
Abstract
Women and gender-diverse people with disabilities are at an elevated risk of gender-based violence (GBV). This study examines how women and gender-diverse people with disabilities experience GBV and how such experiences impact their sexual and reproductive health (SRH) across the life course. We conducted a community-engaged qualitative study from 2022 to 2023 with women and gender-diverse people with disabilities aged 18 years and older living in Canada. Using an inductive thematic approach, we analyzed 26 semi-structured interviews about experiences of GBV and SRH across the life course, including childhood, the reproductive years, and older adulthood. Disability and GBV intersected over time: GBV experienced earlier in life caused mental health disabilities that impacted subsequent life course stages. Ableism meant participants were targets of violence and made disclosure more difficult. GBV experiences impacted SRH by (a) causing new SRH concerns (e.g., unintended pregnancies and forced abortions); (b) amplifying existing SRH concerns (e.g., endometriosis); (c) influencing reproductive decision-making (e.g., contraception and sterilization); (d) shaping sexual practices and relationships (e.g., engagement in high-risk sexual behaviors and intimacy); and (e) changing interactions with SRH services (e.g., painful pelvic exams). Characteristics of services (e.g., availability of disability-related accommodations) also affected disclosure and trust. These findings highlight the long-lasting impacts of GBV on SRH among women and gender-diverse people with disabilities. There is a need for provider education on disability and GBV, and trauma-informed and disability-affirming SRH services developed and implemented in collaboration with people with lived experiences of disability and GBV.
Introduction
Gender-based violence (GBV) is a sexual and reproductive health (SRH), human rights, and gender equity issue. GBV includes physical, sexual, psychological, or economic violence directed at a person because of their gender, and/or violence that disproportionately impacts persons of a particular gender, such as violence against women and gender-diverse people (European Commission, n.d.; World Health Organization [WHO], 2020a). While GBV affects people of all identities, its distribution is shaped by intersecting structural inequalities, including cis/sexism and ableism.
People with disabilities experience all types of violence at higher rates than people without disabilities (Badakhshiyan et al., 2024; Fang et al., 2022; K. Hughes et al., 2012), and women and gender-diverse people with disabilities are at amplified risk of GBV (Amborski et al., 2022; Bowen & Swift, 2019; Domínguez-Martínez et al., 2023; García-Cuéllar et al., 2023). As per queer feminist disability theory, we understand this disproportionate risk of GBV not as a consequence of having a disability but as a structural vulnerability rooted in ableism—the systemic devaluation and exercising of power over disabled people—and intersecting social positions that amplify disabled people’s exposure to harm, such as cis/sexism, racism, economic exclusion, institutionalization, power imbalances with caregivers, and care inaccessibility (Chin, 2021; Kafer, 2013; Mingus, 2017; Schalk, 2022; Sins Invalid, 2019).
GBV can be experienced by disabled women and gender-diverse people in every life stage, from childhood (Fang et al., 2022), to the reproductive years (Alhusen et al., 2023; Brown, Saunders, et al., 2022), and older adulthood (Lundy & Grossman, 2009). While GBV can impact disabled and nondisabled people in similar ways, people with disabilities encounter unique and compounded vulnerabilities that evolve across the life course. Children with disabilities are twice as likely as nondisabled children to experience violence (Fang et al., 2022), relying on abusers for caregiving and encountering ableist barriers to knowledge and disclosure, such as doubts of credibility (Jones & Taylor, 2018; Shah et al., 2016). Disabled women are at high risk of GBV during the reproductive years and pregnancy (Alhusen et al., 2023), facing reproductive coercion and fears of disclosing GBV due to concerns like losing custody of their children (Alhusen et al., 2020; Anyango et al., 2023). Providers often fail to screen for GBV in pregnant people with disabilities, even though such screening is recommended (Alhusen et al., 2020). Older adults with disabilities are also vulnerable to caregiver violence, including head/neck injuries (Frazão et al., 2014).
Specific age-cohort risks of GBV point to the importance of a life course perspective, which is used in public health to identify the influence of life stage-specific vulnerabilities on GBV (e.g., childhood abuse, reproductive coercion, and caregiver violence), trace how early experiences of GBV are associated with revictimization and harms that accumulate over time (Rogers et al., 2023; Sharratt et al., 2023), and document longitudinal health effects of violence (e.g., health issues in adulthood resulting from childhood abuse; McLindon et al., 2023). In the context of SRH, a life course approach can advance inquiry into how earlier GBV experiences shape SRH trajectories and how shifting power relations (e.g., from childhood to adulthood) can expose disabled people to different forms of harm over time.
Research has shown how GBV produces and reinforces health disparities across the life span. GBV has detrimental impacts on physical, mental, and social well-being (Dembo et al., 2018; R. B. Hughes et al., 2019); it can compromise SRH by increasing risks of pelvic pain, abnormal menstrual bleeding, urinary incontinence, sexually transmitted infections (STIs), unintended pregnancy, and perinatal complications (Coleman et al., 2024; Hassam et al., 2020; Pastor-Moreno et al., 2020) and limiting access to SRH services like cervical cancer screening (Cadman et al., 2012; Musa et al., 2019). Exposure to heterosexist/homophobic and cissexist/transphobic GBV at an early age can impact gender-diverse people’s social well-being (e.g., economic insecurity and homelessness; Bradford et al., 2013) and health outcomes (e.g., poor mental health and HIV transmission; Bockting, 2014; Stieglitz, 2010) both at the time of exposure and in later life.
People with disabilities who experience GBV are at increased risk of poor physical (Barrett et al., 2009) and mental health (Rowsell et al., 2013; Scherer et al., 2016), compared to those without disabilities. SRH inequities also disadvantage disabled people; ableism in health care leads to worse SRH outcomes for disabled compared to nondisabled people, particularly when providers are untrained in disability-informed care or fail to provide accommodations (Besoain-Saldaña et al., 2023; Biggs et al., 2023; Brennand & Santinele Martino, 2022). Thus, the intersection of GBV and SRH is compelling to examine, as the disproportionate harms of GBV may further compound SRH inequities for disabled people.
Studies have explored how disabled people’s experiences of GBV intersect with SRH concerns, such as perinatal health (Laughon et al., 2025). Yet, prior research has not explored intersections of disability, GBV, and SRH across the life course. This gap is notable in the context of gender-diverse and multiply marginalized disabled people, whose experiences are overlooked in both GBV and SRH research (Brinkman et al., 2023; Slothouber et al., 2025). Insight into how GBV shapes SRH outcomes for people with disabilities across the life course is needed, especially in light of the COVID-19 pandemic’s disproportionate impact on disabled people’s health (Brown, Saha, et al., 2022; Gignac et al., 2021; McBride-Henry et al., 2023) and its role in escalating rates of GBV globally (Kim & Royle, 2024). Building on existing disability and GBV scholarship, this qualitative study applies a life course theoretical framework (McLindon et al., 2023; Figure 1) and draws on queer feminist disability theory to investigate how women and gender-diverse people with disabilities experience GBV and how these experiences impact SRH needs and access to care over time.
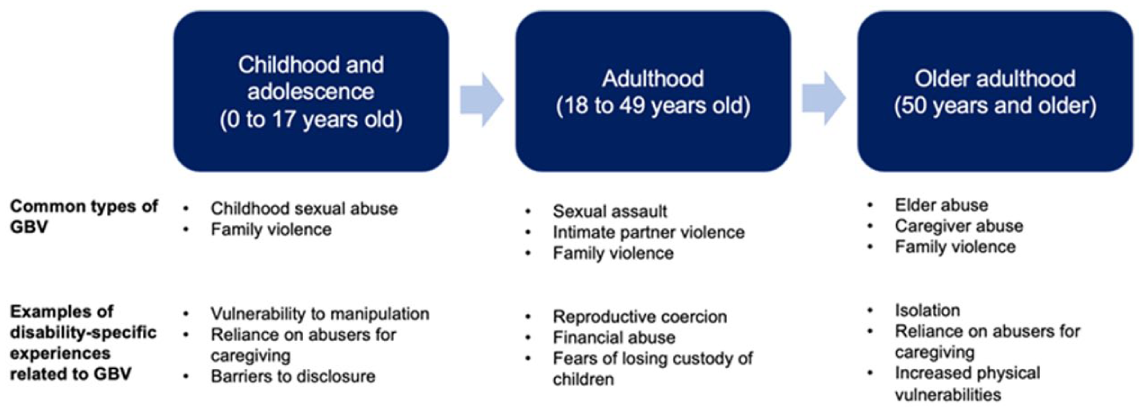
Summary of the life course perspective on GBV and disability.
Methods
Study Procedures
This study is part of a community-engaged qualitative project that explored the SRH experiences of women and gender-diverse people with disabilities in Canada during the COVID-19 pandemic. We worked with an advisory committee of disability advocates and collaborated with peer researchers with disabilities to colead the research. Participants were recruited via purposive sampling to prioritize diversity of identity and experience (Berg, 2001). Recruitment strategies included sharing accessible study materials (e.g., text and video) through disability organizations, the advisory committee, and the research team. Participants were 61 cisgender women, transgender women and men, nonbinary, genderqueer, and Two-Spirit people, 18 years or older, living in Canada, who self-identified as or could be identified as having a physical, sensory, cognitive, and/or mental health disability. This study was approved by the University of Toronto Research Ethics Board (Protocol Number 42194).
We conceptualize disability as a social experience rather than solely a medical/biological condition (Shakespeare, 2006), inclusive of people who self-identify as disabled – whether or not they are formally recognized as such by medico-legal systems – and those with impairments who may not identify as disabled for reasons like ableism or intersecting forms of oppression that complicate social identities (Schalk, 2022), or because they identify with specific communities (e.g., culturally Deaf; Skelton & Valentine, 2003). We use person-first (e.g., “with a disability”) and identity-first language (e.g., “disabled”) to reflect the varied self-conceptualizations of participants and the community (Andrews et al., 2022).
Participants provided verbal or written consent. A postdoctoral fellow and three peer researchers conducted 60-min semi-structured interviews by Zoom or telephone from May 2022 to March 2023. Accommodations (e.g., sign language interpreters) were available as needed. Participants were given an honorarium (40 CAD gift card) and a list of SRH resources. Interview questions covered disability experiences, SRH history, experiences with SRH services before and during the COVID-19 pandemic, and recommendations for improving SRH services. SRH was broadly defined to include experiences related to GBV. Participants were reminded they could skip questions and were not obligated to discuss any topics that made them uncomfortable. Data saturation was satisfied when consistent themes were reflected in the responses (Saunders et al., 2018).
The current descriptive study is based on a subset of 26 participants (43% of the overall sample) who voluntarily disclosed having experienced GBV during the COVID-19 pandemic or as part of their SRH history. While, broadly defined, GBV includes structural violence (Montesanti, 2015), this study focuses on interpersonal GBV perpetrated by family members and intimate partners (i.e., intimate partner violence and family/domestic violence, including childhood sexual abuse) and community members (e.g., sexual violence, abuse, or assault perpetrated by friends, acquaintances, caregivers, or strangers) throughout the life course (WHO, 2020b).
Data Analysis
A professional service transcribed interviews. The research team verified and de-identified transcripts and used NVivo 12 for coding. Initially, all 61 transcripts from the broader study were deductively coded by a peer researcher (AR) using descriptive and structural coding to identify SRH topics, including GBV. For the current analysis, we conducted a reflexive thematic analysis of the 26 transcripts in which participants discussed experiences of interpersonal GBV, following Braun and Clarke’s (2021) six-phase approach to inductive coding. The lead author (KJL) engaged in data familiarization through repeated close readings of the transcripts, making preliminary notes and impressions. Descriptive and interpretative open codes were generated inductively (Saldana, 2021), reflecting emerging patterns in GBV experiences. Codes were organized thematically, guided by a life course perspective. Themes were collaboratively reviewed with the research team to ensure coherence and relevance, drawing on research and lived expertise. Through elaborative coding and team discussion (Creswell, 2014), themes were defined and refined. Finally, thematic narratives were constructed to reflect shared patterns and divergent experiences.
Researcher Positionality and Reflexivity
The research team included women and gender-diverse people with lived experiences of disability and GBV and research expertise in disability, SRH, and GBV. This expertise enhances rigor by incorporating a range of perspectives and mitigating domination of singular truths in analysis (Birks et al., 2014). Our positionalities and commitment to anti-ableism and anti-oppressive praxes shaped how we engaged with the data: members with lived experience of disability brought attention to the nuances of participants’ experiences of ableism, while those with research expertise helped situate those narratives within broader policy contexts. We engaged in reflexive dialogue about how our positions informed interpretation and critically examined assumptions via iterative discussions. This reflexivity helped mitigate bias and supported an inclusive understanding of the data. Reporting adheres to the Standards for Reporting Qualitative Research guidelines (O’Brien et al., 2014).
Results
Table 1 summarizes the 26 participants’ pseudonyms and demographics. We identified 4 themes: intersections of disability and GBV experiences across the life course; impacts of GBV on reproductive health across the life course for people with disabilities; impacts of GBV on sexual health across the life course for people with disabilities; and impacts of GBV on access to and experiences with SRH services for people with disabilities (see Table 2).
Participant Demographic Information.
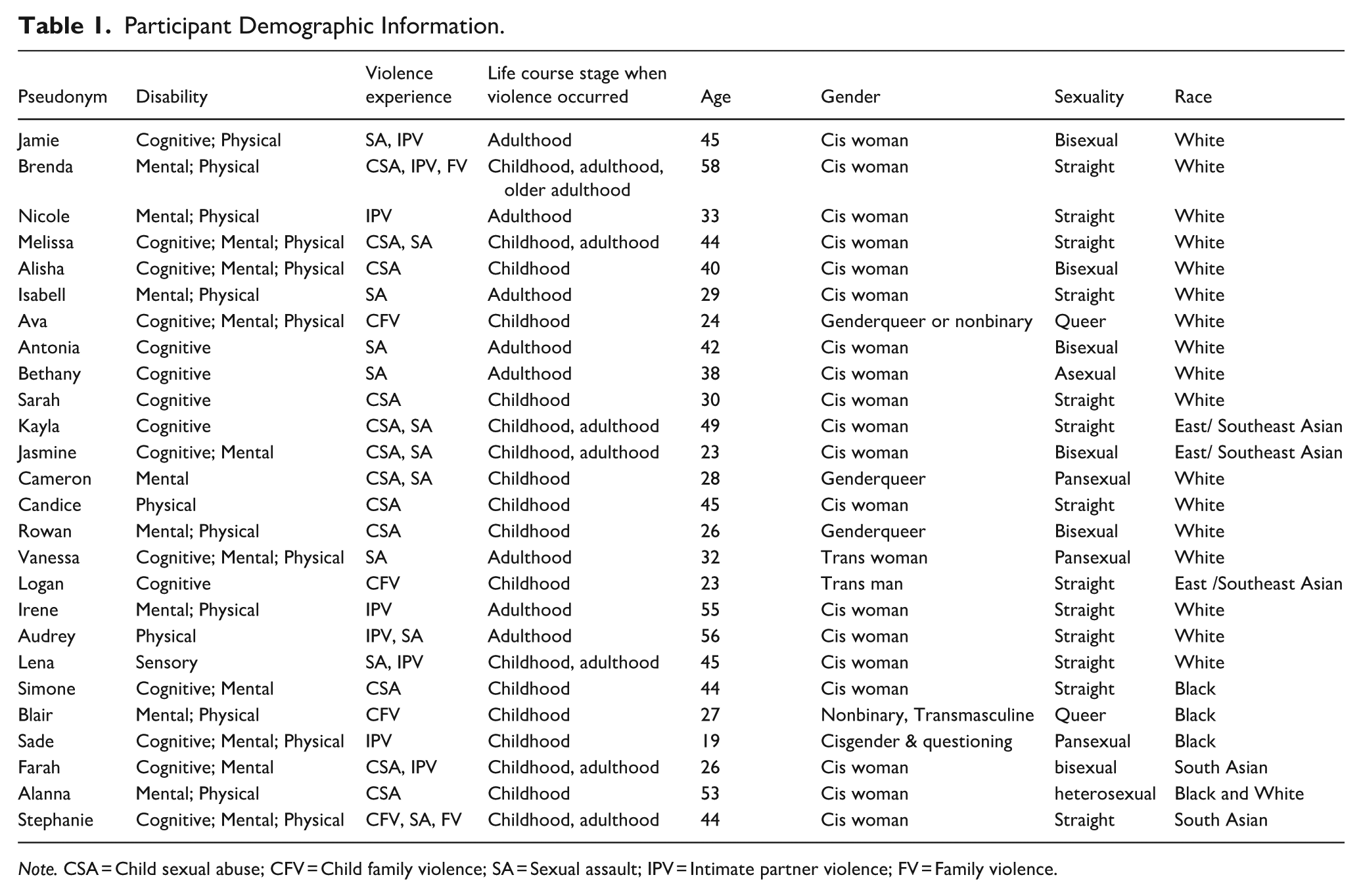
Note. CSA = Child sexual abuse; CFV = Child family violence; SA = Sexual assault; IPV = Intimate partner violence; FV = Family violence.
Summary of Themes, Subthemes, and Representative Quote.
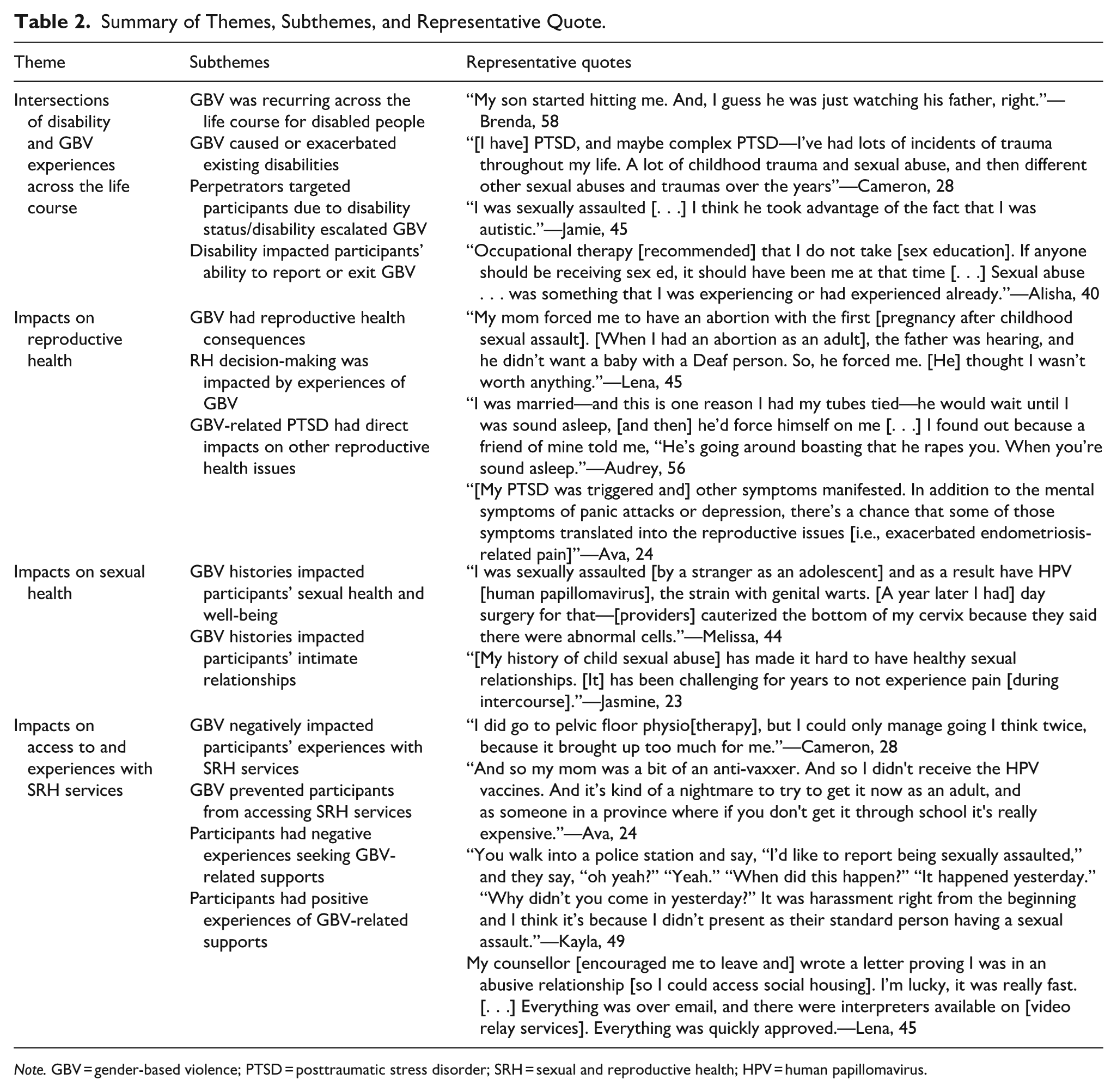
Note. GBV = gender-based violence; PTSD = posttraumatic stress disorder; SRH = sexual and reproductive health; HPV = human papillomavirus.
Intersections of Disability and GBV Experiences Across the Life Course
GBV recurred across the life stages of people with disabilities; many participants reported experiencing violence in childhood in addition to further violence in adulthood. For example, Brenda (58) experienced childhood abuse, followed by abuse from her ex-husband and, later, from her son (“My son started hitting me. And I guess he was just watching his father”).
GBV was intertwined with disability across the life course, causing the onset of some disabilities or exacerbating existing disabilities. Early experiences of violence during childhood caused mental health disabilities for several participants, such as posttraumatic stress disorder (PTSD), complex PTSD (C-PTSD), depression, and anxiety that persisted throughout adulthood.
[I have] PTSD, and maybe complex PTSD—I’ve had lots of incidents of trauma throughout my life. A lot of childhood trauma and sexual abuse and then different other sexual abuses and traumas over the years. (Cameron, 28) I have anxiety, depression, and it goes along with PTSD—mainly around abuse and sexual abuse and more [during] childhood, but then also as a mother, a wife, I was abused too. (Brenda, 58) My disability comes from the actions I took to flee [childhood] domestic violence. [Service providers] forced me onto Disability [social assistance], “We can’t expect you to work and we’re going to make a referral to Disability.” (Stephanie, 44)
Mental health disabilities caused by childhood GBV exacerbated some participants’ physical and cognitive disabilities in young and older adulthood. Ava (24) described experiencing abuse as a child, which led to “severe C-PTSD and through that a lot of comorbidities and sub-disorders [. . .] I have unidentified chronic pain but it’s probably [because] of C-PTSD.” Alanna (53) also attributed her physical disabilities (chronic illness, autoimmune issues, inflammatory arthritis) in older adulthood to the PTSD she acquired from being sexually abused in childhood: “they’re comorbid and interplay with each other. [. . .] Stress can trigger things. [. . .] Posttraumatic stress interacts with everything.”
Experiences of GBV were shaped by ableism; perpetrators exploited participants’ disabilities at different life stages to exert control, escalate harm, or entrap them. Some participants were targeted as children because of their disability, as perpetrators dehumanized and took advantage of their cognitive differences.
I was raped when I was younger, partly because I was Deaf. [. . .] I was only 14 and I couldn’t hear anything, and I didn’t know what was going on. [A group of boys] chased me [and] raped me on the way home [from school]. I was Deaf, and I was treated like I was no good. (Lena, 45) Being molested [as a child], there was so much shame with that. People with my [developmental/intellectual] disability are very gullible, so if you tell [me I’m] going to get in trouble [if I tell anyone], I’ll believe it, sure. (Kayla, 49)
In adulthood, perpetrators exercised power over participants’ disabilities, controlling communication, taking advantage of cognitive differences, or exploiting physical symptoms.
I was in an abusive relationship with my husband. [. . .] Physical, financial, emotional, sexual. [. . .] It escalated [during the pandemic]. I never was allowed to be by myself at home [. . .]. He controlled communication [. . .] he talked about what he wanted. That’s the only time he would sign [i.e., use American Sign language]. (Lena, 45) Part of my disability involves [not] knowing what’s [socially] acceptable [and that you have] the right to be able to [react when] you are being harassed. [. . .] That led to unwanted behaviour [and difficulty being able to] express myself and to use the right behaviour or body language to say, “leave me alone, I don’t want this.” (Bethany, 38) I found myself wondering since that [sexual assault] happened, whether that I would have been in that position if I wasn’t suffering from my physical disability. If I wasn’t on a whole bunch of pain meds and I wasn’t exhausted from pain all day [. . .], would it have even got that far? (Vanessa, 32)
Some participants experienced the ableist escalation of abuse by their perpetrators at different life course stages. Alisha (40) recalled that getting sick as a child with disabilities was a “huge trigger [. . .] for violence [and] abuse.” After Brenda (58) acquired physical disabilities in midlife, her husband “started to escalate [the abuse] and not think of [her] as a person.” Unsafe housing, financial insecurity, and reliance on caregivers, as well as the embodied realities of disability (e.g., chronic pain and exhaustion) made it difficult to leave.
To get this housing placement, I filled out paperwork that said I was fleeing domestic violence [. . .] I experienced assault and violence within the first year that I arrived [there]. (Stephanie, 44) I took a long time to leave [. . .] I didn’t feel strong enough because I was so tired with the chronic fatigue and a lot of pain. I thought I wouldn’t be able to do it. (Brenda, 58)
Impacts of GBV on Reproductive Health Across the Life Course
Participants reported GBV-related reproductive health consequences across the life course. Ableist restrictions on reproductive autonomy were reflected in experiences of reproductive coercion, including unintended pregnancies resulting from GBV, abortions enforced by caregivers, pressure to have abortions from intimate partners who did not want children with disabled persons, and providers imposing their own views about pregnancy.
[My ex-husband] would wait until I was sound asleep, [and then] he’d force himself on me. When I found out I was pregnant with twins, I pinpointed the day I got pregnant and I’m like, I don’t recall doing anything. And I found out because a friend of mine told me, “He’s going around boasting that he rapes you. When you’re sound asleep.” (Audrey, 56) My mom forced me to have an abortion with the first [pregnancy after childhood sexual assault]. [When I had an abortion as an adult], the father was hearing, and he didn’t want a baby with a Deaf person. So, he forced me. [He] thought I wasn’t worth anything. (Lena, 45) Growing up, there was abuse. I left home. I didn’t have any sexual education. I got pregnant. The person who impregnated me, I didn’t know them. They took advantage of the situation. [. . .] Because I’m a survivor of abuse, I dissociated from whether I was pregnant or not. I didn’t know the signs. I went to a doctor [who] imposed their view that I should get an abortion. [They] seemed judgmental of me, [and] I never got the proper information to make a decision. I wasn’t able to talk to anyone. I couldn’t make a decision [so] I kept moving further in the pregnancy. (Stephanie, 44)
At the same time, participants responded to experiences of GBV by making autonomous reproductive health decisions; several took actions at different life stages to regain control over their bodies, such as by using emergency contraceptives and seeking elective abortions in young adulthood, and pursuing sterilization in midlife.
I’ve had to use emergency contraception a few times [. . .] mostly [for] non-consensual stuff. (Jasmine, 23) My choice to terminate that pregnancy was because I was being abused. (Nicole, 33) [The abuse from my husband] is one reason I had my tubes tied. (Audrey, 56)
GBV-related PTSD impacted reproductive health issues across the life course, such as intensifying symptoms of endometriosis in early adulthood and menopause in later life.
[My PTSD was triggered and] other symptoms manifested. In addition to the mental symptoms of panic attacks or depression, there’s a chance that some of those symptoms translated into the reproductive issues [i.e., exacerbated endometriosis-related pain]. (Ava, 24) When I had my [hysterectomy], it ended up triggering my severe posttraumatic stress experience [. . .] That triggered memories, experiences, pain, lots of strange things happening in my body. With the instant menopause combined with it, I was a mess. (Alanna, 53)
Impacts of GBV on Sexual Health Across the Life Course
GBV histories had lasting impacts on participants’ sexual health throughout the life course. Melissa (44) continued to experience recurrent genital warts and abnormal cervical cells as a result of human papillomavirus (HPV) contracted from sexual assault in adolescence. Others described how histories of abuse influenced their engagement in high-risk sexual behaviors, showing how early experiences of GBV shaped sexual decision-making over time.
After being in an abusive relationship, I engaged in risky sexual behavior. I experienced pregnancy. And then I also had to deal with abortion. That was difficult and especially at a very young age, that affected my mental health a lot. (Farah, 26) I was romance scammed. Then I almost killed myself. I walked in front of vehicles. [. . .] I got caught in this cycle, which really was not good because it was tied into my PTSD [from childhood GBV]. It’s almost like I was hurting myself all the time, as I was trying to mess with the scammers. [. . .] I had to get out of an addiction to being an online romance junkie. Part of it was a sexual addiction. Some of them, we had sex over the phone or internet. [. . .] Some, I met them in person and had sex. [. . .] It was not safe. [. . .] I was assessed [and] told it was my PTSD. (Brenda, 58)
Early experiences of GBV impacted participants’ relationships later in life, making it difficult to engage in or enjoy sexual intimacy. Participants who experienced GBV in childhood described how its effects persisted into young adulthood, impacting their capacity to form trusting, pleasurable sexual relationships. In midlife, some reflected on how violence caused lasting challenges for their intimate lives with spouses. Some reported sexual dysfunction or pain disorders, such as dyspareunia, which they linked to earlier childhood trauma.
[My history of child sexual abuse] has made it hard to have healthy sexual relationships. [It] has been challenging for years to not experience pain [during intercourse]. (Jasmine, 23) I wasn’t ever really into [being intimate with my husband] because of my past of being assaulted and abused [. . .] It didn’t click to me as a way of expressing our affection to each other—it was, to me, something that happened to me with people who were scary, people who hurt me. [My husband and I] are openly affectionate but our actual sex life isn’t what I had wished it would’ve been. [I’ve] got this past that is still presenting barriers. (Kayla, 49) I was sexually abused as a young child [and recently] sought some counselling because I was having a lot of pain with intercourse [that] my doctor couldn’t explain [. . .] I’m on a waitlist to see a gynaecologist about the issue. I still have a wonderful intimate life with my husband but there are just some things that we avoid because of pain right now. (Candice, 45)
Impacts of GBV on Access to and Experiences with SRH Services
Across childhood and adulthood, participants had negative experiences seeking GBV-related supports, particularly when service providers (i.e., child protection services, health care providers, and police) responded with victim-blaming attitudes. For some, these early interactions led to a long-term reluctance to disclose violence and engage services.
I disclosed [childhood sexual abuse perpetrated by a sibling to child protection services]. [My parents] were absolutely horrified and disgusted. They put a lot of blame on me and [my sibling], and said that it was us doing it, and we couldn’t be allowed to be alone together. It was quite a horrible experience. There was no support [from child protection services] at all. I think that solidified those beliefs that it’s not safe to talk about these experiences. (Cameron, 28) [The gynecologist] shamed me. I’m like, “How is [being sexually assaulted] my fault?” He said, “How do you not know who this person is? Why didn’t you keep yourself safe?” [That experience years ago] is why I don’t like disclosing [my history of sexual assault to providers today], because I still feel that judgement. (Melissa, 44).
Participants described how service providers lacked the knowledge or skills to accommodate their disability-related needs, such as failing to adjust interview methods or recognize how people with disabilities may process or respond to situations differently.
The police didn’t know how to interview me correctly as an autistic person. [. . .] He kept asking me, “why did you go into the house?” Over and over again. [. . .] I felt I was being asked what I was wearing. He kept asking me, “[were you] drinking?” [. . .] [The psychiatrist also said] “if you didn’t go into the house, you wouldn’t have been raped. If you were able to read the social cues, if you weren’t autistic, you wouldn’t have been raped.” (Jamie, 45) You walk into a police station and say, “I’d like to report being sexually assaulted,” and they say, “oh yeah?” “Yeah.” “When did this happen?” “It happened yesterday.” “Why didn’t you come in yesterday?” It was harassment right from the beginning and I think it’s because I didn’t present as their standard person having a sexual assault. I was more calm, or I was too together about it or something. And that seems to really confuse people. Like it blows their mind. They can’t reconcile that a person standing there being calm and communicating clearly. (Kayla, 49) [Service providers] only understand medical [disabilities], not accommodations around violence against women. [. . .] They don’t understand the difference between disclosure and reporting, if I say, “I’m someone impacted by domestic violence.” [. . .] They don’t have a category for people impacted by domestic violence in accessibility [. . .] For example, if you don’t want to be in the waiting room or have them call out your name, how can we arrange it? If I tell the receptionist that, they will say to ask the doctor, and the doctor will say this is not a medical question. (Stephanie, 44)
Experiences of domestic and family violence from parents and caregivers in childhood restricted participants’ access to SRH services, which continued to affect them as young adults. Ava’s (24) abusive parent withheld consent for her to receive the HPV vaccine in grade school, and she was encountering financial barriers trying to access the vaccine as a young adult. Logan (23), a trans man, experienced cissexist/transphobic family violence from his parents throughout childhood and struggled to access gender-affirming care as an adolescent living in their home. After he moved into a group home for queer youth, staff at the 2SLGBTQIA+ community health clinic helped him navigate transition-related care:
I didn’t have the information [. . .] but the lady that was working [at the 2SLGBTQIA+ community health clinic] actually was a counsellor that does intake. And I was able to get the information, get a pamphlet and go straight to the doctor to get the medical stuff out of the way such as transition‑related care and finding chest binders.
Participants’ GBV histories impacted their relationship to SRH services as adults. Some avoided care altogether due to fear and discomfort stemming from earlier trauma, while others reported interactions with services (e.g., painful pelvic exams) shaped by ableism and intersecting forms of oppression, such as racism.
I let the family doctor do [the pap test] and [she assumed] I was not sexually active [and that] she could use a smaller probe. She kept digging around and it was one of the worst pap smears I ever had in my life. [. . .] I haven’t had pap smears since [that negative experience]. I need [providers] to understand that our sexuality and our health is intertwined and comorbid. Many [older Black women] have experienced sexual violence or physical violence, which I have as well, which comes along with trust issues with the medical field. (Alanna, 53) Because of the PTSD that I have, anytime I’m going through any menstrual, pelvic floor, or reproductive issue of any kind, there’s a lot of blame associated with that [and] thinking that this is my fault. [I have] pelvic floor [related] muscular pain as well. [. . .] I did go to pelvic floor physio[therapy], but I could only manage going I think twice, because it brought up too much for me. (Cameron, 28)
Some participants had positive experiences seeking GBV supports in adulthood, often for violence that occurred earlier in life, when service providers facilitated disability-related accommodations and were knowledgeable about disabilities. For example, with the increase in telehealth availability during the COVID-19 pandemic, Candice (44) sought counseling in her mid-40s for abuse she experienced as a child, showing how opportunities for healing can emerge later in life when care is accessible. Lena’s (45) counselor supported her to leave her abusive ex-husband and access social housing; this process was accommodating for her as a Deaf woman, as “everything was over email, and there were interpreters available.” Jamie (45) described the benefit of finding a counselor with knowledge of autism, who helped her process her sexual assault. Such experiences highlight how disability-affirming, trauma-informed care can facilitate recovery across the life course.
Discussion
Using a life course perspective, this qualitative descriptive study documented experiences of GBV, and their impacts on SRH, among women and gender-diverse people with disabilities. Disability, GBV, and SRH were closely intertwined: GBV recurred across the life course and was disabling for participants; ableism made participants more vulnerable to GBV; and GBV had significant consequences for SRH outcomes and access to care across the life course. Impacts on SRH were far-reaching, including reproductive coercion, constrained decisions about contraception and sterilization, negative experiences with menopause, high-risk sexual behaviors, and difficulties with sexual intimacy. Negative experiences with SRH services undermined trust in providers and discouraged disclosure of GBV histories; positive experiences with services facilitated paths to recovery and empowered some to exit violent situations. These findings show the value of applying a life course perspective to understand how the effects of GBV accumulate over time to shape SRH among people with disabilities.
GBV has previously been conceptualized as disabling (Mays, 2006; Neath, 1997), with studies documenting implications related to physical health (e.g., traumatic brain injury, Karakurt et al., 2021; activity limitations, Sanz-Barbero et al., 2019; headaches and gastrointestinal disorders; Gilbert et al., 2022) and mental health (e.g., PTSD, depressive symptoms, and suicidal ideation; Rowsell et al., 2013; Scherer et al., 2016). Our study is consistent with these studies, depicting how GBV was seen as a disability-inducing event with mental health consequences (e.g., C-PTSD from childhood sexual abuse) and how these mental health disabilities exacerbated physical disabilities (e.g., chronic pain) later in life.
The high rates of GBV (Amborski et al., 2022; Bowen & Swift, 2019; García-Cuéllar et al., 2023) and other violence by people with disabilities are well-documented. GBV risks have been studied at important points across the life course, including in childhood (Fang et al., 2022), the reproductive years (Alhusen et al., 2023; Brown, Saunders, et al., 2022), and in older age (Lundy & Grossman, 2009). We provide an important perspective by drawing a connection between experiences of GBV during these life stages and subsequent SRH outcomes and access to services. This important contribution moves beyond examining disability as a risk factor for GBV at certain life stages (e.g., childhood and pregnancy) to show how the SRH impacts of GBV intersect with and compound experiences of ableism and other forms of oppression (e.g., cis/sexism, racism, and classism) over the life course.
The SRH of people with disabilities has received little attention (Addlakha et al., 2017), particularly in relation to GBV. Prior studies in the general population have shown GBV compromises other SRH outcomes, increasing risks of gynecologic conditions, urinary incontinence, STIs, unintended pregnancy, and perinatal complications (Hassam et al., 2020; Pastor-Moreno et al., 2020). People who have experienced GBV are also less likely to access SRH services like cervical cancer screening (Cadman et al., 2012; Musa et al., 2019). Our study adds to and affirms these findings by showing disabled people experience the SRH impacts of GBV in similar and unique ways; we documented participants’ ableist experiences of GBV (e.g., being targeted due to disability), interactions between disabilities and SRH concerns (e.g., PTSD exacerbating endometriosis pain), and experiences of ableist barriers to care when seeking GBV and SRH services (e.g., assumptions of sexual inactivity during pap smears). To our knowledge, this is the first study that examines the SRH impacts of GBV among people with disabilities using a life course perspective. Given the high, and likely underreported, prevalence of childhood sexual abuse among disabled people, it is important to draw attention to the SRH impacts of GBV over the life course in this group.
Several factors likely explain our observations. People with disabilities experience many of the known risk factors for GBV at elevated rates compared to their peers, including poverty (Ballan & Freyer, 2017), social isolation, power imbalances with caregivers in childhood (e.g., parents) and adulthood (e.g., intimate partners; Jones & Taylor, 2018; Shah et al., 2016), and reduced access to education related to violence (Jones & Taylor, 2018). Tools typically used for GBV screening in clinical settings also do not include items about forms of violence that are unique to individuals with disabilities (e.g., refusal to assist with activities of daily living; Bradbury-Jones et al., 2015), and people with disabilities encounter ableist barriers to disclosure (Jones & Taylor, 2018; Shah et al., 2016), including victim-blaming. In parallel, people with disabilities experience barriers accessing SRH care, including being less likely to receive SRH education in school (Frawley & Wilson, 2016) and SRH services in primary care (Marquis et al., 2023). These dual barriers to GBV and SRH care may contribute to the significant SRH consequences of GBV reported by participants in our study, and these issues are further compounded by intersecting social and structural inequities like gender identity and race (Kafer, 2013; Schalk, 2022).
Our findings add an important life course perspective to the topic of GBV and SRH among people with disabilities. However, the sample underrepresented people of color, gender-diverse people, queer people, older people, and people with sensory disabilities, limiting the study’s ability to capture diverse experiences. Future studies should explore the intersections between ableism and racism, cissexism, heterosexism, and ageism in the context of GBV and SRH, as well as the experiences of specific disability groups (e.g., Deaf communities). Because our analysis of GBV was based on voluntary disclosures within an SRH-focused study, not exclusively centered on GBV, there is a possibility of selection bias. Those who felt more comfortable disclosing experiences may be overrepresented, while others may have withheld disclosures due to discomfort or lack of direct questioning. Safety was prioritized and participants were encouraged to only share what they felt comfortable. Since GBV was not systematically explored across all interviews, data saturation may be incomplete. As such, findings should be interpreted as exploratory rather than exhaustive. Finally, while institutional violence is disproportionately experienced by people with disabilities (Spivakovsky & Steele, 2022), our study is limited to interpersonal GBV.
Our findings show the need for disability education for service providers who deliver GBV (e.g., police, emergency department physicians and nurses, shelter staff) and SRH care (e.g., primary care providers, gynecologists, obstetricians), including information about accessibility needs, unique types of violence that may be experienced by disabled people (e.g., withholding communication supports), and available resources (Ballan & Freyer, 2017; Shelton, 2020). Training needs to address the intersection of GBV and SRH among people with disabilities; for example, some health care providers hold the misconception that people with disabilities do not engage in intimate relationships and may underestimate their risk of forms of GBV such as intimate partner violence (Thompson et al., 2014), despite intimate partners being the most common perpetrators of abuse against disabled women (Ballan & Freyer, 2017). Enhanced training will help combat these misconceptions and ableist attitudes.
Findings also support the need to develop disability-affirming and trauma- and violence-informed SRH and GBV services across the life course. We recommend that SRH services prioritize the development of accessible resources, such as education and peer support, to help people with disabilities prevent, identify, and manage GBV (Mingus, 2017; Shelton, 2020). SRH services should incorporate screening tools for GBV that consider the unique types of violence often experienced by people with disabilities (Houck & Dracobly, 2023). In parallel, GBV services (e.g., sexual assault clinics and shelters) should ensure services and referrals accommodate disability-related needs (e.g., hiring interpreters and making facilities wheelchair-accessible) and hiring peer navigators to support people with disabilities accessing care (Eliacin et al., 2023). Finally, to make services anti-ableist and disability-affirming, GBV and SRH providers should collaborate with lived experience experts and advocates in the development and delivery of care (Hasstedt & Rowan, 2016).
Footnotes
Acknowledgements
The authors wish to acknowledge the study participants for their essential contributions to this research. The authors also wish to express thanks to the members of the study advisory committee who assisted with recruitment and development of the data collection materials.
Ethical Considerations
This study was approved by the University of Toronto Research Ethics Board (Protocol Number 42194, approved January 21st, 2022). Participants provided verbal or written consent, per University of Toronto Research Ethics Board guidelines.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by a Canadian Institutes of Health Research Operating Grant on Emerging COVID-19 Research Gaps & Priorities (Funding Reference # 179437). This research was undertaken, in part, thanks to funding from the Canada Research Chairs Program to Hilary K. Brown (2019-00158). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
Data cannot be shared due to research ethics board restrictions.