
Abstract
Despite several parallels between intimate partner violence (IPV) and sexual assault (SA), programs designed to reduce either of these forms of violence against women rarely evaluate the impact on both IPV and SA. Accordingly, we investigated whether one such program (the Enhanced Assess, Acknowledge, Act (EAAA) Sexual Assault Resistance program), designed to help university-aged women resist SA, could also reduce subsequent IPV. Women university students who were enrolled in the Sexual Assault Resistance Education (SARE) randomized controlled trial examining the impact of the EAAA program on SA, were recruited immediately after completing the last survey in the SARE trial. From this trial, 153 women completed the IPV substudy, which included an additional survey. Occurrence of IPV was assessed using the Composite Abuse Scale. Of the 93 new relationships reported by 66 women in the control group, the 1-year risk of IPV was 26.8%. In contrast, of the 113 new relationships reported by 87 women in the EAAA program group, the 1-year risk of IPV was 12.2%. Effectively, the EAAA program significantly reduced the 1-year risk of IPV by 54.4% (p = .037, 95% CI [2.9%, 79.8%]). Our findings suggest that the EAAA program is effective in reducing the risk of IPV and highlights the generalizability of programming that targets the foundational underpinning of multiple forms of gender-based violence.
Keywords
Introduction
Intimate partner violence (IPV) and sexual assault (SA) against women are internationally recognized public health concerns. IPV is a pattern of emotional, sexual, and/or physical violence committed against an intimate partner (Smith et al., 2018), whereas SA is any form of sexual abuse committed by anyone (Basile et al., 2022). These two forms of violence against women are distinct, but can and do overlap as intimate partner sexual violence (IPSV; Bagwell-Gray et al., 2015). However, research on IPV and SA has often occurred in silos, despite conceptual and practical reasons for bringing together these areas of research. This may be especially true for programing designed to reduce either IPV or SA, many of which have been implemented on postsecondary campuses and high schools because these forms of gender-based violence (GBV) are especially concerning to young adults (DeKeserdy & Kelly, 1993; Jeffrey et al., 2022; Oswalt et al., 2018; Smith et al., 2018). It is important that these problems are tackled comprehensively; however, it can be difficult to implement multiple GBV programs specifically for women on a campus or in a high school. As such, the current work considers whether a program designed to reduce SA against women can also reduce IPV.
Conceptual Similarities Between IPV and SA
IPV and SA are distinct forms of violence against women, but share similarities in risk, perpetrator characteristics, and survivor impact. For example, a first incident of IPV or SA is likely to occur before the age of 25 years; 72.3% of IPV survivors (Leemis et al., 2022) and 83% of SA survivors (Basile, 2022), according to recent research. Women are also most at risk from men that are known to them, especially acquaintances in cases of SA (e.g., Basile et al., 2022) and by definition, intimate partners in cases of IPV. Consistent with this, police report data indicate that men commit 83% of violent crimes against women and that intimate partners (45%) and friends/acquaintances (27%) are responsible for most of these crimes (Sinha, 2013). In cases of SA against women, the pattern is even clearer: men commit 99% of these crimes, and in 75% of cases, the woman knows her attacker, who is often an intimate partner (17%) or a friend or an acquaintance (45%; Sinha, 2013). Since the #MeToo movement, reports to police have increased, but this pattern in SA perpetration has continued (Rotenberg & Cotter, 2018).
Other similarities include the attitudes and tactics of men who commit IPV and/or SA. Research on SA (e.g., PettyJohn et al., 2019) and IPV (e.g., Laslett et al., 2021; Malhi et al., 2020; Schwartz et al., 2005) has shown that male perpetrators are likely to hold misogynistic attitudes and adhere strongly to masculine ideologies. A desire to control is also a principal element of IPV and SA (e.g., Dutton & Goodman, 2005; Fawson, 2015). As well, a substantial percentage of male college students admit to having perpetrated both sexual and physical assault (10.9%; White & Smith, 2009).
There are also similar social and psychological barriers to resisting and seeking help for IPV and SA that are rooted in cultural norms and gender role socialization. Since the early days of the violence against women movement, work on learned helplessness (Walker, 1984) and critiques of learned helplessness (Gondolf & Fisher, 1988) have highlighted how difficult it is for women to seek help for IPV. More recent work also shows that survivors of IPV continue to experience difficulty in seeking help because of social barriers (e.g., stigma, bias, institutional racism; Carney, 2024; Hulley et al., 2023). Similarly work on SA has long noted that women’s desire to be “nice,” avoid hurting others, and maintain relationships can delay their resistance to a SA (Rozee & Koss, 2001). Further, research continues to document the social barriers that SA survivors face in seeking support (e.g., fear of being blamed or not believed; McMahon & Seabrook, 2020). In both cases, then, to protect themselves and to seek help, women must go against social norms which are difficult, especially when the abuser takes advantage of their desire to maintain these norms. A final interconnection concerns others’ reactions to the survivor and the survivor’s response to these reactions. SA and IPV are illegal in Canada and the United States, but elements of both are implicitly condoned through victim-blaming. As such, survivors of SA and IPV often engage in self-blame, which is related to increased psychological distress, negative physical health, and difficulty naming the abuse as “abuse” (e.g., Bhuptani & Messman, 2023; Bondurant, 2001; Campbell et al., 2009).
These conceptual similarities suggest that programming for, and research on, IPV and SA against women could benefit from cross pollination. Bringing together efforts in both sectors can reinforce findings that demonstrate why and how women are vulnerable to GBV, such as known risk factors for both. Additionally, programming developed in one area might be leveraged to address other forms of GBV against women.
Historic Separation of Programming on IPV and SA
Despite the similarities between IPV and SA, until recently, research and prevention efforts have occurred in silos where work was explicitly focused on one or the other. For example, programs for adolescents focused on “dating violence” (i.e., IPV) prevention, whereas those created for college students were usually aimed at SA prevention. Although this does not apply to all programs, it is notable that early reviews of IPV prevention programs for youth (e.g., Cornelius & Resseguie, 2007; De Grace & Clarke, 2012; Ting, 2009) did not include college students, and those available for SA programs were limited only to college students (e.g., Anderson & Whiston, 2005; Vladutiu et al., 2011). However, a close look at IPV and SA intervention program content indicates substantial overlap. After examining 52 dating violence and SA prevention programs, Weisz and Black (2009) concluded that most of the content (e.g., warning signs, risk, healthy relationships, victim-blaming, gender roles, victim empathy) was relevant for both dating violence and SA prevention. Others have noticed this overlap and are breaking down silos to address GBV more broadly. More recent reviews of promising programs have included work on both IPV and SA (Barata & Senn, 2019; Crooks et al., 2019; Ellsberg et al., 2015), although the specific programs included still largely focused on only one or the other, an exception being Park and Kim (2022) whose review was limited to only one kind of intervention program (i.e., bystander intervention).
Designing programs to focus specifically on IPV or SV is reasonable given that more focused programs may be more successful and trying to do too much may dilute programming effectiveness. Still, given the overlap between IPV and SV, understanding the possible extension of program effects to other forms of GBV is prudent.
Evaluating the Impact of Intervention Programs
Of the many programs designed to ameliorate IPV or SA in young people, most have not evaluated subsequent violence. Research often focuses on knowledge or attitudinal changes (e.g., rape myth acceptance, gender norms) or bystander behavior (e.g., helping behavior; Park & Kim, 2023), instead of IPV or SA perpetration or victimization (Ellsberg et al., 2015). Measuring the impact on IPV
Coker et al. (2016, 2017) used separate measures for IPV and SA to examine the impact of a bystander program on university campuses and in high schools. They showed that the Green Dot program may be more effective at reducing some forms of GBV (i.e., sexual harassment, stalking, incapacitated sex, and psychological IPV) compared to others (i.e., physically forced sex, coerced sex, and physical IPV), despite program content that addressed both IPV and SA. Rowe et al. (2015) reported reduced sexual victimization of high school girls three months following an assertive resistance training program. The rates of physical and psychological victimization remained unchanged, though this may have been due to the small pilot sample, short follow-up period, or lack of IPV specificity (i.e., physical violence was measured using a subscale of the Conflict in Adolescent Dating Relationships Inventory and could have been perpetrated by any “boy”). Measuring both IPV and SA may be particularly important when a program targets the gendered norms that facilitate both and can inform our understanding of the program’s underlying mechanisms and contribute to knowledge translation efforts to increase program uptake.
EAAA SA Resistance Education
The Enhanced Assess, Acknowledge, Act (EAAA) SA Resistance program, also known as Flip the Script, targets the gendered norms that contribute to violence against women by arming young women with the knowledge and skills they need to defend themselves against SA (Senn et al., 2013, 2015). The EAAA program is also the only program that has demonstrated a significant reduction in the 1-year incidence of completed rape as well as other forms of SA and coercion among women in university (Senn et al., 2015), and demonstrated sustained effects for 2-years (Senn et al., 2017). We hypothesize that the EAAA program may also be effective at reducing IPV, including nonsexual IPV, in part, because it recognizes that women are most at risk from men they know, including intimate partners, and all units include exercises that help women practice their new skills in this context (e.g., one exercise has women visualize how they would physically defend themselves against a specific man that they know if he were to attempt SA). Thus, it may help women acknowledge earlier in a relationship or before the relationship becomes serious, that the man has the potential to be abusive which may give women reasons to avoid the relationship altogether.
Other topics covered by the program include risk factors, stereotypes, gender norms, and alcohol use, providing women with knowledge that may also protect women against IPV. For example, perpetrator tactics, which are known risk factors for SA and IPV, are covered in part to help women recognize men’s controlling behavior before abuse occurs. Also, alcohol is discussed as a risk factor, while emphasizing that it does not excuse abuse. If this generalizes to IPV, women would be more likely to name their partner’s behavior as abuse even when he is drinking. Stereotypes, gender norms, and victim-blaming that implicitly condone SA and IPV are addressed, and program facilitators are trained to challenge participants’ victim-blaming, because self-blame can hinder women’s ability to label their experiences as SA and seek support. Likewise, the program emphasizes that the blame for SA always lies with the perpetrator. If these messages generalize to IPV, the program may also provide resistance to IPV.
The mechanisms through which the EAAA program reduces SA have been examined, and included rape myth acceptance, which reduces SA through risk detection (Senn et al., 2021). Rape myths are attitudes about SA that work to blame survivors and exonerate perpetrators (Grubb & Turner, 2012). In this way, they are quite similar to IPV-related myths (Peters, 2008). For example, the Illinois Rape Myth Acceptance Scale (Payne et al., 1999), includes items that exonerate perpetrators of SA (e.g., “men don’t usually intend to force sex on a woman, but sometimes they get too sexually carried away,” p. 50), which is similar to items on the Domestic Violence Myth Acceptance Scale (DVMAS) (Peters, 2008) that exonerate abusive men (e.g., “abusive men lose control so much that they don’t know what they’re doing,” p. 21). Likewise, both scales include items that blame the survivor of abuse. It is possible that in programs such as the EAAA program that target gender norms and stereotypes about survivors, a generalization of rape myth reduction to IPV myth reduction might also occur.
The Present Study
To our knowledge, no SA resistance education program for university women has examined the long-term impact on IPV, although the EAAA program has been shown to reduce the long-term impact of SA (Senn., et al., 2017). This constitutes a significant gap as sleeper effects may be evident in the absence of immediate effects because intimate relationships take time to develop. The EAAA program is delivered to first-year university women who are less likely to be in long-term/committed relationships than more senior students. At baseline, 45% reported a current intimate relationship, but this increased to 75% at the 2-year follow-up (Senn et al., 2015, 2017); thus, older university women are at greater risk for IPV. The primary aim of this study was to determine whether participation in the EAAA program decreased the incidence of IPV in new relationships compared to women in the control group. The secondary aim was to assess any difference between groups in their domestic violence myth acceptance.
Methods
Participants
This study capitalized on an existing randomized controlled trial (RCT) examining the impact of the EAAA program on completed SA (see Senn et al., 2015, 2017). The original RCT eligibility criteria were an identification of a woman, in first-year university, and between the ages of 17 to 24 years. Participants were recruited at three Canadian universities through a mix of recruitment strategies that included registration in psychology participant pools, posters/flyers around campus, email messages from professors and presentations in classes, and at student events. More detailed methodological details are available in previously published work (Senn et al., 2015, 2017). Participants in the RCT were followed for up to 2 years. To avoid interfering with the conduct of the trial, participants were invited to participate in the IPV substudy only after completing the 2-year follow-up for the RCT. Those who consented to participate in the IPV substudy completed a detailed relationship and IPV information survey. Participants received $20 for completing the survey. The program RCT and the IPV substudy were approved by the Research Ethics Boards at three Canadian universities.
Of the 358 participants (181 control, 177 program) who completed the 2-year follow-up survey for the RCT, 320 (162 control, 158 program; 89%) agreed to participate in the present IPV substudy. Of these, 87 women did not have an intimate relationship since beginning university, another 71 women did not have a new relationship lasting 1 month or more, and nine participants did not complete the IPV survey. The remaining 153 (66 control, 87 program) participants were included in the analyses.
Measures
Participant and Relationship Information
Participants provided demographic, as well as current and previous relationship information. Specifically, they were asked if they had been in an intimate relationship that lasted 1 month or longer since beginning university. If they had, they provided the gender of each partner, and the start and end dates (i.e., month and year) of each relationship.
Composite Abuse Scale
The CAS (Hegarty et al., 1999, 2005) is a validated measure of IPV against women that contains four subscales: severe combined abuse (8 items; e.g., “took my wallet and left me stranded”), physical abuse (7 items; e.g., “beat me up”), emotional abuse (11 items; e.g., “told me I was crazy,” and harassment (4 items; e.g., “harassed me at work.” Women indicated how often each of 30 acts of abuse occurred from never (0) to daily (5) in an intimate relationship. Three items in the severe combined subscale assess SA. As we aimed to study the effects of the program on IPV beyond IPSV, we excluded these three SA items from the total score, with no effect on the scale’s internal consistency; Cronbach’s alpha for the full scale was .89 and .88 when the three SA items were omitted. The three SA items were excluded for the main analysis to avoid confounding the results with a decrease in IPSV only, given that that EAAA program has already been shown to reduce SA (Senn et al., 2015). However, this did not exclude women who experienced IPSV if they met the IPV cut-off without those items.
We used the following recommended cutoff scores (obtained from a draft of the CAS Manual provided in personal correspondence with Hegarty) to determine IPV: CAS total (excluding and including three SA items) score ≥3; severe IPV (excluding and including three SA items) score
Domestic Violence Myth Acceptance Scale
The DVMAS (Peters, 2008) is a valid 18-item measure of the extent to which individuals accept domestic violence myths, which are generally false but widely and persistently held. Participants indicated the strength of their agreement on items such as “when a man is violent, it is because he lost control of his temper” and “making a man jealous is asking for it” on a scale from strongly disagree (1) to strongly agree (7). The internal consistency, Cronbach’s alpha, for the scale was .89.
Data Analyses
The primary analysis compared the incidence of IPV (excluding three SA items) between the EAAA program and control groups using a Kaplan–Meier failure curve and the log-rank test. As the analysis included all new relationships that participants had after their entry into the RCT, variance estimates were appropriately inflated to account for within-participant clustering. Given that participants only reported the month and year for the start and end dates of their relationship, a computer-generated random day within a given month served as a proxy for the exact date. For ongoing relationships, the date of the 2-year follow-up survey served as the end date. The benefit of the program was described in terms of absolute and relative risk reductions. For the secondary analysis, mean DVMAS scores were compared between the EAAA program and control groups using a t-test. All statistical analyses were carried out using SAS 9.4 (SAS Institute Inc., Cary, NC, USA), and p-values below .05 were considered statistically significant.
Results
Overall, the mean age of participants at trial entry was 18.4 years (SD = 1.1), more than three-quarters were White or of European descent, more than 90% identified as heterosexual, approximately one-half lived in a university or college residence, and all had a previous intimate relationship (Table 1). The number of new relationships reported by the participants was similar between the two groups (93 control, 113 program). As the new relationships occurred, on average, approximately 11 months after the participants’ entry into the trial, the overall mean age at the time of the new relationship was 19.3 years (SD = 1.3). Over 90% of the relationships were with a man and the relationship lasted, on average, between 7 and 8 months.
Participant and Relationship Information.
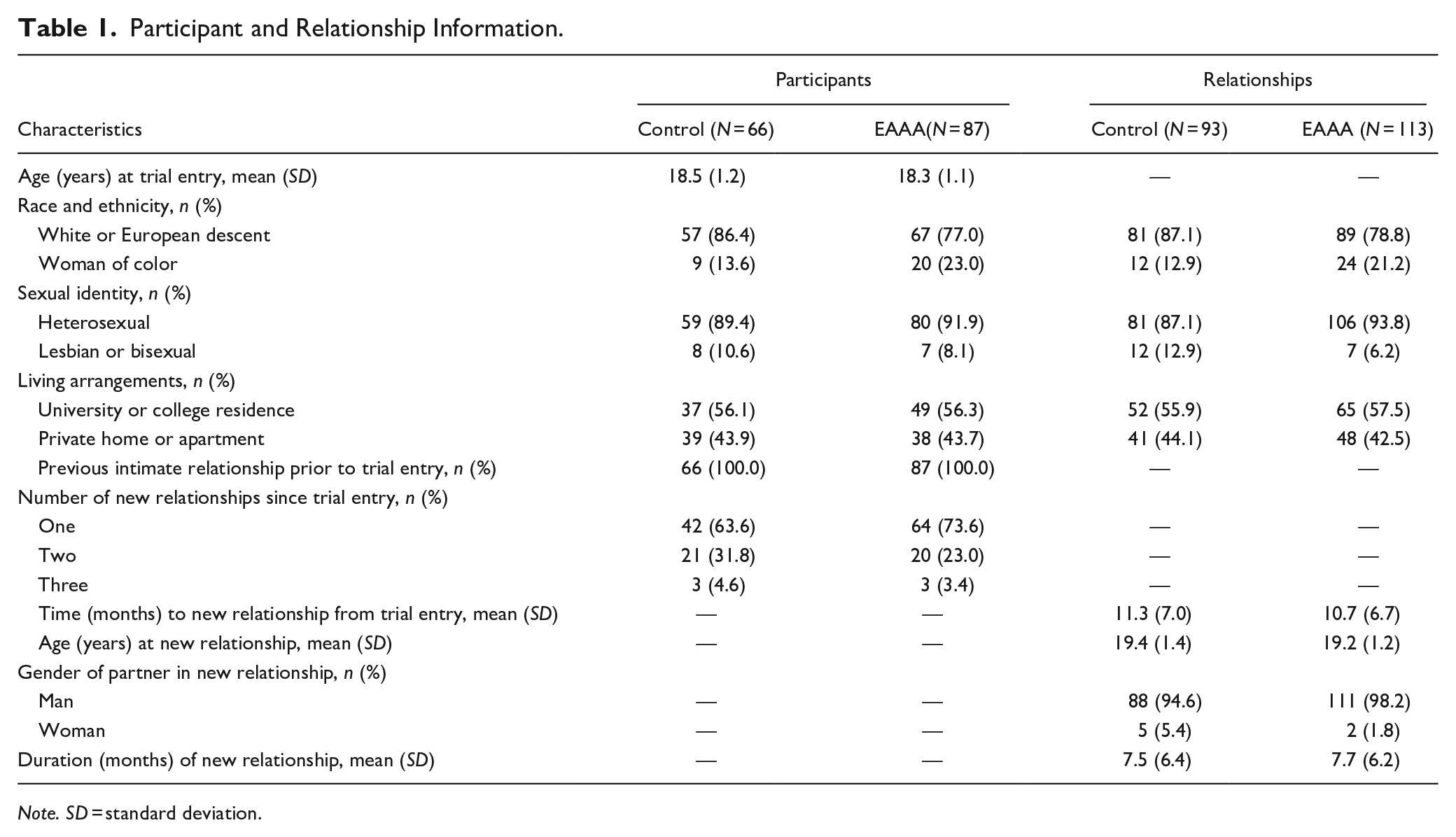
Note. SD = standard deviation.
Among the 66 women in the control group, there were 15 occurrences of IPV in 93 relationships. In comparison, among the 87 women in the EAAA program group, there were 8 occurrences of IPVs in 113 relationships. The 1-year Kaplan–Meier risks of IPV (excluding three SA items) for women in the control and EAAA program groups were 26.8% and 12.2%, respectively (Table 2 and Figure 1, log-rank p = .037), which resulted in a significant 54.4% relative reduction in IPV risk (95% CI [2.9%, 79.8%]). Including the 3 SA items strengthened the results (see Table 2). Similar risk reductions were observed for both physical and emotional abuse (54.4% and 52.2%, respectively), and a lower risk reduction for harassment (37.4%). The occurrence of severe abuse (excluding the three SA items), was rare. Despite the observed reductions in IPV, the EAAA program had no effect on domestic violence myth acceptance. The mean DVMAS scores were not significantly different between the EAAA program and control groups (program: M = 1.99, SD = 0.75; control: M = 1.93, SD = 0.71), (p = .57, 95% CI [−0.30, 0.17]).
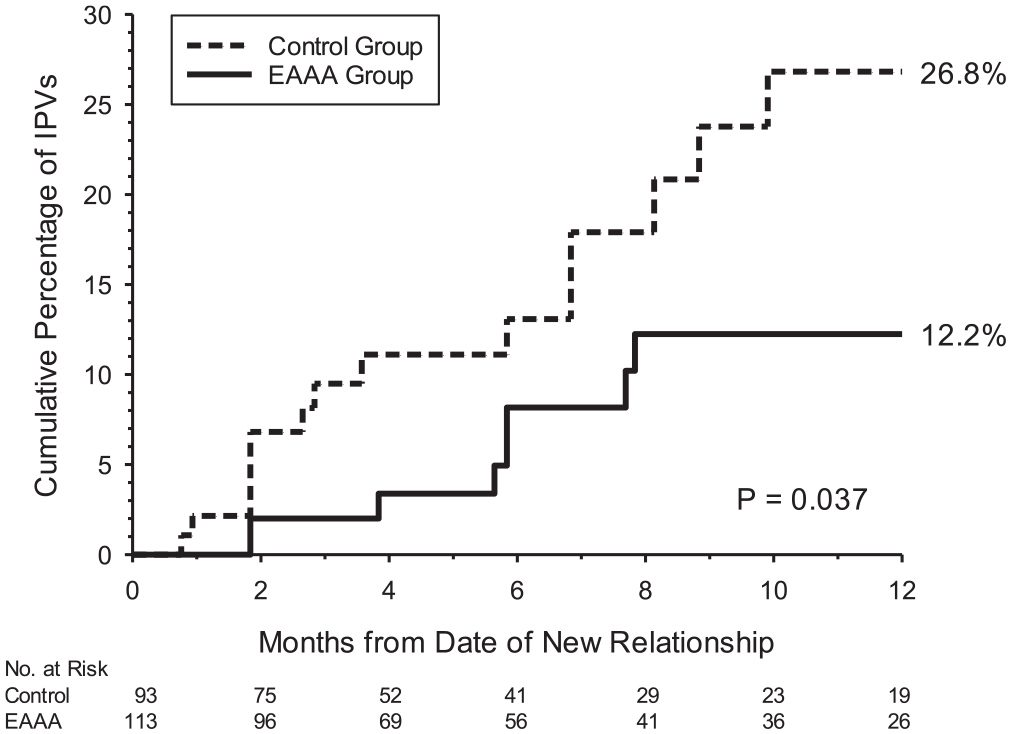
Kaplan–Meier failure curves for intimate partner violence.
One-Year Risks of Type of IPV, Absolute and Relative Risk Reductions.
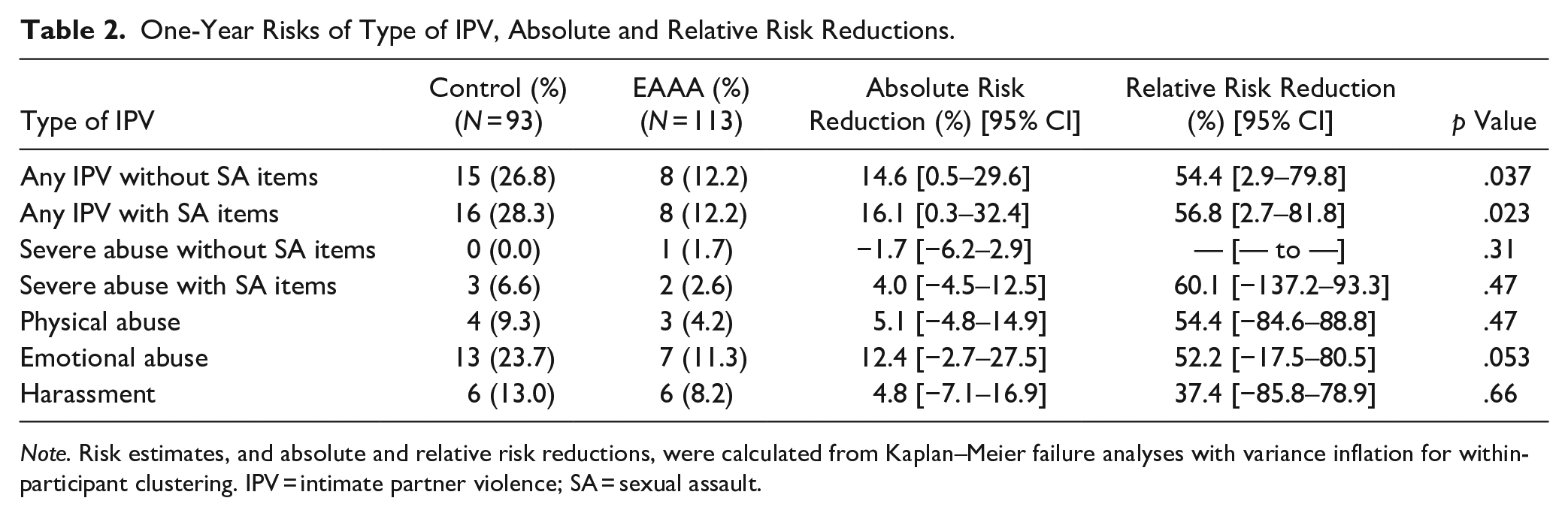
Note. Risk estimates, and absolute and relative risk reductions, were calculated from Kaplan–Meier failure analyses with variance inflation for within-participant clustering. IPV = intimate partner violence; SA = sexual assault.
Discussion
Our aim was to determine whether a successful SA resistance program could also reduce IPV among young women. We provide evidence that women randomly assigned to the EAAA program were less likely to experience IPV in a new relationship compared to control women. Importantly, our measure of IPV excluded the three SA items that are in the CAS, and as such indicates a reduction beyond IPSV.
The generalizability of the knowledge acquired in the EAAA program may account for our study’s findings. The first three units of the EAAA program focus on contexts with men and women know, and as such also provide information and teach skills that are relevant to IPV. The first unit, Assess, assists women to identify risk for SA more quickly in social situations, and the following cues in men’s behavior are explored at length: verbal and physical persistence, feelings of sexual entitlement, need for power and control, expressions of hostility and anger, and acceptance of interpersonal violence (Norris et al., 1999; Rozee et al., 1991; Senn et al., 2015; Warshaw, 1988). Importantly, these cues are also relevant in contexts that are not necessarily sexual (e.g., persistence in what he wants despite knowing it is not what she wants) and women are told these “warning signs” are also relevant to IPV. The second unit, Acknowledge, focuses on the social norms and emotional experiences that hinder women’s ability to identify risk (e.g., the need to be nice, the fear of losing a relationship). Additionally, this unit explores how coercive men deliberately use these norms to their advantage such as insisting that sex is an obligation in an intimate relationship, which is of direct relevance to IPV. The third unit, Act, not only focuses on effective verbal and physical self-defense but also addresses the social and emotional barriers to using these strategies. As such, women develop a toolbox of effective verbal and physical self-defense strategies (Tark & Kleck, 2014; Ullman, 2002) they would be willing to use with a man they know, which could be an intimate partner. Together, these could help women more quickly identify early abusive behavior from an intimate partner and have a toolbox of strategies (including leaving) to interrupt them before they escalate.
The final unit in the EAAA program includes content that is directly relevant to IPV. It deals with sexuality and healthy relationships and is based on the Our Whole Lives curriculum (https://www.uua.org/re/owl). This unit was included to help women integrate knowledge from the previous three units into their sexual lives and intimate relationships. The unit makes clear that engaging in desired, consensual sexual activity is not at odds with strong resistance against SA and provides guidance on how to communicate about desired sexual activities. If a woman cannot imagine communication of this kind with a current partner, it may signal to her that something is wrong in the relationship. The unit also includes a specific activity (“what makes a good relationship”) that is directly relevant to IPV. Discussion is largely driven by participants’ contributions but always includes the importance of trust (rather than jealousy), respect, and other noncontrolling characteristics. Additionally, women engage in several activities like negotiating safer sex and communicating their sexual desires where it is likely that they picture their intimate partner if they have one. Taken together, the activities of this unit may help women identify intimate relationships where their sexual boundaries are not respected, knowledge that may generalize to relationships that ignore their nonsexual needs, desires, and boundaries. This may lead to earlier termination of relationships before there is explicit abuse, and/or avoidance of relationships with controlling men. Our study did not examine whether the EAAA program could increase the likelihood that an abusive relationship would be terminated altogether or terminated earlier because only new relationships were included, but this is also a possibility and should be examined in future studies. Additionally, it is also possible that the EAAA program could encourage women to seek help earlier, and possibly reduce repeat violence.
Research has shown that the EAAA program reduces rape myth acceptance (Senn et al., 2017), whereas our findings suggest it has little impact on IPV myths. This is perhaps not surprising given that the EAAA program does not directly address IPV myths in the way it does address rape myths. Nevertheless, there is overlap between rape myths and IPV myths, given their shared patriarchal roots, and continuing to explore what if any learning might generalize is worthy of exploration, perhaps with more tailored measures. It is also possible that the mechanisms through which the EAAA program generalized to IPV are broader than specific myths. Future research should examine possible mechanisms which may include the challenging of social norms about gendered behavior and early recognition of risk cues in men’s controlling behavior.
Strengths and Limitations
A strength of the current study was that it capitalized on an existing RCT that allowed us to demonstrate the effects of the EAAA program on mitigating IPV in new relationships without recruiting a new cohort of participants. However, as we prioritized data collection for the original trial and only invited participants for our substudy after they completed their 2-year follow-up surveys for the original trial, this resulted in both a smaller sample size and some participants not completing the CAS; nevertheless, the response rate of 89% from the main trial into the substudy was good. Participants completed the CAS only once to mitigate survey fatigue, regardless of the number of relationships they had reported. This decision was successful in that only nine women did not complete the CAS. However, this means we were unable to determine whether participants met the cut-off score for IPV in each relationship. However, with 69.3% of the women reporting one new relationship and 26.8% reporting two, of which only one relationship per participant was abusive, we are confident we correctly identified (non)abuse for most relationships. Nonetheless, it is possible that the number of IPV occurrences reported in this study may be an underestimate because IPV was defined as a score of three or more on the CAS scale, and therefore, it is possible that women who had experienced one or two incidents of abuse left the relationship before further abuse was experienced. Future research could explore whether the EAAA program (or other GBV programs) accelerate terminating an IPV relationship. Finally, our sample was not sufficiently diverse with respect to ethnicity or sexual identity to examine program effects by relevant subcategories. However, results from the original trial suggest that the EAAA program’s effects on SA maintain across racial and sexual identities (Senn et al., 2019), so there is reason to expect that this would also apply to IPV. Because gender identity was not collected in the RCT, program effects by gender identity could not be examined. Understanding if and how the program can be adapted for trans and nonbinary students is underway (Peitzmeier et al., 2024).
Implications
The IPV incidence results reported in this study is not directly comparable to past work as our sample was not randomly selected, but rather a substudy of an RCT with a SA program component. Nevertheless, the high incidence of IPV observed in this study suggests that many university women at risk for IPV are amenable to participating in a SA resistance education program, and that the benefits of that program include a reduced likelihood of experiencing IPV. This is good news for university administrators who can offer one program that targets at least two forms of GBV.
The development of a booster for the EAAA program has been suggested (Senn, et al., 2017). At the 2-year mark, the risk for SA remained reduced in the RCT, but the effects had attenuated, particularly for completed rape (Senn, et al., 2017). The authors speculated that women might have been increasingly at risk for IPSV and a booster could address that issue directly. The risk for SA may be highest in first-year university women (Krebs et al., 2016; Smith et al., 2003), but the risk for IPSV increases as women progress through university (Smith et al., 2003) suggesting a booster should have an increased focus on IPSV and IPV.
The results of this study also demonstrate the value of measuring related but unintended outcomes for any program that seeks to reduce GBV. As noted earlier, there are similarities between SA and IPV, and there are likely to be similarities with other forms of GBV, but measuring the program impacts on multiple forms of violence is still rare. Understanding these unintended, but positive, consequences would help demonstrate the foundational roots of many forms of GBV and should be encouraged for programs that seek to shift gender and societal norms that contribute to rape culture (Radtke et al., 2020). It would be important to know, for example, whether programs focused on youth dating violence also impact attitudes and behaviors related to SA, especially SA that is not IPSV. Likewise, the EAAA program has been adapted for high school girls, and a trial is currently in progress. It will be important to determine the impact of the program on both SA and IPV at this critical developmental period when many adolescents begin dating.
It is important to be clear that resistance programs such as the EAAA program are only one facet of a comprehensive solution to ending GBV. We need to continue to develop and evaluate programs designed to target potential perpetrators of abusive behaviors as well as bystander programs that target the community. Nevertheless, there is increasing evidence that resistance programs provide women with the skills they continue to need to protect themselves against abuse. A next step is to develop resistance programs for populations other than women who are also at increased risk of GBV, such as people from gay, trans, and queer communities as well as children of all genders. Such work is already underway (e.g., Peitzmeier et al., 2024; University of Windsor, 2023).
Conclusion
The EAAA program reduced rape and other forms of SA in a RCT (Senn, et al., 2015), and more recently in real-world conditions (Senn et al., 2023). The program is now being delivered in four countries (https://www.sarecentre.org/), and language and population adaptations are in various stages of evaluation (i.e., French adaptation, high school girls, and trans/nonbinary students). The results of this study demonstrate an additional benefit of the EAAA program in reducing the incidence of IPV. SA and IPV have continued unabated for university women for too long, but we may now be at a turning point. There is potential to reduce GBV, but to realize this goal we must avail ourselves of the progress made on evidence-based programming.
Footnotes
Acknowledgements
We thank our research assistants, program facilitators, and the rest of the Sexual Assault Resistance Education Trial team for their help with this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Senn, C.Y, Barata, P., Eliasziw, M., Newby-Clark, I. Thurston, W. (2010) CIHR Operating Grant, Randomized Controlled Trials ($1,313,891, over 5 years) Sexual assault resistance education for university women: A trial in three Canadian universities