
Abstract
Childhood abuse (CA) may not only eventuate in distorted basic beliefs among survivors but also in survivors’ doubt regarding key aspects of the abuse, of themselves during the abuse, and regarding the perpetrator. This phenomenon, which we term doubt regarding abuse-related appraisals (DARA), has not been empirically investigated. Filling this gap, this study evaluated the psychometric properties of a new measure: the Abuse Doubt Scale (ADS). The study was conducted using online surveys among convenience samples of female CA survivors. In Study 1, the ADS was administered to 155 participants. In Study 2, the ADS and a battery of questionnaires assessing abuse features, guilt, shame, dissociation, and posttraumatic stress disorder (PTSD) symptoms were administered to 192 participants. Three reliable ADS factors emerged from Study 1: doubt regarding the abuse, doubt regarding the perpetrator, and doubt regarding oneself. In Study 2, a confirmatory factor analysis confirmed the scale’s underlying factor structure. Recurrence of CA, closeness and dependence upon the perpetrator, and the perpetrator being a parental figure were associated with higher scores. Additionally, scores were correlated with guilt, shame, dissociation, and PTSD symptoms. The current studies provide evidence for the psychometric properties of the ADS, demonstrating high internal consistency as well as good construct and concurrent criterion validity. However, further longitudinal research is needed to assess the test-retest reliability and criterion validity of the ADS.
Introduction
Childhood abuse (CA), which denotes exposure to emotional, physical, or sexual abuse during childhood, has been widely recognized as a risk factor for long-term detriments, manifested in the physiological, intra-personal, and inter-personal realms (Cloitre et al., 2019; Ford & Gómez, 2015; Gewirtz-Meydan & Lahav, 2020; Harford et al., 2014; Lahav et al., 2020, 2024; Liu et al., 2018; Messman-Moore & Bhuptani, 2017; van der Kolk et al., 2005; Vonderlin et al., 2018). Evidence has indicated that CA negatively shapes victims’ basic views regarding themselves, others, and the world, and can lead to distorted cognition (e.g., Aakvaag et al., 2016; D’Andrea et al., 2012). Furthermore, interpersonal trauma such as CA appears to impede the victim’s ability to make confident judgments around abuse-related issues, resulting in their having doubt around key aspects of the abuse, of themselves during the abuse, and of the perpetrator. This phenomenon, which we term as doubt regarding abuse-related appraisals (DARA), has received some theoretical and clinical attention in the trauma field. Nevertheless, to the best of our knowledge, it has not to date been empirically investigated. As such, the goal of this study was to fill this gap by evaluating the psychometric properties of a new measure: the Abuse Doubt Scale (ADS).
CA often takes place within an invalidating environment, which is characterized by inappropriate responses to the child’s experiences, so that the child’s thoughts, feelings, and needs are disregarded, trivialized, or negated (e.g., Linehan, 1993). Over time, this invalidating attitude is internalized by the child, leading to their doubting their own feelings and judgments (Koivisto et al., 2022). Nevertheless, under conditions of CA exposure, victims’ doubt may not undermine all types of judgments equally. Instead, they may be particularly prominent around abuse-related issues due to the complex nature of the abusive dynamic and the defensive psychological mechanisms activated during abuse, described in the following sections. This phenomenon, which we term as DARA, denotes survivors’ experience of uncertainty around the qualities of the abuse itself (e.g., its severity, its legitimacy, and its labeling), themselves during the abuse (e.g., their control over the abuse and their ability to prevent it), as well as their perpetrator (e.g., whether they are dangerous or trustworthy).
It is important to note that DARA does not refer to one’s questioning whether acts defined as abuse occurred or not, but, rather, to questioning one’s appraisals of central aspects of the abuse. Additionally, DARA differs from maladaptive appraisals among trauma survivors, such as negative cognitions regarding the self (Foa et al., 1999; Gómez de La Cuesta et al., 2019), and negative appraisals of the event's severity (Kucharska, 2017). Specifically, DARA does not refer to the extent to which one holds specific appraisals regarding past abuse, but, rather, signals one’s difficulty in evaluating central aspects of the abuse with some degree of confidence. Furthermore, whereas the negative valence of one’s views is the main feature of maladaptive appraisals, the level of uncertainty around abuse-related aspects is the focus of the concept of DARA.
According to the DARA theory, developed by the first author, the complex nature of the abusive dynamic and the defensive psychological mechanisms activated during abuse are key contributors to the emergence of DARA. The following sections will describe these factors. The overwhelming nature of trauma could hamper one’s cognitive processing (e.g., Brewin et al., 1996; Ehlers & Clark, 2000; Kolk & Fisler, 1995), and this detrimental effect may be more substantial in abused children, who, due to their developmental stage, cannot modulate arousal independently (van der Kolk, 2005). Moreover, dissociative reactions during the abuse (i.e., derealization and depersonalization) may result in disorganized narratives and memories (e.g., D’Andrea et al., 2012; Halligan et al., 2003), and may lead to a breakdown in the child’s capacity to “categorize what is happening” (van der Kolk, 2005, p. 403). In this way, abused children may experience a considerable confusion around the abuse itself, themselves during the abuse, and their perpetrators, and these core aspects may thus be tinged with substantial doubt.
The abused child and perpetrator dynamic, which is characterized by an asymmetric distribution of power, complexity, elusiveness, and unpredictability (Herman, 1992), might serve as an additional source for DARA. The perpetrator often attacks the child’s mind by repeatedly denying the abuse and undermining the child’s basic perceptions (Harsey et al., 2017). Moreover, the perpetrator might convey contradictory dissociative motivations and exhibit distorted interpretation of the abusive reality: brutality and aggression might be labelled by the perpetrator as affection, and exploitation might be interpreted as indicating that the child is special to the perpetrator (Jackson et al., 2015). In this way, the perpetrator induces confusion in the child, shattering their ability to trust their own perceptions of the abuse.
The negative implications of the abusive dynamic for DARA might be further fueled by the phenomenon of identification with the aggressor. Identification with the aggressor denotes a reaction that aims to promote the child’s survival by fusing with the perpetrator and adopting their experience (Ferenczi, 1933; Frankel, 2002; Lahav et al., 2020). This reaction, which may be particularly prominent within a specific self-state of the child, may co-exist in a disconnected manner alongside other self-states, which hold contradictory feelings and views regarding the abuse (Davies & Frawley, 1994). Thus, whereas the self-state that identifies with the aggressor may normalize the abuse, and blame the child themself for the abuse, other self-states may appraise the situation differently (Lahav et al., 2017). Due to the dissociative nature of these self-states, the child's ability to reconcile these contradictions and to produce integrative evaluations regarding the abuse is impaired. Instead, irregularities and uncertainty emerge (Davies, 2004).
The chronic nature of the aforementioned processes involved in CA (Herman, 1992; Lahav, Talmon, & Ginzburg, 2019; van der Kolk, 2005) implies that their potential harm to victims’ ability to trust their judgements might not be limited to the time of the abuse, but rather will be evident even years after it has ended. Moreover, based on the literature, DARA among CA adult survivors may be linked with CA features as well as with survivors’ distress subsequent to the abuse.
As mentioned earlier, the perpetrator’s attacks on the victim’s views may result in DARA (Davies, 2019). These effects might be particularly prominent when the victim had lengthy interactions with the perpetrator. Therefore, it is reasonable to expect that survivors who underwent recurrent abuse would suffer from elevated DARA. Additionally, in cases in which victims are highly dependent and emotionally connected to their perpetrators, the victims’ need to preserve the relationship is particularly evident, thus leading to heightened reliance upon defensive mechanisms, such as dissociation and identification with the aggressor (Lahav, Talmon, & Ginzburg, 2019). Although these mechanisms enable victims to emotionally survive the abuse (Freyd, 1997), they may impede their ability to trust their judgments. Therefore, it is reasonable to expect that DARA would be linked to survivors’ closeness to and dependence upon their perpetrators and would be more prominent among survivors of abuse inflicted by family members.
The experience of DARA may be associated with survivors’ distress and manifested in elevated guilt, shame, PTSD symptoms, and dissociation symptoms. Difficulties in trusting one’s judgments regarding the abuse might limit victims’ ability to acknowledge the mistreatment and its subsequent injuries. This, in turn, may fuel self-attributions of shame or “badness,” intensify feelings of blameworthiness, and pose a substantial obstacle to reprocessing the trauma (Frankel, 2002). Thus, elevated DARA is expected to be related to survivors’ shame and guilt over the abuse, as well as with trauma-related symptomatology manifested in PTSD and dissociative symptoms.
The conceptualization of DARA suggested by the current authors aligns with trends identified in research. For example, studies have shown that some CA survivors were unsure as to how to label their abuse (Hammond & Calhoun, 2007; Stander et al., 2002) and reported confusion and difficulties in making sense of it (Leahy et al., 2003). Additionally, studies that explored a general tendency for doubt regarding one’s judgment have indicated it to be linked to distress, manifested in depression and anxiety (Mirels et al., 2002). However, none of the aforementioned studies directly investigated DARA itself; instead, they examined factors associated with DARA or suggestive of its existence. As a result, they do not provide empirical validation of the concept. The present study seeks to address this gap by introducing a new instrument—the ADS—designed to facilitate the systematic investigation of DARA. This article describes the ADS and the results of two studies assessing its psychometric properties. The first study presents the ADS and its structure. The second study aims to confirm the scale’s structure and evaluate its reliability and validity.
Study I
This study aims to develop the ADS—creating its items and analyzing its factor structure.
Methods
Participants and Procedure
We conducted an online survey of a convenience sample of Israeli adults. The survey, which was advertised as a research project examining the effects of early adverse life events, was distributed through social media platforms, such as Facebook, and was accessible via Qualtrics, a secure data collection system. It was available from September 15 to November 15, 2021, and took approximately 20 min to complete. The inclusion criteria were: (a) participants must be 18 years of age or older, and (b) they must be fluent in Hebrew. No data linking participants to recruitment sources were collected, and the survey was designed to ensure the anonymity of respondents. The Tel Aviv University Institutional Review Board (IRB) approved all procedures and instruments. Clicking on the link to the survey guided potential respondents to a page that provided information about the purpose of the study, the nature of the questions, and a consent form. The first page also offered researcher contact information. Each participant was given the opportunity to take part in a lottery that included five gift vouchers worth $30 each.
To prevent duplicate survey entries, the Qualtrics platform’s built-in “Prevent Ballot Box Stuffing” feature was enabled. Additionally, to identify and exclude potential fraudulent responses from bots, records associated with duplicate IP addresses were removed from the dataset. Data were collected in 2021, before concerns about AI-generated responses emerged. Standard data quality checks were applied to ensure the integrity of the responses. These included the exclusion of non-admissible or implausible values in quantitative items (e.g., out-of-range responses) and removal of unintelligible or nonsensical entries in open-text fields (e.g., random characters or off-topic responses). In addition, minimum completion time thresholds were used to identify inattentive responding.
A total of 350 participants completed the survey; however, for this study, we only used data gathered from participants who were classified as having a history of CA based on the short form of the Childhood Trauma Questionnaire (SF-CTQ; Bernstein et al., 2003). Participants were classified as having a history of CA if they had scores higher than the following cutoff scores suggested by Tietjen et al. (2010): physical abuse ≥ 8; sexual abuse ≥ 6; and emotional abuse ≥ 9.
The final sample consisted of 192 (54.8%) participants who were classified as having a history of CA. Of these, 66 (34.4%) were classified as having a history of physical abuse; 88 (45.8%) were classified as having a history of sexual abuse; 164 (85.4%) were classified as having a history of CA; and 101 (52.6%) were classified as having a history of at least two types of abuse. The sample was heavily biased towards women (84%), with 29 participants (15%) identifying as male, and 2 participants (1%) identifying as other. Due to a priori differences that may arise between genders, and the potential statistical bias in a non-balanced sample, we included only female participants in our study. A Mahalanobis test for detecting outliers suggested deleting six more observations from our data (Mahalanobis, 1936; Penny, 1996); hence, the final sample consisted of 155 female participants. Mean age was 41.74 (SD = 11.69), and 77% (n = 119) of participants were secular. The distribution of income was left-skewed: 47% (n = 72) had a below-average income; 26% (n = 41) had an average income; and the remaining 28% (n = 42) had an above-average income. The majority of participants (79.9%, n = 124) had attained different levels of tertiary education: 12.9% (n = 20) held a vocational/technical diploma, 40% (n = 62) held a Bachelor’s degree, 25.8% (n = 40) held a Master’s degree, and the remaining 1.3% (n = 2) held a PhD. Roughly half of the participants, 53.5% (n = 83), reported being involved in an intimate relationship.
Measures
Background Variables
The questionnaire included demographic questions assessing age, gender, education, income, marital status, and sexual orientation.
The ADS
The ADS was developed to assess DARA. Based on the DARA theory described above, the operational definition of DARA refers to survivors’ doubts concerning three core abuse-related appraisals: doubts regarding the features or qualities of the abuse, doubts regarding the survivor’s own experience and behavior in the context of the abuse, and doubts regarding the characteristics of the perpetrator. In accordance with these expressions, an initial pool of 39 items was generated.
To evaluate the initial pool of items, experts in CA were recruited through purposive sampling. Inclusion criteria were: (a) a minimum of ten years of professional experience in treating or assessing survivors of CA; (b) advanced academic qualifications (a master’s degree or higher); and (c) demonstrated expertise through research publications or clinical practice related to interpersonal trauma and CA. Potential experts were identified through institutional affiliations and professional networks. A total of seven experts were invited by email, which included information about the study’s purpose, their expected role in evaluating item relevance and clarity, the estimated time commitment, and assurances of confidentiality. Four experts agreed to participate, consisting of two academic researchers and two clinical practitioners, with an average of 16.3 years of experience in the field (SD = 2.5). They were provided with the definition of DARA and asked to rate the extent to which they believed each item reflected DARA. Additionally, they were encouraged to suggest modifications, identify any missing items, and note any redundancies.
Next, to assess the clarity, comprehensibility, and interpretability of the scale items among laypeople, the scale was presented to three university undergraduate students who were fluent in Hebrew and unfamiliar with both the study and the CA literature. These individuals were asked to review the items and identify any that were unclear in meaning. Based on feedback from both the experts and the students, minor wording revisions were implemented, and six redundant items were removed.
The final version of the questionnaire included a total of 33 items. To avoid social desirability bias, and to ensure that the items assessed the experience of doubt rather than the strength of appraisals, they were phrased in a way that comprised both possible responses to unanswered questions regarding past abuse (e.g., I have doubts as to whether the harm inflicted was severe or not severe). Respondents were presented with the items deemed to address “doubts that may arise in regard to harm inflicted by another person.” Participants were asked to rate, on a 5-point Likert-type scale ranging from 0 (not at all) to 4 (very much), the extent to which they had experienced each manifestation of doubt in regard to the CA they had reported earlier.
Data Analysis
The analysis was performed using R software. Of the total 155 participants, none of the data was missing. Since a theoretical model underlies the analysis, and questionnaire items are designed to be reflective, we employed an Exploratory Factor Analysis (EFA) procedure (Schmitt, 2011). Our extraction procedure was based on Principal Axial Factoring (PAF), since it requires no distributional assumptions (Fabrigar et al., 1999). We applied the Mahalanobis distance measure for our raw data, to detect and omit outliers, and applied a conservative threshold of p < .0001 to set a critical
The item screening procedure relied on the primary and secondary factor loadings. We retained items with primary loadings of 0.4 or more, and eliminated items with cross-loadings >0.32 (e.g., Tabachnick & Fidell, 2001). Since we aimed to achieve a simple structure, we took into consideration row-complexity indices and eliminated items that failed to load on a single factor (Pettersson & Turkheimer, 2010). We employed Kaiser’s and Jolliffe’s eigenvalue criterion and Cattel’s scree test as preliminary tests for the optimal number of factors to be retained. Since both methods are prone to over-factoring, we also employed the Parallel Analysis method, which is more effective in identifying the optimal number of factors in EFA (Finch, 2020). We also took into consideration the percentage of variance extracted by the process, using 0.5 as an acceptable threshold for the total variance explained, and 0.75 as the desired threshold (Beavers et al., 2013). To assure interpretability of the factor structure, we applied Velicer’s Minimum Average Partial (MAP) test, and Revelle and Rocklin’s Very Simple Structure (VSS) criterion for the correlation matrix.
We tested for model fit using the common thresholds requiring a Tucker–Lewis Index (TLI) value of 0.95 or more and a root mean square error of approximation (RMSEA) value <0.1. The reliability of the scale was assessed using its internal consistency, which was measured using Cronbach’s alpha.
While our sample size is at the threshold of the traditional rule of thumb suggesting a sample size of
Results
Factor Analysis
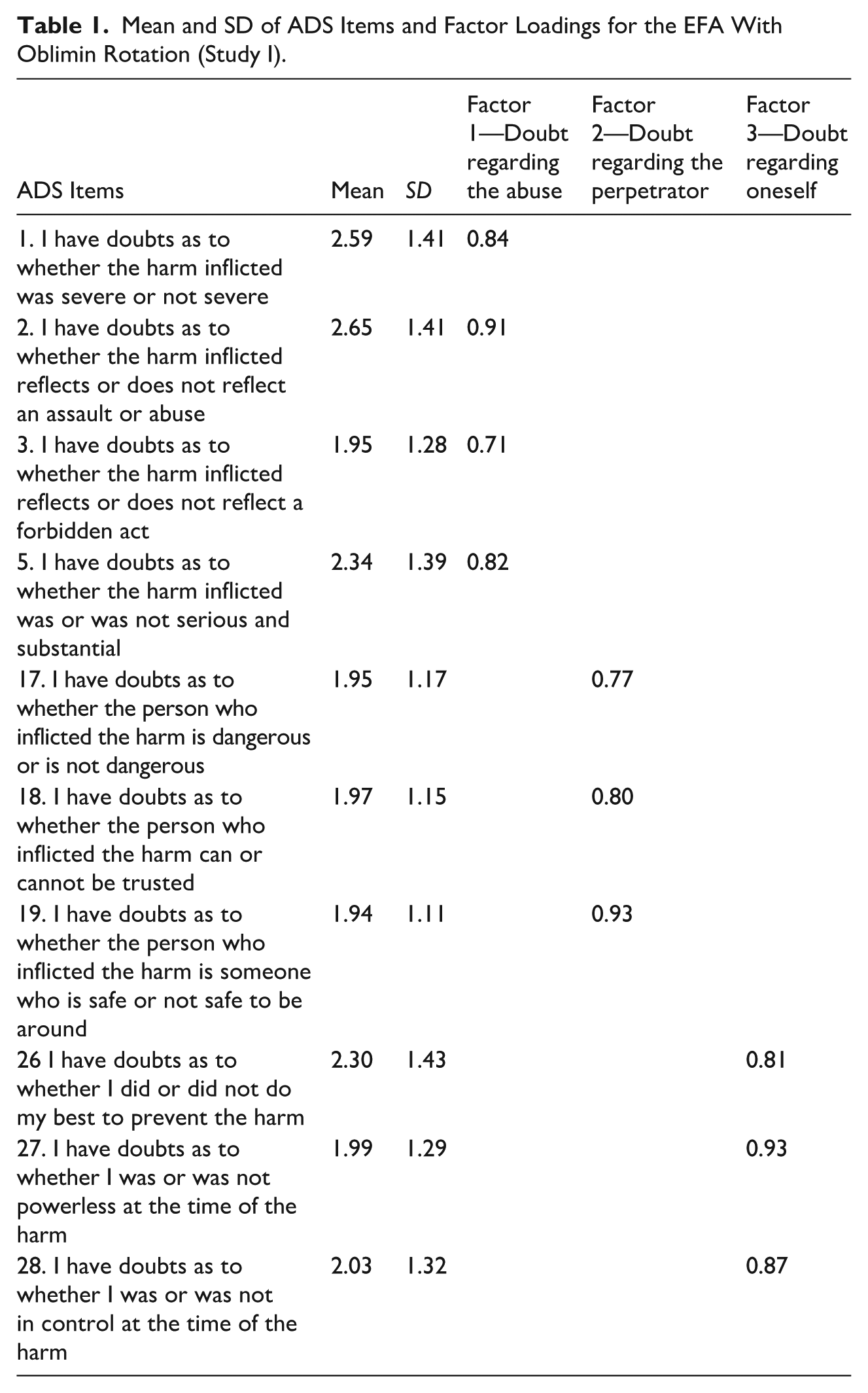
Factor loadings, mean, and SD for the final scale are presented in Table 1. The first step of our analysis included testing for the factorability assumptions on all 33 original items of the ADS questionnaire. The initial correlation matrix proved factorable under both Bartlett’s test (
Mean and SD of ADS Items and Factor Loadings for the EFA With Oblimin Rotation (Study I).
Variance Explained by the Factor Solution
The final 10-item ADS questionnaire accounted for 71% of the total variance. Factor 1, “Doubt regarding the abuse,” comprised four items and explained 27% of the variance (eigenvalue = 4.54); Factor 2, “Doubt regarding the perpetrator,” comprised three items and explained 23% of the variance (eigenvalue = 1.86); and Factor 3, “Doubt regarding oneself,” comprised three items, and explained 21% of the variance (eigenvalue = 1.53).
Reliability
The internal consistency of all three factors and total score was high: 0.89 for Factor 1, 0.87 for Factor 2, 0.90 for Factor 3, and 0.87 for the total score.
Correlation Analysis
The three factors were positively and significantly correlated with one another: Factors 1 and 2
Study 2
Study 2 had three main objectives: (a) Confirming the ADS’s underlying factor structure; (b) assessing the ADS’s criterion validity by testing for its correlation with shame, guilt, PTSD symptoms and dissociation; (c) assessing the ADS’s construct validity by testing for its association with the recurrence of CA, the role of the perpetrator in survivors’ lives, and closeness to and dependence on the perpetrator. Three hypotheses were formed: Hypothesis 1: DARA would be associated with elevated shame, guilt, PTSD symptoms, and dissociation. Hypothesis 2: The recurrence of CA, and the role of the perpetrator in the survivor’s life, would be linked with DARA, so that individuals who reported recurrent CA or CA inflicted by a family member would have elevated DARA than individuals who reported single-episode CA or CA inflicted by an extra-familial figure, respectively. Hypothesis 3: Closeness to the perpetrator and dependence upon the perpetrator would be linked with elevated DARA.
Methods
Participants and Procedure
We conducted an online survey of a convenience sample of Israeli adults. Inclusion criteria were: (a) being 18 years of age or older and (b) fluency in Hebrew. A web-based survey was published on social media and made accessible through Qualtrics. The survey took 25 min to complete and was open from February 1, 2022, to March 1, 2022. Data were collected approximately 1 year after Study 1, and participants were asked to provide their email addresses in both studies to ensure that no participant from Study 1 was mistakenly included in Study 2. As with Study 1, data were collected in early 2022, before concerns about AI-generated responses had emerged. Standard data quality checks were applied.
The Tel Aviv University IRB approved all procedures and instruments. Clicking on the link to the survey guided potential respondents to a page that provided information about the purpose of the study, the nature of the questions, and a consent form. The first page also provided contact information for the researcher. Each participant was given the opportunity to take part in a lottery that included five gift vouchers worth $30 each.
Of 510 participants who filled the survey, 211 were classified as having a history of CA based on the SF-CTQ (Bernstein et al., 2003). Of these, 19 were omitted from the sample: first, since Study 1 included only female participants, 17 male participants were omitted from the sample, leaving female participants only. Second, a Mahalanobis test for detecting outliers suggested deleting two additional observations from our study. Thus, the final sample consisted of 192 female adult survivors of CA. Of these, 77 (40.1%) were classified as having a history of physical abuse; 180 (93.8%) were classified as having a history of sexual abuse; 136 (70.8%) were classified as having a history of emotional abuse; and 134 (69.8%) were classified as having a history of at least two types of abuse. The mean age of participants was 41.9 (SD = 10.84), and 72% (n = 139) were secular. The distribution of income was left-skewed: 53% (n = 101) had a below-average income; 22% (n = 43) had an average income; and 25% (n = 48) had an above-average income. The majority of participants (79.2%) had attained some level of tertiary education: 19.2% (n = 37) had a vocational/technical diploma; 32.3% (n = 62) had a Bachelor’s degree; 24.5% (n = 47) had a Master’s degree; and the remaining 3.1% (n = 6) had a PhD.
Measures
Background Variables
The questionnaire included demographic questions assessing age, gender, education, income, and marital status.
Features of Abuse
Participants with a history of CA were asked to specify the features of abuse via four items designed by the research team. These features were: (a) whether the abuse had been a one-time event or recurrent; (b) whether the perpetrator was a family member or extra-familial figure; (c) their closeness to the perpetrator before the abuse took place, indicated on a 5-point scale from not at all to very much; and (d) their dependency upon the perpetrator before the abuse took place, assessed on a 5-point scale from not at all to very much.
Shame and Guilt
Shame and guilt were assessed via the shame and guilt subscales of the Abuse-Related Beliefs Questionnaire (Ginzburg et al., 2006), comprising six and eight items, respectively. Respondents were asked to indicate to what extent they agreed with each statement on a 5-point Likert-type scale ranging from 1 (strongly agree) to 5 (do not agree at all). The ARBQ has high validity and reliability (Ginzburg et al., 2006). In this study, the internal consistency reliabilities were 0.82 and 0.89 for shame and guilt, respectively.
PTSD Symptoms
PTSD symptoms subsequent to CA were measured via the PCL-5 (Weathers et al., 2013), a 20-item scale that corresponds to the criteria in the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013). Participants were asked to indicate the extent to which they experienced each symptom on a 5-point Likert scale ranging from 0 (not at all) to 4 (extremely). The original version was adapted so that the index event was CA. A total score of PTSD symptoms was calculated by summing all 20 items. The PCL-5 demonstrates high internal consistency and test–retest reliability (Bovin et al., 2016). In this study, internal consistency reliability was excellent (α=.96).
Dissociation Symptoms
Dissociation was measured by the Dissociative Experiences Scale-II (DES-II; Carlson & Putnam, 1993), a 28-item self-report questionnaire that measures the frequency of dissociative experiences. The total score was computed as the mean of these 28 items, ranging from 0 to 100. The DES-II has been shown to have high validity and reliability (Frueh et al., 1996). In this study, the inventory was found to have high internal consistency (α = .95).
Data Analysis
The analysis was performed using R software. None of the data was missing. We employed a Confirmatory Factor Analysis with a PAF extraction procedure. We again tested for outliers using the Mahalanobis distance measure for the raw data. We tested for the model’s fit using several criteria: We applied the normed chi square (
The reliability of ADS was tested using Cronbach’s alpha for internal consistency. The ADS’s criterion validity was tested via correlation tests between its factors and shame, guilt, PTSD symptoms, and dissociation. The ADS’s construct validity was tested by using correlation tests between factors of ADS and the victim’s levels of closeness to and dependency on the perpetrator as well as comparative t-tests and ANOVA for the scale’s factor scores between measures of recurrence of CA and the role of the perpetrators in survivors’ lives. Correlations in this part of our work were corrected for attenuation (Bobko, 1983).
Results
ADS Structure
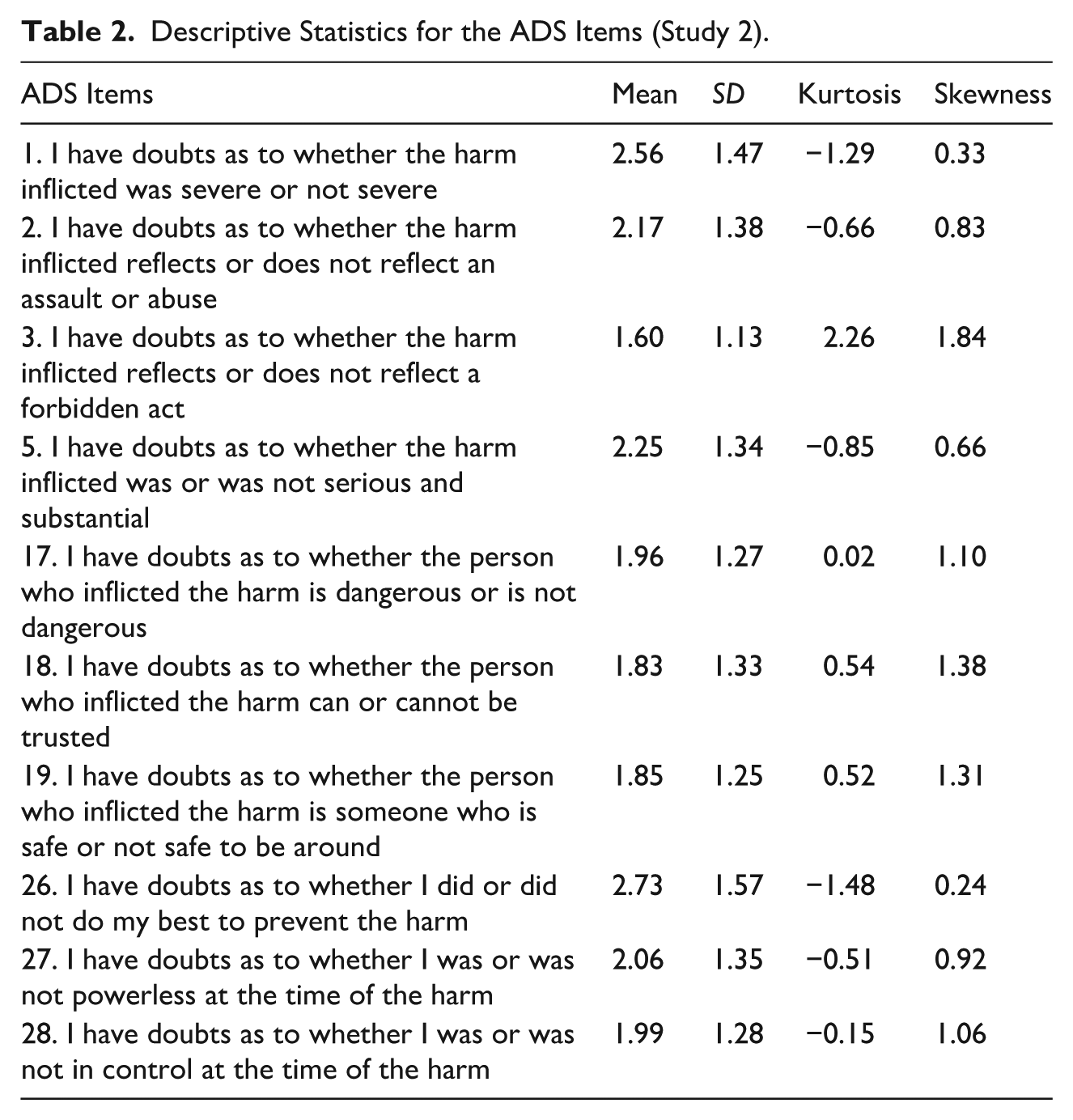
Central tendency indices for the ADS items are shown in Table 2, and the hypothesized three-factor model is presented in Figure 1. Predicted regression coefficients were all significant with
Descriptive Statistics for the ADS Items (Study 2).
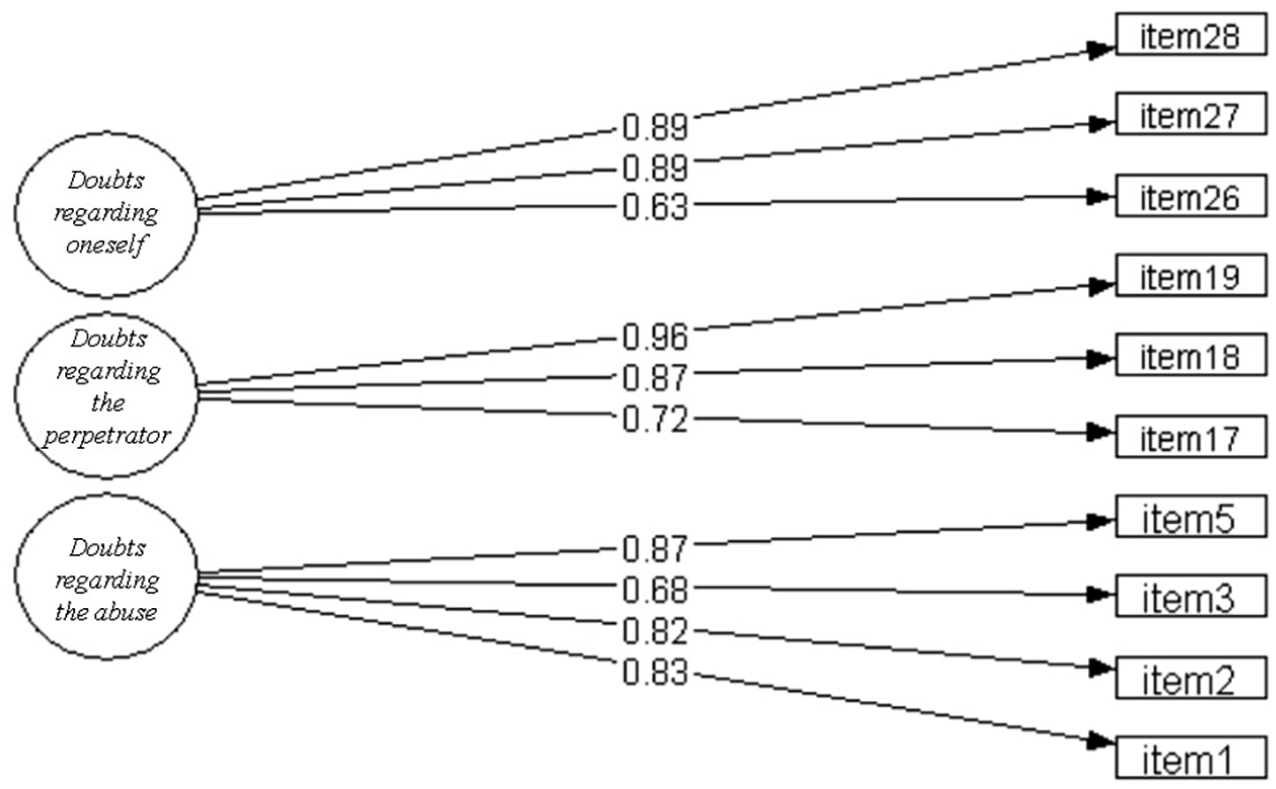
Results of the confirmatory factor analysis (Study 2).
Reliability
The internal consistency of all three factors and the total score was high: 0.88 for Factors 1 and 2, 0.83 for Factor 3, and 0.86 for the total of the scale.
Criterion Validity
All three factor scores and the total ADS score were correlated with shame and guilt—the higher the levels of doubt regarding the abuse, the perpetrator, and oneself, the higher the levels of shame and guilt regarding the abuse (Table 3). Factor 1, Factor 3, and the ADS total score were correlated with PTSD total score—the higher the levels of doubt regarding the abuse and regarding oneself, the higher the levels of PTSD symptoms. Factor 3 and the ADS total score were correlated with the dissociation total score—the higher the level of doubt regarding oneself and the greater the total levels of doubt, the higher the levels of dissociation symptoms.
Pearson and Spearman Correlations Between ADS Factors, Closeness and Dependency Upon the Perpetrator, PTSD, Shame, Guilt, and Dissociation.
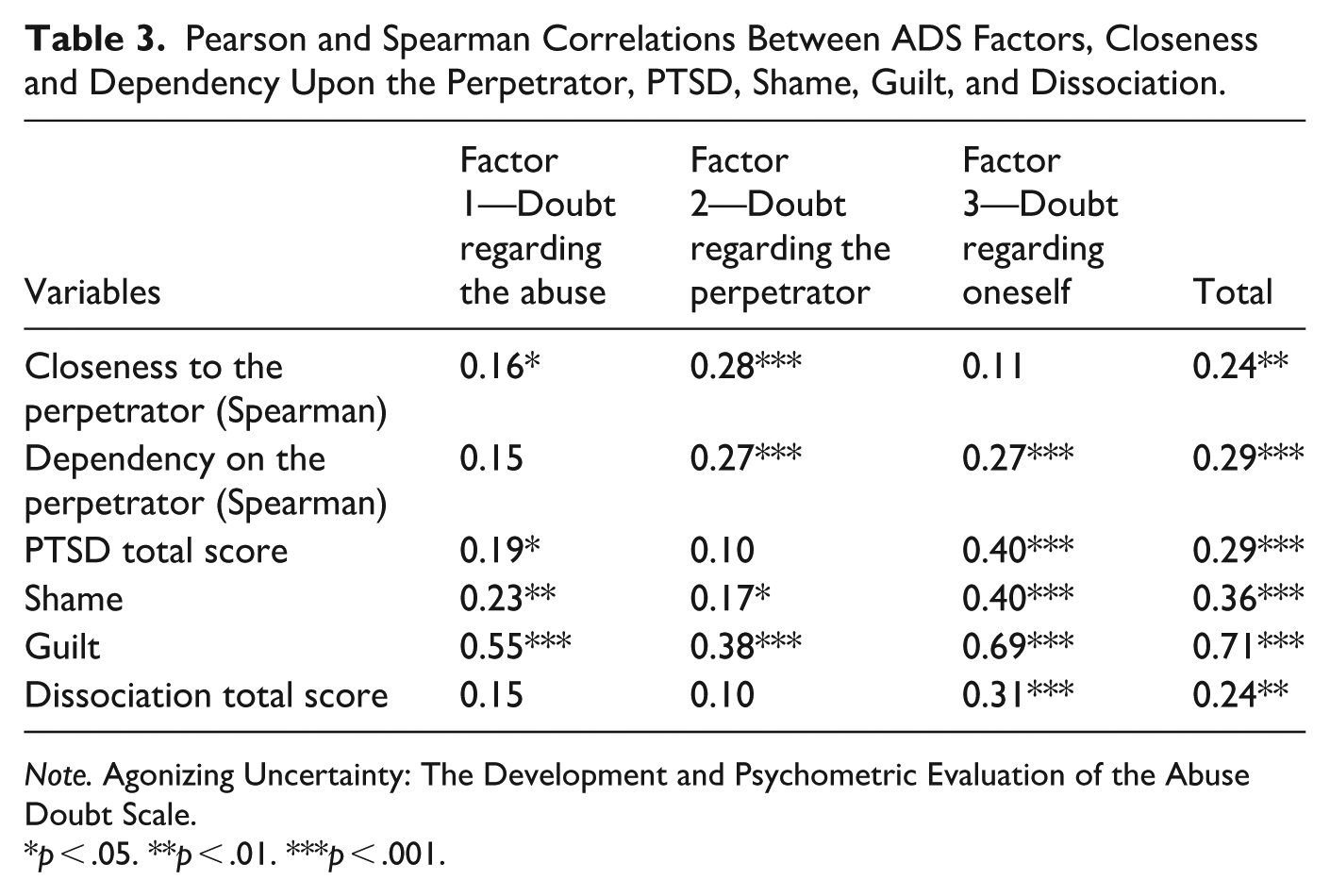
Note. Agonizing Uncertainty: The Development and Psychometric Evaluation of the Abuse Doubt Scale.
p < .05. **p < .01. ***p < .001.
Construct Validity
As hypothesized, Spearman correlations indicated that closeness to the perpetrator was positively associated with Factors 1 and 2, and with the total score. Dependency on the perpetrator was positively associated with Factors 2, 3, and the total score (Table 3). Factor scores and the ADS total score were significantly higher for participants who had experienced recurrent CA than for those who had experienced a single episode (t(124.4) = -1.92, p = 0.03, t(165.1) = 4.86, p < 0.001, t(190) = 3.1, p = 0.001, t(144.4) = 4.36, p <0 .001, respectively). Factor scores and the ADS total score were significantly higher for participants abused by a family member than those abused by extra-familial figure (t(186.2) = 2.51, p < 0.001, t(187.5) = 3.57, p < 0.001, t(188) = 2.11, p = 0.018, t(187.7) = 3.59, p < 0.001, respectively).
Discussion
Although the trauma literature points toward the potential implications of CA for survivors’ doubts concerning their abuse-related appraisals (Lahav, Talmon, & Ginzburg, 2019; Leahy et al., 2003; van der Kolk, 2005), research on the concept of DARA has, until now, been lacking. This gap might be partly rooted in the absence of a measurement for assessing this phenomenon. Therefore, the construction and validation of the ADS are imperative. Our work consisted of two studies: the first explored the factor structure of the ADS, and the second confirmed its validity. The current results support the psychometric properties of the ADS and suggest that the ADS may operate as a valuable tool in assessing DARA among CA adult survivors. Study 1 revealed three factors of ADS, comprising doubt regarding the abuse, doubt regarding the perpetrator, and doubt regarding oneself. The ADS had good internal consistency for all three factors.
Study 2 revealed that the ADS has good construct and criterion validity. As in the theoretical literature (Freyd, 1997; Lahav, Talmon, & Ginzburg, 2019), DARA levels, as assessed by ADS, were higher among participants who reported recurrent abuse than among survivors of single-episode abuse and among survivors of CA inflicted by a family member than among survivors of CA inflicted by an extra-familial figure. In addition, as hypothesized, levels of DARA were significantly correlated with survivors’ closeness to and dependence upon the perpetrator, as well as with standard measures of shame, guilt, PTSD symptoms, and dissociation.
The findings of Study 2 indicated elevated DARA among survivors who had experienced recurrent abuse or abuse inflicted by a family member compared to survivors of a single episode of abuse or abuse inflicted by an extra-familial figure. Additionally, there was a significant relationship between survivors’ closeness to, and dependence upon, the perpetrator and DARA, such that the higher the levels of closeness and dependence, the higher the levels of DARA. These findings may reflect the long-term detriments of CA on victims’ ability to feel confident when they try to make sense of the abuse. Our findings suggest that exposure to protracted abuse during childhood, when one’s ability to modulate arousal and to form accurate evaluations is yet to be developed (Brewin et al., 1996; Ehlers & Clark, 2000; Kolk & Fisler, 1995; van der Kolk, 2005) may eventuate in DARA. Furthermore, it might be that the quality of the victim and perpetrator dynamic shapes DARA among victims, such that being abused by a family member or by a perpetrator to whom victims feel close and upon whom they depend may render them particularly vulnerable. Although reliance upon mechanisms such as dissociation and identification with the aggressor may allow these survivors to protect their relationship with the abuser (Freyd, 1997; Lahav, Talmon, & Ginzburg, 2019), they may also breed confusion and self-doubt. Thus, this specific group of CA survivors may particularly struggle with uncertainty around judgments concerning the abuse, the perpetrators, and themselves.
Study 2 revealed that DARA was significantly correlated with elevated shame, guilt, PTSD symptoms, and dissociation. These findings may reflect the impact of trauma-related distress on survivors’ DARA. Negative appraisals regarding the self, as well as dissociative and PTSD symptoms, may negatively shape survivors’ ability to trust their judgment, thereby intensifying their DARA. At the same time, however, the current findings may reflect some of the potentially negative outcomes of DARA. It may be that elevated doubt concerning abuse-related appraisals may not only illicit discomfort and unease among survivors but may also jeopardize the healing process. Questioning one’s evaluation concerning the abuse might fuel negative self-attribution and lead to feelings of shame and guilt around the trauma. Furthermore, difficulty trusting one’s appraisals of the trauma may erode survivors’ belief systems and hamper their ability to reprocess the trauma, and thus may eventuate in elevated dissociation and PTSD symptoms (Frankel, 2002). Elevated distress and psychopathology manifested in guilt, shame, dissociation, and PTSD have been documented among CA survivors and have been explained by several processes (e.g., Aakvaag et al., 2016; Vonderlin et al., 2018). The present findings suggest that DARA could contribute to the distress of CA survivors, and that taking DARA into account may expand our understanding of these detriments.
Study Limitations
The results of these studies should be considered in light of their limitations. First, both studies were based on self-report measures and may have been subject to response biases. Second, the current studies relied on convenience sampling, were conducted online among Israeli participants, and comprised exclusively female respondents. Although our sample included women from diverse ethnic backgrounds, the concept of race does not align directly with the social and demographic structure of Israeli society, as Israel is not organized around racial categories in the same way as the United States or United Kingdom populations. For example, individuals of Ethiopian, Yemeni, or Moroccan descent may all be categorized as “Mizrahi” or “Sephardi” but are not identified by race in the Israeli context; the terms “Black” or “African Israeli” are not commonly used in population surveys. To address social diversity, we included a measure of religiosity, which is a key variable for ensuring representation across major societal sectors in Israel (e.g., secular, traditional, religious, ultra-Orthodox). We deliberately chose not to ask participants to specify their religion to avoid offending religious minorities. Additionally, we used years of education as a proxy for socioeconomic status (SES), as it is one of the most reliable and non-intrusive indicators of SES in Israel. Nevertheless, given the importance of exploring CSA in Black and minoritized communities (e.g., Gill & Begum, 2022), these factors represent a substantial limitation to the generalizability of the study. They also underscore the need to investigate DARA across a broader range of populations, particularly within clinical samples of male and female CA survivors from diverse ethnic, cultural, and religious backgrounds in various global contexts. Additionally, given the study’s cross-sectional design, readers should be cautious in assuming causal relationships between the study variables. Future longitudinal studies should explore the criterion validity of ADS, its stability over time, and its sensitivity to changes. Finally, while the methodological literature supports the adequacy of our sample sizes under conditions such as high communalities and a simple factor structure, we recognize that larger samples could further strengthen the generalizability of our findings and support future validation efforts.
Implications
Notwithstanding the limitations above, the results of the current studies provide evidence for the internal consistency, construct validity, and concurrent criterion validity of ADS, and therefore may serve as a feasible tool for measuring DARA. It is important to note, however, that the ADS is not intended to replace well-known measures of maladaptive appraisals, as it does not assess the extent to which one holds specific appraisals regarding past abuse. Instead, the ADS appears to serve as an assessment tool that sheds light on DARA—an additional detriment of CA that may co-exist alongside maladaptive appraisals and that has not been empirically investigated to date.
Being subjected to abuse may impede survivors’ ability to trust their judgment concerning their experiences. This could pose a burden for survivors and might jeopardize their ability to reprocess the trauma. Additionally, given that some degree of certainty around one’s appraisals is essential for decision-making and assertiveness (Mirels et al., 2002), it appears that DARA could be implicated in survivors’ difficulties engaging in self-protective behaviors within interpersonal settings, particularly within those that resemble their original abuse (Littleton & Decker, 2017), and thus may explain the elevated risk for re-victimization among CA survivors (Walker et al., 2019). Furthermore, although the theoretical literature on survivors’ experiences of doubt concerning abuse-related appraisals mainly focuses on CA, DARA might also be applicable to survivors of other types of abuse (e.g., intimate partner violence). Thus, investigating DARA might serve as a step forward in the trauma field, promoting better understanding and treatment of survivors of CA as well as of different types of abuse during adulthood.
Footnotes
Acknowledgements
The authors thank Dr. Ron Nasim, Dr. Anat Gur, and Dr. Liat Perry Lerer for their helpful insights and contributions to the refinement of the scale.
Funding
The authors received no financial support for the research and/or authorship of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.