
Abstract
Adverse childhood experiences (ACEs) are defined as stressful or traumatic events occurring within a child’s family environment during their first 18 years of life. Research examining the associations between exposure to ACEs in childhood and bullying experiences in adolescence is sparse. To address this gap, data from the first 10 sweeps of the Growing Up in Scotland prospective cohort study was used to evaluate the relationship between 6 different ACEs and the risk of being bullied or engaging in bullying others at age 14 among a sample of 2,669 adolescents. Multiple univariable logistic regression models were fitted to explore independent associations between each of the six ACEs measured, 1+ ACE and 3+ ACEs and bullying perpetration and victimization, respectively. Results showed that a high proportion of young people in Scotland experience bullying victimization (31%) and a very high percentage reported exposure to at least one type of adversity (73.6%). Young people whose parents reported drug or alcohol misuse and females whose parents had divorced or separated had higher odds of engaging in bullying others. Having a parent who had mental health problems was the only ACE that predicted higher odds of experiencing bullying. Substance misuse in the family predicted a higher risk of bullying victimization for females. Logistic regression analyses further showed that females with greater exposure to ACEs were more likely to engage in bullying in mid-adolescence. Our findings underscore the importance of understanding bullying perpetration as a maladaptive way to manage life stressors.
Introduction
Adverse childhood experiences (ACEs) are defined as stressful or traumatic events occurring within a child’s family environment during their first 18 years of life (Walsh, 2020). The original ACEs scale was first tested with adults from the United States, who were asked a series of questions covering childhood psychological, physical, and sexual abuse, emotional and physical neglect, and household dysfunction (Dong et al., 2004). The prevalence of ACEs in the general population is high. For example, in Scotland Marryat and Frank (2019) found that around two-thirds (65%) of a representative sample of children experienced 1+ ACE, with 10% experiencing 3+ at age 8. These rates are comparable to those found in other countries such as the United States of America, England and Wales, and New Zealand (Allen, 2015; Felitti et al., 1998; Reuben et al., 2016).
ACEs have been linked to a range of negative physical and mental health outcomes in childhood and adulthood including physical inactivity, depression, anxiety, poorer self-rated health, and worse global cognition (Albdour et al., 2024; Marryat & Frank, 2019; Zhang et al., 2023). They have also been associated with risky lifestyle behaviors such as alcohol and drug use, smoking, and a higher number of sexual partners (Marryat & Frank, 2019). Furthermore, a recent study found that the preschool children of mothers with ≥2 ACEs were at a significant risk of developing behavioral problems such as conduct problems, impulsivity, and hyperactivity, which was mediated by maternal rejection (Luo et al., 2023). However, research examining the associations between exposure to ACEs in childhood and bullying experiences in adolescence is sparse. The present study attempts to fill this gap by examining the link between individual and cumulative ACE exposure and bullying victimization and perpetration in a recent, nationally representative sample of children from Scotland. Existing research suggests that greater exposure to ACEs is associated with worse outcomes in childhood and adulthood including obesity, depression, anxiety, and suicidality therefore examining both the individual and cumulative effect of ACEs on bullying is important (Trompeter et al., 2024).
Child Bullying
Bullying refers to aggressive behavior that involves an observed or perceived power imbalance, and is repeated or is highly likely to be repeated (Centers for Disease Control and Prevention, 2014). Bullying can involve physical acts (e.g., hitting, kicking, tripping), verbal acts (e.g., name-calling, making threats), relational acts (e.g., spreading rumors, leaving out the group), damage to property, and/or it can occur through technology, which is known as electronic bullying or cyberbullying. Bullying is associated with a range of negative internalizing and externalizing outcomes including depression, anxiety, suicidal ideation, delinquency, and substance misuse (Lereya et al., 2015). There is evidence that these negative outcomes persist well into adulthood. A recent study analyzing data from a 1958 British birth cohort found that being bullied as a child lowers the probability of having a job throughout adulthood and raises the risk of early mortality (Blanchflower & Bryson, 2024). This long-lasting effect may be due to the fact that bullying in childhood negatively impacts an individual’s ability to cope with stressful events later on in life (Powdthavee, 2012).
Family influences may exacerbate or protect children from the risk of bullying. Studies focusing on the family context of young people involved in bullying victimization and/or perpetration have shown that being exposed to negative parenting behavior, such as abuse, neglect, and harsh parenting, increases the risk of bullying victimization (Lereya et al., 2013). On the other hand, parental involvement, support, and the quality of communication between child and parent were found to protect against the risk of bullying victimization (Nocentini et al., 2019). Young people who are exposed to abusive environments tend to develop lower self-confidence and frequently report experiencing feelings of powerlessness against those who are trying to manipulate them or do them harm (Finkelhor & Browne, 1985; Reisen et al., 2019).
In terms of those children and young people involved in bullying, the evidence suggests that a hostile family environment, characterized by violence and conflict, child maltreatment, and an authoritarian and overly controlled parenting style, increases the risk of engaging in bullying toward others (Nocentini et al., 2019). Experiencing family violence is associated with a higher likelihood of offspring engaging in a range of aggressive behaviors including delinquency, bullying, and crime. When children and young people are exposed to a hostile family environment, they perceive violence to be normal and an acceptable way of resolving conflict (Bandura, 1978; Bowes et al., 2013). Furthermore, there is evidence that exposure to family conflicts affects children’s ability to regulate their emotions resulting in overcontrolled emotional reactions that may contribute to externalizing problems (Fraga et al., 2022).
Parental mental health problems, including parental stress, depression, and ill mental health, have also been associated with an increased risk of both bullying victimization and perpetration (Nocentini et al., 2019; Shetgiri et al., 2015). Evidence suggests that the association between parental mental health problems and bullying might be mediated by poor parenting practices including inconsistent discipline and harsh parenting (Shetgiri et al., 2015). It has also been found that parents who experience higher stress and ill mental health are more likely to be exposed to domestic violence (Lereya & Wolke, 2013). In line with social learning theory, children who experience or observe violence at home may learn that the use of violence is an acceptable way of resolving conflict resulting in rejection and victimization from peers (Lereya & Wolke, 2013).
There is less consistent evidence on the role of parental reactions to bullying episodes and subsequent engagement in bullying perpetration and/or victimization. A recent systematic review found that parental acceptance of violence, positive attitudes toward bullying and victimization, and perceived lack of competence and self-efficacy to deal with the child’s bullying experiences were not consistently associated with a higher risk of bullying perpetration and/or victimization (Nocentini et al., 2019).
Adverse Childhood Experiences
Like bullying, ACEs have also been identified as a major public health threat (Baiden et al., 2020). ACEs encompass three broad categories of abuse (physical, emotional, sexual), neglect (physical, emotional), and household dysfunction (caregiver substance use, mental illness, divorce or separation, incarceration, domestic violence) (Felitti et al., 1998). The negative impact of ACEs on health was first documented in the late 1990s in a U.S. retrospective population-based study conducted by researchers at Kaiser Permanente and the Centers for Disease Control and Prevention (Felitti et al., 1998). The study was groundbreaking in that it revealed a high prevalence of ACEs in the general population and a significant dose-dependent relationship between ACEs and a broad range of negative outcomes including smoking, severe obesity, physical inactivity, depressed mood, and problem drinking (Felitti et al., 1998). Subsequent studies that examined the impact of ACEs on health outcomes among diverse samples of youth confirmed these initial findings showing that greater ACEs exposure is associated with greater health risk (Folk et al., 2023). The ACEs framework has been more recently criticized for an overreliance on meso- (family; e.g., domestic violence, divorce) system levels of influence while ignoring the effects of exo-level (extra-familial; e.g., community violence, discrimination, peer bullying) contexts that, according to Bronfenbrenner’s (1986) ecological model of human development, also influence child developmental processes (Folk et al., 2023).
The Link Between ACEs and Bullying
Research on the link between ACEs and bullying has been growing in recent years. A recent study by Hsieh et al. (2021) in Taiwan found that fourth grade children with higher levels of bullying perpetration reported more family violence and neglect at home and parental substance abuse than children who did not self-report as engaging in bullying perpetration. Children who had experienced these adverse experiences were more likely to report post-traumatic stress disorder symptoms and associated externalizing problems that increased the risk of exhibiting bullying perpetration toward others (Hsieh et al., 2021). The high prevalence of ACEs among young people involved in bullying as either victims or perpetrators was also confirmed in a study conducted in Brazil with older young people aged 15 to 19 (Reisen et al., 2019). The risk of ACEs was found to be cumulative in that the greater the exposure to adversities, the higher the likelihood of experiencing bullying victimization (Reisen et al., 2019). The negative association between ACEs and bullying involvement has been reported also among medium-high income families, suggesting that better socioeconomic circumstances do not act as a protective factor (Fraga et al., 2022). However, these studies had limitations as they relied on cross-sectional data and self-reports by children for both predictors and outcomes.
The Current Study
To address these limitations, this study used longitudinal data from a nationally representative cohort of young people from Scotland to evaluate the relationship between six different ACEs and the risk of being bullied or engaging in bullying others at age 14 using parental and child reports of ACEs. The study also aimed to explore the cumulative impact of ACEs on the risk of bullying victimization and perpetration in mid-adolescence. Given the sparsity of longitudinal research on ACEs and bullying (Merrin et al., 2023), this study fills an important gap in the literature that can have important implications for how bullying behavior is dealt with at schools. According to Merrin et al. (2023), while there is some evidence that some ACEs are linked to bullying involvement, it is unclear whether these positive associations extend to all ACEs or whether all ACEs are equally negative for both bullying victimization and perpetration. According to the dimensional model of ACEs and psychopathology by McLaughlin et al. (2014), ACEs can be grouped into threat and deprivation categories. Depending on their nature, different ACEs may influence peer interactions in different ways thus contributing to different types of involvement in bullying (Merrin et al., 2023). For example, young people experiencing parental neglect (i.e., deprivation category) are more likely to withdraw from peers compared to abused youth (i.e., threat category) leading to bullying victimization rather than perpetration (Merrin et al., 2023). Therefore, a more nuanced and comprehensive understanding of the link between ACEs and bullying victimization and perpetration is required (Merrin et al., 2023).
Methods
Data for this study was drawn from the first 10 sweeps of the Growing Up in Scotland (GUS) study, spanning the first 14 years of the young person’s life (Scottish Centre for Social Research, 2022). Funded by the Scottish Government, this study is a prospective social survey that tracks the lives of a cohort of Scottish children from infancy through to their teens and beyond collecting a range of information on cognitive, social, emotional, and behavioral development, health and well-being, childcare, education and parenting, and social networks (http://growingupinscotland.org.uk). Focusing initially on a cohort of 5,217 children, born between June 2004 and May 2005, the first wave of data collection took place in 2005/2006 when the children were 10 months old, comprising 80% of the eligible children (Bradshaw et al., 2007). These children were followed up annually between the ages of 10 months and just under 6 years, then every 2 years until they were aged 14. Families were selected at random from Child Benefit records provided by the Department for Work and Pensions and HM Revenue and Customs (HMRC) and received a letter inviting them to take part in the study. In cases where there was more than one eligible child in the selected household, one child was selected at random. In 2018, as part of sweep 9/age 12 fieldwork, an additional 502 children were recruited to address sample attrition. The additional sample was drawn from Child Benefit records held by HMRC. Children born between June 1, 2004, and May 31, 2005, and in at least one of the two key sub-groups that were under-represented (i.e., mother aged 16–24 at birth; living in 15% most deprived data zones in Scotland) were eligible for inclusion. Further details of the additional sample can be found in the sweep 9 user guide (Scottish Centre for Social Research, 2023a).
Data collection for sweep 10 took place in two phases between 2019/2020 with 2,669 children remaining from the initial birth cohort sample (51.2% of sweep 1). The Covid-19 pandemic necessitated that sweep 10 fieldwork be paused in March 2020 when it was approximately 80% complete. Fieldwork was restarted in May 2020 using an alternative methodology, where a computer-assisted web survey replaced the computer-assisted self-completion interview element and a telephone survey replaced the computer-assisted face-to-face in-home interview portion (Scottish Government, 2022). The GUS study has been ethically approved by the following bodies: The initial sweep of data collection was subject to medical ethical review by the Scotland “A” Multi-Centre Research Ethics Committee (application reference: 04/M RE 1 0/59). Up until and including sweep 8, subsequent annual sweeps have been reviewed via substantial amendments submitted to the same committee. Sweep 9 and 10 were subject to ethical review by the National Centre for Social Research Ethics Committee.
Measures
Adverse childhood experiences
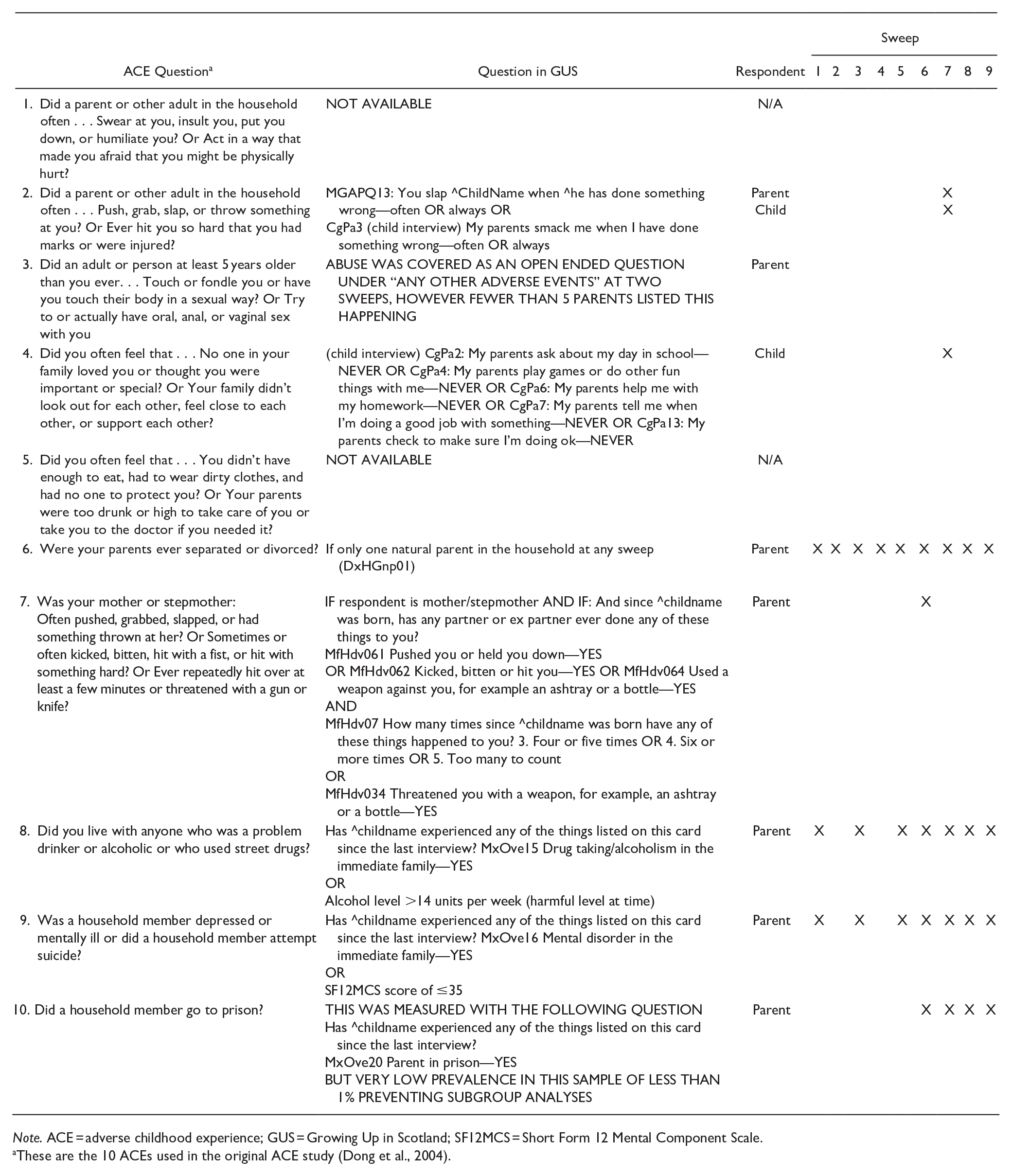
Data from across the first nine sweeps of the GUS study were mapped onto the original ACE questions (see Appendix A for the full details). Proxy measures of six ACEs were derived: physical abuse, domestic violence, drug or alcohol misuse, family mental illness, parental separation, and emotional neglect. Physical abuse was based on measures of the parent reporting slapping the child often or always or the child reporting experiencing smacking often or always. Domestic violence was measured by asking the mother/stepmother if any partner or ex-partner had pushed or held her down or kicked, bitten, or hit her at least four times since the child was born, or ever used a weapon against her. Drug or alcohol misuse was measured by asking the main caregiver whether the child had experienced drug taking or alcoholism in the family or if they reported drinking more than 14 units of alcohol a week. Family mental illness was a caregiver-reported measure of whether the child had experienced a mental disorder in the immediate family or if the main caregiver reported a high score (≤35) on the Short Form 12 Mental Component Scale. A child was coded as experiencing parental separation if there was only one natural parent living in the household at any of the first nine sweeps. Finally, emotional neglect was a child-reported measure consisting of five items that asked whether the parents were involved in different facets of the child’s life (e.g., play games with me, help me with my homework). If the child reported “never” in any of these five questions they were classified as experiencing emotional neglect. A measure for emotional abuse and physical neglect was not available. Sexual abuse was measured however fewer than five participants had responded positively to this, and it was thus excluded (Marryat & Frank, 2019). A measure of parental incarceration was available but excluded from the analyses due to the small number of children experiencing this (0.8% of the overall sample) that precluded subgroup analyses. A cumulative incidence of ACEs was derived by summing the ACEs present for each child across the study period.
Bullying Victimization and Perpetration
At sweep 10, children were asked for the first time in the study at the age of 14 how often they had picked on others by calling them names or making fun of them in a way that they didn’t like, leaving them out of games and chats, shoving, pushing, hitting, or picking a fight, or sending messages or posting things online. They were classified as engaging in bullying if they answered most days, about once a week or about once a month. A young person was classified as having experienced bullying if they reported having been picked on in any of the above ways most days, about once a week, or about once a month.
Covariates
Sex was coded as 1 = male and 2 = female. The ethnicity of the child was coded as 1 = White and 2 = other ethnic background. The Scottish index of multiple deprivation (SIMD) from sweep 1 was used to assess the socio-economic status of participants. The SIMD provides a relative ranking of the data zones in Scotland from 1 (least deprived) to 5 (most deprived) based on a weighted combination of data for seven domains: income, employment, health, education, skills and training, geographic access to services, crime and housing (Scottish Government, 2020).
Analyses
Binary variables of one or more ACE (vs. none) (1+ ACE) and three or more ACEs (vs. <3) (3+ ACEs) were derived. We used a cut-off point of 3 or more ACEs as this study collected information on only six ACEs. Univariable and multivariable logistic regression models were fitted predicting the odds of bullying perpetration and bullying victimization, respectively. Crude and adjusted odds ratios with 95% confidence intervals were calculated adjusting for sex, ethnicity, and socioeconomic deprivation. Subgroup analyses by gender were also performed. Nagelkerke R2 was used to determine the goodness of fit of the multivariate logistic regression models. Only cases with full data were used in the logistic regression analyses. Data were weighted using the longitudinal weights produced by the survey team, and the stratification of the sample was accounted for using the Complex Samples module within SPSS29.0.2.0 (IBM Corp., 2023). More detailed information on weighting is provided in the survey data user guide for Sweep 10 (Scottish Centre for Social Research, 2023b).
Results
Chi-square analyses (see Table 1) indicated that those lost to attrition (n = 2,548) were more likely to live in the most deprived areas of Scotland (χ2 = 169.45, p < .001) and in urban areas (χ2 = 50.03, p < .001) compared to those not lost to attrition (n = 2,669).
Proportion of Children Who Were Included or Missing at Sweep 10 by Demographic Characteristics.
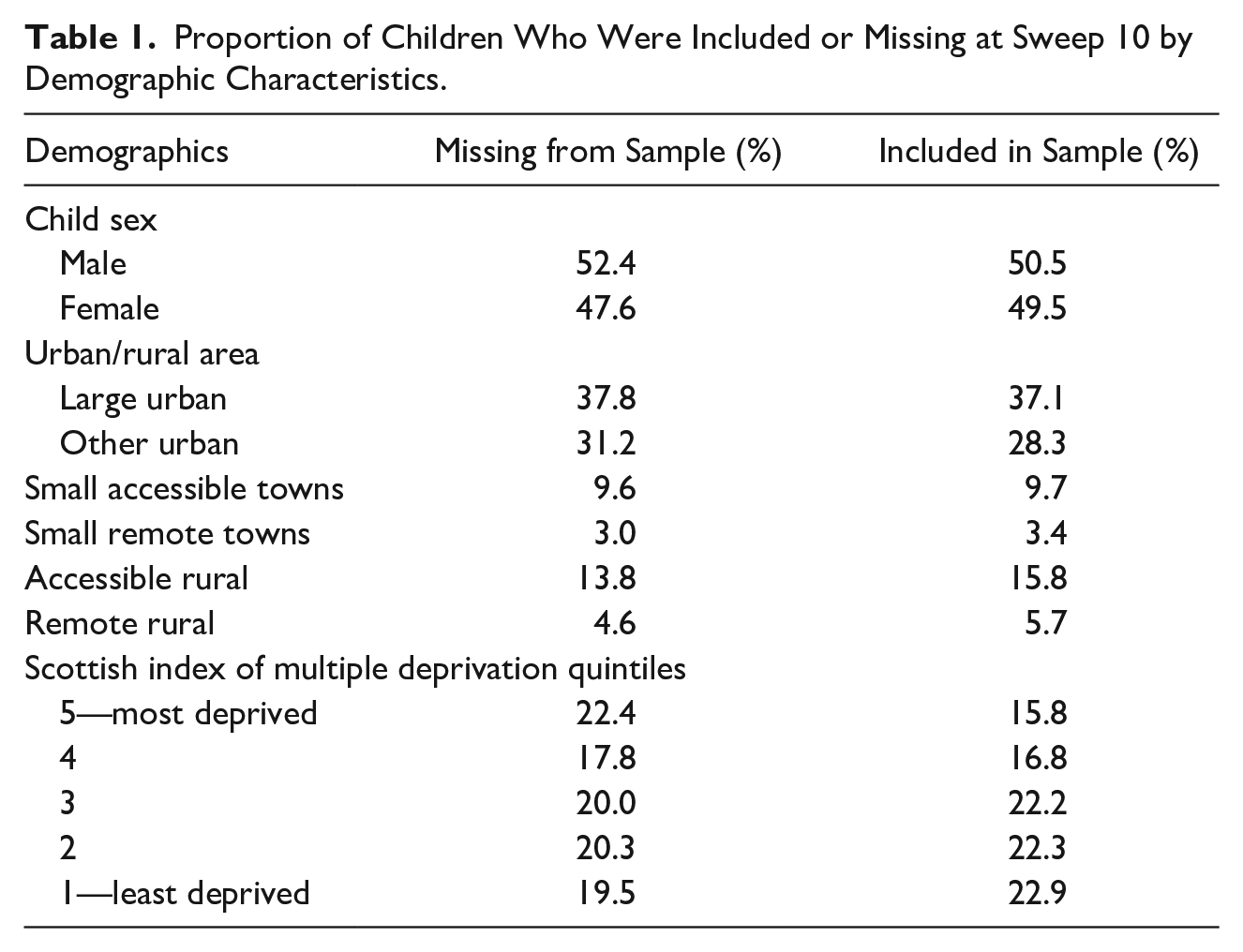
Around one-third (31%) of young people had experienced bullying victimization and 6.8% reported engaging in bullying others. More than two-thirds (73.6%) of young people had experienced at least one ACE, with 14% experiencing 3+ at age 14 (see Table 2). The most common ACEs were having parents who were separated or divorced (37.5%) and parental mental health problems (27.1%). There was also a high proportion reporting frequent physical punishment (22.5%) (see Table 2). ACEs did not significantly vary by sex but varied by SIMD area quintiles: 6.2% of young people in the least deprived areas had experienced 3+ ACEs compared with 22.2% in the most deprived areas (see Table 3).
Proportion of Children Reporting Each Experience.

Note. For the current study, don’t know and refused to answer were both re-coded as missing in order to get the most precise estimate of the known reported prevalence of the behaviors (yes this did occur). Thus, n’s vary slightly across analyses and rates may be underestimated. ACE = adverse childhood experience.
Proportion of Children in Each ACE Category by Sex and SES.

Note. Only one person answered “other” in the respondent’s sex question and was therefore removed from the analyses. ACE = adverse childhood experience.
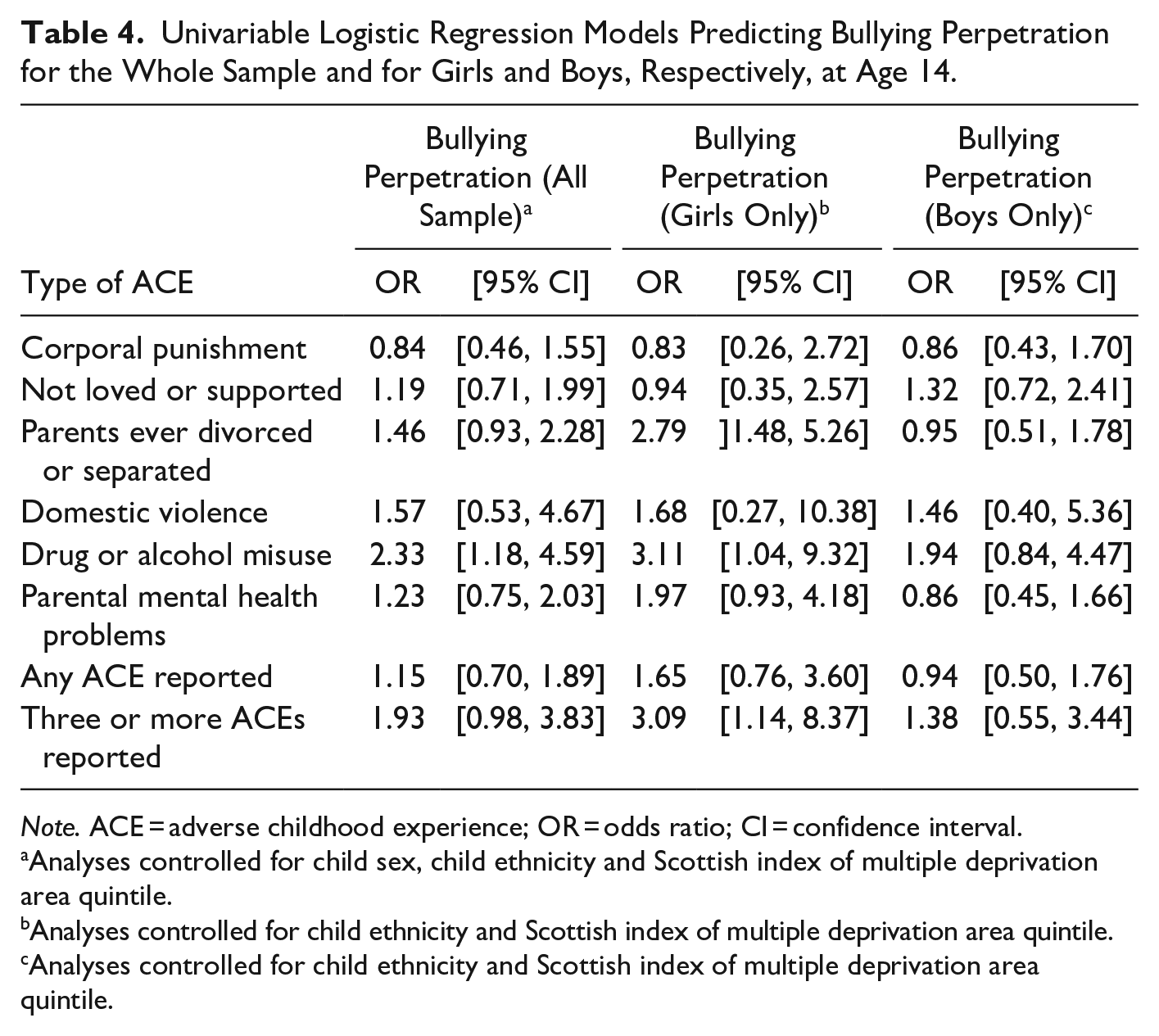
Independent associations were explored between each of the six ACEs measured, 1+ ACE and 3+ ACEs, and bullying perpetration and victimization, respectively (Table 4). Analyses controlled for sex, ethnicity, and SIMD area quintile. The only statistically significant predictor of bullying perpetration at age 14 was drug or alcohol misuse in the family (OR 2.33). However, this effect did not remain significant in the multivariate analysis (see Table 5).
Univariable Logistic Regression Models Predicting Bullying Perpetration for the Whole Sample and for Girls and Boys, Respectively, at Age 14.
Note. ACE = adverse childhood experience; OR = odds ratio; CI = confidence interval.
Analyses controlled for child sex, child ethnicity and Scottish index of multiple deprivation area quintile.
Analyses controlled for child ethnicity and Scottish index of multiple deprivation area quintile.
Analyses controlled for child ethnicity and Scottish index of multiple deprivation area quintile.
Multivariable Logistic Regression Models Predicting Bullying Perpetration for the Whole Sample and for Girls and Boys, Respectively, at Age 14.

Note. OR = odds ratio; CI = confidence interval.
Analyses controlled for child sex, child ethnicity and Scottish index of multiple deprivation area quintile.
Analyses controlled for child ethnicity and Scottish index of multiple deprivation area quintile.
Analyses controlled for child ethnicity and Scottish index of multiple deprivation area quintiles.
In subgroup analyses within each sex, significant effects were observed only among the female sample. Having parents who were divorced or separated (OR 2.79) and drug or alcohol misuse in the family (OR 3.11) significantly predicted the risk of bullying perpetration among females. Furthermore, those females who had experienced 3+ ACEs were three times more likely to engage in bullying compared to those who had experienced less or no ACE (see Table 4). In the multivariable model, only having parents who were divorced or separated remained a statistically significant predictor. According to this model, females who had experienced parental divorce/separation had 2.8 times higher odds of engaging in bullying (see Table 5).
Regarding bullying victimization, the only statistically significant ACE predictor was parental mental health problems (OR 1.39). Young people who had experienced parental mental health problems were 1.4 times more likely to experience bullying victimization compared to those who had not experienced this ACE. However, this effect did not remain significant in the multivariate analysis (see Table 7).
In subgroup analyses within each sex, significant effects were observed only among the female sample. Drug or alcohol misuse in the family (OR 2.97) and parental mental health problems (1.50) were the only ACEs that predicted the risk of bullying victimization in the female sample. Furthermore, those females who had experienced at least one ACE were 1.5 times more likely to report bullying victimization compared to females who had experienced no ACE (see Table 6). In the multivariable model, only drug or alcohol misuse in the family remained a statistically significant predictor. According to this model, females who had experienced drug or alcohol misuse in the family had 2.2 times higher odds of being a victim of bullying (see Table 7).
Univariable Logistic Regression Models Predicting Bullying Victimization for the Whole Sample and for Girls and Boys, Respectively, at Age 14.

Note. ACE = adverse childhood experience; OR = odds ratio; CI = confidence interval.
Analyses controlled for child sex, child ethnicity and Scottish index of multiple deprivation area quintile.
Analyses controlled for child ethnicity and Scottish index of multiple deprivation area quintile.
Analyses controlled for child ethnicity and Scottish index of multiple deprivation area quintile.
Multivariable Logistic Regression Models Predicting Bullying Victimization for the Whole Sample and for Girls and Boys, Respectively, at Age 14.

Note. OR = odds ratio; CI = confidence interval.
Analyses controlled for child sex, child ethnicity and Scottish index of multiple deprivation area quintile.
Analyses controlled for child ethnicity and Scottish index of multiple deprivation area quintile.
Analyses controlled for child ethnicity and Scottish index of multiple deprivation area quintile.
Discussion
This study found that a high proportion of young people in Scotland experience bullying victimization (31%). This percentage is similar to those reported in other countries (Biswas et al., 2020). A very high percentage of young people reported exposure to at least one type of adversity (73.6%). This result is slightly higher to the one reported in the study by Marryat and Frank (2019) that investigated prevalence of ACEs in the GUS study at age 8 (65%). This difference is not surprising given that there was more time in this sample to “accumulate” ACEs.
Regarding the link between ACEs and bullying, this study aligns with previous research that indicated heterogeneity across ACEs in terms of their associations with bullying perpetration and victimization (Merrin et al., 2023). In relation to bullying perpetration, drug or alcohol misuse in the family emerged as a statistically significant predictor of bullying perpetration in the overall and the female only sample and parental divorce/separation in the female only sample. There have been very few studies previously that have examined the association between this ACEs and bullying perpetration and their results have been mixed (Merrin et al., 2023; Morcillo et al., 2015). Interestingly, Morcillo et al. (2015) found in a sample of Puerto Rican children that caregiver substance use was positively associated to bullying perpetration. However, this association failed to reach statistical significance once child variables (i.e., early aggression, academic achievement) were added to the model. This suggests that differences in results may be attributable to methodological differences between studies including what factors they controlled for in the analyses (Merrin et al., 2023).
The finding that parental substance misuse increases the risk of bullying perpetration aligns with previous research that suggests bullying perpetration could be a means of externalizing anger, anxiety, or depression resulting from previous negative events in the family domain (Awad et al., 2021; Connell et al., 2016; Hsieh et al., 2021). Thus, our findings underscore the importance of further researching whether bullying perpetration should be considered a maladaptive way to manage life stressors (Connell et al., 2016).
The lack of a positive association between the two ACEs of physical abuse and domestic violence and bullying perpetration was somewhat surprising given that a recent systematic review found that most studies to date have reported a positive association between these two ACEs and bullying perpetration consistent with Bandura’s (1978) social learning theory (Merrin et al., 2023). The lack of a significant positive association in our study highlights the need to examine further protective factors that may mitigate the relationship between ACEs and bullying (Merrin et al., 2023).
Regarding bullying victimization, this study found that parental mental health problems are linked to a higher risk of experiencing bullying in the overall sample and among the female-only sample. The limited research that has been conducted on this ACE in the past has shown that parental mental health problems could promote lower social competence, lower self-esteem, higher anxiety, lack of social self-efficacy, and greater withdrawal in the child, consequently making them more vulnerable to bullying victimization (Azeredo et al., 2015). However, more research on the relationship between this ACE and bullying victimization is required (Merrin et al., 2023). Only three ACEs (physical abuse, emotional abuse, and witnessing domestic violence) have been shown to be consistently positively associated with bullying victimization in previous research (Merrin et al., 2023). Although emotional abuse was not measured in this study, the lack of a positive association between the two ACEs of physical abuse and witnessing domestic violence and bullying victimization in this sample could be attributed to the methodological features of this study (e.g., longitudinal design, lack of control for child variables).
The finding that divorce/separation was positively related to bullying perpetration (but not victimization) in the female sample, whereas parental mental health was positively related to bullying victimization (but not perpetration), supports the notion that the etiological mechanisms underlying the association between ACEs and bullying behaviors may differ across ACEs (e.g., threat- vs. deprivation-related ACEs; Felitti et al., 1998; McLaughlin et al., 2014; Merrin et al., 2023). Deprivation-related ACEs such as parental mental health problems could cause internalizing problems such as depression and anxiety increasing children’s vulnerability to bullying victimization (Felitti et al., 1998; Merrin et al., 2023). It is interesting that bullying perpetration in this sample was linked to both threat (i.e., parental substance misuse) and deprivation-related (i.e., divorce/separation) ACEs in the female sample. These findings underscore the importance of considering the specific nature of each ACE profile rather than simply grouping ACEs into categories when studying how they relate to bullying perpetration and victimization (Merrin et al., 2023).
Another important finding of the present study is that, among females, the higher the exposure to ACEs, the higher the risk of them engaging in bullying. However, this effect was not found within the overall sample or the males-only sample. This highlights the need to continue to investigate the cumulative impact of ACEs on bullying perpetration and victimization rather than focusing on single factors. Indeed, a recent systematic review found that only a few studies to date have examined cumulative ACE scores in relation to bullying behaviors (Merrin et al., 2023).
Finally, this study revealed some important gender differences in the associations between ACEs and bullying. Stronger associations were found between ACEs and bullying among females than among males. Also, cumulative ACE predicted bullying perpetration only among females but not males. This is in contrast to previous research that found the cumulative risk of ACE to be more strongly associated with school violence perpetration among males compared with females (Forster et al., 2020). Our finding is surprising given that females are more likely to seek out support in response to stress compared with males (Forster et al., 2020). Given the conflicting findings, research should continue to investigate gender differences in the associations between ACEs and bullying and potential protective factors that may mitigate some of the effects of ACEs on males.
Strengths and Weaknesses
This study is one of the first to use prospective data on ACEs collected from both parents and children to analyze associations with bullying perpetration and victimization in a current generation of children. The original ACE questionnaire was not included in the GUS study and therefore proxy measures of ACEs had to be used, which may not accurately reflect the ACE questionnaire. Two ACEs (emotional abuse and physical neglect) were not measured through the GUS study. In addition, the percentage of parents disclosing sexual abuse and parental incarceration was so low that we were not able to include these ACEs in our analyses. Furthermore, it is possible that due to social desirability some parents did not disclose ACEs that were occurring. Therefore, the GUS study may have underestimated the prevalence of ACEs. Also, as a result of significant attrition in the GUS study, a more socioeconomically advantaged group of participants was included in this study. Nevertheless, as previous studies have observed, the inclusion of the more disadvantaged group is likely to only widen the observed differences (Fraga et al., 2022). Another limitation of our study was that our analyses only controlled for sex, ethnicity, and level of socioeconomic deprivation of the area in which the participants lived. We did not control for the change in interview mode due to the Covid-19 pandemic and this should be acknowledged as a limitation as mode of interview might have an influence on the rate of disclosure of sensitive information (Pickard & Roster, 2020). Also, this study did not measure bully victims which are problematic given the significant overlap between bullying perpetration and victimization (Merrin et al., 2023). Finally, the results of this study cannot be generalized to other countries.
Implications of Findings
The evidence base on the effectiveness of universal anti-bullying programs is weak to modest at best particularly in adolescence (Gafney et al., 2019; Merrin et al., 2023; Salmivalli et al., 2021). There is also evidence that universal anti-bullying programs are not effective for all children (Hogye et al., 2022). Furthermore, as Merrin et al. (2023) point out, these programs often fail to address the needs of those experiencing bullying and perpetrate it against others. Therefore, by providing further evidence on the link between ACEs and bullying, this study has implications for improving the quality and effectiveness of anti-bullying interventions.
First, our findings point to the need for interventions to strengthen parent-child relationships to prevent bullying (Hogye et al., 2022; Huang et al., 2019; Ttofi & Farrington, 2012). This includes not only parenting programs but also the critical need to ensure that responsibility for problems borne out of structural inequalities is not erroneously misplaced on individual families (Jahanshahi et al., 2022; Walsh, 2020).
Further, given the associations between ACEs and bullying found in this and previous studies, early screening for ACEs could help accelerate early prevention of bullying (Merrin et al., 2023) although Walsh (2020) cautions against interventionist state activities that stigmatize and pathologize children, parents, and families especially as the literature consistently shows a link between socioeconomic deprivation and ACEs.
Finally, findings from this study highlight the potential of integrating trauma-informed and strengths-based approaches into anti-bullying prevention and intervention initiatives with the aim of avoiding retraumatizing young people (Blitz & Lee, 2015; Merrin et al., 2023; Taylor & Siegfried, 2005). As part of this, educators would receive training on identifying distress symptoms among young people and developing a better understanding of the causes and effects of trauma in children’s lives (Blitz & Lee, 2015). This includes developing an understanding of how common ways of interaction at school, such as using an authoritative voice, can trigger an unconscious memory or association with family violence that can then, in turn, trigger heightened responses from children and contribute to bullying behaviors (Blitz & Lee, 2015). Trauma-informed approaches aim to ensure that educators do not ask “what is wrong” with the child but instead “what happened” to the child (Blitz & Lee, 2015). Also, within these approaches, parents are seen as partners and have an active role in the school community (Blitz & Lee, 2015).
However, trauma-informed approaches have been criticized in the literature as being easier to talk about than operationalize in practice (Lemke & Rogers, 2022). Limitations have also been reported in relation to the under-researched role of educators in trauma-informed practice and how the intersection of trauma and minority identities is addressed within trauma-informed practice (Alvarez, 2020; Thomas et al., 2019).
This suggests that there is a need for more research into how trauma-informed approaches can be operationalized within school settings and how they can become more effective. There is also a need for more research on the effects of trauma on young people who are involved in bullying as both perpetrators and victims. Finally, more longitudinal studies should investigate the cumulative impact of ACEs on bullying using more advanced multivariate methods that can also identify the mediators and moderators of the associations between ACEs and bullying.
Footnotes
Appendix A: Measurements Derived from GUS Study
| ACE Question a | Question in GUS | Respondent | Sweep | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |||
| 1. Did a parent or other adult in the household often . . . Swear at you, insult you, put you down, or humiliate you? Or Act in a way that made you afraid that you might be physically hurt? | NOT AVAILABLE | N/A | |||||||||
| 2. Did a parent or other adult in the household often . . . Push, grab, slap, or throw something at you? Or Ever hit you so hard that you had marks or were injured? | MGAPQ13: You slap ^ChildName when ^he has done something wrong—often OR always OR |
Parent |
X |
||||||||
| 3. Did an adult or person at least 5 years older than you ever. . . Touch or fondle you or have you touch their body in a sexual way? Or Try to or actually have oral, anal, or vaginal sex with you | ABUSE WAS COVERED AS AN OPEN ENDED QUESTION UNDER “ANY OTHER ADVERSE EVENTS” AT TWO SWEEPS, HOWEVER FEWER THAN 5 PARENTS LISTED THIS HAPPENING | Parent | |||||||||
| 4. Did you often feel that . . . No one in your family loved you or thought you were important or special? Or Your family didn’t look out for each other, feel close to each other, or support each other? | (child interview) CgPa2: My parents ask about my day in school—NEVER OR CgPa4: My parents play games or do other fun things with me—NEVER OR CgPa6: My parents help me with my homework—NEVER OR CgPa7: My parents tell me when I’m doing a good job with something—NEVER OR CgPa13: My parents check to make sure I’m doing ok—NEVER | Child | X | ||||||||
| 5. Did you often feel that . . . You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you? Or Your parents were too drunk or high to take care of you or take you to the doctor if you needed it? | NOT AVAILABLE | N/A | |||||||||
| 6. Were your parents ever separated or divorced? | If only one natural parent in the household at any sweep (DxHGnp01) | Parent | X | X | X | X | X | X | X | X | X |
| 7. Was your mother or stepmother: |
IF respondent is mother/stepmother AND IF: And since ^childname was born, has any partner or ex partner ever done any of these things to you? |
Parent | X | ||||||||
| 8. Did you live with anyone who was a problem drinker or alcoholic or who used street drugs? | Has ^childname experienced any of the things listed on this card since the last interview? MxOve15 Drug taking/alcoholism in the immediate family—YES |
Parent | X | X | X | X | X | X | X | ||
| 9. Was a household member depressed or mentally ill or did a household member attempt suicide? | Has ^childname experienced any of the things listed on this card since the last interview? MxOve16 Mental disorder in the immediate family—YES |
Parent | X | X | X | X | X | X | X | ||
| 10. Did a household member go to prison? | THIS WAS MEASURED WITH THE FOLLOWING QUESTION |
Parent | X | X | X | X | |||||
Note. ACE = adverse childhood experience; GUS = Growing Up in Scotland; SF12MCS = Short Form 12 Mental Component Scale.
These are the 10 ACEs used in the original ACE study (Dong et al., 2004).
Acknowledgements
The author would like to thank two anonymous reviewers for their constructive comments on an earlier version of this manuscript.
Data Availability Statement
Restrictions apply to the availability of the data that support the findings of this study which were used under special license from the U.K. Data Archive Service (Project No 244263).
Declaration of Conflicting Interests
The author declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author received no financial support for the research and/or authorship of this article.
Ethical Approval
The Growing Up in Scotland study has been ethically approved by the following bodies: The initial sweep of data collection was subject to medical ethical review by the Scotland “A” Multi-Centre Research Ethics Committee (application reference: 04/M RE 1 0/59). Up until and including sweep 8, subsequent annual sweeps have been reviewed via substantial amendment submitted to the same committee. Sweep 9 and 10 were subject to ethical review by the National Centre for Social Research Ethics Committee.