
Abstract
Psychological and physical intimate partner violence (IPV) in young adult couples is a major public health concern with devastating consequences. IPV shatters fundamental assumptions of safety and trust and exerts profound consequences for emotional and relational well-being. Understanding the factors associated with IPV in young adults is therefore essential. One factor may be an attachment injury, a potentially serious stressful relational event that occurs when one partner feels betrayed or abandoned by the other during a critical moment of need, damaging trust and emotional security. An attachment injury can trigger or intensify couple distress, which may increase the risk for IPV. This study examined associations between variables related to a specific attachment injury (i.e., severity, onset, stress-related symptoms, and frequency of other such injuries in the current relationship) occurring at least 3 months prior to participation, and the perpetration and victimization of physical and psychological IPV within the past 3 months. In total, 347 young adults who identified as the injured partner completed questionnaires online. Controlling for IPV that did not occur in the past 3 months but did happen before in the relationship, greater attachment injury-related stress symptoms, and greater severity of the attachment injury were linked to increased perpetration of physical IPV. In addition, greater attachment injury-related stress symptoms were associated with increased victimization of physical IPV. These findings suggest that a more severely experienced attachment injury may contribute to situational physical IPV in young adults. Efforts to promote relational well-being in this population should prioritize enhancing attachment security by addressing unresolved attachment injuries, as this may help reduce vulnerability to situational IPV.
Introduction
The victimization and perpetration of psychological and physical intimate partner violence (IPV) represent major public health concerns affecting millions of people worldwide (e.g., Smith et al., 2017), and are especially prevalent among young adults (e.g., Cénat et al., 2022; Cotter, 2021; Emond et al., 2023; Lafontaine et al., 2021). Psychological IPV involves emotional harm expressed through verbal and nonverbal acts such as yelling, isolating, insulting, ignoring, belittling, controlling, and humiliating (Center for Disease Control and Prevention [CDC], 2015). Physical IPV is characterized by an intention to cause physical harm or pain, whether lethal or not, to one's partner through actions such as grabbing, hitting, biting, choking, shoving, slapping, or burning (CDC, 2015). Psychological and physical IPV have serious and far-reaching consequences for emotional functioning and couple well-being (Shorey et al., 2012). Accordingly, a comprehensive understanding of the factors that may contribute to psychological and physical IPV remains critically important. One such unexplored aspect may be the experience of an attachment injury.
An attachment injury involves a critical breach in romantic support during a moment of emotional vulnerability, resulting in profound feelings of betrayal or abandonment in the injured partner (Johnson et al., 2001). Rooted in attachment theory as a theory of trauma, an attachment injury constitutes a significant stressful relational event that can trigger stress-related symptoms (e.g., intrusions and preoccupations, avoidance, and increased vigilance) in the injured partner and undermine the couple’s overall well-being (Johnson et al., 2001; Lafontaine et al., 2023). An attachment injury shatters basic assumptions of safety and trust in the relationship and the injuring partner, (re)defining the bond as insecure and the partner as untrustworthy (Johnson et al., 2001). This erosion of trust and security can negatively impact the couple’s interaction patterns and increase couple distress and conflict (Johnson et al., 2001), which in turn has been associated with increased risk for psychological and physical IPV (Heyman et al., 2023). Given that the foundations and expectations of romantic partnerships are established during young adulthood (Fincham & Cui, 2010), investigating the associations between variables related to an attachment injury (i.e., its perceived severity and onset, associated stress symptoms, and frequency of other attachment injuries) and psychological and physical IPV is essential for advancing our understanding of relationship well-being in this population. To date, however, such a conceptual model has not been examined.
Attachment Injury and IPV in Young Adults
Young adulthood represents a critical period of identity development and the establishment of relational patterns, including expectations within romantic relationships (Arnett, 2014; Fincham & Cui, 2010). Most young adults also experience major life transitions, such as choosing a career, moving out of their parents’ home, or relocating for post-secondary education. These developmental transitions can foster situations in which young adults feel vulnerable and in need of support and care from their loved ones, including their romantic partner. An attachment injury can occur when the expected support and care from the romantic partner is nonoptimally provided or entirely absent, leaving the injured partner feeling hurt, betrayed, abandoned, or rejected during moments of emotional vulnerability. Various experiences have the potential to create an attachment injury and disrupt the security of the romantic bond, such as feeling abandoned or betrayed when experiencing a profound loss or hardship (e.g., miscarriage and death of a family member) or a significant life transition (e.g., going to university and moving out of the parent’s home), or, in many cases, infidelity. Following an attachment injury, the injured partner may develop negative views of their partner as untrustworthy and their relationship as unsafe, while also internalizing negative self-views, including doubts about their judgment and feelings of unworthiness (Johnson et al., 2001). This may be particularly relevant for young adults, many of whom are often in their first serious relationships and may lack a comparative framework, making them more likely to normalize harmful dynamics and internalize blame (Couture et al., 2023).
Although IPV is a complex phenomenon that can be understood via various theoretical frameworks (Burelomova et al., 2018), attachment theory offers particularly compelling lens by highlighting how breaches in the support that is expected from a romantic partner (i.e., an attachment injury) can give rise to both the perpetration of IPV by the injured partner and their experience of IPV victimization (i.e., IPV perpetration by the injuring partner). An attachment injury has been conceptualized as a form of interpersonal trauma (Johnson et al., 2001), defined as a significant stressful relational event that involves betrayal, harm, or neglect by someone on whom an individual depends for safety and care, particularly in times of vulnerability (Charuvastra & Cloitre, 2008). Interpersonal traumas are known to have a particularly strong potential to lead to enduring trauma-related distress, in that they disrupt attachment-related security and often contribute to the reliance on maladaptive emotion regulation strategies to manage distress (Charuvastra & Cloitre, 2008; Hannan & Orcutt, 2020). These strategies can manifest as hyperactivated (e.g., a protest response to unmet attachment needs, intense efforts to re-establish proximity) or hypoactivated (e.g., emotional withdrawal, avoidance of vulnerability in the face of perceived rejection). From an attachment perspective, these nonoptimal emotion regulation strategies contribute to negative interaction patterns (i.e., attack/pursue and withdraw/defend) that perpetuate couple distress and conflict (Mikulincer et al., 2003), which can sometimes escalate to both the victimization and perpetration of IPV (Spencer et al., 2021; Velotti et al., 2022), including in young adults (Neilson et al., 2023).
Attachment Injury-Related Variables and IPV
Beyond the mere presence of an attachment injury, certain variables related to the attachment injury experience (i.e., its perceived severity and onset, associated stress-related symptoms, and frequency of other attachment injuries in the relationship) may provide valuable insights into the circumstances under which IPV may occur in a young adult relationship. From both a theoretical and empirical standpoint, an attachment injury that is experienced as more severe (i.e., characterized by the disruption of the injured partner’s sense of safety and trust, greater stress-related symptoms, a more recent onset, and compounded injuries) may contribute to the use of more maladaptive strategies to regulate emotional and relational distress, which can escalate to the perpetration of IPV by the injured partner, as well as their own IPV victimization (i.e., IPV perpetration by the injuring partner; Slootmaeckers & Migerode, 2020).
The occurrence of an attachment injury, in theory, is believed to be less influenced by its objective content and more by the emotional significance it holds for the injured partner (Johnson et al., 2001). As a result, the severity of an attachment injury, conceptualized as the degree to which the attachment injury is perceived to have disrupted the injured partner’s sense of safety and trust within their relationship (Johnson et al., 2001; Makinen & Johnson, 2006), is highly subjective and may be linked with the extent of the distress and conflict it creates, as well as how the injured partner copes with the attachment injury (Lafontaine et al., 2023). Following an attachment injury, injured partners, including young adults (Roos et al., 2019), can experience heightened emotional reactivity manifested as stress-related symptoms, including intrusive preoccupations, thoughts, and images surrounding the attachment injury; avoidance of, or hyper-reactivity to, reminders of the attachment injury; intense fear that it will happen again; anger and irritability; and deep sadness among others (Lafontaine et al., 2023; Lonergan et al., 2022). Such a stress-related response, which can also underlie difficulties with emotion regulation (e.g., Hannan & Orcutt, 2020), has been linked with IPV perpetration and victimization in prior research (Miles-McLean et al., 2021; Stein et al., 2024), including in young adults (Marshall et al., 2011).
It is equally possible that a more recent onset of the attachment injury is linked to greater IPV perpetration and victimization, potentially through emotional overload. For instance, the acute phase following the experience of infidelity, one example of a potential attachment injury, has been described as an emotional roller coaster involving heightened reactivity in both partners (Olson et al., 2002). Moreover, some authors have noted that, like trauma exposure, experiencing multiple attachment injuries can create compound injuries that severely damage trust and intensify relationship conflict (Makinen & Johnson, 2006; Pelling & Arvay-Buchanan, 2004). Thus, the timing of a specific attachment injury, along with the presence of compounded injuries, may heighten individuals’ susceptibility to resorting to nonoptimal emotion regulation strategies when faced with perceived threats (i.e., attachment injury), thereby increasing the possibility for IPV.
Study Objectives and Hypotheses
The objective of this study was to examine the associations between attachment injury-related variables (i.e., perceived severity and onset of the attachment injury, stress symptoms related to the attachment injury, and frequency of other attachment injuries in the relationship) that occurred at least 3 months prior to study participation and psychological and physical IPV victimization and perpetration that happened in the past 3 months in young adults who experienced an attachment injury as the injured partner. After controlling for past IPV in the relationship (i.e., IPV that occurred more than 3 months ago), it was expected that greater perceived severity of the attachment injury, greater attachment injury-related stress symptoms, a shorter time since the attachment injury (i.e., onset), and a greater frequency of other attachment injuries in the relationship would be associated with greater psychological and physical IPV perpetration and victimization within the past 3 months.
Method
Participants
Eligible participants were young adults currently in a romantic relationship of at least 3 months in duration (to ensure a minimal level of relationship stability) and residing in Canada. In this study, young adult was defined as individuals between the ages of 18 and 30 years old to capture a larger span of emerging adulthood (Arnett, 2014). Moreover, only participants who experienced an attachment injury in their current romantic relationship more than 3 months prior to participation were retained, to ensure that IPV was present after the attachment injury occurred. Participants were also required to understand written English to complete the questionnaires. Participants were not eligible to participate if the attachment injury involved physical or sexual violence, in accordance with the feedback received from the University’s Research Ethics and Integrity Board. Individuals who indicated having been diagnosed with posttraumatic stress disorder by a mental health professional were also not eligible to participate, as posttraumatic symptoms stemming from exposure to other traumatic events could overlap with those relevant to an attachment injury. Ineligible participants were not directed to the informed consent form and were offered a list of psychological resources.
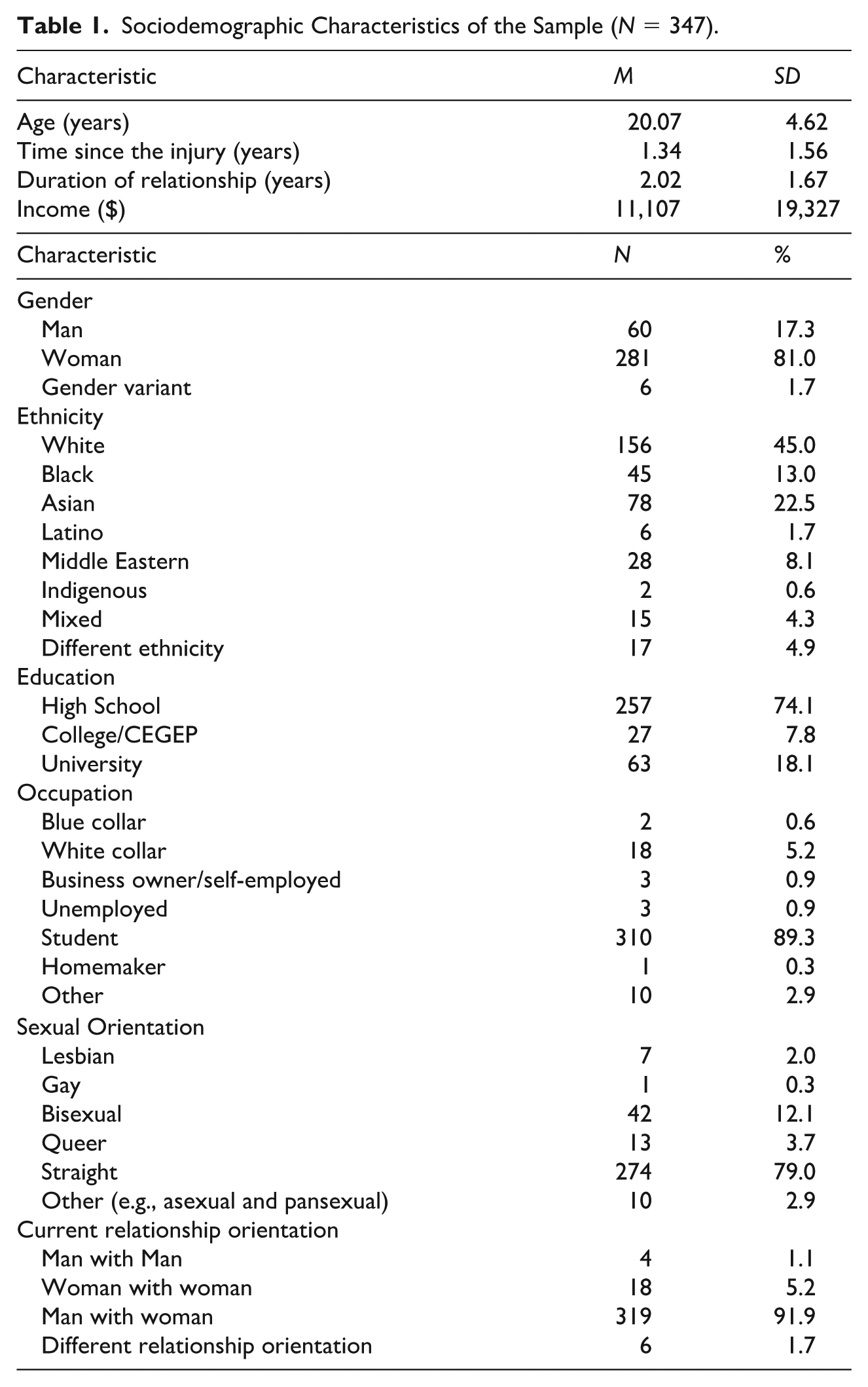
The total number of respondents was 696 individuals who identified as injured partners. Of these, two participants were in a couple relationship together, and their data were therefore excluded. Of the 694 remaining participants, 18 participants did not report their age, and 87 were older than 30 years old; these data were therefore excluded, resulting in 589 participants who were between the ages of 18 and 30 years old. Of these, 87 completed no items on the measure of the psychological and physical IPV, resulting in 502 participants. Additionally, to examine how an attachment injury experienced at least 3 months prior to study participation may be linked to more recent (i.e., previous 3 months) IPV, participants who reported that the attachment injury occurred within the previous 3 months were excluded (n = 155). Although the research design was cross-sectional and does not permit establishing causality between study variables, the 3-month time frame was chosen to account for a chronological order between the occurrence of the attachment injury and the occurrence of IPV in the relationship. Thus, the final sample consisted of 347 participants between the ages of 18 and 30 years old who identified as the injured partner, and who reported that they experienced an attachment injury 3 or more months prior to study participation (see Table 1 for sociodemographic details).
Sociodemographic Characteristics of the Sample (N = 347).
Measures
Sociodemographic and Relationship Questionnaire
A questionnaire was used to collect relevant sociodemographic information (e.g., age, educational level), relationship variables (e.g., relationship status, relationship length, cohabitation length).
Psychological and Physical IPV
The victimization and perpetration of psychological and physical IPV were assessed using the Revised Conflict Tactics Scales (CTS2; Gabbay & Lafontaine, 2020; Straus et al., 2003). Using an 8-point scale, participants reported how often each behavior had occurred during the past 3 months: This has never happened (0), Once (1), Twice (2), 3–5 times (3), 6–10 times (4), 11 to 20 times (5), 21 or more times (6), and Not in the past 3 months, but this has happened before (7). On the psychological IPV subscale, eight items measure IPV victimization (e.g., “My partner insulted or swore at me”), and eight items measure IPV perpetration (e.g., “I insulted or swore at my partner”). On the physical IPV subscale, 12 items measure IPV victimization (e.g., “My partner threw something at me that could hurt”), and 12 items measure IPV perpetration (e.g., “I threw something at my partner that could hurt”). Internal consistency for the current sample, as measured by Cronbach’s α, was .75 for psychological IPV victimization, .76 for psychological IPV perpetration, .92 for physical IPV victimization, and .91 for physical IPV perpetration.
First, for the main analyses, all items were recoded using the mid-point of each response category to estimate the frequency of IPV acts in the past 3 months: 0 = 0 times, 1 = 1 time, 2 = 2 times, 3 = 4 times, 4 = 8 times, 5 = 15 times, and 6 = 25 times (Straus et al., 2003). To isolate recent (i.e., within the past 3 months) IPV frequency from prior IPV, the response Not in the past 3 months, but it did happen before (7) was recoded as 0. Thus, scores on each of the psychological IPV subscales range from 0 to 200, and scores on each of the physical IPV subscales range from 0 to 300, with higher scores indicating a greater estimated frequency of IPV victimization or perpetration (see Table 2).
Means, Standard Deviations, and Range of Attachment Injury-Related Variables and IPV.
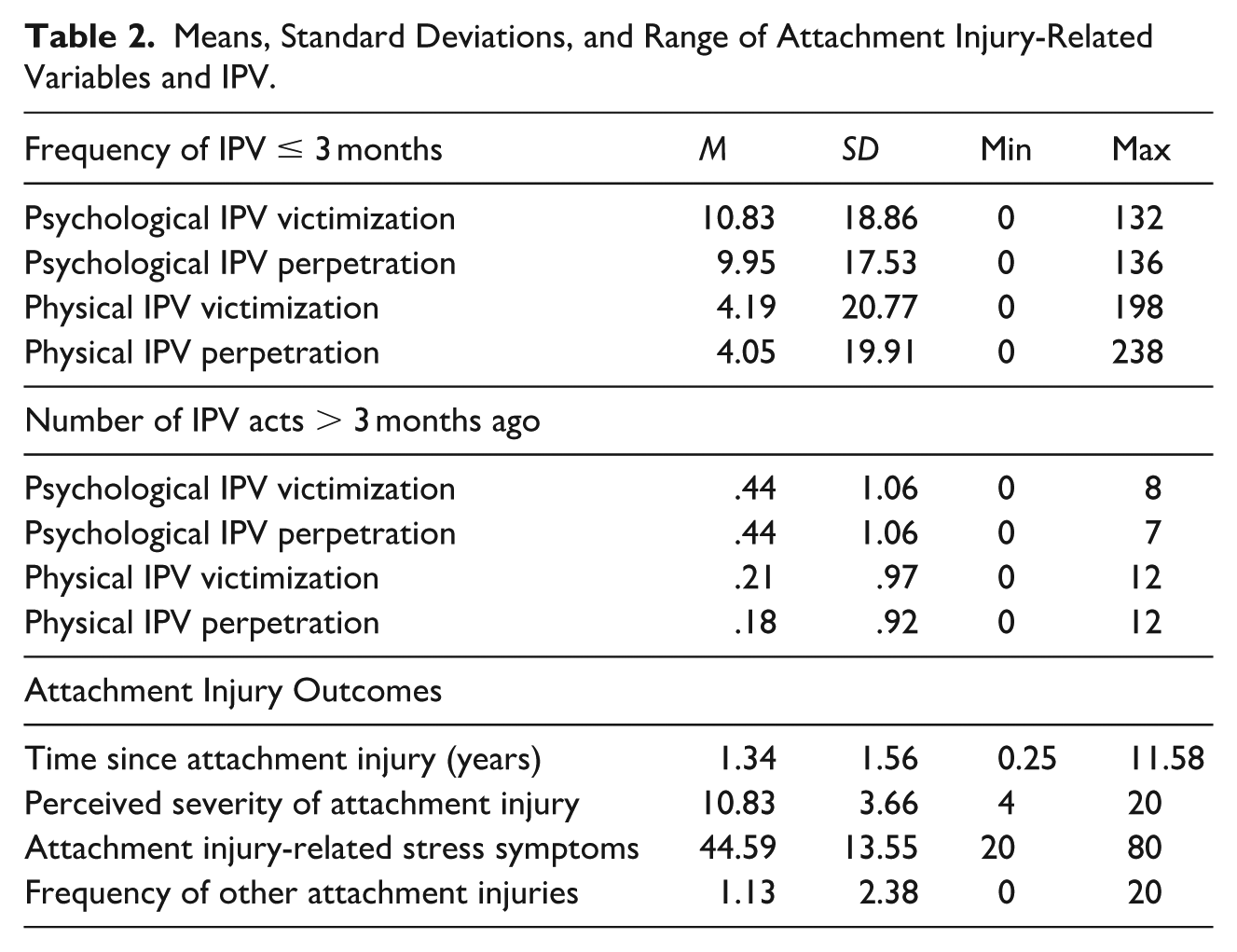
Second, to control for prior IPV in the relationship, defined as a response of Not in the past 3 months, but it did happen before, four variables were created by summing the number of endorsed items for each type of IPV (Straus et al., 2003). For example, if a participant selected this response item for three of the eight items measuring the perpetration of psychological IPV, their score for prior perpetration of psychological IPV would be 3. Thus, scores ranged from 0 to 8 for prior perpetration and victimization of psychological IPV, and scores ranged from 0 to 12 for prior perpetration and victimization of physical IPV.
Severity of the Attachment Injury
The perceived severity of the attachment injury was measured using the 4-item Attachment Injury Measure (AIM; Makinen & Johnson, 2006). The items “How do you currently rate the significance of the event that injured your relationship bond?”, “How does the attachment injury currently affect the level of trust between you and your partner?”, “How does the attachment injury interfere with your relationship now?”, “When you talk to your partner about the attachment injury, how much of a problem does it currently create?” was rated using a 5-point scale from Severe (1) to Negligible (5). The total score (sum of all items) ranges from 4 to 20, with lower scores indicating greater perceived severity of the attachment injury. Scores > 10 have been used to indicate attachment injury resolution, or in other words, that the attachment injury is not perceived to have a severe impact on the relationship (Makinen & Johnson, 2006). Internal consistency for the current sample, as measured by Cronbach’s α, was .76.
Attachment Injury-Related Stress Symptoms
Stress symptoms related to the attachment injury (i.e., intrusions/preoccupations, impairment in function, depressed mood, anxiety, and impulse disturbance) were measured with the reliable and validated 20-item Adjustment Disorder New Module (ADNM-20; Lorenz et al., 2016). On this measure, participants indicate how often they typically experience each symptom, such as “Since the attachment injury, I feel low and sad” on a 4-point Likert scale from Never (1) to Often (4). Total scores (sum of all items) on the ADNM-20 range from 20 to 80, with higher scores indicating greater symptom severity and scores > 47.5 indicating risk for an adjustment disorder (Lorenz et al., 2016). Internal consistency for the current sample, as measured by Cronbach’s α, was .94.
Onset of the Attachment Injury and Frequency of Other Attachment Injuries
Two items were used to collect information about how long it had been since the specific attachment injury occurred, and the number of other attachment injuries in the current relationship. The first item was “How long has it been since the event occurred?” and the second was “Can you identify any other incidents where you felt that your partner betrayed or abandoned you?”; if participants answered Yes to this item, they were then asked, “If so, how many times has this occurred?”. Participants who responded No to this question were coded as 0, indicating they had not experienced any other attachment injury in the current romantic relationship.
Procedure
Recruitment took place from July 2020 through December 2022. Participants were recruited through the University’s Integrated System for Participation in Research (ISPR) pool and the community via online advertisements (e.g., Facebook, Instagram, Twitter) and listservs. Participants resided in one of two Eastern Canadian provinces. All participants were presented with a study information page. After clicking on a secure Qualtrics link, participants filled out a brief screening questionnaire to confirm their eligibility.
Participants were given the following definition of an attachment injury in the study information page: “An attachment injury is defined as a hurtful event involving feelings of abandonment or betrayal during a time when you really need your partner’s caring and support.” The presence of an attachment injury was assessed by answering Yes to the screening question: “Can you recall an instance where you felt betrayed or abandoned by your current romantic partner?” and No to the screening question: “Does the betrayal or abandonment event that occurred in your current romantic relationship involve physical or sexual abuse in that relationship?”. Eligible participants then provided informed consent and completed the sociodemographic questionnaire as well as the self-report questionnaires. All participants received a randomized identification code to preserve anonymity. Participants recruited from the ISPR pool received one course credit, and the participants recruited from the community received a chance to win CAN$50 for their participation. The University’s Office of Research Ethics and Integrity approved all procedures.
Statistical Analyses
As missing values on the questionnaires were minimal (< 1% of all values), scores were calculated for participants who completed at least 80% of the items on each questionnaire. Accordingly, the physical IPV victimization score was not computed for one participant, and the perceived severity of the attachment injury score was not computed for another; these were treated as missing. In addition, 10 participants did not report the frequency of other attachment injuries in the relationship and were also treated as missing. Descriptive statistics (means, standard deviations, frequencies, and percentages) were calculated for all sociodemographic, relationship, attachment injury-related, and IPV variables. Bivariate correlations were examined among independent, dependent, and control variables.
To test the main hypotheses, a path analysis was conducted. The analysis included four attachment injury-related variables (perceived severity and onset, stress-related symptoms, and frequency of other attachment injuries) as the independent variables, and four IPV outcomes (psychological and physical IPV perpetration and victimization within the past 3 months). In addition, past IPV (psychological and physical IPV perpetration and victimization occurring more than 3 months ago) was included as a control variable. Model fit was assessed using the standardized root mean square residual (SRMR; < .08), the comparative fit index (CFI; > .90), and the root mean square error of approximation (RMSEA; < .08), along with its 90% confidence interval (Hu & Bentler, 1999). All analyses were conducted using R software (version 4.4.3; R Core Team, 2024) with the lavaan package (Rosseel, 2012).
Results
Descriptive Analyses
Means, standard deviations, and range for all study variables can be found in Table 2, and correlations between study variables are reported in Table 3. Half (50%) of the participants obtained scores on the measure of the perceived severity of the attachment injury above 10, which has been previously used as an indicator that the attachment injury does not have a severe impact on the relationship (Makinen & Johnson, 2006). On average, participants’ levels of attachment injury-related stress symptoms were moderate in severity, and 40.1% of participants fell above the cut-off score for a possible adjustment disorder. Of the sample, 73.8% reported at least one occurrence of psychological IPV victimization, 73.4% reported psychological IPV perpetration, 20.4% reported physical IPV victimization, and 23.5% reported physical IPV perpetration in the previous 3 months. In addition, 69.7% of participants reported bidirectional (victimization and perpetration) psychological IPV in the last 3 months, whereas 15.7% of participants indicated bidirectional physical IPV in the same period.
Correlations Between Attachment Injury-Related Variables and IPV.
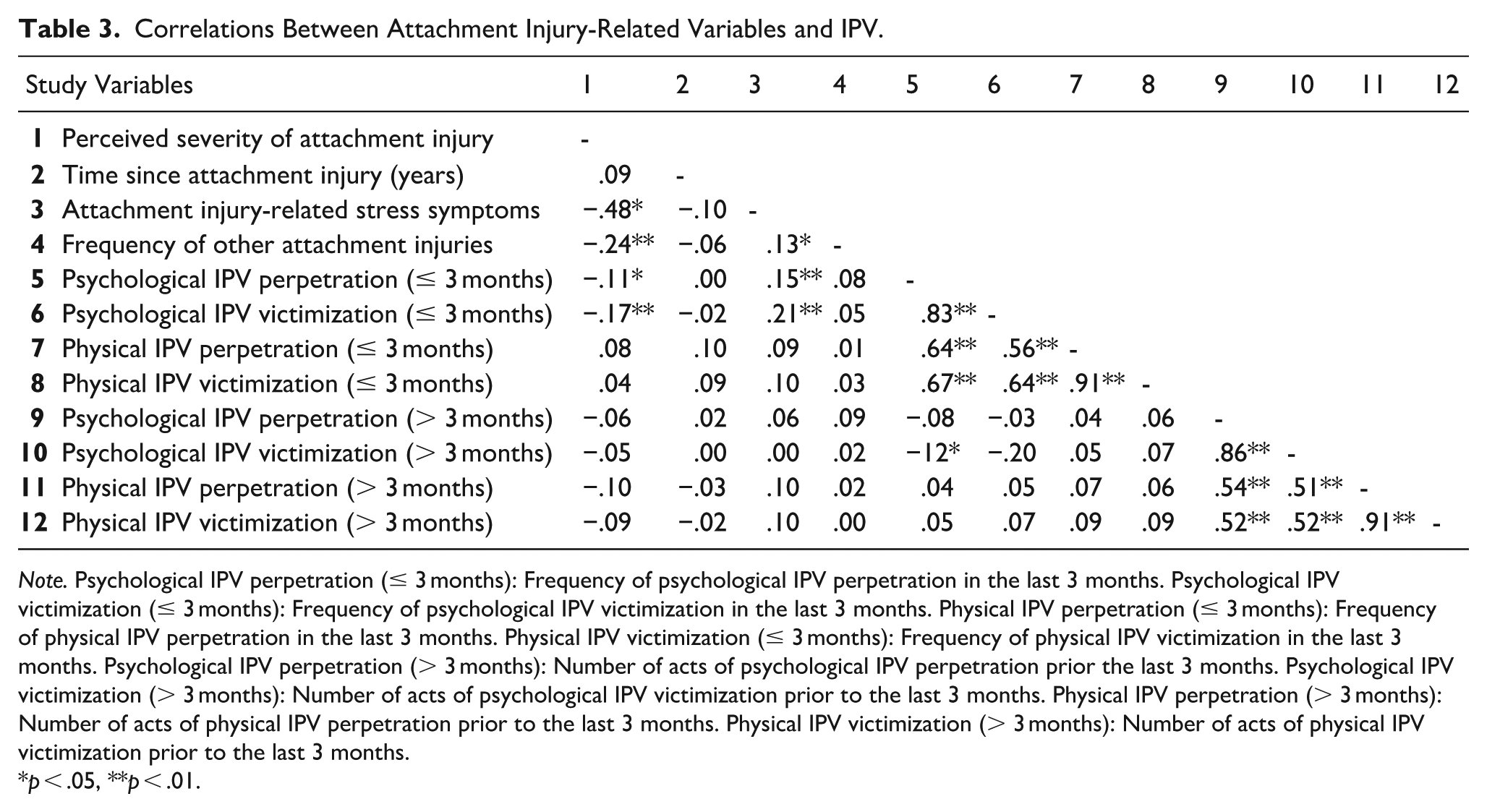
Note. Psychological IPV perpetration (≤ 3 months): Frequency of psychological IPV perpetration in the last 3 months. Psychological IPV victimization (≤ 3 months): Frequency of psychological IPV victimization in the last 3 months. Physical IPV perpetration (≤ 3 months): Frequency of physical IPV perpetration in the last 3 months. Physical IPV victimization (≤ 3 months): Frequency of physical IPV victimization in the last 3 months. Psychological IPV perpetration (> 3 months): Number of acts of psychological IPV perpetration prior the last 3 months. Psychological IPV victimization (> 3 months): Number of acts of psychological IPV victimization prior to the last 3 months. Physical IPV perpetration (> 3 months): Number of acts of physical IPV perpetration prior to the last 3 months. Physical IPV victimization (> 3 months): Number of acts of physical IPV victimization prior to the last 3 months.
p < .05, **p < .01.
Association Between the Attachment Injury-Related Variables and Different Types of IPV
Before conducting the path analysis, the underlying assumptions were tested. Due to the presence of outliers and non-normality of the data, bootstrapping with 5000 samples was employed to provide robust estimates (Awang et al., 2015). Figure 1 and Table 4 present the model results. Controlling for past IPV (i.e., not in the past 3 months), greater attachment injury-related stress symptoms were significantly associated with increased perpetration and victimization of physical IPV. Additionally, greater perceived severity of the attachment injury was significantly associated with increased perpetration of physical IPV. No other significant associations were found. The model demonstrated good fit to the data: χ2(1) = 1.29, p = .256, SRMR = 0.01, CFI = 1.00, RMSEA = 0.03, 90% CI [0.00, 0.15].
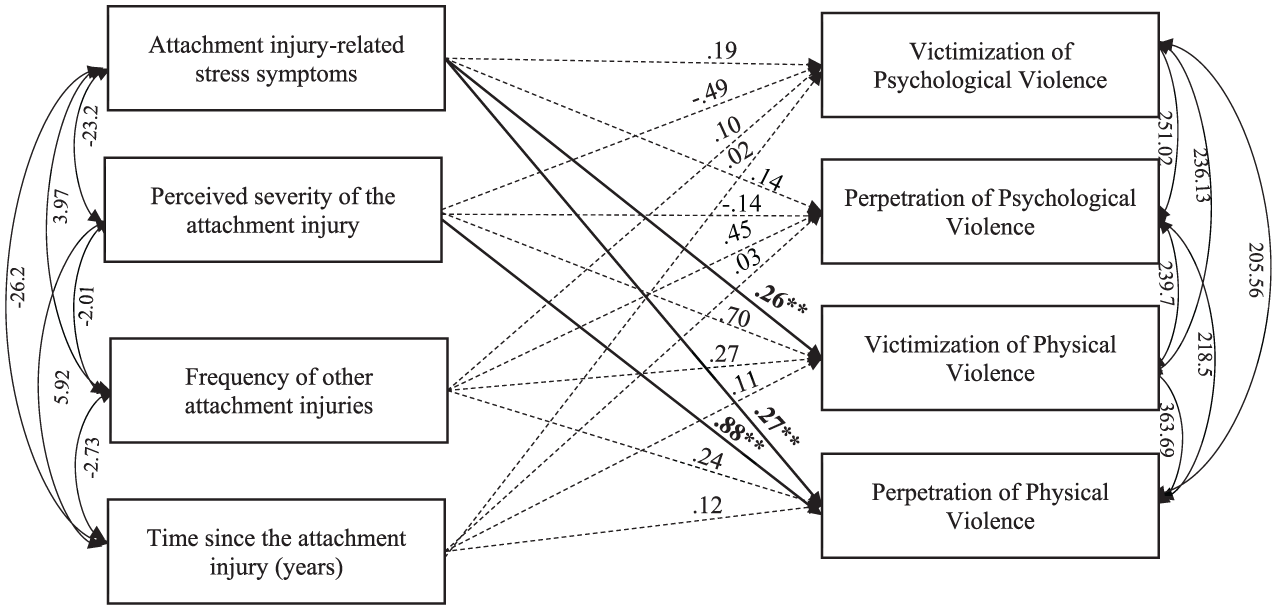
Attachment injury-related variables associated with perpetration and victimization of psychological and physical IPV.
Unstandardized Estimates and Standard Errors with Bootstrapped Bias-Corrected 95% Confidence Intervals and p-values for the Associations Between Attachment Injury-Related Variables and IPV.
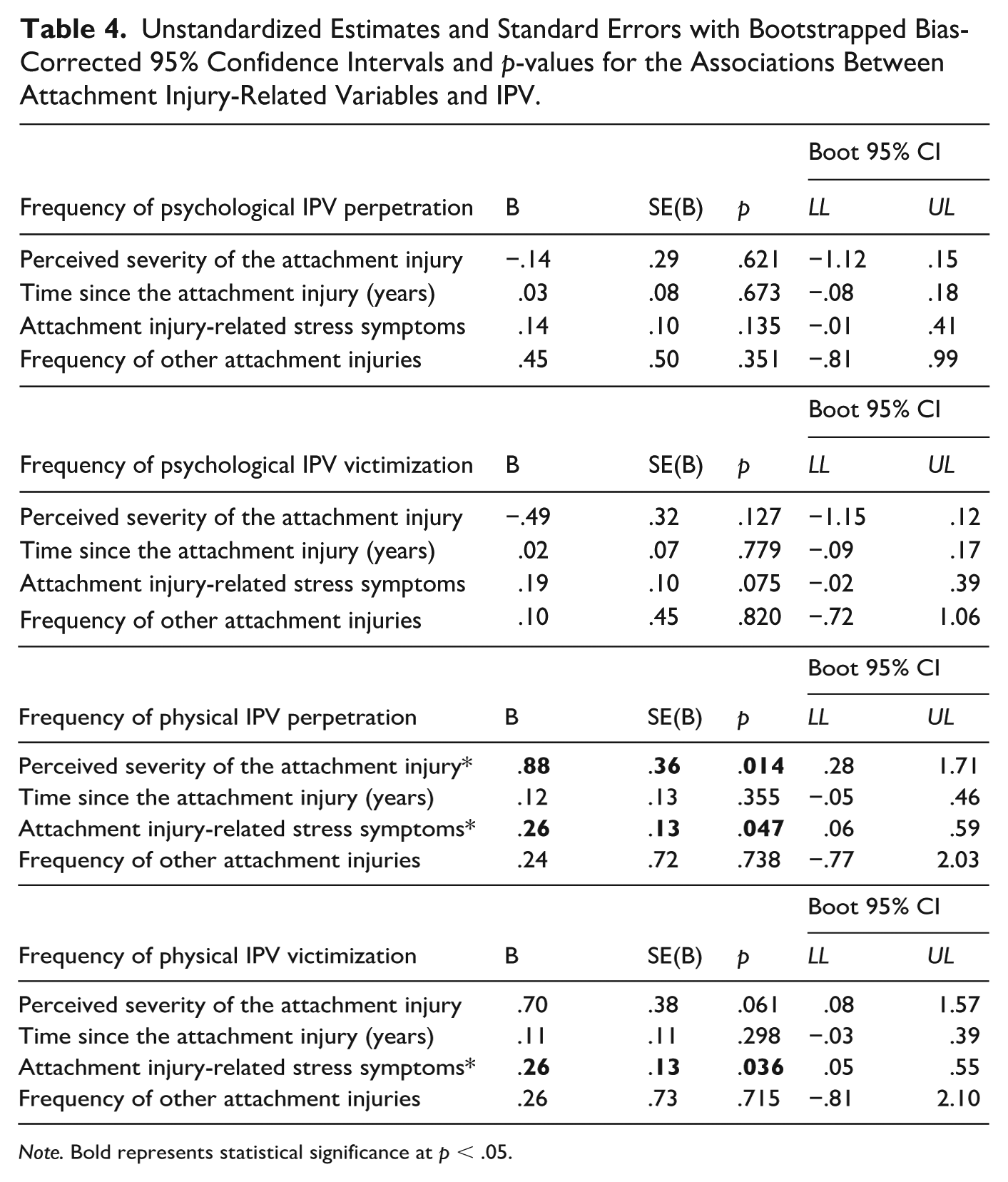
Note. Bold represents statistical significance at p < .05.
Discussion
In this study, the associations between attachment injury-related variables (i.e., attachment injury severity and onset, attachment injury-related stress symptoms, and the frequency of other attachment injuries in the current relationship) and recent experiences of psychological and physical IPV perpetration and victimization among injured young adults were examined. To put the results in context, approximately three-quarters of participants reported both psychological IPV victimization and psychological IPV perpetration, with an average frequency of approximately 10 acts over the previous 3 months. Moreover, between 20% and 24% of participants reported physical IPV victimization and perpetration, with an average frequency of approximately four acts over the previous 3 months. Bidirectional psychological and physical IPV was present in many participants’ relationships. It is possible that the present study’s community sample consisted of individuals who may have been experiencing situational couple violence, which, according to Johnson’s (2008) typology of IPV, involves anger and frustration stemming from unresolved conflict (see also Gulliver & Fanslow, 2015), such as that created by an attachment injury.
The Role of an Attachment Injury in IPV
The notion that participants in this sample may have been experiencing situational couple violence is further supported by the study’s main findings, which highlight how specific dimensions of an attachment injury experienced more than 3 months ago may be linked to recent physical IPV in young adults. As expected, when accounting for IPV that occurred more than 3 months prior to study participation, young adults who reported greater attachment injury-related stress symptoms and felt that the attachment injury more severely damaged their sense of trust and emotional security with their partner reported greater physical IPV perpetration in the past 3 months. Moreover, more severe attachment injury-related stress symptoms among injured young adults were associated with higher levels of physical IPV victimization, that is, instances of physical IPV perpetrated by the injuring partner.
Overall, these results align with the conceptualization of attachment theory as a theory of trauma (Atkinson, 1997). Findings suggest that certain trauma-related dimensions of the attachment injury experience, including heightened attachment injury-related stress symptoms and diminished sense of safety and trust, may be particularly relevant for understanding the perpetration and victimization of physical IPV in young adult injured partners. In this context, physical IPV perpetration by both partners may reflect an unsuccessful strategy for navigating the intense relational distress and conflict (Bartholomew & Allison, 2006; Lafontaine et al., 2018) that is triggered or intensified by an attachment injury. The young adults in this sample may have been more likely to resort to physical rather than psychological IPV to cope with overwhelming feelings of fear, anger, or emotional pain related to the attachment injury. Indeed, greater perceived severity of the attachment injury and elevated attachment injury-related stress symptoms might underlie more impulsive emotional responses, consistent with Johnson’s (2008) typology of situational couple violence characterized by reactive, conflict-driven physical acts (e.g., hitting, slapping).
Interestingly, however, and contrary to expectations, no associations were found between the attachment injury-related variables under study and psychological IPV perpetration or victimization. As in other areas of romantic life (e.g., O’Leary et al., 2018), it is possible that the attachment injury experience is differentially associated with psychological and physical IPV. For instance, psychological IPV tends to be a more socially accepted, yet still problematic, way for partners to interact, particularly during conflict (Doherty & Berglund, 2008). Indeed, psychological IPV was highly prevalent in this sample, leaving little variance to be explained by the experience of the attachment injury. Conversely, physical IPV may represent a more severe escalation of conflict that may be more likely to occur in the context of an attachment injury that is experienced as more severe. Thus, while psychological IPV may consist of a more normative aspect of relational distress and conflict in couples who have experienced an attachment injury, physical IPV may be indicative of a threshold being crossed because of the intense emotional and relational distress created by the attachment injury. Further research is therefore needed to clarify the role of the key variables related to a specific attachment injury in different forms of IPV and the mechanisms involved in these associations.
Limitations and Future Directions
Despite its strengths and novelty, several limitations of this study and directions for future research should be noted. While the sample evidenced some diversity in terms of ethnicity and sexual/gender identity, increasing the diversity of future samples would permit a deeper investigation of how the attachment injury experience and its association with IPV may vary across different cultural backgrounds, gender identities, and relationship contexts. Moreover, this study focused specifically on young adults, a population at a critical developmental stage during which identity and relationships are being explored. Future research could examine whether the proposed conceptual model applies to other age groups, such as adults who may be in more long-term relationships. In addition, because the study was conducted in a highly selected sample, caution is warranted when extrapolating the observed associations between attachment injury-related variables and IPV to individuals not meeting the same eligibility criteria.
Another important consideration relates to the conceptual model, which aimed to put forth a chronological sequence between the attachment injury experience and IPV. However, the correlational nature of the study precludes drawing any causal conclusions between the study variables. Future research employing a longitudinal design is needed to clarify the associations between an attachment injury assessed at an initial time point and subsequent IPV. Additionally, the onset of concomitant attachment injuries was not assessed in this study. For some participants, it is possible that an attachment injury beyond the one of focus occurred within the past 3 months. Future research could account for the timing of concomitant attachment injuries to better understand their cumulative effects on psychological and physical IPV. In the current study, only psychological and physical IPV data were collected. Given that it is well-established that various forms of IPV often co-occur, it would be pertinent to integrate sexual IPV into future research. Moreover, the focus of this novel study was on examining the direct associations between certain attachment injury-related variables and psychological and physical IVP. To further expand knowledge in this field, future studies could also examine the mechanisms through which these associations occur and the conditions under which they hold, considering variables such as personality traits or attachment orientations. Finally, considering that an attachment injury, as well as IPV, are dyadic phenomena (Johnson et al., 2001; Lafontaine et al., 2018), future research could incorporate both partners to further investigate the dyadic associations between an attachment injury and IPV.
Implications and Conclusion
Findings from this study suggest that certain dimensions related to an attachment injury may be meaningfully associated with situational couple IPV among some young adults. An attachment injury—defined as a significant relational betrayal that undermines a fundamental sense of safety and trust—can have profound implications for both partners and the couple. If experienced as severe and unresolved, such injuries may disrupt emotional regulation, contribute to maladaptive interaction cycles, and intensify relational conflict, which may escalate to physical IPV. Given that young adults are in a formative stage of identity exploration and romantic development, experiencing an attachment injury during this period may negatively shape how they perceive themselves as romantic partners and how safe or reliable they believe others to be. Thus, it is important to raise awareness, through conferences and trainings tailored to young adults, about how a major rupture in romantic support can negatively impact a young person’s emotional and relationship well-being.
As an attachment injury may even constitute a potential risk factor for situational IPV, it is important for service providers in clinical, educational, or social settings to discuss the circumstances surrounding an attachment injury, particularly its perceived severity and associated stress symptoms, when working with individuals or couples who have experienced such a stressful relational event. One promising intervention in this area is the Attachment Injury Resolution Model developed by Johnson et al. (2001), which offers a structured framework for addressing unresolved attachment injuries within the emotionally focused therapeutic approach in the absence of high-risk IPV that threatens physical and mental health safety (Johnson, 2019). Moreover, Slootmaeckers and Migerode (2018, 2020) endorse this attachment-based approach, particularly for addressing situational IPV, which they conceptualize as emerging from insecure relational dynamics and unmet emotional needs rooted in unresolved conflict. With respect to the Attachment Injury Resolution Model, the attachment bond is repaired through a structured process in which the injured partner expresses their pain, the injuring partner responds with empathetic acknowledgment, and both partners work toward forgiveness and reconciliation to rebuild trust and emotional safety (Johnson et al., 2001; Zuccarini et al., 2013). In doing so, the painful emotions tied to the attachment injury are processed within a secure context, which fosters healthier emotional regulation and reduces the likelihood of reactive or destructive behaviors, such as those associated with situational IPV. One resource consistent with this model and accessible to young adults is the Hold Me Tight program (Johnson, 2019), which includes a section on the resolution of an attachment injury and is available in multiple languages and formats, including books, workshops, online courses, and videos.
In summary, findings of this study emphasize the importance of helping individuals and couples break the cycle of situational IPV, while promoting attachment security through the resolution of an attachment injury. By placing equal emphasis on emotional healing and physical safety, service providers and young adults themselves are better equipped to foster the development of secure, supportive, and violence-free relationships among young adults.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by an Insight Grant from the Social Sciences and Humanities Research Council of Canada (155220). The second author, M.L., held a postdoctoral fellowship from the Social Sciences and Humanities Research Council of Canada while working on this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.