
Abstract
Despite an extensive body of literature that explores potential mechanisms explaining the factors associated with intimate partner violence (IPV) experienced by women, very few studies have studied the association of food security status with women’s experience of IPV in sub-Saharan Africa countries, including Cameroon. Using data from the 2018 Cameroon Demographic and Health Survey (n = 4,690), we explore the association between food security status and three distinct forms of IPV (i.e., emotional, sexual, and physical IPV) among ever-married women in Cameroon. Adjusting for socioeconomic, demographic, and attitudinal and behavioral characteristics, we found that women with severe (odds ratio [OR] = 2.09, p < .01), moderate (OR = 1.88, p < .05), and mild (OR = 1.76, p < .05) food insecurity were more likely to experience sexual IPV, compared to those without any food insecurity, whereas women with severe food insecurity were more likely to experience physical IPV (OR = 1.89, p < .001). Although women with severe (OR = 1.51, p < .01) and moderate (OR = 1.67, p < .001) food insecurity had a higher likelihood of experiencing emotional IPV at a bivariate level, we found that these associations became no longer significant in our adjusted model. These findings suggest that food insecurity is a critical risk factor for IPV among ever-married women in Cameroon. Addressing IPV requires a comprehensive strategy that places special emphasis on households experiencing food insecurity. There is also an urgent need to implement educational programs to increase awareness of the interconnection between food insecurity and IPV and to allocate resources to community-based initiatives that empower women both economically and socially.
Keywords
Introduction
Declared as the “Decade of Action” (2020–2030), the pursuit of the Sustainable Development Goals (SDGs) stands as a cornerstone for fostering not only holistic well-being but also in building equitable, fair, and inclusive societies. Many governments are actively engaged in implementing strategies to improve gender equity, especially given that achieving this target is directly tied to meeting other goals (Guaita-Fernández et al., 2024). Notably, gender equity increases women’s health and well-being, productivity at the household and national level, and unlocks multi-generation benefits for children (Kaltenborn et al., 2020). Yet, gender-based violence, recognized as a grave violation of human rights and a pressing public health, remains pervasive, and hampering progress toward broader development goals.
Intimate partner violence (IPV), defined as any act causing physical, sexual, or psychological harm, stands out as one of the most prevalent forms of such violence (World Health Organization [WHO], 2021). While IPV remains a pervasive global issue, the WHO (2021) has identified regional disparities, highlighting that sub-Saharan Africa (SSA) has experienced a higher lifetime prevalence of IPV at 33%, in contrast to the global average of 26%. Research underscores that Cameroon, like many other SSA countries, struggles with endemic IPV, with 31% of women having experienced violence during their lifetime (Mulat et al., 2022). Cameroon’s situation is particularly troubling, as indicated by its placement on the United Nations Development Programme’s 2019 Gender Inequality Index, where it ranks 141 out of 162 countries in terms of gender equality (OCHA, 2019). Although Cameroon promulgated a national strategy to eliminate violence against women, the policy has been criticized for lacking tangible measurable targets (Djapou Fouthe, 2017). Additionally, the ongoing insecurity concerns in certain regions of Cameroon have exacerbated the situation, leading to increased instances of gender-based violence as well as displacement and disruption of support services for survivors (Human Rights Watch, 2023; Lekunze & Page, 2023).
This situation in Cameroon and other countries in SSA requires policy attention due to the severe health consequences associated with IPV. For example, women who have experienced IPV face elevated risks of mental and emotional health issues, including substance use disorder, attempted suicide, and major depressive disorder (Kinyanda et al., 2016). Moreover, IPV has been linked to adverse physical health outcomes, such as injuries, limitations in daily activities, and chronic conditions like diabetes and hypertension (Epstein et al., 2020). Maternal health is also impacted by IPV. Research has revealed that women with a history of IPV are less likely to access essential antenatal care services compared to those without such experiences (Ragetlie et al., 2020). Similarly, exposure to IPV is associated with adverse perinatal outcomes, such as miscarriage, low birth weight, and pre-term birth (Pastor-Moreno et al., 2020).
Reflecting on these dire health repercussions, extensive research has been conducted to identify factors associated with IPV in SSA countries, including Cameroon. For example, women’s socioeconomic characteristics, such as education, household wealth, and employment status, have emerged as key structural determinants of their vulnerability to IPV (Amegbor & Pascoe, 2021). Within the context of many patriarchal SSA societies, economic opportunities, such as employment, often play a critical role in redressing the power balance between wives and husbands within household settings, with the ability to assert their agency and independence (Sano et al., 2018). The availability of these socioeconomic resources can be instrumental in empowering women to challenge traditional gender norms and beliefs, possibly leading to a tangible reduction in their exposure to IPV (Tandrayen-Ragoobur, 2020). Studies have also highlighted the importance of demographic and attitudinal characteristics in understanding IPV. Specifically, younger women and those residing in rural areas have been found to be at a higher risk of experiencing IPV compared to their older and urban counterparts (Nabaggala et al., 2021). Furthermore, women’s attitudes toward domestic violence and justification of spousal abuse have been positively linked to their own experiences of IPV (Aboagye et al., 2021). In Uganda, it was further revealed that married women face a higher risk of experiencing IPV when their partners engage in controlling behaviors, such as limiting their autonomy and participation in household decision-making (Gubi et al., 2020). The literature has also underscored that substance use, such as alcohol consumption by their partners, serves as a strong predictor of women’s exposure to IPV (Yaya & Ghose, 2019).
Beyond these characteristics, however, several studies have explored the association between women’s experience of IPV and food insecurity—defined as the “restriction or uncertain availability of nutritionally adequate and safe foods or limited or uncertain ability to acquire food in socially acceptable ways” (Stuff et al., 2004). For instance, in line with other resource dynamics, men are often expected to undertake the role of primary breadwinners in their households, assuming the gendered responsibility of providing household necessities, including nutritious food, for their family members (Awungafac et al., 2021). Consequently, a failure to provide sustenance for the family can potentially disrupt established patriarchal norms, fostering an environment in which some men resort to IPV as a means to reaffirm their male dominance within the household (Hatcher et al., 2019). Furthermore, existing research has demonstrated that women with a history of food insecurity are more susceptible to distress and mental health challenges compared to those without such experiences. This could be particularly critical, as evidence has indicated the mediating role of mental health in the association between food insecurity and IPV (De Moraes et al., 2016). In this context, it is plausible that stress triggered by food insecurity plays a crucial role in the conflicts experienced between spouses within household settings (Diamond-Smith et al., 2019). Other studies have also posited that poverty, a marker of food insecurity, is positively linked to women’s experiences of IPV, particularly when financial and material resources within the household are not equitably distributed to women, reflecting unequal power dynamics between wives and husbands (Ricks et al., 2016).
Despite these observed mechanisms, very few studies have explored the association of food security status with women’s experience of IPV in SSA countries, and Cameroon in particular (McKay & Bennett, 2023). According to the Food and Agriculture Organization of the United Nations (FAO, 2023), nearly 60% of households in SSA struggle with moderate and severe food insecurity. At the national level, Cameroon mirrors this trend, as 59% of households experienced moderate and severe food insecurity between 2020 and 2022 (FAO, 2023). In light of this combined challenge involving food insecurity and IPV in Cameroon, using a nationally representative survey, the present study aims to advance the literature by examining the association between food insecurity and three distinct forms of IPV: emotional, sexual, and physical IPV. We will discuss our findings in the context of advancing the SDGs, with a particular emphasis on looking at the intersection between two targets—Target 2.1 (i.e., universal access to safe and nutritious food) and Target 5.2 (i.e., ending all violence against and exploitation of women and girls). Within this policy framework, we offer comprehensive implications that address the complex nature of the combined burden of food insecurity and IPV.
Methods
We used the 2018 Cameroon Demographic and Health Survey (CDHS) to explore the association between food security status and three types of IPV: that is, emotional, sexual, and physical IPV. The 2018 CDHS, conducted in collaboration with the Ministry of Public Health by the National Institute of Statistics, is a nationally representative survey. It employed a multi-staged sampling framework that involved systematic sampling with probability to size, enabling the identification of enumeration areas from which households were selected. The CDHS conducted in-person interviews with selected households as part of its data collection process. Trained interviewers visited households in the selected clusters and administered questionnaires to collect information on various health and demographic indicators. These interviews were conducted face-to-face, and in the preferred language of the respondent to ensure accurate data collection and to address any questions or concerns respondents may have in real-time. The survey interviewed a total of 13,527 women aged 15 to 49, achieving a response rate of 98%. This in-person, face-to-face approach may explain the high response rate. Although men were also interviewed in the 2018 CDHS, this study concentrates exclusively on women. The 2018 CDHS includes the domestic violence module that asks questions regarding the experience of emotional, sexual, and physical IPV among 4,690 ever-married women aged 15 to 49.
Measures
There are three dependent variables, namely women’s encounters with emotional, sexual, and physical IPV within the past 12 months. Regarding emotional IPV, participants were asked about whether their partner engaged in actions such as (1) humiliating them in front of others, (2) threatening them or loved ones, and (3) insulting or demeaning them. In terms of sexual IPV, three inquiries were employed to ascertain whether their partner: (1) physically compelled them into sexual intercourse, (2) physically coerced them into other sexual acts, and (3) threatened or used coercion to induce engagement in sexual acts. Concerning physical IPV, seven questions were utilized to determine if women experienced: (1) pushing, shaking, or having objects thrown at them; (2) slapping, (3) arm twisting or hair pulling, (4) punching or hitting with potentially harmful objects, (5) kicking, dragging, or beating; (6) choking or burning; and (7) threats or attacks involving a weapon. To align with prior research, dichotomous variables were established for each question related to physical, sexual, and emotional IPV. Consistent with prior studies (Mulat et al., 2022; Ragetlie et al., 2020) we created a binary variable for physical, sexual, and emotional forms of IPV. Participants were classified as having “experienced IPV” if they provided a positive response to any of the questions (0 = did experience IPV; 1 = did not experience IPV).
The Food Insecurity Experience Scale (FIES), first developed by the Food and Agriculture Organization as part of its Voices of the Hungry Project, was used to construct our key independent variable—food security status. This validated psychometric tool comprises eight binary questions that assess respondents’ experiences related to food access over the past 12 months. These questions were formulated to assess specific aspects, asking respondents whether they were concerned about (1) not having enough food to eat, (2) not being able to eat a variety of healthy and nutritious foods, (3) only eating a small number of different types of foods, (4) having to skip meals, (5) eating less than they thought they should, (6) their household running out of food, (7) being hungry but not eating, and (8) going without food for an entire day. The FIES has demonstrated its validity in capturing a diverse array of common challenges concerning food acquisition across various geographical regions, including SSA (Amoak et al., 2023; Cafiero et al., 2018; Wambogo et al., 2018). As the FIES score ranges from 0 to 8, calculated by summing the responses to the eight questions, we have aligned our classification with the recommendation provided by the Food and Agriculture Organization (Cafiero et al., 2018). Thus, we have established four distinct categories to categorize levels of food security, namely: food security (i.e., 0), mild food insecurity (i.e., 1–3), moderate food insecurity (i.e., 4–6), and severe food insecurity (i.e., 7 and 8).
The association between women’s experience of IPV and food security status may further be impacted by other factors. To account for possible confounding factors, informed by prior studies (Ahinkorah et al., 2018; Dhillon et al., 2023; Mulat et al., 2022; Stöckl et al., 2021), we have incorporated three sets of control variables—socioeconomic, demographic, and attitudinal and behavioral variables—in order to account for any confounding effects. Three socioeconomic factors were introduced: the quintile of household wealth (0 = richest; 1 = richer; 2 = middle; 3 = poorer; 4 = poorest); the job status (0 = employed [both formal and informal sectors]; 1 = unemployed); and the education (0 = secondary/higher education; 1 = primary education; 2 = no education). The respondents’ age (0 = 45–49; 1 = 40–44; 2 = 35–39; 3 = 30–34; 4 = 25–29; 5 = 20–24; 6 = 15–19) and place of residence (0 = urban; 1 = rural) were among the demographic factors. The analysis also added three attitudinal and behavioral variables: spousal abuse justification (0 = no; 1 = yes), partner-controlling behaviors (0 = no; 1 = yes), and partner drinking (0 = no; 1 = yes).
Statistical analysis
We used descriptive and regression analyses in our study. As a first step, descriptive statistics were employed to comprehend the characteristics of the analytical sample. Subsequently, logistic regression analysis was utilized to examine the connections between the dependent and independent variables. Models were built sequentially. There were six models in total—two each for emotional, sexual, and physical IPV. In Models 1, 3, and 5 we first explored the bivariate relationship between the dependent and independent variables, while control variables were incorporated in Models 2, 4, and 6. We use odds ratios (ORs) to present the results, where values exceeding 1 suggest a higher likelihood of experiencing emotional, sexual, and physical IPV, and values below 1 indicate reduced odds of encountering these forms of IPV. All analyses were conducted using STATA 17 (State Corp, College Station, TX, USA). The “svy” function was applied during the statistical analysis to account for the cluster sampling design and sampling weights.
Results
Table 1 presents the characteristics of the sample. The findings revealed that over the past 12 months, women experienced emotional (22%), sexual (7%), and physical (20%) violence. Additionally, 25% experienced severe food insecurity, 25% faced moderate food insecurity, and 24% encountered mild food insecurity, with 26% reporting no food insecurity. In terms of socioeconomic status, more than a quarter of the women (27%) had no formal education, although the majority (71%) were employed. For demographic factors, more than half of the women (52%) resided in rural areas, with the largest age group being 25 to 29 (22%) followed by 30 to 34 (20%). Exploring attitudinal and behavioral characteristics, we found that nearly 7 in 10 women (68%) reported the justification of spousal violence, whereas 37% experienced partner-controlling behaviors. Moreover, approximately half of the women (46%) reported that their partner consumed alcohol.
Sample Characteristics (n = 4,690).
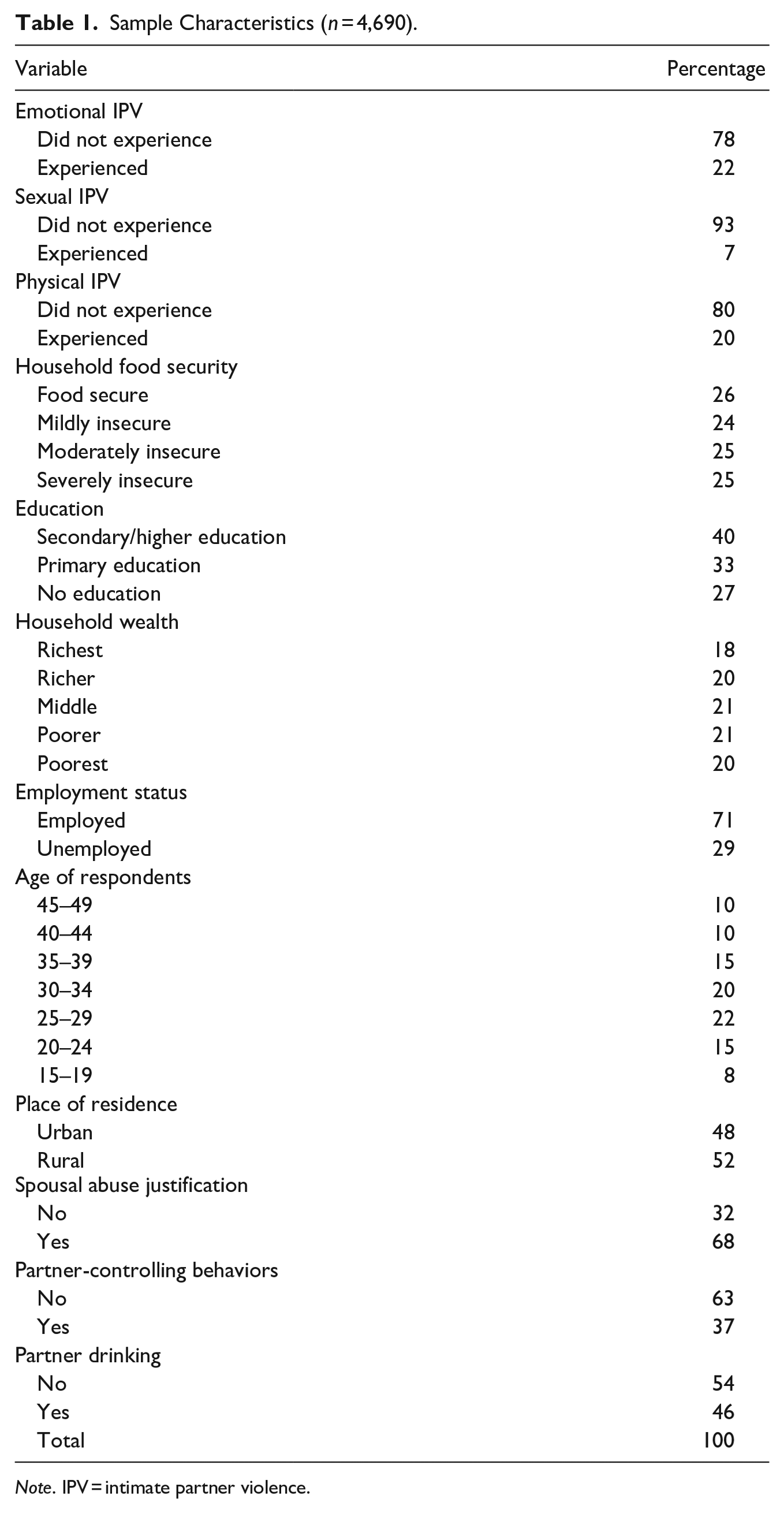
Note. IPV = intimate partner violence.
Table 2 presents the results from the regression analysis. In Model 1, the bivariate analysis demonstrated that women experiencing severe (OR = 1.51, p < .01) and moderate (OR = 1.67, p < .001) food insecurity were more likely to encounter emotional IPV than those without any food insecurity. However, after adjusting for control variables in Model 2, these associations were no longer statistically significant. Further analysis revealed that attitudinal and behavioral factors, such as partner-controlling behaviors and partner drinking, played a significant role in nullifying these relationships. Regarding sexual IPV, as indicated in Model 3, the bivariate analysis showed that women facing severe (OR = 2.45, p < .001), moderate (OR = 2.30, p < .001), and mild (OR = 1.83, p < .05) food insecurity were more susceptible to sexual IPV compared to those without any food insecurity. Despite a reduction in the level of statistical significance, these associations remained largely robust even after adjusting for control variables in Model 4, indicating that women experiencing severe (OR = 2.09, p < .01), moderate (OR = 1.88, p < .05), and mild (OR = 1.76, p < .05) food insecurity continued to be at a heightened risk of sexual IPV. In Model 5, the bivariate analysis showed that women with severe (OR = 2.40, p < .001) and moderate (OR = 1.78, p < .001) food insecurity were more likely to encounter physical IPV compared to those without any food insecurity. However, after incorporating control variables in Model 6, the significance of moderate food insecurity completely disappeared. Nevertheless, the difference between women with severe food insecurity and those without any food insecurity remained statistically significant (OR = 1.89, p < .001). Notably, the adjustments made for attitudinal and behavioral factors, specifically partner-controlling behaviors and partner drinking, played a significant role in the observed alterations within the relationship between food security status and sexual and physical IPV. These outcomes, although not explicitly displayed in Table 2, emphasize the critical impact of these influential factors on the associations under investigation.
Logit Models Predicting Emotional, Sexual, and Physical Intimate Partner Violence Among Women in Cameroon.
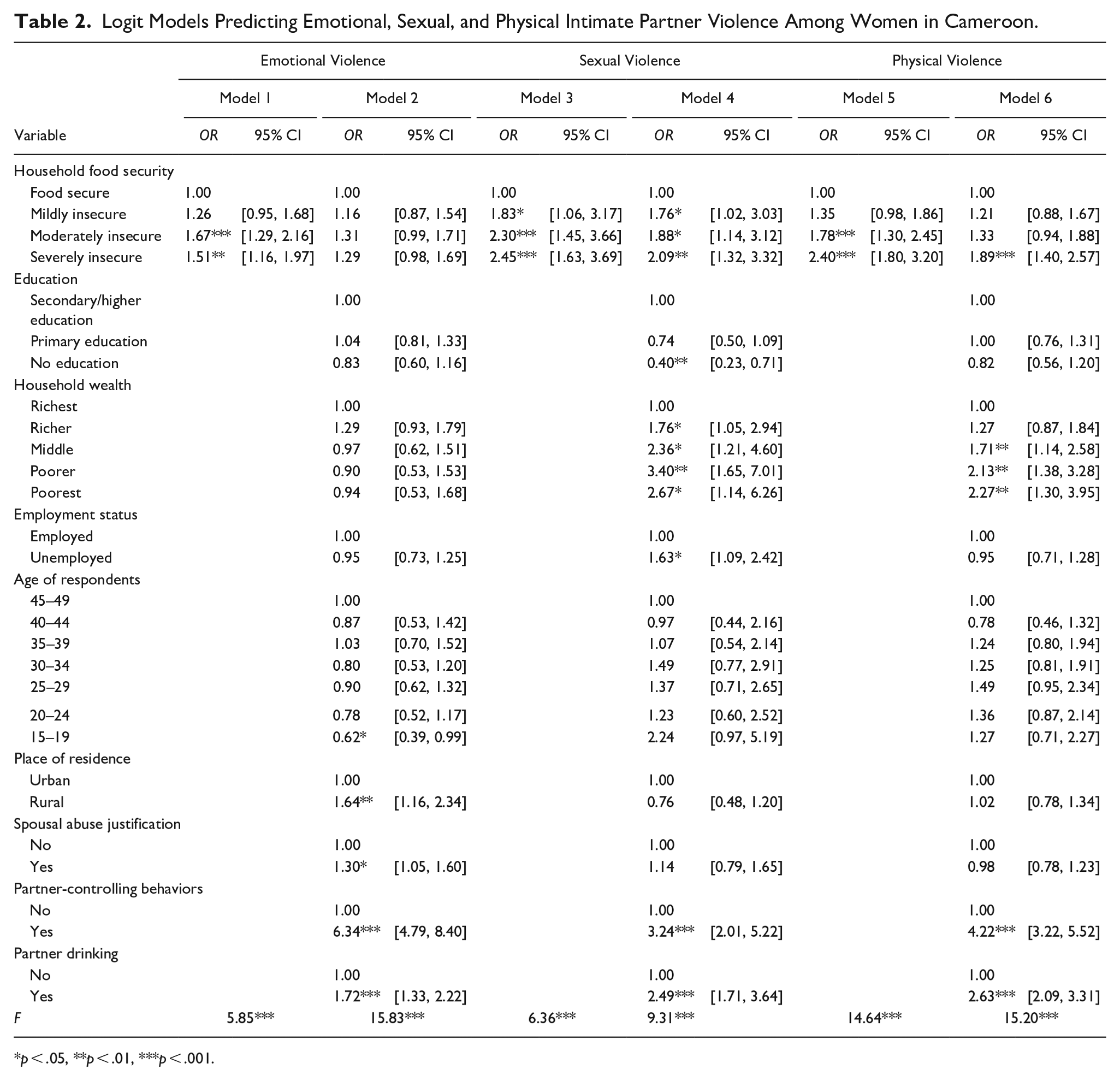
p < .05, **p < .01, ***p < .001.
In addition to food security status, our study identified various control variables associated with emotional, sexual, and physical IPV. For example, women from the “poorest” (OR = 2.67, p < .05), “poorer” (OR = 3.40, p < .01), “middle” (OR = 2.36, p < .05), and “richer” (OR = 1.76, p < .05) households were more likely to experience sexual IPV, contrasting with their “richest” counterparts. Similarly, women from the “poorest” (OR = 2.27, p < .01), “poorer” (OR = 2.13, p < .01), and “middle” (OR = 1.71, p < .01) households were more likely to experience physical IPV. In addition, unemployed women had a higher likelihood of experiencing sexual IPV compared to their employed counterparts (OR = 1.63, p < .05). Regarding demographic characteristics, women aged 15 to 19 had a lower likelihood of experiencing emotional IPV compared to those aged 45 to 49 (OR = 0.62, p < .05), whereas rural women were more likely to experience emotional IPV compared to their urban counterparts (OR = 1.64, p < .01). With respect to attitudinal and behavioral attributes, women justifying spousal abuse were more likely to experience emotional IPV compared to those who did not (OR = 1.30, p < .05). Furthermore, partner-controlling behaviors were significantly associated with heightened odds of experiencing emotional (OR = 6.34, p < .001), sexual (OR = 3.24, p < .001), and physical (OR = 4.22, p < .001) IPV. Similarly, women whose partners consumed alcohol demonstrated an increased likelihood of experiencing emotional (OR = 1.72, p < .001), sexual (OR = 2.49, p < .001), and physical (OR = 2.63, p < .001) IPV, compared to those whose partners did not.
Discussion and Conclusions
Despite an extensive body of literature that explores potential mechanisms explaining the factors associated with IPV experienced by women, very few studies have studied the association of food security status with women’s experience of IPV in SSA countries, including Cameroon. This void in the literature requires policy consideration, especially as approximately 60% of households in SSA struggle with moderate to severe food insecurity. Cameroon is not very different from this trend, as the period between 2020 and 2022 witnessed 59% of households in the country experiencing moderate to severe food insecurity. To address this void, we use the 2018 CDHS to investigate the relationship between food security status and three distinct forms of IPV (i.e., emotional, sexual, and physical IPV) among ever-married women in Cameroon.
In our analysis, once we controlled for partner-controlling behaviors and partner alcohol consumption, the association between emotional IPV and food insecurity became no longer significant. In contrast, its impact on sexual and physical IPV was only partially explained by these two control variables. These observations may further be supported by previous studies, showing that the responsibility of providing adequate and safe food is often perceived as a traditional obligation of men in many SSA countries (Awungafac et al., 2021). Consequently, it is plausible that men who fail to fulfill this role may resort to controlling behaviors to assert their dominance over their partners (Hatcher et al., 2019; Ragetlie & Luginaah, 2023). Similarly, research has demonstrated that alcohol misuse is a common coping mechanism in response to hunger and distress stemming from food insecurity, and such misuse when used as a coping strategy has been linked to an escalation in IPV incidents (Ragetlie et al., 2021). Considering these possible mechanisms, food insecurity as an indirect pathway to IPV may exist wherein food insecurity fosters a gendered environment that encourages husbands to exert control over their partners. Simultaneously, alcohol consumption may serve as a coping strategy, both of which can contribute to an increased risk of all three types of IPV, particularly emotional IPV.
However, unlike emotional IPV, our research reveals that women facing food insecurity are disproportionately vulnerable to experiencing sexual and physical IPV compared to their more economically better counterparts, even after considering other relevant factors. This finding is consistent with previous studies suggesting that food insecurity often signals heightened economic dependency among women (Krishnan et al., 2008). Concurrently, emotional IPV has been identified as a precursor to various other forms of IPV, including sexual and physical violence (Zarza et al., 2009). Our study also provides partial support for this assertion, as the prevalence of women’s reported experiences was notably higher for emotional IPV (22%) in comparison to sexual (7%) and physical (20%) IPV. Within this framework, it is possible that women struggling with food insecurity could encounter structural barriers when attempting to leave abusive relationships—even with their experience of emotional IPV as a possible warning sign, as they may lack the means to provide basic necessities such as food, clothing, and shelter for themselves and their children.
Considering our findings, we explore the relationship between the policy objectives of two interconnected SDG targets: Target 2.1 (i.e., universal access to safe and nutritious food) and Target 5.2 (ending all forms of violence against women and girls). Our analysis underscores the strong association between food insecurity and various forms of IPV, including emotional, sexual, and physical violence. Therefore, it is critical that food assistance programs go beyond the mere provision of safe and nutritious food, incorporating strategies for preventing IPV. To effectively address this issue, these programs should consider integrating culturally and socially sensitive initiatives that promote awareness of safe drinking practices and foster healthy, balanced relationships between spouses, especially within the context of food insecurity. Moreover, it has been proposed that implementing direct cash transfers to women as part of social protection interventions can help reduce their dependence on male partners, thereby partially alleviating both food insecurity and IPV. For a more sustainable approach, it becomes crucial to confront the root causes of male dominance and gender inequality. Establishing a training infrastructure that ensures women have access to opportunities to develop valuable human capital is essential. Empowering women in this manner may serve as a long-term strategy for tackling the challenges of both food insecurity and IPV, ultimately contributing to the achievement of the SDGs.
Notwithstanding the valuable insights shared by our study, it is critical to acknowledge several limitations. One significant limitation arises from the cross-sectional nature of the CDHS, making it challenging to identify the direction of the association. This suggests the potential for a bidirectional relationship, wherein food insecurity could be influenced by various forms of IPV. Unfortunately, our findings are confined to establishing statistical associations and do not provide a basis for establishing causality. Furthermore, existing research has indicated that IPV and food insecurity are sensitive topics, prompting individuals to underreport these experiences due to social desirability bias (Darteh et al., 2021; Trudell et al., 2021). Consequently, there might be an underestimation of the prevalence of these phenomena within the dataset. Considering these limitations, it is crucial to recognize the importance of collecting longitudinal quantitative data and conducting in-depth qualitative research. Such a comprehensive approach may be useful for unpacking the underlying mechanisms and processes that underpin the complex relationship between IPV and food insecurity. Despite these limitations, our study stands as one of few studies to explore the association between IPV and food insecurity in SSA, and Cameroon in particular. This contribution highlights the significance of further research in this domain, emphasizing the need for more nuanced and comprehensive investigations to effectively address these critical societal issues.
Footnotes
Author Contributions
DA and YS contributed to conceptualizing, planning the analysis, carrying out statistical analysis, and drafting the manuscript. DA, RA, and YS contributed to the design of the analysis and review of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Ethical Approval
Informed Consent
Informed consent was obtained from all participants of this DHS survey. For participants aged below 18 years, parental informed written consent was obtained.