
Abstract
Maltreatment at an early age is a well-established risk factor for the development of mental health issues in adulthood. An understanding of how the type and timing of such experiences confers vulnerability to psychopathologies among young adults, who have high rates of mental illness, is needed. The current study examined whether specific types of trauma exposures and their occurrence during sensitive developmental periods prior to the age of 18 (based on the Maltreatment and Abuse Chronology of Exposure), map onto symptoms of depression, anxiety, and suicidal ideation among Canadian university students (N = 238). Undergraduate students attending universities across Canada were recruited via snowball sampling to participate in an online study. Random forest regression with conditional inference trees revealed distinct associations with mood symptoms and suicidal thoughts when considering trauma type and timing of highest predictive importance. Specifically, non-verbal emotional abuse between ages 12 and 13 most strongly predicted depressive symptoms; sensitivity to emotional neglect from ages 12 to 15 was associated with suicidal ideation; and parental verbal abuse at age 15 was most predictive of anxiety symptoms. Moreover, resilience attenuated the relationship between non-verbal emotional abuse at age 12 and depressive symptoms, an effect not found for anxiety or suicidal ideation. These findings suggest that sensitive developmental periods and specific trauma types differentially associate with symptoms of anxiety, depression, and suicidal ideation. Identifying those at highest risk emphasizes the need for timely and accessible interventions, particularly for those with experiences of childhood maltreatment. Consideration should also be given to systemic barriers to mental health care, such as long waitlists for campus mental health services. Accessible trauma-informed interventions accounting for trauma type and timing could improve mental well-being among university students with histories of childhood maltreatment.
Introduction
Adverse experiences during childhood and early adolescence are strong risk factors for mental health disturbances in adulthood (Teicher et al., 2022). Childhood maltreatment, which encompasses exposure to abuse and neglect before the age of 18, is unfortunately common (Afifi et al., 2014). Nationally representative data show a significant rise in reports of childhood abuse among Canadians aged 18 to 27, ncreasing from 21.7% in 2012 to 26.8% in 2022 (Afifi et al., 2025). Within this demographic, university students also experience high rates of childhood trauma, wherein 32.6% of surveyed Canadian undergraduate students reported physical or sexual abuse, or experiences of bullying (Bhattarai et al., 2022). When considering adverse childhood experiences (ACEs) as defined by Felitti et al. (1998), over half of Canadian adults reported one or more ACEs before the age of 18 (Tough & McDonald, 2014). ACEs are strongly tied to stress-related disease in adulthood and account for an estimated 30% of mental health disorders worldwide (Kessler et al., 2010). Systematic review and meta-analytic evidence show childhood maltreatment is associated with a twofold increased risk of depression, anxiety disorders, and suicidality in adulthood (Sahle et al., 2022). Despite these findings, some individuals who experience adversity display relatively high levels of resilience, which may buffer some of the damaging effects of early-life trauma (Wingo et al., 2010).
A dose-response relationship has been widely reported, such that increases in ACEs correspond to greater risk of psychiatric disease in adulthood, including depressive and anxiety disorders (Naicker et al., 2021). Yet, vulnerability to psychiatric disorders can vary as a function of both type and timing, alongside the frequency and severity of maltreatment. For example, among a clinical population of German young adults, specific combinations of types of trauma, in addition to their timing, differentially associated with the severity of subsequent depressive and dissociative symptoms. PTSD, however, was correlated with total trauma severity (Schalinski et al., 2016). This is consistent with the view that neural development in early life is shaped, in part, by genetic and environmental interactions, during which discrete periods of increased neuroplasticity may render the brain susceptible to stressor-provoked changes (Zhu et al., 2021). Additionally, specific brain regions, including the hippocampus and amygdala appear to be especially affected by particular early-life adverse experiences (Luby et al., 2020). For instance, the type and timing of childhood maltreatment were associated with two distinct periods of enhanced neuroplasticity in corticolimbic regions among American young adults, aged 20 to 25 (Zhu et al., 2023). These findings highlight the importance of considering trauma type and timing on mental health disorders.
Several questionnaires have been developed to assess childhood maltreatment (Bethell et al., 2017). However, most of these instruments fail to consider the timing of exposure (Teicher & Parigger, 2015). Given that many types of trauma experiences tend to co-occur, it is difficult to isolate the impact of individual trauma types (Schimmenti, 2018). The Maltreatment and Abuse Chronology of Exposure (MACE) Scale was developed to address these gaps (Teicher & Parigger, 2015). In brief, the MACE assesses 10 types of maltreatment from ages 1 to 18, including emotional, physical, and sexual abuse; emotional and physical neglect; witnessing interparental violence or violence to siblings; and peer emotional abuse and physical bullying. Importantly, the MACE allows for the testing of hypotheses related to sensitive periods of development using random forest modeling, a machine-learning algorithm that is not subject to the confounds of collinearity. Earlier studies using this scale found that among young adults (ages 18–25), non-verbal emotional abuse at age 14 showed the strongest association with depression in men, whereas peer emotional abuse at the same age was associated with depression in women (Khan et al., 2015).
Notably, past year prevalence of depressive episodes is highest among young adults aged 18 to 25 in the United States (National Institute of Mental Health [NIMH], 2021). Within this age group, young women in Canada are twice as likely to meet the diagnostic criteria for mood and anxiety disorders (Statistics Canada, 2023). In fact, rates of depression and anxiety in young women have doubled from 2012 to 2022, highlighting them as a particularly vulnerable group (Statistics Canada, 2023). While early-life maltreatment serves as a transdiagnostic predictor of many mental illnesses, there are protective factors that serve to promote resiliency (McLaughlin et al., 2020). Yet, individuals with a history of early-life adversities tend to score lower on resiliency measures (Ward et al., 2020). Thus, it is important to identify critical windows of vulnerability to mental illnesses owing to specific trauma types among high-risk groups (Yang et al., 2023), and whether resilience (i.e., one’s perceived ability to adapt and bounce back from stress) can buffer these effects. This study used the MACE to examine how different forms of childhood trauma and the specific timing of these experiences (ages 0–18) map onto young adult depression and anxiety symptoms, and suicidal ideation. We also investigated whether self-reported resiliency would moderate these relationships. Based on previous studies using the MACE (Khan et al., 2015; Schalinski & Teicher, 2015), we expected that emotional abuse and neglect trauma types during adolescence would most closely align with symptoms of depression, anxiety, and suicidal ideation.
Method
Procedure
First- and second-year undergraduate university students (N = 238) were recruited from February to July of 2021 through snowball sampling using social media platforms and emails. Interested students completed an online eligibility questionnaire. Inclusion criteria comprised being 17–24 years old, currently residing in Ontario, and fluent in English. Note, the actual age range of those who participated was 18–23 years. Eligible participants were provided with a link to the study via email. Participants completed informed consent followed by online questionnaires (Qualtrics, Provo, UT, USA). These included demographics, depressive symptoms and suicidal ideation in the past 2 weeks, symptoms of anxiety in the past week, experiences of maltreatment in childhood, and resilience. Participants were debriefed with a document appearing at the end of the online survey and compensated for their participation. Ethics approval for the procedures in this study was provided by the Research Ethics Boards at Carleton University (REB # 111223) and the Royal Ottawa Mental Health Centre (REB # 2019024).
Measures
Demographics
Participants completed questions regarding their age, sex assigned at birth, gender identity, ethnicity, family income, and year of standing in university. Participants were also asked if they currently had a psychiatric disorder(s) diagnosis, or if they had in the past but no longer do (yes/no), and if so, they were asked to specify which disorder(s). For detailed participant characteristics, see Table S1.
Depression
Depressive symptoms in the past 2 weeks were assessed using the 21-item Beck Depression Inventory (BDI; Beck et al., 1961). All items identify a range from minimal (score of 0) to severe (score of 3) depressive symptoms and one item that assesses suicidal ideation. Scores for each item were summed to inform a total depression score (α = .90), with higher scores reflecting greater depressive symptom severity.
Suicidal Ideation
Suicidal thoughts were measured using item 9 from the BDI scale. This item assessed the extent of suicidal ideation in the past 2 weeks. Responses were then recoded into a binary variable, where 0 = no suicidal ideation, and 1 = scores greater than or equal to 1, indicating any thoughts of self-harm or suicidal ideation.
Anxiety
Anxiety symptoms in the past week were assessed using the 21-item Beck Anxiety Inventory (BAI; Beck et al., 1988). Items in this scale are scored from 0 (low) to 3 (high). Scores for each item were summed for a single measure of total anxiety (α = .90), with higher scores indicating greater severity of anxiety symptoms.
Resilience
Resilience was assessed using the 6-item Brief Resilience Scale (Smith et al., 2008). Questions include those such as ‘It does not take me long to recover from a stressful event’ and ‘I tend to take a long time to get over setbacks in my life’. Participants indicated their level of agreement ranging from 1 to 5 (1 = strongly disagree, to 5 = strongly agree). The mean of all 6 items reflected the total resilience score (α = .87).
Trauma
Exposure to maltreatment prior to the age of 18 was assessed using the 52-item MACE scale (Teicher & Parigger, 2015). The MACE assesses severity of exposure to 10 different maltreatment types, including: emotional neglect, non-verbal emotional abuse, parental physical maltreatment, parental verbal abuse, peer emotional abuse, peer physical bullying, physical neglect, sexual abuse, witnessing interparental violence, and witnessing violence to siblings, specifying each year in which it occurred throughout childhood. Each maltreatment type is provided a severity score, which ranges from 0 to 10. The scale provides a multiplicity score ranging from 0 to 10 indicating the number of different trauma types experienced before the age of 18. A duration score indicates the number of years with exposure to at least one type of maltreatment from ages 0 to 18. Total severity of exposure was quantified by summing the incidence of exposure to any type of trauma before the age of 18, with scores ranging from 0 to 100.
Statistical Analyses
Statistical analyses were performed using RStudio version 2023.06.1+524 (Posit Software, Boston, MA, USA) and SPSS for Mac OS version 29 (SPSS Science, Chicago, IL, USA). Data screening and cleaning were conducted to detect out-of-range scores. Validity and data quality checks included minimum completion time (30 min), consistency in responses to similar items across questionnaires, and use of student email addresses. There were no instances of missing data. Independent samples t-tests were used to assess differences in mental health symptoms. Note that there were too few individuals who reported their gender identity as other than men/women (n = 17). Therefore, these individuals were excluded from analyses where gender appears as a covariate (n = 221). Separate multiple linear regression analyses were conducted to assess total severity and number of different trauma types experienced as predictors of mental health symptoms, with gender, age, and ethnicity included in these models. For a comprehensive assessment of general linear model assumption testing, see Supplemental Extended Results. Separate binary logistic regression models were used to assess total severity and number of different trauma types experienced as predictors of suicidal ideation, with gender, age, and ethnicity included in these models. Moderation analyses with resilience scores were conducted using PROCESS (Hayes, 2017) for depression, anxiety, and suicidal ideation. Effects were considered significant at p < .05 (two-tailed).
Random Forest Regression
Sensitive periods of development were identified using random forest regression with conditional inference trees. In brief, random forest modeling is a machine-learning algorithm that generates predictions by aggregating the outputs of multiple decision trees, each constructed from random subsets of the data and predictor variables. This methodology enhances predictive accuracy and robustness by mitigating the risk of overfitting associated with individual trees. The model yields measures of variable importance, indicating the relative contribution of each feature to the model’s decision-making process (Grömping, 2009). In essence, it distinguishes important predictors from a large set of possible predictors (Schalinski et al., 2019).
In this instance, predictor variables included the 10 subtypes of maltreatment covered in the MACE scale for each year from age 1 to 18, as well as total severity, multiplicity, and duration of MACE scores. For analyses using the type and timing model, gender did not emerge as a predictor with significant predictive importance, and therefore, models were re-run without gender. It should be noted, however, that this may be due, in part, to a relatively low sample size of men (n = 44). Given the much larger sample size of women (n = 177), the type and timing models were re-run using women only, and while the overarching results are presented in this manuscript, detailed results from these models can be found in the Supplemental Material.
Results
Participant Characteristics
The current study comprised 238 first- and second-year undergraduate students (M = 19.0 years, SD = 1.0, Range = 18–23 years). The majority of participants identified as women (74.4%; n = 177), and participants were of diverse ethnic backgrounds; see Table S1 for comprehensive participant demographics.
Prevalence of Trauma and Mental Health Disorders Among University Students
Childhood maltreatment and abuse experiences before the age of 18 were highly prevalent, with 67.9% (n = 161) of students reporting at least one type of maltreatment or neglect. Of those reporting maltreatment, 60.9% of students experienced between 1 and 5 forms of childhood maltreatment, and a smaller subset of the sample, 7.1%, reported experiencing greater exposure (6–9 forms) to childhood maltreatment. Moreover, approximately one-third of participants (35.7%, n = 85) reported having a current mental health disorder diagnosis. For details on specific types of disorders reported, see Table S1.
Trauma and Severity of Depression and Anxiety Symptoms
Separate multiple linear regression models were conducted to examine the associations of total severity and the number of trauma types experienced with symptoms of depression and anxiety, adjusting for gender, age, and ethnicity. For total trauma severity, the overall models for depression (R2 = .19) and anxiety (R2 = .15) were significant (Table S2). On average, every 1-point increase in total trauma severity was associated with a .30-point increase in depressive symptoms (b = 0.30, SE = 0.05, p = .002, 95% CI [0.20, 0.40]) and a 0.22-point increase in symptoms of anxiety (b = 0.22, SE = 0.05, p = .002, 95% CI [0.12, 0.35]). Gender was a significant predictor in both models, with women reporting significantly greater depressive (b = 3.38, SE = 1.50, p = .03, 95% CI [0.35, 6.55]) and anxiety symptom severity (b = 4.95, SE = 0.05, p = .005, 95% CI [1.42, 8.30]) than men. Ethnicity was not significantly associated with either outcome (p > .05), and age was only significantly associated with symptoms of anxiety (b = −1.43, SE = 0.71, p = .04, 95% CI [−2.73, −0.16]).
Similarly, for the number of trauma types experienced, the overall models for both depression (R2 = .15) and anxiety (R2 = .14) were significant (Table S2). On average, every additional type of trauma encountered (i.e., a 1-point increase in the number of trauma types experienced) was associated with a 1.79-point increase in depressive symptom severity (b = 1.79, SE = 0.33, p = .002, 95% CI [1.10, 2.55]), and a 1.46-point increase in symptoms of anxiety (b = 1.46, SE = 0.35, p = .002, 95% CI [0.77, 2.27]). Gender was a significant predictor in both models, with women reporting significantly greater depressive (b = 4.33, SE = 1.57, p = .01, 95% CI [0.77, 7.76]) and anxiety symptom severity (b = 5.60, SE = 1.73, p = .005, 95% CI [1.88, 9.28]) than men. Ethnicity was not significantly associated with either outcome (ps > .05), and age was only significantly associated with anxiety (b = −1.55, SE = 0.67, p = .03, 95% CI [−2.96, −0.42]; see Figure 1).
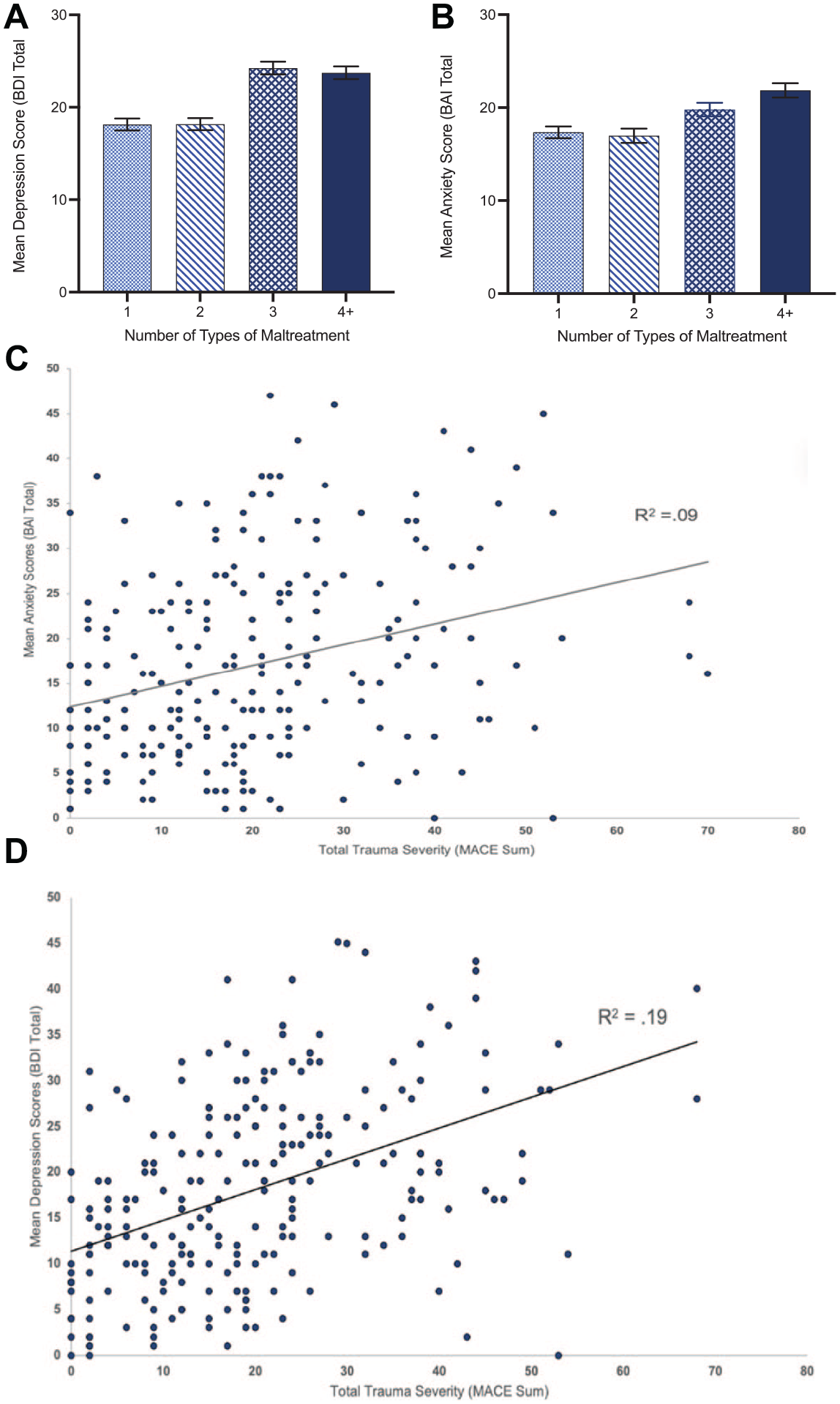
Total severity and number of different types of childhood maltreatment on symptoms of depression and anxiety.
Trauma and Suicidal Ideation
Separate multiple binary logistic regression models were used to assess relationships between total trauma severity and the number of trauma types with suicidal ideation, adjusting for gender, age, and ethnicity. For total trauma severity, the overall model was significant (χ2(14, n = 221) = 29.1, p = .01) and explained 17% of the variance in suicidal ideation (Nagelkerke R2). On average, every 1-point increase in total trauma severity was associated with a 1.04-times increase in the odds of suicidal ideation (b = 0.04, SE = 0.07, Wald’s χ2 = 11.13, p = .01, OR = 1.04, 95% CI [0.002, 0.10]). Similarly, for the number of trauma types experienced, the overall model was significant (χ2(14, n = 221) = 25.4, p = .03) and accounted for 15% of the variance in suicidal ideation. On average, every additional type of trauma encountered was associated with a 1.26-times increase in the odds of suicidal ideation (b = 0.23, SE = 0.10, Wald’s χ2 = 8.04, p = .009, OR = 1.26, 95% CI [0.04, 0.59]). Gender was significant in both the total trauma severity (b = 0.87, SE = 0.47, Wald’s χ2 = 4.74, p = .04, OR = 2.39, 95% CI [1.19, 5.53]), and number of trauma types experienced (b = 0.99, SE = 0.44, Wald’s χ2 = 6.34, p = .007, OR = 2.70, 95% CI [0.21, 2.01]) models, such that women had significantly increased odds of suicidal ideation compared to men. Age and ethnicity were not significant in either model (ps > .05). For a full model summary, see Table S3.
Type and Timing of Childhood Adversities for Depressive Symptoms
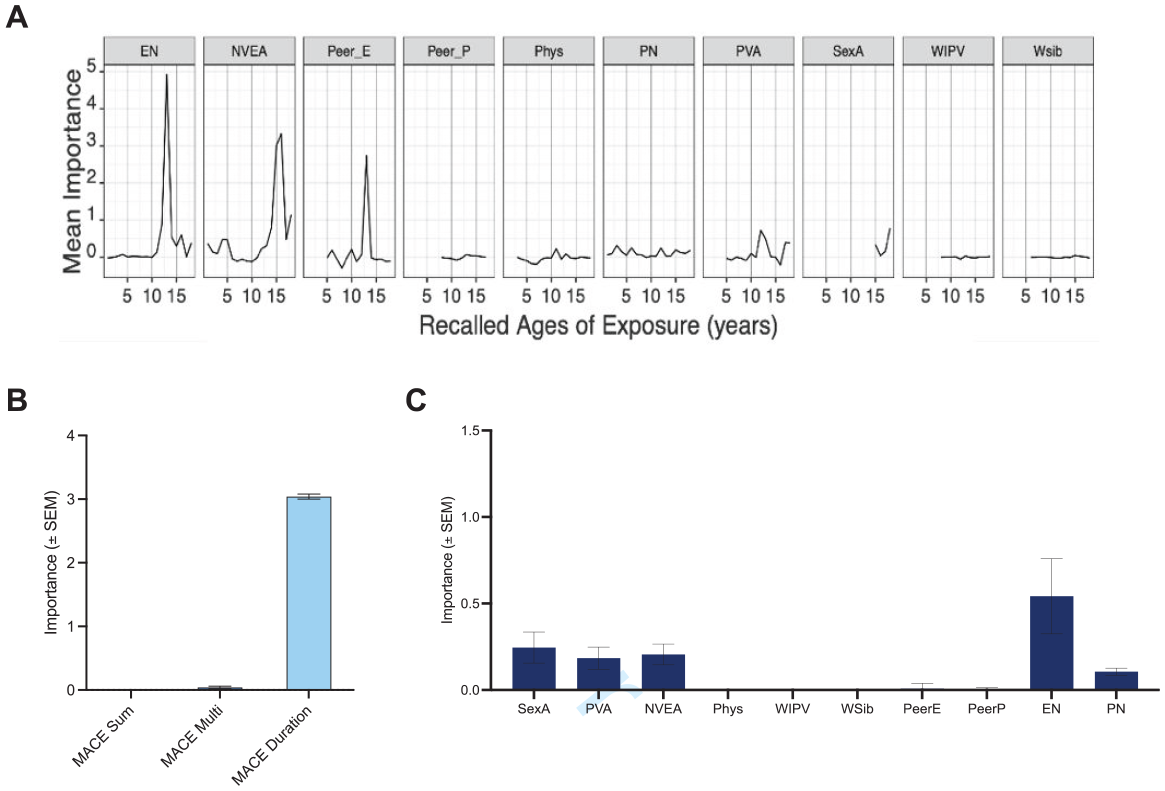
The “Sensitivity by Type and Timing for Depressive Symptoms” analysis showed trauma exposure during adolescence (ages 12–18) was associated with greater depressive symptom severity. Specifically, non-verbal emotional abuse at age 12 had the highest predictive importance (Table 1), although non-verbal emotional abuse experienced at age 13 was also a significant predictor of depressive symptoms. Moreover, parental verbal abuse at ages 15 and 18, as well as emotional neglect at age 15, significantly predicted depressive symptoms (Table 1). However, no time points for the remaining trauma subtypes predicted depressive symptoms (ps = .08–1.00). Taken together, this model revealed a broad susceptibility to emotional trauma, with periods of particular sensitivity occurring at ages 12, 13, 15, and 18 (Figure 2A). The total severity of exposure to childhood adversities was a strong predictor of severity of depressive symptoms (predictive importance: M = 3.23, SD = 0.06), while number of different types of childhood maltreatment experienced and the number of years with exposure to at least one type of maltreatment were not (ps = 1.00; Figure 2B). However, comparing the importance of total trauma severity with predictors from the ‘Sensitivity by Type and Timing for Depressive Symptoms’ model, the predictive importance of non-verbal emotional abuse at age 12 was greater than that of total trauma severity (Table 1). When examining the mean importance across trauma types regardless of time, non-verbal emotional abuse had the highest importance (Figure 2C).
Results for Significant Predictors of Depressive Symptoms in Random Forest Regression.
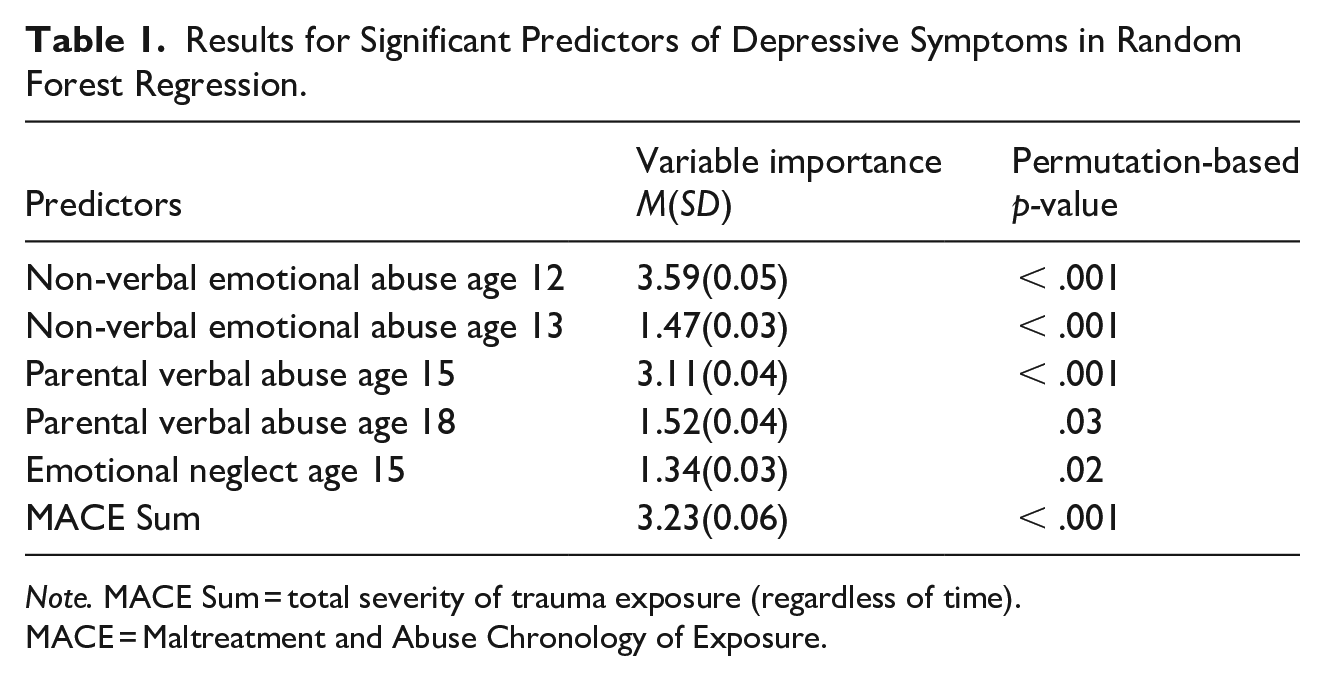
Note. MACE Sum = total severity of trauma exposure (regardless of time). MACE = Maltreatment and Abuse Chronology of Exposure.
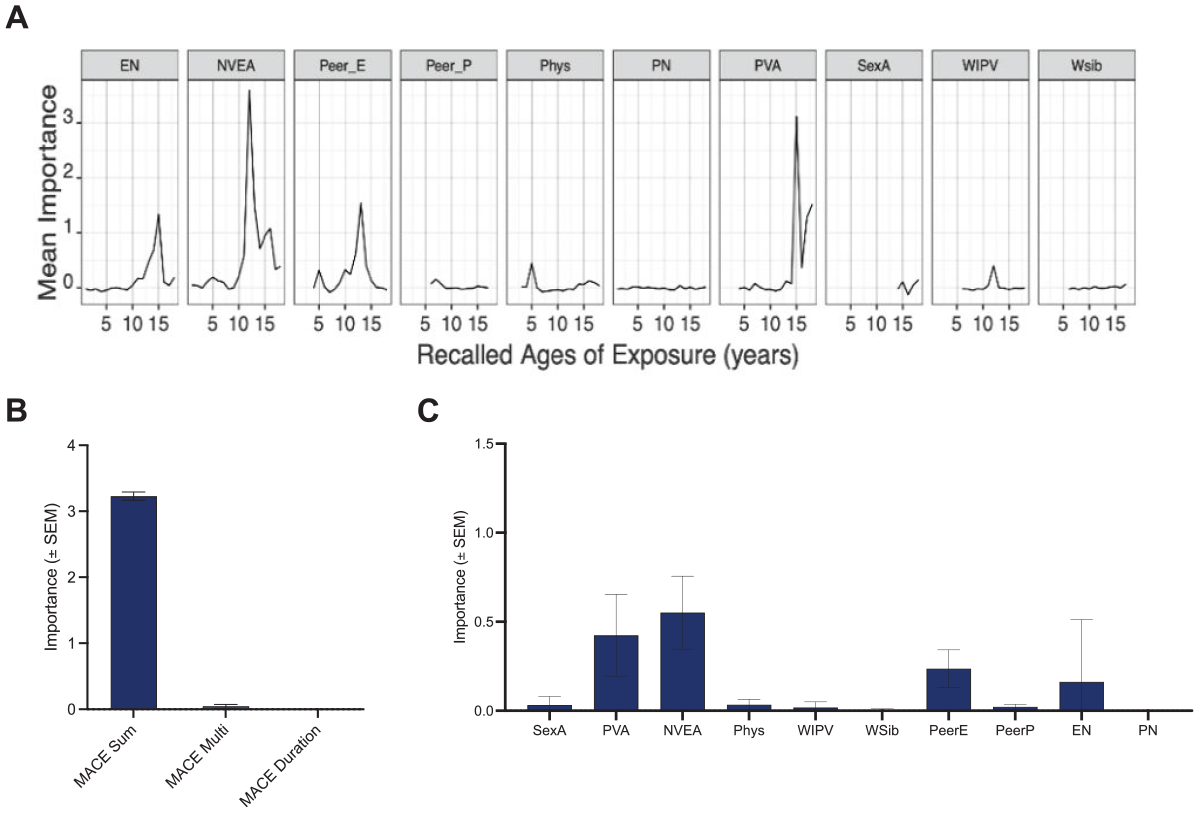
Random forest regression modeling of childhood maltreatment predicting depressive symptoms.
This model was also re-run using women only, wherein non-verbal emotional abuse was no longer a significant predictor; however, parental verbal abuse at age 15 and emotional neglect at age 15 remained significant. Moreover, a high predictive importance of witnessing interparental violence at age 12 was identified, which was not found in the full sample (Table S4, Figure S1).
Type and Timing of Childhood Adversities for Suicidal Ideation
The ‘Sensitivity by Type and Timing for Suicidal Ideation’ analysis revealed significant predictive importance for emotional neglect throughout ages 12 to 15, with the most pronounced mean importance occurring at age 13 (Table 2). No other trauma types predicted suicidal ideation (ps = .17–1.00). This highlights a period of type and timing specific sensitivity for symptoms of suicidal ideation, with the major sensitive period for emotional neglect peaking at ages 12 to 15 (Figure 3A). Duration of trauma exposure was a significant predictor of suicidal ideation (p < .001), while total trauma severity and number of trauma types experienced were not (ps = 1.00; Figure 3B). However, the predictive importance of emotional neglect at age 13 was greater than that of duration of trauma exposure (Table 2). Additionally, when comparing mean importance across trauma type, regardless of timing, emotional neglect had the greatest importance (Figure 3C). Note that this model was re-run using women only, but all variables with significant predictive importance remained the same (Table S5; Figure S2).
Results for Significant Predictors of Suicidal Ideation in Random Forest Regression.
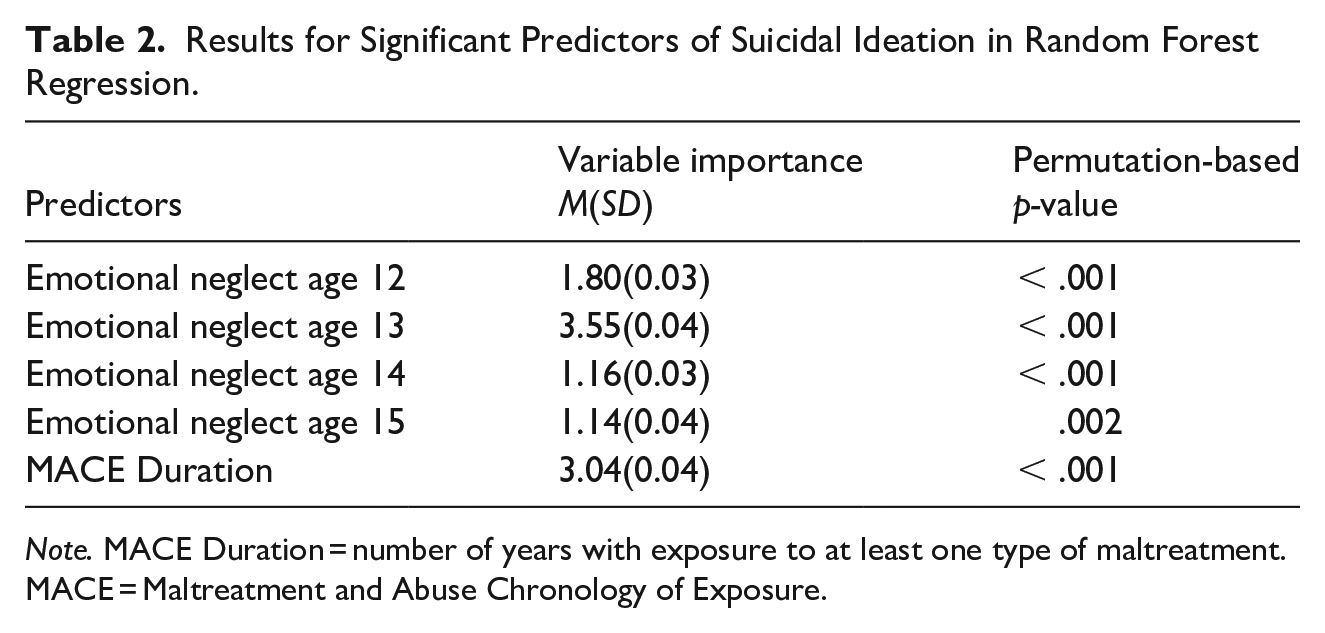
Note. MACE Duration = number of years with exposure to at least one type of maltreatment. MACE = Maltreatment and Abuse Chronology of Exposure.
Random forest regression modeling of childhood maltreatment predicting suicidal ideation.
Type and Timing of Childhood Adversities for Anxiety Symptoms
The ‘Sensitivity by Type and Timing for Anxiety Symptoms’ analysis identified that parental verbal abuse at age 15 had the highest predictive importance, p < .001. In addition, non-verbal emotional abuse at age 12 had a significant predictive importance, p < .001 for anxiety symptoms. No other trauma subtypes were found to be significant in random forest regression (ps = 1.00; Figure 4A). Total trauma severity, number of trauma types, and duration of trauma exposure were not significant predictors of anxiety symptom severity (ps = .60–1.00; Figure 4B). When examining mean importance across type, regardless of timing, parental verbal abuse was found to have the highest importance (Figure 4C). Upon re-running this model with women only, all variables with significant predictive importance remained the same (Table S6, Figure S3).
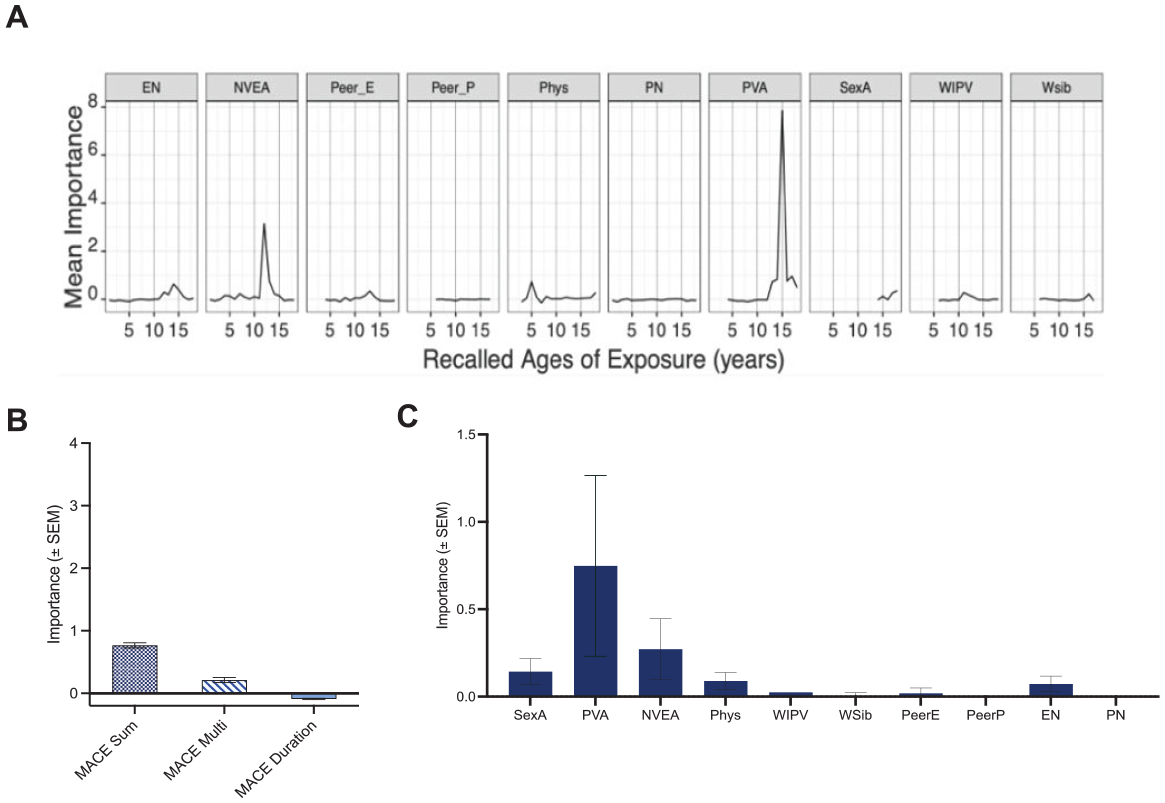
Random forest regression modeling of childhood maltreatment predicting anxiety symptoms.
The Moderating Role of Resilience
Moderation analyses were conducted to determine whether the relationship between total trauma severity, as well as sensitive periods (identified above), and symptoms of depression, anxiety, and suicidal ideation would be buffered by greater resilience. First, no significant interaction existed between total trauma severity and resilience in relation to depressive symptoms, ΔR2 = .006, F(1, 233) = 2.36, p = .12. To assess sensitive periods for depression, non-verbal emotional abuse at age 12 was used given that it showed the highest predictive importance in the ‘Sensitivity by Type and Timing for Depressive Symptoms’ analysis. The overall model for this analysis was significant, p < .001, and a significant interaction existed between non-verbal emotional abuse at age 12 and resilience in relation to depressive symptoms, ΔR2 = .03, F(1, 234) = 14.96, p < .001. Interestingly, the relation was larger for those with high levels of resilience, B = 3.05, 95% CI [2.31, 3.79], p < .001, than low resilience, B = 0.79, 95% CI [0.26, 1.56], p = .04. As seen in Figure 5, regardless of non-verbal emotional abuse, those with low levels of resilience had much greater depressive symptom severity than those with high resilience, and non-verbal emotional abuse at age 12 was associated with increased severity of depressive symptoms across all individuals, even among highly resilient individuals.
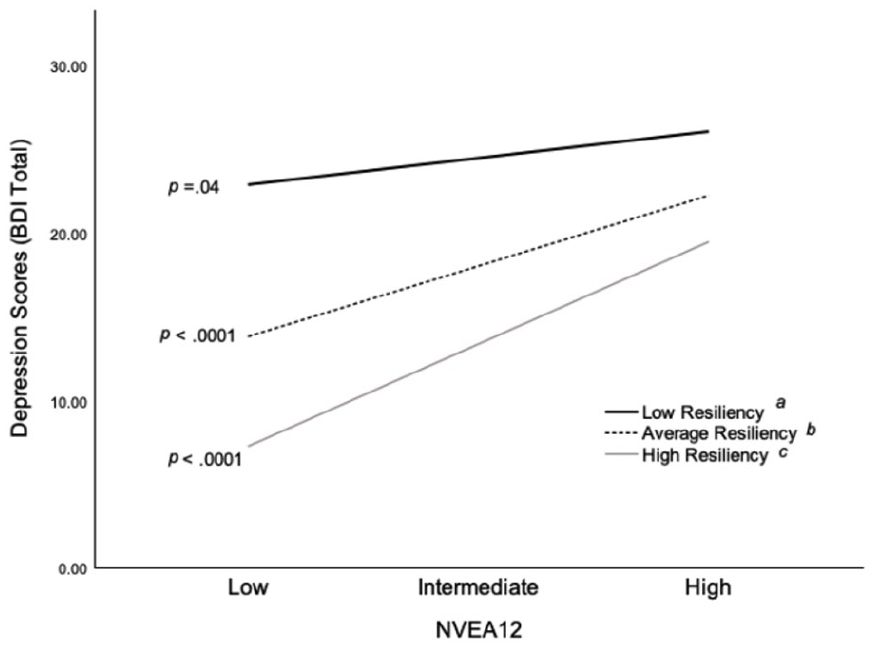
Resilience moderates the relationship between non-verbal emotional abuse at age 12 and depression symptoms.
Similar to the analyses for depression, we assessed whether resilience would buffer the effects of parental verbal abuse at age 15, as it showed the highest predictive importance for anxiety symptoms. There was no significant interaction between the extent of parental verbal abuse at age 15 and resilience in relation to anxiety symptoms, ΔR2 = .009, F(1, 234) = 2.63, p = .11. We then examined whether resilience would buffer the effects of emotional neglect at age 13, given that it showed the highest predictive importance for suicidal ideation. However, there was no significant interaction between extent of emotional neglect at age 13 and resilience in relation to suicidal ideation (b = 0.05, SE = 0.12, p = .69, 95% CI [−0.20, 0.25]).
Discussion
The present study examined the differential importance of trauma type and timing on current symptoms of depression, suicidality, and anxiety in a sample of Canadian university students, and the moderating role of resilience in these relationships. Specific types of traumas experienced at certain ages had greater predictive strength for symptom development than did the global stress load measures of total trauma severity, number of trauma types experienced, and duration of trauma exposure. Notably, non-verbal emotional abuse, emotional neglect, and parental verbal abuse during adolescence were most closely aligned with psychological disturbances. While this finding is in line with previous reports indicating trauma experiences during adolescence are particularly important predictors of depression, others show that childhood maltreatment occurring in middle childhood (i.e., 6–13 years) was the strongest predictor for depression, followed by adolescence (Li et al., 2023). It is likely that beyond the age of exposure, the age of the population assessed and the timing since the trauma occurred are important considerations. Furthermore, individual resiliency moderated the relationship between the variable with the highest predictive importance (non-verbal emotional abuse at age 12) and depression symptom severity, while no such effects were found for anxiety symptoms or suicidal ideation.
In the current investigation, traumatic events in early adolescence, largely between the ages of 12 to 15, had the greatest predictive importance for depression, anxiety, and suicidal ideation. These findings are consistent with reports that trauma experienced throughout the adolescent period was a strong predictor of neuropsychiatric disturbances (Jaye Capretto, 2020; Khan et al., 2015). Elevated neuroplasticity during adolescence may increase vulnerability to stress-related disturbances linked to the development of psychological disorders (Rapee et al., 2019; Romeo & McEwen, 2006). Neurobiological alterations, particularly those occurring in corticolimbic regions such as excessive synaptic pruning, may impair the development of emotional regulation, social connections, and memory formation (Birnie & Baram, 2025). These changes may shape how an individual processes past trauma experiences and copes with new stressors (Gruhn & Compas, 2020).
Our results showed that emotional forms of maltreatment and neglect were most predictive of all mental health symptoms assessed. In addition to non-verbal emotional abuse, depression and anxiety symptoms were also predicted by parental verbal abuse. Emotional neglect was predictive of suicidal ideation and characterized as a lack of parental availability, and not feeling loved, important, or supported by the family (Teicher & Parigger, 2015). Indeed, emotional maltreatment has been identified as one of the most frequent and impactful forms of trauma associated with symptoms of depression and anxiety (LeMoult et al., 2020). Specifically, others report that emotional neglect at age 12 and parental non-verbal emotional abuse between the ages 13 and 14 were the most important predictors of major depression in males, while peer emotional abuse at age 14 had the highest predictive importance among females (Khan et al., 2015). It appears as though traumatic experiences involving emotional disturbances in early adolescence may be important indicators of future psychopathologies.
Although we expected experiences of sexual and physical abuse to be associated with psychopathology, as shown in earlier reports (Li et al., 2016), neither were found to have significant predictive importance for any of the mental health symptoms of interest. However, previous literature has identified that emotional abuse or neglect is a better predictor of depression and anxiety when compared to physical or sexual abuse (McKay et al., 2021). It may be the case that the extent to which our sample was exposed to these types of traumas was limited, and therefore, their relations to mental health symptoms were not observed. In fact, trauma types and timing experienced by less than 5% of the sample were excluded as predictors from their respective random forest models. Therefore, in our sample, reports of sexual abuse before the age of 14 were excluded from type- and timing-based analyses as they were seldom reported. Despite this, our data and others (Dye, 2020) highlight that prevalent forms of maltreatment that may be perceived as subtle or inconsequential, such as emotional abuse or neglect, can have potent and enduring impacts on mental well-being.
The results of the current study indicated that resiliency moderates the relationship between non-verbal emotional abuse at age 12 and symptoms of depression. Specifically, resilience had a large buffering effect at low levels of trauma on depressive symptom severity, whereas this was not apparent in relation to severe trauma. This outcome is consistent with the impact of chronic stressors on the capacity of biological systems to adapt (allostatic overload) so that pathology is more likely to occur. However, resiliency did not moderate the relationship between total trauma severity and depression. It may be that the protective effect of resiliency depends on trauma subtype and time(s) of exposure. Indeed, trauma type and frequency of trauma exposure may influence not only an individual’s level of resilience in the future but also how effective that resilience is as a protective factor (Gee, 2021). Moreover, resiliency did not attenuate the relationship between trauma severity and suicidal ideation or anxiety symptoms. This is congruent with reports that resilience was not protective for those experiencing suicidal ideation (Tripp et al., 2022), or anxiety symptoms (Anyan & Hjemdal, 2016). This discrepancy warrants further investigation, with consideration of sample characteristics and definitions of resiliency.
In the young adult sample, when considering women alone, the established sensitive periods and types of trauma remained the same for suicidal ideation and anxiety symptoms as in the overall sample. However, witnessing interparental violence had significant predictive importance in relation to depression, which was not found when men were included in the model. Going forward, this highlights the importance of considering gender differences in sensitive periods to better understand vulnerability to psychopathology.
The present study is not without limitations. Key among these are the reliance on self-report data, which is subject to reporting and memory biases. While these findings provide valuable insights, generalizability to more diverse samples, communities, or clinical populations are limited. Additionally, the sample size was too small to conduct random forest models in men, as the current study comprised approximately 80% women. While our sample was fairly ethnically diverse, we did not have large enough sample sizes to consider trauma type and timing analyses within each group. Given that random forest modeling only includes ages and types of maltreatment experienced by at least 5% of the sample, the impacts of infrequent types of trauma were not considered. While the total sample size was relatively low for random forest regression, it was comparable to other studies using random forest analyses (Schalinski et al., 2016; Sicorello et al., 2021).
Conclusion
The current study identified early adolescence as a critical window of vulnerability to specific types of emotional trauma that may increase the risk of psychopathology among emerging adults. These findings support a precision medicine framework, wherein specific trauma histories may be considered risk factors for depression, suicidality, and anxiety (McQuaid, 2021). Further, our study highlights the protective effect of resiliency in its ability to buffer the impact of particularly salient traumas on depressive symptoms. We suggest prevention strategies prior to adolescence, such as routine clinical and school-based screenings, alongside resilience-building programs, and public health education initiatives to increase awareness of mental health consequences associated with childhood maltreatment. Additionally, trauma subtype and timing-informed assessments implemented in campus mental health services could be beneficial in detecting and differentiating elevated risk. Special attention should be given to exposures during adolescence including non-verbal emotional abuse (depression symptoms), emotional neglect (suicidal ideation), and parental verbal abuse (anxiety symptoms). These recommendations lend themselves to risk stratification based on trauma profile, which may inspire the development of interventions targeted towards high-risk youth to foster resilience.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605251372562 – Supplemental material for Types and Timing of Childhood Trauma and Their Relationship to Symptoms of Depression, Suicidal Ideation, and Anxiety Among Canadian University Students
Supplemental material, sj-docx-1-jiv-10.1177_08862605251372562 for Types and Timing of Childhood Trauma and Their Relationship to Symptoms of Depression, Suicidal Ideation, and Anxiety Among Canadian University Students by Ayeila Zamani Begum Daneshmend, Frances Elizabeth Sherratt, Mikaela Anne Ethier-Gagnon, Dana Abdulaziz Jarkas and Robyn J McQuaid in Journal of Interpersonal Violence
Footnotes
ORCID iDs
Ethical Considerations
Ethics approval for the procedures in this study was provided from the Research Ethics Boards at Carleton University (REB # 111223) and the Royal Ottawa Mental Health Centre (REB # 2019024) on January 29, 2021. All participants provided written informed consent online prior to participating.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research is funded by the Royal’s Emerging Research Innovators in Mental Health program, awarded to Robyn J. McQuaid at the University of Ottawa Institute of Mental Health Research, Ottawa, Ontario, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available as these data are not approved by the institutional Research Ethics Boards to be shared outside of the research team.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.