
Abstract
Reproductive coercion and abuse (RCA) involves the use of violence, deception, or threats to undermine another person’s reproductive autonomy. Largely perpetrated against women by their male intimate partners or other close family members, RCA is harmful to health and well-being. Despite this, it is under-researched, with conceptually sound, robust data lacking globally. The present study addresses this gap within the Australian context by analysing data from the Australian Longitudinal Study on Women’s Health, a national, longitudinal, representative community survey of over 56,000 women. For this study, we focused on women born in 1973 to 1978. Our aims were to identify the prevalence of partner-perpetrated RCA (both pregnancy-preventing and pregnancy-promoting), explore sociodemographic variables from early adulthood that may predict RCA later in life, and examine associations between RCA and other forms of violence. We found that around 4.5% of our sample had experienced RCA by age 43 to 48 years perpetrated by a current or former partner. We found evidence of associations between financial insecurity, smoking status, and being partnered at age 18 to 23 years and experiences of RCA by age 43 to 48 years. We also found associations between RCA and experiences of physical intimate partner violence, sexual intimate partner violence, and harassment. A history of childhood physical or sexual abuse was also predictive of lifetime RCA victimisation by age 43 to 48 years. Our findings suggest that RCA may affect a considerable proportion of women in Australia. Despite this, RCA has received little attention in policy or practice. Our findings also shed light onto potential risk factors that could be addressed early to reduce the likelihood of experiencing RCA later in life, as well as highlighting the relationship between RCA and other forms of violence. These findings have important implications for risk assessment, identification, and response.
Introduction
Reproductive coercion and abuse (RCA) is broadly defined as behaviour that deliberately undermines a person’s control over their reproductive decision-making (Grace & Anderson, 2018; Tarzia & Hegarty, 2021). It encapsulates the use of physical violence, threats and emotional coercion, deception, rape, and financial abuse to compel a person to (a) become or remain pregnant or (b) prevent pregnancy or terminate a wanted pregnancy (Tarzia & Hegarty, 2021). Although there is some debate amongst scholars in the field (Grace & Miller, 2023; Rowlands & Walker, 2019; Tarzia & Hegarty, 2021), it is generally accepted that RCA is primarily perpetrated against women and those with the capacity for pregnancy, usually by their male intimate partners or other close family members (Grace & Anderson, 2018; Tarzia & Hegarty, 2021). Qualitative research – primarily undertaken in Western cultural contexts – strongly suggests that RCA often occurs in a context of fear and/or control, with perpetrators weaponising the victim/survivor’s reproductive capacity in the context of broader patterns of abuse (Moulton et al., 2021; Tarzia & Hegarty, 2021; Tarzia & McKenzie, 2024). However, recent work also indicates that perpetrators may have different motivations for controlling a pregnancy outcome, with some perpetrators being driven by selfishness rather than a desire to exert long-term control over a partner (Tarzia & McKenzie, 2024). Studies undertaken in low-and-middle-income countries (Pearson et al., 2023; Thomas et al., 2024) or with migrant populations (Suha et al., 2022) have described additional motivations for perpetrating RCA such as son preference, adherence to cultural norms around women’s role in reproduction, wanting to end a relationship, or wanting to prevent a woman from partnering with another man.
Despite increasing attention being paid to RCA – both in Australia (Commonwealth Government, 2023) and globally (American College of Obstetricians and Gynecologists, 2013; Pearson et al., 2023; Wood et al., 2023) – there is a lack of robust data to guide policy and practice. As Tarzia and Hegarty (2021) have argued, the available evidence base is hampered by a number of serious methodological concerns that call into question findings around the magnitude of the problem, the contexts in which RCA occurs, as well as its health impacts and sociodemographic associations. These conceptual oversights need urgent attention as RCA scholarship advances.
Limitations of Current RCA Measurement Tools and The Implications for Interpreting The Evidence Base
RCA research globally is hampered by two major conceptual issues. First, there has been a tendency to define RCA as forced pregnancy alone, excluding forced abortions or forced continuation of pregnancy (e.g. Basile et al., 2019; Black et al., 2010; Miller et al., 2014; Wood et al., 2023). The most widely used measurement tool currently available – the Reproductive Coercion Scale (McCauley et al., 2017) – for instance, does not include items on forced abortion or on forced continuation of pregnancy. Although the Reproductive Coercion Scale has been validated and adapted for use in low-and-middle-income countries (Wood et al., 2023), the omission of these other forms of RCA means that only one portion of potential experiences are being captured.
Another common way to measure RCA is to use a two-item set of questions from the US National Intimate Partner and Sexual Violence Survey (Black et al., 2010). These questions ask about non-consensual condom removal, and forced pregnancy (including preventing the use of birth control), but, again, do not address forced abortion or forced continuation of pregnancy.
The second major conceptual flaw is a failure to consider the role of perpetrator intent in the wording of RCA survey questions (e.g. Black et al., 2010; Fay & Yee, 2020; Katz et al., 2017). The conceptual importance of perpetrator intent in defining RCA has been a topic of some debate among scholars over the last few years (Tarzia & Hegarty, 2021; Grace & Miller, 2023; Graham et al., 2023). In 2021, Tarzia and Hegarty argued that RCA should be understood as behaviours designed to deliberately interfere with someone’s reproductive capacity, rather than being used as a ‘catch-all’ for any behaviour with a reproductive outcome. For example, non-consensual condom removal (known colloquially as ‘stealthing’) can be undertaken for a variety of reasons, many of which have nothing to do with pregnancy (e.g. dislike of latex, reduced sensation, desire to dominate [Brodsky, 2017; Tarzia et al., 2020]). In these instances, stealthing is more accurately described as sexual assault rather than RCA. Similarly, perpetrating physical violence to intentionally cause a miscarriage is RCA; physical violence that incidentally causes a woman to miscarry is still physical violence.
These debates are not simply semantic exercise but have real implications for how we measure RCA (Tarzia & Hegarty, 2021). For example, studies where RCA is measured in an overly inclusive way (e.g. ‘Has anyone ever taken off a condom without your consent?’) tend to report prevalence rates that are far higher than studies where intent to impregnate is specified in the question wording (e.g. Katz et al., 2017). On the other hand, studies missing an entire subset of RCA behaviours are likely to dramatically under-estimate the prevalence. These measurement issues also cast serious doubt on the reliability of data on the risk factors for RCA, its associations with sociodemographic variables, and health impacts (Tarzia & Hegarty, 2021).
We recognise that victim/survivors may not always have insight into the motivation of the perpetrator, creating complexity around measuring intent in surveys. In arguing for intent to be a defining feature of RCA, we are not suggesting that research in this field ought to move away from survivor-centred measurement. Rather, we echo Tarzia and Hegarty (2021) in arguing that measurement instruments need to be able to distinguish – as much as is practicable – between RCA and other abusive behaviours such as sexual assault and intimate partner violence (IPV). We cannot hope to understand this complex phenomenon without robust data to guide policy and practice.
Prevalence of RCA
Conceptual issues aside, the available literature does suggest that RCA is a common experience for many women and girls globally (Grace, Alexander, et al., 2020; Grace & Anderson, 2018; Grace & Fleming, 2016; Grace & Miller, 2023; Wood et al., 2023). A study of RCA in community samples across 10 low-and-middle-income settings in Africa and India, for instance, reported past-year prevalence rates of between 3.1% and 20.3% for pregnancy-promoting behaviours alone (Wood et al., 2023). In the United States, national data suggest that around 4.6% of women had ever experienced a partner trying to get them pregnant when they did not want to be (Basile et al., 2019). In Australia, published national prevalence data are not yet available, although a recent commentary described preliminary findings from the Australian Study of Health and Relationships, suggesting that 5% of a representative sample of over 14,000 individuals had ever experienced at least one type of RCA (Whitehead, 2024). Other studies have explored RCA prevalence in clinical cohorts (Cheng et al., 2021; Galrao et al., 2024; Price et al., 2019; Sheeran et al., 2022) or in self-selecting community samples (Boxhall & Morgan, 2021; Hegarty et al., 2022). Sheeran et al. (2022), for example, found that 15% of pregnancy counselling clients across Australia had ever experienced RCA (6% pregnancy promoting, 7.5% pregnancy preventing, 2% both types), in most cases relating to the pregnancy they were seeking counselling for. On the other hand, Boxhall and Morgan (2021) found that 2.8% of a sample of 10,000 women in the community had experienced pregnancy-promoting behaviour in the previous 12 months during the COVID-19 pandemic.
Associations Between RCA and Sociodemographic and Health Variables
Findings on the sociodemographic and health variables associated with RCA are contradictory and challenging to interpret. For example, in Western contexts, some studies suggest that being younger (Fay & Yee, 2020; Grace, Decker, et al., 2020; Northridge et al., 2017) and non-partnered (Clark et al., 2014; Miller et al., 2014) increases the risk of RCA. However, as discussed earlier, these studies typically measure behaviours such as non-consensual condom removal without asking about the intent behind the behaviour. In other studies, where questions are more specific about the perpetrator’s intent to cause pregnancy, or where RCA victimisation was determined by practitioner consultation, no relationship between age or relationship status and RCA victimisation was found (Cheng et al., 2021; Hegarty et al., 2022; Levesque et al., 2023; Sheeran et al., 2022). There are also mixed findings on the relevance of cultural or racial minority status (Basile et al., 2019; Cheng et al., 2021; Holliday et al., 2017; Levesque et al., 2023; Sheeran et al., 2022), number of current or prior sexual partners (Katz et al., 2017), level of education (Levesque et al., 2023; Miller et al., 2014), and socioeconomic status (Cheng et al., 2021; Levesque et al., 2023). Although there are other possible explanations for these highly variable findings, it is likely that inconsistent measurement has been a major contributor, reinforcing the need for conceptually coherent data. Moreover, all of the extant research to date has examined RCA associations using cross-sectional data, which cannot illuminate the directionality of the relationship between variables.
Relationship Between RCA and IPV
Although the findings in relation to associations of RCA with other variables are mixed, there is consistent evidence that it is closely linked to experiences of IPV in relationships (Galrao et al., 2024; Grace & Anderson, 2018; Miller, Decker, et al., 2010; Miller, Jordan, et al., 2010). A recent study in Australia (Hegarty et al., 2022) suggested that 32.9% of a sample of more than 1,000 women who reported an experience of IPV also reported experiencing RCA in their lifetimes (17.1% forced to terminate a pregnancy and 15.3% forced into pregnancy against their wishes). These findings are also backed by in-depth qualitative research with RCA victim/survivors (McKenzie & Tarzia, 2024; Moulton et al., 2021; Tarzia & McKenzie, 2024; Wellington et al., 2023) and practitioners across the health and legal sectors (Douglas et al., 2020; Tarzia et al., 2019, 2022). Far less understood, however, are the nuances of the relationship between RCA and IPV. There is little information about which types of IPV are associated with RCA – particularly when RCA is measured comprehensively and accurately. Yet, this knowledge is a critical missing piece of the puzzle in terms of effective screening, identification, and response across the health and specialist sectors.
This article addresses these key gaps in our understanding of RCA by analysing data from a national longitudinal survey of women’s health. We focused on RCA perpetrated by a current or former intimate partner (as the most common context for RCA [Grace & Anderson, 2018; Silverman & Raj, 2014]). Our aim was to explore the:
Prevalence of RCA perpetrated by current or former partners amongst women aged 43 to 48 in a national Australian sample.
Sociodemographic and health factors from childhood and early adulthood associated with partner-perpetrated RCA by mid-life.
Associations between partner-perpetrated RCA and types of IPV.
Through this analysis, we hope to strengthen the available evidence by generating robust national prevalence estimates for the Australian context and conceptually sound data on the associations between partner-perpetrated RCA and sociodemographic and health variables earlier in life, as well as enhancing understanding of how RCA intersects with IPV.
Methods
Sample
This study used data from the Australian Longitudinal Study on Women’s Health (ALSWH), an ongoing longitudinal cohort study of Australian women that commenced in 1996. The ALSWH has collected data on over 14,000 women born from 1973 to 1978, measuring aspects of physical and mental health, use of health services, reproductive history, and sociodemographic variables. More information about the study can be found at alswh.org.au or by referring to the cohort profile (Dobson et al., 2015). The ALSWH has ongoing approval from the Human Research and Ethics Committees of [University] and [University]. All participants consented to joining the study and were free to withdraw from the study at any time without providing a reason.
The sample for this analysis was drawn from Wave 9 of the 1973 to 1978 cohort, which has previously been found to be broadly representative of Australian women (Dobson et al., 2015) with an over-representation of women with university qualifications. Wave 9 was chosen because it is the first to include questions on RCA. Data collection for Wave 9 began in June 2021 and was completed in October 2022, with most women aged 43 to 48 years at the time they completed their survey. Among the 6,875 women who completed Wave 9, 6,323 women indicated that they had ever had a partner or spouse and were eligible to answer the four questions on RCA; these 6,323 women were included in the subsequent analysis.
Measures
Reproductive Coercion and Abuse
RCA was measured by four questions developed by the research team and drawing on the extant RCA and broader violence against women literature (Grace & Anderson, 2018; Tarzia & Hegarty, 2021). The question stem asked, ‘Has a current or past partner ever. . .’ with the following four options:
Interfered with contraception in order to get you pregnant when you did not want to be? (e.g. refused to wear/removed a condom during sex, broke/poked holes in condom, threw away contraception, interfered with you accessing healthcare for contraception).
Pressured, threatened, or forced you to become pregnant?
Pressured, threatened, or forced you to terminate a pregnancy?
Used pressure, threats, or force to prevent you from terminating a pregnancy?
Participants could respond with ‘Yes’ or ‘No’ for each item. Although we acknowledge that RCA can also be perpetrated by parents, in-laws, and other family members, the context of these behaviours may be different from that of partner-perpetrated RCA. Moreover, given that the ALSWH contains questions about IPV and we were interested in exploring associations between RCA and other forms of violence in relationships, it made sense for us to focus on partner-perpetrated RCA.
Our questions were designed to capture the four main types of RCA rather than identifying specific behaviours. This was partially a space consideration within a very long and complex health survey, but also a reflection of our desire to capture the underlying dynamics of RCA. We acknowledge, for example, that other surveys may ask about the example behaviours listed in Question 1 as separate items. However, our view is that they are conceptually identical in terms of perpetrator motivation and therefore can be covered by a single broader question. Moreover, by including examples rather than specific behaviours, the item is more inclusive of different experiences.
Intimate Partner Violence
Violence by a partner was measured using the Community Composite Abuse Scale (CCAS). The CCAS has previously been validated in this cohort of women (Loxton et al., 2013) and consists of 28 items measuring emotional abuse (13 items), physical abuse (10 items), sexual abuse (1 item), and harassment (4 items). These four types of abuse were dichotomised to reflect whether the participant had ever experienced that type of abuse perpetrated by a partner.
Violence During Childhood
Violence during childhood was measured using the Adverse Childhood Experiences (ACEs) Questionnaire (Felitti et al., 1998) either at Wave 7 in 2015, or at Wave 8 in 2018 if the participant did not complete Wave 7. The questionnaire consisted of 21 items that measured seven different domains of adverse experiences during childhood. This analysis included three types of abuse measured by 8 items: psychological abuse (2 items), physical abuse (2 items), and sexual abuse (4 items). The degree of missing data was higher for the ACEs variables as not all women who were included in this study completed Wave 7 or Wave 8.
Sociodemographic Variables
Age was measured by calculating the participant’s age at the time of survey completion based on their date of birth. Country of birth was measured at Wave 1 and categorised as ‘Australia’, ‘Other English-speaking country’ (e.g. United States, Canada, England, Zimbabwe), and ‘non-English-speaking country’. Area of residence was calculated using the participant’s address using the Accessibility/Remoteness Index of Australia classification system and was categorised as ‘Major cities’, ‘Inner regional’, and ‘Outer regional/remote/very remote’ (Australian Bureau of Statistics, 2021). Highest qualification was categorised as ‘Year 12 or below’, ‘Certificate/diploma’, and ‘University’. Relationship status was categorised ‘Partnered’ and ‘Non-partnered’. Ability to manage on available income was categorised as ‘Not too bad/easy’, ‘Difficult sometimes’, and ‘Difficult always/impossible’. Alcohol consumption was calculated according to National Health and Medical Research Council guidelines (Pols & Hawks, 1992) and categorised as ‘Low risk drinker’, ‘Non-drinker/rarely drinks’, and ‘Risky/high risk drinker’. Smoking status was categorised as ‘Non-smoker’, ‘Ex-smoker’, and ‘Current smoker’.
Analysis
We estimated the prevalence of partner-perpetrated RCA amongst Australian women aged 43 to 48 years by reporting the prevalence observed in the sample for each of the four items, plus an overall item for women who indicated any of the four items.
Although ALSWH was broadly representative of the Australian population in 1996, the representativeness of the sample had reduced by the time the cohort was surveyed in 2021. In order to address concerns about the representativeness of the sample, we conducted a sensitivity analysis that calculated the same prevalences weighted for sample non-response, thereby accounting for the attrition that has occurred in the sample since 1996. The weighted prevalences were obtained using inverse probability of treatment weighting, accounting for attrition in the sample according to known predictors of sample non-response, including age, country of birth, area of residence, and highest qualification.
We used a Poisson regression model with robust standard errors to estimate risk ratios as an approximation to log-binomial regression (Zou, 2004) to describe the demographic and health factors associated with the experience of RCA. The model outcome was having ever experienced any of the four types of RCA measured in the survey (coded as 1 = yes, 0 = no), with the following factors included as model predictors: age, country of birth, area of residence, highest qualification, ability to manage on available income, relationship status, smoking status, and alcohol consumption. As the survey questions only asked participants if they had ever experienced RCA, not when they experienced RCA, it was not clear which time point should be used for the measurement of predictors. The conservative approach was to measure predictors at Wave 1 when the women were aged 18 to 23 years in 1996, such that the predictors were most likely to have preceded the RCA. However, we acknowledge the limitation that some women may have experienced RCA before the age of 18 to 23.
We also used a Poisson regression model with robust standard errors to examine the association between experiences of different types of violence and RCA. The model outcome was having ever experienced any of the four types of RCA measured in the survey (coded as 1 = Yes, 0 = No), and with the following factors included as model predictors: emotional abuse, physical abuse, sexual abuse, harassment (by a partner) or psychological abuse, physical abuse, or sexual abuse (during childhood). Each predictor was coded dichotomously as ‘Yes’ or ‘No’ for whether they had ever experienced that type of abuse. The CCAS and ACEs were not measured at Wave 1, so we instead examined the associations between having ever experienced each type of violence by Wave 9 and having ever experienced RCA by Wave 9. As such, the conclusions that could be drawn from this model were general in nature, and there was no attempt to estimate the direction of effect.
Results
Sample Characteristics
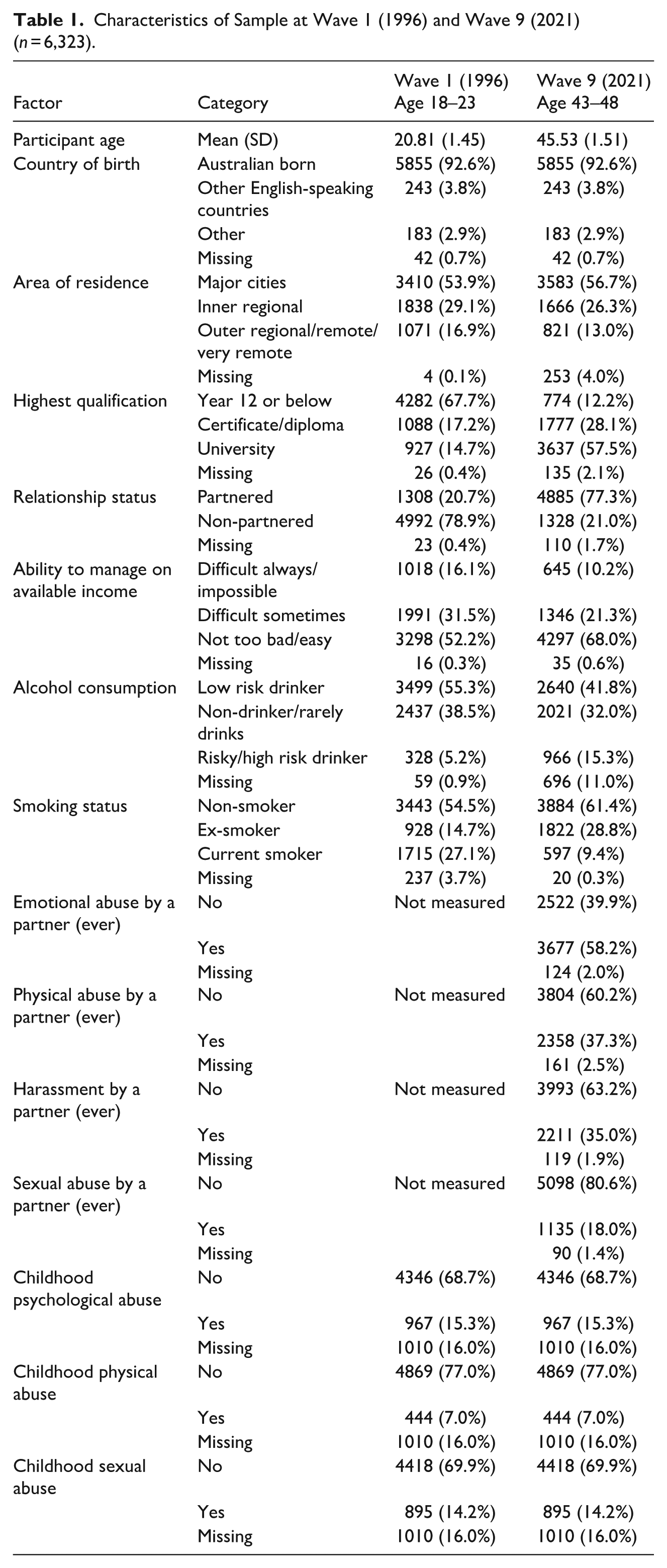
The majority of women in the sample were born in Australia (92.6%), and at age 43 to 48 years, lived in major cities (56.7%), had a university qualification (57.5%), were partnered (77.3%), reported low financial stress (68.0%), were low risk drinkers (41.8%) and non-smokers (61.4%) (Table 1). By age 43 to 48 years, approximately two-thirds of women in the sample had experienced emotional abuse by a partner (58.2%), two in five had experienced physical abuse by a partner (37.3%), and one in five had experienced sexual abuse by a partner (18.0%). During childhood, 15.3% of women in the sample had experienced psychological abuse, 7.0% had experienced physical abuse, and 14.2% had experienced sexual abuse.
Characteristics of Sample at Wave 1 (1996) and Wave 9 (2021) (n = 6,323).
Prevalence of Partner-Perpetrated RCA
Among the 6,323 women in the sample, 1.6% of women reported that a current or former partner had interfered with their contraception in order to get them pregnant when they did not want to be (n = 99), 1.1% of women reported that they had been pressured, threatened, or forced to become pregnant (n = 72), 2.6% of women reported that they had been pressured, threatened, or forced to terminate a pregnancy (n = 164), and 0.4% of women reported that they had been pressured, threatened, or forced to not terminate a pregnancy (n = 25). Overall, 4.5% of women reported one or more of the four RCA items (n = 283), with a 95% confidence interval of 4.0% to 5.0%. Among these 283 women, 78.8% reported one item (n = 223), 16.3% reported two items (n = 46), 3.9% reported three items (n = 11), and 1.1% reported four items (n = 3). The sensitivity analysis observed weighted prevalences that were within 0.1% of the unweighted prevalences.
Predictors of Partner-Perpetrated RCA
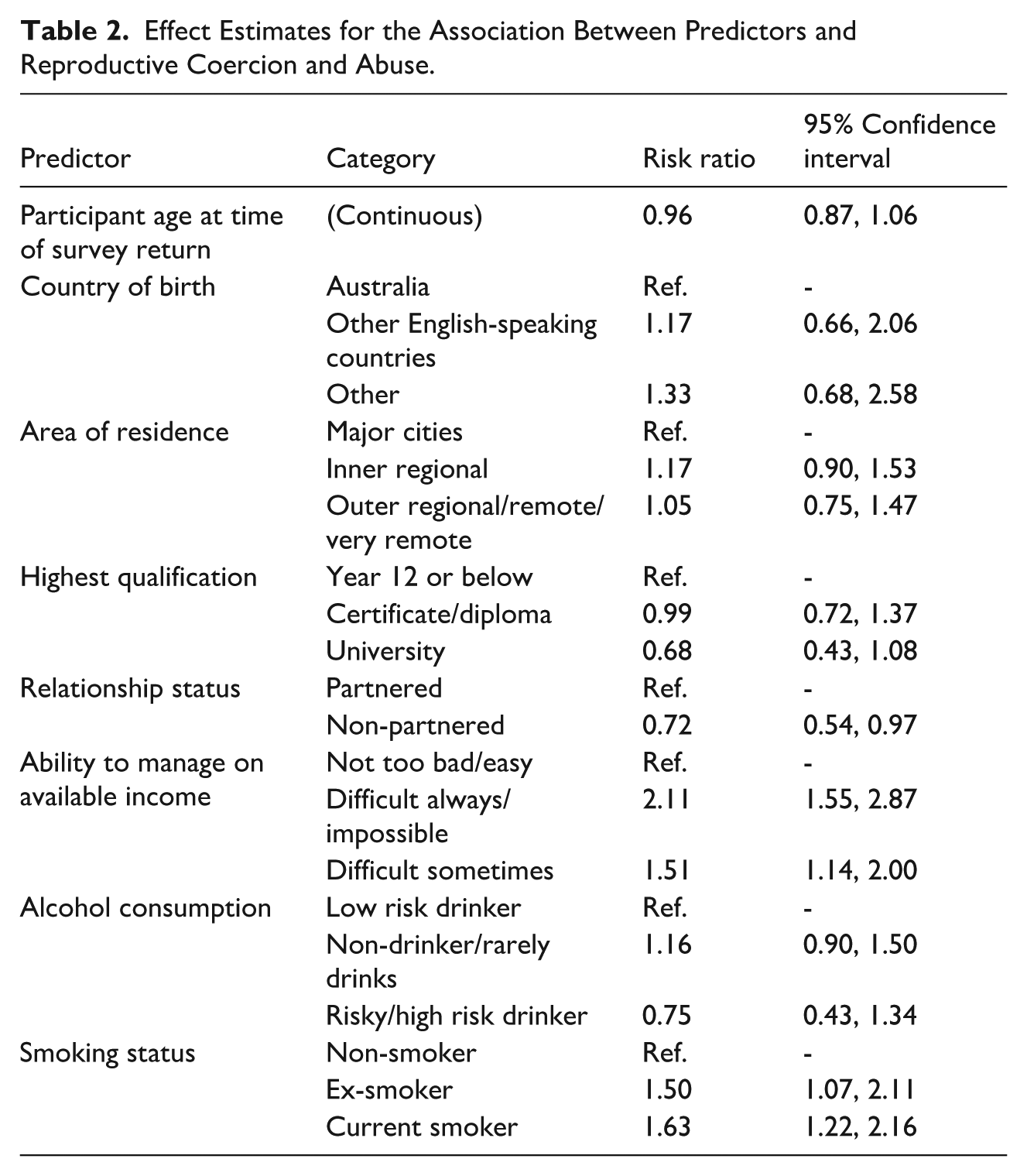
Women who reported their ability to manage on available income as ‘difficult always’ or ‘impossible’ when they were aged 18 to 23 years were twice as likely to experience RCA by the time they were aged 43 to 48 years, compared to women who reported their ability to manage on available income as ‘not too bad’ or ‘easy’ (RR = 2.11, 95% CI [1.55, 2.87]) (Table 2). Women who were current smokers when they were aged 18 to 23 years were 63% more likely to experience RCA by the time they were aged 43 to 48 years, compared to non-smokers (RR = 1.63, 95% CI [1.22, 2.16]). Similar associations were observed for ex-smokers (RR = 1.50, 95% CI [1.07, 2.11]). Women who were non-partnered when aged 18 to 23 years were 28% less likely to experience RCA by the time they were aged 43 to 48 years, compared to women who were partnered when aged 18 to 23 years (RR = 0.72, 95% CI [0.54, 0.97]). There was no evidence for an effect of age, country of birth, area of residence, highest qualification, or alcohol consumption measured at age 18 to 23 years on the risk of experiencing RCA by age 43 to 48 years.
Effect Estimates for the Association Between Predictors and Reproductive Coercion and Abuse.
The Relationship Between Partner-Perpetrated Reproductive Coercion and Other Forms Of Abuse
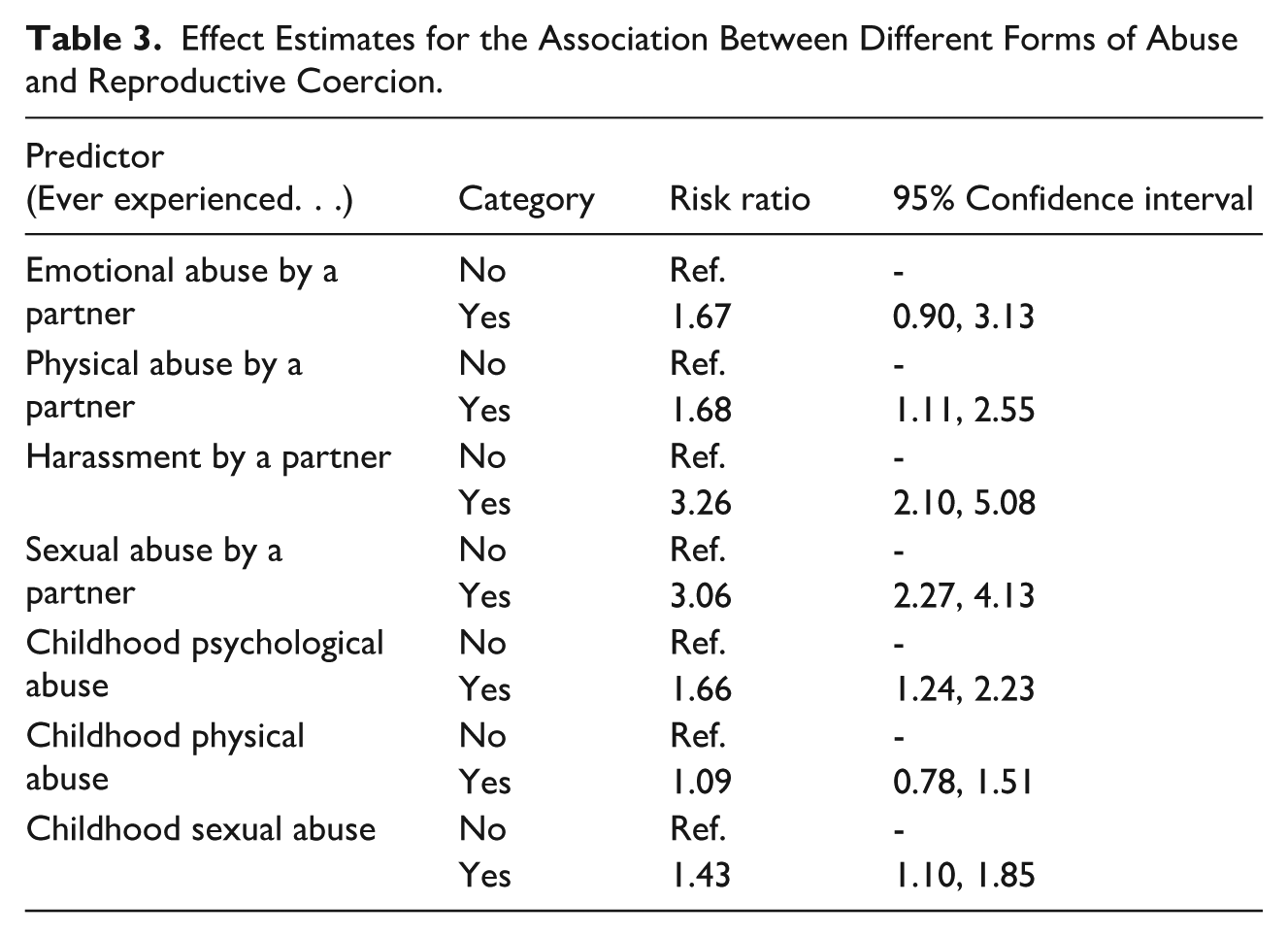
Women who had ever experienced physical abuse by a partner were 68% more likely to have experienced partner-perpetrated RCA (RR = 1.68, 95% CI [1.11, 2.55]), compared to women who had not experienced physical abuse by a partner (Table 3). Women who had experienced harassment by a partner or sexual abuse by a partner were approximately three times more likely to report partner-perpetrated RCA compared to women who had not experienced these types of abuse (RR = 3.26 and 3.06, respectively). Women who experienced psychological abuse during their childhood were 66% more likely to have experienced partner-perpetrated RCA (RR = 1.66, 95% CI [1.24, 2.23]), and women who had experienced sexual abuse during childhood were 43% more likely to have experienced partner-perpetrated RCA (RR = 1.43, 95% CI [1.10, 1.85]), compared to women who did not experience these types of abuse during childhood.
Effect Estimates for the Association Between Different Forms of Abuse and Reproductive Coercion.
No evidence of an association was observed between the domain of emotional abuse by a partner and partner-perpetrated RCA, which is inconsistent with much of the qualitative literature on RCA (Moulton et al., 2021; Tarzia & McKenzie, 2024; Wellington et al., 2023). To explore this further, we conducted a closer examination of the association by creating a similar model to that presented in Table 3, except for the overall indicator for emotional abuse by a partner was replaced by the individual items from the emotional abuse domain. We found that two individual items included in the emotional domain of the CCAS were associated with partner-perpetrated RCA, but all other individual items were not. The two items in the emotional domain that showed evidence of an association with partner-perpetrated RCA were ‘Kept me from medical care’ (RR = 1.71, 95% CI [1.24, 2.35]) and ‘Took my wallet and left me stranded’ (RR = 1.42, 95% CI [1.04, 1.94]).
Discussion
Main Findings
This study provided national Australian prevalence estimates for partner-perpetrated RCA among women aged 43 to 48 years. Our findings suggest that 4.5% of women in this age bracket may have experienced RCA perpetrated by a current or former partner in their lifetimes, with 2.4% reporting pregnancy promoting behaviours (being forced or pressured into getting pregnant [1.1%]; having contraception tampered with to cause pregnancy [1.6%]; or being prevented from having a termination [0.4%]), and 2.6% reporting pregnancy-preventing behaviour (being pressured, threatened or forced to terminate a pregnancy).
Additionally, we examined sociodemographic and health factors from young adulthood (age 18–23 years) that may be predictive of partner-perpetrated RCA by early midlife. We found evidence of associations between financial insecurity, smoking status, and being partnered at age 18 to 23 years and experiences of RCA victimisation by age 43 to 48 years. No relationship was found between age, country of birth, area of residence, highest qualification, or alcohol consumption measured at age 18 to 23 years on the risk of experiencing RCA by age 43 to 48 years.
We also found an association between experiences of physical IPV during a woman’s adult lifetime and reporting RCA by age 43 to 48 years. An even stronger association was found for sexual IPV and harassment, both of which were linked to a threefold increase in the likelihood of reporting RCA in early midlife. Childhood experiences of physical or sexual abuse were also predictive of lifetime RCA victimisation by age 43 to 48 years.
Interpretation
Overall, the RCA prevalence (4.5%) in our study was lower than rates reported in other high-income countries such as the United States (Black et al., 2010), despite the fact that we measured both pregnancy-promoting and pregnancy-preventing behaviours. We suggest that this is because the wording of our questions very specifically referred to the intent behind the behaviour, in order to ensure that we captured RCA rather than sexual assault (Tarzia & Hegarty, 2021; Tarzia et al., 2020). The prevalence in our study is also lower than that suggested by preliminary findings from the Australian Study of Health and Relationships (Whitehead, 2024), most likely due to the fact that their study measured RCA by any perpetrator (e.g. family members, health practitioners, religious figures), whereas we focused only on current or former intimate partners. To date, intimate partner RCA has been the main focus of qualitative research, and we are confident that our questions address the context and dynamics reported by victim/survivors in these studies (Tarzia & McKenzie, 2024; Wellington et al., 2023). Moreover, a strength of our study is that it covers the majority of the reproductive lifecycle by measuring prevalence at age 43 to 48 years. As a result, we suggest that the prevalence estimates reported in this article are likely to be some of the most accurate presented to date for RCA perpetrated by a partner, both in Australia and globally.
A further novel contribution of our study is that it explores variables from early adulthood that might be predictive of RCA victimisation later in life. Other research on RCA has utilised cross-sectional datasets, which do not provide information about the directionality of an association. Our study instead drew on a large longitudinal dataset with multiple data collection points over women’s adult lives. Although we cannot say with complete certainty that some women had not had an experience of RCA prior to age 18, it is reasonable to assume that for many of them, the RCA occurred sometime between Survey 1 in 1996 and Survey 9 in 2021. Further refinement of the survey items so that they ask about RCA experiences during a specific period will enable us to provide more accurate information about predictive variables in future analyses.
We found that women who reported significant financial stress at age 18 to 23 years were twice as likely to experience RCA by age 43 to 48 years compared to those who reported no difficulty managing on their current income. This makes sense in the context of existing qualitative RCA research, where both victim/survivors and service providers have described perpetrators using money as a tool to coerce women into a particular reproductive outcome (e.g. withholding money for an abortion or refusing to provide financial support for a child (Moulton et al., 2021; Tarzia et al., 2022; Tarzia & McKenzie, 2024; Wellington et al., 2023)). It also aligns with broader research on IPV, where associations between financial stress and increased risk of victimisation have also been reported (Ahmadabazi et al., 2020) (although there is some debate about the extent and nature of this relationship [Abramsky et al., 2011]). Research on contraceptive choice (Swan et al., 2022) has also found that financial stress is significantly associated with a lower likelihood of using one’s preferred contraceptive method. Being unable to afford effective, woman-led and less-detectable methods of contraception such as injectables, implants or IUDs may place women in a position where they are forced to rely on forms of birth control that are more easily tampered with or sabotaged by a perpetrator, such as the withdrawal method or condoms (Moulton et al., 2021; Tarzia & McKenzie, 2024).
Our findings also suggest that those who were current smokers or ex-smokers at 18 to 23 years were respectively 63% and 50% more likely to report RCA by age 43 to 48 compared to non-smokers. Whilst no prior studies have explored the relationship between smoking and RCA specifically, smoking has been recognised as a factor associated with IPV more broadly, particularly for pregnant women (Crane et al., 2013). Scholars have hypothesised that smoking may be a maladaptive response to the high levels of stress, anxiety, and trauma caused by IPV (Crane et al., 2013). Given the relationships found in our study between childhood experiences of abuse and violence and RCA by mid-life, it may be that women were using smoking as a way of coping with childhood trauma (Loxton et al., 2021).
Women who were partnered in early adulthood were 28% more likely to report RCA by early midlife compared to those who were non-partnered when aged 18 to 23 years. A similar phenomenon has been reported in the qualitative literature on intimate partner sexual violence (Tarzia, 2021), where women who entered into serious relationships very young – particularly with a partner who was significantly older – described themselves in hindsight as being vulnerable to unhealthy relationship dynamics, controlling behaviours from a partner, and normalisation of abusive behaviours (Tarzia, 2021). Related to this, the extant literature describes a relationship between experiences of childhood abuse (particularly sexual abuse) and earlier entry into serious cohabiting relationships (Friesen et al., 2010), as well as between child abuse and IPV in adulthood (Li et al., 2019). Indeed, amongst our sample, there was also a significant association between childhood experiences of psychological or sexual abuse and RCA victimisation at age 43 to 48. More research is needed to understand the mechanisms that underlie revictimisation in general, and RCA in the context of current or past child abuse in particular.
Although the literature is consistent in reporting associations between RCA and IPV (Grace & Anderson, 2018), our study provided a glimpse into the nuances of this relationship. Women who had ever experienced physical abuse by a partner were 68% more likely to have experienced RCA by age 43 to 48 years. An even stronger relationship was found between RCA and the intimate partner harassment domain of the CCAS (which covers behaviours such as stalking and harassment at work) and for sexual IPV, with women reporting these types of violence approximately three times more likely to also report RCA by early midlife. The relationship between RCA and sexual violence found in our study is highly coherent with qualitative research. Victim/survivors frequently describe being forced to have unprotected sex against their will in order to maximise the likelihood of pregnancy (Tarzia & McKenzie, 2024). Whilst we did not find evidence of an association between emotional abuse overall and RCA, two key items in the emotional abuse domain of the CCAS showed evidence of an association: ‘Kept me from medical care’ and ‘Took my wallet and left me stranded’. This aligns with our earlier finding about financial stress, suggesting once again that using money to control a victim/survivor is a key tactic of RCA perpetrators.
Strengths and Limitations
This study has several strengths, including a conceptually robust measurement of RCA, which included both pregnancy-promoting and pregnancy-preventing behaviours. Previous studies on RCA have not included such a robust definition, which has led to complications concerning how survey participants have interpreted the questions, and by extension, to varying prevalence rates. Furthermore, the large nationally representative sample of over 6,000 women analysed in this study lends credence to the estimated prevalence of partner-perpetrated RCA against women in Australia of 4.5%. A further strength of the study was the wide range of predictors that we were able to examine alongside other forms of abuse.
However, it must be noted that while the survey items used to measure RCA were a notable strength of this study, they have not yet been properly validated. The items were also limited in that they focused only on partner-perpetrated RCA and did not ask participants when the RCA experiences occurred. Knowing the timing of women’s RCA experiences would have allowed for a much closer examination of the risk factors associated with RCA and the directionality of these associations. The time period and age range included the majority of the reproductive life cycle, with women aged from 18 to 48 years, although the study did not represent women born earlier or later than this cohort. As such, there is the potential that the findings presented are a result of a generational effect and that the experience of RCA may be different for women outside this age group. It must also be noted that women in this sample are more likely to have a tertiary education and less likely to speak a language other than English at home than the general population. Finally, the frequency of women who experienced RCA who were born in countries other than Australia was particularly low (n = 21), and so the finding that country of birth did not show evidence of an effect should be interpreted with caution.
Implications
Although RCA is not as prevalent as other forms of intimate partner or sexual violence (Australian Bureau of Statistics, 2021–2022), our findings suggest that it may affect a considerable proportion of women in Australia. Indeed, it is almost as common as many well-recognised chronic health conditions in the 43 to 48-year-old cohort, such as diabetes, cardiac disease, and cancer (Harris et al., 2021). Despite this, RCA has received comparatively little attention to date in policy and practice, although the National Women’s Health Strategy 2020–2023 (Commonwealth of Australia, 2020) and the Senate Inquiry into Reproductive Healthcare (Commonwealth Government, 2023) both acknowledge that it is a critical emerging priority area. Considering the impacts of RCA on women’s health and well-being (Fay & Yee, 2020; Miller et al., 2014; Sheeran et al., 2024; Silverman et al., 2007), the lack of recognition of this insidious form of violence is concerning, and in need of urgent redress. As Australia grapples with a national conversation about prevention and responses to violence against women, it is vital that RCA be considered alongside IPV and sexual violence.
Our findings also shed light on potential risk factors that could be addressed early to reduce the likelihood of experiencing RCA later in life, as well as highlighting the relationship between RCA and other forms of IPV. These findings have important implications for risk assessment, identification, and response in health and specialist settings.
Recommendations
Given the links between RCA and financial stress, we suggest that providing free contraception for women in Australia (as has been done in Canada) may provide them with greater reproductive autonomy and reduce rates of RCA (Secura et al., 2014). Whilst there has been strong advocacy in this area, it has not yet occurred in the Australian context. Similarly, free abortion provision and enhanced access for women in rural, remote, or regional areas may reduce the ability of perpetrators to use the cost of abortion care as a coercive strategy (Thompson et al., 2021). Other initiatives to reduce financial stress connected with pregnancy could also be explored, including greater financial support for single mothers and subsidised childcare. Younger women (aged 18–23 years) who are smokers or who are already partnered could be provided with universal information about their reproductive rights, their options if they have an unplanned pregnancy, and what supports are available as a strategy to prevent future RCA.
Practitioners across the health, specialist, and legal sectors could consider asking women of reproductive age about RCA if controlling behaviours or sexual violence are disclosed. Physical or financial abuse could also be considered as possible red flags for RCA, as could a history of childhood psychological or sexual abuse. Although validated screening questions have not yet been developed, sensitive inquiry about a woman’s sense of reproductive autonomy in the relationship or her partner’s feelings about children may encourage disclosure. As with all forms of violence, asking only once may not be sufficient. Similarly, if a woman discloses RCA, it could prompt sensitive inquiry about other forms of violence given their close relationship.
Finally, we suggest that further research is needed in this area, both in Australia and globally. We urge those developing national prevalence surveys on violence against women to consider including questions on RCA that are conceptually robust and cover both pregnancy-preventing and pregnancy-promoting behaviours. The co-occurrence of different types of RCA would be another area for further exploration. Future studies should also consider including different perpetrator types in order to explore the different contexts of RCA and the overlaps with other forms of abuse.
Conclusion
This study explored the prevalence and predictors of RCA perpetrated by a partner in a nationally representative cohort of women aged 43 to 48 years. Our findings suggest that RCA may be as common as other well-recognised health conditions in this age group, despite RCA receiving little attention in policy and practice. This study also highlighted possible sociodemographic predictors of partner-perpetrated RCA by early midlife, including financial stress, smoking, and being partnered at a younger age. Finally, our analysis helps to unpack the nuance of the relationship between RCA and IPV, suggesting that sexual violence and ‘harassment’ (i.e. controlling behaviours) may be most strongly associated with RCA.
Footnotes
Acknowledgements
The research on which this paper is based was conducted as part of the Australian Longitudinal Study on Women’s Health by the University of Queensland and the University of Newcastle. We are grateful to the Australian Government Department of Health and Aged Care for funding and to the women who provided the survey data.
Ethical Considerations
The Australian Longitudinal Study on Women’s Health has ongoing approval from the Human Research and Ethics Committees of The University of Newcastle (EC00144) and The University of Queensland (EC00456/7). All participants consented to joining the study and are free to withdraw from the study at any time without providing a reason.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: The Australian Longitudinal Study on Women’s Health is funded by the Australian Government Department of Health and Aged Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the Australian Longitudinal Study on Women’s Health, but restrictions apply to the availability of these data, which were used for the current study and so are not publicly available. The data are only available to researchers who apply via the Australian Longitudinal Study on Women’s Health Data Access Committee. Further information about this process is available at ![]() .
.