
Abstract
Intimate partner violence (IPV) remains a significant global issue, mostly affecting women. South Africa has among the highest rates of IPV and IPV-related fatalities globally. This study examines the factors influencing IPV among ever-partnered women, aged 18 to 49 years, in South Africa. This study analyzed secondary data from the 2016 South Africa Demographic and Health Survey, using a weighted sample of 4,169 women, aged 18 to 49 years. The study focused on the experience of IPV in the 12 months preceding the survey. Univariate, bivariate analysis (χ2 test), and binary logistic regression analyses were used to explore the relationships between the selected factors and IPV. About 15.0% of women reported experiencing IPV. The findings showed that women aged 18 to 19 years (AOR: 2.23), 25 to 29 years (AOR: 2.10), those with primary (AOR: 1.84) and secondary education (AOR: 1.71), those who witnessed parental violence (AOR: 1.96), accepted wife-beating (AOR: 2.83), and whose partner drank alcohol (AOR: 2.67) had significantly higher odds of experiencing IPV. Conversely, employed women (AOR: 0.74), and women from middle-wealth (AOR: 0.64) and rich households (AOR: 0.58) had lower odds of experiencing IPV. Furthermore, the odds of women experiencing IPV were more than three times higher in the Western Cape (AOR: 3.32), Eastern Cape (AOR: 3.02), and North West (AOR: 3.33) than in the other provinces. The study highlights critical socio-demographic and behavioral factors influencing IPV among women in South Africa. Addressing these factors through targeted interventions and challenging societal norms on violence is important in preventing IPV.
Keywords
Introduction
Intimate partner violence (IPV) is a global social problem and affects both men and women. The prevalence of IPV is often disproportionately higher among women than men (Aye et al., 2020; Fanslow et al., 2022). Although IPV is a significant concern worldwide, its prevalence varies across countries and regions. For instance, global estimates show that lifetime IPV was highest in South-East Asia (37.7), Eastern Mediterranean (37.0%), and Africa (36.6%), while it was lowest in high-income regions (23.2%), such as Australia, the United States, Germany, Japan, and the United Kingdom (World Health Organization, 2013). Another study found regional differences in non-partner sexual violence, where Sub-Saharan Africa had the highest prevalence of non-partner sexual violence (Abrahams et al., 2014). Although developing nations, particularly the sub-Saharan African region, have a higher incidence of IPV, there is variation between countries. These regional differences in the prevalence of IPV highlight the importance of understanding the context-specific influence of socio-cultural, economic, as well as legal factors in dealing with IPV in different regions.
In sub-Saharan Africa, at least one in three women is abused by their intimate partner (Devries et al., 2013; Shamu et al., 2011). The central sub-Saharan Africa region accounts for the highest prevalence of IPV (65.6%), while the southern sub-Saharan Africa region accounts for a 29.7% prevalence of IPV (World Health Organization, 2013). In some conflict-affected settings, like the Central African region, factors such as persistent conflict and political instability tend to contribute to higher rates of IPV (Cardoso et al., 2016). Variations in the prevalence of IPV also exist between countries of these sub-regions. The varying levels of IPV in sub-Saharan Africa (Ahinkorah, 2021; Izugbara et al., 2020), show the differences in the contexts in which IPV is experienced by women in different societies.
IPV often limits women from having their autonomy (decision-making power) over sexual and reproductive health. Being in abusive relationships can increase the risk of HIV infection, as power imbalances may prevent women from negotiating condom use, refusing unwanted sex, or accessing HIV-related services (McCloskey et al., 2020; Rigby & Johnson, 2017; Shi et al., 2013; Sullivan, 2019). IPV significantly increases women’s vulnerability to HIV infection, thus reinforcing a cycle where violence and disease are interconnected. IPV-related deaths continue to be an issue in South Africa. In 2023, South Africa recorded some of the highest IPV-related death rates globally (United Nations, 2024). A study by Abrahams et al. (2024) revealed that South Africa has among the highest rates of intimate partner femicide. Intimate partner femicide refers to the killing of a woman by a current or former intimate partner (e.g., boyfriend or husband; World Health Organization & Pan American Health Organization, 2012). In South Africa, about 4.9 per 100,000 female population were murdered by their intimate partners in 2017, which is higher than the reported world average (Reis & Meyer, 2024; United Nations Office on Drugs and Crime, 2023). The critical need for strong legislative and policy measures to address IPV and protect women is highlighted by this extreme form of violence.
To eradicate IPV and consequent femicide, South Africa has put in place several legal initiatives. An important piece of legislation aimed at providing comprehensive protection for victims of domestic violence, including physical, sexual, emotional, and financial abuse, is the Domestic Violence Act of 1998 (Government of South Africa, 1998). The Domestic Violence Act offers broad protection for IPV victims and details the procedures for obtaining protection orders and support services; it also expands the definition of domestic relationships to include dating, engaged, and cohabiting partners, and extends legal protection beyond marriage (Government of South Africa, 1998). In addition, a multi-sectoral strategy to address gender-based violence in the nation is outlined in the National Strategic Plan on Gender-Based Violence and Femicide 2020 to 2030 (Department of Women, Youth and Persons with Disabilities, 2020). This approach emphasizes victim protection, prevention, and support in addition to holding perpetrators accountable (Department of Women, Youth and Persons with Disabilities, 2020). Moreover, in 2013, the National Council Against Gender-Based Violence was implemented by the Inter-Ministerial Committee to reduce IPV and factors contributing to it (South Africa & UN Human Rights Council Secretariat, 2017). Furthermore, the Sustainable Development Goals (SDGs) also respond to issues of gender equality as well as the increasing prevalence of IPV and femicide in many contexts. SDG 5 aims to eliminate all forms of violence against all women and girls in public and private spheres, and particularly addresses gender-based violence-related issues, including intimate partner femicide (United Nations, 2015). As part of the 2030 vision, the National Development Plan of South Africa also acknowledges the urgent need to eliminate gender-based violence.
Despite extensive studies conducted on IPV, there is still a gap in understanding the variables impacting IPV in South Africa’s various demographics. The individual situations and varied experiences of women from various socioeconomic, cultural, and geographical origins have not been considered in the overall findings of previous studies. To close this gap, this study will look at the variables related to IPV experiences among South African women who have ever been in a relationship while considering the nation’s diversity in terms of socioeconomic status, cultural background, and geographic location. Understanding IPV dynamics is further complicated by the intersectionality of variables, including age, education, and work position. This study can help shape policies and initiatives that better address the needs of South African women by highlighting the distinctive experiences of various groups. Therefore, this study aims to examine the factors influencing ever-partnered women’s experience of IPV in South Africa.
Methods
Data Source
This study used cross-sectional data sourced from the 2016 South Africa Demographic and Health Survey (SADHS), a nationally representative study managed by the Demographic and Health Survey Program. The 2016 SADHS dataset was chosen because of the inclusion of relevant socio-economic and demographic variables of interest in the current study. Households were selected from the 2011 Census frame using a two-stage sampling process (National Department of Health et al., 2019). In the first stage, enumeration areas were randomly selected; in the second stage, households within each area were randomly selected to achieve national representativeness (National Department of Health et al., 2019). This cross-sectional study focuses on women who experienced IPV in the 12 months before the survey, with a sample size of 4,169 ever-partnered women aged 18 to 49 years. For this study, we defined ever-partnered women as those who were aged 18 to 49 years old and: (a) had a regular boyfriend/partner/fiancée, (b) were currently married or living together (cohabiting), (c) were ever married or in union, and (d) has had a boyfriend (currently and/or in the past). This definition aligns with the one used in the SADHS report and by Puoeng and Tsawe (National Department of Health et al., 2019; Puoeng & Tsawe, 2024). Women aged 17 years or younger were excluded from the study because the SADHS only collected data from women aged 18 to 49 years in the domestic violence module (National Department of Health et al., 2019). The sample selection process is shown in Figure 1.
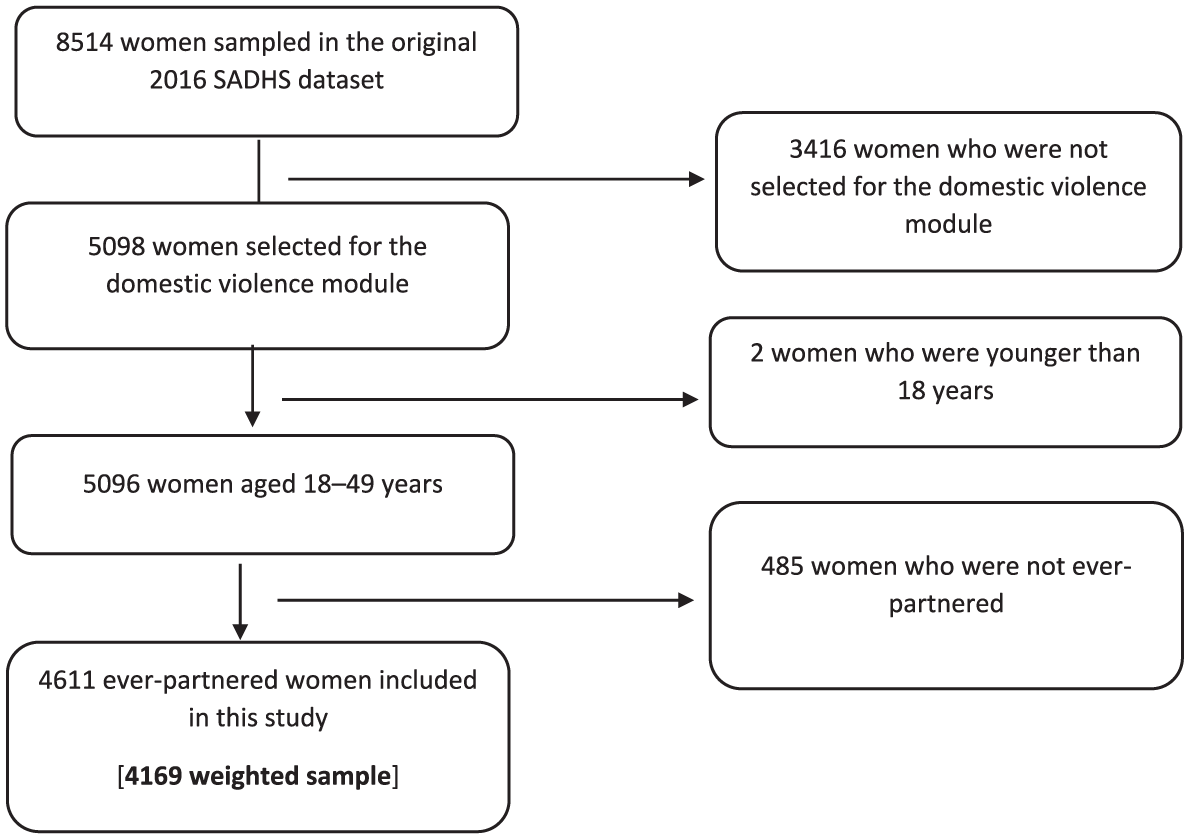
Schematic presentation of the selection of the sample for the study of the prevalence of intimate partner violence experienced by women aged 18 to 49 years old in South Africa.
Description of Variables
Outcome Variable
In this study, the outcome variable is IPV. The outcome variable is a combination of emotional or physical or emotional or sexual violence. Emotional violence includes questions on whether a woman has (a) ever been humiliated by her husband/partner, (b) ever been threatened with harm by her husband/partner, (c) ever been insulted or made to feel bad by her husband/partner, and (d) been humiliated, threatened to hurt, insulted or made feel bad by a previous husband. Physical violence questions focused on whether a woman has (a) ever been pushed, shook or had something thrown by her husband/partner, (b) ever been kicked or dragged by her husband/partner, (c) ever been strangled or burned by husband/partner, (d) ever been threatened with knife/gun or other weapon by husband/partner, and (e) ever been hit, slapped, kicked or physically hurt by previous husband. Sexual violence questions focused on whether a woman has (a) ever been physically forced into unwanted sex by her husband/partner, (b) ever been forced into other unwanted sexual acts by her husband/partner, (c) ever been physically forced to perform sexual acts respondent didn’t want to, (d) been physically forced to have sex or to perform sexual acts by a previous husband, (e) been ever forced to have sex by anyone other than husband/partner in last 12 months, (f) been ever forced to perform unwanted sexual acts, and (g) experienced any sexual violence by husband/partner.
The outcome variable is coded as 0 = No (did not experience IPV in the past 12 months preceding the survey) and 1 = Yes (experienced IPV in the past 12 months preceding the survey). The sample was not restricted to those currently in a relationship, as IPV can occur post-separation and still fall within the reference period. The definition of IPV used in this study follows the DHS methodology, which includes both partner and non-partner sexual violence; this is done to ensure consistency with official DHS reports.
Explanatory Variables
Ten explanatory variables were included in this study. The selected explanatory variables are briefly described in Table 1. Previous studies have highlighted the importance of these factors in explaining IPV (Chernet & Cherie, 2020; Izugbara et al., 2020; Phiri et al., 2023; Puoeng & Tsawe, 2024).
Description of Explanatory Variables.
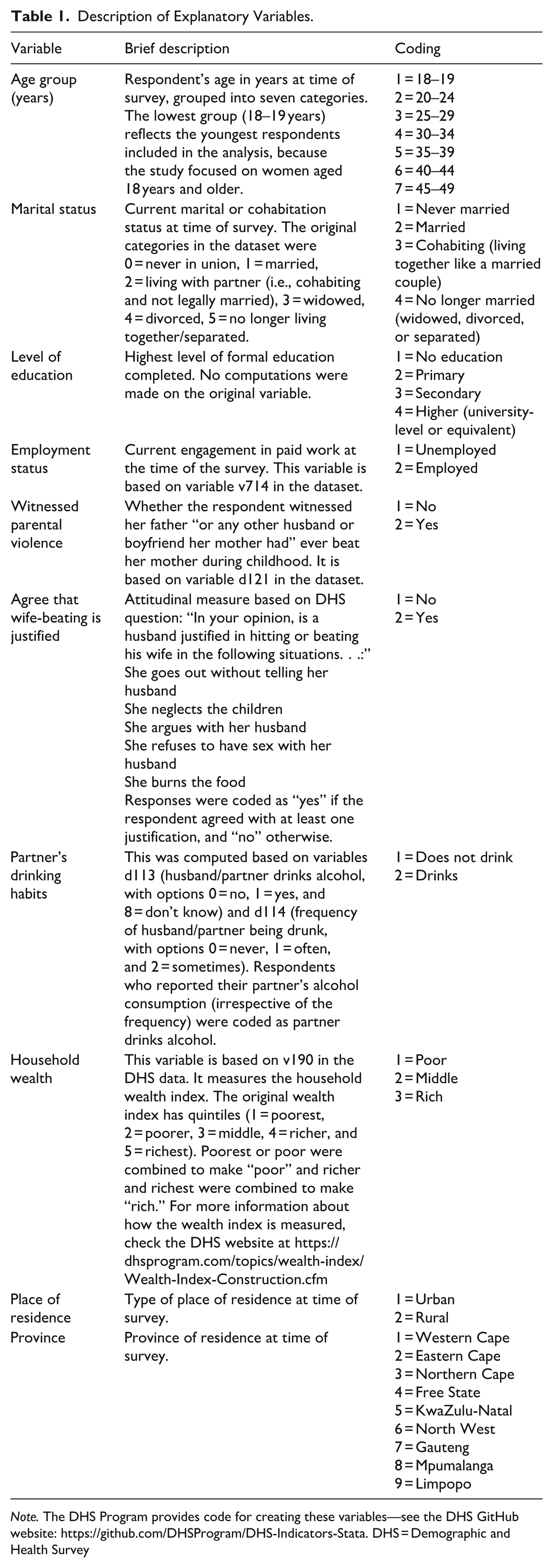
Note. The DHS Program provides code for creating these variables—see the DHS GitHub website: https://github.com/DHSProgram/DHS-Indicators-Stata. DHS = Demographic and Health Survey
Statistical Analysis
The analysis was performed using Stata version 16 (StataCorp, 2019). All analyses accounted for the complex survey design of the data using the svyset command in Stata, which incorporated sampling weights, clustering, and stratification. The study used descriptive and inferential statistics to analyze the data. The first part involved the use of descriptive statistics to describe the study sample. The second part involved the use of bivariate analysis, with a Pearson’s chi-square test (χ2) of independence to assess associations between explanatory variables and IPV. The third part involved the use of binary logistic regression analysis to measure the relationship between socio-demographic factors and IPV, while controlling for potential confounding variables. Model fit was assessed using the Pearson goodness of fit test, which indicated an adequate fit (F[9, 670] = 1.28, p = .2455), suggesting that the logistic regression model appropriately captured the observed data patterns. To visualize provincial differences in IPV prevalence, a choropleth map was generated using the ggplot2 package in R (R Core Team, 2023; Wickham, 2016a, 2016b). This map shows the spatial distribution of IPV across South Africa’s provinces. In this study, the statistical tests were conducted at the 0.05 level of significance (p ≤ .05).
Results
Socio-Demographic Characteristics
A sample of 4,169 ever-partnered women aged 18 to 49 years was included in this study. The findings, in Table 2 showed that most women (a) were aged 25 to 29 years (19.9%), (b) were never married (49.6%), (c) had secondary education (75.5%), (d) were unemployed (60.4%), (e) did not experience their father beat their mother (85.5%), (f) did not agree that wife-beating is justified (97.7%), (g) did not have a partner who drank alcohol (56.6%), (h) were from poor households (39.9%) and rich households (38.9%), (i) were from urban areas (67.9%), and (j) were from Gauteng province (28.3%).
Distribution of Respondents, Prevalence, and Factors Associated with Intimate Partner Violence Experienced by Women aged 18 to 49 Years Old in South Africa.
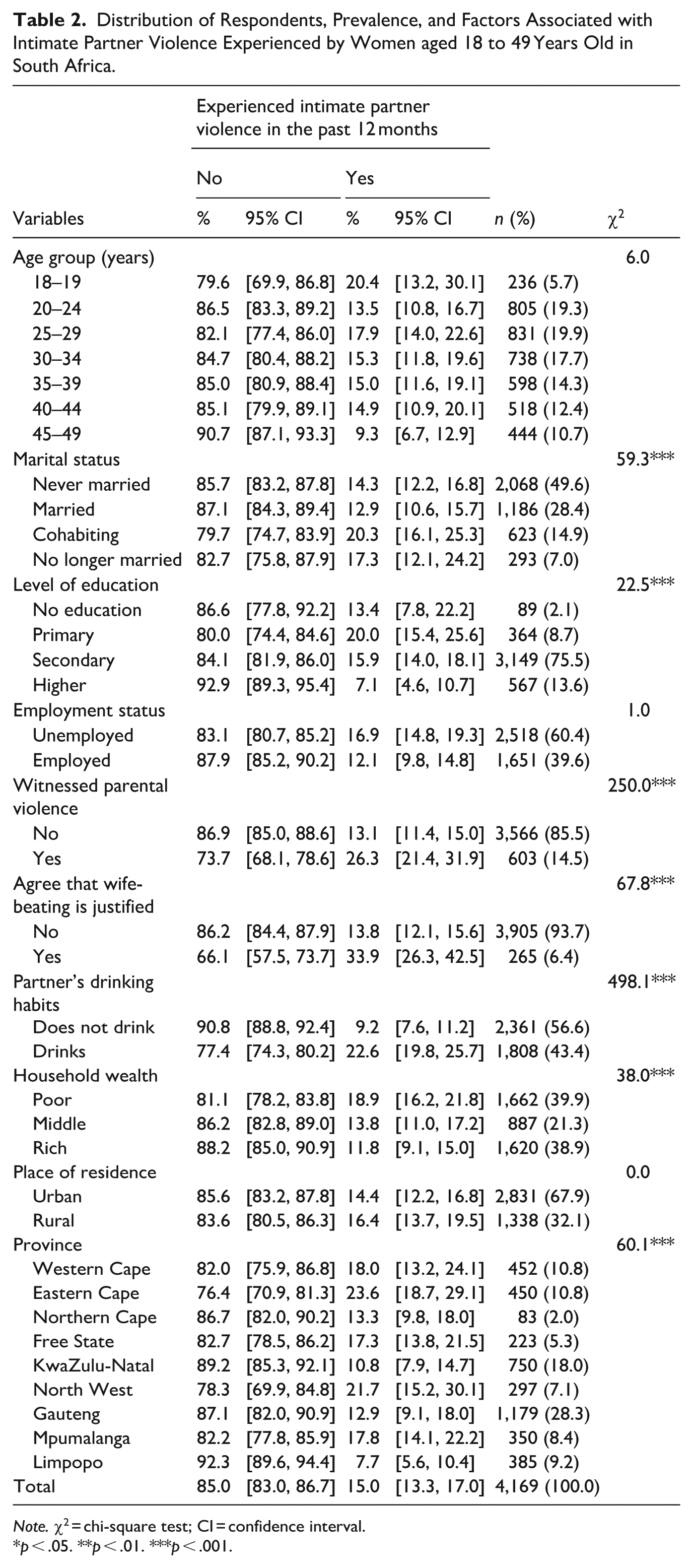
Note. χ2 = chi-square test; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Prevalence of IPV
Table 2 presents the prevalence of IPV, with a χ2 test, among ever-partnered women by background characteristics. The findings showed that marital status, level of education, witnessed parental violence (respondent’s father ever beat her mother), agreement that wife-beating is justified, partner’s drinking habits, household wealth, and province were statistically associated with experiencing IPV in the 12 months preceding the survey. Overall, 15% [95% CI 13.3, 17.0] of women reported that they had experienced IPV in the 12 months preceding the survey. Moreover, the findings showed that women aged 18 to 19 years had a higher prevalence (20.4% [13.2, 30.1]) of IPV, while it was lower (9.3% [6.4, 12.9]) among women aged 45 to 49 years. Cohabiting women had a higher prevalence (20.3% [16.1, 25.3]) of IPV, while it was lower (12.9% [10.6, 15.7]) among those who were married. In terms of level of education, women with primary education had a higher prevalence (20.0% [15.4, 25.6]) of IPV, while it was lower (7.1% [4.6, 10.7]) among those with higher education (i.e., university-level or equivalent). Moreover, unemployed women had a higher prevalence (16.9% [14.8, 19.3]) of IPV, while it was lower (12.1% [9.8, 14.8]) among employed women.
Furthermore, the findings showed that women who witnessed violence at home (father beat her mother) had a higher prevalence (26.3%, 95% CI [21.4, 31.9]) of IPV, while it was lower (13.1% [11.4, 15.0]) among those who did not witness parental violence. Likewise, women who agreed that wife-beating is justified had a higher prevalence (33.9% [26.3, 42.5]) of IPV, while it was lower (13.8% [12.1, 15.6]) among those who did not agree with the justification of wife-beating. Moreover, women with a partner who drinks alcohol had a higher prevalence (22.6% [19.8, 25.7]) of IPV, while it was lower (9.2% [7.6, 11.2]) among those whose partner did not drink alcohol. The findings also showed that IPV decreases with household wealth status. Women from poor households had a higher prevalence (18.9% [16.2, 21.8]) of IPV, while it was lower (11.8% [9.1, 15.0]) among those from rich households. In terms of geographical location, women from rural areas had a higher prevalence (16.4% [13.7, 19.5]) of IPV, while it was lower (14.4% [12.2, 16.8]) among those from urban areas. Moreover, women from the Eastern Cape province (23.6% [18.7, 29.1]) and North West (21.7% [15.2, 30]) had a higher prevalence of IPV, while it was lower (7.7% [5.6, 10.4]) among those from Limpopo. The visual presentation of the prevalence of IPV in the provinces of South Africa is illustrated in Figure 2.
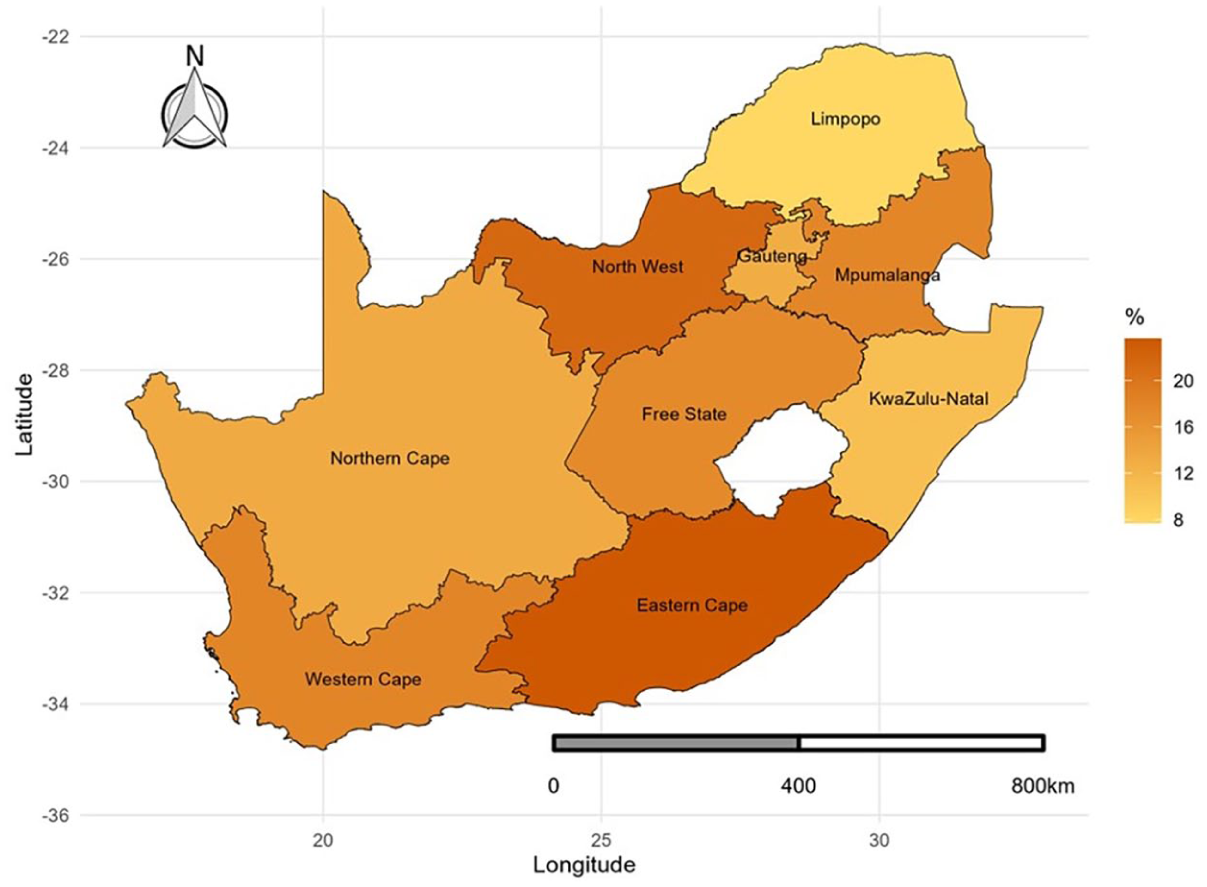
Prevalence of intimate partner violence by province in South Africa.
Factors Associated with IPV
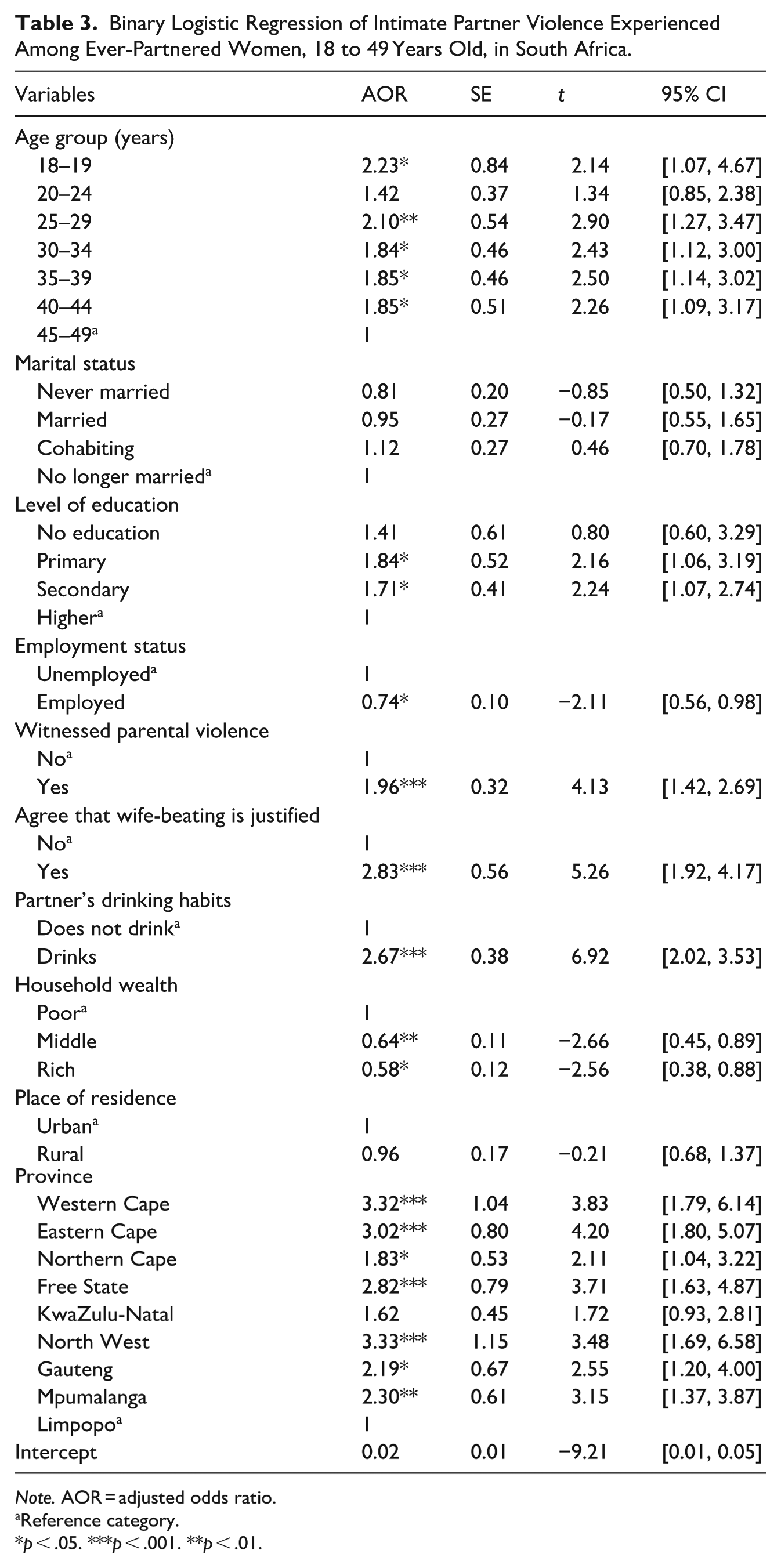
Table 3 presents the multivariate logistic regression results for the relationship between background characteristics and IPV. The logistic regression model allowed for the estimation of independent effects while controlling for other covariates. The findings showed that women aged 18 to 19 years and those aged 25 to 29 years had higher odds of IPV, with more than twofold odds of experiencing IPV in the 12 months preceding the survey. Women aged 18 to 19 years (AOR: 2.23, 95% CI [1.07, 4.67]) as well as those aged 25 to 29 years (AOR: 2.10 [1.27, 3.47]) had higher odds of IPV compared to women aged 45 to 49 years. Similarly, women aged 30 to 34 years (AOR: 1.84 [1.12, 3.00]), those aged 35 to 39 years (AOR: 1.85 [1.14, 3.02]), and those aged 40 to 44 years (AOR: 1.85 [1.09, 3.17]) had almost two times the odds of experiencing IPV compared to those aged 45 to 49 years. Moreover, women with primary education had higher odds (AOR: 1.84 [1.06, 3.19]) of IPV compared to those with higher education. Likewise, women with secondary education had higher odds (AOR: 1.71 [1.07, 2.74]) of IPV compared to those with higher education. In terms of employment status, women who were employed had lower odds (AOR: 0.74 [0.56, 0.98]) of IPV compared to those who were unemployed.
Binary Logistic Regression of Intimate Partner Violence Experienced Among Ever-Partnered Women, 18 to 49 Years Old, in South Africa.
Note. AOR = adjusted odds ratio.
Reference category.
p < .05. ***p < .001. **p < .01.
The findings further showed that witnessing parental violence plays a significant role in women’s experience of IPV. Women who witnessed parental violence had higher odds (AOR: 1.96, 95% CI [1.42, 2.69]) of IPV compared to those who did not witness parental violence. Women who agreed that wife-beating is justified had higher odds (AOR: 2.83 [1.92, 4.17]) of IPV compared to women who did not agree with wife-beating. Moreover, the findings showed that the partner’s alcohol consumption is a significant factor in women’s experience of IPV. Women whose partners drank alcohol had higher odds (AOR: 2.67 [2.02, 3.53]) of IPV compared to those whose partners did not drink alcohol. The findings further showed that IPV decreased with household wealth. Women from rich households had lower odds (AOR: 0.58 [0.38, 0.88]) of IPV compared to women from poor households. Likewise, women from middle-wealth households had lower odds (AOR: 0.64 [0.45, 0.89]) of IPV compared to women from poor households. Furthermore, the findings showed that women’s provincial location plays a key role in experiencing IPV. Women from the Western Cape province (AOR: 3.32 [1.79, 6.14]), the Eastern Cape province (AOR: 3.02 [1.80, 5.07]), and the North West province (AOR: 3.33 [1.69, 6.58]) had three times the odds of experiencing IPV compared to women from Limpopo. The odds of women’s experience of IPV were also higher among those from the Northern Cape province (AOR: 1.83 [1.04, 3.22]), the Free State province (AOR: 2.82 [1.63, 4.87]), the Gauteng province (AOR: 2.19 [1.20, 4.00]), and Mpumalanga province (AOR: 2.30 [1.37, 3.87]) compared to those from Limpopo.
Discussions
This study examined the factors associated with IPV among ever-partnered women during the 12 months preceding the survey in South Africa. In this study, just over one in seven women had experienced IPV in the past year preceding the survey. Our findings revealed significant associations between IPV and various socio-demographic and behavioral factors, such as marital status, education level, witnessing parental violence, acceptance of wife-beating, partner’s drinking habits, household wealth, and province of residence. Previous studies focusing on past-year IPV (Namer et al., 2024; Phiri et al., 2023; Shamu et al., 2018; Tsegaw et al., 2022) and those focusing on lifetime IPV (Kebede et al., 2022; Puoeng & Tsawe, 2024; Tiruye et al., 2020) have also found an association between these factors and IPV. Our findings also revealed a complex relationship between age and IPV. Women aged 18 to 19 and 25 to 29 experienced higher odds of IPV compared to women aged 45 to 49. A study conducted in Liberia found similar results where older women had lower odds of IPV compared to younger women (Tsegaw et al., 2022). Another study focusing on global and regional estimates of IPV found that the prevalence of IPV within the past year was high among women aged 15 to 19 and 20 to 24, with rates of 16% in both age groups (Sardinha et al., 2022). Younger women tend to be more vulnerable to IPV due to their limited experience in intimate relationships as well as power imbalances within those relationships, which results in limited decision-making autonomy in these relationships (Gunarathne et al., 2023). Economic dependence on abusive partners tends to exacerbate this risk, because financial dependence can make it difficult to leave abusive relationships (Rafiq et al., 2023; Zungu et al., 2010).
Although marital status was significantly associated with IPV in the bivariate analysis, this relationship did not continue in the multivariate model. This suggests that the observed association may be confounded by other socio-demographic factors, especially province, which showed strong independent associations with IPV. The provincial variation in IPV risk likely reflects underlying contextual differences (economic issues, cultural norms, and access to support services), which may play a stronger role in shaping IPV experiences than marital status alone. In terms of educational status, the study found that, in contrast to women with higher education, those with primary as well as those with secondary education had higher odds of IPV. These findings highlight the importance of educational diversity because women with limited access to education may have increased vulnerability, which includes economic dependence and reduced decision-making autonomy, which tend to increase their risk of IPV. Studies focusing on past-year IPV (Getachew et al., 2022; Kibret et al., 2024) and lifetime IPV (Kabir et al., 2023; Nabaggala et al., 2021) have found a strong association between lower levels of education and IPV in low- and middle-income countries. Higher levels of education are often linked with financial independence. Financial independence or higher education alone does not guarantee freedom from IPV, as social and cultural norms can pressure women from leaving abusive relationships (Gordon, 2016). In traditional societies, a highly educated wife may be perceived as a threat by her husband, leading to emotional or physical abuse as a means of asserting control (Oluwagbemiga et al., 2023). Likewise, when women contribute to household income and shift the socioeconomic balance, some men may feel their authority is undermined, resulting in increased IPV as they attempt to reassert their dominance (Buller et al., 2018).
Employment status was also associated with IPV, with employed women experiencing lower odds of IPV than unemployed women. This finding aligns with research on past-year IPV in East Africa, which suggests that employment can serve as a protective factor against IPV by improving women’s financial autonomy and decision-making power (Tessema et al., 2023). Employed women often have the financial resources and access to support services needed to leave abusive relationships, thereby reducing their vulnerability to IPV (Tenkorang, 2018; Vyas & Heise, 2016). Economic empowerment through employment also strengthens women’s decision-making autonomy, further reducing their risk of IPV (Aizer, 2010). However, it is important to note that employment alone may not be sufficient to protect women from IPV, as many employed women earn below minimum wage, which could potentially limit their financial independence and ability to escape abusive relationships (Ghoshal et al., 2023; Jabbi et al., 2020). Although employment improves financial autonomy and decision-making power, financial independence may also trigger IPV in cases where the male partner feels their authority is challenged. Research from Australia shows that women’s economic autonomy can provoke coercive control, including financial abuse and control over decision-making, as men attempt to reassert dominance in the relationship (Boxall & Morgan, 2021).
The study found that, in contrast to those who did not witness parental violence, women who witnessed parental violence had higher odds of IPV. This finding is consistent with studies on past-year IPV, indicating that exposure to parental violence can normalize IPV and increase vulnerability (Alothman et al., 2024; Coll et al., 2021; Parcon & Makani, 2024). It is important to note that not all individuals who witness parental violence experience IPV as adults; resilience factors, such as strong social support networks, can mitigate this risk (Fulu et al., 2017). In the South African context, patriarchal norms contribute to highly alarming IPV incidents in households, which result in children normalizing violence (Gibbs et al., 2020; Livings et al., 2023). The acceptability and perpetuation of IPV across generations are frequently encouraged by these cultural norms (Sikweyiya et al., 2020). As a result, to end the cycle of IPV, specific interventions that address the current perpetrators as well as cultural elements that exacerbate the perpetration of IPV are needed.
Similarly, the study found that acceptance of wife-beating was a strong predictor of IPV. Compared to those who did not agree, women who agreed that wife-beating is justified had higher odds of IPV. This finding aligns with previous research on past-year IPV, showing that women who internalize gender norms that accept violence are more vulnerable to IPV (Alothman et al., 2024; Reese et al., 2021). The association between acceptance of wife-beating and IPV reflects deeply ingrained patriarchal norms that validate violence as a form of control within intimate relationships. Women who internalize patriarchal norms tend to believe that violence is an acceptable part of their relationship, and this often lowers their resistance to abusive behavior and increases their vulnerability to IPV (Mutisya et al., 2017; Noda & Ishida, 2024; Saunders et al., 2023). In environments where such attitudes are prevalent, the abusers often feel more justified and empowered to continue engaging in violent behavior, believing that it is socially acceptable. This cycle of justification of violence contributes to the continued perpetuation of IPV.
Partner’s alcohol consumption was a strong predictor of IPV. Women whose partners drank alcohol faced significantly higher odds of IPV. Heavy alcohol use is recognized as a factor associated with increased aggression and IPV (Coll et al., 2021; Phuntsho et al., 2022). While some scholars argue that alcohol does not “cause” IPV but may be used as an excuse for abusive behavior (Devries et al., 2014; Javaid, 2015), the high rates of alcohol consumption in South Africa may worsen aggression in environments where patriarchal norms and toxic masculinity are already prevalent, thereby increasing the risk of IPV (Grobler, 2020). In these contexts, alcohol use can act as a catalyst for violence, thus reinforcing harmful gender dynamics and increasing the risk of IPV. Moreover, for the abused woman, IPV may lead to substance use. Women who experience IPV tend to have higher rates of alcohol use over time than those who do not experience violence (Davis et al., 2017). Women in these situations may use alcohol as a coping mechanism for the violence they experience in their relationship (Jones et al., 2019).
In terms of household wealth, the study found an inverse relationship between household wealth and IPV. Women from middle- and high-wealth households experienced lower odds of IPV compared to those from poor households. These findings are in line with previous studies, which indicate that better and higher economic status lowers the vulnerability of women to IPV (Phuntsho et al., 2022; Tessema et al., 2023). Economic hardship has been linked to increased IPV risk due to financial stress and power imbalances (Iman’ishimwe Mukamana et al., 2020; Phuntsho et al., 2022; Puoeng & Tsawe, 2024). Women who experience economic empowerment tend to have greater autonomy, which reduces the likelihood of being in abusive relationships (Abramsky et al., 2019; Giri & Parveen, 2024; Okumu et al., 2022). Socio-economic inequality rates in South Africa are among the highest in the world, with a large part of the population living in poverty (Francis & Webster, 2019; Sulla & Zikhali, 2018). In addition, poverty can cause social isolation, which makes it harder for women experiencing IPV to receive support and intervention from their networks (Giacomini et al., 2023; Voth Schrag et al., 2020).
We also observed significant provincial variations in the odds of IPV. Women in the Western Cape, Eastern Cape, North West, and Mpumalanga provinces had higher odds of experiencing IPV compared to women in Limpopo province. A study conducted in Liberia also found regional differences in the odds of experiencing IPV (Tsegaw et al., 2022). These regional differences may be attributed to a combination of socioeconomic disparities, cultural norms, and varying levels of gender inequality (Arenas-Arroyo et al., 2021; Stöckl et al., 2021). Provinces such as the Eastern Cape, Mpumalanga, and North West are predominantly rural, with high levels of poverty and limited employment opportunities (Statistics South Africa, 2017), which may also contribute to the higher odds of IPV. The higher IPV prevalence in some of these provinces may be linked to factors such as economic stress, stronger patriarchal norms, and limited access to social support systems. Moreover, the lower odds of IPV in Limpopo are interesting as this is a predominantly rural province; the province is home to diverse cultural groups, who have strong community structures and cultural practices that may discourage IPV—it would be interesting for future studies to explore the reasons for the lower odds of IPV in this province.
Implications for Research and Practice
The findings of this study hold several implications for both research and practical interventions aimed at addressing IPV among ever-partnered women in South Africa. The associations between several factors with IPV highlight the complex relationship between socio-demographic and behavioral factors influencing IPV risk. This suggests that researchers should do further explorations on how these factors contribute to IPV in different geographic regions, population groups, and socio-cultural environments. Specifically, the finding that younger women (aged 18–19 and 25–29 years) have higher odds of IPV compared to older women calls for age-specific interventions. The lack of consensus on which age group is at most risk of IPV highlights the need for and importance of longitudinal studies aimed at understanding how the risk of IPV progresses over time among women. In addition, the finding that employed women have lower odds of IPV calls for more refined research on the impact that employment and economic independence have on IPV risk for women; this could guide future policies aimed at economic empowerment of women as a strategy to reduce IPV.
Moreover, the strong relationship between witnessing parental violence and experiencing IPV indicates the intergenerational transmission of violence and emphasizes the need for early intervention programs (i.e., Stepping Stones and Soul City) targeting families to end this cycle of violence. Such programs could include school-based violence prevention curricula, community dialogues that challenge harmful gender norms, and media campaigns that raise awareness about IPV and promote gender equality. Likewise, the acceptance of wife-beating as a predictor of IPV shows that societal norms and attitudes are central to perpetuating IPV. Therefore, there is a need to challenge and change these norms through community education and media campaigns as a means of reducing the prevalence of IPV. Furthermore, the provincial differentials in IPV risk suggest the need for locality-specific interventions tailored to the specific needs and contexts of different provinces in dealing with IPV. While the study addresses various socio-demographic factors such as employment and household wealth, a deeper understanding of how cultural attitudes and norms about gender and violence differ across diverse populations could inform more targeted interventions. For example, differences between the predominantly rural and urban provinces, and related cultural norms, may influence the acceptability and prevalence of IPV. There is also a need for research focusing on marginalized communities within the country, including the experiences of LGBTQ+ individuals or immigrants, whose experiences of IPV may differ due to increased discrimination.
Strengths and Limitations of the Study
The study’s strength lies in its use of nationally representative data, which ensures that the findings are generalizable to women aged 18 to 49 years in South Africa. However, the study has some limitations. The cross-sectional design prevents the establishment of causality (i.e., one cannot argue that employment causes IPV). In addition, the use of self-reporting may lead to recall bias as well as social desirability bias. Some women may choose not to report cases of violence due to fear of retaliation, stigma, or not wanting to shame their partners and families. Moreover, the measure of witnessed parental violence was limited to male-perpetrated abuse against mothers and does not capture female-perpetrated violence during childhood. Although variables such as number of children, pregnancy status, and other variables are available in the SADHS dataset, they were not included in this study. We acknowledge that these are important predictors of IPV and plan to include them in future studies. Regardless of these limitations, the study provides valuable insights into the factors associated with IPV in South Africa.
Conclusion
The study found that at least one in seven women had experienced IPV from their intimate partner in the 12 months before the survey. Moreover, the study found that several socio-demographic and behavioral factors (such as marital status, level of education, witnessed parental violence, agreement that wife-beating is justified, partner’s drinking habits, household wealth, and province) were associated with IPV. Younger women, particularly those aged 18 to 19 and 25 to 29 years, were found to have higher odds of IPV, which underscores the need for age-specific interventions in dealing with IPV. The higher odds of IPV among women with primary and secondary education suggest the need for educational interventions that not only aim to increase access to education but also aim to integrate IPV prevention strategies within the curriculum. This needs to be explicitly included in school subjects like Life Orientation, at least in high schools. Moreover, the relationship between witnessing parental violence as well as acceptance of wife-beating and IPV indicates the importance of addressing intergenerational transmission of violence as well as transforming societal norms through community and policy initiatives aimed at preventing IPV. In addition, the partner’s alcohol consumption was found to be an important predictor of IPV, suggesting that addressing substance abuse could be important in IPV prevention. Furthermore, the provincial variations in the odds of IPV suggest the need for interventions that consider regional contexts in programs aimed at preventing IPV. Overall, the findings of this study emphasize the need for multifaceted policies that address the various socio-demographic and behavioral factors contributing to IPV, thus promoting comprehensive and effective prevention strategies. Future research should focus on longitudinal studies to better understand the dynamics of IPV over time and to evaluate the effectiveness of these interventions.
Footnotes
Acknowledgements
The authors acknowledge the DHS Program for providing us with access to the SADHS data.
ORCID iDs
Ethics Approval
The survey protocol for the SADHS was approved by the South African Medical Research Council (SAMRC) Committee and the ICF Institutional Review Board. The DHS maintains strict ethical procedures in collecting data for its surveys; the details are available at ![]() . Since the SADHS had ethical approval from the SAMRC and ICF, the authors did not need to seek further ethical approval.
. Since the SADHS had ethical approval from the SAMRC and ICF, the authors did not need to seek further ethical approval.
Consent to Participate
All participants gave consent to participate in the DHS data collection.
Consent for Publication
Not applicable.
Author Contributions
SKM and MT conceptualized this study. SKM, MDT, and MT worked on data acquisition, data cleaning, and analysis. SKM, TVB, LNM, MT, MDT, LS, KMEM, and BKMN wrote the manuscript. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research and/or authorship of this article.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interests with respect to the authorship and/or publication of this article.