
Abstract
Intimate partner violence (IPV) victimisation is a pressing global health issue. Research suggests childhood maltreatment (CM) increases the risk of IPV in adulthood, yet gaps remain in understanding these links. Few studies examine all five types of CM and IPV, and between specific CM types (and co-occurring types) and specific IPV types. Studies seldom employ robust approaches to obtain reliable data, and few studies involve nationally representative samples, or control for co-occurring CM experiences. This study analyses data from 8,503 Australians, a nationally representative sample, who reported CM and lifetime IPV via validated tools. Logistic regression and multinomial models assessed links between each CM type and three IPV types, plus multi-type IPV. Overall, 56.8% of participants who experienced any CM experienced a type of IPV, compared to 24.4% who did not experience CM. Childhood Sexual Abuse (CSA; OR 1.9, 95% CI [1.6, 2.2]) and Childhood Emotional Abuse (CEA; OR 1.7, [1.4, 2.0]) had the strongest associations with any IPV, and with each type of IPV (CSA: OR 1.8 [1.5, 2.1] for physical IPV, 2.7 [2.2, 3.4] for sexual IPV, 1.7 [1.4, 2.0] for psychological IPV; CEA: OR 1.5 [12, 1.7] for physical IPV, 1.9 [1.4, 2.4] for sexual IPV, 1.7 [1.4, 2.0] for psychological IPV). Each type of CM was associated with individuals’ lifetime experience of all three co-occurring types of IPV; however, CSA (OR 4.6, [3.7, 5.6]) and CEA (OR 2.1, [1.7, 2.7]) were most strongly associated, followed by CPA (OR 1.9, [1.5, 2.3]). Multi-type CM, especially involving all three forms of CM involving direct acts of commission (CSA, CEA and Childhood Physical Abuse [CPA]), increased the likelihood of experiencing multi-type IPV. Findings demonstrate the need for interventions to reduce CM and address its impacts, especially in individuals who experience multiple forms of maltreatment, to reduce cycles of revictimisation.
Keywords
Introduction
Intimate partner violence (IPV) in adulthood is globally recognised as a major public health issue (Sardinha et al., 2022; World Health Organization, 2019). IPV is one of the most common forms of violence against women and causes multiple devastating effects. IPV is a leading cause of intimate partner femicide worldwide (Stöckl et al., 2014), and is strongly associated with mental health disorders (White et al., 2024), drug and alcohol problems (Stubbs & Szoeke, 2022), suicide attempts (Devries et al., 2013), and a myriad of physical health conditions (Stubbs & Szoeke, 2022). IPV remains a persistent global issue, encompassing physical, sexual, emotional, and economic abuse within intimate relationships, driven by societal norms and systemic inequalities (García-Moreno et al., 2015). Recent worldwide estimates indicate IPV is a common phenomenon (Sardinha et al., 2022); the 2018 review by Sardinha et al. found a prevalence of 27% of ever-partnered women aged 15 to 49 years who experienced physical and or sexual IPV in their lifetime (Sardinha et al., 2022).
Child maltreatment (CM) also represents a global public health concern (World Health Organization, 2024). A large body of literature has identified many long-term adverse health and behavioural consequences of CM, with sexual abuse and emotional abuse being particularly harmful over the life-course (Noll, 2021). Theoretical frameworks provide important foundations for understanding how CM may increase risk of IPV victimisation in adulthood. While the relationships between CM (and its specific types) and IPV victimisation are complex and poorly understood (Brunton & Dryer, 2024; Richards et al., 2017), theoretical work has posited diverse pathways between the experience of some types of maltreatment in childhood, and subsequent victimisation in adult intimate partner relationships (Butler et al., 2020). A prominent theoretical understanding of this association is social learning theory (Bandura & Adams, 1977), through which those who experience some types of CM may, through observational learning and operant conditioning, develop a learned expectation or acceptance of violence as a normal method of conflict resolution (Widom, 1989). A second theory is that some maltreatment types compromise secure attachment behaviours, which undermines the individual’s capacity to form healthy relationships, in turn increasing risk of revictimisation (Alexander, 2015; Bowlby, 1982). A third pathway may be related to the impact of socio-economic status and social class differences, given their correlations with some types of CM (e.g., neglect), and the likelihood that these status-based differences may involve a greater likelihood of children’s exposure to parental partnership interactions characterised by violence (Widom et al., 2014). Finally, trauma-based theories provide further insight into the mechanisms of revictimisation. In particular, experiential avoidance can limit emotional processing of prior trauma, which may inadvertently heighten risk of repeated victimisation (Bell & Higgins, 2015). Together, these frameworks underscore the multidimensional nature of CM-IPV links and guide the present study’s investigation of these associations.
Research into associations between CM and its different types and IPV victimisation is still developing (Brunton & Dryer, 2024), although empirical research indicates pathways between the two forms of victimisation (Fulu et al., 2017). A systematic review and meta-analysis of 46 studies found that four forms of CM (childhood physical abuse – CPA, emotional abuse – CEA, sexual abuse – CSA, and neglect) were significantly associated with IPV victimisation in adulthood, but that physical, psychological, and sexual abuse had stronger associations than neglect (Li et al., 2019). Several national studies have found a significant association between CM and its different types and IPV victimisation. For example, a Canadian study using 2014 General Social Survey data from 10,608 men and 11,458 women reported that CPA, CSA, and childhood exposure to domestic violence (EDV) were significantly associated with IPV victimisation in adulthood for both women and men (Shields et al., 2020). This study found that CPA, CSA, and EDV were each associated with a higher likelihood of IPV in both men and women, with CPA, CSA, or EDV having approximately twice the odds of IPV victimisation among men and women (Shields et al., 2020). A study in England and Wales of the influence of physical, sexual, and psychological abuse, and witnessing domestic violence, found each single type increased the odds of IPV victimisation, but that multi-type CM was most strongly associated with IPV (Butler et al., 2020). A United States national longitudinal study similarly found the independently predictive important role of CEA in the “cycle of violence”. In detail, the strong effect between CPA and IPV victimisation was reduced after adjusting for emotional abuse. Thus, victims of child maltreatment including CEA should be identified as a group at-risk for subsequent IPV victimisation (Richards et al., 2017). Prospective studies have also found associations between some types of CM and some types of IPV. Widom et al. (2014), for example, found that CM increased risk for the most serious forms of IPV via physical injury. Physically abused and neglected children had a higher likelihood of IPV victimisation (aOR = 2.5 and 1.6, respectively; Widom et al., 2014).
Knowledge Gaps
Emerging research indicates associations between the experience of CM and later IPV victimisation (Butler et al., 2020; Li et al., 2019; Richards et al., 2017; Shields et al., 2020). However, these studies vary widely in sampling, content, and comprehensiveness, which may explain the contradictory results characteristic of this field. A body of rigorous, comprehensive empirical evidence about the potential associations between CM and IPV has not yet been developed. Major knowledge gaps remain, which limit our understanding of which types of CM are, or are not, more strongly associated with specific types of IPV victimisation. First, much research focuses on only one or two forms of CM or collapses all types into a single variable (Kisely et al., 2024; Spencer et al., 2023). This gap in knowledge is highly significant given the qualitative differences between different types of CM and between different types of IPV, including, for example, the likelihood of differences between CM types that involve direct maltreatment of the child (physical, sexual, and emotional abuse) and those that do not (neglect, EDV between parents; Widom et al., 2014). The absence of evidence about EDV is particularly notable, given it is now recognised as a distinct type of CM (Higgins & Hunt, 2024) and has plausible potential pathways to subsequent IPV victimisation through theoretical mechanisms. The meta-analysis of 46 studies by Li et al. (2019) could only pool effects from four types of CM (CPA, CEA, CSA, and neglect) because EDV was not considered by the included studies (Li et al., 2019). The lack of research on EDV as part of the CM-IPV relationship limits our understanding of the full spectrum of how CM may influence the risk of IPV victimisation. It is vital to assess all forms of CM, since, as indicated by some studies, different forms of CM are likely to be differentially associated with IPV victimisation, and these associations can be different for women and men. The Canadian study, for example, found CPA, CSA, and childhood EDV were each associated with IPV in adulthood for women, but only CPA had a significant association for IPV in men (Shields et al., 2020). In addition, it is essential that studies should employ statistical methods to adjust for the potential confounding effect of multiple types of maltreatment in order to isolate the specific type or types of CM that produce the association with subsequent victimisation.
Second, and similarly, few studies measure all three types of IPV victimisation, including physical, sexual, and psychological violence. It is important to measure all three types of IPV because there may be different pathways between some types of CM and specific types of IPV. Research considering CM and associated psychological IPV is less developed, but psychological IPV is increasingly recognised as a distinct and important type of victimisation by leading researchers (Heise et al., 2019) and policy bodies (World Health Organization, 2019), and should not be assumed to be of lesser significance than those types having physical manifestations. Furthermore, some studies have not employed validated instrumentation to assess IPV. Third, few studies assess the association between specific types of CM and specific types of IPV. Without such nuanced analyses, we lack evidence about, for example, the distinct contribution of CSA with subsequent sexual IPV; of CPA with subsequent physical IPV; and of emotional abuse in childhood and psychological IPV. This information may assist in explaining the reasons for the association between CM and IPV victimisation, informing preventative interventions for those maltreated as children. To the best of our knowledge, no study has measured all five types of CM and their associations with subsequent IPV in all three domains, using a nationally representative sample and robust instrumentation. Fourth, few studies have assessed the influence of multi-type CM on IPV victimisation. It is well-established that few children experience only one type of child maltreatment in isolation (Higgins et al., 2023). Far more children experience two or more types of CM, and therefore it is essential that research is undertaken to consider which constellations of CM are more strongly associated with IPV victimisation.
Fifth, wide variance is evident in how studies define and measure the individual types of child maltreatment (Curtis et al., 2023). This has major consequences for the strength of the evidence generated by each study, and by the collected body of evidence. The use of accurate concepts and definitions to capture reliable, valid data about each type of child maltreatment is an essential prerequisite to generating reliable information about the association between CM and IPV, while differentiating between each type of CM. This is a challenging task requiring careful development or selection of survey instrumentation. Some approaches to the measurement of CM may employ definitions of some types of CM that are too narrow, which will inappropriately exclude some experiences of that type of CM and lead to underestimates of the association with IPV. This can occur through the selection of data source (e.g., only including a case of child maltreatment if it has been officially substantiated by a child protection agency or other authority, which will dramatically undercount actual cases), and or by employing a definition that is incongruent with conceptual models of that maltreatment type so as to truncate the appropriate scope and breadth of these experiences (e.g., limiting child sexual abuse to acts by adults, which will also dramatically undercount actual cases). Similarly, some definitions of some CM types may be too wide, and inappropriately include some non-abusive experiences as CM, thus leading to overestimates of their association with IPV. Definitional variance may explain the contradictory results found by reviews of diverse studies globally (Li et al., 2019) and in Africa (Wadji et al., 2024). Some studies have found CSA to be most strongly associated with IPV victimisation (Krause-Utz et al., 2021; Spencer et al., 2023) while others have found the strongest predictor to be CPA (Hébert et al., 2021; Schuster & Tomaszewska, 2021), CEA (LoCascio et al., 2018; Richards et al., 2017), or EDV (Bair-Merritt et al., 2013; Kerley et al., 2010; Wadji et al., 2024). In addition, discrepancies in findings often reflect broader differences in study design concerning how CM is defined and measured, for example, studies may focus on a single type of CM as opposed to a broader range of types of CM (Hébert et al., 2021). IPV measurement also varies, with some studies relying on unvalidated screening items (Hébert et al., 2021; Wadji et al., 2024). In contrast, the present study employed validated measures of both CM and IPV, capturing multiple subtypes through standardised protocols. This approach reduces definitional variability and strengthens the reliability of results relative to prior research. Sixth, a further definitional limitation exists in relation to how studies circumscribe the relational definition of “intimate partner.” Many studies limit IPV measurement to relationships between current spouses, de facto relationships, or former spouses, and exclude non-cohabiting and dating relationships (Shields et al., 2020). This is a major limitation, given the particularly strong associations between CM and IPV among dating couples (Li et al., 2019). This measurement bias may lead to underestimation of the association between CM and IPV.
Finally, few studies have considered these questions using nationally representative samples of the population. With notable exceptions, much research to date has typically employed convenience samples, or clinical samples (Kisely et al., 2024), which may overestimate family victimisation rates compared to the general population (Chan et al., 2021). These gaps therefore, constrain the capacity to understand the magnitude of the problems associated with specific types of CM for IPV victimisation, whether as first-time adult victimisation or as revictimisation in those with prior CM experiences. Additionally, these gaps hinder efforts to identify the pathways through which experiences of some types of violence in childhood can influence subsequent IPV victimisation. The Sustainable Development Goals require nations to reduce IPV (United Nations Department of Economic and Social Affairs, 2015), and this demands the generation of evidence about factors associated with IPV so that policymakers can develop targeted prevention strategies to break cycles of violence.
Current Study
This current study analysed data from the Australian Child Maltreatment Study (ACMS), which surveyed a nationally representative random sample of 8,503 participants aged 16 or older to generate the first population-wide estimates of the prevalence of all five forms of child maltreatment (Mathews, Pacella, et al., 2023). Informed by a systematic review of best practice in design of epidemiological surveys of child maltreatment (Mathews et al., 2020), and extensive conceptual and empirical testing of the study’s survey instrumentation (Mathews, Meinck, et al., 2023), the ACMS was designed to comprehensively and reliably capture the population wide prevalence of childhood physical abuse, sexual abuse, emotional abuse, neglect, and EDV (Mathews, Meinck, et al., 2023). These maltreatment experiences were captured across the entire span of childhood up to age 18, as required by best international practice (Mathews et al., 2020), and international policy (United Nations Department of Economic and Social Affairs, 2015), and reflecting the internationally-accepted definition of the age of childhood (United Nations, 1989). The ACMS also generated evidence of the prevalence of multi-type CM, namely the experience of more than one type of maltreatment, and different co-occurring combinations of maltreatment types (Higgins et al., 2023). In addition, the ACMS measured mental disorders, health risk behaviours, and a range of other outcomes, in order to analyse associations with CM and its specific types (Mathews et al., 2021). One such other outcome assessed was the lifetime prevalence of IPV victimisation, including physical, sexual, and psychological violence. This was assessed by administering the Composite Abuse Scale (Revised) – Short Form (CASR-SF), a validated measure comprising 15 items covering physical IPV (5 items), sexual IPV (2 items), and psychological violence (8 items).
Results of the population-wide prevalence of IPV, published elsewhere, revealed the widespread scale of IPV in Australia, across each type, and for multiple types (Mathews et al., 2025). More than two in five (44.8%) participants had experienced some form of IPV since age 16, and prevalence of each type was common (physical violence: 29.1%; sexual violence: 11.7%; psychological violence: 41.2%). Over one quarter of participants had experienced two or more types of IPV (28.6%), and one in 12 (8.6%) had experienced all three types (Mathews et al., 2025). Compared to men, women experienced significantly greater prevalence of each of the three types of IPV, and of multi-type IPV (including of all three types of IPV). The comprehensive and robust data generated by these components of the ACMS about both CM and IPV, facilitated a novel and thorough analysis of associations between CM and IPV victimisation going beyond prior research. To date, no nationally representative survey has examined associations between CM, and its various types (and multi-type CM in various forms), and IPV and its various types.
Research Objectives
This study aims to provide evidence on the associations between five types of CM (CPA, CSA, CEA, neglect, and EDV), and three forms of IPV (physical, sexual, and psychological) in adulthood. The purpose of this analysis is to examine the associations between distinct types of CM and IPV victimisation, as well as to identify which combinations of CM subtypes more strongly predict IPV victimisation, and especially multi-type IPV victimisation. We hypothesise that:
Exposure to any form of CM is associated with an increased likelihood of experiencing any type of IPV in adulthood.
Each specific subtype of CM-including CPA, CSA, CEA, neglect, and EDV-is positively associated with adult IPV victimisation across physical, sexual, and psychological IPV types.
Experiencing a greater number of CM subtypes (multi-type maltreatment) confers a higher risk of experiencing multiple forms of IPV (multi-type IPV) in adulthood, compared to exposure to fewer maltreatment types.
Particular combinations of CM subtypes are especially strong predictors of multi-type IPV victimisation.
Understanding these complex interrelationships can help understand pathways between different childhood experiences of maltreatment and subsequent adult IPV, thus informing clinical responses for adult IPV victims, and the development of tailored, integrated interventions to support progress toward the Sustainable Development Goals.
Materials and Methods
Data Source and Sample
The study utilised data from the ACMS, a nationally representative survey that explores childhood maltreatment experiences and various adult outcomes, including IPV. The survey sampled 8,503 participants aged 16 years and older, using random digit dial of mobile phone numbers to ensure a diverse and representative sample across gender, age, and geographic regions in Australia. The participant recruitment period ran from April 9 to October 11, 2021. A comparison with Australian census data and the 2017 Australian National Health Survey confirmed that the weighted sample was representative of the Australian population aged 16 years and older (Haslam et al., 2023). For this analysis, we focused on participants who reported ever being in a partnered relationship (whether co-habiting or not), as they were eligible to respond to IPV-related questions, in line with the World Health Organization’s definition of IPV as “violence by both current and former spouses and partners” (World Health Organization, 2022). The final analytic sample comprised 7,022 respondents.
Measures
Lifetime IPV: The primary outcome variable, lifetime IPV exposure, was assessed using 15 behaviourally specific items derived from the CASR-SF. These items captured three forms of IPV: five items measured physical violence, two measured sexual violence, and eight assessed psychological violence (Ford-Gilboe et al., 2016). To capture the spectrum of IPV experiences, we created an IPV pattern variable that categorised respondents based on the presence or absence of these forms of IPV. The IPV pattern variable included eight categories: no IPV, sexual IPV only, physical IPV only, physical and sexual IPV, psychological IPV only, psychological and sexual IPV, psychological and physical IPV, and all three forms of IPV. The CASR-SF was selected over the more widely used Revised Conflict Tactics Scales (CTS-2) because it provides a concise, psychometrically robust measure of multiple IPV dimensions while minimising participant burden-an essential consideration given the study’s extensive assessment battery and pilot feedback on administration time. Economic violence was not included due to the absence of validated CASR-SF subscales and the lack of brief, psychometrically sound items suitable for inclusion without substantially increasing burden; this exclusion is acknowledged as a limitation.
Childhood Maltreatment: Following best practice principles for CM surveys (Mathews et al., 2020), all five forms of childhood maltreatment were assessed over the entire span of childhood to age 18. The survey instrumentation – named the Juvenile Victimisation Questionnaire (JVQ)-R2: Adapted Version (ACMS) – was based on the JVQ-R2, with some modifications which were carefully tested and validated through a five-stage process detailed elsewhere (Mathews, Meinck, et al., 2023). The survey employed behaviourally-specific questions with dichotomous Yes/No response options in order to comprehensively and reliably capture self-report data about experiences of CM. To ensure prevalence estimates were neither overestimated nor underestimated, each question was tested for congruence with robust conceptual models of the respective maltreatment types, for CPA (World Health Organization, 2006), CSA (Mathews & Collin-Vézina, 2019), CEA (Kairys & Johnson, 2002), neglect (Dubowitz et al., 2005), and EDV (MacMillan & Wathen, 2014).
In total, 16 screener items captured information on the five types of CM. CPA (by parents or parent-like adult caregivers) was measured with two items assessing moderate abuse (e.g., being hit or punched) and severe abuse (e.g., being beaten up, choked, or burned). CEA by parents was measured through three items covering hostility/denigration, rejection, and emotional unavailability. CSA (by any person) was measured using four items measuring non-contact sexual exhibitionism or voyeurism, sexual touching, attempted forced intercourse, and completed forced intercourse. Neglect was assessed by three items about environmental neglect, nutritional or physical neglect, and medical neglect. EDV was measured using four items, about seeing or hearing physical violence between parents, threatened physical violence between parents, property damage in the course of a parental argument, and diverse forms of coercive intimidation or control. Congruent with conceptual models of CM, for physical abuse, sexual abuse, and EDV, any endorsement was counted as a case of that type of CM, regardless of how many times it happened. For emotional abuse, and for neglect, participants who endorsed items were asked over what period of time it occurred, with response options of days, weeks, months or years; endorsed items were only counted as a case of CEA or child neglect respectively if it occurred over a period of at least weeks. The chosen instrument was preferred over others, such as the Childhood Trauma Questionnaire, as it better captured the nature and various manifestations of all five maltreatment types, including neglect subtypes and EDV (Mathews et al., 2020). To preserve feasibility, some piloted screeners (e.g., educational neglect, supervisory neglect, sibling domestic violence) were excluded, and emotional abuse and emotional neglect were combined into a single category – a limitation given that these distinct forms may differentially influence IPV risk. Overall, these methodological decisions balanced psychometric rigour, participant burden, and feasibility in a large-scale survey while acknowledging limitations related to the measurement of economic violence and specific CM subtypes (Mathews, Meinck, et al., 2023).
Sociodemographic factors: Key demographic factors were controlled as potential confounders, including age, gender, childhood financial hardship, and current financial strain. Participants were grouped into three age categories: 16 to 24 years (3,500 participants), 25 to 44 years (2,000 participants), and 45 years and older (3,000 participants). The ACMS age groups reflect key developmental stages relevant to CM and IPV, represent broad generational trends, and provide sufficient numbers for statistical power. Individuals aged 16 to 24 constitute those in adolescence and early adulthood, when IPV often emerges in dating contexts and early relationships. Those aged 25 to 44 represent individuals in adulthood with additional relationships, including more long-term partnerships. Those aged 45 and older cover midlife and beyond. These groupings enable analysis of the extent to which CM and IPV associations are evident across life stages, and inform insights into prevention and service needs for different populations (Haslam et al., 2023). Gender was categorised into three groups: men, women, and diverse gender identities, based on a list of 14 response categories. Childhood financial hardship was assessed through a Likert scale question: “How often did your family struggle to provide food, medical care, or other basic necessities?” Current financial strain was measured with a binary question: “In the past 12 months, has your household been unable to meet its basic needs?”. Detailed measurement information is available in the ACMS protocol (Haslam et al., 2023; Mathews et al., 2021).
Statistical Analysis
All statistical analyses were conducted using SAS software (version 9.4) (SAS Institute Inc., Cary, NC, USA), with a significance threshold set at p = .05 for all tests. Visualisations were generated using Stata 17. Survey-weighted prevalence rates for each form of IPV were calculated based on respondents’ experiences of five forms of childhood maltreatment (no maltreatment, any child maltreatment, any CPA, any CEA, any CSA, any EDV and any child neglect), with results stratified by gender and age group. It is important to clarify that CPA does not refer to those who only experienced physical abuse and no other CM type, but encompasses “any physical abuse,” including individuals who may have also experienced CSA, EDV, CEA, or child neglect. This approach extends to each CM type, and therefore the distinct categories represent potentially overlapping, not mutually exclusive, groups, which is essential to understanding the subsequent analyses. The Rao-Scott χ² test with a second-order correction for survey data was used to assess differences in prevalence by gender and age groups, and 95% confidence intervals were calculated using Taylor series expansion (Wolter, 2007). To estimate the relationship between CM and IPV patterns, we fitted multivariable logistic regression models. These models provided adjusted odds ratios (AORs) for the association between the IPV pattern variable and five types of childhood maltreatment. Two adjustment models were specified: a simple model adjusting for gender and socio-economic status (SES) only, and a full model that included additional controls for age group, childhood family financial hardship, current financial strain, and SES based on postcode of residence and quintiles of the Index of Relative Socio-Economic Disadvantage. These control variables were selected because gender and SES are well-established confounders influencing both childhood maltreatment exposure and IPV risk. Age group accounts for developmental differences in IPV patterns, while financial hardship variables capture economic stressors known to increase vulnerability to both maltreatment and IPV. SES further controls for contextual socio-economic influences (Haslam et al., 2023). To model and visualise the relationship between patterns of IPV and various predictor variables, including CM patterns, gender, and age groups, we fitted multinomial logistic regression models, using the generalised logit link function, to account for the different categories of the response variable (absence or presence of three forms of IPV). These models generated predictions for all possible combinations of the three forms of IPV. We calculated the corresponding predicted probabilities. These relationships are visualised in graphical form to understand how different forms of CM influence the IPV pattern in adulthood. Three multinomial logistic models were fitted in three patterns of CM (a) all five forms of CM, (b) four forms of CM (excluding EDV) and (c) three forms of direct CM (excluding EDV and child neglect). Model diagnostics were assessed via Likelihood Ratio Test, Goodness-of-Fit, Variance Inflation Factors for Multicollinearity.
Ethics Statement: The study protocol was approved by the Queensland University of Technology Human Research Ethics Committee [#1900000477]. Informed consent was obtained from all participants. Each survey respondent provided verbal informed consent to participation.
Results
Among the 8,503 participants, 7,022 (82.6%) reported having ever been in a partnered relationship. Figure 1 presents the weighted prevalence rates of lifetime IPV among participants with a history of five different forms of CM, stratified by gender. The prevalence of IPV was significantly higher among individuals who experienced CM across all subtypes, compared to those without a history of CM, with women who experienced CM victimisation reporting higher rates of IPV than men.
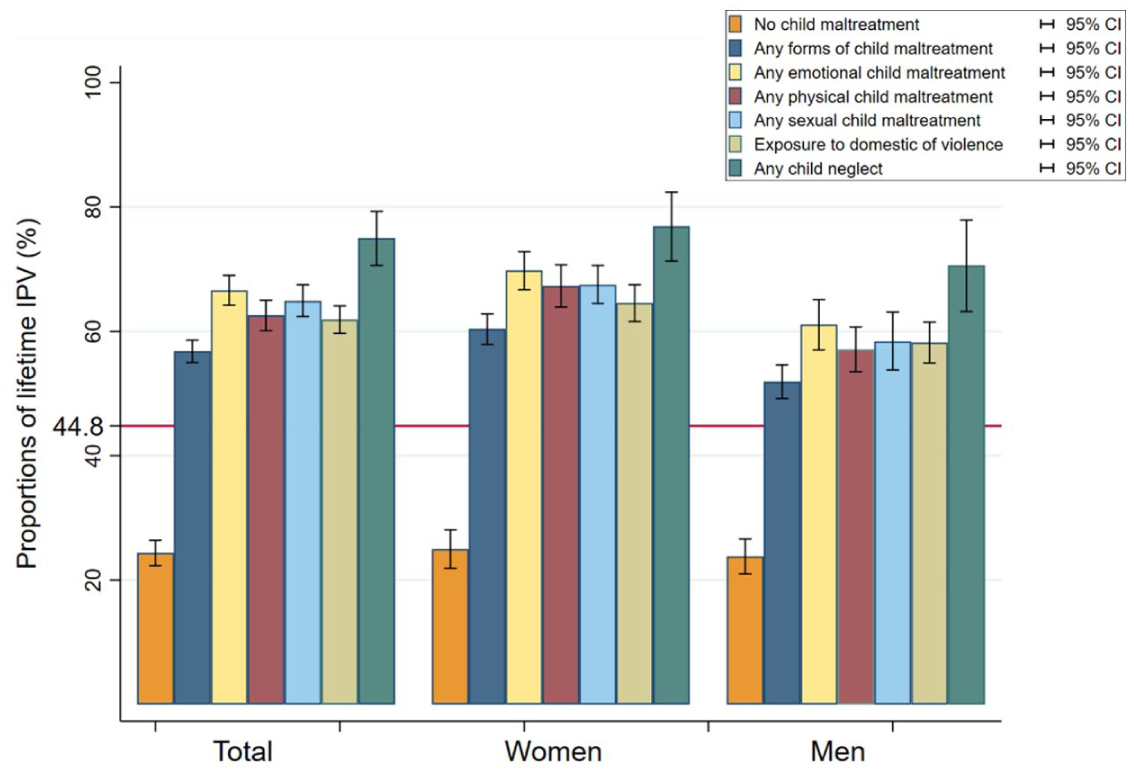
Weighted proportion of participants reporting lifetime experience of any IPV among those who have ever been partnered and experienced any CM subtypes, by men and women.
Prevalence of any IPV among people who experienced any CM: Figure 1 shows the overall descriptive significant differences in any IPV victimisation, comparing all participants who experienced any CM (56.8%) and those with no CM (24.4%). The red line at 44.8% indicates the prevalence of any IPV in the Australian population (Mathews et al., 2025). There was also a significant difference in IPV victimisation by gender: 60.4% of women who experienced any CM reported IPV, compared to 51.9% of men. In contrast, among those without CM, 25.0% of women reported IPV compared to 23.8% of men.
Prevalence of any IPV by specific types of CM: Figure 1 demonstrates the weighted prevalence of participants who experienced any IPV, specific type of CM: CEA 66.6%; CPA 62.6%; CSA 64.9%; EDV 61.9%; neglect 75.0%. Females and individuals with diverse gender identities who experienced any form of CM subtypes (except child neglect) have a greater prevalence of lifetime IPV than male participants.
Prevalence of any CM by specific types of IPV: Table 1 shows the overall descriptive significant difference in any CM and different forms of IPV. Those who experienced any CM had a higher prevalence of IPV subtypes compared to those who did not. For example, physical IPV victimisation was reported by 37.5% of people with any CM, compared to 14.7% of those without CM; sexual IPV victimisation was reported by 16.5% with any CM, compared to 3.7% without CM; and psychological IPV victimisation was reported by 52.7% of those with any CM, compared to 21.7% without CM. Significant differences were also observed by gender and age group (Supplemental File, Table 1).
Weighted Proportion of Participants Reporting Lifetime Experience of Any IPV Among Those Who Have Ever Been Partnered, by Any CM, CM Subtypes, Age, and Gender (n = 7,022*).
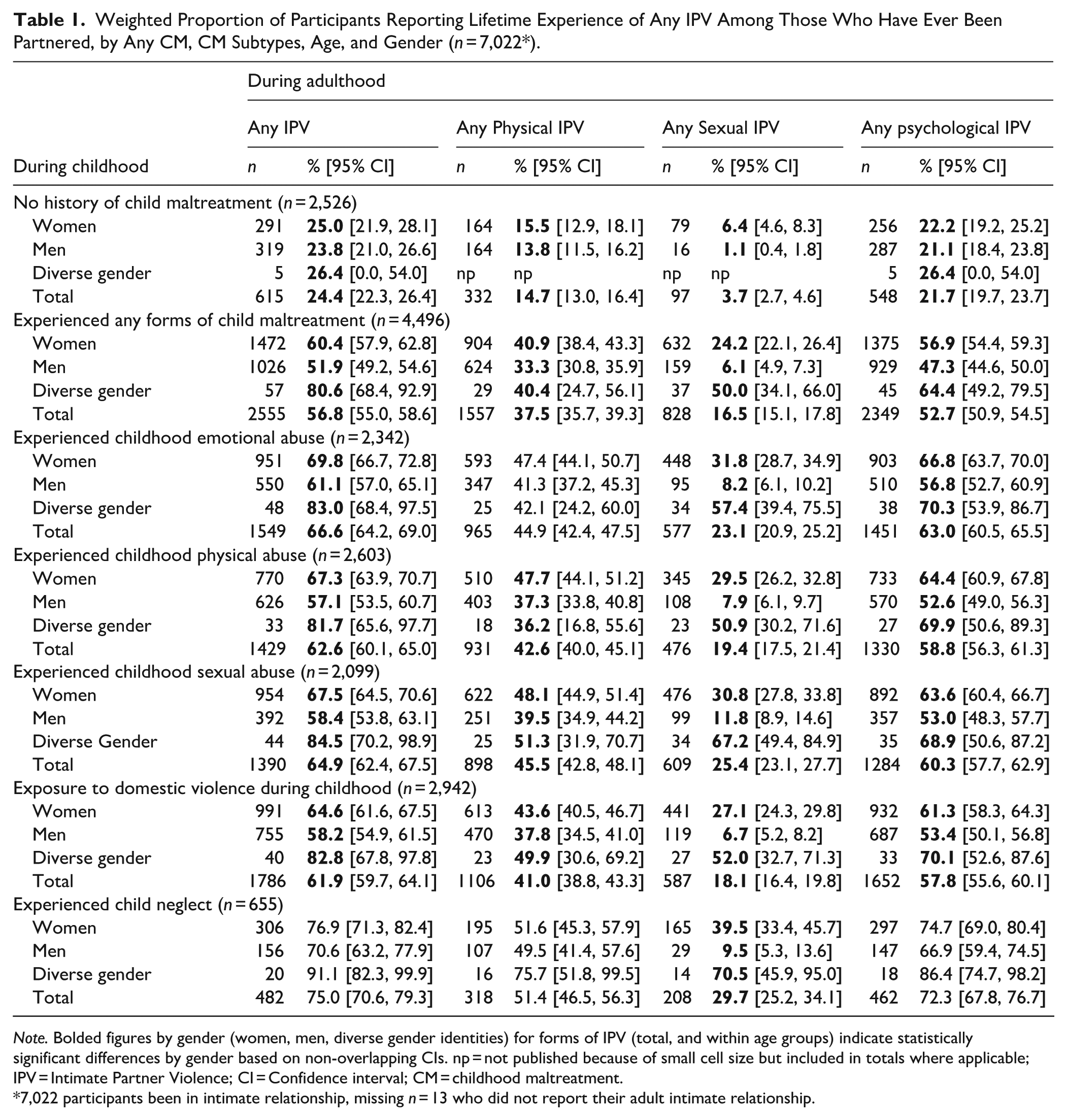
Note. Bolded figures by gender (women, men, diverse gender identities) for forms of IPV (total, and within age groups) indicate statistically significant differences by gender based on non-overlapping CIs. np = not published because of small cell size but included in totals where applicable; IPV = Intimate Partner Violence; CI = Confidence interval; CM = childhood maltreatment.
7,022 participants been in intimate relationship, missing n = 13 who did not report their adult intimate relationship.
Prevalence of specific types of CM by specific types of IPV: Psychological abuse was the most common form of IPV experienced by the majority of people with experiences of each form of CM: CEA (63%), CPA (58.8%), CSA (60.3%), neglect (72.3%), and EDV (57.8%). Sexual IPV was greater among those who experienced child neglect (29.7%), CSA (25.4%), CEA (23.1%), CPA (19.4%) and EDV (18.1%). Those who experienced child neglect, and sexual abuse had the highest prevalence of physical IPV (51.4% and 45.5% respectively), followed by child physical or emotional abuse (approx. 42%) and EDV (41%) (Table 1). No significant differences were observed for EA/PA and any IPV prevalence based on whether the perpetrator was the mother or father. Further details on the prevalence of lifetime IPV and specific types of IPV by different CM perpetrator types can be found in Supplemental File, Table 2.
Association between any CM and any IPV/ specific types of IPV: Multivariable logistic regression models (Table 2) were used to examine the relationship between any form of CM, its five subtypes, and various forms of IPV. After adjusting for age, gender, SES, and financial hardship, the findings revealed that experiencing any form of CM significantly increased the likelihood of experiencing any form of IPV (aOR = 1.3, 95% CI [1.1, 1.6]). Although the association between CSA and any IPV had the greatest point estimate (aOR = 1.9, [1.6, 2.2]), all associations had overlapping CIs, suggesting non-significant differences in the strengths of associations for CEA (aOR = 1.7, [1.4, 2.0]), EDV (aOR = 1.6, [1.3, 1.8]), child neglect (aOR = 1.5, [1.1, 1.9]), and CPA (aOR = 1.4, [1.2, 1.6]). Importantly, SES and financial hardship did not significantly impact the associations between CEA, EDV, and any IPV.
Odds Ratios for Each Type of IPV, by Five Forms of Child Maltreatment, Controlling Other Confounders.
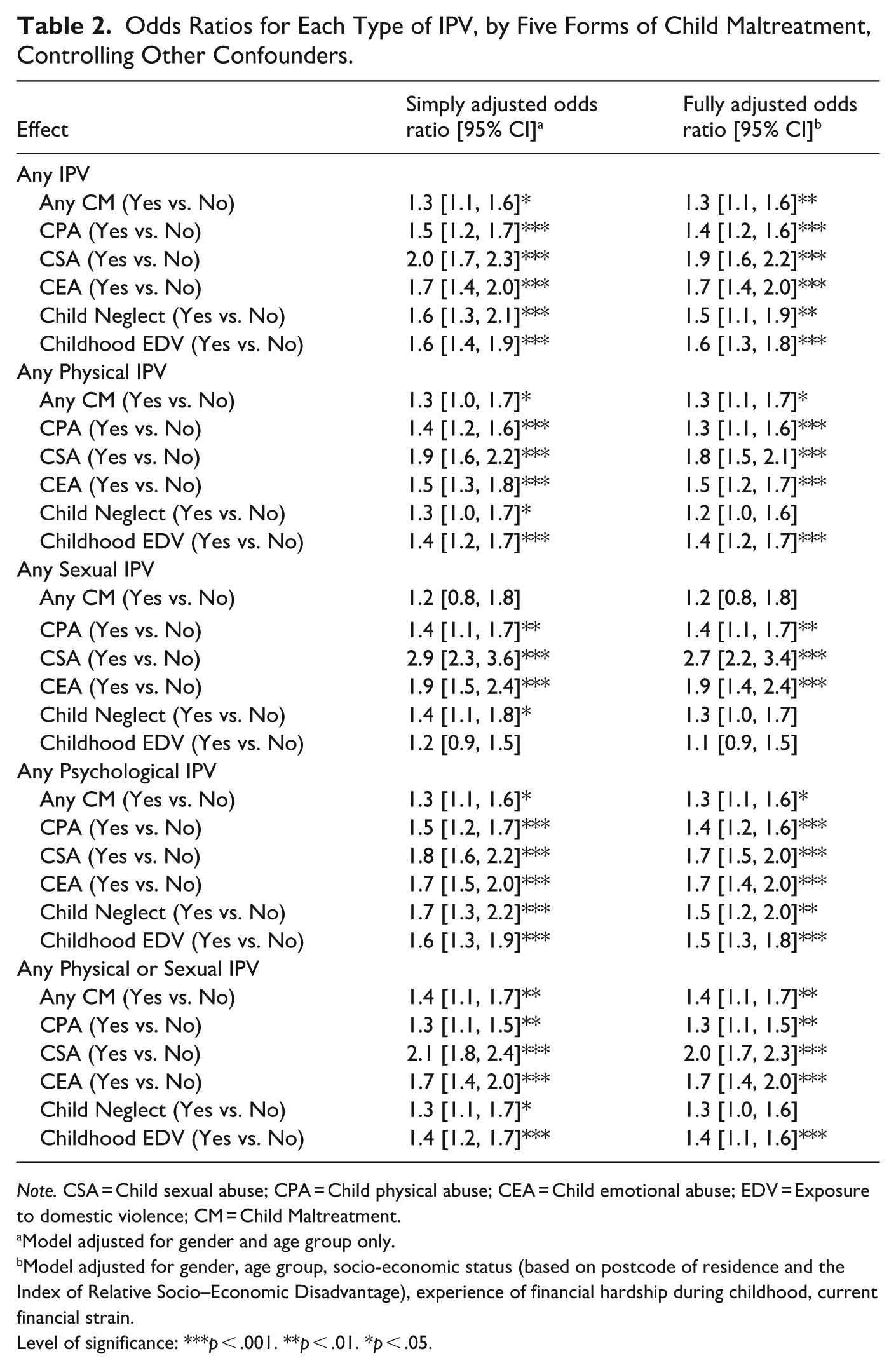
Note. CSA = Child sexual abuse; CPA = Child physical abuse; CEA = Child emotional abuse; EDV = Exposure to domestic violence; CM = Child Maltreatment.
Model adjusted for gender and age group only.
Model adjusted for gender, age group, socio-economic status (based on postcode of residence and the Index of Relative Socio–Economic Disadvantage), experience of financial hardship during childhood, current financial strain.
Level of significance: ***p < .001. **p < .01. *p < .05.
Association between specific types of CM and specific types of IPV: The association between specific types of CM and specific types of IPV shows that CSA and CEA are strongly and significantly associated with multiple specific types of IPV (Table 2). Individuals who experienced CSA were more than twice as likely to experience sexual IPV (OR = 2.7, 95% CI [2.2, 3.4]) and almost twice as likely to experience physical IPV (OR = 1.8, [1.5, 2.1]) and psychological IPV (OR = 1.7, [1.5, 2.4]).any Those who experienced CSA were significantly more likely to experience sexual IPV compared to those who experienced CPA, EDV or neglect. Child neglect was associated with increased odds of experiencing any form of IPV, particularly psychological IPV, while EDV was specifically related to physical and psychological IPV. EDV also showed an association with IPV revictimisation, although it was weaker and not significant for sexual IPV, while child neglect did not produce significant associations with IPV subtypes except for psychological IPV (aOR = 1.5, [1.2, 2.0]).
Association between each and multiple specific types of CM and each and multiple specific types of IPV: Table 3 presents the results of multinomial logistic regression models estimating the likelihood of experiencing multiple specific types of IPV based on CM exposure, while controlling for demographic confounders. Model 1 examines the influence of five forms of CM, Model 2 excludes EDV, and Model 3 focuses on three direct forms of CM, excluding both EDV and child neglect. The ORs in Model 1 are slightly lower than those in Models 2 and 3, but the patterns and associations remain consistent across the three models. Experiencing any form of CM significantly increased the risk of a participant experiencing all three forms of IPV victimisation in adulthood. This pattern of ORs suggests strong associations between multi-type CM and the likelihood of experiencing various forms of IPV later in life (Supplemental File, Table 3). CSA consistently shows a strong association with all three forms of IPV, particularly sexual IPV alone (aOR = 2.8, 95% CI [1.7, 4.4]) and sexual IPV combined with physical or psychological IPV (OR = 4.4). The fully adjusted OR for CSA and all three forms of IPV is 4.8, [3.9, 5.9], with SES and financial hardship not significantly altering these results. This association is notably stronger than that observed for CEA/CPA.
Interconnection Between Three Forms of IPV by Different Combinations of Five Forms of Child Maltreatment, Generated From Multi-Nominal Logistic Regression Models.
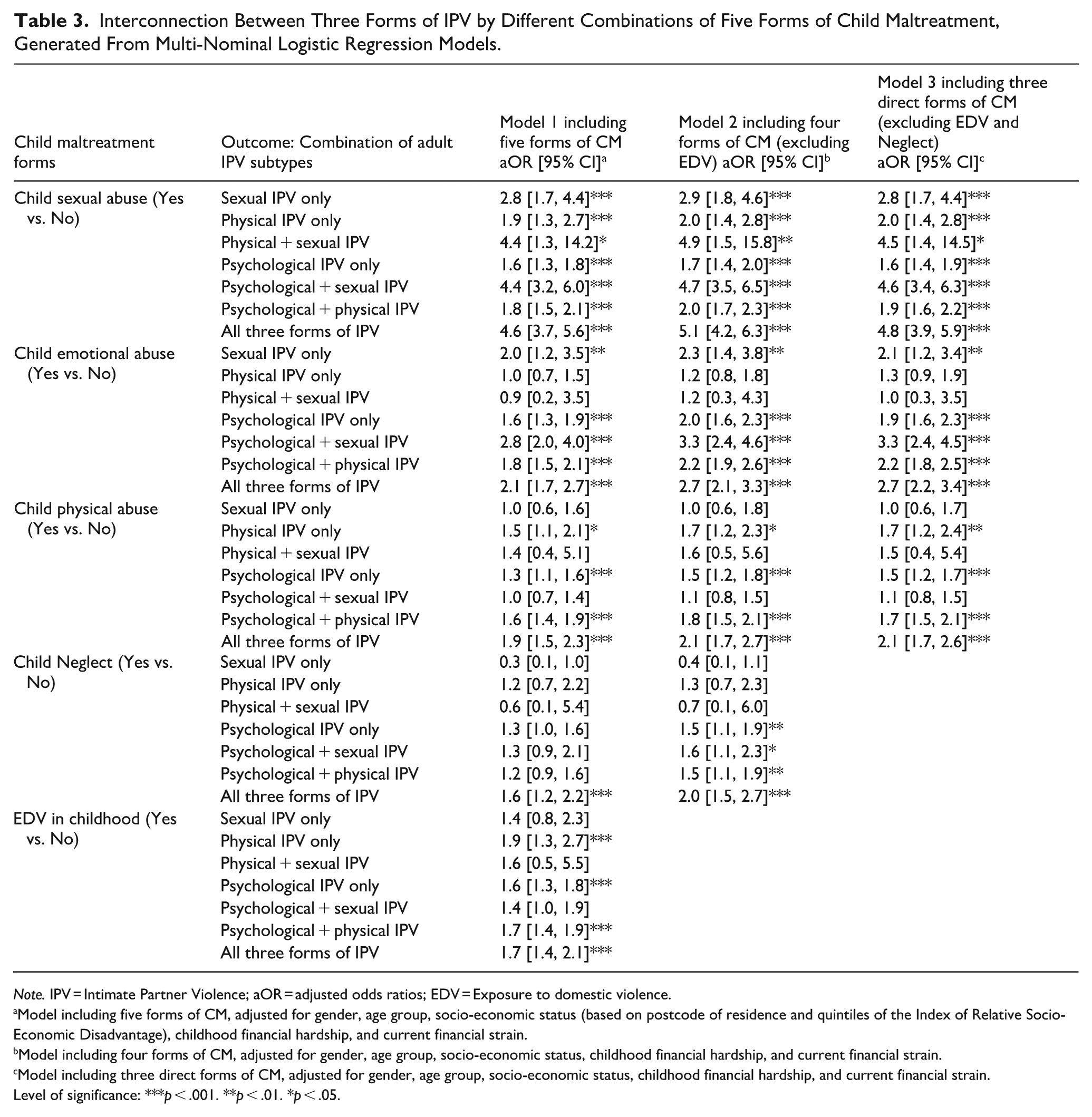
Note. IPV = Intimate Partner Violence; aOR = adjusted odds ratios; EDV = Exposure to domestic violence.
Model including five forms of CM, adjusted for gender, age group, socio-economic status (based on postcode of residence and quintiles of the Index of Relative Socio-Economic Disadvantage), childhood financial hardship, and current financial strain.
Model including four forms of CM, adjusted for gender, age group, socio-economic status, childhood financial hardship, and current financial strain.
Model including three direct forms of CM, adjusted for gender, age group, socio-economic status, childhood financial hardship, and current financial strain.
Level of significance: ***p < .001. **p < .01. *p < .05.
CEA and CPA also show significant associations with IPV, particularly psychological and/or physical IPV. The fully adjusted OR for CEA and all three forms of IPV is 2.7, 95% CI [2.2, 3.4], and for CPA, it is 2.1, [1.7, 2.6], with SES and financial hardship having no significant effect on these relationships. Childhood EDV is generally associated with an increased risk of most forms of IPV, particularly physical and psychological IPV (aORs ranging from 1.6 and 1.9), but the association is non-significant for sexual IPV (aOR = 1.4, 95% CI [0.8, 2.3]). Child neglect exhibits a less consistent pattern, with no significant independent associations after controlling for other child maltreatment types across most IPV subtypes (aORs ranging from 0.4 to 1.3), although it shows some significant associations with psychological IPV (aOR = 1.5, 95% CI [1.1, 1.9]) and all three forms of IPV combined (aOR = 2.0, [1.5, 2.7]).
Association between the experience of multi-type CM and IPV victimisation: Figure 2 illustrates the model predicted percentages of individuals who experienced each of the eight adult IPV patterns (none, individual types of IPV, and combinations of IPV types), demarcated by their exposure to the eight possible combinations of the three types of direct childhood maltreatment (none, individual types of CM, and combinations of CM types, including CPA, CSA, and CEA). The IPV risk followed a consistent pattern across gender and age groups, with the highest likelihood of experiencing all three forms of IPV observed among participants exposed to all three types of direct CM, ranging from 12.4% to 38.0% across different age groups and gender. This was followed by those who experienced a combination of two types of direct CM (e.g., CPA + CSA; CEA + CSA; and CEA + CPA), where the percentages ranged from 3.9% to 26.3%. Participants who experienced only one type of direct CM had a likelihood of 1.8% to 16.0%. In stark contrast, participants with no history of CM exhibited only a 0.9% to 4.6% predicted prevalence of experiencing all three types of IPV victimisation (Figure 2; Supplemental File, Table 3). Notably, IPV was strongly associated with CSA, then CEA and CPA, with a higher percentage of IPV among those who experienced a combination of two of these types of direct CM (e.g., CSA + CPA, CEA + CSA, CEA + CPA). Furthermore, the comparisons between genders and age groups underscore the heightened vulnerability to IPV of young women who experienced multiple types of CM. For example, among women aged 16 to 24 who experienced all three direct types of CM (CPA, CSA, and CEA), approximately 38% experienced all three types of IPV in adulthood by age 24 (physical, sexual, and psychological IPV). In comparison, the corresponding percentage for men in the same age group is significantly lower, at approximately 17.6%. Similar patterns on the associations between the five forms of childhood maltreatment and the three forms of IPV are indicated in Supplemental File.
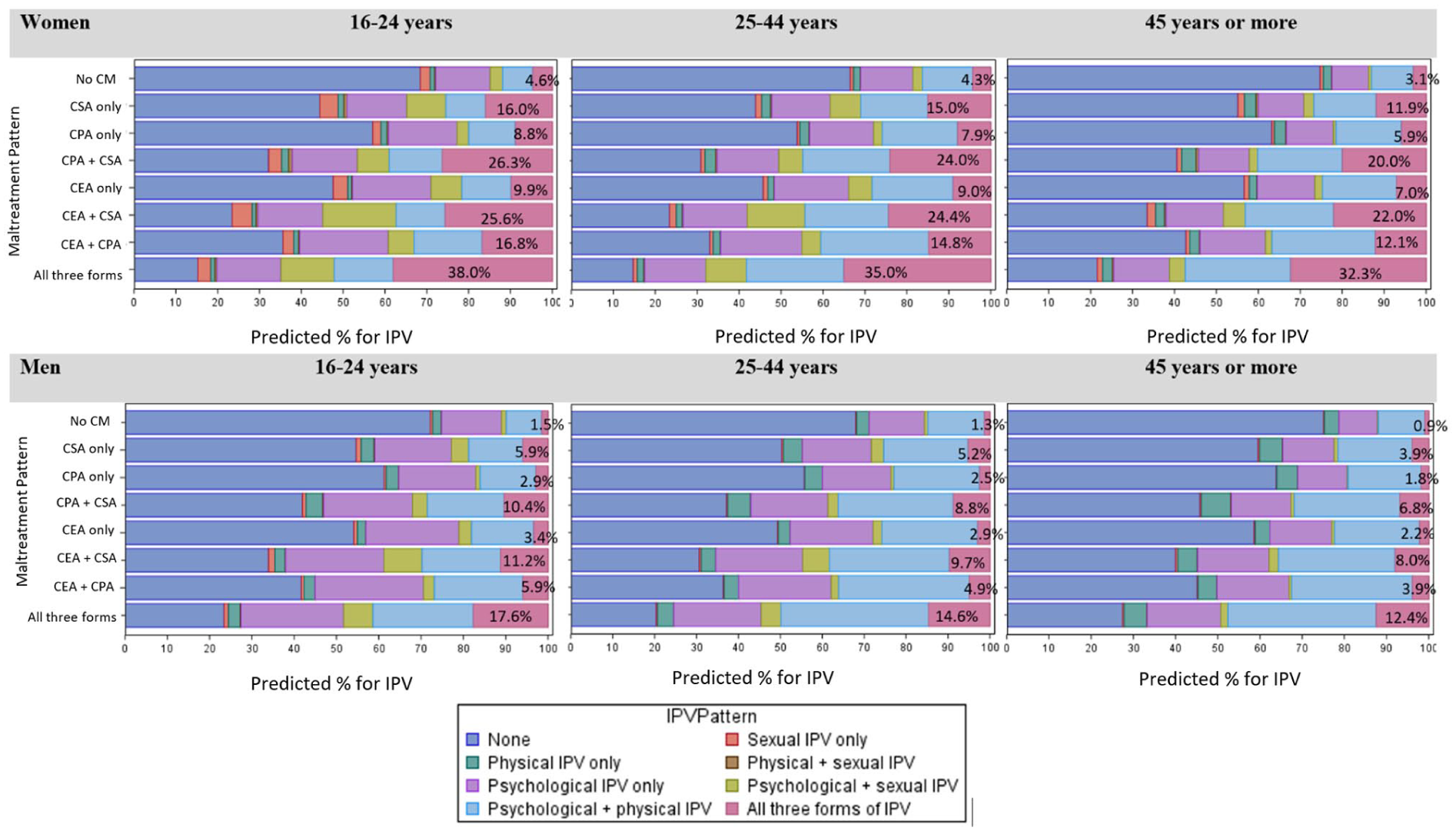
Association between the experience of multi-type CM and IPV victimisation by gender and age groups.
Discussion
This study elucidates the diverse and complex relationships between different forms of childhood maltreatment and subsequent IPV victimisation. Our analyses help to further explain and add nuance to previous research, especially by clarifying the qualitative differences between different CM types, and accordingly their different influence on and potential pathways to subsequent victimisation. Some but not all CM types are strongly associated with IPV, with specific types of IPV, and with all three co-occurring types. Findings underscore the importance of tailored interventions and prevention strategies targeted at specific types of CM, and specific types of IPV. Five major findings emerged from our analysis.
Child maltreatment is strongly associated with IPV victimisation: The first major finding is that experiencing CM significantly increased the likelihood of IPV victimisation. Overall, 56.8% of participants who experienced CM had experienced IPV, compared with only 24.4% of participants who did not experience CM. This association was strong across genders: 60.4% of women who experienced CM had experienced IPV compared to 25.0% who did not; 51.9% of men who experienced CM had experienced IPV compared to 23.8% who did not. Among participants with diverse gender identities, the likelihood was even higher (80.6% vs. 26.4%), although small cell sizes require caution in interpretation. Moreover, this association was found across age groups. For example, among those aged 16 to 24, 63.4% of women who experienced CM had experienced IPV compared to 24.3% who did not; among women aged 25 to 44, 64.7% of women who experienced CM had experienced IPV compared to 28.0% who did not. Fully adjusted, CM increased the odds of experiencing any IPV by 1.3, with SES and financial hardship in childhood not affecting this higher likelihood. This first finding is consistent with other research, but also identifies the overall extent of this relationship, its crystallisation in early adulthood, its application across genders, and the persistence of the relationship despite socio-economic differences.
Multi-type direct CM is strongly associated with various types of IPV, and with multi-type IPV: The second major finding is that there is a strong relationship between multi-type CM, and between specific combinations of CM types experienced, and the likelihood of experiencing multiple forms of IPV in adulthood. Individuals who experienced multiple forms of CM had far higher odds of experiencing all three forms of IPV. This was especially evident for those who experienced all three direct forms of CM – CSA, CEA, and CPA – among whom the prevalence of experiencing all three forms of IPV ranged from 12.5% to 38.0% among different age groups and genders. In contrast, participants who experienced only one form of CM were far less likely to experience all three forms of IPV (ranging from 1.8% to 16.0% among different age groups and genders). The significant and immediate impact of experiencing multiple forms of direct CM can be seen among women aged 16 to 24 who experienced all three direct forms of CM (emotional, physical and sexual abuse), where approximately 38% experienced all three types of IPV by age 24.
This finding suggests the cumulative impact of different types of direct CM experiences may have a dose effect in accelerating the various pathways between specific types of direct victimisation in childhood and subsequent victimisation in adult intimate relationships. Multiple types of five forms of CM is very common in Australia, with two in five people experiencing two or more CM types, and one in four experiencing three or more types (Higgins et al., 2023). The finding of this current study reinforces and extends previous research (Butler et al., 2020), and suggests that those who experience multi-type CM, especially where this experience involves all three types of direct child maltreatment, are not only at heightened risk of experiencing any IPV, but are at significantly heightened risk of experiencing all three types of IPV. This significant outcome has major implications for prevention policy, since the experience of cumulative violence in both childhood and adulthood is highly likely to produce intensified adverse outcomes.
Child Sexual Abuse is the Form of CM Most Consistently Associated With All Forms of IPV
Our statistical modelling provides further nuance to the first two findings by identifying which specific CM types hold particular salience for IPV victimisation. Multivariable and multinomial logistic regression showed that of all five CM types, experiencing any CSA was most consistently associated with any IPV (OR 1.9), and with multiple specific types of IPV victimisation (OR 1.8 for physical IPV, 2.7 for sexual IPV, and 1.7 for psychological IPV). CSA was also most strongly associated with the subsequent experience of all three co-occurring types of IPV, increasing this likelihood by an odds ratio of 4.6.
These findings are consistent with previous studies which indicate the strong developmental pathway between CSA and IPV victimisation among both men and women (Hébert et al., 2021; Schuster & Tomaszewska, 2021), and extend other work (Shields et al., 2020). The elevated strength of the relationship between CSA and IPV victimisation may be attributable to the unique traumagenic impacts of CSA which differ from and exceed those of other CM types (Noll, 2021). These traumagenic impacts can foster long-lasting psychological vulnerabilities through feelings of betrayal, powerlessness, and stigmatisation, which may increase the likelihood of entering and remaining within abusive relationships in adulthood (Finkelhor & Browne, 1985). Sequelae of CSA, including mental disorders and risk behaviours, may elevate the risk of isolation and vulnerability to abusive victimisation in adult intimate relationships. Altered emotional-cognitive processing and maladaptive emotion regulation mediate the association between CSA and sexual IPV victimisation (Hébert et al., 2021). Similarly, CSA survivors are more prone to physical and psychological IPV due to maladaptive coping strategies and attachment issues stemming from early trauma (Vaillancourt-Morel et al., 2023). Maladaptive emotion regulation (e.g., self-blame) significantly hampers CSA victims from seeking social support and disclosing their perpetrators (Kellogg et al., 2020), making them more vulnerable to sexual and other IPV victimisation in romantic relationships (Krause-Utz et al., 2021). Furthermore, women with a history of CSA report heightened risks of sexual dysfunction, including negative cognitive associations with sexuality and body image issues, which impede their ability to navigate adult relationships and cope with sexual IPV (Zerubavel et al., 2018). The markedly higher odds of experiencing sexual IPV for those exposed to any CSA, compared to other forms of CM, emphasise the need for targeted intervention strategies addressing the severe long-term impacts of CSA.
Childhood Emotional Abuse is Also Strongly Associated With IPV Victimisation
After any CSA, any CEA was the most powerful predictor of IPV, being strongly associated with any IPV (OR 1.7), and with multiple specific types of IPV victimisation (OR 1.5 for physical IPV, 1.9 for sexual IPV, and 1.7 for psychological IPV). CEA was also strongly associated with the subsequent experience of all three co-occurring types of IPV, increasing this likelihood by an odds ratio of 2.1. Our findings about the impact of CEA relative to other CM types are broadly consistent with others (LoCascio et al., 2018; Richards et al., 2017).
Our finding about the importance of CEA for subsequent IPV can plausibly be explained by considering likely pathways. Properly understood, CEA involves repeated interactions by a child’s parent(s) that convey to the child they are worthless, unloved, unwanted, or only of value in meeting another person’s needs (Kairys & Johnson, 2002). An extensive body of theory has posited that CEA undermines secure attachment to one or both parental caregivers, which is essential for healthy development (Riggs, 2010; Riggs & Kaminski, 2010). A common consequence of CEA is attachment anxiety, in which the child lacks self-worth, and fears abandonment, with consequent erosion of the child’s feeling of security and safety, of the child’s capacity to regulate emotion (e.g., awareness of emotions, securing emotional clarity, and impulse control; Christ et al., 2019). Emotionally abused children often experience chronic low self-esteem (Zhang et al., 2022), particularly among women (Willis & Yates, 2023). Often, the child will also internalise the parent’s negative attributions, and develop negative cognitive models all of which can catalyse harmful coping mechanisms and mental disorders including depressive disorder and anxiety disorders (Schlensog-Schuster et al., 2024).
These prominent outcomes of CEA produce a high potential to contribute to a cycle of revictimisation in intimate adult relationships. Reviews show that CEA compromises general wellbeing in intimate relationships (Cao et al., 2022), and is associated with higher IPV victimisation (Li et al., 2019). The myriad effects of CEA on development, attachment, health and behavioural disorders, increases the likelihood of entering and remaining within abusive relationships (Pereira et al., 2020). The emotional scars left by CEA – particularly in terms of emotion dysregulation and maladaptive coping strategies – create distinct pathways that elevate the risk for multiple forms of IPV later in life.
Childhood EDV and its Differential Associations With IPV Victimisation
Experiencing any childhood EDV increased the likelihood of experiencing physical and psychological IPV in adulthood, although not as strongly as CSA, CEA, and CPA. This finding aligns with studies highlighting the direct association between EDV and later IPV victimisation (Bair-Merritt et al., 2013; Kerley et al., 2010; Wadji et al., 2024), particularly in teen dating violence for physical and economic abuse (Cheung & Huang, 2023). Explanations for theoretical pathways between these experiences and outcomes are consistent with social learning theory, in which the modelling of parental behaviour has influenced children’s internalisation of the violent dynamics they witness, perceiving such abusive behaviours as justified or normal in relationships. A recent systematic review concluded that children who witness IPV between their parents tend to have stronger beliefs that the use of violence in intimate relationships is acceptable (Evans et al., 2022). In addition, this finding is consistent with trauma theory, whereby early exposure to violence and accompanying feelings of fear and helplessness can disrupt brain development and neural functioning, impairing the individual’s ability to form secure attachments and increasing vulnerability to physical and psychological IPV by affecting emotional regulation, social functioning, and cognitive processing, which are key factors in maintaining healthy intimate relationships (Howell et al., 2016; Wadji et al., 2024). Our finding that EDV was not as strongly associated with IPV victimisation compared with direct CM types (physical abuse, sexual abuse, and psychological abuse) is explicable by its nature as indirect maltreatment, whereas the other forms are acts directed specifically towards the child and therefore plausibly have more profound effects.
Child Neglect is Not Strongly Associated With IPV
This study found neglect is neither clearly nor strongly associated with IPV. Relative to the other four types of CM, experiencing any neglect was the least strongly associated with IPV, and results of several analyses showed no association. These findings are consistent with those of the systematic review which found very few significant associations between neglect and IPV victimisation (Li et al., 2019). This finding is explicable because of the nature and lived experience of neglect, and its qualitative differences from other CM types, especially of direct forms. Neglect, as translated to the child’s functional home environment, availability of meals and clothing, and provision of medical care, is largely attributable to socio-economic circumstances, as experienced by the child’s parents and as influenced by broader social and structural forces (Drake & Jonson-Reid, 2014). These inconsistencies may arise from the heterogeneous nature of neglect, its conceptual and measurement challenges, previous studies not measuring all forms of child maltreatment and therefore not being able to identify the contribution of each to IPV, and the connection between neglect socio-economic adversity, which itself influences IPV risk. Unlike direct forms of CM, being physical, sexual and emotional abuse, most neglect does not involve acts directed specifically against the child of clear malevolence, or of negligence or strain. For example, the absence of adequate food or clothing will typically reflect contextual resource limitations rather than parental intent, and understandings of neglect can vary across cultural and social settings (Norman et al., 2012). The ostensible experience of neglect can occur in an environment otherwise marked by love, warmth, care and support, hence not creating theoretically-recognised pathways to IPV victimisation by undermining self-worth, affecting attachment or creating normative expectations of violence as a means of conflict resolution. While neglect is not consistently or strongly associated with IPV across studies or in all ours analyses, its role should not be dismissed outright but interpreted cautiously within a broader social and developmental context.
Gender and Age Affect the CM-IPV Relationship, but Socio-economic Status Does Not
This study also found that gender and age significantly shape the relationship between CM and IPV, but SES in adulthood and financial hardship in childhood had minimal influence. This is consistent with prior reviews which have found SES is not directly associated with either IPV perpetration or victimisation (Curtis et al., 2023). However, gender differences are evident, with young women aged 16 to 24 who experienced all three direct forms of CM (CSA, CEA, CPA) having a 38% likelihood of facing all three forms of IPV in adulthood, compared to 17.6% of young men. In Australia, multi-type CM is more prevalent among gender-diverse participants (66.1%) and women (43.2%) than men (34.9%; Higgins et al., 2023), significantly heightening their risk of multi-type IPV. These gender differences are supported by research showing that childhood trauma is more strongly linked to physical and sexual IPV victimisation in women, while it is more associated with IPV perpetration in men (Fulu et al., 2017; Wadji et al., 2024). Young adults are particularly vulnerable as the association between CM and IPV is particularly prominent in dating relationships in young adulthood (Li et al., 2019). This emphasises the need for early detection and trauma-informed responses (Mathews, Thomas & Scott, 2023), with pre-service training and education aimed at identifying CM and intervening during critical developmental stages (Walsh et al., 2022).
Strengths and Limitations
Insights from this study illuminate the complex associations between five forms of CM and three forms of IPV, drawing from a nationally representative survey of 8,503 participants in Australia. This study is the first of its kind to use a randomly selected, nationally representative population-wide sample to investigate the full spectrum of five CM types – CSA, CEA, CPA, EDV, and neglect – and their combined effects on IPV in romantic relationships at the national level. With a large sample size, and comprehensive measurement of each type of CM and IPV with validated measures congruent with robust concepts of these diverse forms of violence, the study provides reliable, weighted estimates of national IPV prevalence and associations with different types of CM. Our analytical approach adjusted for a range of confounders, including socio-economic status in childhood and adulthood, and the experience of multiple types of child maltreatment, enabling a more accurate understanding of the contribution of specific types of CM to any IPV, distinct types of IPV, and the experience of all three forms of IPV.
Practically, these findings inform targeted prevention and intervention strategies by identifying which maltreatment types most strongly predict specific forms of IPV, highlighting the importance of addressing multi-type maltreatment in clinical and policy frameworks. For future research, the study underscores the need to explore underlying mechanisms, such as dissociation and experiential avoidance, and to examine culturally sensitive approaches to maltreatment and IPV measurement across diverse populations. Overall, this work significantly advances knowledge by integrating comprehensive CM typologies with nuanced IPV outcomes within a robust epidemiological framework, offering critical evidence to guide evidence-based practice and policy to reduce cycles of violence (Li et al., 2019).
Despite its strengths, several limitations should be noted. First, the cross-sectional design limits the ability to establish causality, which also affects the study’s external validity. Second, retrospective self-reporting may lead to underestimation due to recall inaccuracy, particularly for early childhood events or for older participants (aged 65+). Third, the study cannot fully capture developmental or intergenerational pathways from CM to IPV, Other factors, such as exposure to peer bullying in childhood, may also influence the relationship between CM and IPV, which were not fully explored in this study. Future research could consider the impact of poly-victimisation, namely the experience of both CM and other types of violence such as peer bullying, witnessing community violence, and property crime (Finkelhor et al., 2009), on various forms of IPV. Fourth, a degree of overlap between CSA and sexual IPV may have occurred among those aged 16 to 17 years, although this was likely small given that among the 378 participants aged 16 to 17 years, 111 (29.4%) reported ever being in an adult intimate relationship, and of these, 20 (18%) had experienced CSA perpetrated exclusively by romantically known adolescents. Fifth, this study focused on the associations between CM and IPV victimisation, and equally important questions concern the nature and extent of associations between CM and IPV perpetration (Fulu et al., 2017). Sixth, we did not consider the influence of contextual characteristics of CM experiences, such as the age of onset, and chronicity. Future research could explore such developmental trajectories, and dose-response relationships to extend understanding of pathways between specific contextual circumstances of CM and IPV victimisation. Similarly, we did not capture information on frequency of IPV, or perpetrators, and further research into these characteristics would further illuminate the impact of CM on IPV experiences. Findings related to individuals with diverse genders should be interpreted with caution due to small cell sizes. Further, a limitation of combining child abuse and emotional neglect is that it may obscure the distinct effects of each form of maltreatment. While this approach provides a broader view, it reduces specificity and may influence the interpretation of results by conflating the unique contributions of abuse and neglect to later outcomes like IPV. Future research could examine these factors separately to better understand their individual impacts. Finally, the study was conducted in Australia, which is a high-income country with its own social, cultural, and geographic attributes; accordingly, cultural and contextual factors may further limit the generalizability of these findings to other cultural settings.
Conclusions
This study highlights the influence of experiencing CM on subsequent IPV victimisation and identifies the complex variation in the differential impact of specific types of CM on sexual, physical, and psychological IPV victimisation in adulthood. Experiencing any form of CM significantly increases the risk of IPV. However, CSA and CEA are consistently more strongly associated, followed by CPA, whereas EDV and neglect are not strongly associated. In addition, the experience of multi-type CM, particularly when involving the three direct forms of CM, strongly influence the likelihood of experiencing all three co-occurring IPV types. These findings confirm an understanding of the “chain of violence,” where the experience of CM heightens the risk of experiencing further violence in adult intimate relationships (Fulu et al., 2017; Shields et al., 2020). However, they advance existing knowledge by indicating distinct pathways linking some but not all types of childhood trauma to adult victimisation, and are particularly salient for women, who experience both more CM, and more IPV. The elevated risk for IPV associated with CM, especially among young women and people with diverse gender identities, underscores the urgent need for tailored early interventions that prevent and respond to childhood trauma, and which provide ongoing support for survivors throughout their lives. A deeper understanding of these complexities is crucial for designing effective prevention and intervention programmes capable of breaking the cycle of violence.
Supplemental Material
sj-pdf-1-jiv-10.1177_08862605251398466 – Supplemental material for Association Between Childhood Maltreatment and Adult Intimate Partner Violence Victimisation: Findings From a National Survey in Australia
Supplemental material, sj-pdf-1-jiv-10.1177_08862605251398466 for Association Between Childhood Maltreatment and Adult Intimate Partner Violence Victimisation: Findings From a National Survey in Australia by Ben Mathews, Huyen P. Do, David M. Lawrence, Monica Madzoska, Daryl J. Higgins, James G. Scott, Timothy I. C. Cubitt and Sarah Napier in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We extend deep gratitude to all ACMS survey participants. We also thank the Social Research Centre’s interviewers and managerial staff, particularly Nikki Honey and Diana Nguyen, for their invaluable contributions.
Ethical Considerations
The study protocol was approved by the Queensland University of Technology Human Research Ethics Committee (Approval #1900000477) for the period from August 16, 2019, to August 16, 2025.
Consent to Participate
Informed consent was obtained from all participants. Participants provided informed consent verbally after being read details about the nature of the study by the interviewer. All participants were able to give informed consent, including those aged 16 to 17, who were able to provide their own consent as endorsed by the institutional ethics approval.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by the Australian Child Maltreatment Study (ACMS), funded by a National Health and Medical Research Council Project Grant (APP1158750) from 2019 to 2023, and with further funding from the Australian Department of the Prime Minister and Cabinet, and the Department of Social Services. The Australian Institute of Criminology provided additional funding to support the inclusion of survey items on IPV.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
Data cannot be shared publicly because the data that has been used is currently embargoed under a Data Management Plan but will be made publicly available in January 2026, on a publicly accessible data archive. Supplemental Materials related to additional analysis will be shared online.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.