
Abstract
Theory suggests that intolerance of uncertainty (IU), a tendency to perceive uncertain events as threatening, may serve as a potential risk factor for increased intimate partner violence (IPV) perpetration; however, few studies have investigated this association, and none have taken a longitudinal approach. We investigated the issue in two longitudinal online investigations (initial N = 282 and 1,118), with time periods ranging from just before the COVID-19 pandemic to the fourth pandemic wave, approximately 1.5 years later. IU was a significant predictor of IPV cross-sectionally, and in the short term longitudinally (i.e., over periods of weeks); however, it did not predict IPV over the longer term (i.e., over periods of months or years). In addition, our longitudinal design allowed assessment of IPV trends across pandemic waves. Physical IPV rates remained low and steady across time. Psychological IPV rates showed an increase in the early days of the pandemic, but then dropped and stabilized, albeit at a somewhat higher rate than pre-pandemic. Study 2 had ample representation of LGBTQ+ respondents and showed that the patterns and processes worked similarly for LGBTQ+ and non-LGBTQ+ individuals.
Keywords
The experience of uncertainty (i.e., having to deal with circumstances where key information is missing) can be aversive for anyone. However, uncertainty may be especially difficult for individuals high in dispositional intolerance of uncertainty (IU), who perceive uncertain situations as threatening or aversive (Carleton, 2016). Mounting evidence suggests that IU may be associated with risk factors for perpetration of intimate partner violence perpetration (IPV), such as hypervigilance, mental health difficulties, jealousy, and anger. Despite the strong theoretical reasons to anticipate an association between IU and IPV perpetration, empirical assessments are sparse to date, and no longitudinal studies have yet been conducted.
In this article, we assess whether IU is associated with increased IPV perpetration frequency, whether cross-sectionally, in the short term (i.e., over periods of weeks) or in the longer term (i.e., over periods of months or years). We conducted two studies addressing this issue, before and during the first four waves of the COVID-19 pandemic, a highly relevant time period where uncertainty regarding pandemic risks and coping strategies was heightened for all. These assessments also provided a prime opportunity to assess whether and how IPV frequency itself changed over that same time period, as the pandemic continued to unfold. Fears of a “shadow pandemic” of heightened IPV were raised in the earliest stages of the pandemic (Kourti et al., 2023). Did that shadow pandemic in fact materialize, and if so, how long did it last? Finally, most research on IPV has lacked diversity, focusing primarily on the experiences of cisgender individuals in mixed-sex relationships (Lorenzetti et al., 2017). One of our two studies contained substantial representation from LGBTQ+ individuals, providing the opportunity to assess whether IU, IPV, or their association differed for LGBTQ+ and non-LGBTQ+ individuals.
IU and IPV Risk
The COVID-19 pandemic undoubtedly heightened uncertainty for everyone, as daily routines were disrupted and prognoses about the future became unclear. Some individuals, however, may have faced greater difficulties coping with this uncertainty (Rettie & Daniels, 2021). IU is a dispositional tendency to perceive situations where key information is missing or insufficient as being threatening or aversive, resulting in increased emotional distress and maladaptive efforts to gain greater certainty (Carleton, 2016; Shihata et al., 2016).
A growing body of literature suggests that those high in IU may display behaviors that place them at heightened risk of IPV perpetration. When faced with uncertainty, they become hypervigilant and make negatively biased threat appraisals, resulting in increased emotional distress and maladaptive efforts to gain greater certainty (Tanovic et al., 2018). IU may also contribute to outward expressions of anger and aggression, particularly among those who view uncertainty as unfair and unavoidable (e.g., Fracalanza et al., 2014 1 ). IU has been proposed as a contributor to jealousy in relationships (Leahy & Tirch, 2008), a known risk factor for IPV perpetration (Langhinrichsen-Rohling et al., 2012). Further, IU is associated with a variety of mental health problems, including anxiety and PTSD (see Carleton, 2016 for review), which are also known risk factors for IPV perpetration (Spencer et al., 2019).
Despite the strong theoretical justification for expecting an association between IU and IPV perpetration, there has been relatively little empirical research to date. Some studies have considered related constructs, such as general aggressive behavior (Celik et al., 2021) or IPV victimization (Momeñe et al., 2022), or focused on only very specific forms of IPV perpetration (i.e., cyber aggression and social media surveillance; McMillan et al., 2022). We were only able to find one directly relevant study. In a study conducted at the beginning of the COVID-19 pandemic, Glowacz et al. (2022) determined that those higher in IU tended to feel more anxious and depressed, which in turn was associated with an increased likelihood of perpetrating psychological and physical IPV. This study was limited, however, by its cross-sectional design, making it difficult to discern the directionality of the association. It also assessed study variables only at one time point early in the pandemic’s first wave. Would similar results also apply in other time periods?
To extend Glowacz et al.’s (2022) findings, we explored the association between IU and IPV perpetration prior to the pandemic’s onset and across the initial four pandemic waves in North America. We predicted that higher levels of IU would predict more perpetration of psychological and physical IPV, cross-sectionally and longitudinally, over both shorter time periods (i.e., weeks to a few months) and longer time periods (i.e., multiple months to 1.5 years). As addressed more in the “Discussion” section, if IU does in fact emerge as a consistent predictor of IPV, it opens up potentially fruitful new avenues for clinical intervention.
IPV During the COVID-19 Pandemic
Because our studies were conducted across the first four pandemic waves, we can also add to the growing body of literature assessing IPV risk during the COVID-19 pandemic. Past research, prior to the pandemic, suggested that during times of crisis and health emergencies, increases in gender-based violence, including relational conflict and IPV, are often observed (Stark et al., 2020). Consistent with this prior research, IPV rates did appear to increase following the onset of lockdowns during the COVID-19 pandemic. A systematic review and meta-analysis of studies found an increase in IPV rates post-lockdown across most studies, particularly within the United States (Piquero et al., 2021). However, many of these studies were conducted during the pandemic’s very early days, when lockdowns were common; they also focused predominantly on IPV victimization, rather than perpetration (see Kourti et al., 2023, for review). The lockdown period might have been associated with especially high rates of IPV, given forced time together for couples during a period of increased stress and social isolation. On the other hand, the lockdown period might have potentially underestimated any IPV increase. Most studies reviewed by Piquero et al. (2021) drew on data obtained from crisis hotlines and police or emergency department records. Access to some of these resources might have been reduced during the lockdown period, with IPV victims trapped at home being unable to reach out for support.
Our study will contribute to the existing literature by providing information on IPV perpetration rates, as well as victimization rates (in Supplemental Material). We provide self-report data, to provide convergent validity for prior research that primarily relied on archival reports. We will examine IPV rates pre-pandemic, in the early stages (first pandemic wave; original variant), and then across time, in the second (Alpha variant), third (Delta variant), and fourth (Omicron variant) pandemic waves, providing much more extensive longitudinal data than has heretofore been present in any one study. If the increased IPV that occurred in the earliest days of the pandemic was only a short-term effect, then the need for temporarily heightened interventions has passed; if the effects should prove to be much longer term, then service providers must explore ways to bolster support on an ongoing basis. Consistent with previous research, we anticipate an increase in IPV rates in the first pandemic wave relative to pre-pandemic baseline; however, given the paucity of longitudinal data, we leave the issue of whether IPV rates remained elevated in later pandemic waves as an open research question.
IU and IPV in LGBTQ+ Populations
In one of our two studies, we made strong efforts to recruit LGBTQ+ participants, to learn more about their pandemic experiences. Considering the LGBTQ+ population is important for diversity, as it is severely underrepresented in research. For example, Walch et al. (2020) found that although the number of empirical psychological studies containing LGBTQ+ representation quadrupled from 2000 to 2015, such studies still represented only 0.2% of all literature reviewed.
IPV certainly occurs within sexual and gender minority relationships (Rollѐ et al., 2018; Wirtz et al., 2020). IPV victimization may be higher, on average, for LGBTQ+ individuals than their cisgender and heterosexual counterparts (Jaffray, 2021a, 2021b). IPV perpetration patterns are much less clear, in part due to definitional and measurement issues (Mason et al., 2014). Overall, research on IPV in LGBTQ+ relationships, including during the COVID-19 pandemic, remains sparse. However, some preliminary research suggests that LGBTQ+ individuals may have been particularly vulnerable to IPV during the early stages of the pandemic, due to issues such as social isolation, stigmatization, and health disparities (Stephenson et al., 2022).
In addition, because LGBTQ+ individuals are not well represented within the IU/uncertainty literature, little is known about how well they might tolerate uncertainty relative to their non-LGBTQ+ counterparts, or about the extent to which IU among LGBTQ+ individuals might contribute to other problems, including IPV. Only one known pre-pandemic, unpublished study compared IU average scores between LGBTQ+ and non-LGBTQ+ individuals, with LGBTQ+ individuals reporting higher mean IU than their non-LGBTQ+ counterparts (Kelders et al., 2019). We extend the existing literature by comparing IPV and IU scores across LGBTQ+ and non-LGBTQ+ groups, as well as assessing whether the association between those variables is similar or different across groups. If there are important group differences, that information can help service providers to better tailor their treatment to their clients’ unique needs.
Current Study
To summarize, the purpose of the current study was to: (a) examine the relationship between IU and IPV perpetration prior to and during the COVID-19 pandemic; (b) investigate changes in IPV perpetration rates from pre-pandemic baseline and across the first four pandemic waves in North America; and (c) determine if IPV rates and IU, and/or the association between these two variables, varied depending on LGBTQ+ group status.
Research Questions and Hypotheses
H1: IU will predict IPV perpetration, cross-sectionally, and prospectively over the short term (i.e., weeks to a few months) and the longer term (i.e., many months to 1.5 years).
H2: There will be an increase in IPV perpetration from pre-pandemic baseline to the first wave.
RQ1: How will IPV rates change over the course of the first four waves of the pandemic?
RQ2 (Study 2 only): Will IU levels, IPV rates, or the association between the two differ for LGBTQ+ versus non-LGBTQ+ individuals?
Method
Recruitment and Procedures
Study 1
Both studies’ procedures were approved by the participating universities’ Research Ethics Boards. Between December 2019 and early January 2020, that is, shortly before the COVID-19 pandemic’s March 2020 onset in the United States, participants for Study 1 were recruited online from Amazon’s Mechanical Turk (MTurk) for a study on uncertainty and relational conflict. Participants had to be 18 years or older, currently in a mixed-sex intimate relationship and residing in the United States. Participants completed a consent form, demographics, and a series of online questionnaires that took approximately 45 min to complete. Participants were compensated US$1.50. Following survey completion, participants were directed to a debriefing form, including contact information for mental health resources.
Consistent with best practices (Chmielewski & Kucker, 2020), various techniques were employed to ensure data quality in all Study 1 surveys: participants had to have completed a minimum of 1,000 MTurk tasks, with a cumulative approval rating >99%; a CAPTCHA was used to deter bots; an attention check requiring a specific open-ended response was used; and participant responses to open-ended responses were reviewed for nonsensical responses.
Those who met all criteria in the baseline survey (N = 282) were invited to participate in a series of four 15 to 20 min follow-up surveys, one every 2 weeks, during the first pandemic wave (i.e., spring 2020), each focusing on experiences in the previous 2 weeks. Survey invitations were sent on the first date noted, with a reminder sent on the second day. Participants had until the third day to complete the survey: April 13 to 15 (Time [T]1; N = 118), April 27 to 29 (T2; N = 145), May 11 to 13 (T3; N = 135), and May 25 to 27 (T4; N = 142). Payment increased gradually from US$1.25 to US$2.00, plus a bonus for completing at least three of the four surveys.
Participants who completed at least two biweekly surveys (N = 150) were later invited to complete three longer-term follow-up surveys during the second pandemic wave (August 3–5, 2020; T5; N = 93), the third pandemic wave (February 1–3, 2021; T6; N = 74), and the fourth pandemic wave (February 7–9, 2022; T7; N = 65). Compensation was US$2 per survey.
Study 2
Participants, 18+ (or 16+ if a university student), were recruited to participate in an online survey of pandemic experiences, with an emphasis on recruiting LGBTQ+ participants. To be included in the current analyses, participants had to be in a romantic relationship, and have completed the relevant measures (N = 1,118). The intake survey was completed during the first pandemic wave (i.e., May–June 2020). Participants provided consent, completed a 45-min survey, and were debriefed, including information on supports and resources.
Participants could then elect to complete 10-min daily diary surveys for up to 28 days, if desired. The measure for the current study was administered only twice, on Days 14 and 28. To be included in the current analyses, participants had to be in a relationship with the same partner as at intake and have completed at least one of the two relevant diary surveys (N = 336).
Approximately 1.5 years later, in November 2021 (i.e., fourth pandemic [Omicron] wave), intake participants were recontacted and invited to participate in a follow-up survey, repeating many of the original measures. To be included in the current analyses, participants had to still be with the same partner as at intake and have completed the relevant measure (N = 399). Participants were compensated via entry into prize draws at all stages.
Measures
Participants answered demographic questions in each study. They also completed a wide variety of additional measures; only ones relevant to the current study are described below.
Intolerance of Uncertainty
Study 1 employed the full 27-item version of the Intolerance of Uncertainty Scale (IUS; English translation, Buhr & Dugas, 2002), administered at the pre-pandemic intake survey and at T6. Study 2 employed the shortened 12-item version of the IUS (Carleton et al., 2007), at intake only. Items assess a discomfort with uncertainty (e.g., “I can’t stand being taken by surprise”) and difficulty coping with uncertain situations (e.g., “When I am uncertain I can’t function very well”). Items are rated on a 5-point Likert scale ranging from 1 = not at all characteristic of me to 5 = entirely characteristic of me, and are summed to create a total IUS score. In past research, the full IUS has shown excellent internal consistency (α = .94), good test–retest reliability (r = .74), and good convergent and divergent validity (Buhr & Dugas, 2002). The brief version correlates highly with the full version (r = .96), and also shows excellent internal consistency (α = .91; Carleton et al., 2007), as well as good discriminant validity (Khawaja & Yu, 2010). In the current study, Cronbach’s alphas were excellent (Study 1 intake = .97; Study 1 T6 = .96; Study 2 intake = .91).
Intimate Partner Violence
Study 1 intake employed the full 78-item version of the Revised Conflict Tactics Scale (CTS2; Straus et al., 1996), whereas all other timepoints for both studies used a shortened 40-item version. In both cases, only the items assessing psychological and physical IPV perpetration frequency are presented here; data from the victimization items are presented in Supplemental Material. The measure uses a 7-point Likert scale, ranging from 0 = Never to 6 = More than 20 times, to assess acts of IPV perpetration and victimization. The time period covered varied: 1 year for Study 1 intake, 1 month for Study 2 intake and long-term follow-up, and 2 weeks for all other timepoints in both studies. Frequency scoring was used, in which the midpoint of the range of options provided for each scale response is assigned (e.g., “3–5 times” is scored as 4), and a total score is calculated across the items.
The psychological and physical IPV subscales of the CTS2 have adequate internal consistency and good construct, concurrent and discriminant validity (Shorey et al., 2011; Straus et al., 1996). In the current study, most Cronbach’s alphas were acceptable for Study 1, ranging from .76 to .99; however, Cronbach’s alphas were lower (in the .60 range) for three timepoints (T3, T6, T7) for Study 1, and for all time points for Study 2. Cronbach’s alphas for physical IPV could also not be meaningfully calculated at some time points because the variability was so low. We address this issue of low reliability in “Discussion” section.
LGBTQ+ Identity
Participants who indicated any sexual identity other than straight, any gender identity other than man or woman, or that their gender identity did not match their sex assigned at birth, were coded as having an LGBTQ+ identity; other participants were coded as not LGBTQ+. “Not Listed” responses to gender and/or sexual identity questions were coded appropriately (e.g., demisexual = LGBTQ+; “heterosexual” = not LGBTQ+).
Participants
Complete demographic information is given Supplemental Material: Part 2. The modal participant in both studies was a straight, White, relatively well-educated young to middle-aged adult in a long term, committed relationship, cohabiting with their partner. Study 1 respondents were all American, whereas Study 2’s were primarily Canadian.
Analysis Strategy
Single imputation was used to replace any individual missing items on the IU or CTS2 scales, before creating total scores. Primary analyses were conducted using regression for cross-sectional analyses and multilevel modeling for longitudinal analyses (via the lme4 package in R; Bates et al., 2015). List-wise deletion was employed for regression analyses, and full-information maximum likelihood was used to deal with missing data for multilevel models. The dependent variable for all analyses was the frequency of IPV perpetration over the relevant time period. The primary predictor variable was IU, mean-centered (Level 2). Where appropriate to the analyses, the moderating variables of time (Level 1) and LGBTQ+ status (Level 2) were added to the models, along with all possible interaction terms. If interactions were present, simple slopes were probed using the interactions package in R (Long, 2019). See Supplemental Material: Part 3 for details on exploratory analyses applying different variations of the time coding and Part 4 for information on the results when the covariates of age, cohabitation, and time commencing the study were included in the analyses (i.e., no changes except for one instance, noted below).
Results
Descriptive Statistics
Table 1 shows both the frequency and prevalence of IPV perpetration for both studies at all time points. Comparable results for IPV victimization are shown in Supplemental Material: Part 5. Psychological aggression was relatively common in both studies; however, with the exception of Study 1 intake, physical aggression frequencies were extremely low. Given the floor effects, the analyses for physical IPV perpetration were only conducted for Study 1 intake.
Frequency and Prevalence of Intimate Partner Aggression Perpetration, All Timepoints for Both Studies.
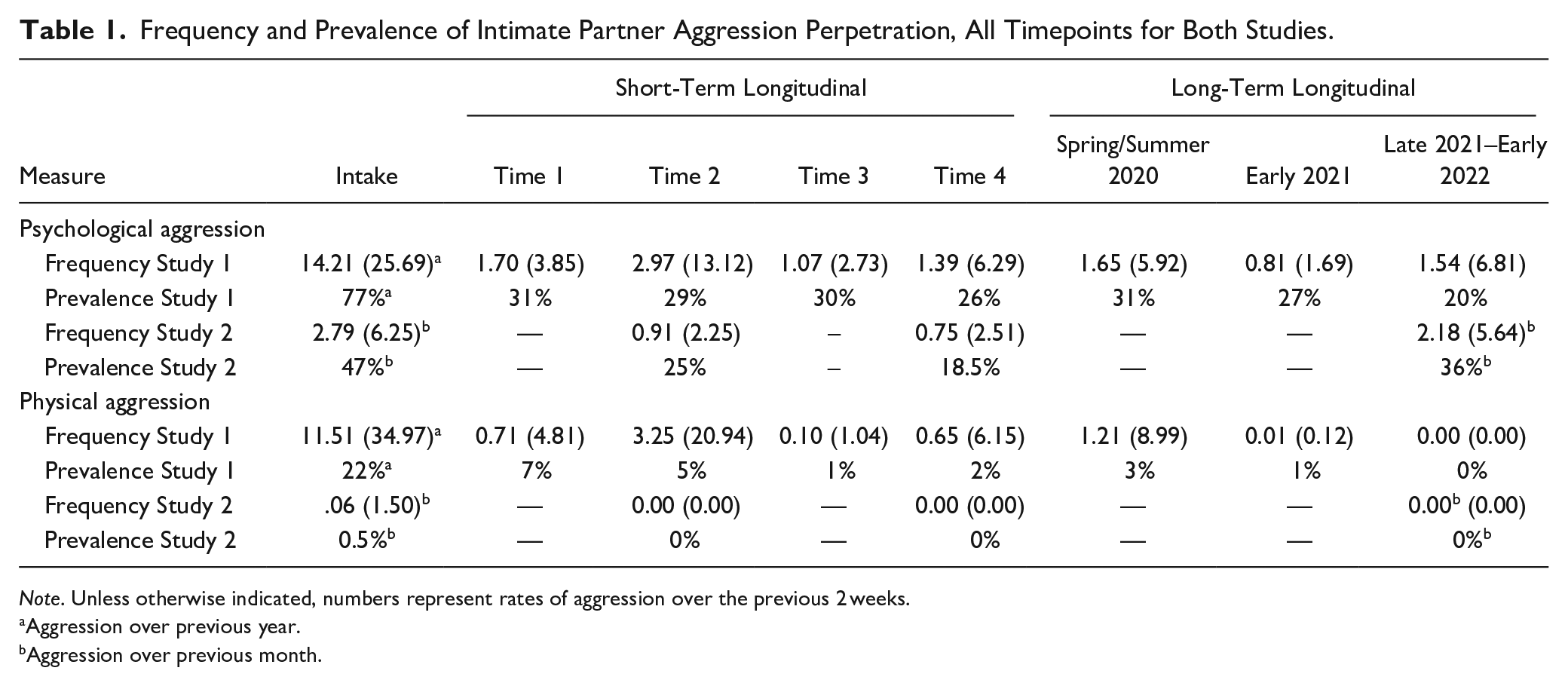
Note. Unless otherwise indicated, numbers represent rates of aggression over the previous 2 weeks.
Aggression over previous year.
Aggression over previous month.
Primary Analyses
Table 2 shows the results of the primary analyses for psychological IPV perpetration, for both studies and all timepoints. H1 was supported in both the cross-sectional and short-term longitudinal analyses. As predicted, higher IU scores were associated with higher levels of self-reported psychological IPV perpetration. The association was significant in four of the five analyses, and marginally significant in the fifth. The cross-sectional analyses on physical IPV perpetration for Study 1 intake also supported H1 (b = 0.50, SE = 0.08, p < .001). However, H1 was not supported in the long-term longitudinal analyses.
Intolerance of Uncertainty as a Predictor of Psychological Intimate Partner Aggression.
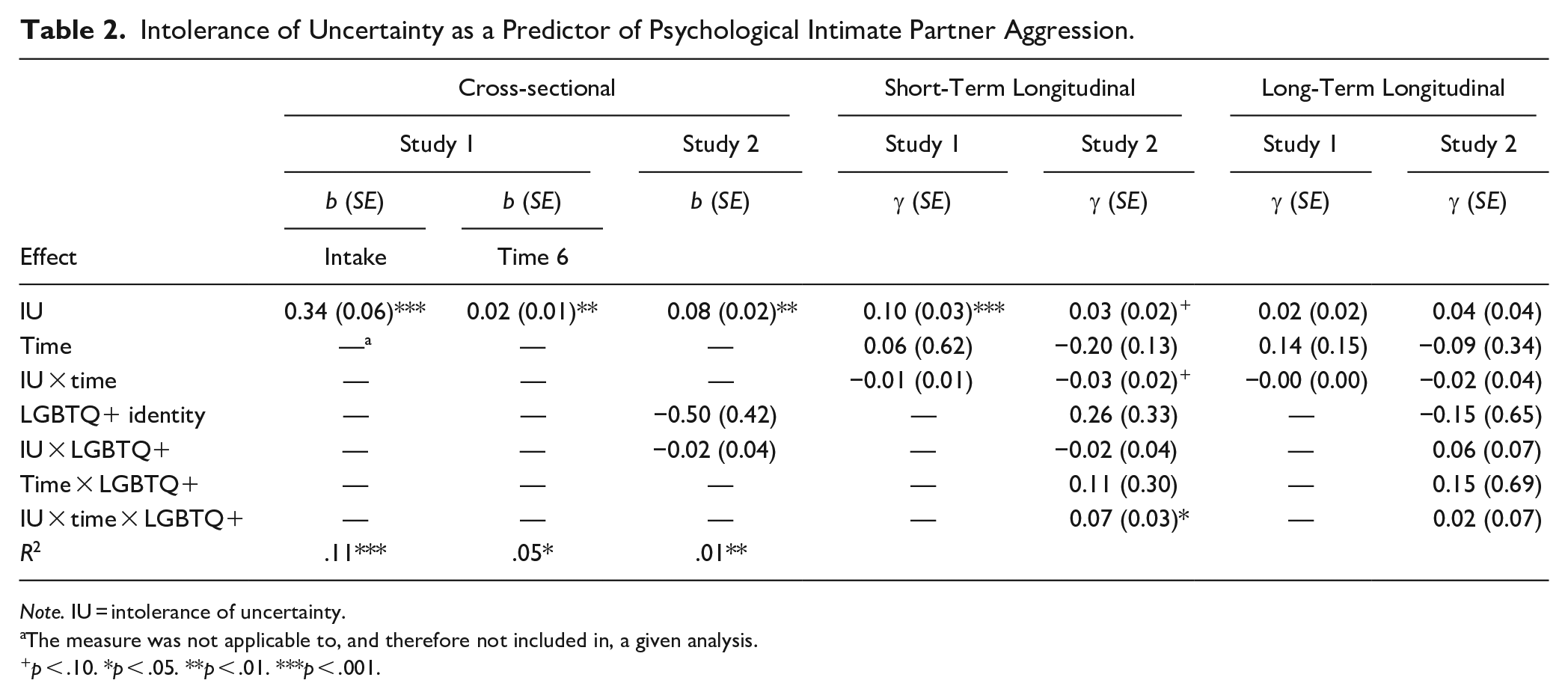
Note. IU = intolerance of uncertainty.
The measure was not applicable to, and therefore not included in, a given analysis.
p < .10. *p < .05. **p < .01. ***p < .001.
In general, the research questions were answered in the negative. Time and LGBTQ+ identity generally did not predict IPV perpetration, whether alone, together, or in combination with IU. The sole exception was in the short-term longitudinal analyses for Study 2, where there was a significant three-way interaction between IU, time, and LGBTQ+ identity, graphed in Figure 1. At Time 1, there was a slightly stronger association between IU and psychological IPV perpetration for non-LGBTQ+ individuals (b = 0.03, p = .09) than for LGBTQ+ individuals (b = 0.01, p = .76). However, at Time 2, the positions had reversed. Now, there was no association between IU and psychological IPV perpetration for non-LGBTQ+ individuals (b = −0.00, p = .98), while the association was slightly stronger for the LGBTQ+ group (b = 0.05, p = .11).
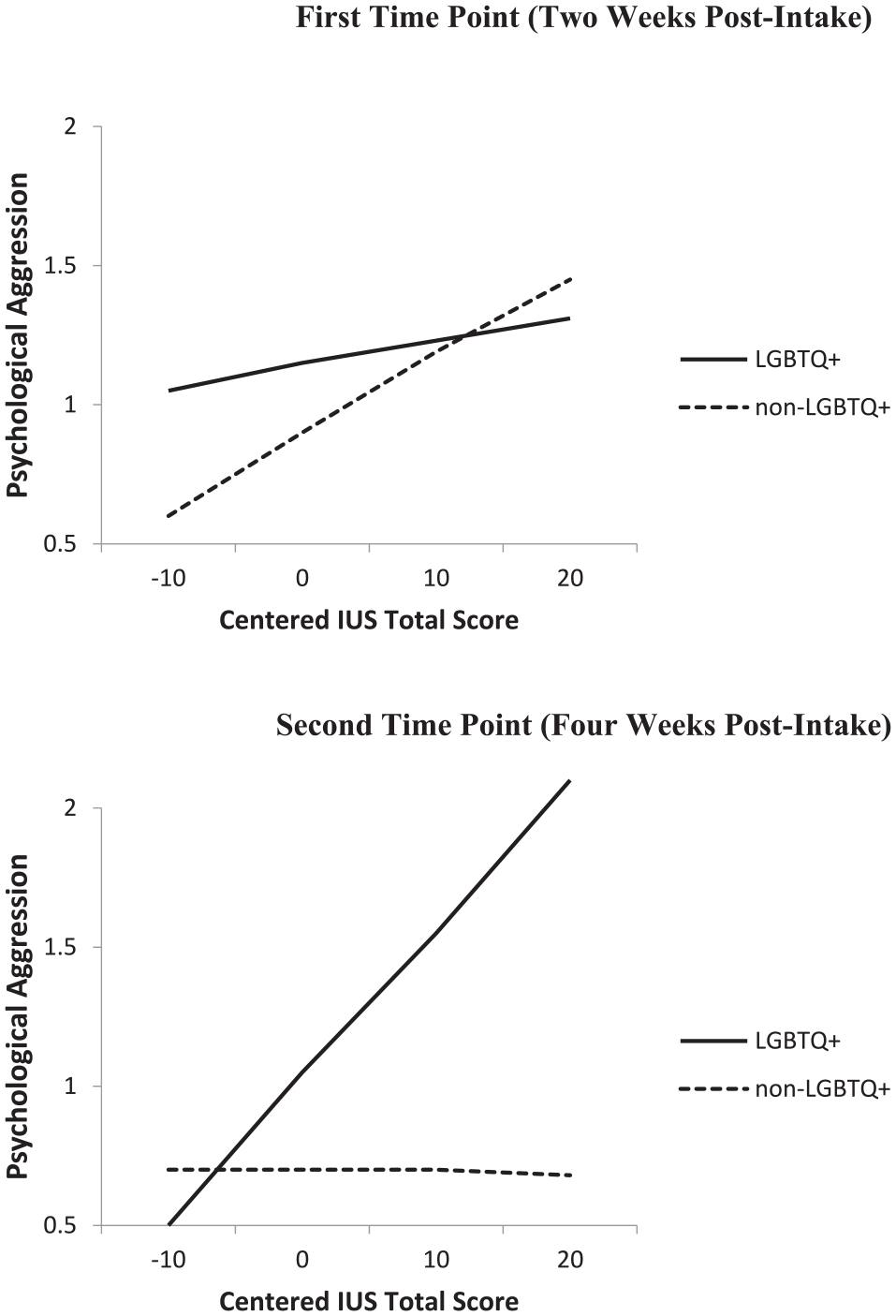
Interaction between Intolerance of Uncertainty Scale scores, LGBTQ+ identity and time, predicting psychological aggression within the Study 2 short-term longitudinal analyses.
IPV Perpetration Rates Across Time
There were no significant main effects of time in any of the primary analyses, suggesting psychological IPV rates remained relatively stable across the course of the pandemic. However, these analyses would only capture linear effects of time, and the trajectory of IPV across the pandemic might have followed a more complex pattern. It is difficult to make across-time comparisons with confidence when reports encompass different timeframes; however, on an exploratory basis, frequency scores were divided as appropriate to rescale all scores to a 2-week reporting period. Within-subjects t-tests were then conducted, comparing scores at every time point to every other time point. Full details are presented in Supplemental Material: Part 6. Key findings are that physical IPV perpetration rates remained low and stable across time. For psychological IPV perpetration, consistent with H2, there appeared to be a small, short-term increase in psychological aggression early in the pandemic, followed by a drop-off; however, rates still remained slightly elevated, relative to pre-pandemic levels, across time.
LGBTQ+ Group Differences
LGBTQ+ identity did not predict psychological IPV frequency in any of the primary analyses; however, these analyses included additional predictor variables, with overlapping variance that might have obscured group differences. To confirm, we conducted between-subjects t-tests, comparing psychological IPV frequency between LGBTQ+ and non-LGBTQ+ participants at each time point. No differences emerged (all ts < 0.80; all ps > .40).
We also conducted a between-subjects t-test comparing the two groups on IU at Study 2 intake. LGBTQ+ individuals (M = 32.82, SD = 9.80) had significantly higher IU levels than non-LGBTQ+ individuals (M = 29.62, SD = 8.82) with the t-test: t(531) = −5.05, p < .001, d = .35. However, this group difference disappeared when an ANCOVA was conducted (adjusted LGBTQ+ M = 31.06; non-LGBTQ+ adjusted mean = 30.31; group effect F[1, 1,094] = 1.28, p = .26). Specifically, the covariates of age (F[1, 1,094] = 57.45, p < .001) and the week the participant began the study (F[1, 1,094] = 10.23, p = .001) were both significant. LGBTQ+ individuals only appeared to be higher in IU because, on average, they happened to be younger and to have started the study slightly later than the non-LGBTQ+ participants.
IU Across Time
Contrary to expectations, IU was not a significant predictor of IPV perpetration in the longer term. One possible explanation is that people’s experiences of IU changed over the course of the pandemic. In Study 1, IU was assessed twice, once at intake (pre-pandemic) and again at T6, just over a year later. Scores at these two time points were very highly correlated, r(73) = .85, p < .001, suggesting strong test–retest reliability. However, those who completed the T6 measure started out with marginally lower IU scores at intake (M = 60.16, SD = 24.54, N = 74), compared to participants who did not complete the T6 measure (M = 66.24, SD = 25.96, N = 208; t[280] = 1.75, p = .08, d = .24). Furthermore, those who reported the IU measure at both time periods showed a significant drop in their IU scores from intake (M = 60.16; see above) to T6 (M = 53.07, SD = 21.52; t[72] = 4.43, p < .001, d = .52).
Discussion
IU and IPV
As hypothesized, IU was a significant predictor of both physical and psychological IPV perpetration cross-sectionally, consistent with Glowacz et al.’s (2022) findings. These associations were not limited to the pandemic period, as they also occurred at Study 1 intake, before the pandemic began. Individuals who are higher in IU generally may be more hypervigilant to uncertainty and more apt to interpret it as threatening and unfair (Fracalanza et al., 2014). Such cognitions may elevate emotional distress and lead to maladaptive coping behaviors (Tanovic et al., 2018), including anger and aggression (e.g., Fracalanza et al., 2014). These findings are consistent with other conceptualizations of uncertainty’s impact on stress and relational functioning (e.g., Boss, 2016). Additional research is needed to better understand how IU and uncertainty in different contexts contribute to relational problems.
Importantly, IU represents a potential nexus for intervention. Early IPV perpetrator interventions, still commonly used in the United States, often focus on psychoeducation and consciousness-raising (i.e., Duluth-model-based interventions) but afford few to no benefits in reducing IPV recidivism (Babcock et al., 2024). Targeting malleable IPV perpetration risk factors such as IU may be more fruitful. There are promising new CBT-based interventions that help to reduce IU (see Shihata et al., 2016), that could be used as standalone or supplemental treatment to existing IPV interventions. Helping clients improve their ability to cope effectively with uncertain situations may also have associated benefits (e.g., reduced distress, better problem-solving and communication skills) that indirectly reduce IPV risk. Thus, teaching clients to better tolerate uncertainty may be a key skill for therapists to incorporate into their treatment programs for IPV perpetrators.
Associations Between IU and IPV Across Time
Our study extends previous work by examining associations between IU and IPV across time. Consistent with H1, we found earlier IU to be a significant predictor of later psychological IPV perpetration over the shorter term (i.e., weeks to a few months). Longitudinal studies such as ours effectively rule out reverse causation: for example, heightened IPV at Time 2 cannot cause elevated IU measured at Time 1. However, we still cannot rule out potential third variables, such as chronic stress or long-term chaotic living situations, being responsible for both heightened IU and IPV. In fact, we expect such complex, mutually reinforcing webs to exist. Again, however, IU represents a potentially treatable construct that could potentially disrupt maladaptive cycles.
Although IU did predict IPV as expected cross-sectionally and in the short term, it did not predict over the longer term. This finding requires replication and further analysis. One potential explanation might be attrition bias. More of the “action” in the association between IU and IPV might be driven by those who are higher in the constructs. IPV dropped over time, and those who continued in the study over time had relatively low IU levels, perhaps leading to floor effects.
Another issue could be changes in IU itself over time. Although assumed to be trait-like, previous research has only assessed test–retest reliability of the IUS over fairly short periods of time (i.e., 6 months or less; Bredemeier et al., 2019). We added to the literature by assessing test–retest reliability over a period of more than 1 year. We found it to be strong, indicating that the relative ranking of participants remained very stable over time. However, the group’s average IU dropped over time. Most individual changes in IU scores were small, but some were large (e.g., a drop of 52 points), suggesting IU can at times be quite malleable. Further research is needed to understand the extent to which IU is truly trait-like versus responds to environmental factors. If IU is less trait-like than assumed, then it may be a promising target for intervention. However, less-stable IU also means that IU measured at one time in one set of circumstances may not predict outcomes measured under very different circumstances. In the context of the pandemic, for example, individuals may have become acclimated over time to the new realities, reducing their feelings of uncertainty and making IU a less relevant predictor. Alternatively, as lockdowns lifted over time, those high in IU may have had more opportunity to aggress against a wider range of targets when emotionally distressed, reducing the association with aggression against their intimate partner specifically. Overall, additional longitudinal research is needed to clarify when, whether, and how IU changes over time, as well as the utility of its predictive power under different life circumstances.
LGBTQ+ Versus Non-LGBTQ+ Participants
In Study 2, we assessed whether our results were moderated by LGBTQ+ status. With the exception of one very small interaction effect that should likely not be over-interpreted, they were not. LGBTQ+ and non-LGBTQ+ individuals did not differ in their IPV perpetration rates. There have been mixed findings from prior, albeit limited, research on differences in IPV perpetration rates among LGBTQ+ and non-LGBTQ+ individuals (Edwards et al., 2015): sometimes IPV perpetration rates are higher in LGBTQ+ samples, and sometimes they are not, as in our study. Given the general lack of research on IPV within LGBTQ+ communities, particularly among gender minority individuals, more research is needed to better understand the dynamics of IPV perpetration within LGBTQ+ relationships.
In our study, LGBTQ+ and non-LGBTQ+ groups did not differ in their levels of IU, after controlling for covariates, particularly age. This finding contrasts with results from Kelders et al. (2019), who found heightened IU in LGBTQ+ participants; however, they did not control for age or other potential demographic differences between their groups, which may account for the study differences. Tentatively, however, our findings suggest that LGBTQ+ and non-LGBTQ+ groups experience similar levels of IU.
Importantly, we also found that the association between IU and IPV perpetration did not generally vary by LGBTQ+ status. As is often the case (Kurdek, 2006), basic relationship processes seem to work very similarly, regardless of relationship type. In the area of IPV as well, past research suggests that many IPV perpetration risk factors are similar for LGBTQ+ and non-LGBTQ+ individuals (Edwards et al., 2015). It is always important for service providers to maintain awareness of the unique needs of any minority populations they serve; still, our findings tentatively suggest that treatments targeting IU to reduce IPV risk might be beneficial for LGBTQ+ and non-LGBTQ+ individuals alike.
IPV Across Time in the Pandemic
Finally, although our primary focus was on the association between IU and IPV, the fact that the data were collected across four different pandemic waves during the first 2 years of the pandemic allows us to comment on temporal trends of IPV in that period. Our rates of physical IPV perpetration (and also victimization; see Supplemental Material) were extremely low and stable throughout the measurement periods. Psychological IPV perpetration appeared to be slightly elevated during the earliest stages of the pandemic, but then fell back again (see Supplemental Material for details).
These results are partially consistent with existing cross-sectional IPV studies conducted during the pandemic, which often found a rise in IPV during the initial pandemic phase, coinciding with lockdowns (Piquero et al., 2021). However, in our research, this rise in IPV during the initial stages of the pandemic was found only for psychological IPV perpetration, not physical IPV. Similarly, another longitudinal study with a community sample also found a rise in verbal conflicts shortly after the pandemic’s onset, but no increase in physical aggression (Lee et al., 2021). The uptick in calls to crisis lines, police, and emergency room visits noted by Piquero et al. (2021) suggests that physical IPV rates may have spiked in the earliest stages of the pandemic. However, our results, along with Lee et al.’s, tentatively suggest that increase might have been driven primarily by increased rates in individuals already at risk of IPV. In low-risk community samples like ours, the early pandemic stresses seemed to manifest in the form of heightened psychological aggression, rather than physical. For either type of IPV, the fact that the strongest effects coincided with the periods of lockdown suggests that isolation and a lack of access to traditional services might have been particularly problematic. Increased accessibility options, for example, telehealth, pioneered during the pandemic, should be continued, to make certain that vulnerable persons can be reached through a variety of means.
Our study then goes beyond most, allowing for longer-term tracking of IPV rates, well beyond the initial pandemic stages. Although caution must be exercised due to the assessment of IPV on different time scales, it appears that psychological IPV perpetration (and victimization) rates remained somewhat elevated, even after one to two years. The acute stage of the pandemic may have passed, but its effects appear to linger, and risk becoming endemic. Clinicians and policymakers should be aware of these ongoing heightened risks, and effective interventions and treatments for IPV should be a priority, now more than ever.
Strengths and Limitations
Our assessment of the association between IU and IPV goes far beyond previous research. We were able to establish the connection across two studies with multiple time points extending for well over a year, utilizing responses from both LGBTQ+ and non-LGBTQ+ participants from two North American countries. Even though our effect sizes were relatively modest, as discussed above, this association still has very important implications for practitioners and policymakers. IU is potentially treatable and could therefore serve as a key target for intervention.
Of course, our study also had limitations. We focused on only one member of the dyad and did not get both partners’ perspectives. We tracked respondents over the first four pandemic waves but have not continued our tracking into the current period, in which COVID-19 has become endemic. It did not assess individuals beyond North America; patterns might look different in other countries. Furthermore, because it was beyond the scope of our study, we did not consider important issues of how country, regional (i.e., state and provincial/territorial), and local variations in COVID-19 responses and anti-LGBTQ+ political rhetoric and legislation, along with cross-border media consumption of political views and responses, could have influenced our participants’ sense of uncertainty, safety, and security.
Study 2 had good inclusion of LGBTQ+ respondents, increasing our sample diversity in that respect. However, there was not sufficient representation of all groups to conduct a more detailed and nuanced examination of our findings, for example, assessing whether minority sexual identities versus gender identities had differential effects. Also, we chose to focus on LGBTQ+ identity, rather than current relationship status, because the minority stress associated with such identities may contribute to heightened experiences of uncertainty, regardless of the nature of one’s current relationship. Still, a case could be made that the more appropriate focus, given that we were examining IPV, might have been on the nature of the current relationship (e.g., same-sex, mixed-sex, gender diverse). An ideal study would have sufficient representation in all groups to allow for comparisons incorporating both sexual identity and current relationship configuration.
Although we considered LGBTQ+ identity in our analyses, our samples were not highly diverse in other respects (e.g., generally well-educated, White, in stable, healthy relationships). We had a community sample, and our findings cannot be generalized to individuals at very high risk of IPV. For example, temporal trends in IPV across the pandemic might look very different if one tracked recipients of IPV support services. Perhaps related to the nature of our sample, we had some challenges with low Cronbach’s alphas at some time points. The CTS2 is a very widely used, well validated, reliable instrument. The issue for our samples seemed to be that there was adequate variability on the less severe items, but almost zero variability and complete floor effects for some of the more severe items. That pattern led to issues of truncated range and associated low inter-item correlations for those items. Reliability would have been improved had we focused only on the less severe items, but we chose to retain the standard full-scale scores, to facilitate comparison to other studies, and future reviews or meta-analyses. Potentially contributing to our sample’s low levels of physical IPV, particularly more severe forms of IPV, was our inclusionary criteria, requiring participants to be in a romantic relationship. Prior research suggests that intact relationships may experience lower rates and less severe forms of IPV (e.g., Johnson et al., 2014); as such, our sample may have included higher functioning couples who were less likely to experience more severe IPV.
Our study focused on IU as a relatively novel predictor of IPV, but a more complete assessment should also include assessments of other known predictors of IPV perpetration, such as substance use, PTSD symptoms, stress, and financial strain. Lastly, our current study did not consider actual levels of uncertainty within one’s relationship as a predictor of IPV perpetration, particularly among individuals who might have greater difficulty in tolerating that uncertainty. Though relatively limited empirical research exists currently, relationship uncertainty theories suggest that uncertainty in one’s relationship can trigger negative emotions (e.g., anger, jealousy) and lead to maladaptive communication strategies, including aggressive communication with one’s partner (see Theiss, 2017 for further discussion). Research is needed to better understand the extent to which uncertainty within relationships might lead to IPV perpetration, particularly among those higher in IU. If those who struggle to cope adaptively with uncertainty are trained in effective strategies to better tolerate that uncertainty, they may then be better equipped to cope with whatever stressors life might potentially throw their way—hopefully not up to and including another worldwide pandemic.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605241270064 – Supplemental material for The Perils of the Unknown: Intolerance of Uncertainty and Intimate Partner Violence Across the First Four Pandemic Waves
Supplemental material, sj-docx-1-jiv-10.1177_08862605241270064 for The Perils of the Unknown: Intolerance of Uncertainty and Intimate Partner Violence Across the First Four Pandemic Waves by Kathryn M. Bell, Diane Holmberg and Zoey A. Chapman in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We thank Dr. Karen L. Blair and all members of the research team for their contributions to Study 2, and Bre O’Handley and Kim Cadman for their assistance in data preparation. We also thank Erin Norris for her involvement in Study 1 design and data collection.
Authors’ Note
Portions of this article are based on the honors thesis of Chapman, and were presented at the 2023 meeting of the Canadian Association of Cognitive and Behavioral Therapies and the 2024 World Meeting of the International Society for Research on Aggression.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: We received funding from a Nova Scotia Health Research Coalition grant (PIs: Drs. Karen L. Blair and Kathryn M. Bell) and from the Acadia University Research Fund.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.