
Abstract
Intimate partner violence (IPV) against women is a global public health problem. Conceptual frameworks suggest misperceived norms around IPV might drive perpetration of violence against women in southern and eastern Africa. We conducted a cross-sectional, population-based survey of all men residing in a rural parish in southwest Uganda, eliciting their endorsement of IPV in five hypothetical scenarios and their reported frequency of perpetration of violence against their wife/main partner. They also reported their perceptions about the extent to which most other men in their villages endorsed and/or perpetrated IPV, which we compared against the population data to measure the primary explanatory variable of interest: whether individuals misperceived norms around IPV. We fitted multivariable Poisson regression models specifying personal IPV endorsement and IPV perpetration as the outcomes. Overall, 765 men participated in the study (90% response rate): 182 (24%) personally endorsed IPV, and 78 of 456 partnered men (17%) reported perpetrating one or more acts of IPV at least once per month. Although most men neither endorsed nor reported perpetrating IPV, 342 (45%) men mistakenly thought that most other men in their villages endorsed IPV and 365 (48%) men mistakenly thought that most other men perpetrate IPV at least monthly. In multivariable regression models, men who misperceived most men to endorse IPV were more likely to endorse IPV themselves (adjusted relative risk [aRR] = 2.44; 95% CI [1.66, 3.59]; p < .001). Among partnered men, those who misperceived IPV perpetration to be normative were more likely to perpetrate IPV themselves (aRR = 4.38; [2.53, 7.59]; p < .001). Interventions to correct misperceived norms about IPV may be a promising method for reducing violence against women in rural Uganda.
Keywords
Violence against women is a global public health issue (White et al., 2024). Intimate partner violence (IPV) victimization rates range from 16% in East Asia to 66% in Central Africa (Devries et al., 2013). Victims of IPV often suffer severe short- and long-term health consequences affecting mental health, medical well-being, and reproductive health (Hung et al., 2012; Tsai et al., 2015; Wright et al., 2019). However, health systems and other institutions often lack support for women exposed to IPV (Gezinski & Gonzalez-Pons, 2019; Iyengar & Sabik, 2009; Jewkes, 2022). Additionally, IPV victims often do not seek help due to social sanctions they encounter, including from close social ties, when reporting IPV and also the stigma associated with IPV (Barnett et al., 2016; McCleary-Sills et al., 2016; Robinson et al., 2020).
Many factors contribute to male IPV perpetration against women, including gender-inequitable norms; sex-based disparities in economic power, economic status, and education; alcohol consumption; and childhood experiences with violence and abuse (Fulu et al., 2013; Jewkes, 2002; Shannon et al., 2012; Tsai, 2013). Misperceived norms about IPV may also drive IPV perpetration (Dardis et al., 2016; Fabiano et al., 2003; Mulla et al., 2018; Neighbors et al., 2010; Witte & Mulla, 2013). These studies indicate that individuals overestimate the extent to which IPV is accepted by peers and also the extent to which IPV is perpetrated by peers. These misperceptions are associated with personal IPV-related attitudes and perpetration of IPV. Existing work on injunctive (i.e., attitudinal) norms and descriptive (i.e., behavioral) norms (Cialdini et al., 1990) as drivers of IPV perpetration focuses on young adults in the United States, particularly within institutional settings. However, identifying and correcting misperceptions about local IPV norms may reduce the risk of IPV perpetration (Berkowitz et al., 2022; Mulla et al., 2018; Orchowski, 2019).
In Uganda, the focus of the present study, 1 in 4 men report having perpetrated IPV against a partner (Uganda Bureau of Statistics [UBOS] and ICF, 2018) and many endorse IPV as acceptable (Tsai et al., 2017). The extent to which misperceived norms might drive IPV attitudes and behavior in this setting is largely unknown. Prior studies in Africa have found that adults overestimate the prevalence of health risk behaviors and underestimate the prevalence of health behaviors, and that these misperceptions are associated with individuals themselves engaging in the behavior they mistakenly believed to be common among peers (Carey et al., 2011; Mulawa et al., 2016; J. M. Perkins, Kakuhikire, Baguma, Evans, et al., 2023; J. M. Perkins et al., 2022; J. M. Perkins, Krezanoski, et al., 2019; J. M. Perkins, Nyakato, Kakuhikire, Mbabazi, et al., 2018). This literature is consistent with studies from Niger and Uganda suggesting that community norms may play a role in IPV risk (Green et al., 2020; Shakya et al., 2022).
The public health relevance of this work is that using a social norms approach (Berkowitz et al., 2022; Dempsey et al., 2018; H. W. Perkins, 2003) to highlight actual local norms may catalyze personal and collective change (D. T. Miller & Prentice, 2016; Orchowski, 2019; Prentice, 2018) by reducing false consensus (mistakenly assuming “everyone is like me” [Ross et al., 1977]) and pluralistic ignorance (mistakenly assuming “everyone is different from me” [D. T. Miller & McFarland, 1987]). Men who are aware of actual local norms may be less likely to endorse, initiate, and/or perpetrate IPV themselves and/or support or tolerate IPV perpetration in their communities.
The Current Study
We conducted a population-based study of men in southwestern Uganda to explore IPV endorsement and IPV perpetration norms. Specifically, we assessed men’s attitudes about IPV, self-reported IPV perpetration, and perceptions about whether other men in their villages endorsed IPV (i.e., injunctive norms) and/or perpetrated IPV (i.e., descriptive norms). Additionally, the data structure of this study—in which we surveyed all men residing within a defined place—permitted us to identify misperceived norms by comparing men’s perceived norms to the actual population prevalence of personal IPV endorsement and perpetration (based on aggregated perpetration reports from all men in the study population). Thus, in this study, we were able to measure the type and extent of misperceived norms about IPV endorsement and perpetration and then estimate the associations between perceived (or misperceived) norms and personal reports of IPV endorsement and perpetration.
Methods
Study Population and Procedure
We conducted a cross-sectional, population-based study of all men residing in eight villages of a rural parish in Mbarara, Uganda. Most households engage in an agriculture-based economy or small-scale trading/enterprise, and food and water insecurity are common (J. M. Perkins, Nyakato, Kakuhikire, Tsai, et al., 2018; Tsai et al., 2016). Prior to data collection, we met with village and parish leaders to describe the study foci and the study procedures. In collaboration with local leaders and colleagues, we held a series of community sensitization meetings to provide residents with a general overview of the study purpose and procedures and elicit feedback on the study design (Kakuhikire et al., 2021). The survey was framed generally as a study about the health, wellbeing, behaviors, and social lives of parish residents. We then conducted a parish-wide census to identify individuals eligible for participation. Eligibility was restricted to adult men aged 18 years and older who were permanent residents in one of the eight villages within the parish.
Research assistants fluent in the local language (Runyankore) received training in best practices for collecting sensitive data, as well as psychosocial issues related to IPV in general (including gender equity, emotional support and skills building, questionnaire training, when and how to refer study participants for professional counseling); they also received ongoing supervision during the conduct of fieldwork (Jansen et al., 2004). Survey questions were first written in English, translated into Runyankore, and then back-translated to English to verify the translation’s fidelity to the original.
Using the census, a research assistant approached an eligible adult, typically at their home, and conducted the informed consent process. They again described the study as being about the social lives and health of residents of that parish. Participants were told that they would receive a kilogram of sugar or a bar of soap for participating in the study (per local norms). Participants were also informed that their participation was completely voluntary. The study team made multiple attempts to reach every eligible individual during the study period. Ethical approval was granted by Harvard University, the Research Ethics Committee at Mbarara University of Science and Technology, and the Vanderbilt Human Research Protections Program. We also received clearance from the Uganda National Council of Science and Technology and the Office of the President of the Republic of Uganda.
Measures
Personal IPV Endorsement
Every participant was asked whether he personally thought a husband was justified in hitting or beating his wife/main partner in each of five hypothetical scenarios. The scenarios were modeled after those that have been administered in the Uganda Demographic and Health Surveys since 2000 to 2001 (Uganda Bureau of Statistics [UBOS] and ICF, 2018; Uganda Bureau of Statistics [UBOS] and ORC Macro, 2001): (a) if the wife goes out without telling the husband, (b) if the wife neglects the children, (c) if the wife argues with the husband, (d) if the wife refuses to have sex with the husband, and (e) if the wife burns the food. These specific survey items have also been previously administered in Mbarara (Tsai et al., 2017). Study participants were classified as endorsing IPV perpetration if they agreed that a husband was justified in hitting or beating his wife/main partner in any of the five scenarios.
Perceived Norms About IPV Endorsement
Perceived injunctive norms were elicited using questions that paralleled the previously described ones about eliciting personal attitudes. Study participants were prompted to imagine that there were 10 men in their own village and then asked how many men out of 10 would endorse IPV for each of the five hypothetical scenarios. Participants who thought that at least 6 out of 10 (i.e., most) men would endorse the use of IPV in at least one of the five scenarios were classified as perceiving IPV to be normatively acceptable.
Personal IPV Perpetration
Among men who had a cohabiting main partner or wife in the past 12 months (hereafter described as “partnered”), we asked them to report frequency of eight acts of physical and sexual violence against their wife/main partner in a typical month (Ellsberg & Heise, 2005; Speizer, 2009; Straus et al., 1996): (a) slapping her; (b) pushing or shaking her, or throwing something at her that could hurt; (c) punching her with a fist or with something that could hurt; (d) kicking or dragging her; (e) choking or burning her; (f) threatening or attacking her with a knife, machete, hoe, or gun; (g) forcing her to have sexual intercourse when she did not want to; and (h) forcing her to engage in sexual activity other than intercourse when she did not want to. The study team used “a typical month” as the time reference because this study aimed to assess frequent and ongoing IPV perpetration (as opposed to lifetime events). Response options were “never,” “once per month,” “2 to 3 times per month,” “once per week,” “a few times per week,” and “almost every day.” Men were classified as having perpetrated IPV if they reported perpetrating any act with any frequency (vs. no IPV perpetration).
Perceived Norms About IPV Perpetration
Perceived descriptive norms were elicited similarly. Participants were asked to say how often, if ever, most men in their village perpetrated each of the eight acts of physical and sexual violence as above. The same set of response options were used, ranging from “never” to “almost every day.” Men who thought that most other men in their village engaged in IPV (i.e., perpetrated any act at least once per month) were classified as perceiving IPV perpetration to be the village norm. Both sets of questions about perceived norms specified “most men in your village” as the reference group. Our pilot testing indicated that this group was a recognizable and tractable social group in this context.
Additional Covariates
We also collected information about age, marital status, education (primary education or less vs. some secondary education or more), household asset wealth (Filmer & Pritchett, 2001; M. L. Smith et al., 2020), whether a participant had witnessed during childhood their mother or female guardian being subjected to domestic violence (Gubi et al., 2020), severe food insecurity (based on the Household Food Insecurity Access Scale [Tsai et al., 2012]), and current personal alcohol consumption (1+ days per week vs. less often or never) (Gubi et al., 2020). Missingness across these variables ranged from 0% to 3.4%.
Statistical Analysis
First, we aggregated men’s self-report of personal IPV endorsement and personal IPV perpetration to calculate the prevalence rates of IPV endorsement and perpetration at the village level. We then determined actual local norms. IPV endorsement was classified as normative (in the study population and in each village) if more than 50% of men endorsed IPV as being justifiable in at least one of the five hypothetical scenarios. Likewise, IPV perpetration was classified as normative if more than 50% of partnered men reported having perpetrated any act of physical or sexual violence per month. Similar thresholds to identify actual norms have been used in the social norms literature in Uganda and in other settings (Haines & Spear, 1996; Klika et al., 2019; Larimer & Neighbors, 2003; Mennicke et al., 2018; J. M. Perkins, Krezanoski, et al., 2019; Perkins, Nyakato, Kakuhikire, Mbabazi, et al., 2018; S. W. Smith et al., 2021).
Second, we compared individuals’ perceptions of the norm to the actual local norm to determine the extent to which village-level norms were misperceived by participants. A participant was categorized as misperceiving the norm when his perception of the village norm did not match the actual village norm. For example, if a participant lived in a village where most men did not endorse IPV, but he nonetheless (incorrectly) thought that most other men in this village endorsed IPV, then he would be categorized as misperceiving the norm. This approach to measuring misperceived norms by comparing perceived norms to actual norms in a whole-population study draws on methods from previous studies in this setting and elsewhere (J. M. Perkins et al., 2022; J. M. Perkins, Kakuhikire, Baguma, Jeon, et al., 2023; J. M. Perkins, Nyakato, Kakuhikire, Mbabazi, et al., 2018; J. M. Perkins et al., 2019).
Next, we assessed the extent to which study participants’ misperceptions of local norms were concordant or discordant with their self-reported personal behavior. If personal belief or behavior was consistent with the misperception (e.g., a study participant reported perpetrating acts of IPV while falsely believing that most other men in his village were also perpetrators), then the participant was considered to be in a state of false consensus. If personal belief or behavior was inconsistent with the misperception (e.g., a study participant did not endorse IPV while falsely believing that most other men in his village did endorse IPV), then the participant was considered to be in a state of pluralistic ignorance.
We then tested for overestimation of IPV endorsement at the item level by using a series of paired-sample t-tests to assess whether the proportion who personally endorsed IPV differed from the average estimated proportion of IPV endorsement by others in each scenario. Similarly, we tested for overestimation of IPV perpetration by using a series of non-parametric Wilcoxon matched-pairs signed tests to assess whether the median self-reported frequency of perpetrating a particular IPV act differed from the median frequency perceived (among most other men) of perpetrating that act.
Finally, we fitted two multivariable Poisson regression models to estimate associations between misperceived norms and personal IPV endorsement and perpetration while adjusting for covariates. With a binary dependent variable, the Poisson regression model with robust estimates of variance (“modified Poisson”) has been shown to yield estimated incidence rate ratios that can be interpreted straightforwardly as relative risk ratios (Zou, 2004). In the first model, any personal IPV endorsement was specified as the outcome and perceiving any IPV endorsement as the local norm was the main explanatory variable. In the second model (including only partnered men), self-reported perpetration of any act of IPV was specified as the outcome and perceiving any IPV perpetration to be the norm was the main explanatory variable. Both models adjusted for sociodemographic factors and used cluster-correlated robust estimates of variance to account for potential clustering of study participants at the village level. We also adjusted for any personal IPV endorsement in Model 2 (Shakya et al., 2018; Shannon et al., 2012; Uthman et al., 2011).
For a sensitivity analysis, we used methods proposed by Vanderweele & Ding (2017) to calculate the e-value. The e-value represents the minimum strength of association (on the risk ratio scale) that an unobserved confounder would need to have with both the exposure (perceived norm) and the outcome (IPV endorsement/perpetration) to completely account for the estimated association, conditional upon the included covariates. A large e-value suggests that an unobserved confounding would need to have very strong associations (with both the exposure and outcome) in order to sufficiently explain away the observed association.
Results
Overall, 756 of 840 eligible men were interviewed (90% response rate): 317 (42%) were less than 30 years of age, 455 (60%) had no education or only a primary education, 456 (60%) had a primary partner, 235 (31%) witnessed domestic violence during childhood, 122 (16%) experienced severe food insecurity, and 243 (32%) reported consuming alcohol on at least a weekly basis (Supplemental Table 1). Parish residents who did not participate in the study were generally either unavailable to participate despite repeated attempts (e.g., due to migrant work or incarceration) or unable to participate despite repeated attempts (e.g., acutely intoxicated or cognitively impaired, or too ill to tolerate the study procedures).
Prevalence of IPV Endorsement and Misperceived Injunctive Norms
Approximately a quarter of participants (182 [24%]) agreed that IPV against a wife/partner would be acceptable in one or more of the five hypothetical scenarios. At the village level, the prevalence of IPV endorsement ranged from 21% to 31%. Thus, given that most men did not endorse IPV, it was not the local norm. In contrast, 342 (45%) participants believed that most other men in their own village endorsed IPV in at least one scenario. Given our population data, these participants misperceived the injunctive (attitudinal) norm. Among men who misperceived IPV endorsement as the local norm, 89 (27%) incorrectly believed that most men would endorse IPV in two scenarios, and 115 (34%) incorrectly believed that most men would endorse IPV in three or more scenarios. Paired-sample t-tests indicated that participants overestimated the extent to which other men in their villages endorsed IPV against a wife/partner (p < .001 for each of the five hypothetical scenarios; Table 1).
Endorsement of IPV When Presented With Five Hypothetical Scenarios, Among Adult Men in Eight Villages in Rwampara District, Southwestern Uganda (N = 748).
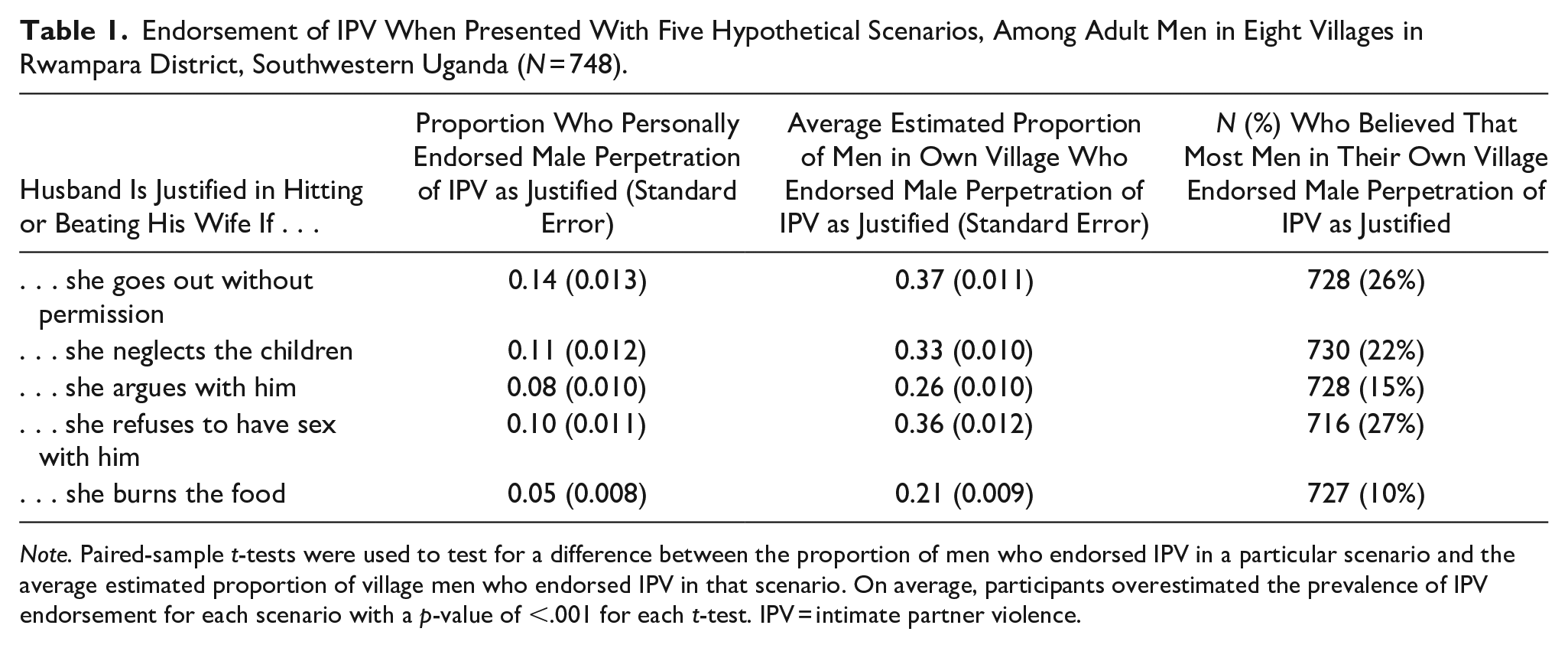
Note. Paired-sample t-tests were used to test for a difference between the proportion of men who endorsed IPV in a particular scenario and the average estimated proportion of village men who endorsed IPV in that scenario. On average, participants overestimated the prevalence of IPV endorsement for each scenario with a p-value of <.001 for each t-test. IPV = intimate partner violence.
Prevalence of IPV Perpetration and Misperceived Descriptive Norms
Among 456 partnered participants, 78 (17%) reported perpetrating at least one act of physical or sexual IPV against a wife/partner. At the village level, the prevalence of self-reported perpetration ranged from 5% to 19%. Thus, given that most men did not report perpetrating IPV, it was not the local norm. In contrast, 365 (48%) participants thought most other men in their own villages perpetrated IPV. Given our population data, these participants misperceived the descriptive (behavioral) norm. Among men who misperceived IPV perpetration as the local norm, 149 (41%) incorrectly believed that most men perpetrated one to two acts of physical or sexual IPV at least monthly; 105 (29%) incorrectly believed that most men perpetrated three to four acts at least monthly; and 109 (30%) incorrectly believed that most men perpetrated five to seven acts at least monthly. For each type of IPV, Wilcoxon matched-pairs signed tests indicated that participants overestimated the frequency of IPV perpetration against a wife/partner by men (p < .001 for each act). Supplemental Figure 1 displays this finding visually: the prevalence of perceived frequency of each type of IPV was much greater than the prevalence of reported perpetration for each act.
Pervasiveness of Misperceived IPV Norms
The prevalence of misperceiving IPV norms was pervasive across all sociodemographic subgroups (Supplemental Table 2). False consensus was common. Among participants who endorsed IPV in at least one scenario, 120 (66%) mistakenly thought that most other men also endorsed IPV in at least one scenario. Likewise, among participants who reported perpetrating IPV on at least a monthly basis, 65 (82%) mistakenly thought that most other men also perpetrated IPV on at least a monthly basis. Pluralistic ignorance was also present. Among participants who did not endorse IPV in any of the five hypothetical scenarios, 222 (39%) mistakenly thought that most other men endorsed IPV in at least one scenario. Among participants who denied perpetrating IPV, 300 (44%), mistakenly thought that most other men were perpetrators.
Associations Between Misperceived Norms and IPV Endorsement and Perpetration
After multivariable adjustment, men who misperceived IPV endorsement as the local norm were more likely to personally endorse IPV (adjusted relative risk [aRR] = 2.44; 95% CI [1.66, 3.59]; p < .001) compared with men who correctly perceived that IPV endorsement was not the local norm. The e-value associated with this estimate was 4.31. Alcohol consumption was also associated with personal IPV endorsement (aRR = 1.49; [1.07, 2.07]; p = .019). No other factors were associated with endorsement (Table 2).
Multivariable Poisson Regression Estimates of the Association Between Misperceived Norms and Endorsement of IPV, Among Adult Men in Eight Villages in Rwampara District, Southwestern Uganda (N = 669).
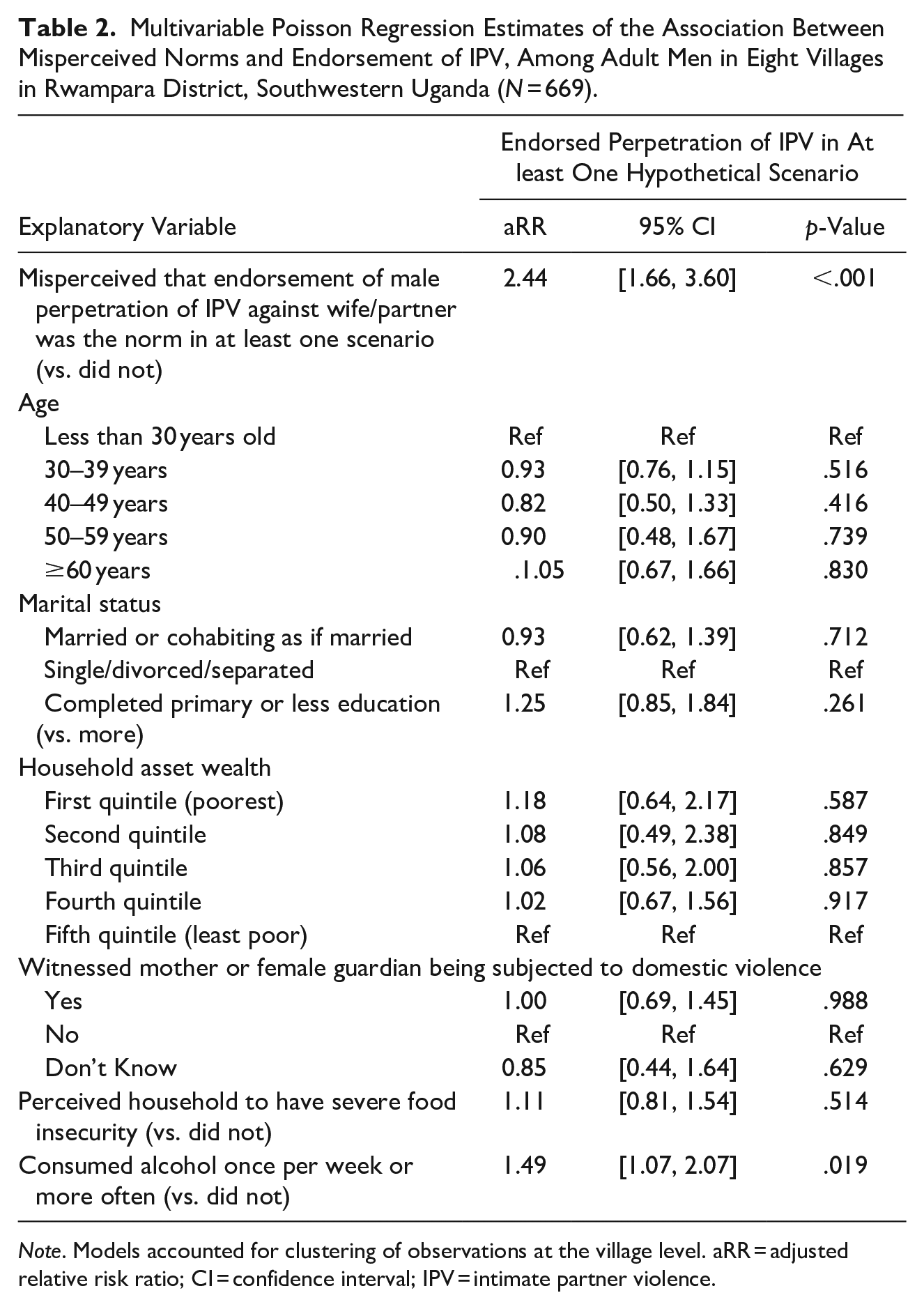
Note. Models accounted for clustering of observations at the village level. aRR = adjusted relative risk ratio; CI = confidence interval; IPV = intimate partner violence.
In a multivariable Poisson regression model fitted to the subsample of partnered men, those who misperceived IPV perpetration as the local norm were more likely to report perpetrating IPV themselves (aRR = 4.38; 95% CI [2.53, 7.59]; p < .001). The associated e-value for this estimate was 8.23. Partnered men who endorsed IPV in the hypothetical scenarios were also more likely to report perpetrating IPV (aRR = 2.26; [1.52, 3.36]; p < .001), as were partnered men who witnessed domestic violence during childhood (aRR = 1.53; [1.10, 2.11]; p = .011). Men of older age were less likely to endorse IPV (Table 3).
Modified Multivariable Poisson Regression Estimates of the Association Between Misperceived Norms and Self-Reported Perpetration of IPV, Among Partnered Men in Eight Villages in Rwampara District, Southwestern Uganda (N = 418).
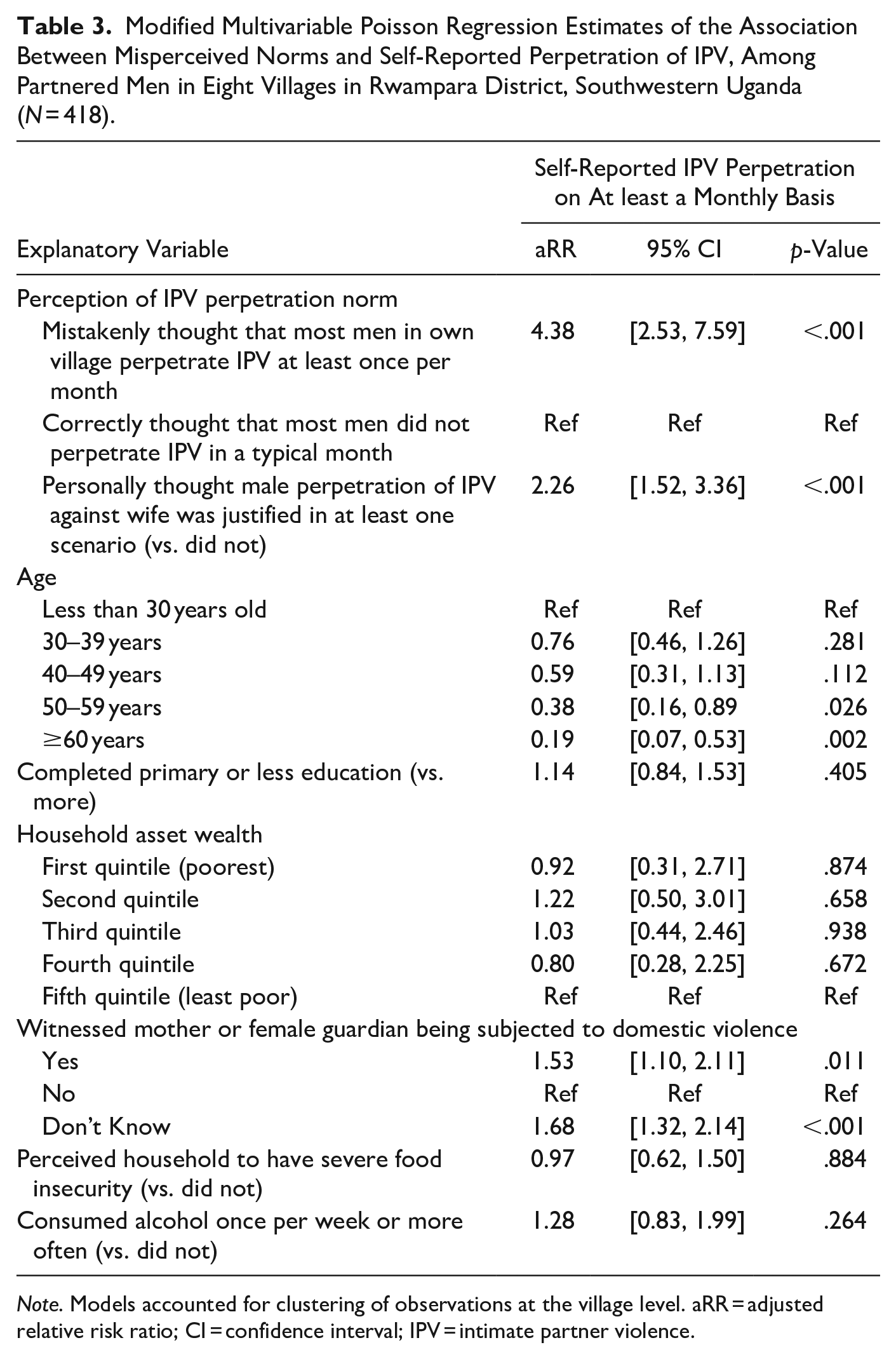
Note. Models accounted for clustering of observations at the village level. aRR = adjusted relative risk ratio; CI = confidence interval; IPV = intimate partner violence.
Discussion
This population-based study of men in a rural parish in southwest Uganda found that many men overestimated the extent to which other men in their villages endorsed IPV and overestimated the extent to which other men perpetrated IPV. For example, while the prevalence of self-reported IPV perpetration ranged from 5% to 19% across villages, nearly half of men mistakenly believed IPV perpetration to be the norm. These men incorrectly thought that most men in their villages perpetrated at least one type of IPV at least once per month. Misperceived norms were present across all demographic, attitudinal, and behavioral subgroups. Men who misperceived local IPV norms were more likely to endorse and perpetrate IPV themselves. Our findings echo previously published studies showing the pervasiveness of misperceived descriptive and injunctive norms about IPV found in other contexts and populations and their power to influence personal attitudes and behavior (Dardis et al., 2016; Fabiano et al., 2003; Mulla et al., 2018; Neighbors et al., 2010; Witte & Mulla, 2013).
These findings suggest a social norms approach would be effective in addressing IPV in this context. Such an approach would focus on highlighting positive local norms as a way to correct misperceived norms and, ultimately, reduce IPV endorsement and perpetration (Cislaghi & Berkowitz, 2021; H. W. Perkins, 2003). Many studies on other topics have found that changing perceived norms leads to changes in behavior and attitude (Dempsey et al., 2018; D. T. Miller & Prentice, 2016; Prentice, 2018; Tankard & Paluck, 2016). This approach could contribute to efforts to reduce individual acts of violence against women and potentially create a climate less tolerant of violence against women within a population. As an example, an education-entertainment field experiment conducted in rural villages in Uganda changed perceived norms about the acceptability of disclosure about violence against women (Green et al., 2020). These changes were then associated with subsequent greater disclosure of violence and reduced victimization. Similarly, an intervention correcting misperceptions among married men in Saudi Arabia about the acceptability of permitting women to work outside the home by communicating that most men privately support women working outside the home led to an increase in women interviewing for jobs (Bursztyn et al., 2020). A study addressing sexual assault and sexual risk has targeted reducing misperceived IPV norms among male adolescent students in South Africa (Berkowitz et al., 2022). Preliminary data have shown it to be feasible, acceptable, and effective.
Actual norm information could be spread through personalized normative feedback via existing programs (e.g., via couples-based testing and counseling or contraception programs), social norms marketing campaigns (e.g., billboards, radio ads, SMS messages, etc.), and small group settings such as community conversations and education-entertainment showings (Abramsky et al., 2014; National Research Council, 2015). Stigma associated with domestic violence in these settings may reduce individual reporting and inhibit discussion of IPV (Kaye et al., 2005). These community-based messages may be more socially acceptable. Exemplar messages could be: “Most men in your village do not approve of violence against a wife/partner in any scenario” or “More than X% of men in your village do not beat their wives.” At the same time, caution should be taken to ensure that IPV victims are not further stigmatized. Messages about positive local norms (e.g., around bystander action or supporting someone to seek support) may need to be included as well. Additional research is needed to assess, identify, and diagnose the constellation of critical IPV-related norms. Messaging could be combined with creating greater awareness of resources available for victim support as well as with other IPV reduction efforts and policies. At a minimum, messages should not include images or other text that inadvertently make the problematic attitude or behavior seem common.
This study has limitations. First, under-reporting personal IPV perpetration could cause downward bias in our estimates of prevalence (Cullen, 2022; Lépine et al., 2020; Traunmüller et al., 2019). Our estimates of IPV perpetration prevalence are consistent with data collected through face-to-face surveys elsewhere in eastern Africa (A. P. Miller et al., 2022) and either consistent with or lower than estimates generated through data collected via privacy-enhancing methods like audio-computer assisted self-interviewing (Chatterji et al., 2020; Dunkle et al., 2020). However, it is unlikely that any under-reporting or survey refusals could revise the estimated local norms to such a degree as to appreciably change this study’s findings. For example, even if the 10% of men who declined to participate all reported IPV endorsement and perpetration, both IPV endorsement and IPV perpetration would still not be local norms—and therefore, the high rate of misperceiving these norms would not change. Even if a substantial percentage of participants under-reported IPV endorsement or perpetration (e.g., due to social desirability bias), such under-reporting would have to occur by more than a factor of 2 to 3 to shift the overall estimated local norms (and thereby affect our estimates of the rates at which men misperceived these norms). While privacy-enhancing methods appear to increase reporting of IPV perpetration, they do not appear to do so by more than a factor of 2 to 3 (Cullen, 2022; Jewkes et al., 2020).
Second, it is possible that unobserved confounding variables could have biased our estimates away from the null. For example, we did not collect data on gender-inequitable decision-making patterns within the household. If men who hold gender-inequitable attitudes are more likely to endorse or perpetrate IPV and are also more likely to misperceive the extent to which IPV is normative, then that could potentially bias our estimates away from the null. However, the e-value analysis suggests that such an unobserved confounder would need to have an extremely strong association (of 4–8 on the risk ratio scale) with both IPV endorsement and perpetration, conditional on the measured covariates, to explain away the association observed in our study. Based on other studies in the region, we expect this to be unlikely. For example, in a population-based study of husband-wife dyads in Uganda, women whose husbands reported joint or wife-only decision-making about the husband’s earnings were 9 to 16 percentage points less likely to experience IPV (Zegenhagen et al., 2019). Compared with the baseline prevalence of IPV estimated in the 2016 Uganda Demographic and Health Survey (Uganda Bureau of Statistics [UBOS] and ICF, 2018), these estimates suggest an association (between gender-inequitable norms of decision-making and IPV perpetration) of at most 2 to 3 on the risk ratio scale. Thus, such an unobserved confounder would be unlikely to have a strong enough influence to explain away the estimates we obtained.
Third, although this sample generally represents men from rural contexts in eastern Africa, this sample does not represent populations that consist of young adults in which frequent IPV may be more prevalent nor men in urban settings where more resources for IPV victims may exist nor men in zones of conflict where IPV may occur more often. In contexts where IPV perpetration may be normative, assessing the extent to which both perpetration and endorsement are still overestimated as well as how much support for bystander engagement is underestimated would provide useful intervention information. Messages based on a social norms approach could be tailored in such settings to highlight positive norms where they exist or changes in norms trending away from IPV over time.
Conclusion
In this population-based study in rural Uganda, almost half of men in every village overestimated men’s endorsement and perpetration of IPV against women. These misperceptions were present in all subgroups, including among men who both endorsed and perpetrated IPV and among men who did not endorse or perpetrate IPV. Men with these misperceptions were more likely to endorse IPV and perpetrate IPV themselves. These findings collectively indicate a potential opportunity to reduce violence against women by addressing overestimates of IPV endorsement and perpetration in eastern Africa. Future research should assess the extent to which correcting misperceived norms among men who endorse and perpetrate IPV changes their harmful attitudes and behavior. Additionally, correcting misperceived norms among men who do not support or perpetrate IPV may increase conversation and support for protective behavior and bystander engagement. Providing information that IPV endorsement and perpetration are not normative, alongside information about protective local norms, may hold promise for reducing male-perpetrated violence against women in this setting.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605241254143 – Supplemental material for Misperception of Norms About Intimate Partner Violence as a Driver of Personal IPV Attitudes and Perpetration: A Population-Based Study of Men in Rural Uganda
Supplemental material, sj-docx-1-jiv-10.1177_08862605241254143 for Misperception of Norms About Intimate Partner Violence as a Driver of Personal IPV Attitudes and Perpetration: A Population-Based Study of Men in Rural Uganda by Jessica M. Perkins, Viola Nyakato, Bernard Kakuhikire, Julie Sriken, Cassandra O. Schember, Charles Baguma, Elizabeth B. Namara, Phionah Ahereza, Immaculate Ninsiima, Alison B. Comfort, Carolyn M. Audet and Alexander C. Tsai in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We thank the Emikago cohort study participants, without whom this research would not be possible. We also thank the Emikago Study team, for their assistance with data collection and study administration; and Nicholas Christakis, David Bangsberg, J. Niels Rosenquist, Peggy Bartek, Anna Baylor, Pamela Mbabazi, Nozmo F. B. Mukiibi, Roberts Muriisa, and Sae Takada for their assistance with study administration and infrastructure development. In addition to the named study authors, study team members who contributed to data collection and/or study administration during all or any part of the study were as follows: Patience Ayebare, Allen Kiconco, May Murungi, Tony Rugwira, Pidson Mwebaze, Specioza Twinamasiko.
Data Availability
Data and code for analysis are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by Friends of a Healthy Uganda and U.S. National Institutes of Health (NIH) R01MH125667 and (NIH) P30AG034420. The authors also acknowledge salary support from NIH K01MH115811 (JMP) and K01HD105521 (ABC).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.