
Abstract
Studies have shown that social and interpersonal risk factors often lead to teen dating victimization (TDV); however, scant studies have estimated the link between adolescent depressive symptoms and physical TDV and the mediating effects of peer justification of TDV. Thus, the current study utilized data from the Bullying, Sexual, and Dating Violence Trajectories from Early to Late Adolescence in the Midwestern United States, 2007 to 2013 and General Structural Equation Modeling (GSEM) analysis to address these limitations by (a) exploring the direct association between depressive symptoms and physical TDV and (b) examining the mediating role of peer justification of TDV on the link between depressive symptoms and physical TDV while controlling for cognitive impulsivity, family support, parental monitoring (n = 1,884). Results from GSEM indicated that adolescents who experienced depressive symptoms are more likely to experience physical TDV, which is consistent with the stress generation hypothesis. Indirect effects results suggested that as adolescents experienced depressive symptoms, they were more likely to associate with peers who maintain teen dating violence attitudes, subsequently increasing their likelihood of experiencing physical TDV. Practical and theoretical implications are discussed.
Introduction
Physical teen dating victimization (TDV) refers to experiencing kicking, shoving, punching, or choking during a teen relationship (Wincentak et al., 2017). These experiences are prevalent, as prior literature has suggested that approximately 30% to 50% of adolescents have experienced TDV (Ybarra et al., 2016). Critical risks of physical TDV include, but are not limited to, depression, substance use, eating pathology, school failure, early teen pregnancy (Muñoz-Rivas et al., 2007; Rostad et al., 2020; Spencer et al., 2021), exposure to family violence, child maltreatment (Emanuels et al., 2022), race and gender differences (Foshee et al., 2010), impulsivity (Connolly et al., 2020), inadequate parental monitoring (Reyes et al., 2017), and peer alienation (Sabina et al., 2016). Physical TDV has been linked with a multitude of negative outcomes, including academic challenges, anxiety, depression, suicidal ideation, substance use, and interpersonal effectiveness challenges (Banyard & Cross, 2008).
While mounting evidence has suggested risk factors and consequences of physical TDV, less is known whether mood disturbances, including depressive symptoms, increase the likelihood for adolescents to experience physical TDV. Although prior studies have shown that depressive symptoms increase the occurrence of victimization (Reijntjes et al., 2010; Troop-Gordon, 2015), these studies measured general peer victimization, including bullying and rational victimization, which excludes physical TDV and did not adequately capture the nuances of physical TDV longitudinally. Another omitted contributing factor to physical TDV is the degree to which adolescents associate with peers who justify TDV experiences. That is important because studies have shown that adolescents spend most of their time associating with peers, and if these peers condone TDV, then adolescents are more likely to adopt these attitudes and behaviors in their relationships (Capaldi et al., 2012; Sianko et al., 2019; Wojciechowski & Lawrence, 2024). Consistent with the existing body of literature, the focus of this study is to (a) investigate the direct association between depressive symptoms and physical TDV and (b) explore the indirect effect (mediating) of peer TDV justification on the link between depressive symptoms and physical TDV while accounting for family support, impulsivity, parental monitoring, and demographic variables, including gender and race.
Theoretical Framework
Theoretically, the current study draws from the stress generation hypothesis to estimate the longitudinal link between depressive symptoms and physical TDV mediated by associating with peers who justify TDV. According to the stress generation hypothesis, individuals who experience depressive symptoms are often more likely to encounter stressful live events, which are interpersonal in nature and are often contingent on their interpersonal challenges (Daley et al., 1997; Hammen, 1991). Reasons for this are that individuals who experience depressive symptoms may be prone to experiencing feelings of hopelessness and distorted beliefs (e.g., filtering and polarized thinking) that eventually increase their likelihood of encountering additional life stressors (Liu & Alloy, 2010). For instance, Abramson et al. (1989) suggested that individuals who experience depressive symptoms are more likely to attribute daily stressors as stable and unchangeable, which increases misinterpretation of stressful events and leads to additional interpersonal stress. Prior meta-analytic literature has supported the application of the stress generation hypothesis in various samples, including children, adolescents, and adults (Liu, 2013); however, few studies have utilized this model in the context of teen dating literature. Another limited emphasis is the process by which adolescents associate with peers who justify TDV. First, considering that prior literature has suggested depressive symptoms are often common among adolescents (Shorey et al., 2022), and youth who engage in dating relationships are susceptible to experiencing TDV (Wincentak et al., 2017), applying the stress generation perspective in teen dating literature could highlight the relevance of experiential depressive symptoms on subsequent TDV. Second, prior studies have indicated that adolescents who experience depressive symptoms may experience the emergence of a “risky lifestyle” characterized by excessive antisocial peer approval that increases their likelihood of experiencing adverse experiences (Ciairano et al., 2007; Joiner, 2000; Starr & Davila, 2008). In support of this perspective, prior evidence shows that associating with antisocial peers who maintain favorable attitudes toward dating violence has been identified to shape future dating behavior (Jouriles et al., 2013; Kwon & You, 2023). For instance, co-rumination, referring to a self-regulation tactic in which adolescents self-disclose primarily negative feelings while relying on their peers for support and validation, has been shown to increase peer influence on future behavior (Rose, 2002; Schwartz-Mette & Smith, 2018). Drawing from these theoretical perspectives, it is possible that adolescents who experience depressive symptoms are more likely to encounter physical TDV, and this connection is explained (mediated) by their likelihood of associating with peers who maintain justifying attitudes toward TDV.
Connection Between Depressive Symptoms and Peer Justification of TDV
Depressive symptoms during the adolescent developmental period are common, with prevalence rates suggesting that 34% of adolescents experienced depressive symptoms from 2001 to 2020 (Shorey et al., 2022). Although the onset of depressive symptoms is often comorbid with other distinct psychopathologies, the literature has indicated that depressive symptoms are also often strongly correlated with loneliness and interpersonal difficulties (Clayborne et al., 2019). Loneliness and interpersonal difficulties are crucial consequences of depression because these maladjustments can lead to peer rejection and could disrupt the “normal” developmental trajectory for adolescents (Mulvey et al., 2017). To reduce the occurrence of loneliness and peer rejection, adolescents often develop social networks with peers that are interconnected in nature, which could serve as a negative emotion-alleviating protective mechanism and increase the likelihood of peer social norm conformity (Korzhina et al., 2022; Prinstein, 2007). Understandably, as adolescents become vulnerable to adopting the attitudes and beliefs maintained by their peers, they might encounter peers in abusive relationships who consider TDV a normal occurrence in romantic relationships (Capaldi et al., 2012). As a result, peer TDV justification is positively associated with TDV among adolescents (Arriaga & Foshee, 2004; Hunt et al., 2022).
Despite this, few studies have explored how depressive symptoms could lead to physical TDV via associating with peers who justify attitudes toward TDV. This is important because although adolescents are often susceptible to developing depressive symptoms (Lawrence et al., 2022), they are also heavily influenced by their peers’ dating relationships, as these relationships often influence whom they perceive to be attractive (Oudekerk et al., 2014). As a result, when engaging with peers, adolescents often learn and adopt their peer attitudes and beliefs through observation and imitation (Van Hoorn et al., 2016). Adolescents who endorse and display peer-acceptable behavior are likely to be reinforced by their peer network, which guides their subsequent social decisions (Berger & Rodkin, 2012). This is partially consistent with the homophily framework, which suggests that adolescents often maintain friends who are similar in attitudes and beliefs, and these internal processes are often persistent over time (Brechwald & Prinstein, 2011; Kandel, 1978). Therefore, a synthesis of stress generation hypothesis and homophily framework indicates it is likely that following the onset of depressive symptoms and the associated loneliness and interpersonal difficulties, adolescents who experience depressive symptoms and hence seek less prosocial/antisocial peer approval might be more likely to associate with peers with similar attitudes and beliefs about TDV, subsequently increasing their likelihood of accepting and experiencing physical TDV.
Current Study
The current study utilized the stress generation model hypothesis and homophily framework to investigate the longitudinal direct association between depressive symptoms and physical TDV while estimating the mediating role of peer justification of TDV on the link between depressive symptoms and physical TDV while controlling for family support, impulsivity, parental monitoring, and demographic variables. In congruence with the stress generation hypothesis, which posits that individuals who experience depressive symptoms often encounter adverse experiences, we hypothesize that depressive symptoms would be positively associated with physical TDV (HI1). Consistent with the homophily perspective, we predict that peer justification of TDV would mediate the association between depressive symptoms and physical TDV (HI2).
Methods and Data
Participants
Participants completed online questionnaires consisting of family history, mental health, peer victimization, and dating violence. Overall, there were 1,884 participants in the study, which included 927 boys and 957 girls. The ages of participants ranged from 13 to 17 years of age (M = 14.79; SD = 0.58). Thirty-two percent of the participants identified as Black/African American, 30% White/Caucasian, 23% Hispanic, 1% Asian, 3% biracial, and 11% multi-racial.
Procedure
Research approval was obtained from the University of Illinois Institutional Review Board, and parental consent forms were sent to parents explaining the purpose of the study, the risk, and their option to participate. Parents who consented to participation signed the form and returned it to their child’s school. Parents who declined to participate were removed from the potential participant pool in the classrooms before the study commenced. Participants who chose to participate were informed that the study was voluntary, and adolescents were given an assent form. To ensure confidentiality, students were separated within the classroom and were informed to skip questions that made them feel uncomfortable. Overall, the study instrument took approximately 45 min to complete, and participants were reassessed within 6 months intervals. The study achieved a 95% completion rate. The timing of measurement of control variables used in analyses was chosen to provide temporal ordering between these covariates and the dependent variable. Similarly, the timing of the key independent and mediating variables (Wave 1 and Wave 2, respectively) was chosen to properly establish temporal ordering between these variables and the dependent variable measured at Wave 3 in their proper place in the causal mediation chain.
Measures
Depressive Symptoms
Depressive symptoms were measured at Wave 1 using the Orpinas Modified Depression Scale (Orpinas, 1993). This scale measures the extent to which individuals experienced depressive symptoms over the previous 30 days. An example item is, “Do you feel hopeless about the future?”, which was measured on a 5-point Likert-type scale ranging from 0 (Never) to 4 (Always). Higher scores indicate more frequent depressive symptoms. A Cronbach’s alpha score of .861 indicated good internal reliability for the items used in this scale.
Peers’ Justification of TDV
Peers’ justification of TDV was measured at Wave 2 using created items from the original study. More specifically, 7 items were created that assess adolescents’ peer socialization with peers who justify TDV. Example items include, “My friends generally think it is ok for a boy to hit his/her girlfriend if she did something to make her mad,” and “My friends generally think girls sometimes deserve to be hit by the boys they date.” These items were measured on a 4-point Likert scale ranging from 0 (strongly disagree) to 3 (strongly agree). Higher scores indicate increased association with peers who justify TDV. A Wave 1 measure of this construct was also included in analyses as a control variable. Cronbach’s alpha scores for both the Wave 1 and Wave 2 measures of this construct indicated adequate internal consistency for individual items comprising these aggregate measures with scores of .843 and .852 observed, respectively.
Physical TDV
Physical intimate partner victimization was measured at Wave 3 using the Conflict in Adolescent Dating Relationships Inventory (CADRI; Wolfe et al., 2001). The CADRI contains 25 items with five subscales (Threatening, Relational, Physical, Sexual, and Verbal/Emotional), and the current study only utilized the physical dating victimization subscale, which contained 7 items. For definitional purposes, participants were asked whether they have spent time with someone or were seeing someone in a romantic nature. Example items include “He/she pushed, shoved, or shook me,” and “He/she scratched me and/or bent my fingers.” These items were measured on a 4-point Likert scale ranging from 0 (Never) to 5 (6 or More Times). Higher scores represent more frequent physical TDV. A Wave 1 measure of this concept was also included in analyses as a control variable. Cronbach’s alpha scores for both the Wave 1 and Wave 3 measures used in analyses indicated adequate internal reliability, with scores of .874 and .888 observed for each wave, respectively.
Covariate Variables
Age
Age was measured at Wave 3 in single-year intervals.
Gender
Gender was measured using a binary variable at Wave 1, with boy and girl participants delineated into distinct categories (0 = boys; 1 = girls)
Race/Ethnicity
Race/ethnicity was assessed at Wave 1 using a nominal variable with the following response options: Black, Latinx, Asian, Biracial, White. A series of dummy variables was then coded from this original nominal variable, with participants in each race/ethnicity category delineated from all other participants for each dummy variable (e.g., 1 = black; 0 = all other participants). The dummy variable corresponding to White participants was then omitted from analyses as the reference group.
Number of Dates at Wave 3
The number of dates that participants reported having during the Wave 3 observation period was also included as a control variable, as having fewer dates would necessarily mean lower risk for experiencing TDV perpetration. This variable was a count of the number of dates that each participant reported having during the Wave 3 observation period.
Parental Monitoring
Parental monitoring was measured at Wave 2 using a subscale from the Seattle Social Developmental Project (Arthur et al., 2002). This scale measures the extent to which adolescents are aware of their family rules and their perceived parental awareness regarding their schoolwork, attendance, peer relationships, and alcohol and drug use. Example items are, “My family has clear rules about alcohol and drug use,” and “My parents ask if I’ve gotten my homework done,” which were measured using a 4-point Likert scale ranging from 0 (never) to 3 (always). Higher scores indicate an increase in parental monitoring. Cronbach’s alpha indicated that there was strong internal reliability for the measures used to compute this aggregate score (Alpha = .929).
Family Support
Family support was measured at Wave 2 using a subscale from the Vaux Social Support Record (Vaux et al., 1987). This subscale measures the degree to which adolescents perceive that there is available support from the family. An example item includes “There are people in my family I can talk to,” which was measured using a 3-point Likert scale ranging from 1 (not at all) to 3 (some or a lot). Higher scores indicate increased family support. The Cronbach’s alpha score obtained for these items used to compute the aggregate measure used in analyses indicated strong internal reliability (alpha = .952).
Cognitive Impulsivity
Cognitive impulsivity was measured at Wave 2 using a subscale from the Teen Conflict Survey (Bosworth & Espelage, 1995). This scale measures the extent to which individuals engage in acts or behavior without future consideration. An example item is, “I do things without thinking,” which was measured on a 5-point Likert scale ranging from 0 (never) to 4 (always). Higher scores represent an increase in impulsivity. Adequate internal reliability was observed for these items used to create this aggregate measure based on an obtained Cronbach’s alpha score of .815.
Data Analytic Strategy
The present study utilized generalized structural equation modeling (GSEM) to examine the direct effects of depressive symptoms on physical TDV victimization and the potential influence of peer justification of TDV on mediating this relationship. GSEM was used because of its capacity to identify the distinct pathways of this relationship, determine the magnitude of the effects of each component within this pathway, and extend the method to distinguish whether the full pathway is statistically significant or not. The generalized form of this method was used because of the right-skewed nature of the outcome variable. As such, Poisson regression was used within the GSEM framework to examine these relationships of interest. Coefficients were then interpreted as the predicted difference in log-odds counts on the dependent variable scale given a one-unit change in an independent variable of interest, net of all covariates in the model. Listwise deletion was used to manage missing data, as imputation methods are not compatible with GSEM in Stata. Model 1 examined the direct effects of depressive symptoms on physical TDV scores net of all control covariates. Model 2 then included the hypothesized mediating variable of peer justification of TDV, again net of all control covariates.
Upon estimating the GSEM models to identify direct and indirect effects of interest, the method must be extended to determine whether peer justification of TDV significantly mediates the relationship between depressive symptoms and physical TDV. This process necessitates the use of standard errors to compute a p-value for the pathway. While the delta method can be used in this regard, this can result in non-normally distributed standard errors, which can lead to biased estimates of statistical significance. As such, the Preacher and Hayes (2008) method of bootstrap resampling was used to calculate unbiased standard errors and provide a more valid estimate of statistical significance. A total of 500 bootstrap resamples were calculated and used to compute the coefficient, standard errors, p-value, and confidence intervals for the full mediating pathway. Stata and MP 16.1 Statacorp were used to conduct all analyses for the present study.
Results
Table 1 provides descriptive statistics for all of the variables included in these analyses. Table 2 then provides Model 1 and Model 2 GSEM results. Model 1 results indicated that higher depression scores at Wave 1 were associated with increased TDV scores at Wave 3 (Coefficient = 0.357, p < .013). This meant that for each one-unit difference in depression scores between participants, TDV victimization scores increased by an average of .357 points on this scale. Greater impulsivity, more dates, and higher TDV scores at Wave 1 were also all associated with increased TDV scores at Wave 3 in this model. Model 2’s results indicated that inclusion of the peer justification of TDV variable at Wave 2 attenuated the direct effect of depression from Model 1 by about 10%, though this relationship remained statistically significant (coefficient = 0.328, p < .023). This meant that for each one-unit difference in depression scores between participants, TDV victimization scores increased by an average of 0.328 points on this scale. Greater peer justification of TDV at Wave 2 also predicted greater TDV scores at Wave 3 in this model (Coefficient = 0.452, p < .009). This meant that for each one-unit difference between participants in peer TDV justification, TDV victimization scores increased by an average of 0.452 points on this scale. Greater impulsivity, having more dates, and greater physical TDV scores at Wave 1 were also all associated with greater physical TDV scores at Wave 3. Latinx participants also reported lower TDV victimization scores compared to White participants in this model as well.
Descriptive Statistics.
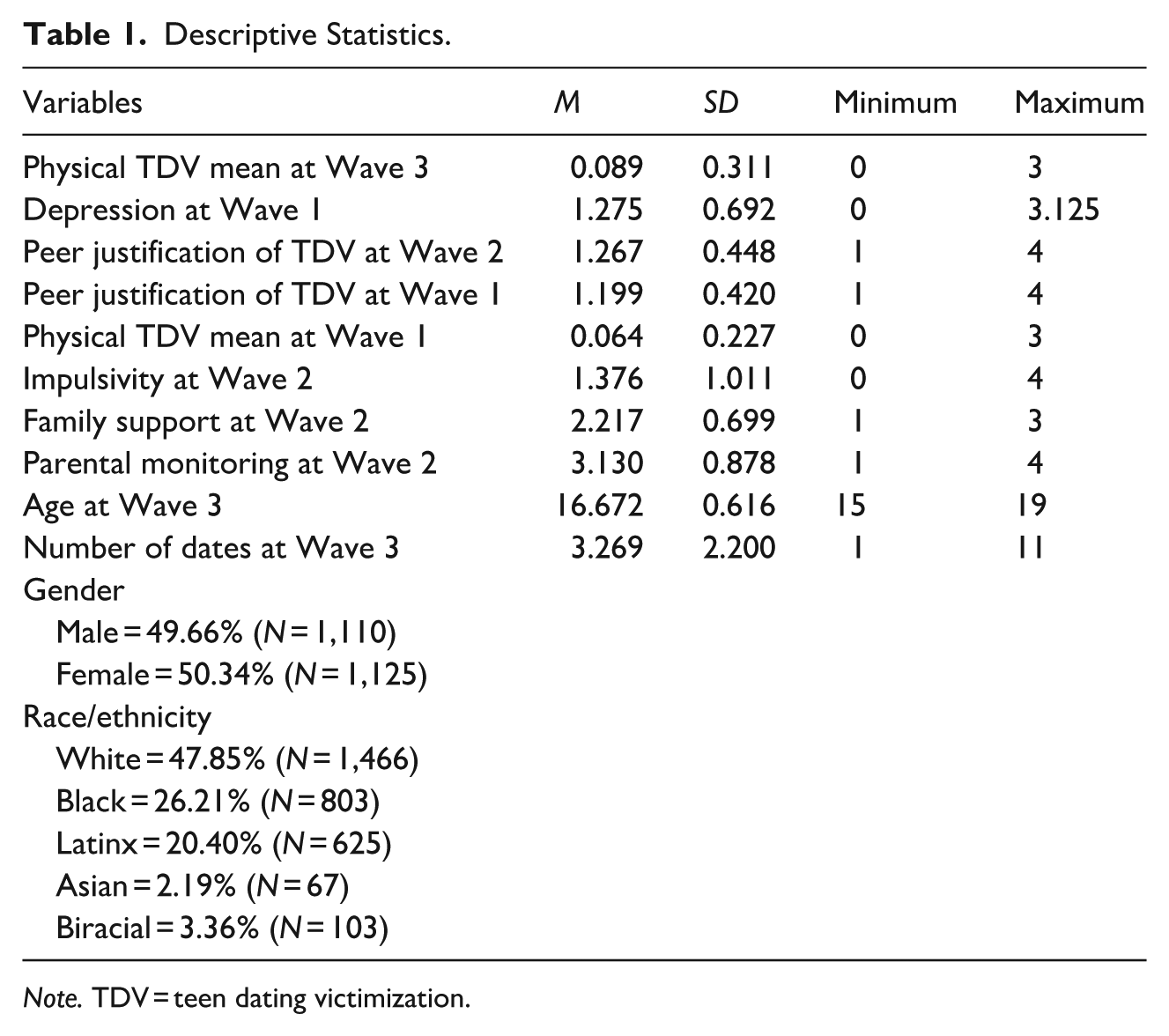
Note. TDV = teen dating victimization.
Generalized Structural Equation Poisson Regression Modeling of Depression on Mean Physical TDV Scores at Wave 3 and Proposed Mediating Pathway (N = 818).
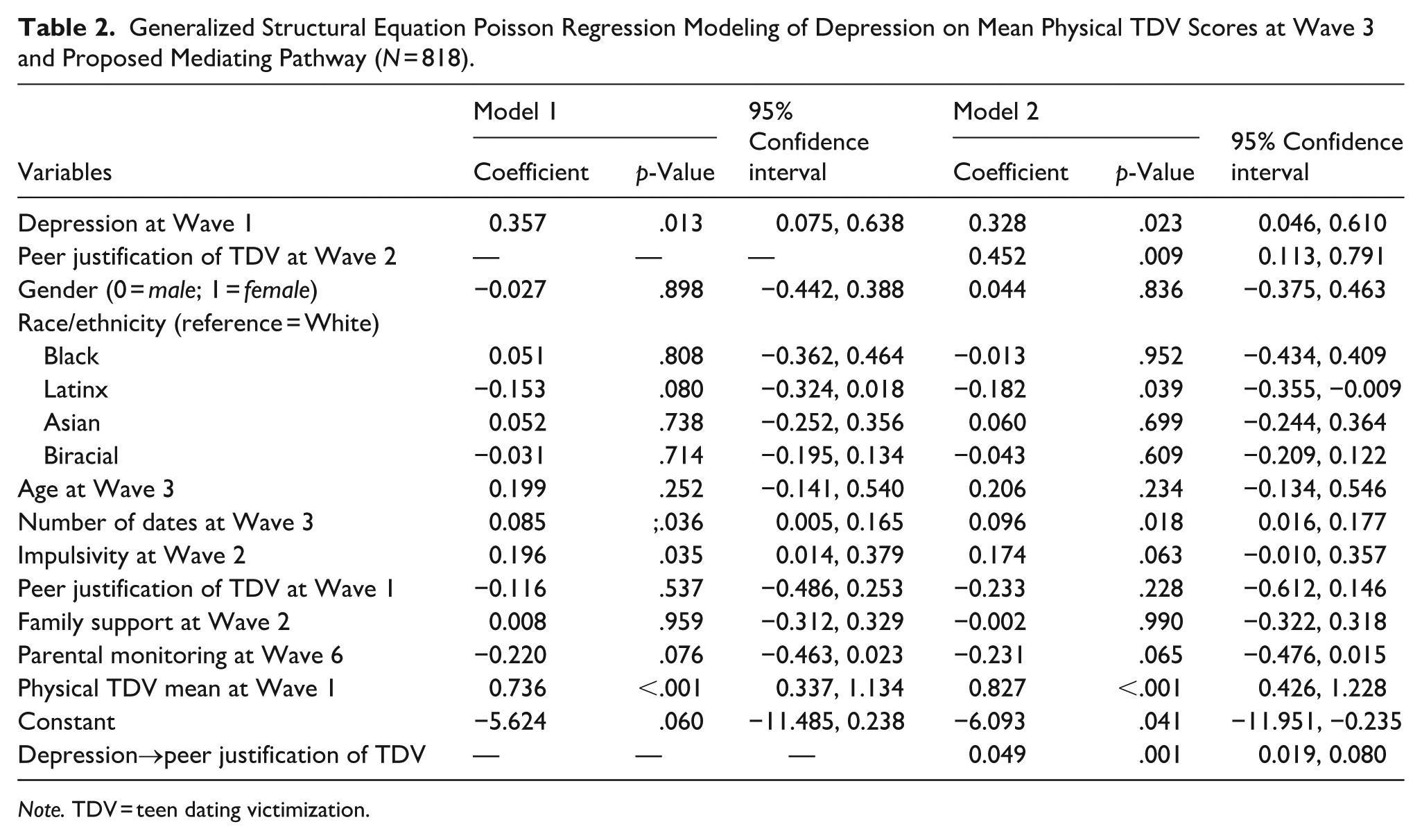
Note. TDV = teen dating victimization.
The Preacher and Hayes (2008) bootstrap resampling process was then used to determine whether peer justification of TDV at Wave 2 significantly mediated the relationship between Wave 1 depression and Wave 3 physical TDV victimization. These results indicated that this mediation effect was indeed statistically significant (coefficient = 0.022, standard errors = 0.011, p < .035, 95% CI [0.002, 0.043]). These findings indicated that the 10% attenuation of the depression effect observed from Model 1 to Model 2 was a significant portion of this effect accounted for by peer TDV justification. Sensitivity analyses were also estimated to determine whether moderation processes, as well as mediation processes, may have been relevant here. The interaction between depression and peer justification of TDV at Wave 1 for predicting TDV at Wave 2 was examined with all relevant control variables also included in the models. Timing of control variable measurement was adjusted for the Wave 2 measurement of the dependent variable in analyses. A Poisson model was used to assess these relationships based on the distribution of the Wave 2 measure of TDV and the lack of overdispersion in these data. Multiple imputation, with variables with missing data regressed on the race variables without missingness, was carried out to manage missing data for these analyses. Findings indicated a null interaction between these constructs for predicting physical TVD scores at Wave 2. These findings further highlight the relevance of the mediation pathway posited here over a potential moderation model.
Discussion
The current study utilized the stress generation hypothesis to test the longitudinal effects of adolescent depressive symptoms on physical TDV. Additionally, this study explored the mediating role of peer justification of TDV on the association between depressive symptoms and physical TDV. The findings contributed to the existing literature by highlighting the longitudinal association between adolescent depressive symptoms and physical TDV while underscoring how adolescents' peer social networks could explain this relationship. More specifically and developmentally, these findings posit that the onset of depressive symptoms among adolescents could lead to antisocial peer association, specifically peers who maintain TDV-justifying attitudes, which increases their risk of experiencing physical TDV victimization at Wave 3.
Longitudinal Link Between Depressive Symptoms and Physical TDV
As hypothesized in HI1, our findings indicated that the onset of depressive symptoms was longitudinally positively associated with physical TDV. Consistent with the stress generation hypothesis, adolescents who experienced depressive symptoms were more likely to encounter adverse outcomes—in this case, experiencing physical TDV. This partially supports previous studies, which could suggest that adolescent who experience depressive symptoms were more likely to maintain distorted beliefs about themselves and engage in negative evaluation of self, the world, and the future, which subsequently increases their likelihood of experiencing interpersonal conflict consistent with TDV (Keser et al., 2020; Lawrence et al., 2023; Rudolph et al., 2009). Additionally, our findings align with previous studies suggesting that adolescents who experience depressive symptoms may be vulnerable to physical TDV by their peers (McLaughlin et al., 2009; Pitula et al., 2014). Moreover, although speculative, these findings could indicate that adolescents who experience depressive symptoms may experience social isolation and difficulties forming interpersonal connections with peers, which could increase their vulnerability to peer relational physical victimization. Prior literature does support this proposition, such that depressed youth reported social skills difficulties, which then elevated their risk for peer victimization (Kochel et al., 2012). In this case, our findings could suggest that experiencing depressive symptoms could increase the likelihood of adolescents maintaining maladaptive romantic relationships that underscore relational abuse and physical violence, characterizing their experience of physical TDV.
The Indirect Role of Peer Justification of TDV on the Link Between Depressive Symptoms and Physical TDV
Although prior literature has shown that peer justification of TDV could lead to TDV (Hunt et al., 2022), we advanced the current literature by determining whether peer justification of TDV indirectly explains the association between depressive symptoms and physical TDV. Consistent with our hypothesis (HI2), adolescents who experienced depressive symptoms were more likely to associate with peers who maintained attitudes that justified TDV, which in turn increases their possibility of experiencing physical TDV. These results partially correspond with previous literature, which suggests that adolescents who experience depressive symptoms are more likely to co-ruminate with peers and engage in over-self-disclosure of their symptoms to alleviate their depressive symptoms, which could subsequently increase their likelihood of experiencing adverse outcomes (Bastin et al., 2015; Spendelow et al., 2017).
Theoretically, our results are consistent with stress generation hypothesis model and previous studies that show that adolescents who experience depressive symptoms may maintain a “risky lifestyle,” categorized as the process in which adolescents associate with antisocial peers and conduct their daily activities without adult supervision, thus increasing their vulnerability of victimization (Gover, 2004; Harned, 2002; Vezina & Hebert, 2007). This is also consistent with the homophily framework, which suggests that adolescents maintain friends similar to them in attitudes and beliefs (Brechwald & Prinstein, 2011). Associating with similar-minded peers and adopting antisocial attitudes through the peer social network is often strongly associated with experiencing adverse outcomes (Dupéré et al., 2021; Rudolph et al., 2020).
Implications for Practice
Our study found that adolescents (13–17 years) who experienced depressive symptoms are likely to experience physical TDV victimization through their association with peers who maintain attitudes that justify TDV, suggesting several implications for TDV prevention and intervention. Since many adolescents spend much of their time at school, school counselors/clinicians should be charged with identifying and reducing school-specific psychosocial stressors that are often associated with depressive symptoms, including peer rejection (Sentse et al., 2017), loneliness, and lack of social support (Auerbach et al., 2011). Specifically, schools that have implemented social-emotional learning (ESL) programs report a significant decrease in internalizing symptoms among adolescents and a reduction in the occurrence of TDV victimization (Espelage & Holt, 2007). Thus, school clinicians can implement ESL programs that could teach healthy communication patterns, emotion-regulation, and bystander intervention specifically adapted for adolescent populations.
Since psychosocial stressors, such as family violence and child maltreatment, often trigger depressive symptoms (Lawrence et al., 2022) and could lead to TDV victimization (Stover et al., 2018), family clinicians can address these maladaptive patterns by using the multisystem therapeutic (MST) approach. This approach addresses several risk factors of internalizing and externalizing symptoms simultaneously through the development of healthy communication patterns among families, strengthening the parent–child relationship, and providing psychoeducation on distress tolerance strategies that could assist in improving peer relationships. Efficacy studies have shown that families who have engaged in MST-specific interventions often report a reduction in both internalizing and external symptoms with adolescents and fewer parent-child conflicts (Butler et al., 2011; Van der Stouwe et al., 2014). This is important because parental psychopathology is related to internalizing symptoms and may increase the vulnerability of TDV (Livingston et al., 2018).
It is crucial to note that most prevention programs are implemented in school and clinical settings (Leen et al., 2013), and the adolescents most in need of TDV prevention and intervention programming may not attend school and/or may not receive reliable healthcare clinical services. Therefore, it would be beneficial to implement community-level prevention and interventions for at-risk adolescent populations. An example of such an intervention is Date SMART (Skills for Managing Aggression in Relationships for Teens; Rizzo et al., 2017) that utilizes cognitive behavioral therapy to target depressive symptoms as a primary mechanism of change to reduce the incidence of TDV among high-risk adolescent girls in the community. Along with supporting existing evidence-based community interventions, it is also highly critical to invest evaluation efforts in community-led, culturally-specific, and trauma-informed interventions that might not have the research bandwidth to evaluate their impact. An example of such an intervention is Women Healing Eternally and Transforming (WHEAT)’s Safe Relationships program, which is a Black- and Survivor-led community organization that provides a youth-centered, community-driven interactive workshop series that seeks to empower at-risk adolescents (ages 10–19) and prevent TDV (WHEAT Organization, n.d.). Furthermore, community-based mental health advocates can play a pivotal role in increasing awareness of TDV by collaborating with community mental health facilities and community-based TDV prevention–intervention efforts by providing psychoeducational services that promote healthy communication, emotion regulation, community building and peer support, parental caregiving support, and help-seeking behaviors (Luo et al., 2022; Smith & Donnelly, 2000). It should also be noted that while Latinx participants reported lower TDV victimization risk in these analyses, prior research has indicated that a large number of Latinx youth still experience TDV victimization (Sabina et al., 2016).
Lastly, the onset of depressive symptoms in teen dating relationships is often associated with low life satisfaction and various forms of TDV victimization, which can lead to associating with antisocial peers and revictimization (Gagné et al., 2005; Karlsson et al., 2016). Indeed, prior research suggests the existence of a feedback loop wherein TDV may contribute to further depressive symptoms, thereby increasing risk for revictimization (Young et al., 2012). Since peer relationships are a major building block of adolescent identity formation, and adolescents with depressive symptoms are more susceptible to conforming with their peers’ attitudes and beliefs, investing research efforts in social network analyses of at-risk adolescents might help in identifying critical nodes of peers that could be trained in peer-to-peer counseling, hence preventing possibility of both depression exacerbation and justification of TDV and indirectly reducing the incidence of TDV.
Limitations and Conclusion
This study has many common limitations that future research can address. Firstly, because depression is a syndrome that includes topologies of depression, including persistent depressive disorder in contrast to major depressive disorder, future studies can include different types of depression in a model associated with peer TDV justification and TDV victimization as maintained in this study. Secondly, TDV is multifaceted, and the effects range from physical to emotional victimization; however, we only measured physical, which could serve as a limitation. Therefore, future studies can address this limitation by estimating TDV, including both constructs. Third, due to the cascade of “risky lifestyles” including adolescent substance use, delinquency, and associating with antisocial peers—that are often strongly associated with depressive symptoms and TDV victimization (Spencer et al., 2021; Temple et al., 2013), future studies should explore whether these risk factors uniquely contribute to adolescent depressive symptoms and the occurrence of physical TDV. Despite these limitations, this study provides novel results that suggest the onset of depressive symptoms could increase adolescents' likelihood of associating with peers who justify TDV, which could lead to physical TDV victimization despite controlling for relevant variables (Figure 1).
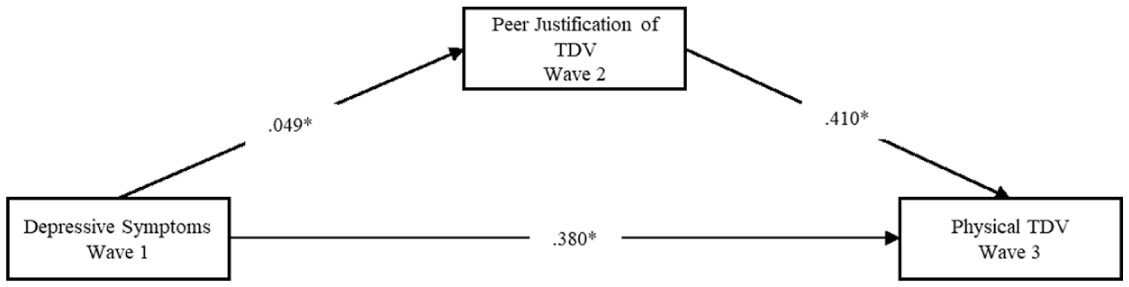
Hypothesized mediation model with coefficient magnitudes (*=statistical significance).
Footnotes
Ethical Considerations
We used secondary data from ICPSR. Therefore, we received approval from our university institutional review board (IRB) to proceed with the study.
Funding
The authors received no financial support for the research and/or authorship of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
Data are readily available upon request.