
Abstract
United States active-duty military members face elevated risk of self-directed harm and interpersonal violence. Prevention resources for family maltreatment in the military context have received notable investments in recent years, culminating in the development of the Personal and Family Strengths Inventory (PFSI), a strengths-based prevention and treatment-planning tool aimed at inventorying key dimensions of individuals’ formal supports, informal supports, family environment, individual fitness, and personal resilience. Research has showcased the utility of the holistic assessment of factors captured by the PFSI, with implications for predicting the perpetration of family maltreatment, broadly speaking, among active-duty members. The purpose of the current study was to assess the capacity of PFSI indicators, distinctly and in combination with each other, to predict other forms of self-directed harm and specific types of interpersonal violence that the U.S. military endeavors to prevent. Leveraging a representative sample of 30,187 active-duty Air Force members who had at least one child and were in a committed relationship, results from weighted regression models indicated that latent profiles marked by low scores across PFSI dimensions were associated with higher predicted probabilities of partner physical perpetration, child physical perpetration, child emotional perpetration, partner physical victimization, partner emotional victimization, suicidality, hazardous alcohol consumption, prescription drug misuse, illicit drug use, and non-suicidal self-harm. Moreover, almost without exception, there were significant standardized mean differences for all PFSI dimension scores between military members who did and did not report each indicator of self-directed harm or interpersonal violence. Taken together, the PFSI appears well positioned as an integrative prevention tool for use in numerous prevention settings, ultimately to promote the health and well-being of military-connected individuals and families. The PFSI could be embedded in various practice settings to support a multitude of prevention efforts and be used to inform broader base-specific, branch-specific, or military-wide policy directives.
United States (U.S.) active-duty military members face increased risk of various forms of self-directed harm and interpersonal violence. For example, the rate of suicide among military members has been rising over time, with 28.3 deaths by suicide per 100,000 active-duty military members in 2023 compared to fewer than 20 deaths by suicide per 100,000 in 2011 (Department of Defense [DoD], 2024). Increasing attention also has been placed on elevated rates of non-suicidal self-injury and problematic substance use among military members (Bandel & Anestis, 2020; Gromatsky et al., 2023; Logan et al., 2020; Osborne et al., 2022; Rachal et al., 2023; Schuler et al., 2022; Tam et al., 2020; Vest et al., 2021). In addition, military members experience higher rates of intimate partner violence victimization compared to civilians (Sparrow et al., 2020). Evidence also suggests that military members likely also perpetrate intimate partner violence at higher rates than non-military affiliated samples (Kwan et al., 2020). These elevated rates and risks have persisted despite ongoing efforts by the DoD to prevent self-directed harm and interpersonal violence.
Research indicates that risk factors for self-directed harm, interpersonal violence perpetration, and interpersonal violence victimization overlap (Jennings et al., 2012; Logan et al., 2020; Trachik et al., 2021; Zimmerman & Posick, 2014). Recognizing this, the DoD recently moved to integrate self-directed harm and interpersonal violence prevention efforts (DoD, 2022). In addition, the DoD established community-level assessment protocols to evaluate and address overlapping violence risk factors (Chinman et al., 2020). However, individual-level integrated prevention tools are currently lacking.
Individual-level prevention resources for family maltreatment in the military context are more developed than for other prevention targets prioritized by the U.S. military (e.g., self-directed harm, suicidality). In this context, family maltreatment can generally be conceptualized as the perpetration of any non-accidental physical, sexual, or emotional trauma, abuse, or neglect toward an intimate partner or child (Air Force Instruction 40–301, November 30, 2009). On this front, a recent systematic review was conducted focused on predictors or correlates of family maltreatment perpetration among active-duty military personnel, which was used to expand the Air Force’s Family Advocacy Program logic model for family maltreatment prevention (Bowen et al., 2017). Results from this review were further corroborated and enriched with analyses of representative data from the Air Force Community Assessment Survey (CAS; Jensen & Bowen, 2018) and efforts to develop a psychometrically valid measure of Comprehensive Airmen Fitness (Bowen et al., 2016a, 2016b). Combined findings were ultimately translated into the formal development of the Personal and Family Strengths Inventory (PFSI), a strengths-based prevention tool that enables military-connected individuals to assess the presence of the following assets in their lives and relationships: formal supports (e.g., unit leader support), informal supports (e.g., sense of community, neighbor support, personal network support), family processes (e.g., family coping, couple relationship quality, partner support, parent-child relationship quality), individual fitness (e.g., financial, physical, and mental fitness), and personal resilience (Jensen et al., 2022). The PFSI also assess one’s readiness or motivation for change in areas of their lives or relationships that present growth opportunities.
Related research has showcased the utility of the holistic assessment of factors featured in the PFSI for predicting the perpetration of family maltreatment (Jensen et al., 2022). Specifically, Jensen et al. (2022) identified five distinct patterns of personal and family strengths among active-duty Air Force members in a committed couple relationship (i.e., spouse or unmarried partner) with at least one child. The patterns were labeled low strengths (i.e., low levels across all personal and family strengths), below-average strengths (i.e., below-average levels across all strengths), mixed strengths (i.e., below-average levels of formal support, informal support, and individual fitness, but above-average levels of adaptive family processes), above-average strengths (i.e., above-average levels of all personal and family strengths), and high strengths (i.e., high levels across all strengths). Predicted probabilities for past-year endorsement of family maltreatment across the patterns were 41%, 22%, 16%, 10%, and 9%, respectively, for the low strengths, below-average strengths, mixed strengths, above-average strengths, and high strengths patterns (while holding the following variables at sample-mean levels: family structure, presence of young children, sex, age, paygrade, and deployment status; see Jensen et al. [2022] for more details).
Despite evidence suggesting overlapping risk factors for family maltreatment and other forms of interpersonal violence and self-directed harm, the PFSI has not yet been evaluated for use beyond efforts to prevent family maltreatment in a broad sense. Thus, the purpose of the current study is to evaluate the capacity of PFSI indicators, distinctly and in combination with each other (i.e., unique patterns of indicator levels), to predict a host of risk outcomes that are high-priority prevention targets for the U.S. military, including various forms of self-directed harm (e.g., suicidality, hazardous alcohol and drug use, non-suicidal self-harm) and specific types of interpersonal violence or family maltreatment (i.e., partner physical abuse perpetration and victimization and child emotional and physical abuse perpetration). Results from this study could highlight the utility of the PFSI beyond family maltreatment prevention efforts in the U.S. military in general and the U.S. Air Force in particular. Indeed, study findings might encourage application of the PFSI in a host of prevention settings intended to cultivate mission readiness and wellness among military members. There also might be implications for the adaption of the PFSI for use in veteran and civilian populations.
Methods
Data Source and Sample
We leveraged data from the 2011 AF CAS to address our study aims. The CAS possesses measures that align closely with the constructs addressed in the PFSI—a relatively new practice tool that was not intended to operate as a formal scientific measure. The 2011 CAS was administered between January and April 2011, with respondents representing active-duty members, reservists, DoD civilians, and spouses of active-duty members and reservists. In general, data provided by the CAS are intended to inform action planning at various levels of the Air Force (e.g., major command, installations). The 2011 CAS included more than 300 survey items, with numerous questions addressing respondent mental health, secretive behaviors, resilience, help-seeking attitudes, family and couple relationships, informal networks, and other experiences related to military life (see Martin & Bowen, 2003 for sources related to many of the items and scales used for the current study).
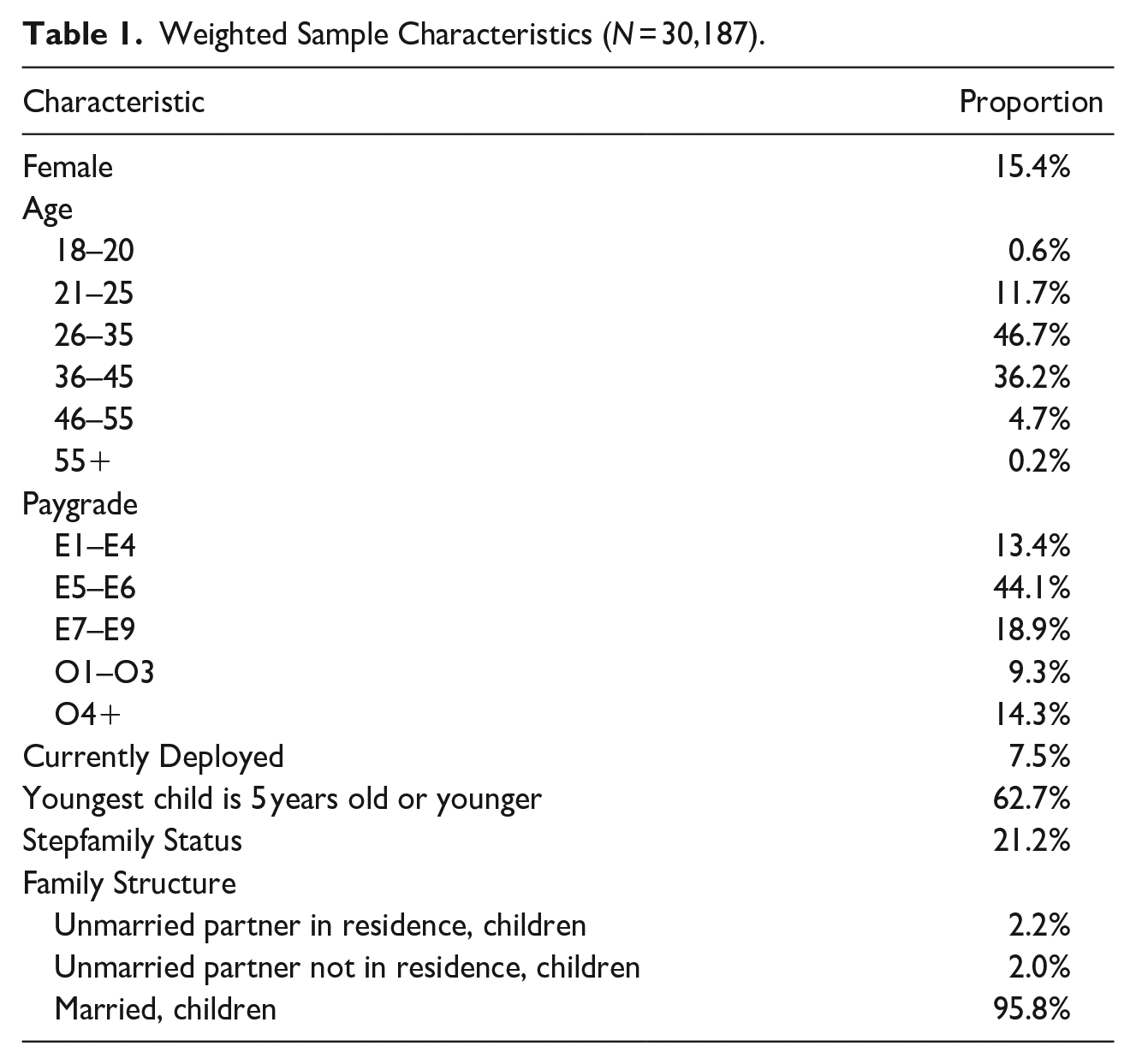
Our analytical sample included 30,187 participants, representing only active-duty Air Force members who had at least one child, were in a committed relationship (i.e., they were married, engaged, or involved in a serious relationship), and had non-missing data for indicators of personal and family strengths (<1.2% of cases had missing data). Our focus on this subset of cases ensured that respondents were embedded in social contexts where various forms of family maltreatment were even possible (e.g., child-directed maltreatment, partner-directed maltreatment). In terms of weighted sample characteristics, about 15% of participants identified as female, with a modal age category of 26 to 35 years (46.7%) and modal paygrade of E5 to E6 (44.1%). Nearly 96% of participants reported being married, nearly 63% indicated that their youngest child as 5 years old or younger, and about 21% identified being part of a stepfamily—a family in which one or both partners in the couple relationship brought a child or children from a previous relationship (Ganong & Coleman, 2017). See Table 1 for more details related to weighted sample characteristics.
Weighted Sample Characteristics (N = 30,187).
Measures
Risk Outcomes
To address our study aims, we assembled a set of risk outcome variables available in the 2011 CAS that represented various high-priority prevention targets in the military, each pertaining to some aspect of family maltreatment or self-directed harm. Specifically, we prepared binary variables indicating whether participants reported any of the following (affirmative responses coded as 1; coded as 0 otherwise): (a) perpetration of partner physical maltreatment, (b) perpetration of child physical maltreatment, (c) perpetration of child emotional maltreatment, (d) receipt of physical maltreatment from partner, (e) receipt of emotional maltreatment from partner, (f) suicidality (i.e., endorsement of suicidal thoughts, planning, or attempts), (g) hazardous alcohol consumption, (h) prescription drug misuse, (i) illicit drug use, or (j) non-suicidal self-harm. We also created two additional binary variables: one indicating whether any of the family maltreatment indicators were reported and another indicating whether any of the listed risk outcomes were reported. For efficient presentation, Table 2 provides details related to how each risk outcome was measured.
Overview of Risk Outcome Measures.
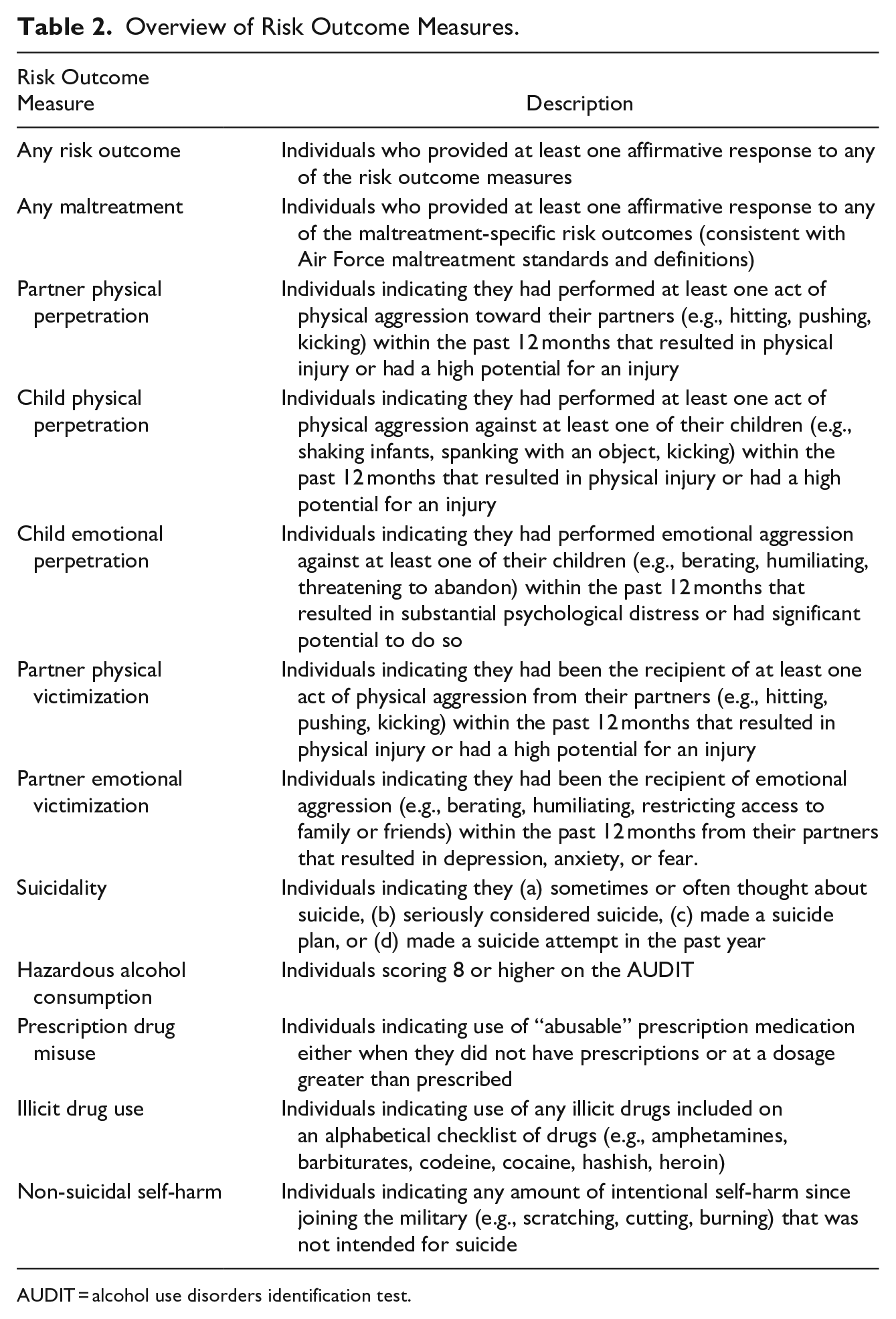
AUDIT = alcohol use disorders identification test.
Profiles of Personal and Family Strengths
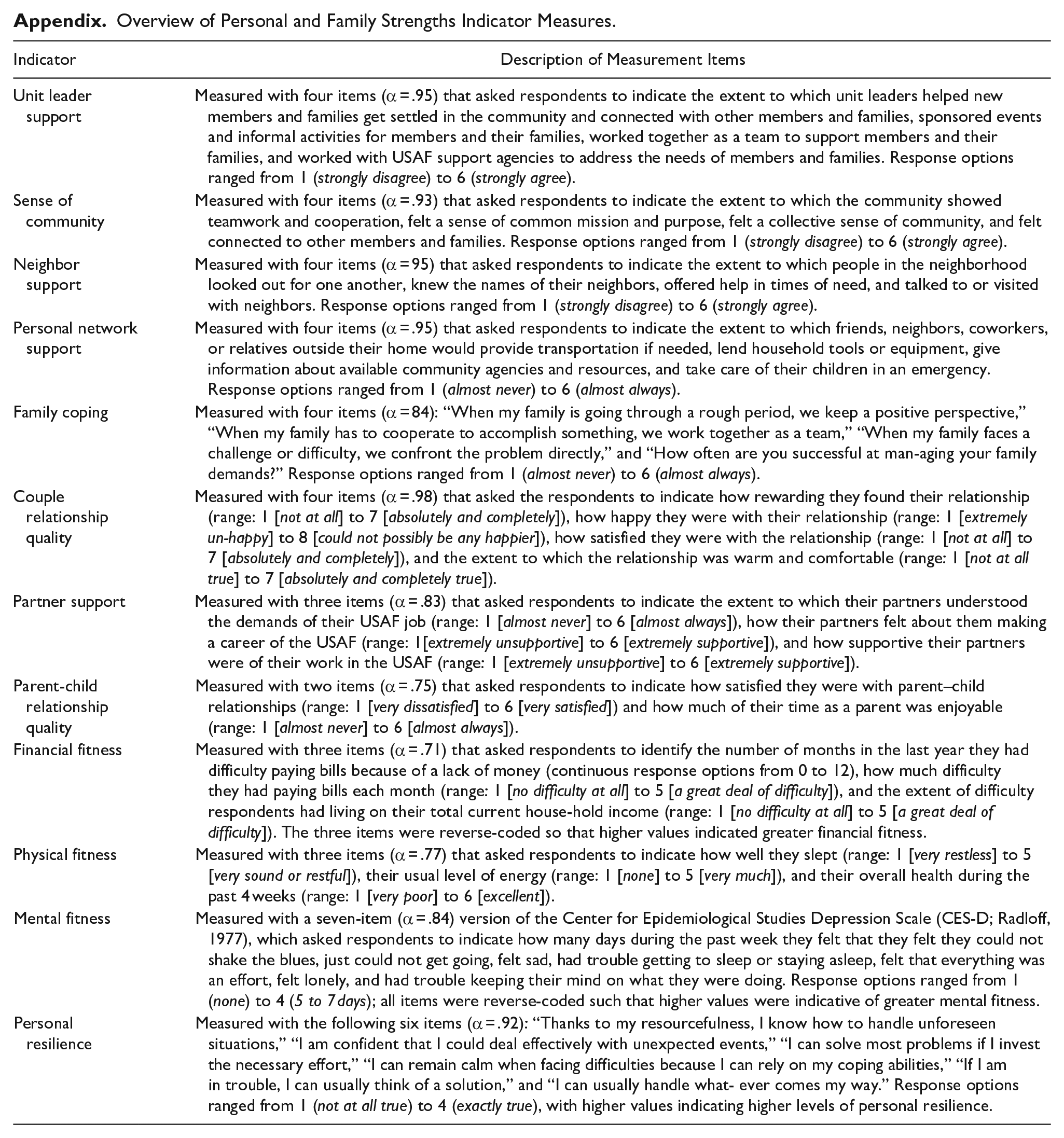
Earlier work employing latent profile analysis (LPA) with the same sample of active-duty Air Force members yielded a five-profile solution representing distinct patterns of personal and family strengths (Jensen et al., 2022), measured with standardized latent-factor scores (continuous) representing dimensions of formal support (i.e., unit leader support); informal support (i.e., sense of community, neighbor support, personal network support); family processes (i.e., family coping, couple relationship quality, partner support, parent-child relationship quality); individual fitness (i.e., financial fitness, physical fitness, mental fitness); and personal resilience. See Appendix for more details related to the specific measures used for each personal and family strengths indicator. Also, see Bowen et al. (2017), Jensen and Bowen (2018), and Jensen et al. (2022) for the conceptual, theoretical, and empirical underpinnings of the personal and family strengths framework.
The five identified profiles of personal and family strengths were labeled low strengths, below-average strengths, mixed strengths, above-average strengths, and high strengths. Table 3 provides an overview of each profile or pattern. Results from the LPA included information about each respondent’s probability of being a member of a particular profile or pattern conditional on their values for each personal and family strengths indicator. We used these pattern-specific probability values as variables in our analyses (described in the Data Analysis subsection). For other analyses, we used each distinct personal and family strengths indicator measure (i.e., standardized latent-factor scores; refer to Appendix for more details about each measure).
Five-Profile Solution with Standardized Construct Scores Across Indicators of Personal and Family Strengths (N = 30,187).
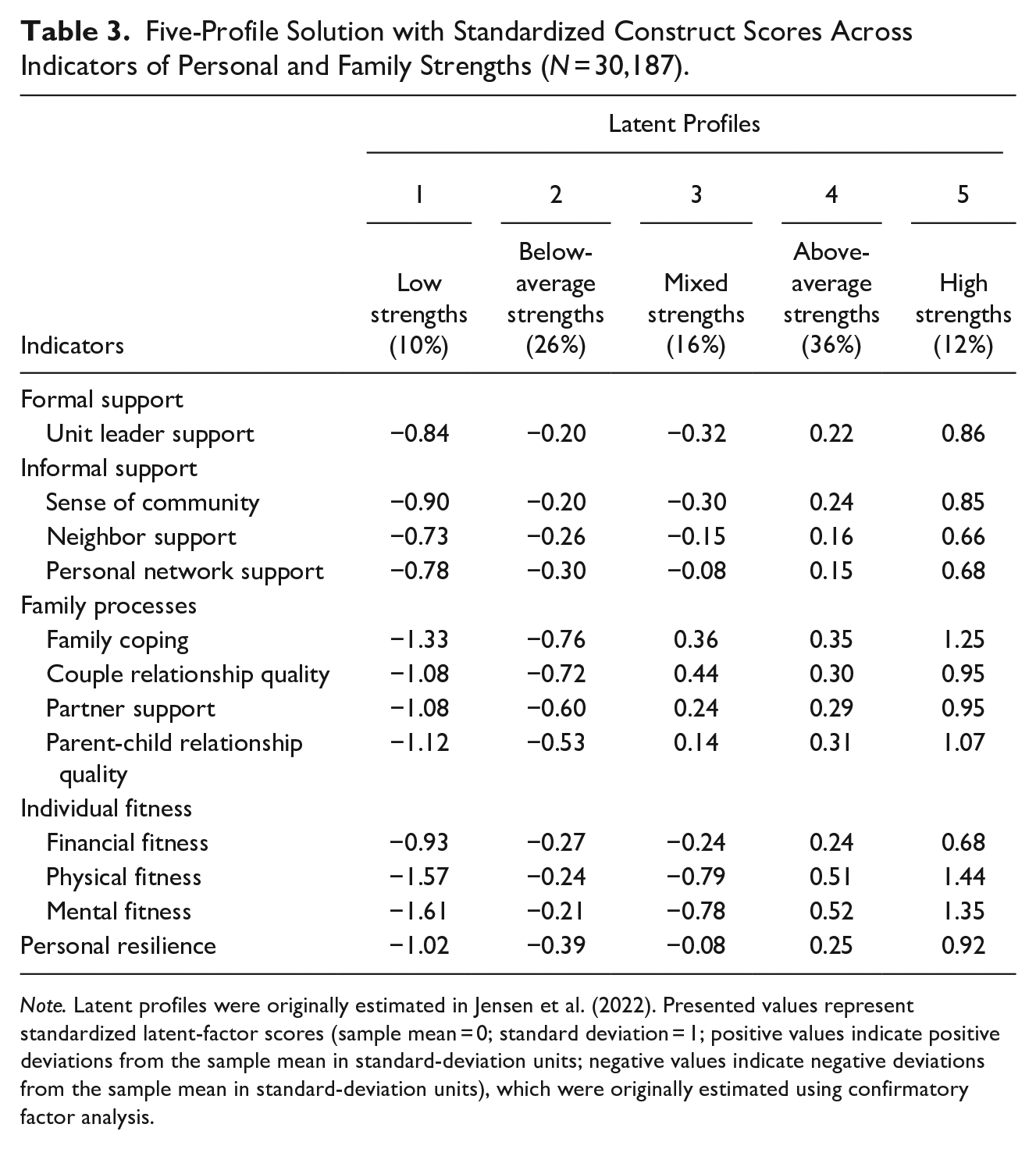
Note. Latent profiles were originally estimated in Jensen et al. (2022). Presented values represent standardized latent-factor scores (sample mean = 0; standard deviation = 1; positive values indicate positive deviations from the sample mean in standard-deviation units; negative values indicate negative deviations from the sample mean in standard-deviation units), which were originally estimated using confirmatory factor analysis.
Covariates
We incorporated several covariates in models assessing associations between specific patterns of personal and family strengths and each risk outcome (Bowen et al., 2017; Jensen & Bowen, 2018). Specifically, we included covariates representing (a) stepfamily status (participant indicated being part of a stepfamily [1], participant did not indicate being part of a stepfamily [0]; Jensen, 2017; Jensen & Weller, 2019), the presence of young children (youngest child was 5 years old or younger [1], youngest child was older than 5 years [0]), biological sex (female [1], male [0]), age group (with dummy coded age categories representing the following: 18–20, 21–25, 26–35 [reference group], 36–45, 46–55, and 55 or older), paygrade (with dummy coded categories representing the following: E1–E4 [reference group], E5–E6, E7–E9, O1–O3, and O4 or higher), and deployment status (currently deployed [1], not currently deployed [0]).
Data Analysis
To begin, we estimated weighted sample proportions for each risk outcome variable (sampling weights were available in the data source to enable the estimation of representative model parameters). These values were intended to provide a general point of contrast for subsequent analyses. We then specified weighted logistic regression models for each risk outcome variable. In each model, the risk outcome was regressed on variables representing patterns of personal and family strengths and covariates. Predicted probabilities for each risk outcome were then estimated for each pattern of personal and family strengths by specifying a 100% probability of possessing a particular pattern and holding all model covariates at sample-mean levels. As a result, the predicted probabilities can be interpreted as the probability of a risk outcome among an average respondent (with respect to covariates) who also had a 100% probability of possessing a particular pattern of personal and family strengths.
We also conducted relatively granular assessments of associations between risk outcomes and specific indicators of personal and family strengths. Specifically, we analyzed weighted regression models with binary risk outcome variables specified as a predictor and a single indicator of personal and family strengths as an outcome. This approach enabled the estimation of significance tests for standardized mean differences (with respect to an indicator of personal and family strengths) between participants indicating possession of a risk outcome and participants not indicating possession of a risk outcome. All data management and analyses were conducted using Stata 17.0 (StataCorp, 2021). The secondary data analyses were deemed non-human subjects research by the Institutional Review Board (IRB) at the first and third authors’ institution (IRB #: 14-0754).
Results
Patterns of Personal and Family Strengths and Risk Outcomes
Table 4 displays the predicted probabilities of each risk outcome with respect to specific patterns of personal and family strengths. Without exception, the low strengths pattern was associated with risk-outcome probabilities notably higher than sample-average levels. Especially high were probabilities of any risk outcome (57.7%), any maltreatment (41.0%), partner emotional victimization (30.0%), suicidality (16.0%), and hazardous alcohol consumption (14.5%). Moving to the below-average strengths pattern, predicted probabilities related to self-directed harm moved closer to sample-mean levels; however, predicted probabilities related to any family maltreatment remained above sample-mean levels (22.0%), as did the predicted probability for any risk outcome (31.6%). The mixed strengths pattern yielded predicted probabilities near sample-mean levels, although probabilities associated with partner physical victimization (0.5%) and partner emotional victimization (2.8%) were markedly lower than sample-mean levels. Predicted probabilities of each risk outcome were appreciably lower than sample-mean levels for the above-average strengths pattern and even more so for the high strengths pattern. The one risk outcome that appeared relatively less influenced by patterns of personal and family strengths was child physical maltreatment perpetration, with predicted probabilities ranging between 11.2% and 7.7% across all five patterns of personal and family strengths. See Table 4 for more details.
Patterns of Personal and Family Strengths and Corresponding Predicted Probabilities of Risk Outcomes.
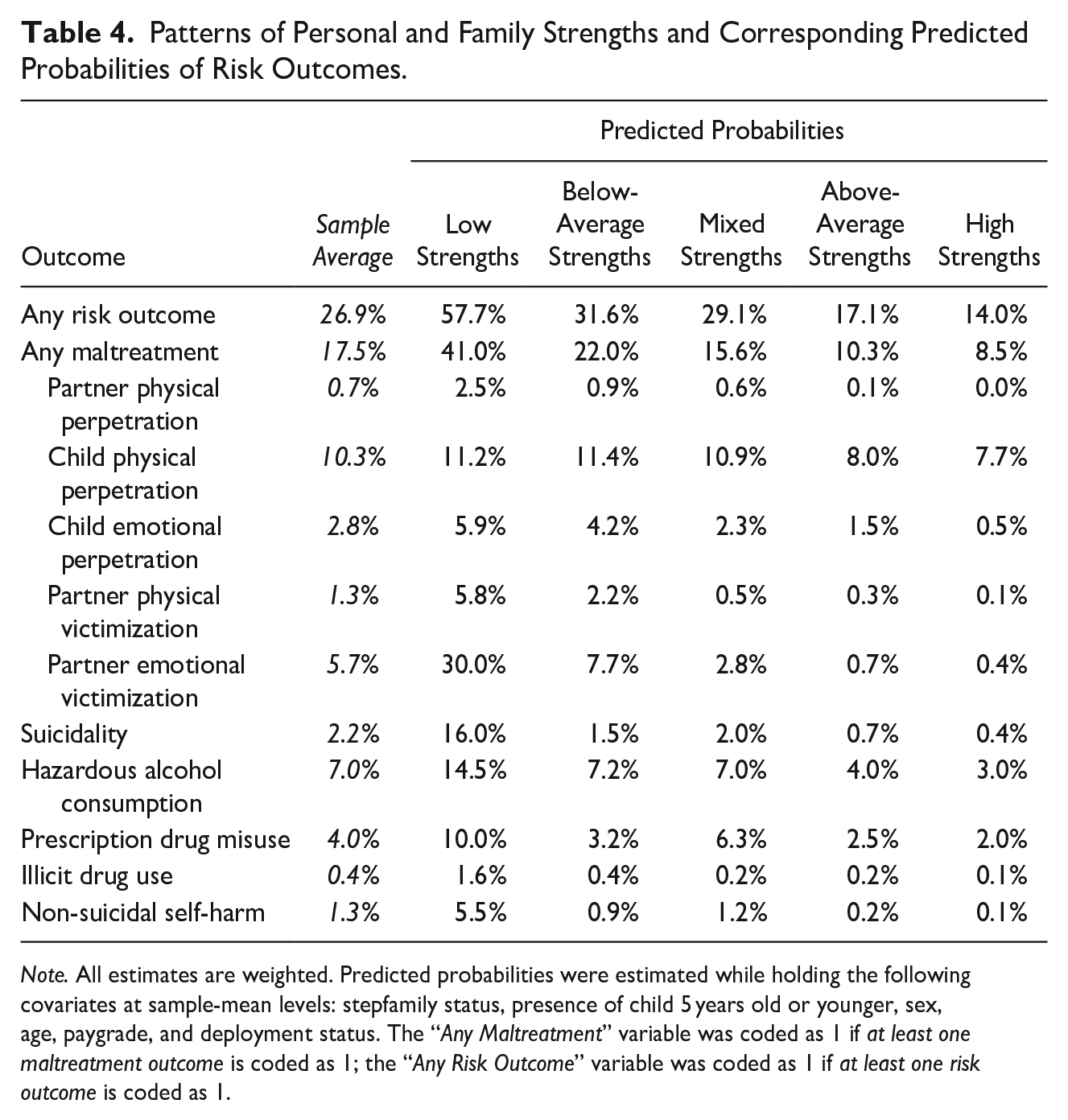
Note. All estimates are weighted. Predicted probabilities were estimated while holding the following covariates at sample-mean levels: stepfamily status, presence of child 5 years old or younger, sex, age, paygrade, and deployment status. The “Any Maltreatment” variable was coded as 1 if at least one maltreatment outcome is coded as 1; the “Any Risk Outcome” variable was coded as 1 if at least one risk outcome is coded as 1.
Distinct Indicators of Personal and Family Strengths and Risk Outcomes
Table 5 displays standardized mean differences between affirmative and non-affirmative risk-outcome reports for each indicator of personal and family strengths. Turning to any risk outcome, standardized mean differences across all 12 indicators of personal and family strengths were significant and ranged from −0.14 (personal network support) to −0.53 (mental fitness). To support interpretation, this means that individuals with any risk outcome possessed mean values of personal network support and mental fitness that were 0.14- and 0.53-standard deviations lower, respectively, than the mean values of their counterparts who did not report having any risk outcomes. A similar pattern of findings emerged for any maltreatment, with all 12 indicators of personal and family strengths being significant and ranging from −0.13 (personal network support and neighbor support) and −0.50 (family coping).
Standardized Mean Differences (Weighted) Between Individuals Indicating a Risk Outcome and Individuals Not Indicating a Risk Outcome.
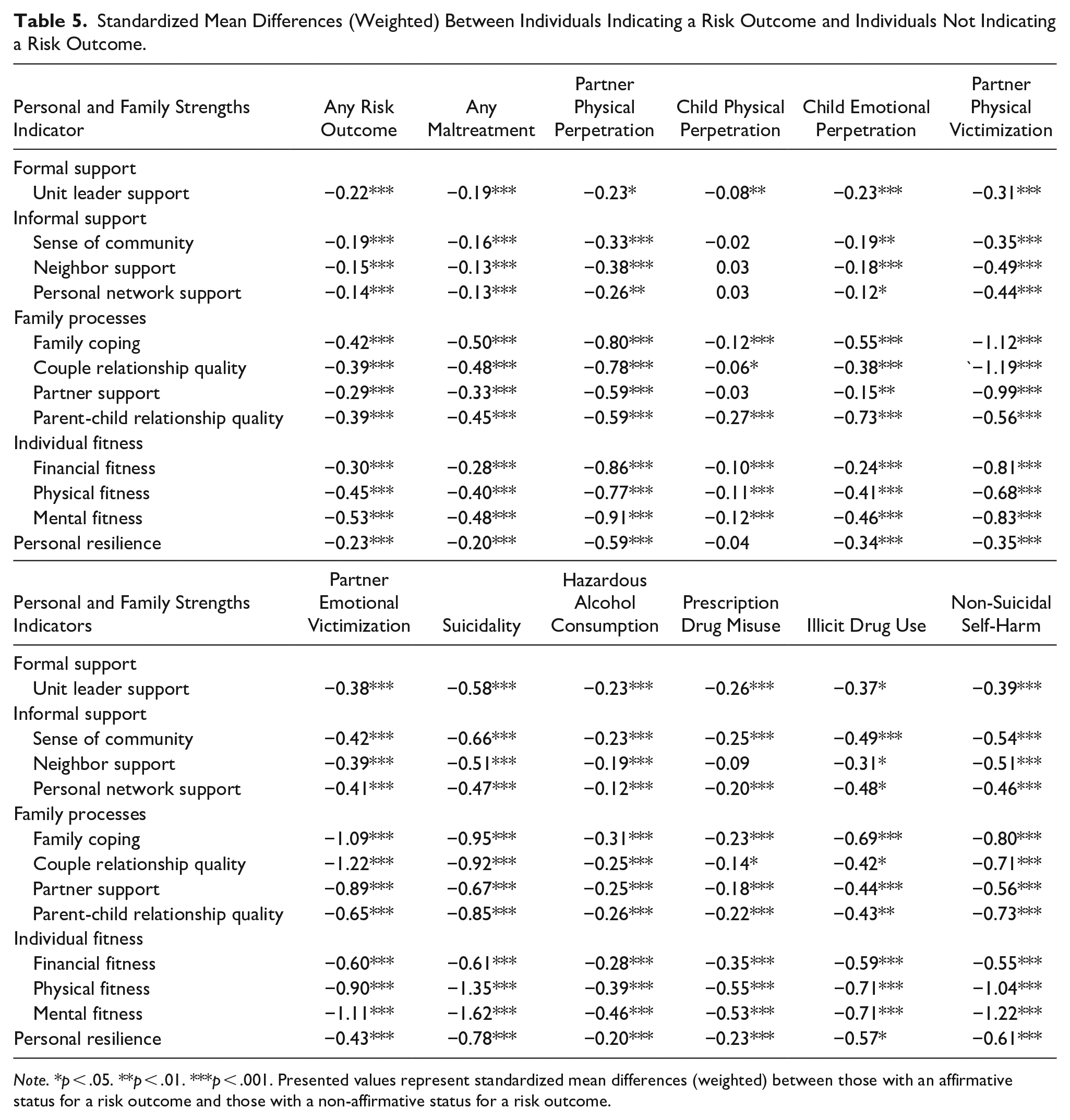
Note. *p < .05. **p < .01. ***p < .001. Presented values represent standardized mean differences (weighted) between those with an affirmative status for a risk outcome and those with a non-affirmative status for a risk outcome.
With respect to partner physical perpetration, standardized mean differences across indicators of personal and family strengths were also significant and ranged from −0.23 (unit leader support) and −0.91 (mental fitness). In terms of child physical perpetration, only 7 out of 12 personal and family strengths yielded significant standardized mean differences ranging from −0.06 (couple relationship quality) to −0.27 (parent-child relationship quality); all three dimensions of informal support, one dimension of the family environment (partner support), and personal resilience were non-significant. In contrast, for child emotional perpetration, standardized mean differences were significant for all 12 indicators of personal and family strengths and ranged from −0.12 (personal network support) and −0.55 (family coping). Overall, standardized mean differences were also significant and even more pronounced in the context of partner physical victimization, ranging from −0.31 (unit leader support) to −1.19 (couple relationship quality), and partner emotional victimization, ranging from −0.38 (unit leader support) to −1.22 (couple relationship quality).
In terms of suicidality, all indicators of personal and family strengths yielded significant and notable standardized mean differences. Indeed, all differences were greater than one-half a standard deviation, ranging from −0.51 (neighbor support) to −1.62 (mental fitness). Turning to hazardous alcohol consumption, all indicators of personal and family strengths yielded significant standardized mean differences that ranged from −0.12 (personal network support) and −0.46 (mental fitness). All but one indicator (neighbor support) yielded significant standardized mean differences for prescription drug misuse, ranging from −0.14 (couple relationship quality) to −0.55 (physical fitness). For illicit drug use, standardized mean differences for all indicators of personal and family strengths were significant and ranged from −0.31 (neighbor support) and −0.71 (physical fitness and mental fitness). Lastly, for non-suicidal self-harm, all indicators of personal and family strengths produced significant standardized mean differences that ranged from −0.39 (unit leader support) to −1.22 (mental fitness). See Table 5 for more details.
Discussion
The purpose of the current study was to evaluate the capacity of PFSI indicators, distinctly and in combination with each other, to predict a host of risk outcomes that are high-priority prevention targets for the U.S. military. Taken together, our findings offer compelling evidence that the constructs featured in the PFSI are well positioned to detect numerous risk outcomes, in particular partner physical perpetration, partner physical victimization, partner emotional victimization, suicidality, hazardous alcohol consumption, prescription drug misuse, illicit drug use, and non-suicidal self-harm. However, a relatively challenging risk outcome to detect is various forms of child maltreatment. This suggests that a military member’s stress threshold for perpetrating child maltreatment could prove lower relative to other risk outcomes or at least have causes and influences that differ from the constructs featured in the PFSI.
Practical Implications
Evidence indicates that the PFSI is an effective tool for assessing factors linked to a wide range of maltreatment and self-directed harm outcomes that are high-priority prevention targets in the military. As the DoD has sought to centralize and integrate prevention efforts across self-harm and interpersonal violence domains, the PFSI may prove an effective prevention and referral tool for a broad range of helping agencies. For example, helping and prevention professionals such as chaplains, embedded mental health consultants, and violence prevention integrators may provide the PFSI to members to self-assess which strength area(s) they might most benefit from bolstering. Helpers and prevention professionals might utilize members’ PFSI results to help inform the selection of optimal referral resources to both increase strengths and reduce risk. Used properly, the prevention or helping professional administering the PFSI would triangulate the inventory’s results with their strong awareness of available resources, along with the goals and preferences of individuals they are aiding. For example, if a prevention professional identified low scores related to financial fitness, they might ask the member what resources they have already considered, what types of interventions most fit their needs and resources (e.g., in person, online, long-term investing, short-term loan), and then based on responses, refer the member to the resource that best fits their needs. In addition to informing micro-level referrals, installation-level PFSI data could prove useful in informing broader base-specific initiatives to fill identified strengths gaps known to increase risk. For example, if results showed suboptimal levels of neighbor support among those living on base, leaders could develop programs and events that promote neighbor engagement. Finally, combined data across installations could inform macro-level changes by identifying broader gaps across the DoD and more specific gaps affecting at-risk subgroups. For example, research indicates that servicewomen and dual-military married members face unique marital struggles that may compromise various aspects of family functioning as captured by PFSI items (King et al., 2025). If combined PFSI results clarified which family processes were most affected (i.e., family coping, couple relationship quality, partner support, and/or parent-child relationship quality) for which family structures (e.g., dual-military, geographically separated, servicewomen with civilian spouses), programs that aid those most at risk could be implemented across the DoD.
Fortunately, infrastructure already exists to implement a tool like the PFSI in the DoD, as current prevention policy requires military leaders to assess base needs, culture, and climate, but does not dictate data collection tools (DoD, 2022). In line with DoD requirements, each military service publishes a prevention instruction that outlines how primary prevention workers will operate. In the Air Force, the instruction reiterates the requirement to utilize data to inform prevention activities and mandates that a “Community Action Team” of interdisciplinary helping professionals and leaders meet monthly to “develop and implement resilience and integrated primary prevention policy, practices, and programs . . . that meet each community’s unique needs.” (Department of the Air Force, 2024, p. 72). The ongoing need to aid individuals struggling, combined with mandates to continuously assess community needs to prevent interpersonal violence and self-directed harm matches the utility of the PFSI. Specifically, in the Air Force, members of the installation’s Community Action Team—which must include representatives from the chaplain’s office, prevention workforce, drug demand reduction office, sexual assault prevention and response office, behavioral health clinic, embedded counseling programs, family advocacy program, and military and family readiness services—already serve as touchpoints for individuals who may be at risk (Department of the Air Force, 2024). Thus, to implement the PFSI as both an individual and community tool, Community Action Team members could all be trained in using the PFSI with individuals seeking resources and evaluating the utility of the PFSI as a community needs assessment that could inform base-wide prevention efforts.
Continuing the Air Force example, if leaders at the highest levels wished to utilize the PFSI to assess the broader force’s needs, the Air Force Integrated Resiliency Office could enable its use, as it oversees all Air Force integrated resilience efforts, including prevention programming and the Community Action Teams. By collecting consistent, evidence-driven, prevention-relevant data across installations, a greater understanding of needs and effective programs could be leveraged to continuously inform service-wide prevention efforts. These bottom-up and top-down implementation examples for the Air Force could also readily be translated to and employed within Army, Navy, and Marines prevention program structures.
Findings from the current study, coupled with findings related to the demographic characteristics of the five focal profiles of personal and family strengths (Jensen et al., 2022), also highlight opportunities for tailored or targeted prevention efforts. For instance, the following demographic characteristics are over-represented among those in the low strengths profile: stepfamilies, those aged 21 to 25, E1 to E4 paygrades, and individuals residing in communities perceived as unsafe. Given the connection between the low strengths profile and relatively high probabilities of various risk outcomes, prevention efforts might benefit from attending to young, junior-enlisted members residing in stepfamilies and communities perceived as unsafe. In addition, military members who identify as female are over-represented in the mixed strengths profile—a profile marked by low levels of physical fitness and mental fitness and, correspondingly, the second highest predicted probability of prescription drug misuse. As a result, prevention efforts focused on managing prescription drug misuse could attend to female-identifying military members.
Although the data that informed the PFSI were collected from Air Force members, both previous research and overlap across military service branches suggest that the PFSI could be tested and refined by other military branches. Additionally, the strengths-focused tool was informed by broader civilian literature and tested with military members, suggesting it could translate into an effective tool for assessing and promoting well-being among veterans and—with some adaptations—non-military-connected civilians. Attending to veterans could be especially important, given veteran’s elevated risk of poor health outcomes relative to their civilian counterparts (Betancourt et al., 2021). Leveraging a tool like the PFSI among veterans might be especially fruitful during the transition period of military members separating from active service—a time when former members and their families can experience pronounced losses in formal and informal support, placing them at elevated risk for negative outcomes (Markowitz et al., 2023; Pease et al., 2015; Sokol et al., 2021).
Limitations and Future Research
Study conclusions should be tempered by important limitations. For one, the analyses featured in the current study are cross-sectional. The absence of longitudinal data limits causal inference, and future research would benefit from the use of multiple time-points of data collection to bolster conclusions related to whether constructs featured in the PFSI are, in any way, causally linked to the various risk outcomes highlighted in this study. Even more likely is that PFSI indicators and risk outcomes are bidirectionally and transactionally associated—dynamics that could be modeled using longitudinal data.
The data used in the current study also were derived from participant self-reports. Consequently, various risk outcomes could be underreported as a result of social desirability bias or fear that one’s responses could negatively impact their career prospects, despite responses being anonymous. Unfortunately, the data source featured in the current study also lacked detailed information about participants’ racial/ethnic identity and other characteristics (e.g., sexual orientation), which limited our ability to assess potential nuances across racial/ethnic groups and other subgroups of potential interest.
In light of our view that the PFSI could be embedded in a host of routine prevention and intervention or practice settings, future research could endeavor to assess the implementation and impact of the PFSI in such settings. Initial work on this front could focus on the implementation of the PFSI in a specific military base or installation, attending to challenges around successful implementation and the relationships among leaders, service providers, and researchers that would be needed to promote implementation success in routine practice approaches (Metz et al., 2022). After identifying critical success factors to promote the uptake of the PFSI, expanded evaluation efforts could be pursued, aimed at experimentally assessing the impact of PFSI use in a set of bases or installations relative to a set of bases or installations that do not implement the PFSI. Designs of this sort could generate internally valid insights about the impact of PFSI use for various prevention efforts.
Moreover, future research could endeavor to adapt and evaluate the use of the PFSI among veterans and non-military-connected civilians. A key consideration on this front would be identifying a suitable replacement for unit leader support, which is featured as a core construct in the PFSI and a source of support not available to veterans or other civilians. The current version of the PFSI does include language suitable for civilian employees on this front (i.e., work supervisor support; Jensen et al., 2022); however, it is unlikely that work supervisors or managers exert the same level of influence on individuals as unit leaders. In any case, future research could assess the extent to which PFSI indicators predict various risk outcomes in veteran and civilian populations, with potential implications for promoting the well-being of individuals beyond the active-duty military context.
Footnotes
Appendix
Overview of Personal and Family Strengths Indicator Measures.
| Indicator | Description of Measurement Items |
|---|---|
| Unit leader support | Measured with four items (α = .95) that asked respondents to indicate the extent to which unit leaders helped new members and families get settled in the community and connected with other members and families, sponsored events and informal activities for members and their families, worked together as a team to support members and their families, and worked with USAF support agencies to address the needs of members and families. Response options ranged from 1 (strongly disagree) to 6 (strongly agree). |
| Sense of community | Measured with four items (α = .93) that asked respondents to indicate the extent to which the community showed teamwork and cooperation, felt a sense of common mission and purpose, felt a collective sense of community, and felt connected to other members and families. Response options ranged from 1 (strongly disagree) to 6 (strongly agree). |
| Neighbor support | Measured with four items (α = 95) that asked respondents to indicate the extent to which people in the neighborhood looked out for one another, knew the names of their neighbors, offered help in times of need, and talked to or visited with neighbors. Response options ranged from 1 (strongly disagree) to 6 (strongly agree). |
| Personal network support | Measured with four items (α = .95) that asked respondents to indicate the extent to which friends, neighbors, coworkers, or relatives outside their home would provide transportation if needed, lend household tools or equipment, give information about available community agencies and resources, and take care of their children in an emergency. Response options ranged from 1 (almost never) to 6 (almost always). |
| Family coping | Measured with four items (α = 84): “When my family is going through a rough period, we keep a positive perspective,” “When my family has to cooperate to accomplish something, we work together as a team,” “When my family faces a challenge or difficulty, we confront the problem directly,” and “How often are you successful at man-aging your family demands?” Response options ranged from 1 (almost never) to 6 (almost always). |
| Couple relationship quality | Measured with four items (α = .98) that asked the respondents to indicate how rewarding they found their relationship (range: 1 [not at all] to 7 [absolutely and completely]), how happy they were with their relationship (range: 1 [extremely un-happy] to 8 [could not possibly be any happier]), how satisfied they were with the relationship (range: 1 [not at all] to 7 [absolutely and completely]), and the extent to which the relationship was warm and comfortable (range: 1 [not at all true] to 7 [absolutely and completely true]). |
| Partner support | Measured with three items (α = .83) that asked respondents to indicate the extent to which their partners understood the demands of their USAF job (range: 1 [almost never] to 6 [almost always]), how their partners felt about them making a career of the USAF (range: 1[extremely unsupportive] to 6 [extremely supportive]), and how supportive their partners were of their work in the USAF (range: 1 [extremely unsupportive] to 6 [extremely supportive]). |
| Parent-child relationship quality | Measured with two items (α = .75) that asked respondents to indicate how satisfied they were with parent–child relationships (range: 1 [very dissatisfied] to 6 [very satisfied]) and how much of their time as a parent was enjoyable (range: 1 [almost never] to 6 [almost always]). |
| Financial fitness | Measured with three items (α = .71) that asked respondents to identify the number of months in the last year they had difficulty paying bills because of a lack of money (continuous response options from 0 to 12), how much difficulty they had paying bills each month (range: 1 [no difficulty at all] to 5 [a great deal of difficulty]), and the extent of difficulty respondents had living on their total current house-hold income (range: 1 [no difficulty at all] to 5 [a great deal of difficulty]). The three items were reverse-coded so that higher values indicated greater financial fitness. |
| Physical fitness | Measured with three items (α = .77) that asked respondents to indicate how well they slept (range: 1 [very restless] to 5 [very sound or restful]), their usual level of energy (range: 1 [none] to 5 [very much]), and their overall health during the past 4 weeks (range: 1 [very poor] to 6 [excellent]). |
| Mental fitness | Measured with a seven-item (α = .84) version of the Center for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977), which asked respondents to indicate how many days during the past week they felt that they felt they could not shake the blues, just could not get going, felt sad, had trouble getting to sleep or staying asleep, felt that everything was an effort, felt lonely, and had trouble keeping their mind on what they were doing. Response options ranged from 1 (none) to 4 (5 to 7 days); all items were reverse-coded such that higher values were indicative of greater mental fitness. |
| Personal resilience | Measured with the following six items (α = .92): “Thanks to my resourcefulness, I know how to handle unforeseen situations,” “I am confident that I could deal effectively with unexpected events,” “I can solve most problems if I invest the necessary effort,” “I can remain calm when facing difficulties because I can rely on my coping abilities,” “If I am in trouble, I can usually think of a solution,” and “I can usually handle what- ever comes my way.” Response options ranged from 1 (not at all true) to 4 (exactly true), with higher values indicating higher levels of personal resilience. |
Data Availability
The datasets generated during and/or analyzed during the current study are not publicly available due to their ownership by the United States Air Force Medical Readiness Agency.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Ethical Considerations
The current study applied secondary data analysis, which was deemed non-human subjects research by the Instititional Review Board at the University of North Carolina at Chapel Hill (IRB #: 14-0754).
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.