
Abstract
Men’s poor mental health is increasingly recognised as a causal factor for their perpetration of intimate partner violence (IPV); however, the majority of studies are from high-income countries and cross-sectional. We conducted a secondary analysis of data collected as part of a randomised controlled trial, among young (ages 18–30 years) men, living in urban informal settlements in eThekwini Municipality, South Africa, to assess whether: (a) changes in depression symptoms, and (b) changes in post-traumatic stress (PTS) symptoms, were prospectively associated with IPV perpetration, after 2-years of follow-up. Among N = 505 men retained at endline, for depressive symptoms in adjusted models, men with consistently high symptoms (adjusted Odds Ratio [aOR] = 2.02, p = .002) and those with increasing symptoms (aOR = 2.80, p < .001) between the two time points were significantly more likely to report IPV perpetration at endline. Similarly, for PTS symptoms, those whose symptoms increased between the two time points were significantly more likely to perpetrate IPV (aOR = 1.95, p = .05). However, neither decrease in depressive symptoms nor in PTS symptoms between the two time points was associated with a significant reduction in IPV perpetration. This analysis suggests that interventions to reduce IPV perpetration should include a focus on preventing the onset of symptoms of poor mental health. It may be that alcohol is also intervening in this relationship, and this requires further research. The original clinical trial was pre-registered at clinicaltrials.gov (NCT03022370: https://clinicaltrials.gov/study/NCT03022370).
Background
Intimate partner violence (IPV) remains a pressing global health concern, with an estimated 27% of women experiencing physical and/or sexual IPV in their lifetime (Sardinha et al., 2022). Experience of IPV has a significant negative health effect on women, including worsened mental health and sexually transmitted infections (Sardinha et al., 2022). The prevalence of IPV is patterned by a range of factors, including background levels of poverty and informality in living conditions (Gibbs, Dunkle, et al., 2020). Studies globally (Weimann & Oni, 2019) and in Nigeria (Okedare et al., 2025), and from an analysis from 34 countries, drawing on Demographic Health Surveillance (DHS) surveys, have found particularly high rates of IPV in urban informal settlements (Chen et al., 2025), driven by overlapping factors of poverty, social disorganisation, lack of policing and gender inequitable norms (Chen et al., 2025; Gibbs, Dunkle, et al., 2020).
Poor mental health is also a major concern globally, including for men. In South Africa, the South African Stress and Health (SASH) survey found a lifetime prevalence of 9.8% for depressive disorders, 15.8% for any anxiety disorder, and 2.3% for post-traumatic stress disorder (PTSD; Herman et al., 2009), although these were higher for women than for men (Herman et al., 2009). Research in urban informal settlements has described high rates of poor mental health, including for young men (Gibbs et al., 2018), shaped by the informality and stress of living in often violent and insecure locations (Zerbo et al., 2020).
More widely, there is also a lack of mental health treatment, with estimates suggesting that the treatment gap for mental health may be as high as 76% to 90% for serious disorders in Low- and Middle-Income Country (LMIC) settings (Patel et al., 2010). Specifically in South Africa, an estimated 75% of people with poor mental health had not sought treatment (Seedat et al., 2009). While in eThekwini Municipality, South Africa, where this study is set, it was estimated that there were 0.98 psychologists per 100,000 population (Siyothula, 2019).
There is increasing recognition that there are several pathways from men’s poor mental health to their perpetration of IPV, although there are concerns about stigmatising men with poor mental health as inherently violent (Oram et al., 2022). It may be that symptoms of poor mental health, such as impulsivity and anger, are key paths through which IPV occurs (Oram et al., 2022). In addition, research suggests that poor mental health impacts negatively on relationship dynamics, relationship quality, and resolution of conflicts, all recognised as risk factors for shaping IPV perpetration (Braithwaite & Holt-Lunstad, 2017; Stern, 2024). Finally, adversity in childhood is a significant risk factor for both poor mental health and IPV perpetration, and it may be that there is no causal relationship between the two (Oram et al., 2022), but rather they share the same risk factors.
There is growing evidence describing how poor mental health is associated with men’s increased likelihood of perpetrating IPV, although most of this is cross-sectional and from high-income settings. A review, in 2014, of the relationship between people with clinically diagnosed poor mental health and their perpetration of IPV, identified 17 studies and found depression, anxiety, and panic disorders were all associated with increased male perpetration of IPV (Oram et al., 2014). However, as the authors recognise, only 2 (of the 17) studies were from LMICs (South Africa and Ukraine), and all were cross-sectional (Oram et al., 2014). Similarly, a more recent systematic review on the relationship between poor mental health and physical IPV perpetration identified 207 studies, of which 16 were from LMICs, and only 7 were prospective analyses (Spencer et al., 2019). This review found that depression, anxiety, PTSD, antisocial personality disorders (PD), and borderline PD were all associated with male IPV perpetration (Spencer et al., 2019). Moreover, many of these analyses did not adequately control for potential confounders – risk factors that might cause both IPV and poor mental health – particularly adverse childhood experiences, but also education level, and age (Oram et al., 2022).
There are studies that have described the relationship between poor mental health and men’s perpetration of IPV cross-sectionally in LMIC settings. For instance, in a multi-country study from Asia-Pacific, Fulu and colleagues found that depression was a risk factor for physical and/or sexual IPV perpetration (Fulu et al., 2013). Similarly, in South Africa, depression has been associated with IPV perpetration (Machisa et al., 2016). There has been less research on the association between PTSD and IPV perpetration in LIMC settings, although one analysis of three studies from two countries (South Africa had two studies, and Ghana one) found that among men with probable PTSD, the likelihood of recent perpetration of physical IPV was significantly increased (Ramsoomar et al., 2023).
To address the limited longitudinal research on poor mental health as a risk factor for IPV perpetration by men, particularly in LIMC settings, we conducted a post-hoc analysis of men involved in the Stepping Stones and Creating Futures (SSCF) intervention trial in urban informal settlements in eThekwini Municipality, South Africa (Gibbs, Washington, et al., 2020). The main trial assessed whether a gender transformative and livelihood-strengthening intervention could reduce men’s perpetration of IPV and strengthen livelihoods (Gibbs, Washington, et al., 2020). The SSCF intervention did not specifically address young people’s poor mental health, though it was assumed that strengthening livelihoods and transforming gender norms would positively impact on mental health. Depressive symptoms were a specified secondary outcome in the trial, but were not significantly reduced 24 months after the baseline (Gibbs, Washington, et al., 2020). While post-traumatic stress (PTS) symptoms were measured in the study, but not pre-specified in the analysis, though there was an indication that men’s PTS symptoms were significantly reduced due to the intervention (Oyekunle et al., 2023). In this analysis, we first assess whether changes in depressive symptoms between baseline and endline were associated with IPV perpetration at endline. Second, we sought to assess whether changes in PTS symptoms between baseline and endline were associated with IPV perpetration at endline.
Methods
Study Setting and Design
This is a secondary analysis of data collected for the evaluation of an IPV prevention intervention through a cluster randomised controlled trial (Gibbs, Washington, et al., 2020). The intervention evaluated was the SSCF intervention, a 21-session, participatory intervention that sought to reduce men’s perpetration of IPV through addressing gender norms and strengthening livelihoods, and also indirectly impact positively on mental health (Gibbs, Washington, et al., 2020). Women were included in the main trial – and were not men’s intimate partner – and results for the trial and similar analyses on mental health as a risk factor for IPV experience for women are reported elsewhere (Gibbs, Washington, et al., 2020; Gibbs et al., 2023). The trial was implemented in urban informal settlements in eThekwini Municipality, KwaZulu-Natal Province, South Africa, with 34 clusters recruited, and details are provided elsewhere (Gibbs, Washington, et al., 2020).
Participant recruitment eligibility criteria were: aged 18 to 30 years old at the point of recruitment, not currently in formal education or full-time employment, able to communicate in English, isiZulu, or isiXhosa, and able and willing to provide informed consent, as well as residing in selected communities. Prior to completion of the survey, participants provided written informed consent. At baseline and endline, participants self-completed questionnaires on an app loaded onto a cellphone briefly lent to them by the study team. This enabled skip, range, and logic checks. At endline, participants also had audio-assist for completion, and in both cases, there were trained fieldwork staff nearby if participants required help. Baseline data were collected from September 2015 to 2016, and approximately 24 months later, we traced participants and readministered the survey. Full study details have been previously published (Gibbs, Washington, et al., 2020).
Ethics Approval
Ethical approval was provided for the study by the South African Medical Research Council’s Human Research Ethics Committee and the Biomedical Research Ethics Committee at the University of KwaZulu-Natal. Participants provided written informed consent for the study.
Measures
Men’s mental health was assessed through scales focused on depressive symptoms and PTS. Depressive symptoms were assessed using the Center For Epidemiologic Studies Depression Scale (CES-D), which comprises of 20 items assessing symptoms experienced in the past week for example ‘During the past week I was bothered by things that usually don’t bother me’, with responses: ‘rarely or none of the time’, ‘some or a little of the time 1–2 days’, ‘moderate amount of time 3–4 days’ or ‘most or all of the time 5–7 days’. Responses were summed (range 0–40) with higher scores indicative of more depressive symptoms. The scale showed good reliability at baseline and endline (Cronbach α = .87 baseline, = .87 endline). To identify participants with potentially clinically relevant symptoms of depression, we coded those scoring 21 or more as potentially depressed (Radloff, 1977).
PTS symptoms were assessed using the Harvard Trauma Questionnaire, which comprises 16 items assessing symptoms about trauma responses in the past week (e.g. restless, recurrent nightmares; Mollica et al., 1992). Responses are on a four-point scale: ‘not at all’, ‘a little’, ‘quite a bit’ and ‘a lot’, with scores 1 to 4. A mean score for the scale is created (range 1–4) with higher scores indicative of more symptoms (Cronbach α = .92 baseline, = .91 endline). To classify participants as having potentially clinically relevant symptoms of PTS, we recoded those with mean scores ≥2.5 as potentially having PTS disorder (Mollica et al., 1992). Throughout, we refer to depressive symptoms, or potentially clinically relevant symptoms of depression, and similarly for PTS, reflecting that these cannot be formally diagnosed using screening tools such as CES-D and the Harvard Trauma Questionnaire, but rather need a formal diagnosis by a doctor/clinical psychologist.
We assessed men’s perpetration of physical and/or sexual IPV using eight items drawn from the UN Multi-Country Survey on violence against women (Fulu et al., 2013). Five items assessed past year physical IPV (e.g. slapped, hit) and three sexual IPV (e.g. forced, coerced). Response options were ‘never’, ‘once’, ‘a few times’, or ‘many times’. A man responding ‘once’, ‘a few times’, or ‘many times’ to one or many items was classified as having perpetrated physical and/or sexual IPV in the past year.
Participants were also asked about several covariates. Specifically, age (18–30), education level (primary only, secondary not complete, secondary complete), and whether they had worked in the past 3 months (yes/no). We also asked about adversity in childhood using 12 items adapted from the Childhood Trauma Questionnaire (Bernstein et al., 2003), which had previously been modified for use in South Africa (Jewkes et al., 2010) asking about experiences of physical, sexual and emotional abuse and physical neglect prior to age of 18 (e.g. Before I reached 18 I was insulted or humiliated by someone in my family in front of other people). Responses were ‘never’, ‘sometimes’, ‘often’, and ‘very often’, and items were summed to create a breadth/severity scale.
Statistical Analysis
All analyses were conducted using StataSE v.18 (StataCorp, 2023). We first describe the baseline characteristics of the cohort who provided data across both timepoints, using percentages and n’s for categorical variables and means and standard deviations (SDs) for continuous variables. We then compare those who were lost to follow-up (LTFU) with those retained at endline on all variables in the models, using chi-squared tests and bivariate regressions to assess differences.
To assess the relationship between poor mental health and physical and/or sexual IPV perpetration at 24 months, we undertook the following analytic strategy. We first grouped men into four possible groups, based on their depression status at baseline and endline: ‘no change – low’ refers to those not depressed at both points; ‘no change – high’ refers to men depressed at both points; ‘down’ – depressed at baseline but not endline; ‘up’ – not depressed at baseline but depressed at endline.
We then describe men in terms of their allocation to each depression group. First, by reporting mean depressive symptoms at baseline, endline, and change for each group, and the proportion reporting IPV at baseline and endline, and the change in IPV perpetration in these groups. Second, we modelled the change in depressive symptoms and its relationship to endline perpetration through fitting logistic regression models, using robust standard errors for the clustering with the outcome IPV perpetration at endline. In model 1, we adjusted only for intervention arm allocation. In model 2 we adjusted for the potential confounders of age, education, work, and childhood adversity and IPV perpetration at baseline, as well as intervention arm allocation.
For change in PTS symptoms, we followed the same strategy as for depressive symptoms. However, given the small sample size in the PTS group ‘no change – high’, while describing this group and relationships seen, we exclude this group from modelling the relationship using logistic regression.
We undertook supplementary analyses where we excluded men who reported IPV perpetration at baseline. Thus, we had a ‘clean’ reference group and used the same modelling strategy as for the main analysis for depressive symptoms and PTS symptoms.
Results
At baseline N = 674 men were recruited into the study. At endline, we retained n = 505 men (74.9%). Table 1 describes the analytic sample (N = 505) used for the main analyses. Overall, mean age was 23.9 years. Only a third (33.1%) had completed secondary education and 8.1% had only primary education. A third (34.9%) reported working in the past 3 months. Men reported high levels of poor mental health. Just under half reported potentially clinically relevant symptoms of depression at baseline and endline (47.6% baseline, 42.2% endline), and potential PTSD was reported by 13.5% (baseline) and 13.9% (endline). At baseline, just over half (55.8%) reported perpetrating past year physical and/or sexual IPV, and this had declined to 46.3% at endline (a 9.8 percentage point decline) in the analytic sample. Supplemental Table 1 shows loss-to-follow-up in the full sample. Notably, childhood adversity was associated with LTFU, as was less education.
Descriptive Statistics for Analytic Sample (N = 505).
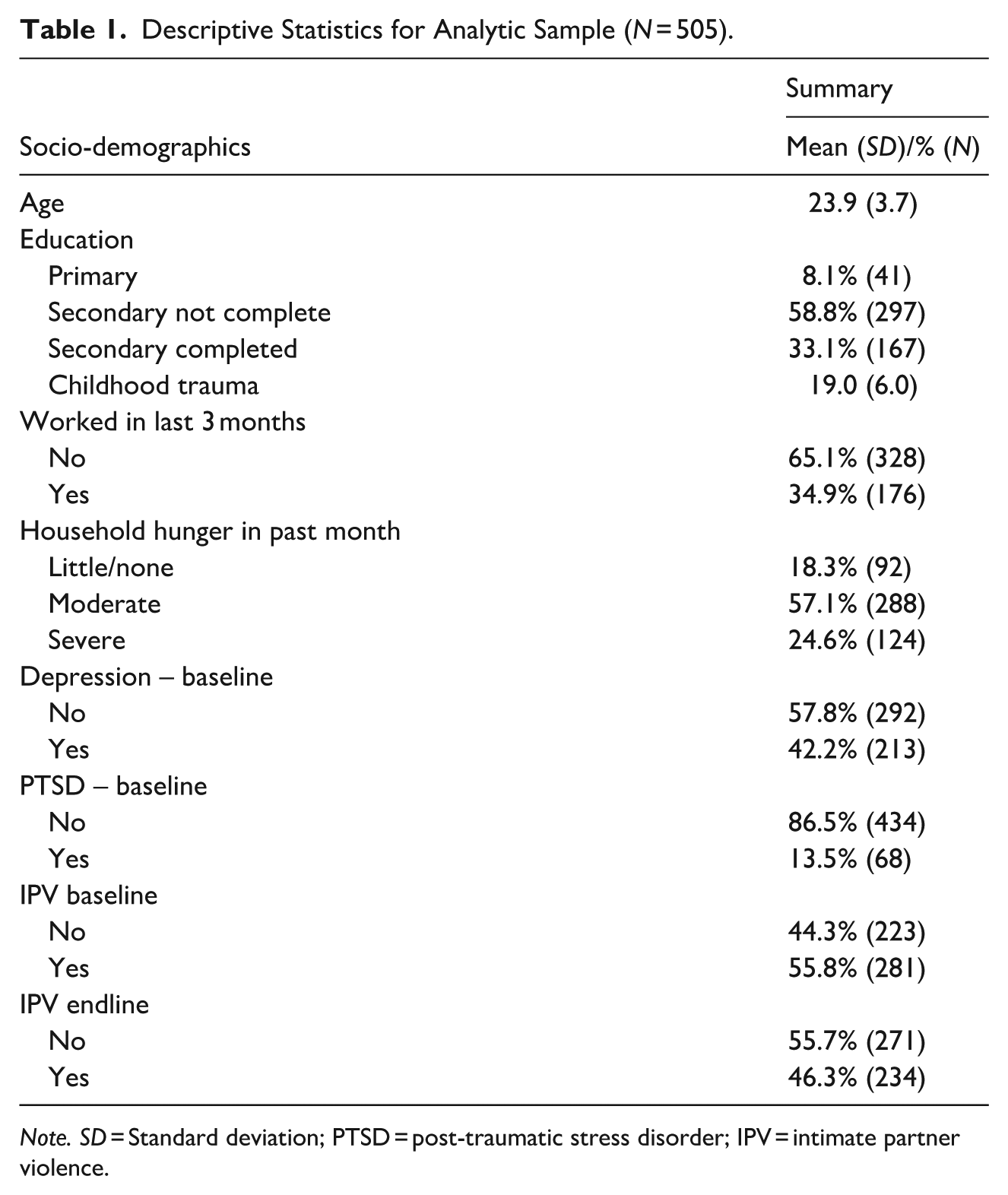
Note. SD = Standard deviation; PTSD = post-traumatic stress disorder; IPV = intimate partner violence.
Changes in Depressive Symptoms and Association With IPV Perpetration
Overall (Table 2), a third (35.3%) of men were in the ‘no change – low’ category (i.e. reported no potential depression at both baseline and endline), a quarter (24.9%) were potentially depressed at both timepoints (no change – high), a fifth (22.7%) reported a downwards trajectory (i.e. potentially depressed at baseline to not depressed at endline), while 17.1% reported an upwards trajectory (not depressed, to depressed). At baseline, the proportion reporting IPV perpetration in each group, was significantly larger in groups reporting depression at baseline, namely the ‘no change – high’ group (66.4%) and in the ‘down’ group (58.8%), compared to those who did not report depression, specifically the ‘no change – low’ where the proportion was 49.7%, and ‘up’ group (50.0%).
Descriptive Associations Between Changes in Depressive Symptom Groups and PTS Symptoms, and IPV Among Men Retained in the SSCF Trial.
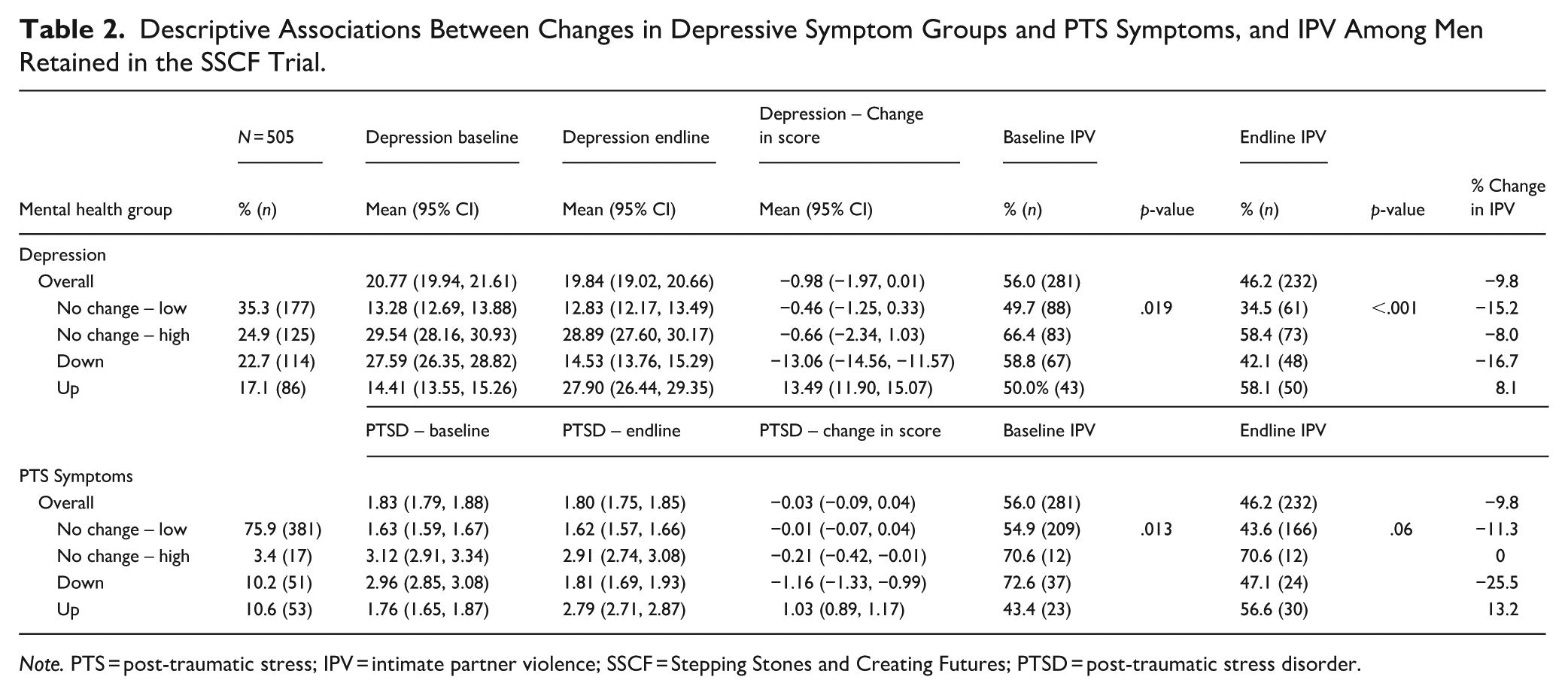
Note. PTS = post-traumatic stress; IPV = intimate partner violence; SSCF = Stepping Stones and Creating Futures; PTSD = post-traumatic stress disorder.
Assessing the relationship between groups and change in depressive scores and IPV perpetration descriptively (Table 2), among those in the ‘no change – low’ group, mean depressive scores at baseline and endline were stable, and IPV perpetration declined by 15.2 percentage points. For those in the ‘no change – high’ group, mean depressive scores were consistent at the two time points, and there was a small decline (8 percentage points) in IPV perpetration from baseline to endline.
For men reporting a reduction in depression classification from baseline to endline, mean depressive scores reduced by 13 points (Table 2), and IPV perpetration also declined by 16.7 percentage points, the largest decline in any group. Finally, among those seeing an increase in depression classification, mean depressive symptoms increased by 13 points, and IPV perpetration also increased by 8.1 percentage points.
In Table 3, Model 1 compared to the ‘no change – low’ group, at endline men in the ‘no change – high’ group were significantly more likely to perpetrate IPV at endline (aOR = 2.62, p < .001), as were men in the ‘up’ group (aOR = 2.62, p < .001). In the fully adjusted models (Model 2), a similar relationship was also seen. Supplementary analyses showed attenuated relationships, while ‘no change – high’ remained significantly higher for IPV perpetration; this relationship was attenuated for those in the ‘up’ group (Supplemental Table 2).
Adjusted Association Between Changes in Depression and Changes in PTS Symptoms and Future IPV Perpetration.
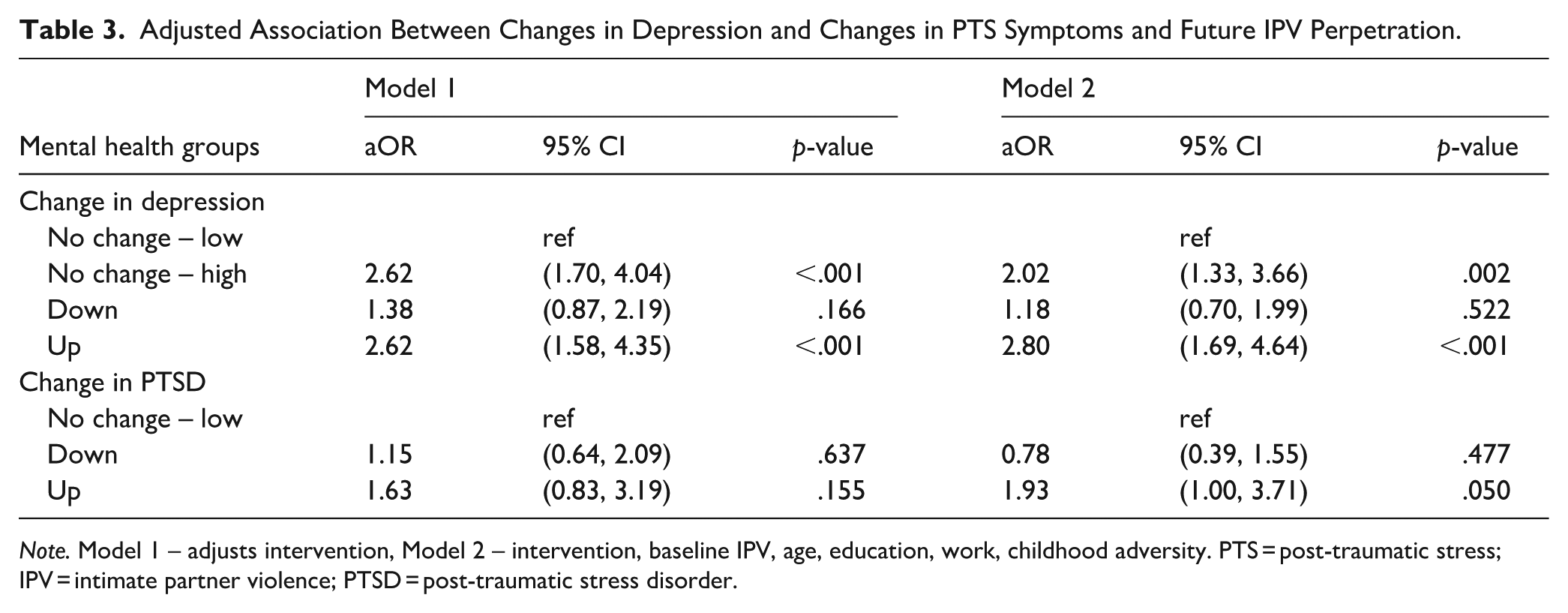
Note. Model 1 – adjusts intervention, Model 2 – intervention, baseline IPV, age, education, work, childhood adversity. PTS = post-traumatic stress; IPV = intimate partner violence; PTSD = post-traumatic stress disorder.
Changes in PTS Symptoms and Association With IPV Perpetration
Overall (Table 2), three-quarters (75.9%) of men reported no PTSD at either baseline or endline, and only 3.4% (n = 17) reported PTSD symptoms at both baseline and endline (no change – high). 10.2% of men were in the ‘down’ group, while 10.6% were classified in the ‘up’ group. At baseline, PTSD group allocation was descriptively associated with IPV perpetration. Specifically, the proportion reporting IPV perpetration was highest in those classified as potentially having PTSD at baseline, specifically ‘no change – high’ (70.6%) and ‘down’ (72.6%), compared to those reporting no PTSD at baseline, ‘no change – low’ (54.9%) and ‘up’ (43.4%).
Changes in PTS symptoms and IPV between baseline and endline by group are described in Table 2. Among the ‘no change – low’ group, there was no change in PTS symptoms, while overall an 11.3 percentage point reduction in IPV to 43.6%. Among those in the ‘no change – high’ group, there was no change in PTS symptoms, and no change in the prevalence of IPV reported. Among the ‘down’ group, mean PTS symptoms reduced by 1.16 points, while IPV reduced by 25.5 percentage points. While among the ‘up’ group, mean PTS symptoms increased by 1.03 points, and IPV perpetration increased by 13.2 percentage points.
Logistic regression models (Table 3) found that compared to those in the ‘no change – low’ in Model 1, there was no difference between this group and those in the ‘down’ or ‘up’ groups. In the fully adjusted model (Model 2), compared to the ‘no change – low’ group, those in the ‘up’ group were significantly more likely to perpetrate IPV at endline (aOR = 1.93, p = .050). Supplementary analyses reflected this analysis and showed a stronger association between IPV perpetration among those in the ‘up’ group (Supplemental Table 2).
Discussion
Among a group of young men who enrolled in an intervention trial and who lived in urban informal settlements in eThekwini Municipality, South Africa, there were generalised high levels of physical and/or sexual IPV perpetration as well as poor mental health. Where men reported increases in depressive symptoms, these were prospectively associated with IPV perpetration, and similarly, increasing PTSD symptoms were also prospectively associated with IPV perpetration. In addition, sustained experience of depression and sustained PTSD were also both associated with future IPV perpetration. However, where men reported reducing symptoms of depression or reducing symptoms of PTS, these were not associated with significantly less IPV perpetration.
Supporting prior research, increasing depressive symptoms and increasing PTS symptoms were associated with men’s future IPV perpetration (Oram et al., 2014, 2022; Ramsoomar et al., 2023; Spencer et al., 2019). In addition, there was also an association between depressive symptoms and PTS symptoms and IPV perpetration, cross-sectionally, again, reinforcing prior research (Oram et al., 2014, 2022; Ramsoomar et al., 2023; Spencer et al., 2019). There are likely several pathways shaping increasing depressive symptoms and IPV perpetration – depressive symptoms are strongly associated with irritability, particularly in young people (Vidal-Ribas & Stringaris, 2021), as well as anger and hostility (Painuly et al., 2005), which could be associated with IPV perpetration. It may also be that increasing depressive symptoms have an impact on relationship functioning and quality (Whitton & Kuryluk, 2012), which are also recognised risk factors for IPV (Stern, 2024). Similarly, there are a range of potential ways in which PTS symptoms may lead to increased IPV perpetration, including hyperarousal and challenges in regulating anger (Shorey et al., 2021). Moreover, with the large treatment gap for psychological ill-health, particularly for those living in informal settlements, many young men may use alcohol to self-medicate and mask symptoms of depression and PTS (Hawn et al., 2020), providing an additional mechanism through which poor mental health increases the likelihood of IPV perpetration, via alcohol use (Ramsoomar et al., 2021).
In neither of the adjusted models was there evidence that decreases in depression or PTSD were clearly associated with reductions in IPV perpetration at endline. In the depression analysis, the decrease in IPV perpetration in this group was of the same magnitude as the overall decrease in the full sample. In the PTSD analysis, the decrease in IPV was double the percentage point reduction seen in the ‘no change – low’ group (−25 percentage points for the ‘down-group’ versus −11 percentage points for the ‘no change – low’ group), but still, this was not associated with significantly less violence. It is unclear why there was no reduction in these groups where mental health improved, particularly as there is growing evidence that mental health interventions can reduce IPV (Greene et al., 2024; Murray et al., 2020). One explanation could be that given the high levels of alcohol and drug use among these young men, and its comorbid nature with depression and PTSD (Jane-Llopis & Matytsina, 2006; Puddephatt et al., 2022), the sustained IPV was seen because alcohol use was not reduced in the same way as depression and PTSD (Gibbs, Washington, et al., 2020). Indeed, in one successful intervention addressing men’s perpetration of IPV via promoting mental health, the intervention directly addressed both depression and alcohol misuse and saw significant reductions in IPV (Murray et al., 2020). Similarly, a recent study among refugees in Uganda sought to combine interventions addressing men’s poor mental health and substance misuse, demonstrating strong outcomes (Greene et al., 2024). Utilising more complex analytical strategies to model simultaneous changes in depression, PTS, and alcohol may be important in disentangling these relationships.
The exceedingly high levels of depressive symptoms were also notable in this sample, with a quarter being potentially clinically depressed at both time points and an additional 39.8% reporting this at either time point; therefore, almost two-thirds (64.7%) reported potentially clinically significant symptoms of depression across 2 years of follow-up in this study. This represents a major unresolved health burden of poor mental health, driven by a complex combination of structural inequalities of poverty, experiences of violence and adversity in childhood and adulthood, inequitable gender norms and ideals of masculinity, and more proximate drivers of poor mental health (Gibbs et al., 2018; Oliffe & Phillips, 2008). Given the limited access to formal treatment for poor mental health in these communities, and the assumption that mental healthcare is a ‘woman’s space’ (Sikweyiya et al., 2025), there remains a major challenge for developing and providing adequate support to these young men.
This study has a series of limitations. Notably, we used screening tools for depression and PTS symptoms rather than clinical assessments, which may mean we overestimated the prevalence of these conditions. In addition, we focused on change in symptoms over 2 years, which may not capture shorter-term fluctuations in symptoms. More intensive follow-ups enabling a more precise understanding of changes would be important. In addition, IPV was assessed in the past 12 months, while depression and PTS symptoms were both assessed in the past week; thus, the temporality of associations is unclear. Future research should consider more intensive data collection approaches, where these issues can be resolved, for instance, through using experience sampling methods (Sullivan et al., 2011). A key limitation is not modelling the relationship between PTS and depression simultaneously, given that these are often comorbid, nor utilising an analytic strategy that could incorporate the role of alcohol in these models. Moreover, the sampling approach of this study, through non-random recruitment into an intervention, suggests these findings are not generalisable to a wider population, nor to those living in urban informal settlements.
This study demonstrated that increasing symptoms of depression and PTS, as well as high and sustained symptoms of depression, in young men were prospectively associated with their recent perpetration of physical and/or sexual IPV. Integrating approaches to ensure that good mental health is maintained may be important in future IPV prevention interventions. There is a range of strategies that may be effective in addressing these interlinkages – brief-interventions based on transdiagnostic therapies have been shown to be effective, particularly when they have integrated addressing alcohol simultaneously (Murray et al., 2020). Others have suggested that broader approaches that recognise the underlying and ongoing challenges that drive poor mental health may be more appropriate for effectively addressing poor mental health (Burgess, 2020). As such, strategies that address the structural drivers or ‘up-stream’ causes of poor mental health – and often IPV perpetration too – such as gender inequalities (Stern, 2024) and poverty (Ridley et al., 2020) may be important. More widely, there remains a large unaddressed burden of poor mental health among young men living in urban informal settlements in South Africa, which requires systematic approaches to address.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605251408126 – Supplemental material for A Prospective Analysis of Associations Between Changes in Mental Health and Men’s Perpetration of Intimate Partner Violence: Post-Hoc Analysis of Young Men Involved in the Stepping Stones and Creating Futures Trial
Supplemental material, sj-docx-1-jiv-10.1177_08862605251408126 for A Prospective Analysis of Associations Between Changes in Mental Health and Men’s Perpetration of Intimate Partner Violence: Post-Hoc Analysis of Young Men Involved in the Stepping Stones and Creating Futures Trial by Andrew Gibbs, Smanga Mkhwanazi, Sivuyile Khaula, Laura Washington and Yandisa Sikweyiya in Journal of Interpersonal Violence
Supplemental Material
sj-docx-2-jiv-10.1177_08862605251408126 – Supplemental material for A Prospective Analysis of Associations Between Changes in Mental Health and Men’s Perpetration of Intimate Partner Violence: Post-Hoc Analysis of Young Men Involved in the Stepping Stones and Creating Futures Trial
Supplemental material, sj-docx-2-jiv-10.1177_08862605251408126 for A Prospective Analysis of Associations Between Changes in Mental Health and Men’s Perpetration of Intimate Partner Violence: Post-Hoc Analysis of Young Men Involved in the Stepping Stones and Creating Futures Trial by Andrew Gibbs, Smanga Mkhwanazi, Sivuyile Khaula, Laura Washington and Yandisa Sikweyiya in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We would like to thank the other researchers involved in the original study, as well as the fieldworkers for collecting the data, and the participants for providing their time and information. For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising from this submission.
Ethical Considerations
The South African Medical Research Council’s Human Research Ethics Committee (HREC) and the Biomedical Research Ethics Committee at University of KwaZulu-Natal provided ethics approval.
Consent to Participate
Participants provided written informed consent to participate in this study.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: The original study for which the data were collected was funded by What Works To Prevent Violence? A Global Programme on Violence Against Women and Girls (VAWG) funded by the UK Government’s Department for International Development (DFID). This analysis was jointly funded by the UK Medical Research Council (MRC) and the Foreign Commonwealth and Development Office (FCDO) under the MRC/FCDO Concordat agreement, project Adapting an evidence-based intervention to reduce IPV for use among young heterosexual couples in South Africa (MR/X004090/1). The funders had no role in study design, in the collection, analysis and interpretation of data; in the writing of the articles; and in the decision to submit it for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.