
Abstract
Studies largely from high-income countries show that children exposed to intimate partner violence (IPV) face potential adverse health and developmental outcomes. Limited research has focused on whether IPV exposure affects children’s early education participation, particularly in low- and middle-income countries where early education is gaining traction. This study examines whether young children aged 3 to 5 years, living in households affected by IPV, are less likely to be enrolled in school using nationally representative data from India. The study involved secondary analysis of data from the fifth round of the National Family Health Survey (NFHS-5), a demographic and health survey conducted in India, which provided data on 19,822 children aged 3 to 5 years. Univariate and multivariable logistic regression models were utilized to explore the relationship between child exposure to IPV and early education enrollment. Our findings from the univariate regression model show that children from households where women reported experiencing IPV were less likely to enroll in early education (OR = 0.83, 95% CI [0.73, 0.94]), and these findings remained significant even after adjusting for child-level covariates (e.g., child sex and age, other young children in the household) (adjusted OR = 0.81 [0.71, 0.92]). However, after further adjusting for household-level demographic confounders, this significant association was lost. These findings demonstrate that IPV in the household may affect children’s participation in early education, but observed effects may be explained by greater socioeconomic vulnerability in households in which IPV is occurring. These findings suggest that programs supporting child entry into early education should not simply target socioeconomically vulnerable households, but they may also need to support women in children in these households who may be vulnerable to violence.
Introduction
Intimate partner violence (IPV), characterized as multiple forms of harm (e.g., physical and sexual) caused by a current or former partner, is a widespread problem that disproportionately affects women (United Nation, 1994). Although it has received significant attention in the past few decades, IPV remains a major concern for women worldwide (World Health Organization, 2021). While IPV is a direct threat to the physical and mental well-being of an individual, IPV against women has been shown to affect several other aspects of their lives, including interpersonal relationships, social cohesion, and labor force participation (Dehingia et al., 2022; Raj et al., 2018). In addition to impacting women directly, IPV has also been shown to be associated with adverse health and cognitive outcomes for their children. Studies have documented that maternal exposure to trauma and violence throughout the lifespan can compromise parenting capacity, which can severely impact the health and developmental outcomes of children (Jiwani et al., 2022). Research globally has found that children who were exposed to violence between parents at an early age show developmental delays in multiple domains (e.g., language, social-emotional, and academic functioning) (Cage et al., 2022; Jouriles et al., 2018; Udo et al., 2016). Moreover, such developmental delays or disruptions caused by IPV exposure predict a higher risk of becoming the perpetrators or victims in children’s later lives (Kimber et al., 2018; Palmwood et al., 2022). Hence, it is of the utmost importance to both eliminate IPV and identify mechanisms that mitigate and prevent the negative effects of IPV exposure on young children.
Globally, early education has been identified as one of the mechanisms that can mitigate the negative impact of early exposure to IPV on child development (Lloyd, 2018). Having a positive relationship with supportive adults (e.g., teachers) can act as a psychological buffer against the harmful effects of stress caused by IPV on the children’s well-being. Research in the United States documents that having a strong and positive connection with teachers can mitigate the development of concerning behaviors among children (e.g., aggressiveness, anxiousness, and impulsivity) (Meehan et al., 2003; Silver et al., 2005). This is especially true for children exposed to IPV in the household—as they are at a higher risk of not being able to form a positive attachment with their parents (Niolon et al., 2017; Vaughan-Jensen et al., 2020). Research in the United Kingdom also indicates that it’s not unusual for children exposed to IPV to exhibit a range of psychological challenges such as separation anxiety, concentration difficulties, and depression, alongside physical symptoms like bruises, sleep disturbances, and disruptions at school. Teachers’ abilities to identify these patterns and to collaborate with professionals can prevent children from being further victimized (Lloyd, 2018).
Mitigating the impact of early exposure to IPV on children’s development through early education and intervention has been well-documented in developed countries (Lloyd, 2018; Sterne & Poole, 2009). However, this is less explored in lower resource contexts such as India, where IPV is pervasive and early education enrollment rates are low relative to that seen in many other middle-income nations (Sardinha et al., 2022; UNICEF, 2024). A recent survey in India indicates that one in three married women report experiencing IPV from their husbands at least once during their lifetime (International Institute for Population Sciences [IIPS] and ICF, 2021), which suggests that a high proportion of children are exposed to violence at home. Moreover, though primary education is close to universal in India, early childhood education is not the norm, with only 40% of children aged under 5 reported having attended preschool (IIPS and ICF, 2021; Singh et al., 2021). The disparity in early childhood education is particularly pronounced among rural, less educated, economically disadvantaged, and marginalized populations, where IPV rates tend to be higher (Chowdhury et al., 2022; IIPS and ICF, 2021; Maher & Hayes, 2023). Data from India suggest that socio-economically vulnerable children are less likely to enter early childhood education due to the lack of financial support and accessibility (Hazarika & Viren, 2013), and IPV may exacerbate this concern, as women affected by IPV may be less able to prioritize the educational needs of the child (Chilanga et al., 2020).
Despite India’s higher levels of IPV prevalence and low early education enrollment, research in this area remains sparse. The dearth of research from India on this issue has persisted despite a plethora of global evidence affirming the efficacy of early education in counteracting the negative effects of IPV exposure on children (Cage et al., 2022). Moreover, research conducted in high-income countries and exploring the associations between IPV exposure and children’s school attendance and educational outcomes has primarily focused on individual-level predictor variables such as maternal age, race/ethnicity, number of children, and relationship status (Kiesel et al., 2016; Scolese et al., 2020). Yet, there remains a notable gap in research, as few studies incorporate factors beyond demographics when exploring the link between IPV exposure and children’s educational outcomes. Research typically considers the roles of mothers or parents in early childhood education, but here we consider the household as an integrated, functional unit of influence in our examination of IPV (Johnson & Ray, 2016). In the context of India, there may be joint families (i.e., multiple related nuclear families from across generations residing together) in a household with multiple women serving as caregivers to a child and influencing decision-making regarding early education. In this study, we assess IPV against a woman in the household, recognizing that household exposure to IPV, or a woman historically affected by IPV, will exist for these children regardless of whether it is against their mother or not. Children frequently interact not only with their parents but also with other household residents, affecting their social development and educational experiences. Our study aims to bridge this research gap in the analysis of IPV exposure at the household level by utilizing nationally representative data from India, examining children aged 3 to 5, and accounting for a range of socioeconomic and demographic factors that could confound the relationship between IPV victimization and educational outcomes within the household context. We hypothesize that children residing in IPV-affected households are more likely to be excluded from early education due to greater household strain.
Methods
Data Source
We used the fifth round of India’s Demographic and Health Survey (DHS), also called the National Family Health Survey (NFHS-5), conducted under the stewardship of the Ministry of Health and Family Welfare, with the International Institute for Population Sciences (IIPS) acting as the nodal agency (IIPS and ICF, 2021). The NFHS is a nationally representative survey of Indian households, covering 28 states and 8 union territories. The survey data collection took place from 2019 to 2021, with the majority of the data being gathered in 2019 (76%), followed by smaller proportions in 2020 (12.66%) and 2021 (11.59%), as the collection process was disrupted by the COVID-19 lockdowns.
The survey implemented a two-stage stratified sampling design. The first stage involved sampling of primary sampling units (PSUs), which were stratified as villages in the case of rural areas, and Census Enumeration Blocks in urban areas. The second stage involved sampling of households within PSUs. Within each sampled PSU, a complete mapping of all households was undertaken prior to the survey. A total of 636,699 households were selected for the survey using this process.
The survey implementation involved the administration of a household-level questionnaire to each of the households in the survey. The household-level questionnaire collected sociodemographic information on all usual members of the household, including demographic details of children living in the household, such as their age, sex, and school attendance. In addition, the survey identified all women aged 15 to 49 years in the sampled households and administered a woman’s questionnaire to all eligible women. The women’s questionnaire included indicators of women’s sociodemographic characteristics such as maternal age, level of education, number of children, caste, and religion. A total of 747,176 eligible women were identified, and interviews were completed with 724,115 women. A subsample of women also completed a domestic violence module that included questions on women’s experiences of IPV and witnessing of IPV against their mothers. The subsample of women for the domestic violence module was drawn by randomly selecting 15% of the households from each state. Within the selected households, one woman aged 18 to 49 years was randomly selected to respond to the domestic violence module. A total of 72,320 women were identified for the domestic violence module (IIPS and ICF, 2021).
Study Sample
The study population was children aged 3 to 5 years in households selected for inclusion of the domestic violence module of the survey, given to an ever-married woman in that household. Data on children aged 3 to 5 years are from the household roster, with data provided by an adult member of the household. Data on IPV and women’s individual characteristics are taken from the women’s survey delivered to a selectwoman in that household. To create the dataset for these analyses, we first merged the household survey and women’s individual survey according to cluster and household number for the subsample of households where the women’s survey included the domestic violence module, yielding a sample of N = 63,851 households. Of these, 17,204 households had a child aged 3 to 5 years, with a total of 19,823 children aged 3 to 5 years. We removed one child from our dataset as data on sex for that case was unavailable or was neither male nor female, resulting in a final dataset N = 19,822 children for our analytic sample (Figure 1).
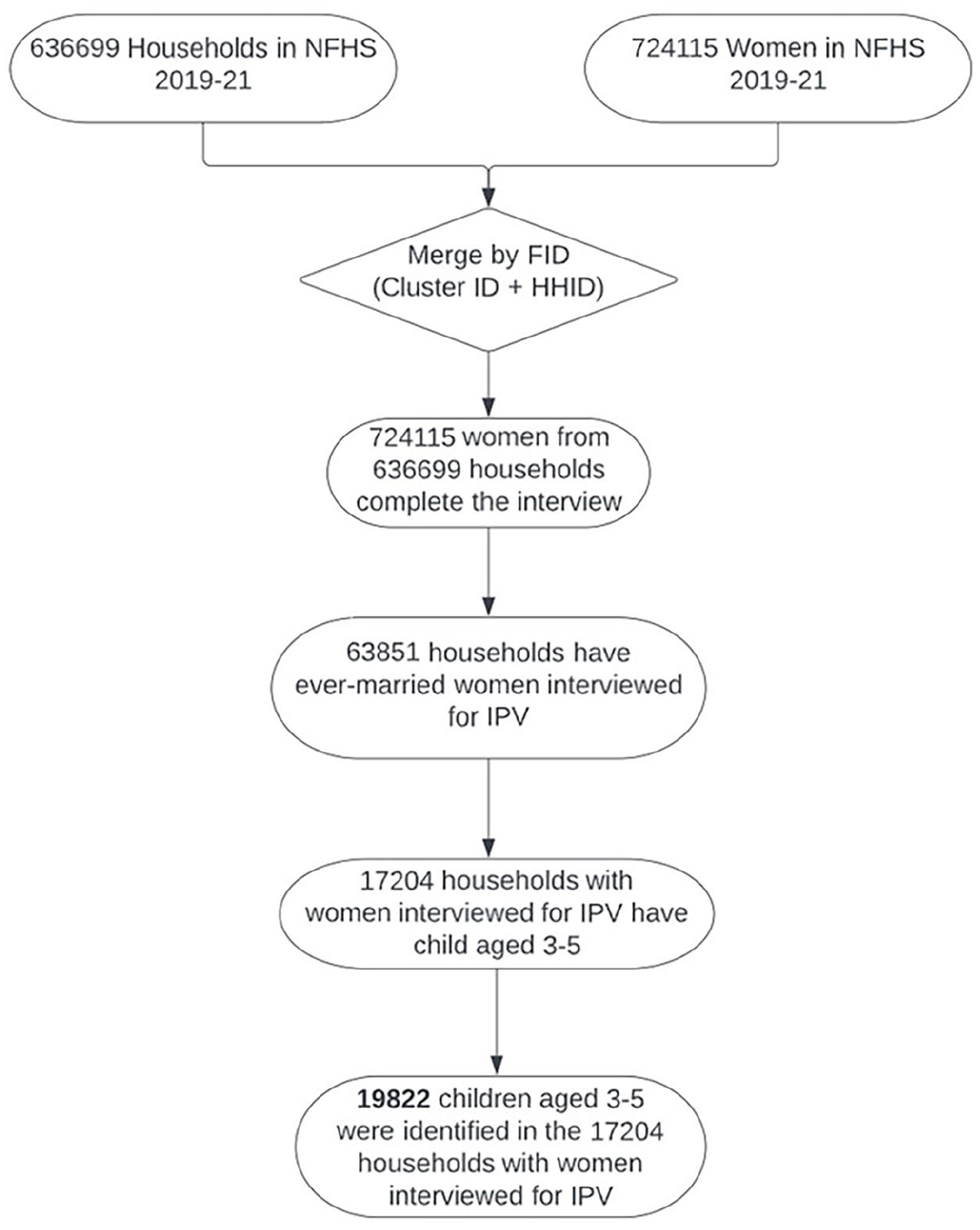
Flowchart depicting the steps involved in the selection of participants in the study.
Study Variables
Outcome Variable
The primary outcome of our study was the school attendance among children aged 3 to 5 years in the school year of 2019 to 2020. We constructed a binary variable to capture school attendance and coded it “1” if the child ever attended school in the year 2019 to 2020 and “0” if the child never attended school in the year 2019 to 2020.
Independent Variables
Our primary independent variable was women’s experience of IPV, which encompassed both physical and sexual IPV experienced by women. We captured women’s experience of physical violence as a binary variable using questions in the survey that asked women if they had ever been (a) pushed or shaken, (b) slapped, (c) punched, (d) kicked or dragged, (e) strangled or burned, (f) threatened with a knife/gun, (g) arm-twisted or hair-pulled by their husband in the past 12 months from the time of the survey. We categorized women as having experienced physical IPV if they responded “yes” to any of the above seven items and coded them as “1.” Women who reported “No” to all of these seven items were coded as “0.” The same methods were also applied to construct the sexual IPV variable by asking women to report if they had ever been (a) physically forced to have sexual intercourse, (b) physically forced to perform any other sexual acts, (c) forced with threats or in any other way to perform sexual acts, even when they refused to in the past 12 months. A final binary variable was created to capture both physical and sexual IPV. If women were categorized as “yes” to either or both of these two IPV variables, they were considered as having experienced recent IPV.
Covariate
We included a number of variables pertaining to the child, household, and women, that could potentially confound the relationship between our independent variable and our outcome. At the child level, we included child age and child sex. At the household level, we included household wealth, place of residence, caste, religion, sex of household head, and the year of interview. Variables related to women included women’s age and the highest level of education. In addition to the demographic information of women, we also considered the potential influence of receiving more information regarding children’s education through mass media by adding indicators of access to information: (a) exposure to media (newspaper, radio, or TV) last week, (b) ever exposed to the internet, and (c) cell phone ownership.
Household wealth was captured using the DHS wealth index used in the DHS as a proxy indicator to assess the economic status of a household. Children’s age was categorized as 3/4/5 years old, and children’s sex was coded as a dichotomous variable—male or female. The number of preschool-age children was treated as a continuous variable. The variable for household wealth was developed by categorizing the DHS wealth index variable into five quintiles. The five categories thus created corresponded to the poorest, poor, middle, rich, and richest households in terms of the number of assets available in the household (IIPS and ICF, 2021). Place of residence and sex of the household head were treated as dichotomous variables categorized as rural/urban and male/female, respectively. With respect to women’s indicators, age was treated as a continuous variable. Level of education was categorical, whereas exposure to media and the ownership of cell phones were treated as yes/no binary variables.
Data Management and Analysis
We performed descriptive analyses on the overall sample and for the subsamples of 3 to 5 years old children, in and out of school. We developed a crude logistic regression model with women’s experience of IPV as a predictor and children’s school attendance as the dependent variable (Models 1). Next, we developed a series of multivariable regression models with our IPV variable to predict our outcome, adjusting for child-level covariates (Model 2), adjusting for child-level and household-level covariates (Model 3), and then adjusting for the child-, household-, and women-level covariates (Model 4). To address the potential influence of shared risks among multiple children of the same age residing in the same household, and their subsequent impact on school attendance, a multilevel regression analysis was employed. This approach aimed to mitigate potential confounding factors arising from this situation by accounting for the nested structure of children within households. However, the result indicates that there is a negligible clustering effect for the current study (ICC = 0.005).
We performed all analyses using domestic violence survey weights, accounting for the PSU, and strata to retain the representativeness of the data and to get reliable estimates of standard errors. We used R version 4.1.3 (R Core Team, 2022) for extracting, recording, and analyzing the data.
Results
In our analytic sample of 19,822 children, the majority were male (51%) and attended school during the school year of 2019 to 2022 (55%). We observed a relatively even age distribution, consistent with the full NFHS-5 sample (IIPS and ICF, 2021). Seventy-two percent of the children were from rural areas, and 24% were from households in the poorest quintile. About three-quarters of children belonged to households that followed Hinduism (76%) and a similar proportion belonged to Scheduled Caste/Scheduled Tribe/Other Backward Class caste categories (73%). The average number of children aged 3 to 5 in the same household was 1.29, and most were in households with a male household head (83%). Women surveyed on IPV experiences in these households have an average age of 30, and 48% of them completed secondary education. While more than half of the women did not have media exposure in the past week (51%) or did not have access to the internet (73%), most of them owned a cellphone (57%) (Table 1).
Prevalence of Intimate Partner Violence and Socioeconomic and Demographic Characteristics of the Sample Across School Attendance in 2019 to 2020. Estimates Include the Number of Cases (n) and Weighted Percentages for Categorical Variables and Weighted Means and Standard Deviations for Continuous Variables. Denominators for the Overall Sample and for Subsamples Across the Enrollment Status of the Child (N) Has Been Presented as Unweighted Numbers.
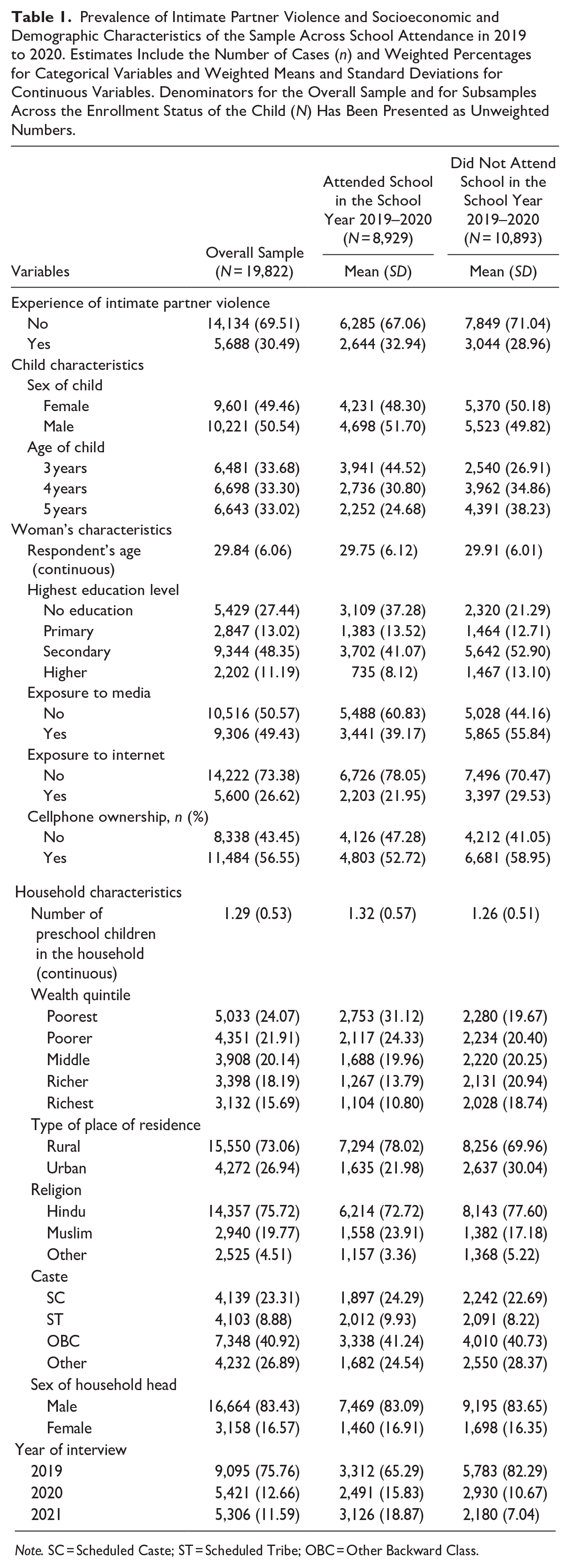
Note. SC = Scheduled Caste; ST = Scheduled Tribe; OBC = Other Backward Class.
In the crude logistic regression model (Table 2; Model 1), women’s experience of IPV (OR: 0.83, 95% CI [0.73, 0.94]) in the household was significantly and negatively associated with school attendance of children aged 3 to 5 years. After adjusting for three child-level covariates (Model 2), we continued to see a significant relationship between IPV and early school attendance (adjusted OR: 0.81 [0.71, 0.92]). However, once our model included household-level covariates for our predictor (Model 3), the significant effect of IPV on children’s early education attendance was lost (adjusted OR: 0.93 [0.81, 1.07]). When further adjusting for women-level covariates (Model 4), the effect of IPV remained insignificant (adjusted OR: 0.95 [0.82, 1.09]).
Logistic Regression Analysis Examining the Relationship Between IPV and Early Education Enrollment Through Various Models: A Crude Model (Model 1), a Child-Level Covariate Adjusted Model (Model 2), a Household-Level Covariate Adjusted Model (Model 3), and a Woman-Level Covariate Adjusted Model (Model 4).
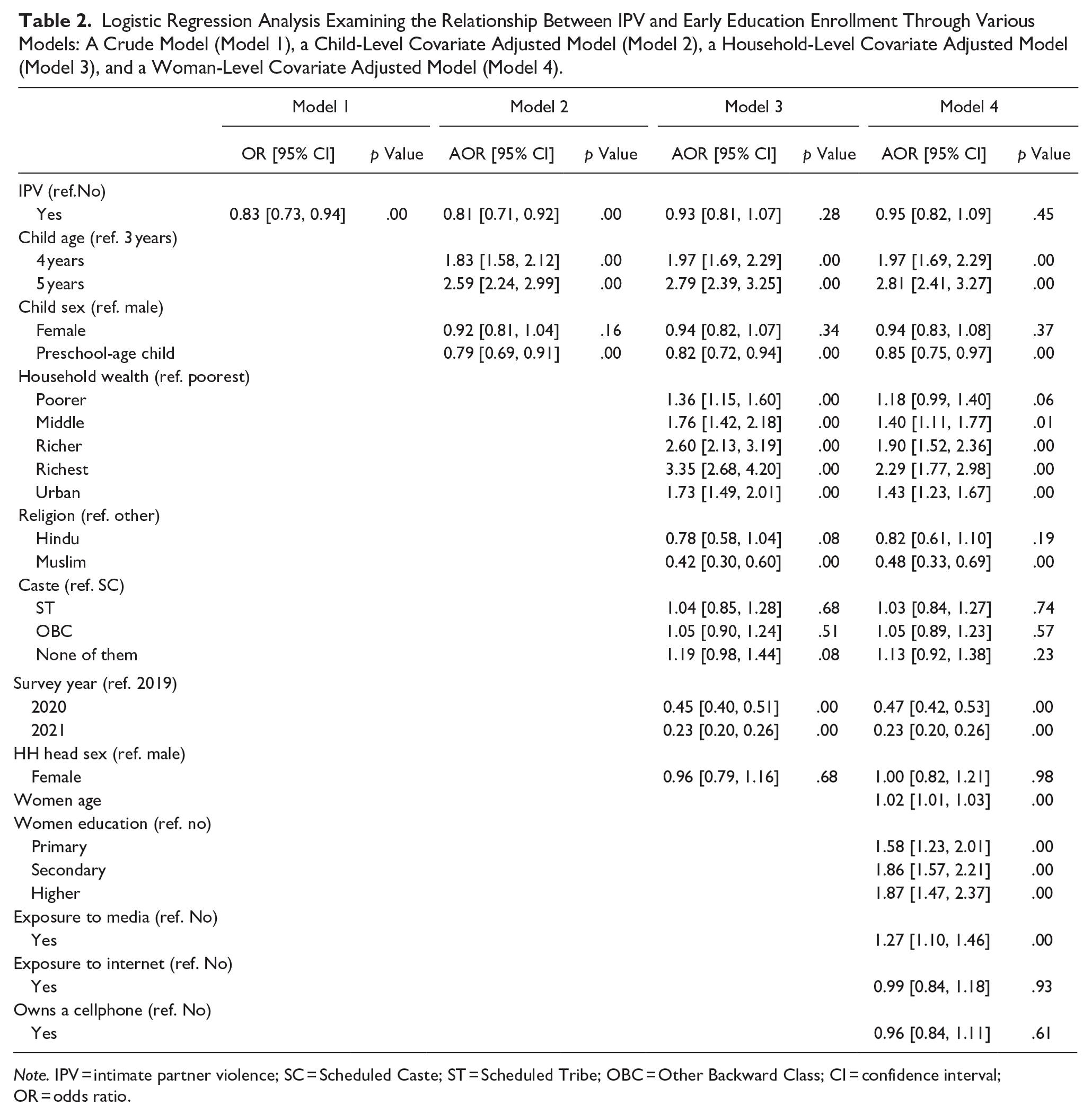
Note. IPV = intimate partner violence; SC = Scheduled Caste; ST = Scheduled Tribe; OBC = Other Backward Class; CI = confidence interval; OR = odds ratio.
Discussion
The current study tests the association between IPV experiences of women and early education entry of children in the same household. The results from Model 1 and Model 2 indicate that children from households where women experienced IPV are less likely to be enrolled in early education. This is consistent with existing research, highlighting an association between IPV and children’s education attendance (Kiesel et al., 2016; Scolese et al., 2020; Wathen & Macmillan, 2013). While research has long established a negative association between IPV exposure and children’s school attendance in Western countries by exploring individual-level variables (e.g., age, sex, and number of children) (Kiesel et al., 2016; Scolese et al., 2020; Wathen & Macmillan, 2013), the current study further accounts for the household and women-level variables. Notably, when adjusting for the household demographics, the observed association between IPV and children’s early education participation is lost. These findings add to the literature on the potential role of IPV in households in children’s entry into early education in India.
Loss of the observed effect in adjusted analyses suggests that household demographics may confound the association between IPV and children’s school attendance. Although this is not aligned with prior research that mostly emanates from high-income country settings (Bedoya et al., 2020; Kiesel et al., 2016; Wathen & Macmillan, 2013), research that demonstrates a negative association between IPV exposure and children’s school attendance from such settings was mostly collected from primary school-aged children, not very young children. The few studies that have focused on this very young child age group; however, document the value of early childhood education in mitigating the negative effects of exposure to IPV on children, underscoring the importance of focusing on this very young child age range and early childhood education (Howell, 2011; Howell et al., 2010). Further investigation is warranted to gain a comprehensive understanding of the effects of IPV within a broader array of national and cultural contexts.
Notably, the year of data collection used in this study is a potential confounding influence, as the years of study included the period of COVID-19 shutdowns. We could have used prior rounds of data for these analyses, but that data would not effectively reflect the evolving landscape of early childhood education in India, which is at a time of expansion. It is imperative to rely on the most recently available data to explore this issue. Data from the upcoming NFHS-6 will offer greater insight into early education in the post-pandemic period, but we are more than a year away in terms of data availability for analysis and understanding of this issue is needed now, given the 2020 update to the Indian education policy, which emphasizes a heightened emphasis on early childhood education (Gupta, 2022).
Additional limitations of the current study appear in both the data collection and the sampling procedures. The data rely on self-report, so are vulnerable to social desirability and recall bias. We cannot presume that the IPV exposure variable is specific to the child’s mother, nor was that the purpose, as we were focused on IPV exposure at the household level. However, maternal IPV exposure may have a more deleterious impact on young children, and future research should seek to tease out effects at the level of the household versus the mother. Our data are limited in that we could not ascertain directly the relationship of the woman surveyed in the household with the child identified for analysis. Qualitative data and longitudinal studies may have further insight. It is also possible that there is IPV in the household but not experienced by the woman participant, but this concern makes our estimate more conservative rather than more likely to have yielded a significant effect.
In conclusion, this study explores the association between IPV exposure in the household and education attendance among children aged 3 to 5 years old and indicates an association, but one confounded by household demographics indicative of socioeconomic vulnerabilities. These findings reinforce the need to focus on socio-demographically vulnerable households with young children to support their entry into early childhood education, but they also suggest that these households and consequently these children may have disproportionate exposure to IPV which may affect the well-being and social-emotional needs of these children. Early childhood education in India will need to consider these needs as its presence expands in the country and coverage of socioeconomically vulnerable households improves. As India seeks to improve child development and early childhood education participation through its National Education Policy of 2020 and with an eye toward addressing the negative education impacts of the COVID-19 pandemic (Howell et al., 2010), increased focus on enrolling children in early education at the age of 3 to 5 years old may mitigate developmental delays and poor health caused by IPV exposure in their later life.
Footnotes
Declaration of Conflicting Interestss
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.