiencing violence as a young adult myself, I thought no one threatens my children. (T11)
Theme 2: Transitioning Between States
This theme captures participants’ experiences of a marked and often sudden shift in the way that they experienced themselves and the world around them during the event. Two states of transition were described—a disconnection from, and then subsequent reconnection to, their usual way of experiencing themselves and the world.
Disconnection
Immediately after becoming overwhelmed by emotions (see Theme 1 above) and prior to their use of physical violence (see Theme 3: Going to the extreme), participants reported the onset of a range of symptoms consistent with the hallmark features of dissociation (American Psychiatric Association, 2022). These included positive symptoms such as emotional and physical detachment, sensory distortions, and observing themselves from a third-person perspective.
At the beginning I was terrified and then there was it was like nothing, and then my hearing left me. (P21) I don’t remember feeling any restriction. No weight, nothing. Just weightless . . . You just can’t feel nothing you just feel, it’s just a hollow feeling. It’s almost robotic. (T4) It felt like I was just like floating up the driveway ready to go to kick [victim] in the head . . . I was looking at him and then next minute he was right in front of me. (T1) Everything just went really slow, like everything else was slow . . . I felt like I was moving quicker than everything else in the room. (T3) It sort of felt like, I dunno, it sounds weird saying it but like I felt like I was looking at myself do it, but it wasn’t me. (P31) I started to feel a bit f***ed up, a bit out of it. That’s when I guess the dream, like separating of myself stuff kind of happened . . . Starting to feel like a different person, like a different side of me was involved in my decisions and stuff . . . it didn’t feel like me, [violence] didn’t feel hard, I looked at my bro and I didn’t even recognize my bro who was with me. (T8) I didn’t really feel anything, I sort of felt like numb I suppose . . . It sort of felt, sort of felt like it, yeah like it hadn’t happened like, yeah, like it, like it wasn’t me that experienced it. But I knew what had happened. Yeah but I couldn’t feel anything. (T9)
Negative symptoms, such as memory blackouts and feeling as if they had no control over their actions, were also reported by participants.
I don’t even remember [violence]. And I have to take [victim’s] word for it, what he’s described through that situation is what I had to believe. (T4) My mind just went totally blank. Everything went blank and I was swinging my arms everywhere, I wasn’t aiming for any specific part of the body I was just flying. (P6)
Participants’ sense of being disconnected from their usual way of experiencing themselves and the world was evident in their conceptualization of these symptoms as “weird,” “confusing,” and difficult to explain.
It was a surreal feeling, very odd . . . I still think about it to this day, and I still quiz myself. And I’m, I’m still puzzled. (P21) Geez, that was quite real strange, it was like real strange. (P30) I don’t know it just, I can’t explain this experience I had . . . I honestly can’t put a like finger on the pulse of it or even explain the lead up to it. (P31) Academically I could see, like what thoughts sort of led to me, to what happened, and. But at the same time, it’s like, it’s just, I don’t know . . . it’s real f***ing confusing. I have been in heaps of fights throughout my life and that felt like, way different. (T8)
Reconnection
As clearly as participants were able to pinpoint their transition to a disconnected state, they were also able to identify the point at which they reconnected with their more usual way of experiencing themselves and the world. This point coincided with the cessation of their violence use. Some participants described a sudden and spontaneous shift in awareness during their violence perpetration; for example, abruptly realizing that the victim was seriously injured, or becoming aware that their child(ren) were watching the violence.
And then all I saw was blood. And I saw his mouth first then I looked at his face and that was it boom . . . it was the blood that got me . . . that’s when everything just stopped . . . it was like a moment of, oh how can I describe it? I awoke. (P7) And then I sort of clicked in, I’m standing there in my underpants, “What the f**k am I doing?”. (T4)
Other participants attributed their return to “reality” to physical intervention by a third party.
My co-offender was pulling me, he pulled me, it felt like he pulled me out of the movie . . . he pulled me out and I realized what I had just done. (T3) Then [fellow gang members] come and smashed me onto the ground. On the ground, like on my stomach and they were all on top of me and I was trying to get up and they were yelling. They were yelling at me but I don’t really know what they were yelling out at the start. But then I, what I heard was that the bro’s dying and we have to help him . . . I couldn’t hear what they were saying. Then I just heard those words and they weren’t yelled, but those were the words that I picked up. And then from there, everything is really clear. (T9) My wife grabbed me and she goes “That’s enough. You’re going to kill [victim], stop” . . . that’s what brought all my focus back. Cause my focus was back to, cause it’s not just anybody telling me to stop. It’s a person in my life that I love . . . because it was my wife, and because she grabbed me too. And that’s the whole thing, like people can yell and scream and all that sort of thing from a distance and it probably wouldn’t have made a difference but because she made contact with me, you know it sort of made me, I stopped . . . if I didn’t get stopped he would have been dead. (T11)
Theme 3: Going to the Extreme
The third and final theme describes the extreme nature of participants’ violence. As we noted earlier, nearly all participants described perpetrating severe physical violence that resulted in the victim’s significant injury or death. While this sometimes involved only one act of violence (e.g., kicking the victim in the head with full force; severing the victim’s hand at the wrist with a knife), it typically involved repetitive violent acts that continued for a few minutes. Several participants did not recall some or all of their physical violence and later filled in their accounts from others’ (e.g., the victim’s) recollection of the event.
I just physically just lost the plot and smashed both of them. And I mean physically smashed them up, like, threw them to the walls, threw them down the stairs, strangled them both till they turned purple . . . till they were not breathing no more. (P2) I really brutally attacked him . . . I was just letting him have it . . . I was punching him I was I was choking him. (P6) I kicked him in the head . . . he just fell back, boom. And he went to sleep. (T1) [I] sliced his face. And hit his arm that had the knife and the knife that he was carrying went straight through his stomach and out his back . . . I kicked him over on to his back. And he was bleeding everywhere . . . And I grabbed the pipe and I started caving his head in. (T11) I ended up choking him, just about killed him . . . I ended up gouging his eye. (T13)
Some participants—including those with significant histories of interpersonal violence—reported that the violence they had perpetrated while in a dissociative state was significantly more severe than any violence they had previously committed. Most participants had no particular plan prior to beginning to act violently; their behavior might traditionally be labeled “reactive.” But even participants who had explicitly planned to use some form of physical violence in retaliation for a perceived transgression by the victim often went on to perpetrate more severe violence than they had initially intended to after experiencing dissociative symptoms. In these instances, an unanticipated action by or interaction with the victim (e.g., being sexually propositioned, being assaulted) or an internal reliving of a prior traumatic experience during the event elicited intense emotions (see Theme 1: Becoming overwhelmed by emotions) and a resulting change in trajectory of the planned violence.
I’ve never experienced that before, not that type of anger, not that type of violence where it was, done so, like, ugly anyway . . . I had done violence in the past, but that was like on a different scale, it was, I think the best thing it was like a mad man . . . even [victim] says to me “I haven’t seen you like that before. Yup I have gotten hidings from you but to see you, how I seen you on that day, that was the first day I was really, like actually scared of you.” (P31) I went way further than I’d initially intended to. (T6) There was never any intention to cause any murder . . . I’ve been in those situations before where I’ve beaten someone up and taken their stuff [planned violence] and it’s like it’s not, it was never a murder. It was never that fucked up. (T8)
The severity of their violence perpetration left a lasting impression on some participants. A few participants described a heightened sense of power regarding their newfound ability to defend themselves, but more often they expressed shock at what they now understood about their capabilities for unexpected extreme violence.
And it still scares me to this day that I was able to do, do that. I do wonder about myself, I wonder, f**k am I capable of doing such a thing again you know blanking out, getting so cross and blanking out and doing something like that again. (P21) I can’t get that out of my head, that I just snapped . . . I don’t wanna ever experience that feeling again. (P31) After we beat up the victim I like felt a way lot bigger, ever since then if people try to pick on me or do anything to me I’ll step back to them real quickly, because I felt like oh I’m not little as, he’s not going to beat up some little yeah you know. (T3) Having that told to me what I’d done without knowing that I’d done it was really confronting . . . that’s taken years for me to, accept what I had done. (T6)
Discussion
The aim of the current study was to explore participants’ experiences of dissociative violence, including the intrapersonal, interpersonal, and situational circumstances in which it occurs, the nature of the violence perpetrated, and how participants viewed and understood their violence use in this context (i.e., when in an apparent dissociative state). The PDEQ (Marmar et al., 1997) was used as a screening measure in the second research project and was completed by nine participants. Participants reported having experienced most of the questionnaire’s symptoms while perpetrating violence, suggesting that more investigation is warranted regarding the relevance of these symptoms in assessing and treating risk for violence in correctional and forensic settings.
Event-Related Themes
Our analysis of the event narratives resulted in three themes—“Becoming overwhelmed by emotions,” “Transitioning between states,” and “Going to the extreme”—which we discuss in turn. The first theme (“Becoming overwhelmed by emotions”) relates to participants’ extreme emotions immediately prior to entering a dissociative state, and in this regard represents events and experiences leading to dissociative violence. A variety of immediately proximate events triggered these emotions, and the sequence was usually reported as if it went rapidly from event to emotion to dissociation to violence. While some of the triggering events (e.g., seeing a friend killed, walking in on a partner and child in bed with another woman) might trigger extreme emotions in almost anyone, these events were often overtly recognized as paralleling childhood experiences such as being sexually propositioned, bullied, witnessing the death of a loved one, or being exposed to third-party accounts of victimization. Some participants reported that the intensity of their emotions was unlike anything they had experienced before. More generally, these results are consistent with the notion that high levels of emotional arousal may precipitate dissociative states during violent events, with dissociation functioning as a coping strategy to manage the arousal and related perceived threat (LaMotte & Murphy, 2017; Moskowitz, 2004). Memory gaps during the most emotionally arousing parts of a violent event have been termed “red-outs” (Swihart et al., 1999). This apparent relationship to prior traumatic events may distinguish other patterns of reactive violence from dissociative violence. Reactive violence, by definition, typically occurs in response to events and their interpretations that trigger strong arousal, alongside high levels of negative affect and increased violence severity (Kroner & Butler, 2020; Tapscott et al., 2012). It seems plausible that experiencing dissociative symptoms that are connected to prior trauma accounts for some incidents of reactive violence (see “Theme 2: Transitioning Between States”). However, within frequent users of violence, reactive violence often doesn’t feature dissociation and is not directly connected to prior traumatic events. And although dissociative violence has typically been considered within the context of reactive violence, prior research has found that dissociative symptoms can be experienced during the perpetration of instrumental violence (Ternes et al., 2020). As identified in Theme 3: Going to the extreme, some participants reported dissociative violence in events that began as proactive (i.e., instrumental) and then became reactive as the event unfolded. The heterogeneity we found highlights the need for violence constructs and theories that account for the dynamic nature of violent events within and across people (see e.g., Stairmand, Polaschek & Dixon, 2020).
In Theme 2, “Transitioning between states,” most participants described some form of awareness of the onset of dissociative symptoms. All participants reported experiencing multiple and varying dissociative symptoms, highlighting the complex and multifaceted nature of dissociation. Prior research (Sierra et al., 2005; Simeon et al., 2008) identified five dimensions of depersonalization/derealization—numbing (physical and emotional), unreality of self (detachment from thoughts, feelings, body, and actions), perceptual alterations (sensory distortion), unreality of surroundings (derealization), and temporal disintegration (disturbance in experience of time)—which were all evident in participants’ accounts. Consistent with prior research (Evans & Mezey, 2007), participants who reported experiencing amnesia reported only partial amnesia for the violent event, alongside other dissociative symptoms.
The “Reconnection” subtheme, in which participants reported an abrupt return to their usual way of experiencing the world, is consistent with prior research exploring people’s experiences of dissociative symptoms while using violence from both perpetrator and victim perspectives. In their study of patterns of intimate partner violence perpetrated by traumatized war veterans, Finley et al. (2010) reported a victim’s observation of their partner’s sudden dawning of awareness during their violence perpetration. Similar experiences have also been reported from the perspectives of those perpetrating the violence. In a qualitative analysis of the meaning of distressing intrusive memories for violent events perpetrated by study participants, participants’ sudden realization of the severity of injury caused was identified as a key theme (Evans & Mezey, 2007). Our finding that reconnection could occur either apparently spontaneously or in response to others intervening has not been described in previous research and would warrant further investigation, especially from the perspective of bystanders or victims to establish if it is a meaningful difference and on what basis bystander intervention may be effective.
The final theme, “Going to the extreme,” referred to participants’ behavior rather than their emotions. The extreme nature of their physical violence was consistent with prior research demonstrating an association between violence-specific dissociation and violence severity (Mantakos, 2008; Simoneti et al., 2000). Whereas the sequence of events from trigger to extreme emotion to dissociation to violence was typically described as rapid, the violence phase itself was often reported as quite prolonged, and whether short or prolonged, was perceived as more extreme than was typical of participants’ previous violence. Participants’ conceptualization of their dissociative violence as being qualitatively different to other violence they had perpetrated is consistent with aspects of Polaschek et al.’s (2009) grounded theory research on implicit theories for violent offending. Specifically, those authors identified two commonly endorsed implicit theories (“Beat or be beaten,” “I am the law”) that were linked to one another through the background assumption that violence was normal, as well as a relatively infrequent and conceptually unrelated implicit theory (“I get out of control”) in which the violence discussed was considered to be abnormal in some way. While the authors attributed “I get out of control” to deficits in self-regulation, participant quotes and descriptions of the violence included in the manuscript (e.g., being consumed by larger forces, intending to carry out a minor act of violence but then becoming engrossed and committing much more severe acts: “All of a sudden I go on a rage,” “I really lost it”) are consistent with our participants’ experiences of dissociative violence.
The few participants whose post-event appraisal was positive described the newfound sense of power that this provided, both in relation to the event described and the possibility of deterring or preventing future victimization. These participants may have been recognizing in others’ responses to their dissociative violence the value of extreme “random” violence. Acting “crazy” or “badass” toward others through apparently random acts of extreme violence is recognized in masculine street culture as a valuable source of protection from the predation of others, and can enhance future violent crime enactment (Brookman et al., 2011). Similarly, establishing one’s reputation through a single act of extreme violence in prison has also been described as valuable in avoiding victimization in prison (e.g., “beat or be beaten” implicit theory for participants in prison; Polaschek et al., 2009). Positive accounts suggested that participants might use their new experience of what they were capable of, and how others reacted to their dissociative violence, to facilitate proactive extreme aggression in the future without dissociation necessarily being “required.” However, most participants expressed shock, fear, or concern at what they were capable of, consistent with reflecting on an episode of behavior in which they essentially felt they had little or no agency. This was consistent with previous research by Evans and Mezey (2007) investigating intrusive memories for violent offending among young incarcerated men, in which “shock or disbelief that they had acted so violently” (p. 106) was identified as a main theme. It is also consistent with growing research that people who use violence may experience their own violence as traumatic (Badenes-Ribera et al., 2021). Unsurprisingly, participants’ negative evaluations primarily occurred for events in which they inflicted violence that caused death, or toward victims who they were in a close relationship with (e.g., a partner or child). This is consistent with prior research findings that participants were more likely to experience trauma symptoms when perpetrating violence toward a family member or friend versus an acquaintance or stranger (Ternes et al., 2020).
Nearly half of the events reported involved non-family members as victims, even though the first project primarily recruited from a family violence organization; a result that supported clinical experience. These findings confirm the importance of not limiting research to intimate partner violence in examining the role of dissociative violence. Intimate partner violence may be particularly important for two reasons. First, there may be higher potential for adult attachment figures (e.g., partners) to trigger dissociative violence, given the complex intertwining of trauma responses with attachment for adults who were extensively abused in childhood by their main caregivers. Second, relationship-based dissociative violence may create much more harm given its potential severity and that it may occur in a private setting and on multiple occasions. But as our research shows, dissociation may be associated with a variety of triggering events outside the immediate family environment, so considering this form of dissociative violence will also be important for future theory, research, and practice.
Implications for Assessment and Treatment of Violent Offending
The findings of this research have multiple implications for the assessment and treatment of violent offending. First and foremost, participants’ use of dissociative violence, including the clear parallels between the context in which this occurs and participants’ prior victimization history (see Theme 1: Becoming overwhelmed by emotions), strongly signals the need to consider screening for Post Traumatic Stress Disorder (PTSD) and to potentially provide trauma-focused treatment either prior to or alongside offense-focused treatment. Peritraumatic dissociation symptoms have been generally found to reduce with treatment for people with PTSD (Thompson-Hollands et al., 2021) and in addition to improving wellbeing more generally, reductions may improve control or amelioration of future violence (Fritzon et al., 2021)—although a significant amount of future research would be needed before such claims could be made with confidence.
Regarding offending-focused treatment, the nature of dissociative symptoms experienced by participants—including memory blanks, perceived loss of control of their actions, and emotional and physical disconnection (see the “Disconnection” subtheme of Theme 2: Transitioning between states)—may pose a barrier to both meaningfully engaging in treatment tasks (e.g., developing an offense map) and applying skills taught in treatment in the moment (LaMotte & Murphy, 2017). As such, when dissociative violence is part of the person’s violence perpetration history, the focus of treatment may need to broaden or shift to understanding and managing proximal factors that contribute to dissociative states (e.g., recognizing early warning signs and high-risk situations related to dissociative symptoms) in which violence is likely to occur (Gold & Seibel, 2009; LaMotte & Murphy, 2017). In this research, most participants had perpetrated multiple other violent offenses, and so a more typical treatment approach could still be taken with other violence patterns. Relating to both Themes 1 and 2, common treatment targets for violent offending such as the ability to self-regulate and to attend to or connect with the internal and external world (e.g., through mindfulness and grounding) may be particularly salient skills for people who experience dissociative violence (Gold & Seibel, 2009).
The lasting negative impact of participants’ dissociative violence and the unpleasant emotions that may be part of that impact (see Theme 3: Going to the extreme) may provide additional barriers to discussing their offending behavior and engaging in the necessary self-reflection to promote behavioral change (Gold & Seibel, 2009; Ternes et al., 2020). This desire to avoid such discussions may be particularly evident in a non-therapeutic assessment context (e.g., case management, probation supervision), especially when the context in which dissociative violence occurs is linked to a person’s trauma history. Given that participants often found it difficult to make sense of their experiences of dissociative violence, psychoeducation will likely be required to help people normalize and make sense of their experiences before seeking more complete disclosures.
Pertaining to risk assessment, given that the current and prior research (LaMotte & Murphy, 2017; Simoneti et al., 2000; Webermann & Murphy, 2019) suggests that dissociative violence is a relatively common experience among those who offend violently, dissociative violence should be routinely screened for in an assessment context (Moskowitz, 2004). Uncharacteristic and particularly severe violence—including violence that involves elements of planning—may be a potential flag that dissociative violence has occurred. Consideration should also be given as to how dissociative symptoms may relate to commonly assessed risk factors for violence and related areas of treatment need. For example, emotional detachment, memory blackouts, and an inability to make sense of dissociative violence may be considered to reflect a lack of empathy, offense-supportive thinking styles such as denial and minimization, and a lack of insight respectively. That said, we are not aware of any research that currently informs whether a history of dissociative violence has implications for assessments of the level of future violence risk.
Limitations and Directions for Future Research
There are several limitations of this research. First, we relied solely on participants’ retrospective accounts of violent events in which they had experienced dissociative symptoms. There is a general concern—both in research and in practice—regarding the potential for those who use violence to intentionally (e.g., lie or manipulate) or unintentionally (e.g., view through the lens of offense-supportive beliefs, forget over time) provide a distorted account of their own violence (Moskowitz, 2004; Polaschek et al., 2009). Dissociative violence can look like the person is avoiding responsibility or crediting their violence to forces outside their control; similar to when they credit alcohol or drug use with being the main reason for their offending. Although this is a possibility in the current study, it is also possible that participants accurately and genuinely reported their experiences (Moskowitz, 2004). In general, once they have been convicted and sentenced, people in prison are likely to be seen in a more positive light if they report that they are “taking responsibility” for their offending. They will be more likely to successfully complete rehabilitative programs and will be viewed more positively by parole boards if they talk about their previous offending as something they can take control of. Our prison-based participants were completing an offending-focused group treatment program that necessarily involved taking responsibility for and critically examining their violent behavior; both generally (e.g., by recognizing and challenging offense-supportive thinking) and in relation to specific violent events (e.g., through creating and sharing offense maps). Many had perpetrated multiple other violent offenses, and did not attempt to present the majority of these as dissociative. And in prison environments, trauma histories can go unacknowledged and personal vulnerabilities are often preyed upon, creating other disincentives for not reporting dissociative symptoms even when they do occur (Hohfeler, 2022). In other words, it is not obvious what participants gained from intentionally fabricating the descriptions they gave.
Second, the relatively small sample size prevented us from looking at potential differences in participants’ experiences of the context in which dissociative violence occurred, where theory and research suggest that these may exist (e.g., family vs. general violence, violence perpetrated by men vs. women).
Third, while most participants described only one episode of dissociative violence, this and other research (LaMotte & Murphy, 2017) suggest that experiences of dissociative violence may not be isolated to one event. As such, it may be useful to understand whether these experiences are similar for each participant across violent events. For example, participants were asked to describe only one episode of dissociative violence, and so may have selected an event that was particularly salient in some way (e.g., because of the emotional impact or “extreme” nature of their violence; see Theme 3). Whilst dissociative experiences are abnormal by definition, participants’ accounts may not have captured their more “typical” experiences of dissociative violence, both in relation to the nature of violence used and the context in which this occurs.
Fourth, we also have limited information due to sample size on more common or rare types of dissociative symptoms experienced, and how often they are experienced without resulting in violence for a given individual. Acknowledging these limitations, the current research provides initial and long-awaited insight into the experiences of dissociative violence in people who are relatively experienced users of violence and who were taking part in psychological treatment based on their violent behavior. The findings echo the need to better understand and account for this phenomenon in how we understand causes of violence in adult survivors of childhood trauma, especially in the process of assessing and treating violent offending.
Footnotes
Acknowledgements
The authors thank Nicky Perkins for her enthusiasm and support for this research.
Ethical Considerations
This research was approved by the University of Waikato Human Research Ethics Committee (HREC[Health]2022#07).
Consent to Participate
All participants provided written informed consent prior to participating.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by funding from the New Zealand College of Clinical Psychologists.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.