
Abstract
Strangulation involves the application of force to the neck to restrict blood flow or breathing. It is often utilized in both homicides and non-fatal incidences of coercive control, interpersonal altercations, and sexual assaults. The intention of this study was to provide a comprehensive understanding of interpersonal fatal strangulation in Australian adults through the documentation and analysis of characteristics and circumstances involved in these fatalities. Currently, there is limited research within this field in Australia leading to a medico-legal knowledge deficit that needs to be rectified to ensure public health intervention and preventative death policies and initiatives. Researchers conducted a retrospective review of all closed interpersonal strangulation coronial cases within Australia between 2000 and 2021 using the National Coronial Information System online repository. Researchers identified 195 cases to be included in the study. Strangulation currently accounts for 1.1% to 5.8% of all assault fatalities in Australia per year. Most victims of strangulation are women (68.2%), under the age of 45 (52.3%), and Anglo-European (73.3%). Most individuals are killed by someone they know (89.2%), often in the context of intimate partner violence (52.3%). The leading cause of death within the sample is directly related to the strangulation (90.8%), and the leading manner of death is homicide (94.4%). The study is the first of its kind to utilize descriptive forensic epidemiology to explain the circumstances and characteristics of fatal interpersonal strangulation in Australia providing an Australia-specific medico-legal voice to aid in future research, policy development, and criminal prosecution. The findings within this study are foreseen to contribute to improvements in public health policy surrounding fatal and non-fatal strangulation and assist future medico-legal death investigations, and provide LGBTQ+ and Indigenous Australian representation, which has not been considered in previous studies.
Introduction
Strangulation is a form of asphyxia in which force is applied to the neck (Christensen et al., 2014; Saukko & Knight, 2023). It can occur in various circumstances, including sexual homicide, interpersonal violence, fatal and non-fatal intimate partner violence, and during consensual and non-consensual sex (e.g., see: Douglas et al., 2024; Mcquown et al., 2016; Petreca et al., 2023; Ressler et al., 1998).
Difficulties arise when attempting to differentiate accidental death during “rough sex” and deaths associated with homicidal intent (Bows & Herring, 2020; S. S. M. Edwards et al., 2023; Sowersby et al., 2022). Difficulties also arise when strangulation deaths are staged as suicides or autoerotic accidents, and differentiation can be challenging for death investigators (Geisenberger et al., 2019; Kumar & Kohli, 2019; Leth & Vesterby, 1997; Mallach & Pollak, 1998).
Common causes of death due to strangulation include airway occlusion creating a hypoxic environment within the brain, restriction of vascular networks of the head and neck resulting in stroke, intracranial hemorrhage from increased intracranial pressure, and cardiac complications from vagal stimulation (Dunn, 2025; Saukko & Knight, 2023).
Strangulation often occurs within the setting of intimate partner violence or interpersonal violence. The standard paradigm suggests that female victimization is common, and those who identify as women, are under the age of 50, and have previous experience of intimate partner violence are more likely to be killed, with men being the common perpetrators (Behera & Sikary, 2021; Glass et al., 2008; Marty et al., 2022; Nordrum et al., 1998; Sanford et al., 2006; Sorenson et al., 2014; Suffla & Seedat, 2016). However, some studies highlight that this is not always true as Maxeiner and Bockholdt, 2003, Verma and Lal (2006), and Wahlsten and Eriksson (2020) have highlighted that men of various ages compose the majority of victims in circumstances of interpersonal violence they have researched. However, men are still the most likely perpetrator. Research by Verma and Lal (2006) posited that cultural dimensions of violence may influence victimology with female victimization being common in the West, while male victimization is common in the East. This suggests that geographic location and culture may be drivers of strangulation fatality differences. The pernicious nature of strangulation is outlined by Glass et al. (2008), who found that 43% of all completed homicides against women in domestically violent situations had previously involved some form of non-fatal strangulation. Furthermore, Glass et al. (2008) report an “over seven-fold odds (OR 7.48, 95% CI 4.53–12.35)” of individuals who have previously experienced strangulation at the hands of an intimate partner becoming homicide victims.
Numerous countries report strangulation as one of the most common forms of violent asphyxial death, including Finland (Wahlsten & Eriksson, 2020), Germany (Maxeiner & Bockholdt, 2003), Norway (Nordrum et al., 1998), Australia (Mouzos & Thompson, 2000), South Africa (Suffla & Seedat, 2016), India (Behera & Sikary, 2021; Srivastava et al., 1987; Verma & Lal, 2006), Iran (Karimi et al., 2017), China (Ma et al., 2016), and the United States of America (Sanford et al., 2006).
Medico-legal Challenges
The investigation of a person’s death holds much social and moral currency and is essential in providing closure to those impacted by death (Ranson & Bugeja, 2017). Death investigation is a culturally relative process and is unique to the locality in which it is practiced (Ranson & Bugeja, 2017). In Australia, approximately 12% of all deaths fall under the purview of the Coroner and are subject to investigation, including an individual whose death is related to various forms of strangulation (National Coronial Information System [NCIS], 2024).
The Coroner’s duties are both judicial and investigative. The Coroner, if able, must ascertain the facts surrounding any reportable death within Australia. This can include the identity of the deceased, the cause and manner of death of the deceased, the time and location of the death, and any other information that may be pertinent to the individual’s case (Freckelton & Ranson, 2006; Phillips et al., 2015). In Australia, the presiding Coroners are optimally placed to contribute to (and recommend) public health interventions to reduce preventable deaths. Coroners can provide recommendations through public and private inquests (Saar et al., 2017; Sutherland et al., 2014). Such investigations are undertaken as a “search for the truth” (Freckelton & Ranson, 2006, p. 531). Coroners aim to create a non-adversarial and supportive environment to understand the circumstances surrounding a person’s death and how other similar deaths can be prevented in the future through legislation, education, and advocacy (Freckelton & Ranson, 2006).
Greater knowledge of the circumstances and characteristics of fatal interpersonal strangulation in Australia holds valuable potential for legislation creation and policy reform.
To allow for effective communication and identification of phenomenon currently impacting community members and their ability to live a full life and prevent premature death, there is a need for standardized and communicable epidemiology surrounding strangulation. As strangulation occurs during sex consensually, during sexual assault, in circumstances of coercive control, during workplace accidents, and suicides, it is evident that the phenomenon requires specific attention within an Australian context. By understanding the circumstances and characteristics of strangulation in Australia, future death investigation and homicide monitoring can be improved. With in-depth knowledge of the circumstances and characteristics of strangulation in Australia, medico-legal teams will be well placed to provide a variety of services to the public moving forward including measures to decrease preventable deaths, increased antemortem identification of strangulation-related crimes, advanced knowledge to assist with prosecution of such crimes, and provide public health education on the risks of both consensual and non-consensual strangulation.
Study Aims
This study intends to provide a comprehensive examination of deaths resulting from interpersonal strangulation in Australia. Through a review of interpersonal strangulation deaths reported to Australian Coroners, the study will describe the circumstances and characteristics of interpersonal strangulation deaths in Australia and provide a current Australian perspective on the phenomenon.
Methodology
Database Selection
The researchers used the NCIS to retrospectively identify all interpersonal strangulation cases reported to the Coroner within Australia (https://www.ncis.org.au). The NCIS was selected due to its association with forensic medicine and coronial inquest. While there are other databases and reporting methods in Australia such as the Australian Institute of Criminology National Homicide Monitoring Program (AICNHMP) (https://www.aic.gov.au/), the NCIS was chosen due to their data collection methodology, continuous review of cases, and data availability. The two are also closely related with the NCIS being utilized to inform the Australian Institute of Criminology’s reports of homicide deaths and deaths in custody in Australia. Additionally, researchers also wished to include information related to accidental deaths due to strangulation such as those that occur during consensual sexual activity, as well as more in depth descriptions of antemortem, perimortem, and postmortem events. The researchers found the inclusion of demographic data, autopsy reports, coronial findings, toxicology reports, and police narrative of circumstances advantageous and allow the investigation of researcher-created variables. The AICNHMP presents data predominantly from police reporting and homicide squad investigations, whereas the NCIS reports coronial findings, which were more in line with the authors public health messaging as the AICNHMP (Mouzos, 2002) acknowledge findings by Scott (1990) and the AICNHMP state that “it is important to be aware that police documents cannot be considered as neutral documents, and they cannot be usefully employed in social science if they are not considered in the context of the author’s intentions.” The incorporation of other findings available in the NCIS database allow for better control of bias and aimed for neutrality while acknowledging that perfect neutrality does not exist.
Case Search and Inclusion
Researchers retroactively identified all “closed” and “quality assured” (cases that are confirmed to have correct coding by the NCIS unit see: https://www.ncis.org.au/about-the-data/quality-management) cases of interpersonal strangulation-related deaths in Australia between the years 2000 and 2021. Researchers created search queries using multiple variables to screen for inclusion, including age, mechanism of injury, and intention, in addition to the specific search terms “strangulation” and “neck compression.”
To be included in the study, individuals must have (a) had their case recorded in the NCIS database, (b) be 18 years or older at the time of their death, and (c) strangulation must have been noted as the cause of death or as a contributing cause of death. One hundred and ninety-five cases (n = 195) were included in the study.
Case Review
Once cases were screened for inclusion eligibility, the circumstances and characteristics of the strangulation fatality were documented (where possible) using available coronial findings, police narratives of circumstances, toxicology reports, autopsy reports, and any relevant supplementary reports (contained within autopsy reports) from forensic practitioners, including pathologists, anthropologists, and radiologists.
Once documentation from the NCIS case file was complete, each case was assessed for completion, and missing variable information was assessed. Variables such as sexual orientation or gender presentation are not always collected during the coronial investigation, and thus, researchers manually searched through the case file to find such information from case reports and data matching protocols.
When information surrounding victim–perpetrator relationships and the gender of the perpetrator were missing from the NCIS case file, additional data matching protocols using court reporting agencies were enacted to ensure that the maximum amount of data could be included. There were occasionally inconsistencies within court reporting such as variations in perceived relationship between the perpetrator and victim (such as one noting the perpetrator as a “friend” and the other as a “boyfriend/girlfriend” of the victim, or where there were multiple perpetrators and victim–perpetrator relations were not known for everyone). Data for such variables were only noted if the individual was convicted of the crime and if the verdict had not been overturned by the time of this publication. Additionally, some variables (researcher-created variables) such as manner of death, population affinity, sexual orientation, victim–perpetrator relationships, and employment status were coded and interpreted by the authors and involved the combination of multiple codes from the NCIS database as well as consideration of reports from autopsy, police, and coronial findings.
It was important for the authors to include sexual orientation within the study due to the lack of LGBTQ+ violence literature (K. M. Edwards et al., 2015). However, coding of such information was difficult, and therefore, additional information surrounding coding may be beneficial to the reader of this article. For the purpose of this research, a yes/no binary of “documented LGBTQ+” was created. This acknowledges those in which sexual orientation or gender nonconforming transitions were integral to the case investigation and/or their identity while also acknowledging the nuance and fluidity of sexual orientation, consequences of outness, and an inability to speak posthumously about sexuality. There are multiple scenarios in which individuals may have been LGBTQ+, which were not documented during life or during the coronial investigation (see discussion and limitation sections). A series of seven factors were considered when documenting LGBTQ+ identity within the study including: (a) the pronouns family, friends, and the coroner used to describe the decedent, (b) documented history of gender non-conformity with the sex they were assigned at birth, (c) NCIS and autopsy reporting of sex, (d) police narrative of circumstances, (e) when the sexual orientation of the individual was directly noted in coronial findings, (f) history of partners included both males and females and was documented in coronial findings or police narrative of circumstances, and (g) the gender of the last partner they had or the partner they were in a relationship with at the time of their death.
For all variables when information was not available in the NCIS case file and was not found during the data matching process, the information was noted as “not ascertained,” “not noted,” “unknown,” or “not recorded,” depending on the variable or the circumstances.
Statistical Analysis
Finally, statistical analysis was conducted using IBM SPSS (Version 29.0) to understand the epidemiology of the circumstances and characteristics of strangulation in Australia. Descriptive statistics (e.g.,: measures of frequency, measures of central tendency, proportions, and averages) were generated for each variable in which data were collected.
Ethics
Ethics approval was granted by the Justice Human Research Ethics Committee (ID: CF/23/15818) and the University of Melbourne Human Research Ethics Committee (ID: 2023-26998-43339-3). Ethical requirements dictate that small frequencies are masked to protect the decedent's identity and confidentiality. These frequencies have been noted as “<5.”
Results
Victim Characteristics
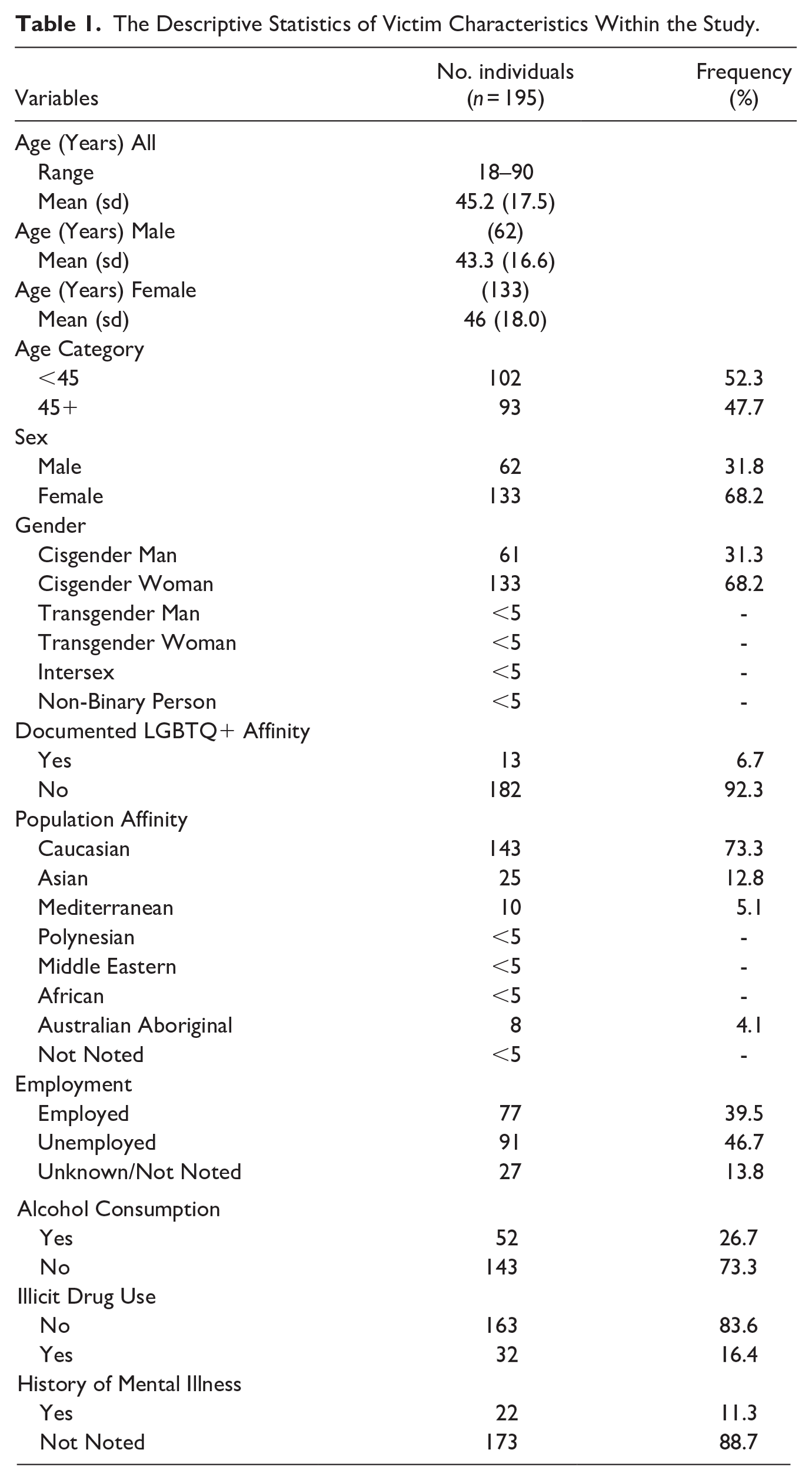
Table 1 explores victim characteristics surrounding fatal interpersonal strangulation in Australia between 2000 and 2021. The age range varied in the study, with victims ranging from 18 to 90 years old. The average age of fatality was 45.2 years, with some minor variations in average age at death when separated by biological sex. The group most impacted by strangulation deaths were those between 40 and 49 years of age (Figures 1 and 2), and most individuals were cisgender women (68.2%). When reviewed against the AICNHMP, the demographic characteristics that are available in both the NCIS and the AICNHMP are relatively consistent indicating a strong ability for each to build upon information supplied by the other to create holistic interpretations of homicide and preventable violent deaths in the future even though all NCIS data must travel through coronial pathways, while AICNHMP data does not have the same requirements.
The Descriptive Statistics of Victim Characteristics Within the Study.
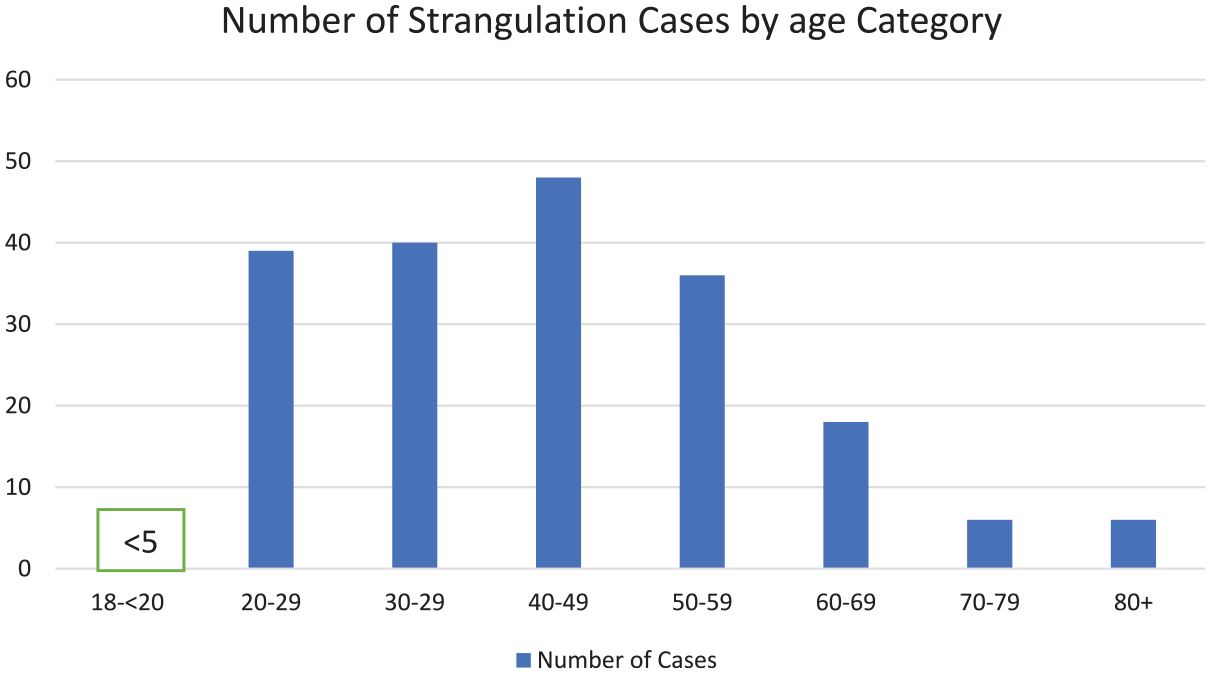
The number of fatal interpersonal strangulations by age category.
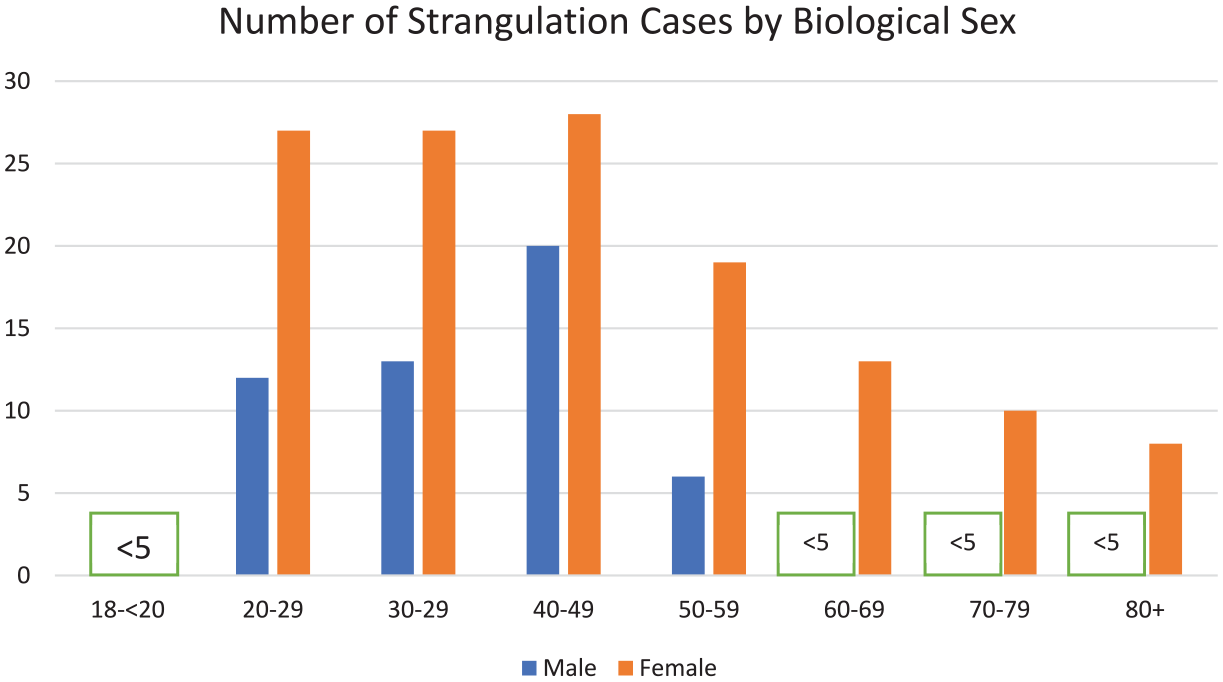
The number of fatal interpersonal strangulations by age category and sex.
Population affinity varied within the sample. Most individuals within the sample were Caucasian (73.3%). Aboriginal and Torres Strait Island peoples accounted for a small portion of the sample (4.1%) but were still overrepresented compared to the general population.
Within the sample, 6.7% of individuals were known to be LGBTQ+.
Almost half (46.7%) of decedents were unemployed at the time of their death. Most of those who were unemployed were pensioners, retired, were unofficial carers, or carried out home duties.
The documented presence of mental illness within the sample was uncommon (11.3%) when compared to the documented prevalence in the Australian population (22%) (Australian Bureau of Statistics [ABS], 2024), with anxiety and depression being the most noted mental illnesses.
Drug and Alcohol Use
Illicit drug use by victims was uncommon within the sample (16.4%). Toxicology screening in these individuals commonly reported the presence of cannabis and methylamphetamines.
Blood toxicology screening highlighted the presence of ethanol in approximately one-quarter of all decedents (26.7%). Individual blood alcohol concentration varied.
Circumstances and Contexts
A variety of circumstantial and contextual information was documented by the researchers (Table 2) to understand the situations in which fatal interpersonal strangulation is occurring in Australia.
The Descriptive Statistics of the Circumstances and Context of Fatal Interpersonal Strangulation in Australia.
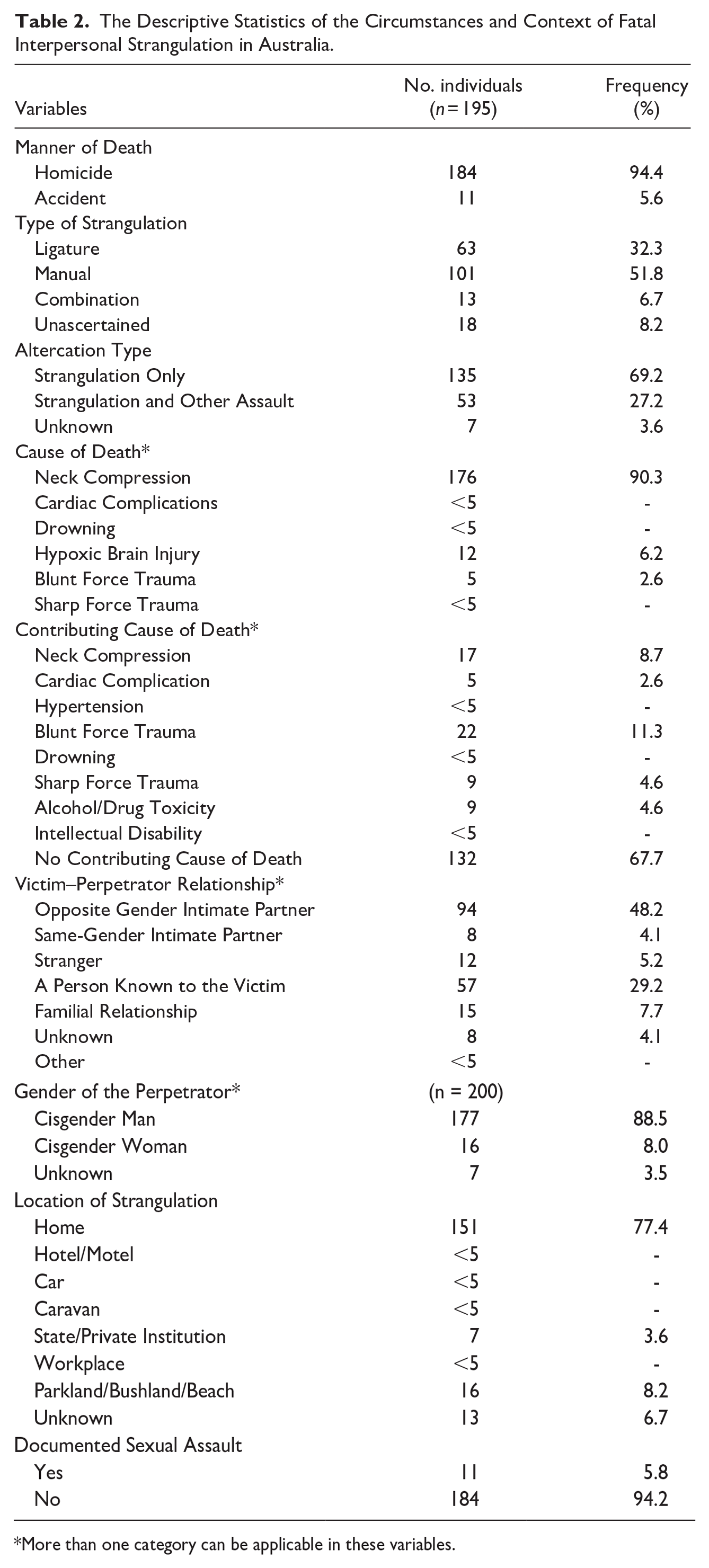
More than one category can be applicable in these variables.
Strangulation-related homicides contributed to between 1.1% and 5.8% of documented homicides between the years 2000 and 2021 (Figure 3). These findings are consistent with the Australian Institute of Criminology National Homicide Monitoring Program. Individuals were killed in a variety of circumstances, including during disputes, episodes or intimate partner violence, breakups, hate crimes, and during consensual and non-consensual sexual intercourse.
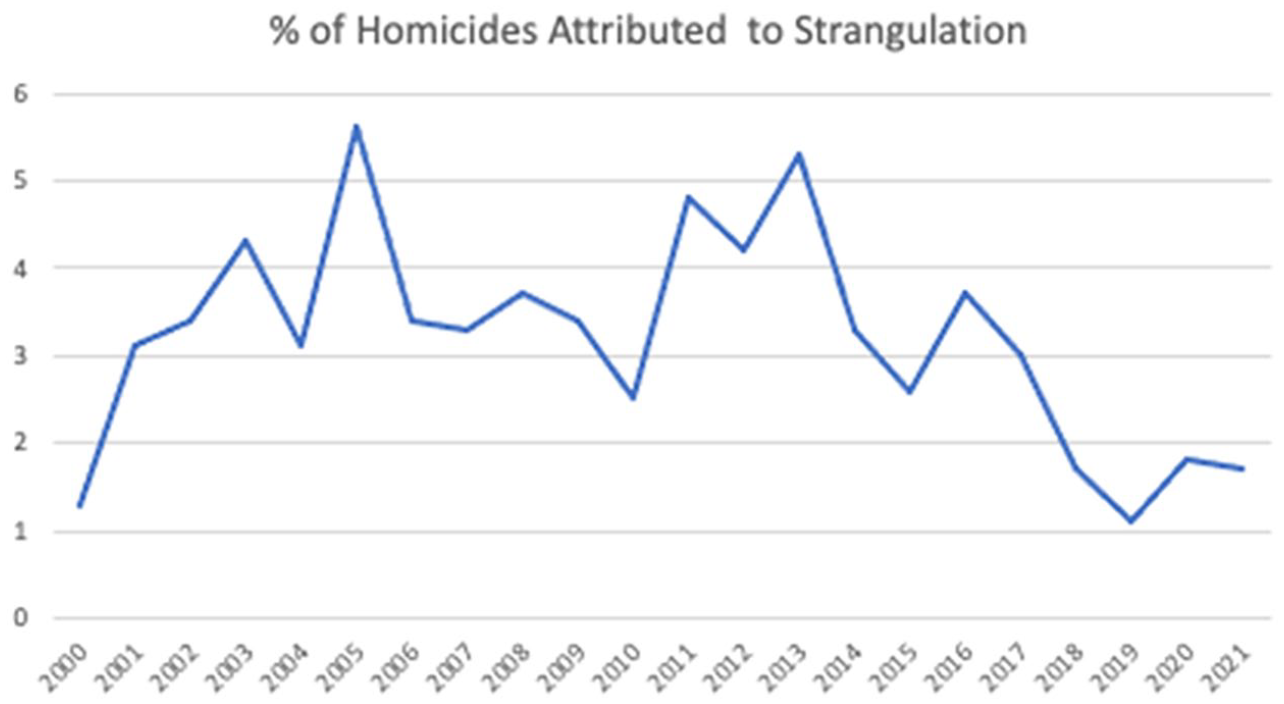
The percentage of homicides attributed to strangulation in the years 2000 to 2021.
Approximately three-quarters of all individuals were killed within the home (77.4%).
The time of strangulation was recorded when the time was documented and verified (N = 158). Most individuals were killed during the hours of 18:00 to 06:00 (Figure 4). The beginning of the week (Sunday to Tuesday) also accounted for a disproportionately higher number of fatalities (Figure 5), and autumn was the most common season for strangulations (Figure 6).
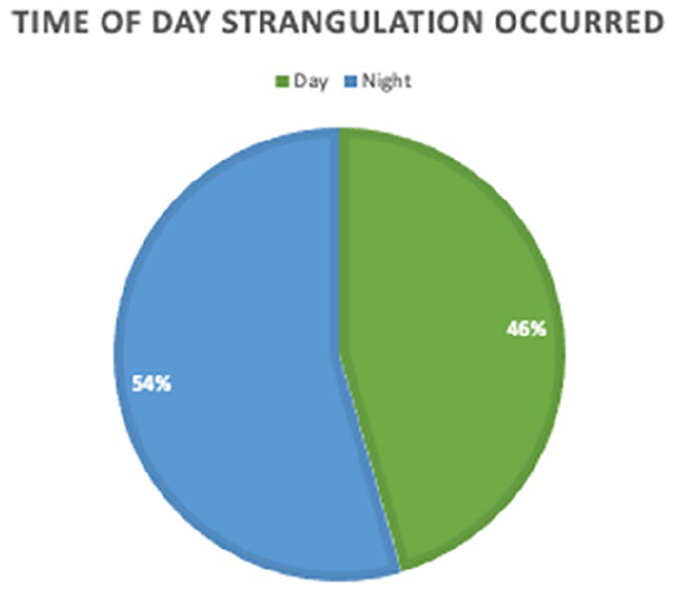
Pie chart displaying the time of day in which strangulation occurred as categorized by day (06:00–18:00) and Night (18:00–06:00) in cases where time of day was recorded (N = 158).
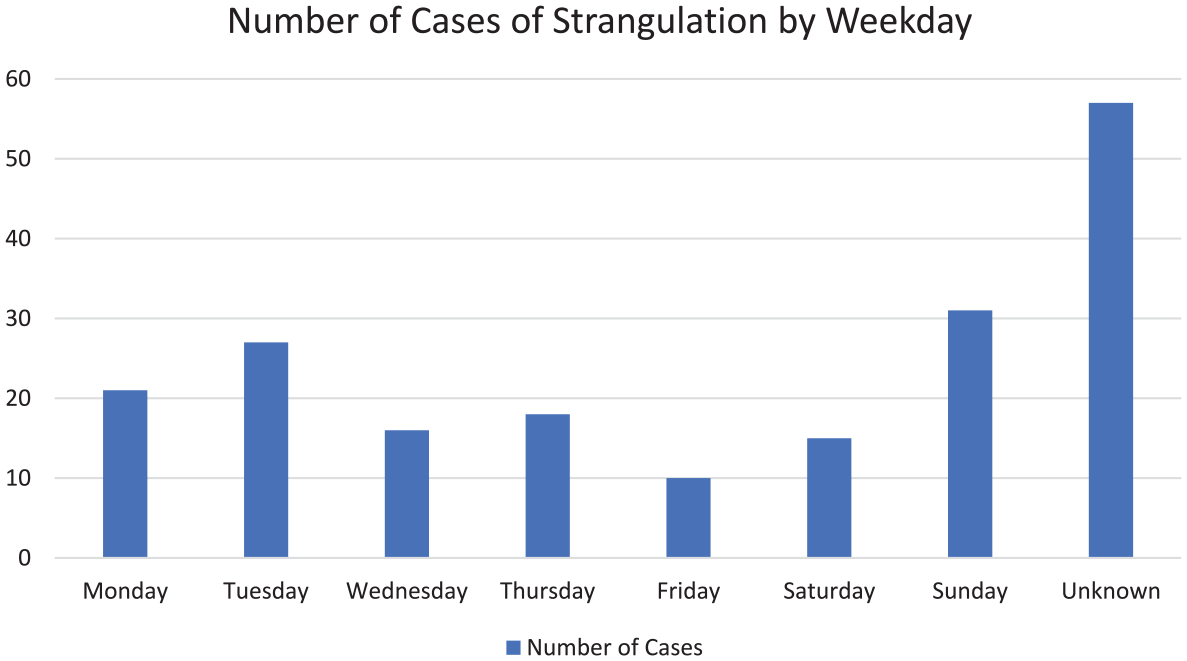
Bar chart displaying the number of strangulation cases by weekday.
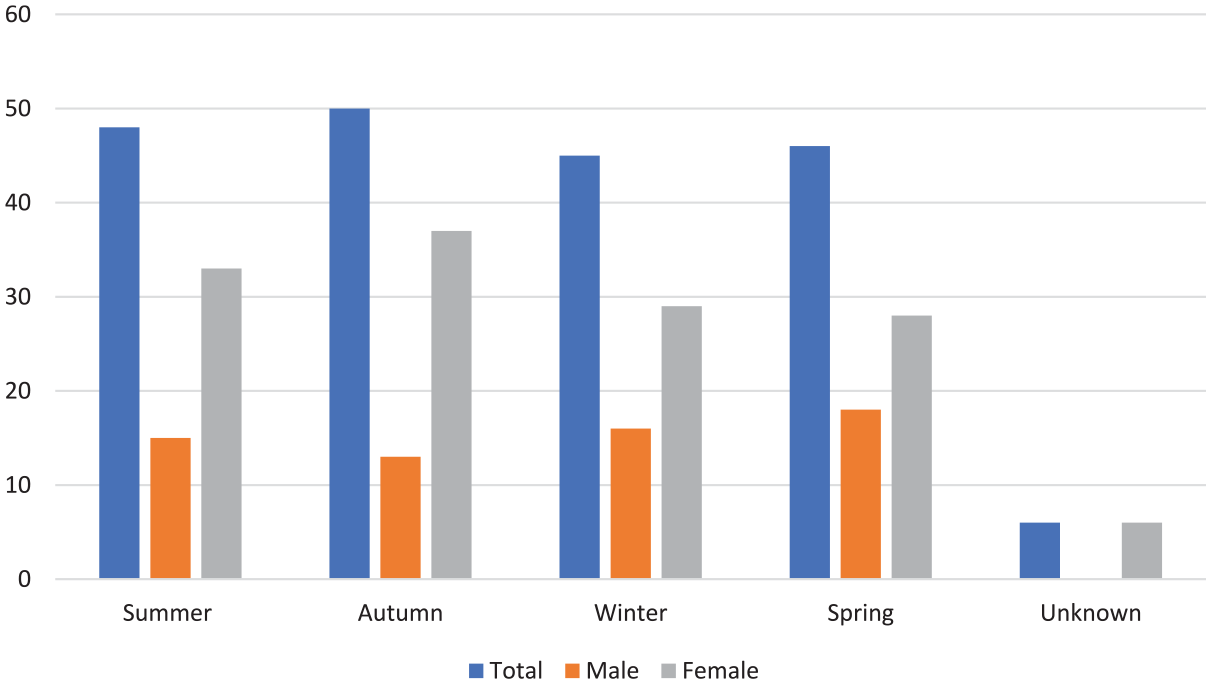
Bar chart displaying the season in which the fatal strangulation occurred by total strangulation cases and by biological sex.
Strangulation Event
Most deaths (90.3%) were directly attributed to strangulation as a primary cause of death. However, other methods of assault, including stabbing (n < 5), drowning (n < 5), or blunt force trauma (5.6%), were experienced by the victim during the fatal assault. Manual strangulation was the most common form of strangulation (51.8%), followed by ligature strangulation (32.3%). Most perpetrators who utilized manual strangulation used their hands or arms. Most ligatures used by perpetrators included everyday household objects such as electrical cords, scarves, belts, and cable ties. However, other implements such as bondage collars or instrument strings were also used.
A considerable majority of perpetrators were male (88.5%), and victims were often strangled by someone they knew (89.2%), with over half of all perpetrator–victim relationships being that of intimate partners (52.3%). Of the 102 cases that occurred between intimate partners, over one-third of perpetrators (37.3%) had previously been involved in intimate partner violence that had been documented by police or emergency services or had been disclosed to family or friends. Of the individuals who had previously been victims of documented cases of assault, 26.3% had previously been strangled by their intimate partner.
In some cases of strangulation (5.8%), there was evidence of perimortem or postmortem sexual assault. While penetrative sex between the victim and perpetrator was noted in these scenarios, there were other instances where sex toys or other objects were also used to assault the victim.
Causes and Contributing Causes of Death
Table 2 demonstrates that in most cases, the cause of death was attributed to some form of strangulation or neck compression. Almost all individuals were noted to have neck compression as the primary cause or contributing cause of death (99%).
Discussion
Victim Characteristics
The study examines the circumstances and characteristics of fatal interpersonal strangulations in Australia and builds upon existing international literature surrounding the phenomenon of strangulation and neck compression deaths. Sex and gender appear to play a role in strangulation homicides. To say that strangulation is a gendered crime would be proportionately appropriate and pertinent when considering all aspects of interpersonal strangulation. Women bear the burden of strangulation (Behera & Sikary, 2021; Glass et al., 2008; Marty et al., 2022; Nordrum et al., 1998; Sanford et al., 2006; Sorenson et al., 2014; Suffla & Seedat, 2016), and this study presents no exception highlighting that individuals who socially present as women, regardless of biological sex, are at risk of fatal strangulation in Australia.
In keeping with research internationally, most individuals were strangled by people they knew. Most fatalities from interpersonal strangulation are perpetrated by an intimate partner or family member. The variation in gender composition in the study is staggering highlighting that women are at a much-increased risk of fatality due to strangulation. Most women within the study were fatally strangled by their current or former intimate partner. A significant proportion of individuals within this study had previous episodes of intimate partner violence indicating a potential predisposition for fatal strangulation in the future. Additionally, previous strangulation attempts prior to fatality were also documented. The study highlights a failure of safe reporting strategies and necessary medico-legal intervention to prevent further harm to these individuals. While some only reported previous violence and/or strangulation to friends or family members, some reported to police or were documented in emergency room settings.
This highlights the complex sociocultural drivers of strangulation and coercive control loops, in which the individual may return to the aggressor or may still be vulnerable. Some individuals within the study were killed when threatening to leave their spouse or while in the process of leaving indicating the dissolution of relationships as a high-risk activity for fatal interpersonal strangulation. Additionally, research by Mcquown et al. (2016) who examined presentations at the sexual assault and domestic violence evaluation center from 2004 to 2008 presented a lethality risk of 97% for those who had experienced strangulation indicating that even if the first episode of strangulation was not fatal, additional violence may prove fatal in the future.
The authors within this study concur that previous intimate partner violence and previous strangulation present high lethality risk in the future evidenced by documentation of previous violent assault within this study. The authors also note that due to difficulties surrounding disclosure such as shame, stigma, fear of repercussions, and control outlined by Montalvo-Liendo (2008) and Alaggia et al. (2012), the rate of previous intimate partner violence is likely underestimated. This indicates the need for better identification, documentation, and treatment of non-fatal strangulation and provision of equitable resources to those most likely to experience strangulation.
LGBTQ+ people presented at a representative level when compared to their estimated incidence in the Australian population (Wilson et al., 2020; Wilson & Temple, 2021) and LGBTQ+ men were more likely to be strangled by their intimate partner than LGBTQ+ women. These trends are mirrored by Harland et al. (2021) who highlight that gay and bisexual men had significantly higher odds of reporting physical or sexual intimate partner violence than heterosexuals and males. The findings suggest that strangulation-related violence may have considerable and currently unrecognized impacts on the LGBTQ+ men. Reports of strangulation in living LGBTQ+ individuals were also recorded by Messing et al. (2018; 2021), highlighting emerging literature on potential risks of LGBTQ+ people in fatal and non-fatal strangulation assaults. Hate crimes, relationship rivalries, and interpersonal altercations also contributed to the death toll. The authors concur with Messing et al. (2018; 2021) and Edwards et al. (2015) that there is a significant lack of LGBTQ+ representative literature, which may lead to increased risk for LGBTQ+ people and failure of detection. Groups such as LGBTQ+ people have been historically excluded from research and have been subjects of intergenerational criminalization (Bull et al., 1991; Gerber, 2014), medicalization (see: Psychopathia Sexualis (von Krafft-Ebing, 1886)) (Bennett & Brickell, 2018; Giami, 2023), and institutionalization, which may lead to decreased likelihood of detection or reporting.
Age at death varied within the study. Across current literature, the age range varies for strangulation-related crimes (Behera & Sikary, 2021; Maxeiner & Bockholdt, 2003; Sanford et al., 2006; Suffla & Seedat, 2016; Verma & Lal, 2006; Wahlsten & Eriksson, 2020); however, most agree that women under the age of 50 are most at risk; this study provides no exception.
The authors posit multiple factors that can influence gendered aspects of strangulation-related deaths. Sociocultural expectations of women in contemporary Western society, their experiences of violence, the perceived social value of women, and associated feminine performance, may contribute to the increased death told among women for strangulation-related violence (Casique Casique & Ferreira Furegato, 2006). Additionally, as discussed by Tittlová and Papáček (2018), the emancipation of women and the feminist movement have changed the role of women significantly enabling women to have more dominant positions which men may be uncomfortable with. Men may then resort to abuse to regain perceived power and control over the relationship. Multiple scenarios recounted by coronial findings and police narrative of circumstances would suggest that jealousy over income disparity, female independence, and changing expectations of the family dynamic may have resulted in increased strangulation and coercive control.
Murder and murder/suicide pacts in geriatric and terminally ill people, and accessibility to weaponry may contribute to variations in age at death both within this study and in international findings. Examples of each scenario were recorded in this study, adding to existing literature surrounding sociocultural dynamics as a plausible explanation for strangulation.
Most individuals were Anglo-European or Caucasian. This is consistent with the population of Australia; however, Anglo-European peoples are underrepresented, making up approximately 90% (ABS, 2021) of the population but only 73.3% of the study population. Considering census data collected by the ABS (2021), underrepresentation continued within Asian populations. Aboriginal and Torres Strait Island peoples are overrepresented in the cohort, representing 4.1% of individuals in the study and only 3.8% of individuals in the Australian population (ABS, 2021), indicating an increased risk for this population. Reasoning surrounding this overrepresentation may include racism (Cave et al., 2019; Durey, 2010; Kairuz et al., 2021; Temple et al., 2020), intergenerational trauma (Australian Institute of Health and Welfare, 2024), and lack of culturally and linguistically specific resources (Australian Institute of Health and Welfare, 2022; Collins et al., 2022; Shepherd et al., 2018). The culmination of these factors has created an environment in where there are not appropriate interventions within the Australian medico-legal system to assist Aboriginal and Torres Strait Island peoples resulting in increased fatality due to strangulation. The lack of assistance, failure of interventions (Sharman, Douglas et al., 2024), racism (Cave et al., 2019; Durey, 2010; Kairuz et al., 2021; Temple et al., 2020), and intergenerational trauma from colonization (Australian Institute of Health and Welfare, 2024) may have deleterious impacts on the mental health of Aboriginal and Torres Strait Island peoples. Issues surrounding reporting of intimate partner violence, perceived seriousness of intimate partner violence, and fear of repercussions after reporting may also impact the decision and ability for Aboriginal and Torres Strait Island to seek care and intervention (Ingram, 2016; Guggisberg, 2018; Spangaro et al., 2018). Such discussion have also been mentioned by Sharman, Douglas et al. (2024) in their difficulty recruiting and representing Indigenous communities within their study. The authors propose that these factors may lead to Aboriginal and Torres Strait Island women being at increased risk of repeated and fatal violence. Facilitation of culturally sensitive and specific interventions for Aboriginal and Torres Strait Island communities regarding interpersonal strangulation are needed to combat the disproportionate fatalities due to strangulation-related violence.
Within this space, culturally sensitive and specific interventions could be designed through a collaborative approach with Aboriginal and Torres Strait Island peoples. Yarning circles to discuss the impacts of violence and how medical providers could better cater to Aboriginal and Torres Strait Island peoples may provide an avenue for culturally safe training and practice, which may increase service provision and uptake among the community. Similar work within the field of oral health has been investigated by Collins et al. (2022) and has provided useful insights regarding collaborative approaches, co-design, positionality of the practitioner, and active listening. These ideas can be further compounded by reproductive coercion and abortion discussion undertaken by the Queensland Health and Clinical Excellence Queensland (2024) who contend that precise language use, listening, and the value of lived experience are essential in improving Aboriginal and Torres Strait Islander health and closing the gap between Indigenous people and their non-indigenous counterparts. As explored by Guggisberg (2018), community, kinship, and social standing are inextricably linked to Indigenous women’s identity, and thus, consideration surrounding intervention should also consider this. Without these considerations, Aboriginal and Torres Strait Island peoples may avoid healthcare having deleterious consequences on care and future intervention in circumstances of interpersonal and intimate partner violence.
The culmination of intergenerational and complex trauma coupled with the lack of culturally relevant mental health interventions disallow for the appropriate management of mental ill health and poor culturally-relative coping mechanism which may increase episodes of intimate partner violence (Choe et al., 2008; Ingram, 2016; Guggisberg, 2018; Spangaro et al., 2018). It must be recognized that intimate partner violence, colonialism, and lack of equity in all services heavily contribute to a disproportionate load on Indigenous communities, and further culturally relative and co-designed methods for harm minimization and intimate partner violence identification and intervention need to be created.
Contextualizing Fatal Strangulation
Considering the context and associated risk factors of strangulation, it is vital to identify circumstances, actions, or behaviors that may increase an individual’s risk of being a victim of fatal strangulation. Within the study, there were at least 200 perpetrators of strangulation. Men were the perpetrators of most strangulations within the study (88.5%) and are documented as the primary perpetrators of strangulation globally (Glass et al., 2008; Institute for Addressing Strangulation, 2024; Petreca et al., 2023). In cases with multiple perpetrators, this usually consisted of a male–male or male–female pairing in which both individuals participated in the strangulation or incapacitation of the victim. There were no instances of a female–female pairing where two women strangled an individual together, and strangulations perpetrated solely by women were uncommon. Biological assumptions may assist in explaining this scenario. Due to the biological restrictions of cisgender women’s bodies, such as muscle strength (Kanehisa et al., 1994), coupled with decreased average height (Franco, 2016) and neck girth when compared to men (Amir et al., 2019; Vasavada et al., 2008), the perpetration of strangulation, particularly against men, may be difficult and other methods of homicide may be selected by women instead. This may also explain the phenomenon of women recruiting men to assist with fatal strangulation, which was documented within this study.
Social constructs such as power, patriarchy, and models of coercive control may also lead to increased strangulation perpetration by men (Bows & Herring, 2020; Douglas et al. 2024). Power, patriarchy, and coercive control as related to strangulation are social phenomena that are deeply entrenched within society and have been influenced by longstanding cultural and societal expectations of men. Strangulation is often used by men in sexually motivated homicides to exert power and control over their victim (Petreca and Patch, 2024, Kim et al., 2023). Strangulation allows for close quarter and intimate contact with the victim as well as psychological and physiological arousal associated with ideas of dominance and control. Additionally, the social value placed on men and longstanding cultural acceptance of violence without repercussions may lead to engrained ideas of misogyny and perceived low value of women compared to the men who victimize them. Through strangulation, “the offender quite literally has the victim’s life or death at their fingertips” (Petreca & Patch, 2025, p. 11). Additionally, there are “blurred lines” (Douglas et al., 2024) between sex and violence as it relates to strangulation, which could also contribute to sociological ideas of power and entitlement by perpetrators.
Manual strangulation was the most prevalent method of fatal interpersonal strangulation. Manual strangulation may be used rather than ligature strangulation because one's body parts are the most accessible weapon. This can be explained by the weapon of opportunity hypothesis, which suggests that one is likely to use weapons that are the easiest to acquire (Kim et al., 2023; Ressler et al., 1998). The majority of strangulation-related deaths within this study have occurred spontaneously, meaning that there does not appear to have been in depth premeditation or planning. This phenomenon is described by Petreca and Patch (2024) as “spontaneous homicide” and refers to a time of heightened negative emotion such as jealousy, panic, or anger (Hill & Hill, 2002) that may then result in fatal consequences. It is important to note that the unplanned nature of crime certainly does not negate that it has occurred or that justice must be dispensed by the appropriate authorities. However, this explanation of violent strangulation is not supported in circumstances where stalking and premeditated sexual assault have been involved or the planned killing of intimate partners by perpetrators.
Socio geo-temporal examination indicated that the home was an area of elevated risk of perpetration of strangulation-related violence as it provides a secluded area in which violence can be inflicted with a decreased likelihood of consequence due to failure or delay of detection. Seclusion, isolation, and ostracization are common methods of coercive control used by perpetrators of domestic, family, and intimate partner violence settings (Bailey et al., 1997; Hegarty et al., 2000; Patch et al., 2022; Stark, 2009) explaining the potential preference for violence in the home. Other areas of social isolation, such as bushland, were also used for strangulation, particularly in cases where the individual was not known to the victim and crimes appeared to be opportunistic. This suggests that physical isolation may be an enabler for perpetration of opportunistic strangulation-related assaults due to the perceived decreased probability of detection.
Chronology was assessed on various levels: annually, seasonally, daily, and multi-hourly. However, few conclusions can be drawn due variability of documentation for each case. One trend is that fatal strangulation events often occurred in the evening or night. This is unsurprising as during these times, individuals spend more time at home, and there is an increased likelihood of alcohol consumption providing ample opportunity for altercations. Room et al. (2013) show drinking is most common in the evenings and weekends which would be consistent with the time of day when strangulation occurs. Considering alcohol and its relation to lowered inhibitions and aggression, an increased likelihood of violence is possible (Beck & Heinz, 2013). Individuals who have consumed alcohol may find it more difficult to fend off their attacker due to neurological and motor function (Kim et al., 2023). Additionally, low amounts of alcohol can also cause vasodilation (Kudo et al., 2015), which can make individuals more susceptible to injury due to physiological responses of the body.
Victim Alcohol and Illicit Drug Use
Victim alcohol and drug use were uncommon within the sample. Alcohol was present in the minority of the study population. Higher levels of inebriation may have impaired neurological and cognitive function (Varghese & Dakhode, 2022), leaving victims at increased risk of fatal strangulation. Consumption of drugs and alcohol may lower cognitive, and psychomotor function making individuals easier to restrain during altercations, enabling fatal strangulation due to the individual’s reduced ability to fend off the perpetrator (Houa et al., 2011; Sullivan et al., 2010). Additionally, drug toxicity from cannabis or methamphetamine (which were the most illicit drugs used by decedents prior to death) may lead to life-ending cardiac or neurological complications during or after the strangulation assault (Kevil et al., 2019; Subramaniam et al., 2019). So, while the perpetrator may not have intended to kill the victim, and rather restrain or incapacitate them, in some scenarios, the consumption of drugs may have exacerbated physiological stress responses outlined above, killing the victim.
Cause and Manner of Death
The almost unanimous notation of strangulation as a cause of death or contributing cause of death was expected. However, the notation of strangulation was not standardized. As Petreca et al. (2023) contend, strangulation may be part of an assault with other forms of blunt force trauma, sharp force trauma, or other mechanisms of homicide. This may make it difficult to determine the true role that strangulation has played in the cause of death. The study depicts several scenarios in which strangulation was the direct cause of death, and where consequences of strangulation such as hypoxia or cardiac complications caused death, which is in line with findings proposed by Dunn (2025). The study highlights that while strangulation itself is dangerous, additional consideration must be given to scenarios in which strangulation may exacerbate existing injury or illness resulting in death. In some scenarios, strangulation was used as an incapacitation technique before final cause of death such as blunt force trauma or drowning.
Alternative modes of killing were also used, with perpetrators noting the length of time strangulation took as a demotivating factor for continuation. Some perpetrators reported strangling their victims for 15 minutes or more, which, given discussions by Sauvageau et al. (2010) surrounding unconsciousness and death from strangulation occurring within minutes, seems unnecessary. It is also possible that perpetrators may have overestimated the amount of time they spent actively strangling the victim. Sauvageau et al.’s (2010) findings juxtapose perpetrator assumptions about the amount of time it may take to kill their victim. However, when considering the amount of time it may take to kill someone with a firearm, incised wounds, or blunt force to the skull, minutes may in fact be a demotivating factor when killing could occur within seconds.
While in the minority, some individuals died due to rough sex. These deaths which were found to be accidental. Emerging literature (Sharman et al. 2025) suggests that strangulation during sex is becoming more common, particularly in younger generations. Sharman et al. (2025) and Herbenick et al. (2022), highlight the alarming trend of increased strangulation practices during sex. Whether the trend is increasing or whether individuals are now more sex-positive and disclosure occurs more often is unknown, and little baseline data exist to explore the phenomenon. This, coupled with the increased ease of access and consumption of violent pornography, may create a challenge for future medico-legal practitioners. Lack of education, inability to regulate the consumption of pornography by individuals, and poor preventative measures of safety within the sex industry may create unrealistic expectations surrounding consensual strangulation, posing a threat to those who are engaging in such activities.
When investigated, individuals who have died during consensual sex (and their partners) were unaware of the severe consequences associated with strangulation, and surviving perpetrators noted such activities were taking place regularly in their sex life. Cases of accidental death during sex were seen in a wide range of scenarios including during opposite-sex and same-sex pairings, BDSM activities, group sex, and sex while intoxicated or using illicit substances. The breadth of activities documented in the study coupled with opinions posited by Sharman et al. (2025), Herbenick et al. (2022), and Bows and Herring (2020) highlight the danger posed by strangulation during sex and the potential for further “rough sex” defense scenarios. Widespread safer-sex education may be advantageous in proactively managing preventable deaths. Additionally, instances of fatal interpersonal strangulation during sexual intercourse usually involved ligatures and additional forms of asphyxiation such as ball gags, harnesses, and manual strangulation. Men were more likely to die from accidental strangulation during sex than women, which is contrary to current reporting: however, it is consistent with individuals who die from autoerotic asphyxia or autoerotic neck compression (Mullin et al., 2024, Sauvageau and Racette, 2006). Death of men during sex may be due to higher rates of consumption of commercial sex works and riskier BDSM behavior. Further research into the phenomenon is required to elicit valuable conclusions.
In most cases, manner of death determinations were straightforward. However, there were some instances in which the manner of death was obscured through stages scenarios such as suicidal hangings, exercise accidents, and car accidents, adding to the existing body of literature of staged and simulated cause of death to obscure homicide. When manners were obscured, injuries often highlighted the preponderance of strangulation. The importance of holistic examination of strangulation epidemiology and injury patterns was highlighted in these cases.
Strengths and Limitations
This study has multiple strengths. The study is the first of its kind to examine interpersonal strangulation deaths in Australia. This allows for the contextualization of strangulation deaths and confirmation of anecdotally held beliefs within the medico-legal community. The study also presents the opportunity to “learn from the dead,” a highly valued opportunity in death studies, epidemiology, and public health. The study demographically outlines risk groups and behaviors that may lead to an increased risk of fatal strangulation and provides information that may assist in the identification, documentation, and prosecution of strangulation in living populations.
However, the study is not without limitations. As is the nature of retrospective analysis, researchers can only analyze the information provided, and the more time that has elapsed since the case, the more difficult it is to acquire additional information from credible sources. A significant amount of information was missing when assessing sexual orientation, day of strangulation, and time of strangulation. When information was missing, it has been noted as “not noted” or “unascertained.” The addition of this information would have been beneficial in providing a robust overview of the above listed variables. This was particularly difficult when discussing sexual orientation as individuals may have been bisexual or gay, and this may not have been known or investigated at the time of the coronial inquest. Sexual orientation and relationships are complex, and there are multiple scenarios including polyamory, infidelity, shame, or stigma that may impact findings. For example, individuals may have self-identified as gay, married a woman, and had extramarital relationships with men, or individuals may have been bisexual but have only dated women in recorded history. These scenarios as well as multiple others mean that LGBTQ+ people are most likely underrepresented within the sample.
The researchers also combined various codes from the NCIS database to create codes for researcher-created variables such as manner of death, victim–perpetrator relationship, population affinity, and employment. While both researchers reviewed each case to code and categorize each researcher-created variable, there is still the possibility of bias that must be noted which could impact the results.
Finally, the sample size (n = 195) is small, and more data points may be beneficial. A large-scale, multinational study focusing on strangulation would remedy the deficit.
Conclusions
This study provides a comprehensive examination of the characteristics and circumstances surrounding interpersonal fatal strangulation in Australian adults. The study examined 195 cases of adult interpersonal strangulation fatalities within Australia between 2000 and 2021. The study highlights that there are key demographic factors that are at increased risk of strangulation, including women, those who are Aboriginal and Torres Strait Islanders and those who have previous experience with intimate partner violence. Groups such as the LGBTQ+ community are also at risk (Sharman et al., 2025a), and further research needs to be done to understand the pervasiveness of strangulation within this community fully.
This study demonstrates the pressing need for continued research, policy development, and community education to combat the lethal consequences of interpersonal strangulation. By addressing the identified gaps and leveraging these insights, stakeholders, including healthcare practitioners, forensic practitioners, and those in positions of influence, can work toward reducing the incidence of strangulation-related deaths and ensure safer communities for all Australians.
Footnotes
Acknowledgements
The authors would like to acknowledge the National Coronial Information System (NCIS) Unit for their continued assistance. The authors would also like to acknowledge the Justice Human Research Ethics Committee and the University of Melbourne Human Research Ethics Committee for their feedback and approval of ethics. The authors would like to acknowledge the NCIS as the database source of data, and the Victorian Department of Justice and Community Safety as the organization source of data. Finally, the authors would like to acknowledge the support of the Brian and Ann Dooley Trust for their generous PhD scholarship/stipend that enables the PhD studies of Mr. Scotia Mullin. The PhD Candidate Mr. Scotia Mullin would like to thank the Australian Research Training Program for their support and the Melbourne Dental School Internal Student Research Grants Program for their contribution to funding this project. The authors would like to acknowledge and thank Professor Alastair Sloan and Professor Kelsey Hegarty for their ongoing support and supervision of Mr. Mullin.
Author Contributions
Scotia Mullin (SM), Rita Hardiman (RH): Conceptualisation, SM.; draft methodology preparation, SM., methodology refinement SM and RH; formal analysis, SM and RH; investigation, SM and RH; resources, SM; data curation, SM.; writing—original draft preparation, SM; writing—review and editing, SM and RH; visualization, SM; supervision, RH; funding acquisition, SM and RH. Both authors have read and agreed to the published version of the manuscript.
Data Availability
Due to the nature of this study and agreements between the researchers and the National Coronial Information System, and the outline of data control and handling policies outlined in ethics applications, the data for this research are not available, cannot be disseminated, and are not accessible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was funded by the Melbourne Dental School Internal Student Research Grants Program, the Brian and Ann Dooley Trust, and the Australian Research Training Program.