
Abstract
Research on aggression towards family/caregivers in childhood and adolescence (AFCCA) is still emerging, particularly within the Canadian context. To better understand this behaviour, we examined potential changes in the severity and frequency of different AFCCA types as well as in caregiver-child relationships and disruptions to families’ lives during the COVID-19 pandemic. In this convergent/parallel mixed-method research study, 168 Canadian caregivers living with a young person who exhibited AFCCA completed an online survey that contained self-report questionnaires and open-ended questions. The sample consisted primarily of adoptive mothers. Descriptive and hybrid thematic analyses indicated that around half the sample reported an increase in the severity (verbal 43.9%, threats 39.8%, emotional/psychological 49.2%, physical 44.3%) and frequency (verbal 51.2%, threats 47.8%, emotional/psychological 54.6%, physical 48.3%) of most AFCCA types. The quality of the caregiver-child relationship also worsened significantly after the pandemic (t[115] = 3.5, p = .001). Qualitative analyses supported this finding. While there was no statistically significant difference in AFCCA-related disruptions to families’ lives during the pandemic, thematic analyses revealed increased caregiver disruptions to both personal aspects (e.g. self-care practices, alcohol/substance use) and professional obligations (e.g. missed work). This study underscores the need for sustained and accessible (online and in-person) supports that are grounded in intersectionality, responsive to families’ unique needs and sensitive to young people’s experiences with past adversity.
Keywords
Introduction
The COVID-19 pandemic was associated with increases in the occurrence and severity of aggression within families (Huang et al., 2023; Kourti et al., 2023; Park & Walsh, 2022; Pereda & Díaz‑Faes, 2020) and negative impacts on young people’s mental well-being (Children First Canada, 2024; Guessoum et al., 2020; Jones et al., 2021). To contribute to growing understandings of its global impacts, we examined young people’s aggressive behaviours towards caregivers during the pandemic, primarily by way of adoptive families. We began with a clarification of the definition and frequency of youth-initiated aggression within an ecological framework; we then presented research on the relationship between the pandemic, increased family aggression, decreased youth mental well-being, and increased youth-initiated aggression. Following the literature review and study overview, we presented findings on pandemic-related impacts which informed our family-centred recommendations, concluding with study limitations that point to future research directions.
Defining Young People’s Aggressive Behaviours Within Families
Various terms have been used to describe young people’s aggressive behaviours towards caregivers, including child-to-parent aggression, child-to-parent violence, child/adolescent-to-parent violence, child-to-parent violence or aggression, parent abuse, violence against parents, adolescent violence in the home and parent-directed aggression (Condry et al., 2020; see also Rutter’s, 2023 review of terms). In Canada, the National Consortium on Aggression Towards Family and Caregivers in Childhood and Adolescence (AFCCA) (2021) developed the term Aggression Towards Family/Caregivers in Childhood and Adolescence (AFCCA), which includes a pattern of behaviour that ‘causes significant harm (physical and/or psychological) to the child/adolescent, the person(s) the behaviour is directed toward, and other witnessing family members’ (p. 27). Given the overlap in aggressive behaviours encompassed by the various terms, we selected the term AFCCA as it is inclusive of all family members (e.g. siblings), and incorporates a range of behaviours that extend beyond the more typically examined physical and verbal aggression (e.g. psychological, sexual and threats of harm). Moreover, the term is potentially less stigmatizing as it emphasizes understanding aggression within the family system and recognizing the harmful impacts for all family members, including the young person who initiated the aggressive behaviour (Gervais et al., 2022); National Consortium on AFCCA, 2021; Rutter, 2023). While we have considered implications for other relatives elsewhere (DeCarlo-Slobodnik & Gervais, 2022; Gervais et al., 2022), we are focusing only on the caregiver level in the current study.
Frequency of Occurrence
The occurrence of AFCCA is of concern and has been examined using various terminology in both Canadian and international contexts, such as Spain (Cano-Lozano et al., 2021a, 2021b; Del Hoyo-Bilbao et al., 2019), Chile (Ilabaca Baeza & Gaete Fiscella, 2021; Jiménez-García et al., 2022), Australia (Moulds et al., 2019), United States (Walsh & Krienert, 2009) and United Kingdom (Kuay et al., 2023). Simmons et al. (2018) reviewed 60 years of research, finding that the 12-month prevalence of adolescent-initiated physical aggression towards caregivers ranged from 5% to 21%, while verbal, psychological, and emotional aggression ranged from 33% to 93%. While AFCCA occurs across all family types, our sample included primarily young people in adoptive homes. Selwyn et al. (2014) found that 57% of young people in United Kingdom adoptive families exhibited AFCCA, consistent with international studies and research syntheses. Adopted youth may be especially vulnerable due to past experiences within their biological homes that often included significant, persistent and accumulated trauma and adversity (Lyttle et al., 2021; Selwyn & Meakings, 2016; Selwyn et al., 2014). In Canada, AFCCA research remains limited. A study of 1,175 15- to 16-year-olds from the province of Quebec showed that, over a 6-month period, 13.7% engaged in physical and 64% engaged in verbal aggression towards their mothers (Pagani et al., 2004), while the rates of aggressive behaviour towards fathers among 774 fifteen- to sixteen-year-olds were 11% for physical and 56% for verbal aggression (Pagani et al., 2009). Lyons et al. (2015) sampled 365 Canadian university students about their childhood behaviours, using the Conflict Tactics Scales Child-to-Parent version, and found low mean scores for verbal aggression towards both parents, with a significantly higher score for mothers; physical aggression also was significantly higher towards mothers (6.3%) than fathers (5.5%). Canadian studies align with broader research showing the higher occurrence of non-physical aggression (e.g. Jiménez-Granado et al., 2025; Simmons et al., 2018) and the higher frequency of mothers as targets of aggression (e.g. Ilabaca Baeza & Gaete Fiscella, 2021; Moulds et al., 2019).
Ecological Framework
Factors associated with AFCCA are best understood within an ecological framework (Cottrell & Monk, 2004; Del Hoyo-Bilbao et al., 2019; Ilabaca Baeza & Gaete Fiscella, 2021), which captures the multi-level range of influences (from individual and family to broader social, cultural, political, and ideological factors) and the bi-directional interactions among them. Cottrell and Monk (2004) combined findings from two Canadian qualitative studies, using the ecological framework, to identify youth risk factors of AFCCA (issues with attachment, mental health, substance use, childhood victimization), family factors (parenting difficulties, parental conflict), social factors (financial hardship, limited support) and cultural beliefs (gender inequality, negative media exposure). Additional family-level factors included difficult relationships, low parental warmth, and family violence exposure (Simmons et al., 2018). At the individual level, neurodevelopmental conditions (e.g. prenatal alcohol exposure, autism, intellectual disabilities), along with poor mental health related to isolation, emotion regulation, impulse control and sensory processing challenges, have also been linked to AFCCA (Champagne et al., 2023; National Consortium on AFCCA, 2021).
COVID-19 Pandemic
Given the growing knowledge of the pandemic’s impacts on young people’s mental health and family violence in the home, it was important to examine AFCCA within this context. Reviews show that the pandemic was associated with increases in many forms of family violence, including intimate partner violence and child abuse (Huang et al., 2023; Kourti et al., 2023; McDowell et al., 2024; Park & Walsh, 2022; Pereda & Díaz‑Faes, 2020). At the parental level, Italian data indicate that the pandemic was linked to a poorer sense of psychological well-being in mothers and children, with greater maternal perceived stress and increased depressive symptoms contributing to greater child emotional and behavioural difficulties (Spina et al., 2023). In a Belgian online survey with 506 caregivers during the pandemic, Desimpelare et al. (2023) also found that caregivers of children with complex physical, intellectual, emotional or behavioural needs experienced even greater levels of stress and burnout.
For young people’s mental health, systematic reviews showed the pandemic’s negative impact on anxiety, depression, and post-traumatic stress symptoms (Guessoum et al., 2020; Jones et al., 2021). A U.S. qualitative study with 20 adolescents (12–19 years) already experiencing pre-pandemic mental health difficulties found that the pandemic led to declining mental health, loss of motivation, and negative as well as positive relationship changes – all linked to isolation, routine disruptions, and limited access to resources due to closures (Sobalvarro et al., 2023). In a recent Children First Canada (2024) report on the top 10 threats to Canadian children, poor mental health ranked second, with 51% of 12- to 18-year-olds experiencing depression, and 39% experiencing anxiety, during the pandemic.
Empirical research on AFCCA during the COVID-19 pandemic remains limited. In a U.K. study, Miles et al. (2024) surveyed 104 caregivers of 10- to 19-year-olds experiencing what they referred to as child- and adolescent-to-parent violence and abuse (CAPVA) and the practitioners working with these families. Findings revealed that 70% reported increased CAPVA during the lockdown, primarily explained by spatial confinement (proximity), disrupted structure and routines, fear and anxiety and increased opportunities for CAPVA. Notably, 29% of parents reported a decrease, which was attributed to fewer violence-related stressors during that time. In Spain, Cano-Lozano et al. (2021b) found that 59.4% to 65.2% of 2,245 young adults (18–25 years) reported at least one act of aggression (primarily psychological) towards a parent within a 1-month period. In a more recent Spanish study (Calvete et al., 2023), 1,244 twelve- to seventeen-year-olds completed a self-report measure (Child-to-Parent Aggression Questionnaire-Revised) during the pandemic, and half reported at least one aggressive behaviour in the past year towards their mother (49.9%) or father (51.8%). Verbal aggression (e.g. insulting) was the most reported, followed by intimidation (e.g. making a parent feel scared) and then physical aggression, with no significant caregiver or youth gender differences. Like past research, the authors noted that these aggressive behaviours may have been a function of confinement, changes in structure/routines, reduced access to supports and/or the increase of intimate partner violence and child abuse.
Study Objectives
Building on previous research, we aimed to increase understanding of AFCCA by examining its presentation among families during the pandemic. We focused on AFCCA from the perspective of Canadian adoptive, kinship, customary, biological and foster caregivers (Gervais et al., 2022; Ontario Association of Children’s Aid Societies [OACAS], n.d.) We used a convergent/parallel mixed-methods research design, incorporating survey results from 168 caregivers along with open-ended questions that provided greater context for the quantitative responses. All questions addressed three main research objectives: (1 – a) Examine caregivers’ experiences with AFCCA frequency and severity before and during the pandemic. (b) Explore caregivers’ experiences with a child exhibiting AFCCA during the pandemic. We hypothesized that caregivers would report an increase in the frequency and severity of each AFCCA type during the pandemic. (2 – a) Examine caregivers’ perceptions of the caregiver-child relationship before and during the pandemic. (b) Explore how caregivers with a child exhibiting AFCCA explain their relationship with their child during the pandemic. We hypothesized that the caregiver-child relationship would have significantly worsened during the pandemic. (3 – a) Examine caregivers’ reported disruptions to family life during the pandemic as a function of their child’s AFCCA. (b) Explore how caregivers with a child exhibiting AFCCA explain changes to their family’s life during the pandemic. We hypothesized that AFCCA-related disruptions to family life would have significantly worsened during the pandemic.
Method
Study Design and Procedures
We obtained ethics approval from our university’s ethics review board. To address the study objectives, we applied a convergent/parallel interactive mixed-methods design (Creswell & Plano Clark, 2018), collecting qualitative and quantitative data concurrently, analyzing them independently, and merging the results during interpretation/presentation to allow for triangulation and evaluation of complementary and/or diverging results. Data collection occurred between August 2021 and May 2022 and was managed by a graduate-level research assistant. Participants were recruited primarily through organizations working with adoptive families to offer parenting and mental health resources. These organizations distributed study information virtually to caregivers across Canada through emails or website postings that included a link to the online questionnaire. Eligible participants included adult adoptive, kinship, customary, biological and foster caregivers in Canada caring for a young person with AFCCA-type behaviours. To ensure a sense of inclusivity, recruitment-related communications emphasized that caregivers representing families of diverse identities (including Indigenous backgrounds), geographic locations (e.g. rural and urban, regional), and family compositions and experiences (e.g. blended, adverse) were welcome to participate in the study.
Sample
The original sample consisted of 182 caregivers; however, 14 were removed as they indicated no experiences of AFCCA (n = 168). Among caregivers, 117 were currently experiencing AFCCA, while 51 had experienced AFCCA in the past. Caregiver age ranged from 28 to 71 years (M = 47.2, SD = 9.0). The majority identified as female (94.6%), followed by male (4.8%) and non-binary/third gender (0.6%). The majority of caregivers identified their sexual identity as straight/heterosexual (83.3%), followed by gay or lesbian (8.6%), bisexual (4.3%), queer (3.1%) and two-spirit (0.6%). Most caregivers identified as White (87.4%), followed by a mix of White and Indigenous heritage (3.6%), Indigenous (2.4%), Asian (1.8%), Southeast Asian (1.2%) and Hispanic (1.2%). Most caregivers reported being married (69.5%) and holding an undergraduate degree (44%). Half of the caregivers had full-time employment (51.2%). One-third (33.3%) reported an average yearly household income between $80,000 and $109,999 in Canadian dollars, while 20.8% earned over $150,000. Most caregivers resided in the province of Ontario (67.9%), followed by British Columbia (17%), Québec (6.7%), Saskatchewan (4.8%), New Brunswick (1.8%) and Nova Scotia (0.6%). The language most spoken at home was English (88.1%) and then French (10.7%). The majority reported being an adoptive caregiver (82.7%), followed by kinship caregiver (9.3%), foster caregiver (3.1%), customary caregiver (2.5%) and biological caregiver (1.2%).
The young people, who were identified by caregivers as exhibiting AFCCA, ranged in age from 1 to 20 years (M = 12.7, SD = 4.5) and were mostly male (52.5%), followed by female (43.1%), non-binary/third gender (1.3%) and transgender (1.3%). Half of the caregivers revealed that the young person in their care had not yet (or at all) identified a sexual orientation while the remainder reportedly identified as straight/heterosexual (37.7%), followed by bisexual (7.5%), gay or lesbian (1.9%), queer (0.6%), asexual (.06%), pansexual (0.6%) and two-spirit (0.6%). Most of the young people were White (69.1%), followed by Indigenous (19.7%: First Nation 13.7%, Métis 2.4%, Inuit 3%), Black/African Canadian/Afro-Caribbean Canadian (10.7%), Asian (3.6%), Hispanic (3%), Southeast Asian (1.8%) and Middle Eastern (0.6%). Among non-biological caregivers, the child’s age when coming into their care ranged from 1 to 14 years (M = 4.5, SD = 3.1), and the age range for when their child started showing signs of AFCCA in their home was 1 to 16 (M = 6.2, SD = 3.7). Caregivers reported various confirmed neurodiverse profiles among youth in their care, including Attention-deficit/hyperactivity disorder (ADHD; 74.6%), learning differences (69%) and autism (9.7%). They also reported that many youth had fetal alcohol spectrum disorder (FASD; 28.7%) and showed signs of traumatic stress reactions (26.5%). While certain demographic details are noted with the quotes to provide relational context, other identifying information (e.g. geographic location) was omitted to protect participants’ anonymity.
Measures
We developed an online survey that gathered information on family socio-demographics, the child’s background, lived experiences, functioning, AFCCA (types, frequency, severity, onset, impacts, caregiver coping), child-caregiver relationship, and children’s rights. By way of open-ended questions, respondents were also given opportunities to provide comments (with no word limits) on pandemic-related family impacts and relationship changes. Given the period in which the survey was conducted, there were specific questions about potential changes in AFCCA as a function of the COVID-19 pandemic. The survey items were developed by considering both prevalent and absent themes in the existing AFCCA literature (Berg, 2007; Gervais et al., 2022; National Consortium on AFCCA, 2021; Selwyn & Meakings, 2016; Selwyn et al., 2014; Thorley & Coates, 2019). Although we were aware of certain standardized measures of AFCCA (i.e. Child-to-Parent Aggression Questionnaire), we relied on a U.K. survey (Selwyn et al., 2018) that used items from a previous project (Responding to Child to Parent Violence Project; Ferrando, 2015). We adapted Selwyn et al.’s (2018) survey for adoptive families, allowing for the possibility of making some comparisons with our current study findings. All survey questions were reviewed by a Canadian-based advisory group consisting of professionals, parents, and young people knowledgeable about AFCCA. Based on this review, and similar to revisions applied by other researchers examining this behaviour (e.g. Calvete et al., 2023), we made minor modifications to some items. These changes (e.g. edited or added questions) addressed the Canadian context (e.g. provincial/territorial variations in services), pandemic circumstances (e.g. lockdown implications), importance of diversity-sensitive, non-stigmatizing language and inclusive representation (e.g. recognizing that many children in adoptive families have experienced past adversity and that families often feel stigma when AFCCA has occurred), and the study’s overarching child-rights approach, while also shortening the survey to make it more feasible and accessible for potential respondents.
Frequency of AFCCA Pre-Pandemic
We developed a question on the frequency of AFCCA prior to the pandemic. Caregivers were asked: Prior to the COVID-19 pandemic (March 2020), how often did your child act in the following way towards you? This question was followed by a list of 19 AFCCA items from Selwyn et al. (2018) that covered 5 areas, namely threats of harm (7 items; threatened you or the other parent with a knife or a weapon), psychological/emotional aggression (1 item; tried to stop you from talking to your friends or family), physical aggression (8 items; pushed, grabbed, scratched, or shoved you or the other parent), verbal aggression (2 items; screamed or yelled at you) and sexual aggression (1 item; sexually abusive towards you or the other parent). Each item was scored on a 5-point Likert scale ranging from 1 (never) to 5 (almost every day). Scores could range from 7 to 35 for threats, 1 to 5 for psychological/emotional aggression, 8 to 40 for physical aggression, 2 to 10 for verbal aggression and 1 to 5 for sexual aggression. Higher scores indicated higher levels of AFCCA. The internal consistencies for all AFCCA types with more than one item were in the acceptable range (threats α = .75; physical aggression/abuse α = .81 and verbal abuse α = .61).
AFCCA Frequency and Severity Changes Due to the Pandemic
For frequency, we asked caregivers: Have the aggressive behaviours in the following broad categories happened more often, the same amount, or less often during/since the start of the COVID-19 pandemic? Each item was scored on a 3-point Likert scale, ranging from 1 (happens less often since COVID) to 3 (happens more often since COVID). For severity, we asked caregivers: Have the aggressive behaviours in the following broad categories gotten worse, stayed the same or gotten better during/since the start of the COVID-19 pandemic? Each item was scored on a 3-point Likert scale, ranging from 1 (gotten worse since COVID) to 3 (gotten better since COVID). These questions were followed by a list of five broad AFCCA categories – threats of harm, psychological/emotional, physical, verbal and sexual aggression.
AFCCA-Related Family Impacts Due to the Pandemic
The impacts of AFCCA on families as a function of the pandemic were assessed using a 5-point Likert scale ranging from 1 (not at all) to 5 (a great deal). The items were from Selwyn et al. (2018), based on an adapted version for use by adoptive caregivers of the Caregiver Commitment and Strain Questionnaire (Brannan et al., 1997, 2012). Caregivers were asked: Before the COVID-19 pandemic (i.e. before March 2020), how much of a problem was each of the following as a result of your child’s aggressive behaviour towards you? This question was followed by a list of nine AFCCA impact-related items that covered caregiver-related life domains, namely personal time, job-related obligations, family routines/activities, financial strain, attention to other family members, relationships within the family and community, self-care and alcohol/substance use. Caregivers were asked the same question a second time, but with specific reference to the time period during or following the COVID-19 pandemic. Total scores could range from 9 to 45, with higher scores indicating a greater negative impact on families. Internal consistency was acceptable for both scales (before pandemic α = .75, and since pandemic α = .90).
Child-Caregiver Relationship
We developed two questions to examine caregivers’ perceived relationship with their child before and after the pandemic questions: How would you describe your relationship with your child before the COVID-19 pandemic or before March 2020? And How would you describe your current relationship with your child since/during the COVID-19 pandemic or after March 2020? Responses were along a 5-point Likert scale ranging from 1 (very difficult) to 5 (very positive). Total scores for each item could range from 1 to 5, with higher scores indicating a better-quality relationship.
Data Analysis
Quantitative Methods
The Expectation-Maximization algorithm was used to impute missing data, which ranged from 0.9% to 2.6%. Multivariate normality and outliers were first assessed, as well as skewness and kurtosis, which were screened and deemed acceptable using cut-off scores from < ±2 (George & Mallery, 2009). Study variables were examined using frequencies, total mean scores, standard deviations and correlations. Paired-sample t-tests were conducted to examine mean score changes in AFCCA behaviours from pre- to post-pandemic. A probability level of .05 was used for statistical significance testing. Analyses were conducted using IBM SPSS Statistics (Version 28). This study is part of a larger project, and our current focus is on a more descriptive and broader approach to the topic of AFCCA. Future analyses from the larger project will include more multivariate considerations and evaluate potential indicators of AFCCA, including differences related to caregiver type, child gender, neurodivergence and past adverse experiences.
Qualitative Methods
Using a descriptive thematic analysis, open-ended responses were analyzed with a hybrid approach (inductive and deductive) to coding (Fereday & Muir-Cochrane, 2006). Beginning with a deductive approach, survey questions guided the development of an a priori coding manual, followed by an inductive approach to review the open-ended responses and identify additional categories for the coding manual. Open-ended responses were reviewed by two coders (first and second authors) for inter-rater reliability, with disputes resolved through discussion until a consensus was reached. To address the credibility and trustworthiness of the analysis, coders practised reflexivity where assumptions and personal biases were considered (Finlay, 2002). Reflexivity was achieved through active reflection on our positionality as researchers, including noting memos and on-going collaboration between the researchers/coders, while considering our personal demographics such as age, race/ethnicity, gender, socio-economic status and lived experience with AFCCA.
Results
Objective 1: Frequency and Severity Changes in AFCCA Types
When asked about AFCCA during the time prior to the pandemic, caregiver responses indicated the mean frequency of verbal AFCCA to be 5.2 (SD = 1.6; potential range from 2 to 10). When asked about any changes in verbal AFCCA frequency since the pandemic, 8.3% reported a decrease, 40.5% reported no changes, and a little over half (51.2%) reported an increase. In a rare case involving a decrease, one caregiver recounted how a decline in both verbal and physical aggression was observable after her daughter spent several months in an addiction centre due to excessive screen use at the start of the pandemic: ‘She is still addicted but hardly physically violent to me at all, due to intervention there . . . She still is verbally abusive but much less’ (Adoptive mother of 17-year-old daughter). Comparatively, caregivers described how more frequent pandemic routine disruptions and a lack of socialization resulted in some young people facing an increase in one form of AFCCA while experiencing a decline in another: Beginning with a move & being out of school & daycare . . . not seeing others, it got worse . . . [s]he became more verbal & the insults were more common than physical. Now she is back into more physical again (Adoptive mother of 7-year-old daughter).
For the item about any changes in verbal AFCCA severity related to the pandemic, few (9.8%) caregivers reported a decrease, and a fairly equal number reported either no changes (46.3%) or an increase in severity (43.9%). Among the few who reported a decrease, one caregiver attributed it to a lessening of education-related strains: ‘We realized that our daughter was under a lot of stress at school Pre-COVID. When school wasn’t in the picture, there was a period of calm’ (Adoptive mother of 16-year-old daughter). By contrast, other caregivers faced more intensely vocal children: ‘Often says horrible things now and that’s escalated dramatically’ (Adoptive mother of 17-year-old non-binary/third gender teen).
Recently his behaviours have escalated so much and he started to verbally abuse us and threaten harm to us that the police and child services were called and we have removed him from the home until we can receive mental health/other assistance for him and us (Customary grandmother of 13-year-old son).
Relatedly, caregivers also experienced threats alongside verbal and other forms of AFCCA. The mean frequency of threats of AFCCA reported by caregivers (when reflecting on the period before the pandemic) was 15.1 (SD = 4.9; potential range from 7 to 35). When asked about any changes in the frequency of AFCCA threats since the pandemic, 12.4% reported a decrease, 39.8% reported no changes, and most (47.8%) reported an increase. In response to the item on any pandemic-related changes in the severity of AFCCA threats, 18.6% of caregivers reported decreased severity, and there was a fairly equal number who reported either no change (41.6%) or increased severity (39.8%). In cases where the frequency and severity of threats increased, several caregivers recounted being at risk of very serious, even fatal, harms, while others focused on the extent to which their child communicated the warnings: ‘[She] threatens to kill us in our sleep (explicitly describes how in detail – knife, fire)’ (Adoptive mother of 15-year-old daughter).
The mean frequency of physical AFCCA reported by caregivers (when reflecting on the period before the pandemic) was 19.0 (SD = 4.9; potential range from 8 to 40). When asked about any frequency changes in physical AFCCA since the pandemic, few caregivers (15%) reported a decrease, 38.9% reported no changes, and most (48.3%) reported an increase. Caregivers who recounted an overall decrease referred to the benefits of pandemic-related isolation, togetherness and therapy, whereas age-related growth seemed to have varying implications across families: As our child has gotten older . . . these behaviours have decreased. Also, our child (she) has seen therapists over the past four years . . . and that has also helped. Being together all the time with little outside . . . demands on her time . . . also played a role in decreasing her . . . anxiety, [and] violent . . . behaviours (Adoptive mother of 12-year-old daughter).
Other caregivers also noted mixed experiences. Some increases were due to changes in educational formats and the close proximity of family members over extended times, while some decreases were attributed to pharmaceutical aid: ‘Behaviour increased and worse[ned] during pandemic, but . . . has now significantly improved with medication in the past 3 months’ (Adoptive mother of 8-year-old daughter).
Peaked during . . . shutdowns . . . We were unable to participate in any online learning as it immediately triggered violence. The initial lockdown, with no . . . online learning was actually a very peaceful time (Adoptive mother of 9-year-old son).
Although some caregivers experienced both increases and decreases in physical AFCCA frequency, others faced an ongoing escalation: Incidents happened on average about 1-2x a week prior to the pandemic so I was already fearful and vigilant. When we went on our first lockdown I put in place safety plans but within a few weeks the violence was every day and often more than once a day. Despite . . . respite supports the violence was too much and in March 2021 [our child] went into a temporary care agreement with CAS and into a group home . . . The violence was already increasing steadily before the pandemic, but lockdowns seemed to accelerate the trajectory (Adoptive non-binary parent of 12-year-old transgender pre-teen).
Other caregivers attributed an upsurge in physical forms of AFCCA to a gap in resource provision during the pandemic and clarified the steps used to mitigate potential risks: My [teen] has FASD. They’ve always been aggressive but it’s worse due to COVID and the lack of support for anyone here. We hide lots of dangerous things in our house because we don’t trust their ability to think clearly about outcomes and consequences (Adoptive mother of 17-year-old non-binary/third gender teen).
For any pandemic-related changes in physical AFCCA severity, 20.5% of caregivers reported decreased severity, 35.2% reported no changes, and most (44.3%) reported an increase in severity. When caregivers described the increases, the extent of the implications was made evident: ‘Increased physical aggression and tossing things around the house when frustrated with online schooling. I’m at the point now that I don’t push it because it’s too stressful for her and myself’ (Adoptive mother of 9-year-old daughter).
Intensity and severity ha[ve] increased drastically . . . since COVID started – tried to stab us multiple times – kick, hit, punch, attack, scratch, pull hair, drop me to the floor, throw things, smash things . . . tried to strangle me with her legs around my neck – police involvement 5 times in 6 months – two admissions into hospital – children’s psychiatric (Adoptive mother of 17-year-old non-binary/third gender teen).
Other families that experienced increases in physical AFCCA severity throughout the pandemic also had to deal with criminal justice and health care involvement, the latter of which sometimes applied to both AFCCA-affected young people and their seriously injured caregivers: His behaviour escalated tremendously . . . It broke him and us. Once activity stopped, it became . . . so aggressive we had to physically restrain him from harming us and himself. He ended up being hospitalized in the child mental health un[i]t for 8 da[y]s (Adoptive father of 11-year-old son). [H]e has assaulted me . . . by stabbing me with pencils, a butter knife and earlier this year broke my Tibia bone and crushed my knee so severe [sic] I needed a rod and screws. All because I asked him to take his pills (Adoptive mother of 4-year-old son). My daughter has choked me several times . . . If her older sister was not around to “help” me, I would be dead. She also choked me while I was driving. She tosses me around like a rag doll and pushes and punches me (Adoptive mother of [age omitted] daughter).
When asked about emotional/ psychological AFCCA during the time prior to the pandemic, caregivers’ mean reported frequency was 2.4 (SD = 1.4; potential range from 1 to 5). For any pandemic-related frequency changes in emotional/psychological AFCCA, few caregivers (8.4%) reported a decrease, 37% reported no changes, and more than half (54.6%) reported an increase. In cases of escalation, some parents recounted what they perceived to be fabricated allegations of harm: ‘She has called the police on me and her sister, claiming we have abducted children and have them in our home . . . [and that] her sister had pulled a knife on her. Both accusations are false . . .’ (Adoptive mother of [age omitted] daughter). For severity changes, 13.3% of caregivers reported a decrease, 37.5% reported no changes, and almost half (49.2%) reported an increase in severity. In instances of intensification, caregivers recalled how emotional manipulation sometimes permeated physical forms of AFCCA: ‘Way more aggressive, bigger and stronger. Trys [sic] to damage things that are important to us’ (Adoptive mother of 11-year-old son).
The mean frequency of sexual AFCCA reported by caregivers (when reflecting on the period before the pandemic) was 1.1 (SD = 0.4; potential range from 1–5). When asked about any frequency changes in sexual AFCCA since the pandemic, most caregivers (54.2%) reported no changes, 33.3% reported a decrease, and 12.5% reported an increase. For any severity changes, most caregivers (63.7%) reported no changes, while 36.4% reported decreased severity. In all, both the quantitative and qualitative responses indicated that there was relatively little pandemic-related variation in this form of AFCCA. Any changes that did occur showed decreases in an already rarely occurring form of AFCCA.
AFCCA Subtype Associations
In addition to examining the subtypes individually, we conducted correlations across AFCCA subtype frequency and severity changes during the pandemic. Table 1 shows that, apart from sexual AFCCA, the frequency changes were all positively correlated with one another – indicating that as one AFCCA type increased during the pandemic, the other types increased in frequency as well. Table 2 shows that severity changes were also positively correlated for all AFCCA types, indicating that as one AFCCA type increased, the other types also increased in severity during the pandemic.
Correlations Among AFCCA Subtype Frequency Changes During the Pandemic.
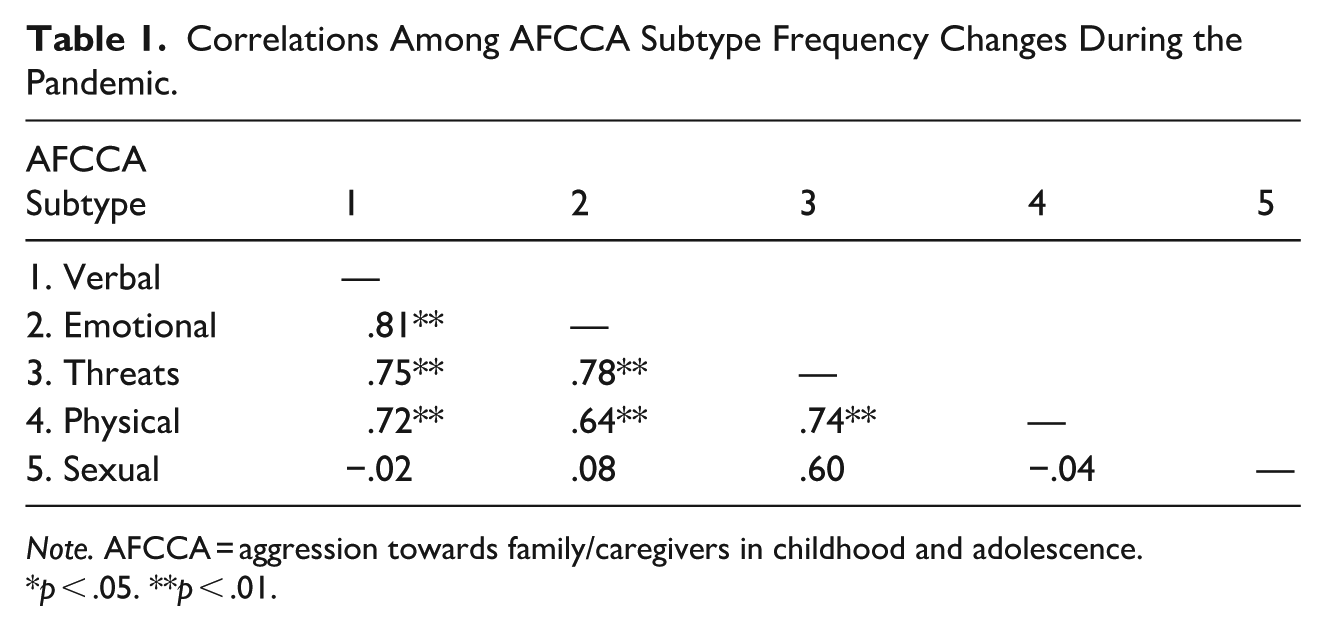
Note. AFCCA = aggression towards family/caregivers in childhood and adolescence.
p < .05. **p < .01.
Correlations Among AFCCA Subtype Severity Changes During the Pandemic.
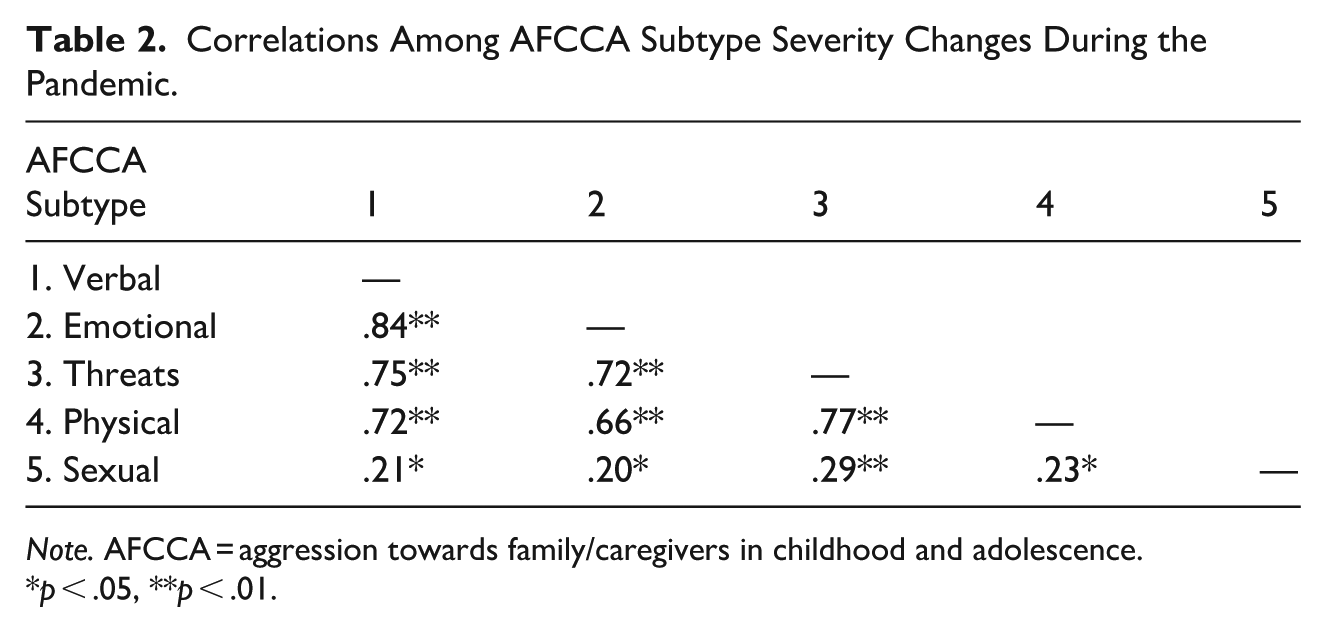
Note. AFCCA = aggression towards family/caregivers in childhood and adolescence.
p < .05, **p < .01.
Objective 2: Impacts on Caregiver-Child Relationships
Results from the paired samples t-test (N = 116) indicated a statistically significant difference from pre- (M = 2.9, SD = 1.2) to post-pandemic (M = 2.6, SD = 1.3; t[115] = 3.5, p = .001), suggesting that the quality of the caregiver-child relationship worsened after the pandemic. While some caregivers reported having a ‘better relationship’ with their AFCCA-exhibiting child ‘than [they] ever had’, and thus had a more ‘peaceful’ home, it was attributable to the fact that prior to the pandemic their child had moved to a resource home where ‘staff deal with the aggressive behaviour now’ (Adoptive mother of 17-year-old non-binary/third gender teen). In contrast, the extent of the eroded relationships came to light as caregivers elaborated on the reasons for changes in their interactions: ‘School was an opportunity for all of us to have a break from one another. Being around each other a lot has increased everyone’s frustration level and contributes to more arguments’ (Adoptive mother of 17-year-old daughter).
Some family situations were particularly acute and required both health care and criminal justice involvement, all of which exacerbated already-strained relationships and heightened parental fears and feelings of regret: My daughter has been hospitalized 4 times . . . in less than a year due to her violence towards me. I had to go to the Justice of the Peace . . . 3 of those times . . . after the super of her apartment called the police as she was beating me up . . . I’m so full of guilt, and want so much to help her, but she is . . . no longer talking to me. I had a missing persons report done . . . after 4 mo[n]ths the police located her but will not tell me where she is. I was worried she was being sex trafficked again. I cannot sleep and worry about her 24/7!! I fear the police will . . . tell me that she has died (Adoptive mother of [age] daughter).
Other caregivers described major tensions, as well as either near breakdowns or actual breakdowns in their families: ‘It is causing a split in the family. My older son cannot stand the behaviour towards me or his children’ (Kinship ‘mother’ of 15-year-old ‘daughter’). As we illustrate next, the deteriorating caregiver-child relationships led to other challenges for caregivers, including impacts on relations, routines and self-care.
Objective 3: Disruptions to Families’ Lives
For caregiver ratings of AFCCA’s impacts before and since the pandemic across nine identified areas, results from the paired-samples t-test (N = 117) indicated no statistically significant difference from pre- (M = 27.2, SD = 7.3) to post-pandemic (M = 27.5, SD = 8.8; t[116] = −0.28, p = .779). To further investigate this non-significant finding, frequency analyses and mean score visual comparisons were conducted on each item, and the following showed an increase in disruptions.
Missing Obligations
Mean score comparisons revealed that caregivers reported an increase in missing job-related obligations or missing other responsibilities due to AFCCA from pre- (M = 3.08, SD = 1.27) to post- (M = 3.31, SD = 1.36) pandemic. This finding was consistent with qualitative results that showed caregivers struggled to maintain employment due to obligations of caring for their child exhibiting AFCCA type behaviours.
We’ve attempted to get [o]ur child help for years . . . Endless waitlists have been the result of . . . endless effort on my part, losing my ability to work to hold a full-time job while needing to pick them up from school when they are aggressive or melting down or not able to be there (Adoptive mother of 17-year-old non-binary/third gender teen).
Caregivers also reported specifically on how mental health challenges due to their child’s AFCCA were compounded by pandemic complications that further affected their ability to work. ‘My depression and anxiety resurfaced during COVID with my child’s increase in verbal and physical aggression. [I] had to take 4 months off work for my challenging [m]ental health’ (Adoptive mother of 17-year-old daughter).
I have feared for my life and have . . . long term physical injuries as a result of COVID and losing our supports . . . aggression has significantly escalated. I have been . . . diagnosed with PTSD and I am not . . . able to work (Adoptive mother of 9-year-old son).
Interruption to Personal Time
Mean score comparisons revealed that caregivers reported a slight increase in interrupted personal time due to AFCCA from pre- (M = 3.77, SD = 1.08) to post- (M = 3.89, SD = 1.14) pandemic. Qualitative comments supported this finding as caregivers revealed that their mental health and obligations to other children in the home were negatively impacted by the time-consuming nature of AFCCA.
Our daughter cannot entertain herself at all and needs to be entertained since COVID. She takes up so much of our time with her meltdowns that I often feel we are failing our son as he doesn’t get as much time (Adoptive mother of 7-year-old daughter). It has had a huge impact on my level of energy or want to do anything. Once they are in bed all I want to do or have the strength to do is go to bed myself as I never know what to expect or when (Adoptive mother of 8-year-old daughter).
Alcohol/Substance Use and Insufficient Self-Care
Mean score comparisons revealed that caregivers reported a slight increase in alcohol or substance use due to AFCCA from pre- (M = 1.61, SD = 0.96) to post- (M = 1.69, SD = 1.12) pandemic and in poor self-care from pre- (M = 3.39, SD = 0.1.33) to post- (M = 3.44, SD = 1.41) pandemic. Caregivers elaborated on their increased dependency on food, prescriptions, and/or alcohol to cope with ongoing challenges. ‘I am on far more medication prescribed by my Dr. than ever before. I have also gained weight due to excessive eating, stress and anxiety’ (Adoptive mother of 9-year-old son).
. . . my daughter’s meltdown . . . and behaviours impact us all so much. I have never been a big drinker . . . now . . . I may have a drink at home with dinner after a very long day with my daughter. This is out of the norm for me (Adoptive mother of 7-year-old daughter).
Discussion
This study contributed Canadian data to a growing understanding of AFCCA during the COVID-19 pandemic, a challenging period marked by exacerbated mental health issues for children and youth (Calvete et al., 2023; Cano-Lozano et al., 2021b; Miles et al., 2024; Sobalvarro et al., 2023). This study also aimed to further support the urgent need for developing effective child-centred, adversity-sensitive interventions that are grounded in intersectionality and can better assist AFCCA-affected families while advocating for their safety and well-being (Kehoe, et al., 2020; Rutter et al., 2023). Mostly aligned with our objective 1 hypothesis, results showed that, except for sexual forms of AFCCA, the majority of caregivers reported that all AFCCA types increased in frequency during the pandemic. For severity, the majority of caregivers reported an increase in emotional/psychological and physical AFCCA. For severity of threats and verbal AFCCA, there was a fairly even distribution between caregivers reporting no changes or reporting an increase. Additionally, we found that as one AFCCA subtype (with the exception of sexual) increased in frequency, the other subtypes tended to increase as well. Similarly, as one AFCCA subtype increased in severity, the others also tended to increase. This suggests that AFCCA subtype changes tend to not happen in isolation but rather simultaneously. These findings are consistent with recent research showing increased occurrences of AFCCA within families during the COVID-19 lockdown (Calvete et al., 2023; Cano-Lozano et al., 2021b; Miles et al., 2024).
Also aligned with our hypothesis for objective 2, results showed a statistically significant worsening of the caregiver-child relationship during the pandemic due to AFCCA behaviours. This was highlighted by caregivers discussing exacerbated strained relationships and heightened fears of their children due to increased AFCCA behaviours related to the pandemic restrictions that were put into place. These findings contribute to understanding the effects of AFCCA on the caregiver-child relationship, an area within family violence which remains under-researched (Calvete et al., 2023; O’Toole et al., 2022). In contrast to our objective 3 hypothesis, results showed no overall significant AFCCA-related disruption to families’ lives during the pandemic, based on quantitative findings. A benefit to applying a mixed methods approach is that it supplements findings and questions certain results that may appear inaccurate. We expected a significant disruption to family lives during the pandemic due to AFCCA. This expectation was reinforced after coding caregiver responses to the open-ended questions, leading us to examine each item in the measure for more detailed information. Mean score comparisons and qualitative findings revealed that caregivers reported increases in missed work obligations, interruptions to personal time, increased alcohol/substance use and poor self-care due to AFCCA during the pandemic. The questionnaire items that did not appear to worsen included family routines, financial strain, attention to other relatives and relationships within the family and community. Given the complexity of the pandemic and the various family impacts, it does seem sensible that there would not be disruptions at all levels. Although the pandemic did pose serious challenges, in some cases, as was found in other studies (Christie et al., 2022), it also allowed people to spend more time at home and maintain relationships, as well as keep up with household routines. This mixed-methods analysis enabled us to not only identify which aspects of families’ lives were impacted by the pandemic, and which remained unchanged, but also shed light on how such complex consequences were variously experienced.
Applied Implications
Caregivers’ insights revealed several applied implications, some echoing prior research and others offering novel contributions. First, at the broader system level, given how some caregivers recognized the crucial benefits of the structure and outlet provided by in-person supports (e.g. respite and school-based hubs for special needs students) during lockdowns, all social services should implement similarly consistent and ability-informed emergency preparedness measures for AFCCA-affected families. Relatedly, due to the variability of adversity among AFCCA-affected families during the COVID-19 pandemic and based on caregivers’ descriptions of support gaps during lockdowns, service provision must be more reliably funded, and more concertedly prioritized across healthcare, education, social work, justice and community sectors (Cano-Lozano et al., 2021b; Condry et al., 2020; Kehoe et al., 2020; Lyttle et al., 2021; Miles et al., 2024; Rutter et al., 2023; Selwyn & Meakings, 2016) to ensure that both proactive and reactive approaches are more inclusive, comprehensive, and effective especially in times of crisis when they are needed most.
Second, at the family level, it is essential to address caregivers’ mental, emotional, and physical well-being on both short- and long-term bases (Condry et al., 2020; Miles et al., 2024). Such parental support is not only important for their own sake, but also for the sake of all their AFCCA-affected children, including both exhibitors and siblings (Desimpelaere et al., 2023; Selwyn, 2019). If caregivers are to properly uphold multiple children’s health and safety simultaneously, especially when facing conflicting challenges during unexpected and widespread societal-level crises, they must be well and safe enough to do so. Thus, to ensure a more consistent whole family approach, both in person and online supports must be more readily available on an ongoing basis and particularly as part of contingency plans (Rutter et al., 2023).
Third, at the individual level, it is necessary to undertake child-centred and diversity-aware approaches for both AFCCA-exhibiting children and their siblings. Support should be forward-looking and committed to upholding the best interest of all children with varying identities and abilities (DeCarlo-Slobodnik & Gervais, 2022; Gervais et al., 2022), while simultaneously considering the long-term wide-ranging implications of the pandemic. Given the higher representation in our sample of children in child protection and adoptive families (indicating a likely history of trauma) who are from diverse racial/ethnic backgrounds (e.g. Indigenous and Black), identify as LGBTQ2S+, and/or have complex neurodevelopmental profiles, it is essential that support be culturally appropriate and queer-informed. These services must also be rooted in an intersectional approach that acknowledges and seeks to overcome the systemic inequalities, cross-cultural adjustments, neurodivergent-based vulnerability and ongoing intergenerational trauma that may be affecting children’s well-being and impacting the presence of AFCCA within families (Miles et al., 2024; National Consortium on AFCCA, 2021).
Fourth, despite the adverse conditions they faced during the COVID-19 pandemic, many caregivers still modelled courage and determination in considering their children’s complex needs, varying abilities and diverse identities while ensuring their well-being in various ways. Thus, service providers should not only listen attentively to parents to more accurately address their challenges (Desimpelaere et al., 2023) but also facilitate constructive spaces to amplify parents’ child rights and ability-informed perspectives on advocacy-oriented best practices that may benefit other families especially when societal-level crises are more acute.
Limitations and Future Directions
First, our study was limited by a small, non-representative sample, primarily made up of adoptive mothers in Ontario, due in part to an established link with a community partner working with this population. We acknowledge that these familial, geographic and gender biases limit the generalizability of our findings to broader caregiver populations. Future studies should broaden recruitment strategies to include more geographically, culturally and gender diverse samples of AFCCA-affected families across Canada (O’Toole et al., 2022), and to examine other impacts, such as filial trauma (Tremblay & Pagé, 2024). Furthermore, the higher representation of mother-participants may also reflect gender differences in child-to-parent aggression as mothers are often the primary victims of certain types of AFCCA (O’Toole et al., 2022). Given the serious implications of gender-based harm, further research aimed at analyzing gender as a meaningful variable is warranted; in particular, studies on how gender may influence the directionality, exposure to, expression of, and coping with AFCCA in Canadian families are needed (Ilabaca Baeza & Gaete Fiscella, 2021; Miles et al., 2024). Second, while we accounted for potential changes between pre- and post-pandemic periods, our study was not longitudinal, similar to other research (Miles et al., 2024). Subsequent studies should go beyond our periodical measures based on self-report data and use recently revised questionnaires to examine the evolving nature of parent-child aggression through different developmental stages (Calvete et al., 2023) over the long-term effects of the pandemic (Cano-Lozano et al., 2021b). Third, we acknowledge that standardized measures were not used in this study; however, we adapted a UK survey from a previous project involving adoptive families, which had incorporated standardized measures. This approach allowed for meaningful comparisons between the project’s findings and our own, as seen in our discussion section. Further, under the advisement of an advisory committee, the survey items were adapted to reflect the Canadian context, pandemic-related experiences and ensure inclusive representation.
Fourth, we acknowledge the potential variability in caregiver experiences during the pandemic due to unique family circumstances, the wide range of young people in our sample (0–20 years), and fluctuations in pandemic-related regulations across the country. As caregivers were asked to consider contexts ‘since the start of the pandemic’, variations in perceived family stress likely occurred depending on when they completed the survey. Relatedly, we also note that the causalities associated with disruptions were subjective interpretations provided by the respondents and may not all be attributable to pandemic and AFCCA-specific relationship challenges. Thus, future studies should include interviews with caregivers, children, and other relatives so that such nuances can be explored more comprehensively. Fifth, for a more comprehensive understanding of pandemic-related AFCCA occurrence and impacts, it would have been desirable to include input from young people (Calvete et al., 2023) and other relatives (e.g. siblings, grandparents). To this end, we undertook a subsequent study with Canadian young people – both exhibitors and their siblings, as first voice experts (DeCarlo-Slobodnik & Gervais, 2022). We encourage other researchers to also include a range of relatives in their data collection to ensure that all AFCCA-affected family members’ rights to be heard are respected so that their needs for services are better understood and fulfilled.
Footnotes
Acknowledgements
We thank the caregivers who participated courageously in this study, as well as the community partners who facilitated recruitment and engaged in beneficial consultations. We recognize Dr. Julie Selwyn’s generous input on data collection instruments and Danika DeCarlo-Slobodnik’s valuable research assistance. We are grateful to the Interdisciplinary Research Laboratory on the Rights of the Child at the University of Ottawa for their infrastructural support of this study.
Ethical Considerations
Approval was granted by the University of Ottawa’s Office of Research Ethics and Integrity.
Consent to Participate
Written informed consent was obtained from all of the study’s individual participants.
Consent for Publication
Written informed consent was obtained for the publication of their data with non-identifying demographic information.
Author Contributions
All authors contributed to the study conception and design. Materials preparation and data collection were performed by Christine Gervais, Elisa Romano, and Danika DeCarlo-Slobodnik (research assistant; latter not authored). Analyses were performed by Sarah Zak, Christine Gervais and Elisa Romano. All listed authors contributed to the manuscript writing, and they approved its final revised version.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: Financial support for research assistantships for this study was provided by the Ottawa Community Foundation and the Interdisciplinary Research Laboratory on the Rights of the Child in the Faculty of Law at the University of Ottawa.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
Statistics and quotes from survey responses have been provided to illustrate key themes and results, but full responses will not be made publicly available. Yet, the survey questions may be available upon request.