
Abstract
Mandatory reporting (MR) among service providers (SP) working with intimate partner violence (IPV) is controversial, and the research is scarce. The potential association of SPs experience with IPV and MR-IPV and their attitudes is the aim of the current study. A total of 374 SPs working with victims and perpetrators (help-seekers) of IPV participated in this study. Factor analysis was conducted to produce a continuous standardized dependent variable as a measure of attitudes toward MR-IPV. Descriptive results indicated that SPs were generally supportive of MR-IPV. Linear regression analyses showed that a higher degree of professional experience with IPV was significantly associated with less skepticism of MR-IPV. The result was significant regardless of (1) severity of violence, (2) category of help-seeker, (3) time of incidents, and (4) number of cases where MR-IPV was considered relevant. Having substantial experience with IPV and MR-IPV remained significant adjusting for the SP category, years in current position, knowledge of MR, and frequency of mandatory reports. Our results indicate that experience is an important part of SPs attitudes toward MR-IPV.
Introduction
Intimate partner violence (IPV) has been established as a serious world health issue (World Health Organization [WHO], 2012) and particularly a serious threat to women’s safety and lives (e.g., Stöckl et al., 2013; United Nations Office on Drugs and Crime, 2022). One action to prevent IPV and intimate partner homicide (IPH) is the law of mandatory reporting (MR). Disclosure required by law is commonly referred to as MR, while disclosure allowed by law is commonly referred to as discretionary reporting. Although laws vary among countries and states, the essence of MR is the same—by law certain individuals or groups are mandated to report certain serious crimes (and/or their impending occurrence) to the authorities. The purpose of mandatory reporting of IPV (MR-IPV) is to protect persons subjected to IPV from the risk of harm, to relieve them of having to report abusive partners themselves, and to improve the involvement of law enforcement and the criminal justice response (Jordan & Pritchard, 2018; Rodriguez et al., 2002; Vatnar et al., 2017). Furthermore, MR-IPV sends a signal to abusive partners that IPV is a serious crime (WHO, 2013) and establishes third-party documentation that may be critical to a criminal or civil legal action (Antle et al., 2010).
Many countries practice a form of mandatory reporting (e.g., Australia: Mathews & Walsh, 2014; Cypros: Panayiotopoulos, 2011; Netherlands: Van Dam et al., 2015; United States of America (US): Lund, 1999; McDowell et al., 1994). However, who is obligated to report what must be reported and to whom a report is made varies between countries and states. For instance, in Kentucky, all individuals are mandated to report to the Cabinet for Human Resources if they suspect abuse, neglect, or exploitation (Mandated Reporter Training, 2022). In California, only health practitioners are mandated reporters and must report to the police if they treat a physical injury they suspect was caused by a firearm or assaultive or abusive conduct (Mandated Reporter Training, 2022). In contrast, five states in the United States (Alabama, Louisiana, South Carolina, Washington, and Wyoming) do not have mandatory reporting laws for domestic violence (Mandated Reporter Training, 2022). Furthermore, MR-IPV is controversial (e.g., Lippy et al., 2019; Rodriguez et al., 2002). At the root of this discourse is the moral balance between (1) the state’s obligation to protect and chase justice on behalf of victims of IPV and (2) the victim’s autonomy over their own life and family. Historically, this is reflected in the growth of women’s rights and awareness of “battered women” in the 1960s and 70s, and calls for public intervention (Barner & Carney, 2011).
As mentioned above, one means of intervention is mandatory reporting, which in many jurisdictions simply means a report must be made to law enforcement about patient injuries. However, criticism has surrounded MR-IPV in contexts in which children might be removed from the home, and the perpetrator could punish the victim (Rodriguez et al., 1998). It is not illegal to stay in an abusive relationship, and victim advocates argue victims should be allowed to choose not to have the abuse reported if other consequences are more feared (Walker, 2017). On the other hand, there is a lack of evidence that suggests victims do not want it reported (Vatnar et al., 2021). Victims might also be in a difficult position to report on their own, for instance, because they fear the consequences or feel the violence is not severe enough (Del Rio & Del Valle, 2016; Robinson et al., 2020).
The current recommendation from the WHO (2013, 2017) is to abolish the implementation of MR-IPV, arguing that it might deter victims from seeking help. The recommendation is based on literature suggesting that service providers (SPs), that is, any professional who works with or meets a victim or perpetrator, are generally negative to MR because of this possible deterrent effect. However, a recent systematic review revealed that the MR-IPV research is limited and has serious methodological issues (Vatnar et al., 2021), and hence further clarification of SPs’ attitudes toward MR is necessary.
Attitudes Toward MR-IPV
Vatnar et al.’s (2021) systematic review revealed indications of skepticism toward MR-IPV among SPs. However, the authors of the review found that methodological bias was high amongst the articles included in the review (i.e., systematically reporting findings of statistical minorities who opposed MR as being more significant than those of statistical majorities who supported MR-IPV; items asking if help seekers were “warned about MR”). The authors concluded that there was a gap between SPs having (1) strong attitudes toward MR-IPV, but (2) limited awareness of the law of MR-IPV (e.g. Cho et al., 2015; Sawyer et al., 2014), and (3) scarce experience with MR-IPV (Smith et al., 2008). Accordingly, the field requires further investigation.
The studies that aimed at exploring SPs’ low compliance with MR-IPV mainly measured barriers to reporting (i.e., circumstances inhibiting reporting) rather than attitudes per se. One study explored perceived barriers to reporting among 181 nurses in Florida (Smith et al., 2008). Of 16 potential barriers, the top 3 were: not enough evidence (32%), patient objected (17%), and confidentiality (9%). However, most attention was given to the nurses’ own personal experiences with being an IPV victim, which significantly influenced reporting behavior (IPV victims reported more often). Barriers were not explored further. Mgopa et al. (2021), through focus groups of health personnel and students in Tanzania, reported that participants mentioned several barriers that made managing IPV cases difficult, including a lack of knowledge about MR-IPV criteria. Health personnel were also more positive about reporting to the police than students were. Accordingly, the current study explored attitudes, not just barriers, toward MR-IPV and how actual professional experience with IPV and MR might be associated with attitudes.
Only two, though older, studies analyzing attitudes beyond a descriptive level were covered by Vatnar et al.’s (2021) systematic review. First, a study conducted in California measured approximately 500 physicians’ experiences with IPV and their attitudes toward MR-IPV (Rodriguez et al., 1999). More than half of the participants (59%) responded that they would not report (despite MR) if their patient objected. Participants who were unaware (self-reported) of the MR law had triple the likelihood of not reporting IPV if their patient objected. Descriptively, participants agreed with both supporting and opposing statements of MR. However, the majority (90%) agreed that under certain conditions (e.g., pregnancy, access to guns) they should report. Group differences were observed between medical specialties (e.g., family medicine vs. gynecology vs. emergency). Items measuring professional experiences with IPV and attitudes toward MR-IPV were not explored in any inferential statistical analyses. In addition to comparing differences between medical specialties, there are other professional groups who are confronted with decisions about MR-IPV. As such, the current study included a variety of different professions managing IPV.
Second, Tilden et al. (1994) questioned 1,521 different health professionals (i.e., dental hygienists; dentists; nurses; physicians; psychologists; social workers) about their attitudes toward abuse intervention and their management of it. The participants were asked about their attitudes toward MR regarding elder, spousal, and child abuse. Overall, participants, regardless of profession, considered MR for spousal abuse more effective (M = 63%, range 55%–76%) than for child (M = 43%, range 36%–52%) and elder abuse (M = 35%, range 32%–39%). The fact that two of three of the most relevant articles were published decades ago also underscores the need for further research on this topic.
Theoretical Framework
Classic studies have illustrated that behavior is determined by many factors other than attitudes and that these affect attitude-behavior consistency. Most theories concerning attitude and behavior aim at understanding how attitudes predict behavior (Forgas et al., 2010; Haddock & Maio, 2004), not how experiences might influence attitudes. The former is what might be called behavior-change focused, and the latter attitude-change focused. Cognitive dissonance (Festinger, 1957) and attitudinal ambivalence (Harreveld et al., 2015) are theories that might contribute to explaining how experiences shape attitudes. The former might explain how past behaviors increase an internal cognitive conflict for individuals when faced with experiences that go against their own attitudes. The latter suggests that there are some topics individuals feel stronger toward than others and that it is possible to hold both positive and negative attitudes toward a target at one time. Hence, it might be that experiences only modify a person’s attitude toward someone or something rather than change it completely. As such, the theories might explain the possible outcomes of change in attitudes in face of attitude-contradicting experiences. In the context of MR-IPV, this could imply that SPs might have previous experiences with reporting under MR-IPV which could influence their evaluation of utilizing MR-IPV in the future, either negatively or positively, in relevant situations with a victim or a perpetrator of IPV. The current study, though not a formal test of theories of attitudes, is informed by these theoretical frameworks.
Context of the Current Study
This research was conducted in Norway, where the main purpose of MR is to avert or prevent current or future crime, or the consequences thereof. Thus, the duty only applies when prevention is in fact possible. This law, as a means of preventing harm, is regulated in section 196 of the penal code (Straffeloven, 2005). Section 196 refers to 52 criminal acts that are covered by MR. Among them are domestic violence (sections 282 and 283). In this jurisdiction, MR applies to all individuals and is required even in cases where the information is initially confidential. The duty to report may be executed by notifying the police or by averting the criminal act or its consequences “by other means.” Failure to report according to section 196 is a punishable crime, unless reporting would expose the reporter, their next-of-kin, or an innocent person, cause a charge or indictment, or cause risk to life or welfare.
Aim and Research Questions
The overall aim of the present study was to investigate attitudes toward MR-IPV among professionals working with IPV. We examined the following research questions:
What are the descriptive professional experiences with and attitudes toward MR-IPV among SPs?
To what extent are there associations between attitudes toward MR-IPV and professional experiences with MR-IPV, and IPV itself?
Are there group differences amongst SP professions or their sociodemographic characteristics regarding attitudes toward MR-IPV?
Methods
The current study is a quantitative part of a larger project called MANREPORT-IPV. This project examines awareness, attitudes, and professional experiences with MR-IPV among IPV victims and perpetrators and SPs who work with IPV in Norway. The study was approved by Oslo University Hospital’s Data Protection Official reference number: 22/00221. Regional Committees for Medical Research Ethics (REK) deemed the study to be health service research, not health research, and hence not within their mandate (Reference number: 257644).
Procedure
Data were collected between March 2022 and January 2023. Recruitment was carried out through planned annual meetings arranged by the SPs’ institutions (i.e., police; IPV treatment centers; domestic violence shelters) where the MANREPORT-IPV research group was allocated time (usually 15 min) to present the project (either online or in-person) for potential participants or their managers. Altogether, approximately 15 meetings were held, online or in person, to recruit participants. During online meetings, potential participants were encouraged to contact the first author to receive a link to the online questionnaire. In person, participants were given a questionnaire and consent form, and time was allocated to complete both. Most participants completed the materials in 45 to 50 min were used to complete the questionnaire, although with some variation. The researchers informed prospective participants that participation was voluntary, and they were given contact information to researchers in case they wished to withdraw. Their identity was concealed by cross-referencing their contact information on their consent form with a unique number in a separate file. Online, participants were given a link to identical online study materials and a randomly generated four-digit ID code, which they could use in case they wished to withdraw from the study.
Measures
A questionnaire was developed comprising measures for attitudes, awareness and professional experience (adjusted for measuring MR-IPV), as well as new items created specifically for the current project. We review the measures used for the current analyses.
Attitudes Regarding IPV
The study adjusted items from the validated questionnaire used by the (Norwegian) Institute for Studies of the Medical Profession (Gaasø et al., 2019). The original questionnaire has used repeated measurements on 2,200 doctors every other year since 1992. The content covers Likert-scale statements on attitudes, awareness, and professional experiences, on societal and organizational conditions for professional work, ethics, values, and prioritization (see Table 1 for the adjusted statements.) We also included gender (options: male, female, or other), age, county of workplace and home, years in current position, and profession.
Results of Items Regarding General Attitudes to Mandatory Reporting of Intimate Partner Violence Reported in n and Valid Percentages.
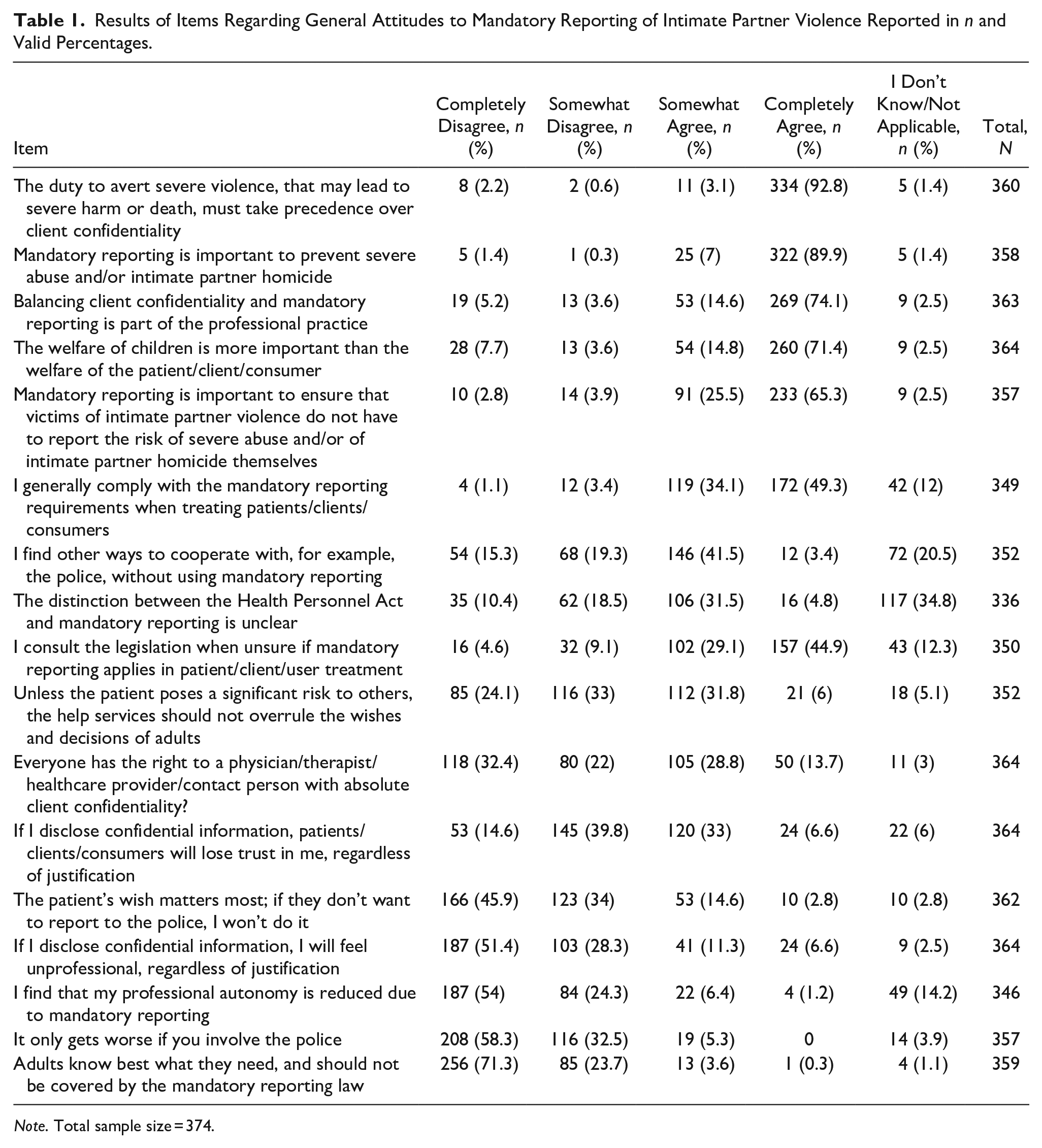
Note. Total sample size = 374.
Professional Experience with IPV and MR-IPV
We developed questions about work experience with IPV and MR-IPV (number of cases with victims and perpetrators). We measured this in intervals of 10 cases (i.e., 1–5, 6–10, 11–20, 21–30, etc.) from none to more than 100 cases. Concerning professional experience with IPV, participants were asked to include any form thereof (i.e., physical, psychological, or sexual). Severe IPV was defined according to the Norwegian penal code for domestic violence and the Norwegian translation (Bendixen, 2005) of the revised Conflict Tactics Scale (CTS2) (Straus et al., 1996). The definitions were described in the questionnaire before the relevant questions as behavior that caused or could cause serious injury or death; was persistent abuse; and/or involved the use of a knife or other dangerous tool/weapon. Additionally, participants were asked if they had professional experience with victims of severe physical injury and perpetrators who have caused severe physical injury.
Participants
Participants (N = 374) included individuals working with IPV victims and perpetrators in six different agencies: police (n = 42); child welfare services (n = 42); emergency primary health care (emergency rooms and assault centers) (n = 83); anger management (n = 67); domestic violence shelters (n = 98); alternative to violence (n = 42). Both the emergency room and assault centers are part of the Norwegian emergency primary health care and work in tandem. SPs very often work shifts in both the emergency room and assault centers and never work completely independently; hence, these groups have been combined. Alternative to violence and anger management both offer therapy to individuals who struggle with issues of violence perpetration. However, they are two independent agencies, in addition to alternative to violence offering therapy to victims of violence. As such these agencies are separated into two groups.
The mean age of participants was 45 (SD = 10), and they had worked, on average, 10 years (SD = 8) in their current position. Most participants were female (79%), 21% were male, and no participants identified themselves as “other gender.”
All participants had some experience working with victims or perpetrators of IPV or both categories and in various degrees of severity. Over half (52%) of participants had experienced between 1 and 50 cases with victims of IPV (no cases = 0.5%). About half (51%) of participants had experienced 1 to 20 cases of victims of severe IPV (no cases = 8.3%). Half (50%) of participants had experienced 1 to 10 cases of victims of severe physical injury (no cases = 15.8%). More than half (55%) of participants had experienced 1 to 30 cases with perpetrators (no cases = 10.4%) and 1 to 20 cases with perpetrators of severe IPV (55%) (no cases = 21.9%), and 56% of participants had experiences with 1 to 20 cases with perpetrators of severe physical injury (no cases = 30.7%). Missing for variables within this section = <2%.
Four percent of participants had professional experience with both incidents where a victim was murdered by an intimate partner and a perpetrator had committed IPH. Five percent had only experience with a victim of IPH, while 4% had only experience with a perpetrator of IPH. The number of cases for those who had these experiences ranged from 1 to 6 cases for victims of IPH, and 1 to 10 for perpetrators of IPH.
Analyses
Basic descriptive analyses were used (frequencies; means; standard deviations) to investigate SPs’ attitudes toward MR at the item level. All variables had some missing values (range 3–81; M = 32 missing values; SD = 16), which were deleted pairwise in analyses. Uni- and multivariate linear regression were utilized to test if independent variables were associated with attitudes toward MR-IPV. STATA version 16.1 (StataCorp LLC) was used to conduct factor analyses (see section below); IBM SPSS version 29 was used for all other analyses. Multicollinearity was not present for any relevant independent variables (variance inflation factor <10).
Factor Analyses: Attitudes Toward MR-IPV
All items regarding perceptions of and attitudes toward MR-IPV were added to an exploratory factor analysis (see Table 2) to investigate if there was a factor solution that captured attitudes toward MR-IPV. The analysis produced three factors with eigenvalues greater than 1. Due to the exploratory nature of this study, the factor loading threshold was set to 0.30 (Costello & Osborne, 2005; Fabrigar et al., 1999; Tabachnick & Fidell, 2001). Four items did not have a factor loading above 0.3, and therefore were excluded. Item 2 was moved from one factor to another for theoretical reasons. When deciding which factors would most adequately measure attitudes toward MR-IPV on a scale, factor 2 was deemed appropriate. Factor 1 was considered to cover professional experience with practice and concerned items on the perception of the use of MR-IPV among colleagues, leaders, and other agencies. Factor 2 covered items on evaluating confidentiality (e.g., If I disclose confidential information, patients/clients/users will lose trust in me, regardless of justification), and perception of autonomy of the patient/client/user (e.g., The patient’s wish matters most; if they don’t want to report to the police, I won’t do it.) Factor 3 did not have a clearly interpretable theme. All items used in the exploratory factor analysis were then added to a confirmatory factor analysis, which produced a root mean square error of approximation (RMSEA) of 0.065, and a comparative fit index (CFI) of 0.867. Participants who responded “I don’t know” to any item were removed from scale construction, which reduced the N for these analyses from 374 to 265. The final attitude score (“Skepticism to MR-IPV”) was standardized (M = 0, SD = 1), and the items included in this factor produced an alpha of .694.
Exploratory Factor Analysis with Oblique Rotation for Items Regarding Attitudes to MR-IPV.
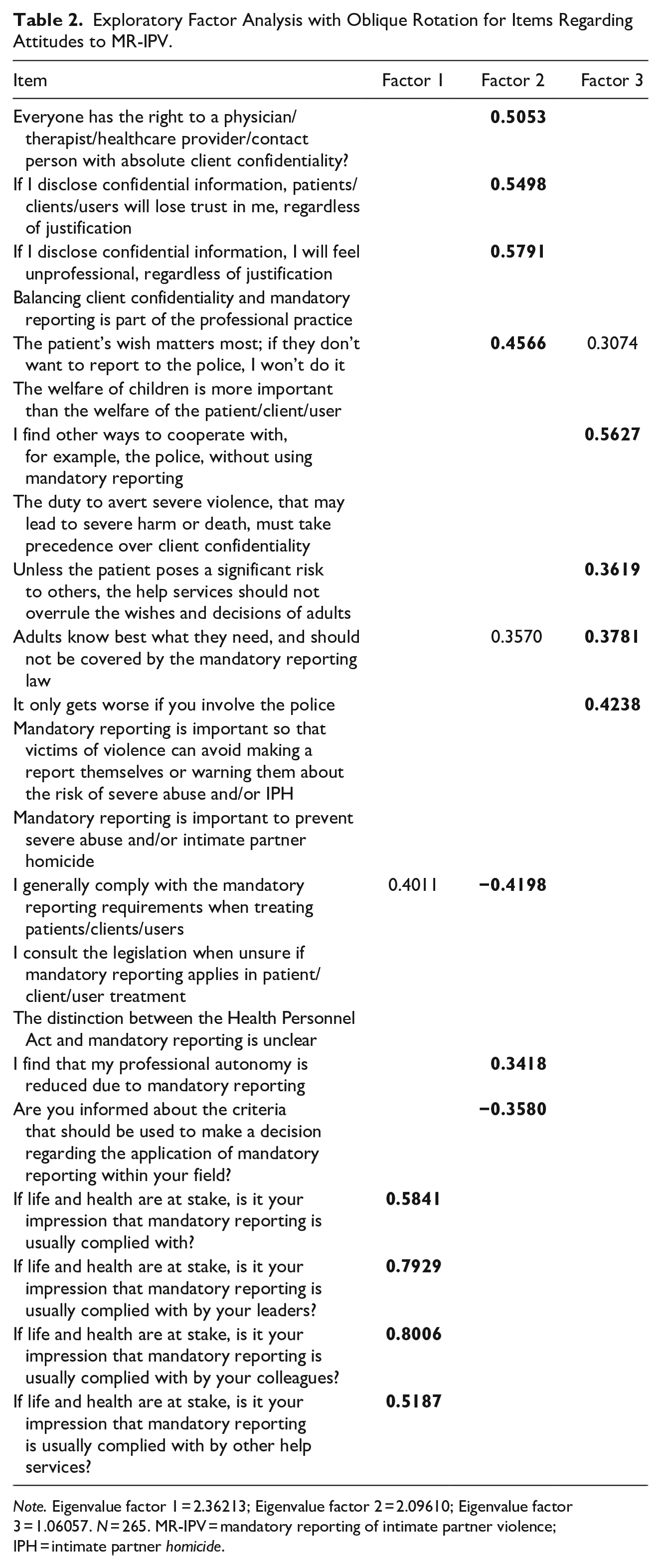
Note. Eigenvalue factor 1 = 2.36213; Eigenvalue factor 2 = 2.09610; Eigenvalue factor 3 = 1.06057. N = 265. MR-IPV = mandatory reporting of intimate partner violence; IPH = intimate partner homicide.
Results
Descriptives
Professional Experience with MR-IPV
With 10 case intervals from 1 to above 100, we measured SPs frequencies of cases where MR was considered relevant (see Table 3). Over half of the participants responded that they had never experienced MR-IPV being relevant when working with a perpetrator while just under a third responded the same regarding victims. Of those who had experience with MR-IPV being relevant regarding perpetrators about a quarter found it relevant for one to five cases, while the remaining 15% of participants responded anywhere between six cases and above 100 (see Table 3). Regarding the victims, just above a third found it relevant for one to five cases, while the remaining 31% responded anywhere between six cases to above 100 (see Table 3). The large majority of participants had never chosen not to report because a victim or perpetrator told them not to, both within the last 12 months and throughout their careers (see Table 3).
Results of Professional Experiences with Mandatory Reporting of Intimate Partner Violence Being Considered Relevant and Choosing Not to Report Regarding a Victim and a Perpetrator Reported in n and Valid Percentages.
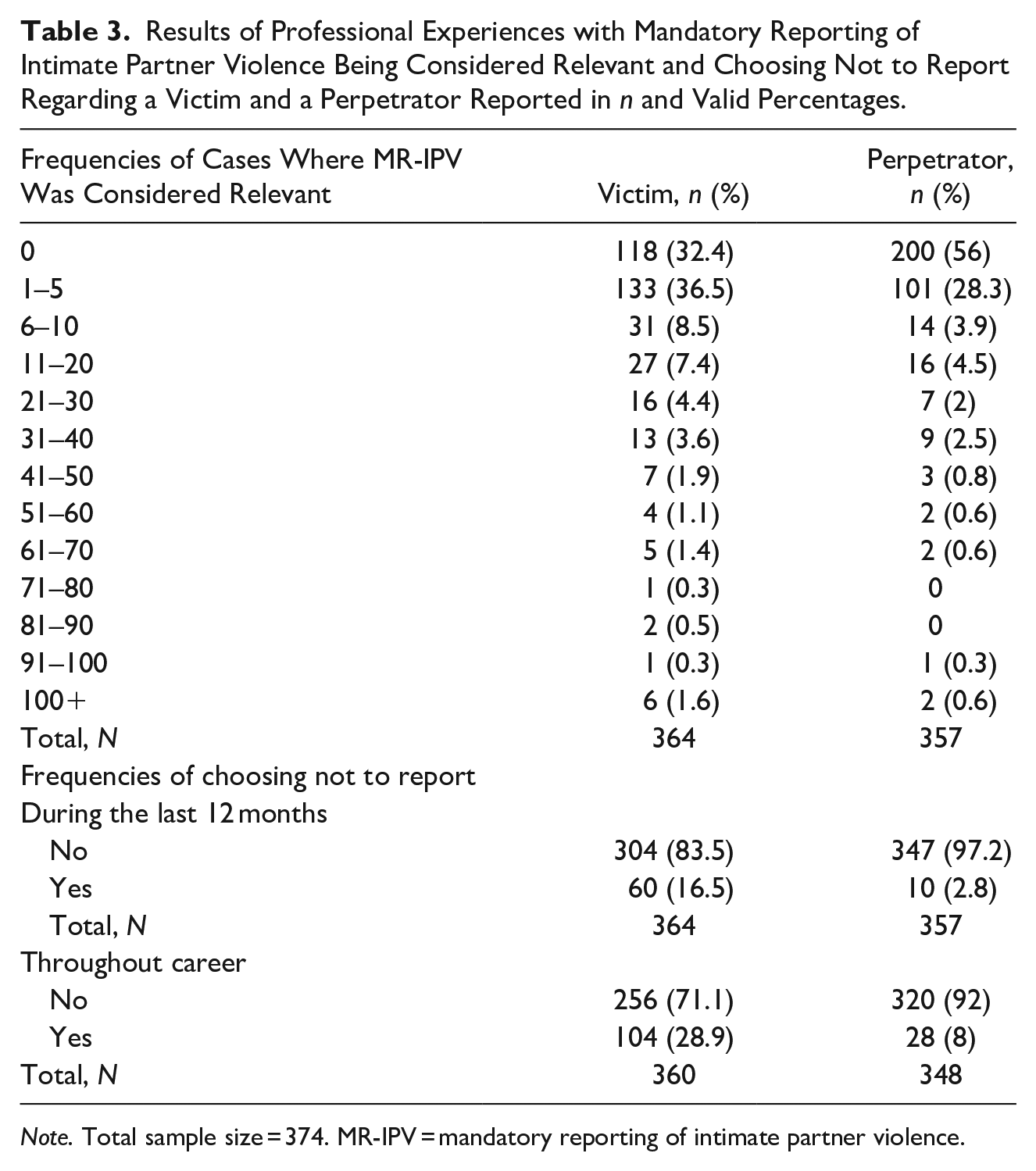
Note. Total sample size = 374. MR-IPV = mandatory reporting of intimate partner violence.
Almost half of participants had never reported IPV under MR without or against their victim and perpetrators’ consent or wish, and 40% of participants had never done this with consent (see Table 4). The remaining participants had done this various number of times from 1 to above 10 with and without consent, and some indicated this was not relevant for them. When asked if the participants had ever experienced the following incidents in their professional practice the majority responded no: ever let a victim or perpetrator go home to persistent IPV; ever overridden a victim or perpetrator’s assessment of such a situation; the use of MR was in some way documented within their system (see Table 5).
Results of Professional Experiences with Reporting With and Without Consent Under Mandatory Reporting Reported in n and Valid Percentages.
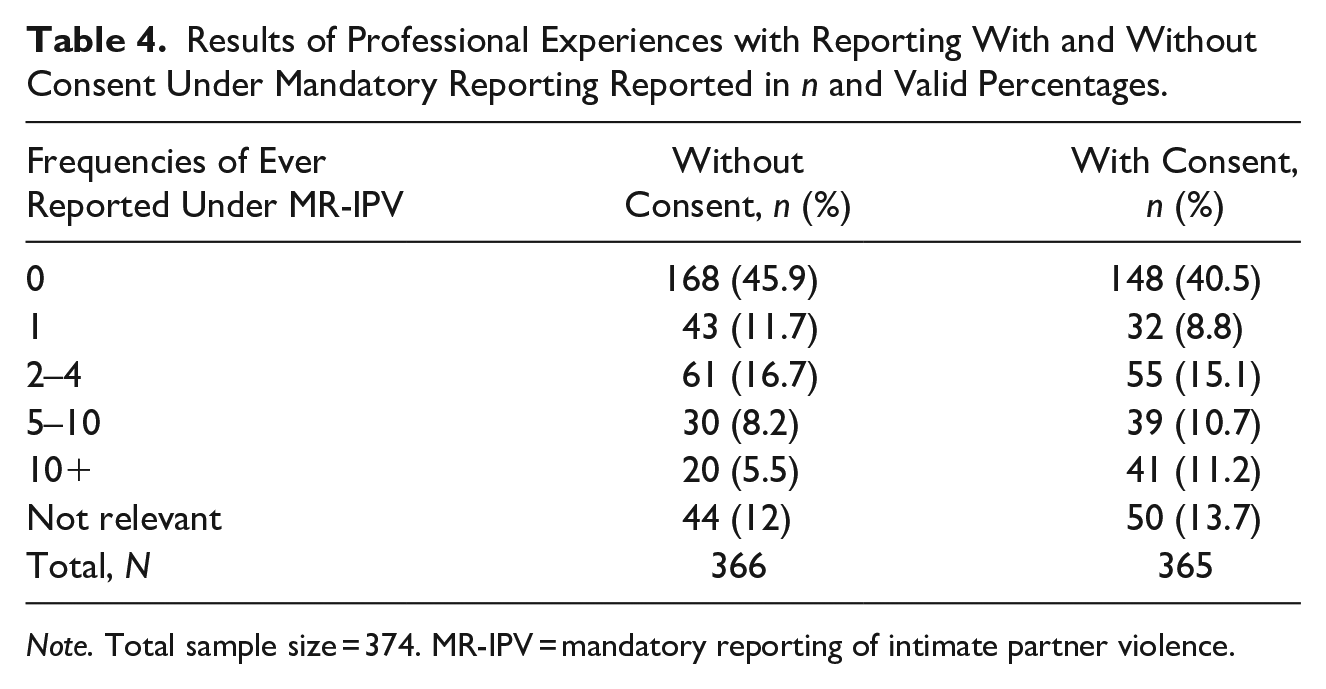
Note. Total sample size = 374. MR-IPV = mandatory reporting of intimate partner violence.
Results of Professional Experiences with Different Incidents Related to Evaluation of MR-IPV Reported in n and Valid Percentages.
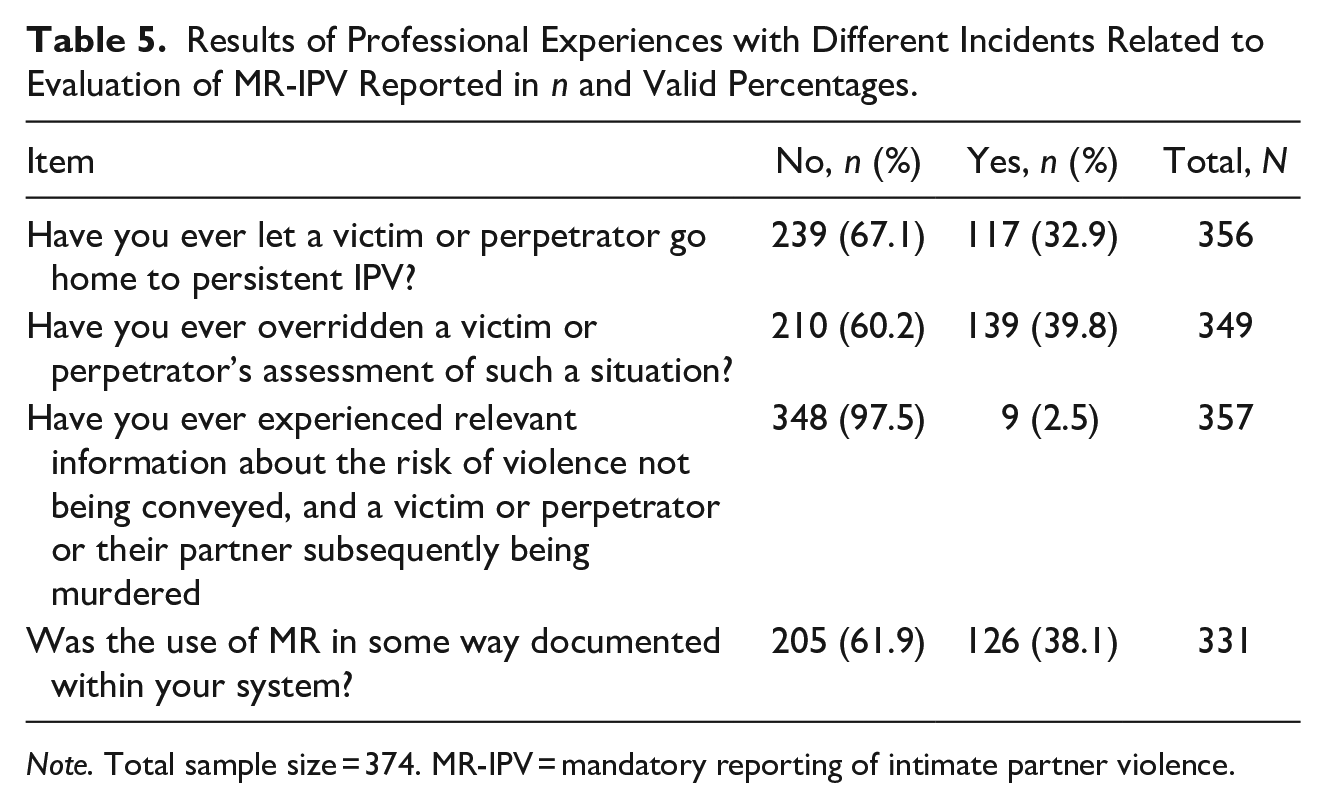
Note. Total sample size = 374. MR-IPV = mandatory reporting of intimate partner violence.
Attitudes Toward MR-IPV
As shown in Table 1, 17 statements were presented to the participants to investigate their attitudes toward MR-IPV. Most participants, regardless of profession, were supportive toward MR-IPV. Some statements reached a higher degree of agreement than others (see Table 1). When responses were skewed toward agreement a higher percentage of participants completely agreed than the percentage of participants who completely disagreed when the responses were skewed toward disagreement. The statement that seemed to reflect the most disagreement across participants (i.e., responses were even across options) concerned whether everyone should have the right to have a doctor or therapist who has absolute confidentiality.
Associations Between Attitudes Toward MR-IPV and Professional Experiences with IPV and MR-IPV
Several predictor variables were significantly associated in regression analyses with the attitude factor score “Skepticism to MR-IPV” used as the outcome (see Table 6 for details). For instance, work experience with IPV (measured by number of cases), both within the last 12 months and throughout career had inverse associations with skepticism to MR-IPV, regardless of the severity of violence or if the cases involved victims or perpetrators. The only variable that was not significant was cases with victims of severe physical injury within the last 12 months. Cases with perpetrators had an overall larger effect size than with victims, meaning that the more cases that participants had with perpetrators overall, the less skeptical they were toward MR-IPV compared to the effect of the experience of cases with victims. This was not tested statistically. Professional experience with IPH was not significant. Having more IPV cases where MR was considered relevant was associated with less skepticism toward MR-IPV, but only if the cases included victims of IPV. There were no significant associations between choosing not to report IPV under MR because the victim or perpetrator requested participants to and being skeptical of MR-IPV.
Univariate Linear Regression Using “Skepticism to MR-IPV” as Outcome Variable and Number of Cases with IPV, Intimate Partner Homicide and Mandatory Reporting of Intimate Partner Violence as Independent Variables.
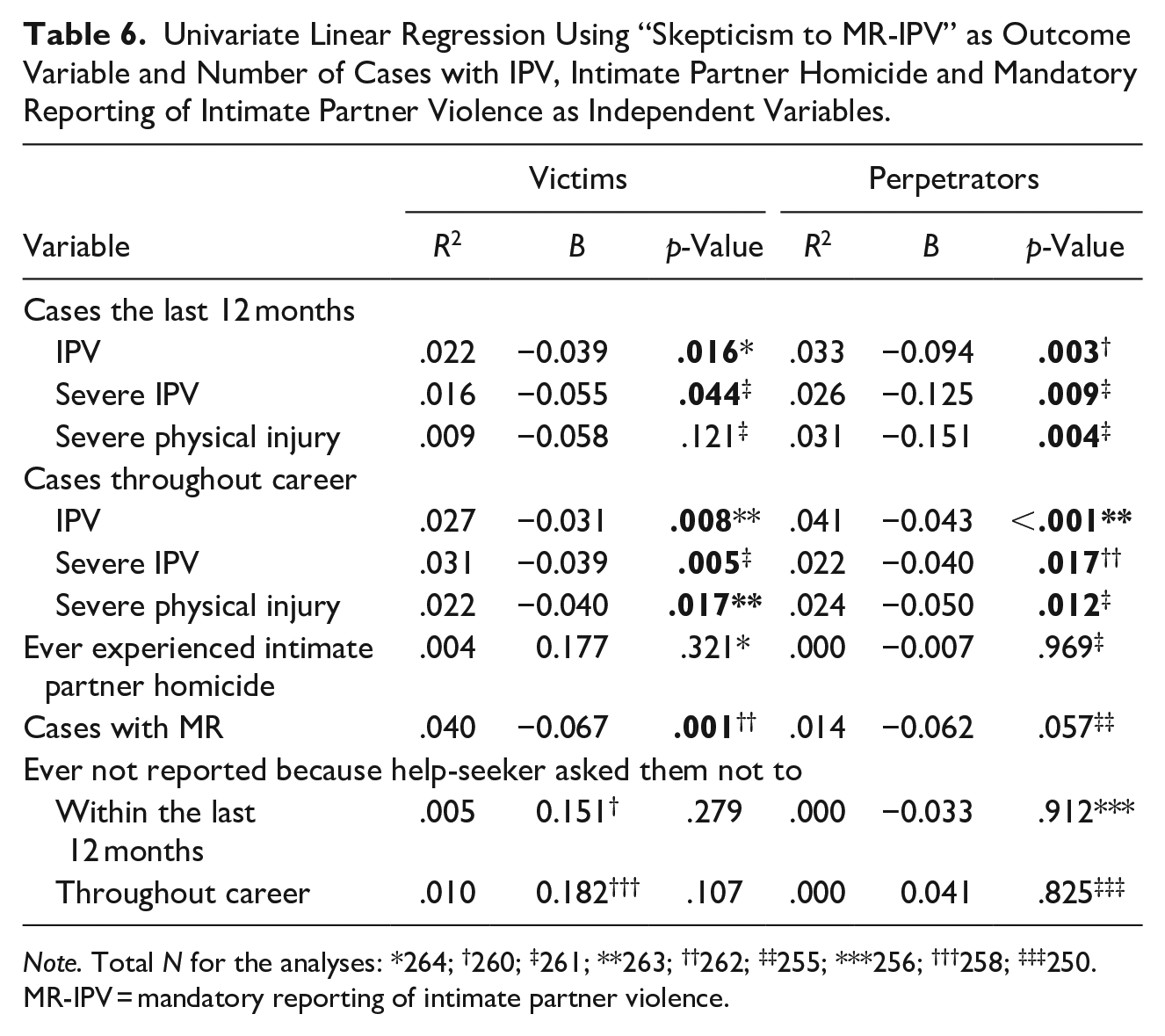
Note. Total N for the analyses: *264; †260; ‡261; **263; ††262; ‡‡255; ***256; †††258; ‡‡‡250. MR-IPV = mandatory reporting of intimate partner violence.
The longer participants had worked in their current position the less skeptical they were (see Table 7). Regarding awareness of MR-IPV, knowing the law in general and applied to their field, both responding yes and no (using dummy variables in linear regression) were significantly associated with skepticism toward MR-IPV. Participants who responded yes to being aware of the law of MR were less skeptical of MR-IPV, and responding no increased skepticism of MR. Additionally, the variables of having reported with consent and without consent from the victim or perpetrator were significantly predictive of being less skeptical of MR-IPV. However, using dummy variables, only reporting a certain number of times emerged as significant. Reporting 2 to 4 times and more than 10 times was significant for both reporting with and without consent, and reporting 5 to 10 times with consent was also significantly associated with being less skeptical of MR-IPV. The result of the MR report was not significant.
Univariate Linear Regression Using “Skepticism to MR-IPV” as Outcome Variable and Professional Contextual Variables as Independent Variables.
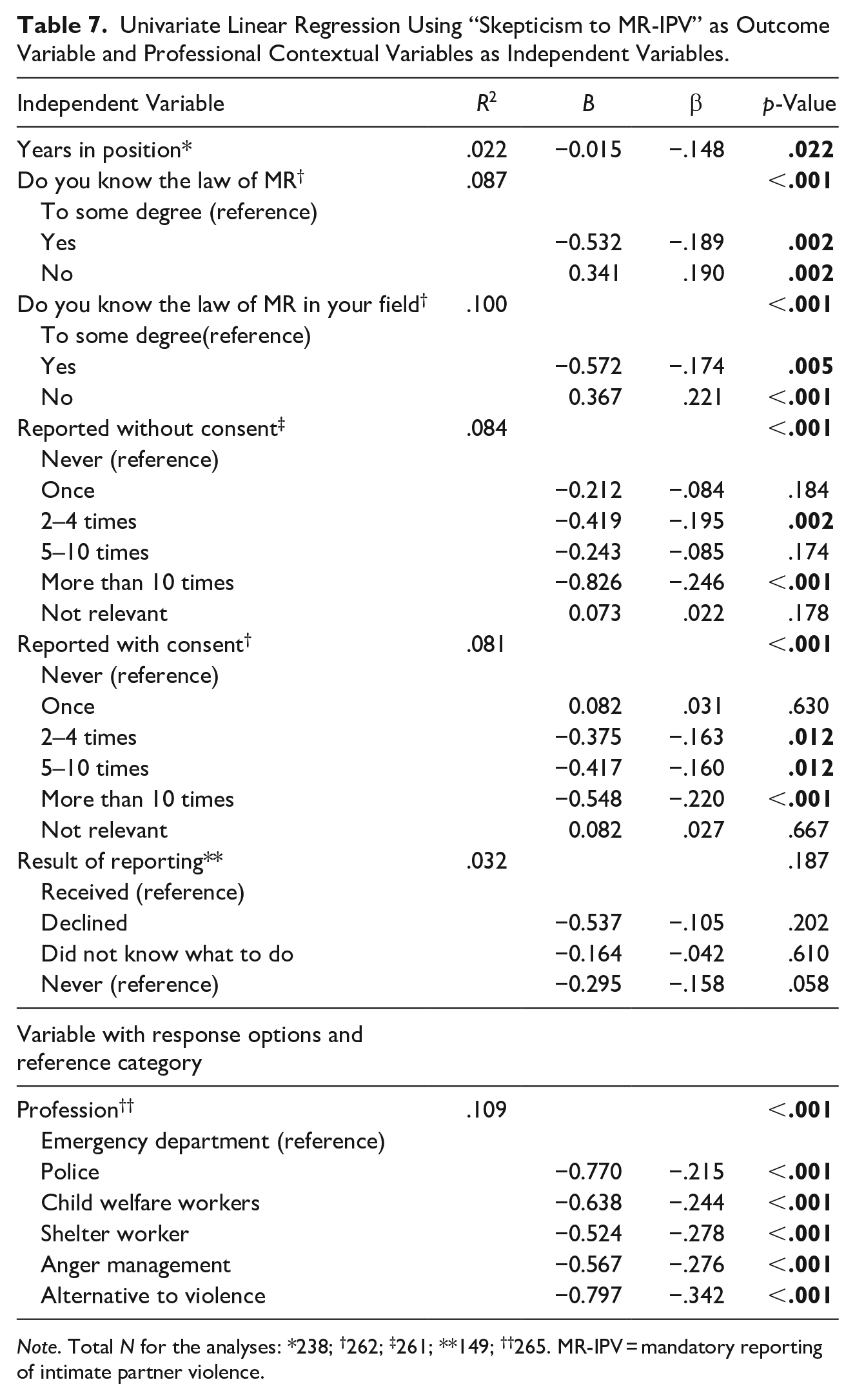
Note. Total N for the analyses: *238; †262; ‡261; **149; ††265. MR-IPV = mandatory reporting of intimate partner violence.
Group Differences Between SPs Regarding Attitudes Toward MR-IPV
Also shown in Table 7, amongst types of professions, only participants from the emergency rooms/sexual assault centers were significantly different than the other professions. They were more skeptical of MR-IPV. However, the longer the participants had worked in their current position, the less skeptical they were toward MR-IPV (see Table 7).
Multivariate Associations Between Professional Experiences with IPV and MR-IPV and Attitudes Toward MR-IPV
We included, as predictor variables, variables that were significant in univariate analyses (the number of cases with IPV, severe IPV, and severe physical injury, as well as the number of cases where MR was considered relevant, for both victims and perpetrators, during the last 12 months and throughout career). The criterion variable, as in the univariate analyses, was skepticism to MR-IPV. Although not significant in the univariate analysis, the number of cases with victims of severe physical injury within the last 12 months was included in the multivariate analyses, to confirm the lack of significance after adjusting for other variables. In addition, professional experience with violence regardless of severity, time of case, and victim/perpetrator is theoretically important and relatively absent in the literature on associations between experience and attitudes. Additionally, as each main variable was adjusted separately, double-checking this variable would have no impact on the results of the other main variables.
After adjustment, most variables with the number of cases of violence remained significant (see Table 8). The only non-significant variables were the number of cases with victims of severe physical injury during the last 12 months (confirming the univariate analysis), and the number of cases with victims of severe physical injury throughout careers. Notably, all significant variables had a negative effect size (indicating less skepticism toward MR-IPV), except for the number of cases with victims of IPV during the last 12 months. Again, cases with perpetrators of any type of violence had a stronger effect size overall relative to the same type of IPV and time frame for victims.
Multivariate Linear Regression Using “Skepticism to MR-IPV” as Outcome Variable and Experience with Intimate Partner Violence and Mandatory Reporting of Intimate Partner Violence.
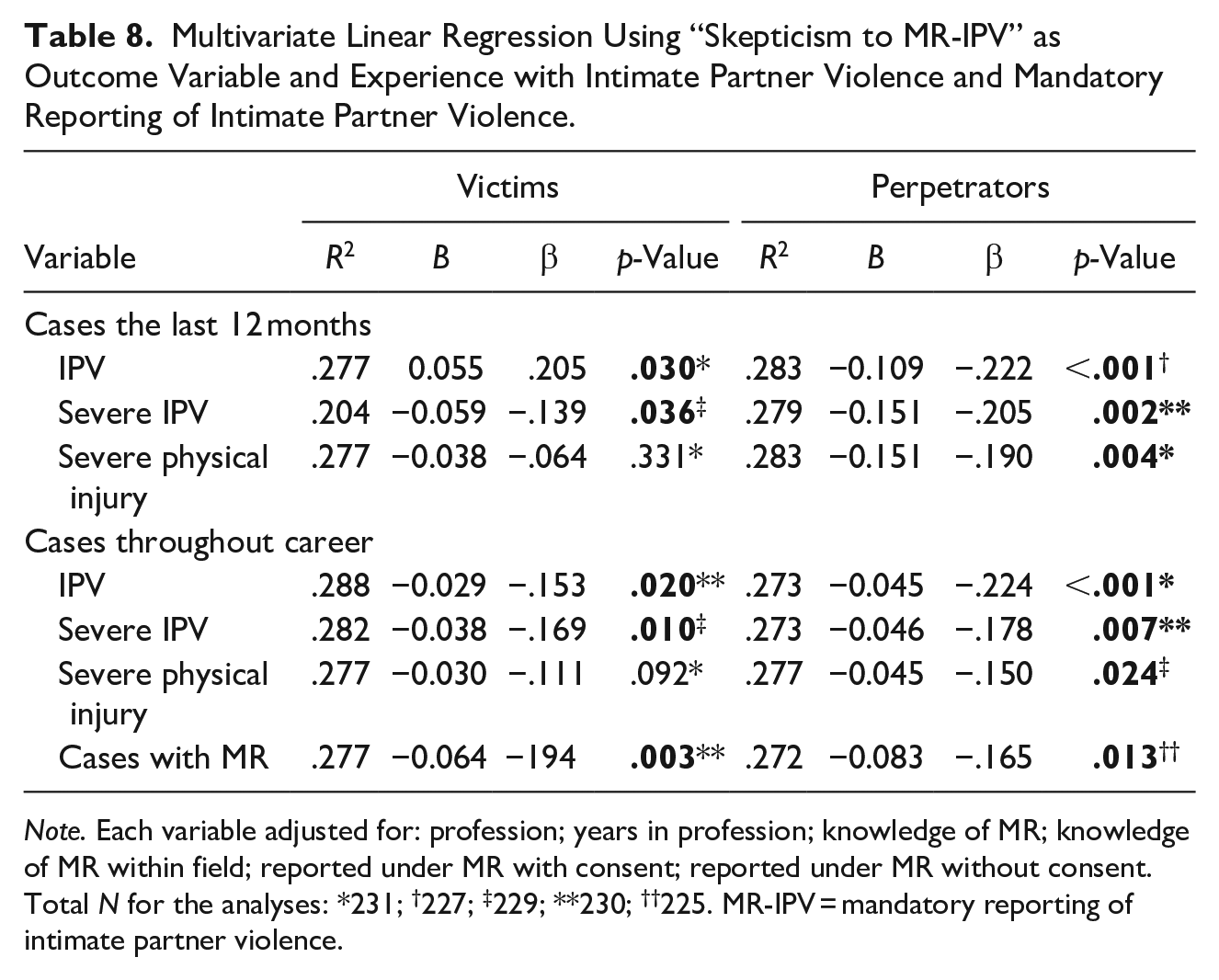
Note. Each variable adjusted for: profession; years in profession; knowledge of MR; knowledge of MR within field; reported under MR with consent; reported under MR without consent. Total N for the analyses: *231; †227; ‡229; **230; ††225. MR-IPV = mandatory reporting of intimate partner violence.
Discussion
Main Findings
The aim of this study was to investigate attitudes toward and professional experiences with MR-IPV amongst SPs. In addition, we evaluated to what extent SPs’ attitudes toward MR-IPV were predicted by professional experience with IPV and MR-IPV, and if there were any group differences amongst types of SPs. These findings are the first to demonstrate statistical associations between professional experience with IPV and MR-IPV and attitudes toward MR-IPV amongst SPs who work with perpetrators and victims of IPV.
Professional Experiences with and Attitudes Toward MR-IPV Among SPs
In accordance with previous studies, we found that SPs had various degrees of professional experience with MR-IPV (Allert et al., 1997; McDowell et al., 1994; Tilden et al., 1994; Smith et al., 2008). Slightly under half had never reported IPV throughout their career—with or without consent from a victim or perpetrator. Approximately 40% had reported IPV under MR, and roughly 10% considered MR not relevant for them. However, the prevalence of having professional experience with MR-IPV was higher in our study than in previous studies (Allert et al., 1997; McDowell et al., 1994; Smith et al., 2008; Tilden et al., 1994). In contrast to previous studies (Rodriguez et al., 1999; Tilden et al., 1994), participants generally agreed with statements that were supportive of MR-IPV and generally disagreed with statements that were opposed to MR-IPV. Agreements with supportive statements appeared, on a purely descriptive level, to be stronger than agreements to opposing statements.
Associations Between Attitudes Toward MR-IPV and Professional Experiences with MR-IPV, and IPV
When analyzing our predictor variables with “skepticism to MR-IPV” as the outcome variable, we found that the more IPV victims and perpetrators that participants had worked with, the less skeptical they were of MR-IPV. This finding was consistent regardless of the severity of violence, the timing of the case (last 12 months or throughout the career), or whether the case involved a victim or a perpetrator of IPV. The same result was observed for the number of cases where MR-IPV was considered relevant. These findings remained in adjusted multivariate models. To our knowledge, this is the only study investigating the associations between professional experience with IPV and MR-IPV and attitudes to MR-IPV. Theoretically, there are some possible explanations that can help us better understand the significance of experience.
Festinger’s (1957) theory of cognitive dissonance suggests that individuals change their attitudes in the face of behavior-attitude inconsistency. The results of the current study indicated that less skeptical attitudes to MR-IPV were associated with more professional experience with IPV cases in general and cases where MR-IPV would be considered relevant in particular. If we follow the framework of cognitive dissonance, it might suggest that their experience pushes their attitudes away from skepticism to MR-IPV. We cannot say, based on these results, that SPs are supportive or opposing MR-IPV because of their experiences, just that increase in experience is associated with being less skeptical. As such, it might suggest that SPs perceive nuances of positive and negative aspects of MR-IPV, as opposed to a dichotomized “pro or con” attitude. This is also supported by the theory of ambivalent attitudes, suggesting individuals can hold both negative and positive attitudes toward a target at one time (Harreveld et al., 2015).
Group Differences Between Types of SPs
Participants from the emergency departments/sexual assault centers were the only SPs significantly more skeptical about MR-IPV than the other SPs. Some previous studies have investigated differences between professions, although only between different types of health personnel. Rodriguez et al. (1999) investigated differences between medical specialties among physicians and found that some specialties were less compliant if a patient would object to reporting. However, this is not directly comparable to our results.
Mgopa et al. (2021) used focus groups (one with employed health personnel and one with health studies students) and found that the health personnel group expressed more positively toward reporting to the police (although they were not mandated to) than the students. This finding concurs with our finding that the longer the participants from emergency rooms had worked in their current position the less skeptical they were regarding MR-IPV. However, because of the qualitative method, professional experience was not measured by cases of IPV or MR-IPV, but rather assigned based on participants being SPs or students.
There might be context-related explanations for the group differences in our study. Confidentiality is highly recognized as a patient right (in Norway and elsewhere), not just among SPs but also the public (Vatnar et al., 2017; WHO, 2014). Although all SP groups included in this study are governed by confidentiality, there might be different perspectives on the primacy of MR-IPV compared to the participants from the emergency department. For instance, the police and child protective services are reliant on other professional groups to put aside confidentiality for the sake of MR for them to follow up both the investigation and for the protection of victims. Hence, it is perhaps not surprising that they would be less skeptical of MR-IPV. Child welfare services also routinely work as mandated reporters with respect to children’s welfare, so they would be more familiar with reporting on behalf of others in a vulnerable position.
The shelter workers, “alternative to violence” and “anger management” therapists, work nearest to IPV victims and perpetrators as their primary line of work. Consequently, they might have more regular professional experiences with MR-IPV and are evaluating and using MR-IPV regularly throughout their work. This might create a more nuanced perspective. Arguably, the SPs in the emergency department are in a more distinct position by working with a larger range of patients than victims and perpetrators of IPV. They might also be less often confronted with the dilemma of confidentiality and MR-IPV than the other groups.
Strengths and Limitations
The current study adds to the limited research on attitudes toward MR-IPV among SPs. It is the first to explore the association between actual professional experience with IPV and MR-IPV and attitudes toward MR-IPV. The methodology of measuring skepticism toward MR-IPV is a strength, as previous research has not evaluated attitudes toward MR-IPV on a continuum, but rather dichotomously. In addition, the sample included several groups of SPs that had not been explored before and was large compared to previous studies of MR-IPV. Notwithstanding, there are some limitations we would like to acknowledge. Unlike in a longitudinal or an experimental study, we were unable to measure attitude change or causality in the current study. Hence, we cannot infer that professional experience with IPV and MR-IPV and attitudes have a cause-and-effect relationship (i.e., whether experience with MR-IPV has led participants to be less skeptical, or less skepticism has led participants to report more.) We can only conclude that there is a statistical association between the two.
As explained in the methodology, our main outcome variable for this study was a collapsed score created through factor analysis. Unfortunately, due to this method, we had to exclude about 30% of our total sample size. Notably, it did not limit utilizing the type of analyses initially planned. The regression analyses, however, were only done on participants who had responded between “completely disagree” and “completely agree.” Participants who had, at any point, responded “I don’t know” were not included in the model. Responding “I don’t know” is still a valid response, and excluding such responses does lead to a bias toward participants who were, arguably, more conscious about their opinions. Missing responses were excluded in the same manner as “I don’t know” responses. On the other hand, after excluding unusable responses, the final responses were valid data, hence we did not have to impute any responses.
In our multivariate model, we discovered an inconsistency that could not be theoretically explained. In the univariate results, all effect sizes were negative (i.e., less skepticism); however, one significant variable changed directions in the multivariate model. This was the variable covering “cases with victims of IPV within the last 12 months.” Such a finding might result from “overadjustment” (Porta, 2008) because of the complex model (i.e., several adjusting variables). Although overadjustment can be a result of unnecessarily adjusting variables (Schisterman et al., 2009), that was not considered to be the case for this result. There can be several reasons for overadjustment (Lu et al., 2021) but it is difficult to say which one our result falls into. This limits our confidence in this finding.
Additionally, the factor analysis produced below desirable CFI, RMSEA, and alpha, which generate concerns. We acknowledge that there is a common standard for the CFI and RMSEA are above 0.90 and below 0.05, respectively. However, we want to point out that there is research that argues not meeting these criteria does not provide grounds to reject the model (Chen et al., 2008; Marcoulides & Yuan, 2016; van Laar & Braeken, 2021). We are aware that our data was not normally distributed which could contribute to the low CFI (van Laar & Braeken, 2021). More importantly, the factor score used as our dependent variable was not meant to be used as a validated scale, but rather a means to collapse items under a conceptual scale to measure an overarching theme. Consequently, we are confident in our results overall.
Generalizability
The current study took place in Norway, which has its own national jurisdiction on MR. Hence, we cannot guarantee that these results would generalize to other jurisdictions. Differences in jurisdictions might have an impact on the attitudes among SPs. As a Scandinavian country, Norway has a unique public health and welfare system where the majority of our participants are employed and the IPV victims and perpetrators seek help. Undoubtedly the accessibility to this system and limited financial cost influence the number of individuals who seek help compared to countries where the health system is either more privatized (and depends more on patients’ insurance) or is underdeveloped. In addition, we wanted to include gender inclusivity and allowed participants to respond “other” if they did identify as anything other than male or female, with space to define what this option might be. However, no participant utilized this option.
Our sample is also representative of all counties in the country, which means we would be able to represent areas with fewer inhabitants, local community cultures, as well as cultures within larger cities and communities. Additionally, it would allow for a more diverse sample where participants with foreign nationalities or ethnicities, who are more concentrated in some areas in the country, participate on the same level as native Norwegians and naturalized Norwegian citizens. Simultaneously, we still recognize that Norway is a small country in the global North and may not be generalizable to all other, even Western, or northern-European countries. There might also be cultural differences that cannot be fully accounted for in this study. Notwithstanding, our results are highly relevant internationally as an example of how attitudes toward guidelines and laws can be influenced by different factors and can differ between professions.
Implications for Future Research
Our findings suggest that although there is general support for MR-IPV among our sample, there are factors that influence the degree of skepticism toward MR-IPV. This is important to consider among SPs. Future research is encouraged within other jurisdictions, in order to test whether our findings are limited to the Norwegian context. Additionally, we encourage exploring other professions that might encounter IPV in other contexts and jurisdictions. We acknowledge there are other factors outside of our study that could influence attitudes and decision-making among professionals, for instance, the influence of authority from administration staff or leaders. This should also be explored. We presented theoretical grounds that might suggest our findings would be generalizable. We also recommend research on whether there are additional factors that might be associated with attitudes toward MR-IPV. Finally, our research will shed light on how attitudes might differ between professions.
Footnotes
Acknowledgements
Acknowledgment is due to Petter Laake for statistical advice. Gratitude is expressed to Stål K. Bjørkly for violence research advice. Acknowledgments are given to Silje L. Dahl, Susanne T. T. Kristiansen, Anita D. Linge, Astrid G. Vølstad for contribution to data collection. The authors express gratitude to the participants in this study for sharing their time and experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Research Council of Norway, project number 313902.