
Abstract
This study aimed to understand parents’ process of centering their child’s interpersonal traumatic event in their lives post-disclosure. Specifically, how it informed their understanding of themselves, their lives, and the world. This phenomenon of centering a traumatic event in one’s life is termed event centrality and has not been previously applied to qualitative research or this population. Participants were 17 primary caregivers (14 maternal caregivers and 3 paternal caregivers) of 27 victims of child interpersonal trauma (14 males and 13 females) located in Canada. The age of participants ranged from 35 to 75 years (average = 54.5 years) and majority self-identified as Caucasian (70.6%). Grounded theory was used to analyze the data. The resulting model was labeled Vicarious Event Centralization and Decentralization, indicating that parents center their child’s interpersonal trauma across many areas of their lives, which orients them to focus on protecting and healing the child. After the child’s functioning improves, parents are then able to reorient to life beyond the trauma, representing decentralization. The grounded theory consists of three phases: Centralization, Decentralization Gateway, and Decentralization. These results illustrate that parents’ centralization of the trauma may be an adaptive mechanism that promotes child recovery, which in turn allows parents to begin to decentralize the trauma and move toward recovery. This study supports that parents are affected by their child’s trauma in a myriad of ways and require unique services to address their needs. This study can help practitioners understand the post-trauma experience for parents and target areas likely to increase recovery.
Keywords
The landmark adverse childhood experiences study (Felitti et al., 1998) illustrated the relationship between a higher number of adverse childhood experiences and adulthood mental health concerns (e.g., depression and suicide attempts), health-risk behaviors (e.g., physical inactivity and alcohol use), and disease (e.g., cancer and sexually-transmitted diseases). Since that time, there has been extensive research on the impact of childhood interpersonal trauma on the well-being of the victimized child (Hailes et al., 2019; Norman et al., 2012). Research on the well-being of parents indirectly exposed to their child’s trauma is relatively smaller, though researchers have found associations with negative mental and physical health (Cyr et al., 2016, 2018; Mangold et al., 2022). We conducted this study to learn more about parents’ experiences after their child’s trauma; specifically, how and why parents may center their child’s interpersonal traumatic event in their lives post-disclosure as this is a gap in the current literature.
Parents of children who experienced interpersonal trauma report impacts to mental health (e.g., posttraumatic stress disorder (PTSD), distress and depression; Cyr et al., 2016, 2018; Davies, 1995) and physical health (Cyr et al., 2016, 2018) after vicarious trauma exposure. Furthermore, parents perceive their mental health concerns (e.g., PTSD, depression, suicidal ideation, and anxiety) as due to their child’s interpersonal traumatic experience (Fuller, 2016; Sparks & Stoppa, 2022; Vilvens et al., 2021). Thus, parents’ well-being is impacted by their child’s experience of interpersonal trauma.
Furthermore, a relationship between child and parent functioning has been reported. For example, a review by Elliot and Carnes (2001) suggested a positive relationship between parental support following child sexual abuse (CSA) and the psychological adjustment of the child. However, others have found that the relationship between caregiver support and child functioning after CSA is relatively weak (Bolen & Gergely, 2015; Wamser-Nanney, 2017). Additionally, researchers have found that parents’ perception of their child’s functioning mirrors their own functioning (Mangold et al., 2022), although this relationship is not present between child-reported self-functioning and parent reported self-functioning (Mangold et al., 2022). Cummings’ (2018) Protecting and Healing model of parenting post-child trauma demonstrated that parents changed their parenting practices in specific ways to focus on protecting and healing their children, often to the detriment of looking after their own well-being and needs. However, once the child began to experience recovery, post-trauma gains and wellness became possible for the parent.
We were interested in expanding this model and understanding parents’ process of centering their child’s interpersonal traumatic event post-disclosure. In other words, how it informed their understanding of themselves, their lives, and the world. This phenomenon of centering a traumatic event in one’s life is termed event centrality (Berntsen & Rubin, 2006). Still, it has yet to be applied to parents of children who have experienced trauma, despite a growing body of literature demonstrating that parents are impacted by trauma experienced by their children.
Event centrality occurs when the memory of a traumatic event becomes a reference point for understanding one’s life story, identity, and everyday experiences (Berntsen & Rubin, 2006). For people who have directly experienced trauma, it is related to negative trauma-related symptomology (e.g., PTSD and depression) and post-traumatic growth (Boals & Schuettler, 2011; Gehrt et al., 2018; Groleau et al., 2013). However, this construct has only been examined once for those indirectly exposed to trauma, in a population of children and grandchildren of Holocaust survivors (Greenblatt-Kimron et al., 2021). Nonetheless, researchers have stated that parents see their child’s trauma as informing their cognitions (e.g., about the self, others, and world) and daily life (e.g., relationships and parenting behaviors) in qualitative research (e.g., Cummings, 2018; Fuller, 2016; Kilroy et al., 2014; McElvaney & Nixon, 2020; Sparks & Stoppa, 2022), lending evidence to the claim that vicarious event centrality is possible.
We used grounded theory, a family of qualitative research methods focused on generating a theory of a human experience using a qualitative approach that is “grounded” in the data (Corbin & Strauss, 2008; B.Glaser, 1978; B. G.Glaser & Strauss, 1967; Willig, 2008). In contrast to a deductive approach (i.e., applying existing knowledge and theory to the data), an inductive approach allowed us to develop theory in areas where there is no previous research. Grounded theory can also be described as a method to develop an explanatory theory of a process from the perspective and context of those who experience it (Birks & Mills, 2015). As a result, grounded theory goes beyond the simple description of themes; it involves understanding these themes’ relationships through constant comparison and theoretical integration (Birks & Mills, 2015). The resultant grounded theory is explanatory rather than simply descriptive.
Method
Participants
This project is part of a larger program of work focused on understanding parental experiences following child trauma. As such, we used a combination of archived interviews described in Cummings (2018) and original data generation with new participants. Participants in the archived data set were collected via a combination of word of mouth, locally-placed recruitment posters, and via a professional survey company. New participants were recruited from advertisements on a university message board. Potential participants were considered eligible to participate if they: (a) were a parent/caregiver whose child had undergone an interpersonal traumatic event, (b) were not the perpetrator of that trauma, (c) the parent/caregiver was involved in the child’s life at the time of the traumatic event, (d) spoke English, (e) resided in Canada, and (f) consented to participate in the study.
Twenty-two participants were interviewed for this study. Fifteen of these participants were collected as part of Cummings’ (2018) study and seven were new participants. Of these 22 participants, 5 were excluded from the current study as they did not meet the inclusion criteria. Participants in the archived dataset were 11 primary caregivers (9 mothers, 2 fathers) of 17 victims of child interpersonal trauma (9 males, 8 females). New participants were 6 caregivers (5 maternal caregivers, 1 paternal caregiver) of 10 victims of child interpersonal trauma (5 females, 5 males). About half of the perpetrators (eight) were previous romantic partners of the caregivers. The other perpetrators were the caregiver’s stepsons, the child’s romantic partner, the child’s classmate, the caregiver’s sister and the sister’s partner, the caregiver’s daughter and the daughter’s partner, the child’s babysitter, the child’s teacher, the caregiver’s previous partner’s new partner, and the caregiver’s brother. The age of participants ranged from 35 to 75 years (average = 54.5 years). The traumatic events experienced by the participants’ children varied; they included sexual abuse/sexual assault, witnessing domestic violence, neglect/abandonment, and physical abuse/assault. Twelve participants self-identified as Caucasian (70.6%), two as Ukrainian (11.8%), one as Métis (5.9%), one as First Nations (5.9%), and one did not disclose ethnicity. Time since the trauma also varied (min = 8 months, max = 46 years). All participants were located geographically in Canada.
Procedure
This study was approved by the University of Saskatchewan Behavioural Research Ethics Board on December 14, 2019. Participants were sent the consent form via email prior to the interview. The informed consent form was verbally reviewed with participants at the start of the interview, and the interviewer answered any questions the participants had about the study. Participants explicitly provided verbal consent before continuing in the interview. Interviews in the archived dataset were conducted either face-to-face or via the phone. New interviews were conducted via phone or video-teleconference. The interview began with an open-ended prompt to gather in-depth data about the parent’s experiences with minimal influence from the interviewer: “Please tell me what this experience has been like for you, from the beginning. Tell me whatever you can about how this has been for you” (Cummings, 2018, p. 119). Consistent with theoretical sampling, we developed additional questions as more data was generated and analyzed to prompt discussion of codes and categories that arose in previous interviews. Three participants also completed follow-up interviews using the questions from the event centrality scale (Berntsen & Rubin, 2006) as a check of construct validity.
At the end of the interview, participants provided demographic information to inform description of the overall sample. Participants were also asked about their experience of the interview and were given the opportunity to discuss this experience with the interviewer. Notably, all participants described the interview as a positive experience. Lastly, participants were debriefed, thanked for their participation, and asked if they consent to be contacted for future interviews. The interviews were on average between 60 and 90 min long. All interviews were audio-recorded and transcribed verbatim. Interviews were transcribed verbatim by a third-party transcription company. A quality assurance check was completed by listening to the audio of the interview while reading the transcript, to correct any errors.
Grounded Theory Analysis
Initial (Open) Coding
As the transcripts were read line-by-line, incidents (i.e., recurring actions, characteristics, experiences, phrases, explanations, images, or sounds) were highlighted in the data and assigned an initial code (Birks & Mills, 2015). Following this initial reading, the transcripts were analyzed again to compare incident with incident (Birks & Mills, 2015; B.Glaser, 1978). This comparison of incidents led to the development of codes through the labeling of patterns of words, phrases, and other phenomena apparent in the data (Birks & Mills, 2015). Questioning the data through memo-writing further informed code development and theoretical sampling (Birks & Mills, 2015; Charmaz, 2014; B.Glaser, 1978). Codes were labeled using “gerunds”; verbs used as nouns with an “-ing” ending (i.e., action labels; Charmaz, 2014). The use of gerunds emphasized processes and relationships occurring within the data, which is essential for the development of a grounded theory (Charmaz, 2014). When possible, in vivo codes (i.e., participants’ wording) were used to describe the data to avoid researcher bias (Willig, 2008).
Focused (Selective) Coding
Initial coding continued until focused codes (i.e., categories) began to form (Birks & Mills, 2015). Focused codes were created by grouping initial codes together that reflected a similar conceptual pattern in the data (Birks & Mills, 2015). Constant comparison to question the relationships between codes resulted in the formation of our initial grounded theory (Birks & Mills, 2015). These focused codes were then used to code more interviews and continue constant comparison, producing a more refined model. Saturation was subsequently confirmed by completing a saturation check whereby each interview was reviewed for the presence of the focused codes (Morse, 2015).
Theoretical Coding and Model Completion
Theoretical coding involves adding explanatory power to model by conceptualizing how the focused codes relate to each other ( B.Glaser, 1978; B. G.Glaser & Strauss, 1967). The researcher moves from describing their findings to explaining those findings (Birks & Mills, 2015). Constant comparison was used in this stage to check the emergent theory across participants and three follow-up interviews were conducted to examine construct validity.
Nine interviews were coded before the final model was made, and 16 interviews were reviewed to check for saturation of the model.
Verification Strategies for Reliability and Validity
In qualitative research, reliability and validity (i.e., rigor) are ensured through verification strategies throughout the analysis (Morse et al., 2002). These strategies include methodological coherence (i.e., consonance between research question and method), sample appropriateness (i.e., participants are appropriate to answer the research question), iterative data collection and analysis (i.e., to know what is known and what needs to be known), theoretical thinking (i.e., open-ended question to avoid bias and constant comparison to build theoretical foundation), and theory development (i.e., literature review to inform consistency with previous knowledge; Morse et al., 2002). This study used each of these strategies to ensure reliability and validity.
Results
Overview
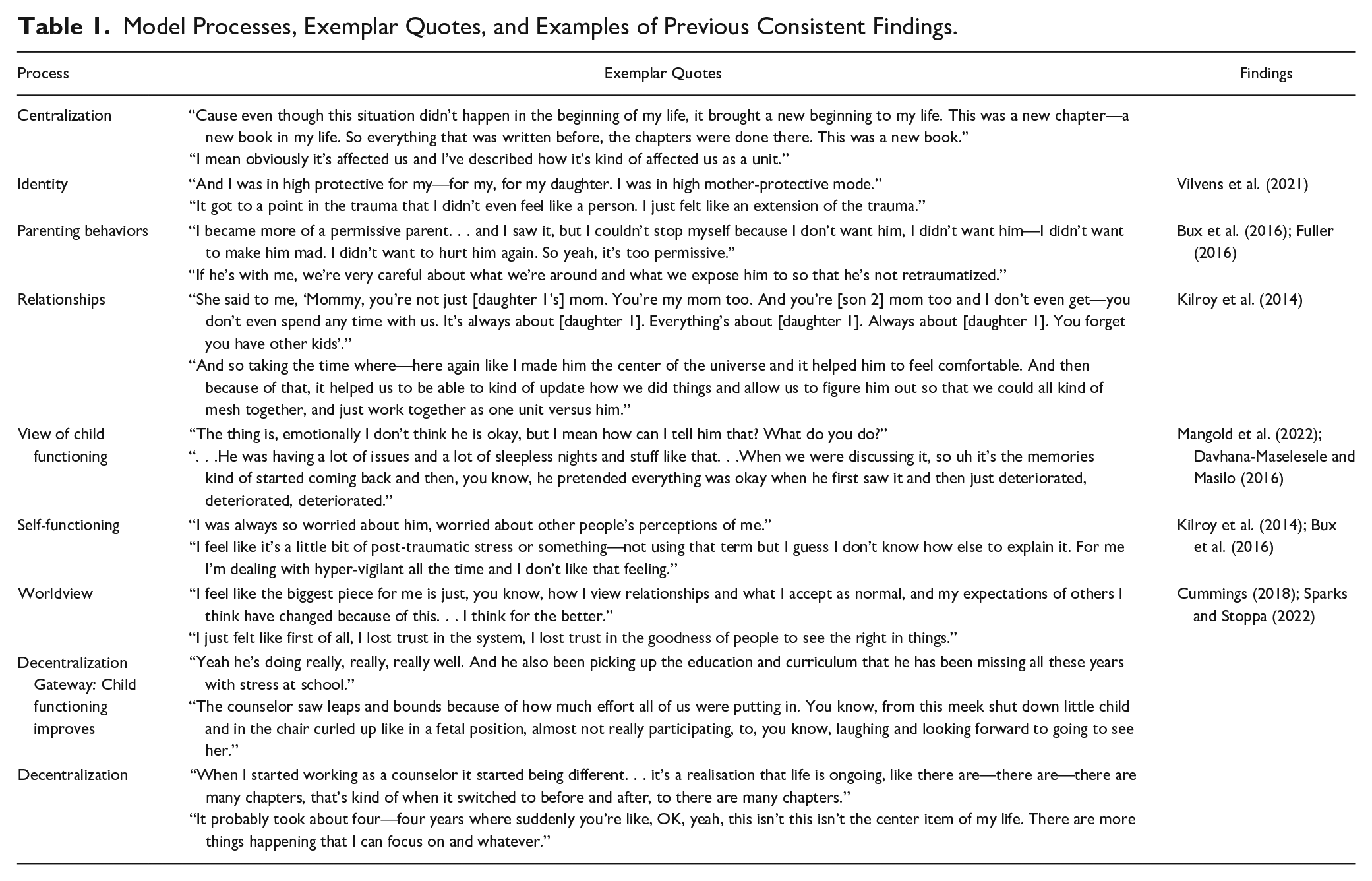
The model was labeled Vicarious Event Centralization and Decentralization, indicating that parents centralize their child’s interpersonal trauma across many areas of their life, which orients them to focusing on protecting and healing the child. After the child’s functioning improves, parents are then able to reorient to life beyond the trauma and healing the child, representing their decentralization of the trauma. The grounded theory consists of three phases, Centralization, Decentralization Gateway, and Decentralization (see Figure 1). In Phase 1, parents’ behaviors, identity, worldview, and views on the functioning of their child, themselves, and family/relationships, become informed by the child’s trauma. Phase 2 represents the gateway to decentralization. It was necessary for parents to view their child’s functioning as improved for them to begin decentralizing the trauma from their lives. Once this gate is opened, parents move forward into Phase 3, decentralization. In this phase, parents begin to focus on life beyond the trauma and start decoupling the trauma from being the main informer of their identity, behaviors, views, and relationships, although the trauma remains a piece of the parent’s life. Each process is discussed below. Exemplar quotes for each stage of our resulting model are shown in Table 1.
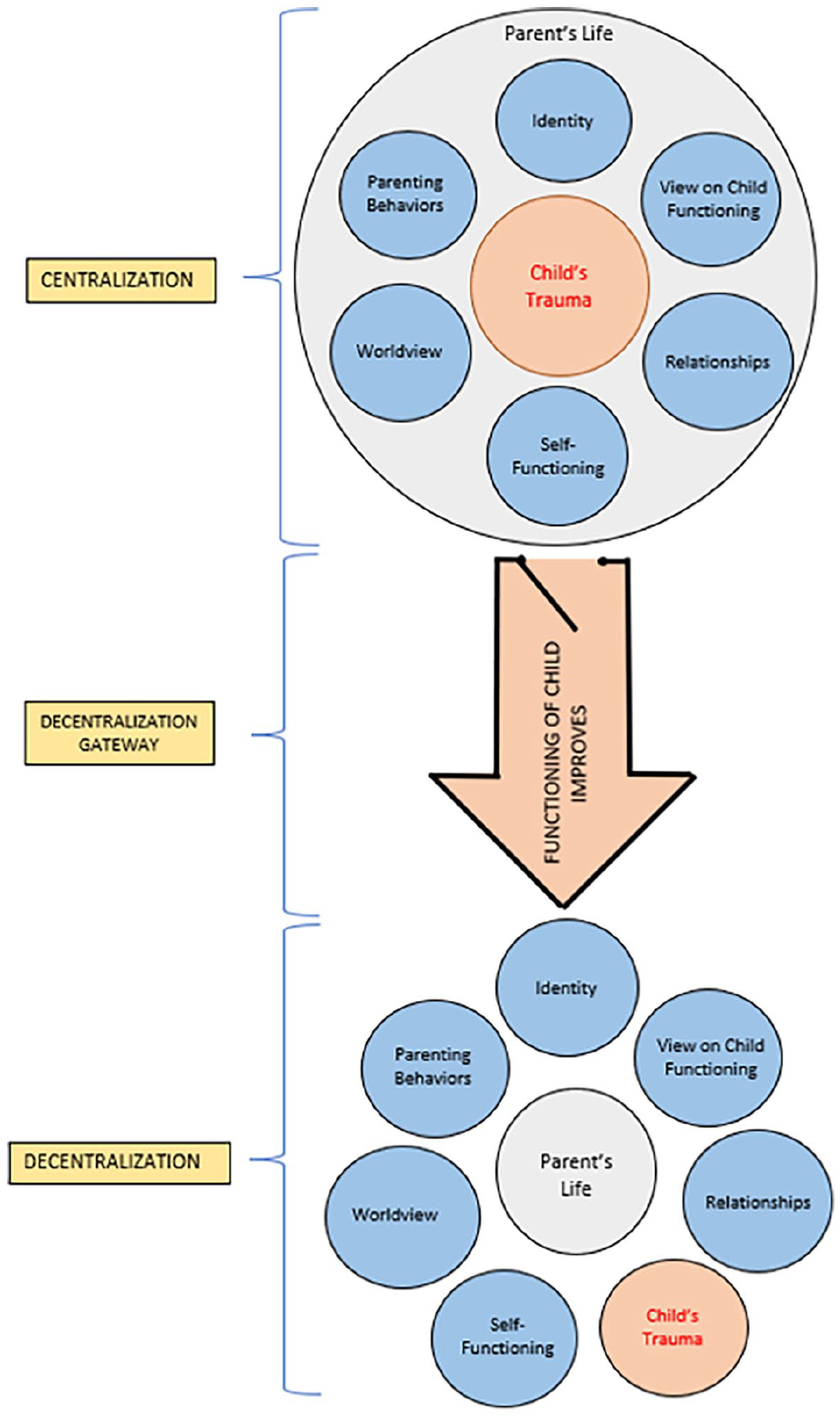
Graphical representation of the Vicarious Event Centralization and Decentralization model.
Model Processes, Exemplar Quotes, and Examples of Previous Consistent Findings.
Centralization
Upon disclosure of the trauma, parents described their lives as profoundly altered (e.g., “I’ve had to change everything because of this event.”). Parents felt as if a new chapter of their lives had begun and that there was a clear “before and after” representing pre-trauma and post-trauma life. This new beginning meant reorienting their behaviors, identity, worldview, and views on the functioning of their child, themselves, and family/relationships to integrate the trauma (e.g., “[The trauma] has informed my entire life.”). This process was seen as adaptive, in retrospect, by parents who had moved through the model, as it was a necessary step to promote their child’s healing. Essentially, centralization allowed parents to join with the child in both the hurt (e.g., “We were the victims.”) and the healing journey (e.g., “We’re going to work at this together.”) so that the child would feel validated, safe, and comforted. The trauma’s centralization in each of the areas of identity, worldview, parenting behaviors, self-functioning, view of child’s functioning, and relationships resulted in a cumulative effect of promoting the protection and healing of the child. Parents that did not centralize the trauma, but instead described “focusing forward” did not enter the model and this appeared to have negative outcomes for their family.
Identity
One of the areas where the trauma was centralized was the parent’s identity. Overall, there was a general sense from parents that the trauma informed their view of themselves (e.g., “I was a completely different person [pre-trauma].”). Parents described a range of impacts to identity. While some parents saw the trauma as informing their identity in negative ways (e.g., “I just felt like a failure.” or “I must be a shitty person.”) others saw the trauma as informing their identity in more positive ways (e.g., bringing out their identity as a protector for their child). Interestingly, parents could initially have positive and/or negative impacts to identity and still move through the model, as long as the identity was tied to an overall sense of responsibility for supporting their child’s well-being. Parents who did not feel a sense of responsibility for their child’s well-being exited the model (e.g., “Of course, I feel a great deal of guilt. But what could I do? I wasn’t going to, sort of say, break up my own marriage for the sake of this [. . . ] I felt like I had really failed as a mother.”)
Parenting Behaviors
The trauma directly influenced parenting behaviors post-trauma. Although these behaviors varied, the underlying reason for the actions remained the same: to protect the child from harm and to promote their healing. These actions ranged from changes in discipline (e.g., overcompensating, permissiveness, and consistency), communication (e.g., increased affection, sharing of emotions, and new rules about not keeping secrets), and environment (e.g., taking child out of unsafe places and relationships) to seeking services/resources for the child (e.g., counseling and child protection services) and/or themselves (e.g., their own counseling to role model or to be the best parent possible for the child). Related to identity, parents who did not feel a sense of responsibility for their child’s well-being did not see their parenting behaviors as influenced by the trauma, and thus did not move through the model.
Relationships
Parents’ relationships in terms of family, friends, and partners were reorganized by the trauma. In the area of family, parents described that the family dynamic was disrupted by the trauma (e.g., “It was just dysfunction.”) and that their relationship with the child was their priority to ensure their protection and healing (e.g., “. . .my priority has always been [child] and making sure that he’s protected.”), sometimes to the initial detriment of relationships with their partner or other children. This meant also changing relationships with close others with different views on the traumatic event, as parents perceived it would be unhelpful or unsafe for them to be around the child (“The relationships with my mom and my sister changed substantially because my view of the event and the seriousness of it. . .”). Some parents described leaning on friendships, family, and partners to discuss the traumatic event. Overall, parents who did not prioritize their relationship with their child who experienced the trauma, but instead prioritized other relationships (e.g., with the perpetrator) exited the model.
View of Child Functioning
Parents described the trauma as negatively impacting their child’s functioning (e.g., “He developed terrible anxiety. . .”). Parents described seeing the child’s negative emotions, behaviors, interactions, and general mental health as being related to the trauma. Again, this served a purpose for parents. Viewing the child as affected by the trauma indicated to parents that they needed to focus on protecting and healing the child. Parents who perceived that their child was not affected by the trauma did not enter the model.
Self-Functioning
Parents own functioning was also informed by the child’s trauma. Post-trauma disclosure, parents described the trauma as influencing their overall well-being, including their mental health and coping behaviors (e.g., “I was always so worried about him, worried about other people’s perceptions of me” and “I did a lot of drugs.”). For example, parents discussed feelings of stress, hypervigilance, depression, sleep difficulties, and worries. Parents coped with these negative impacts to mental health in a range of negative and positive ways, including isolating, using drugs and alcohol, support services, talking with close others, and self-talk. Despite centralizing the trauma, parents described prioritizing improving their child’s functioning above their own. For those that additionally prioritized their own functioning, it remained in service of the child’s functioning (“I really had to make sure that I stayed healthy for [child]. And so I had to make sure that my mental state and her mental state was okay. Otherwise, you know, how is she going to survive if I can’t survive it?”).
Worldview
Post-disclosure, parents described the trauma as being a reference point for their beliefs and expectations about the world around them. These worldviews varied from beliefs about morality (e.g., what is right and wrong), people (e.g., perpetrator, close others, and professionals), systems (e.g., school and protective services), and safety (e.g., not expecting this to happen to their child). Overall, parents experienced themselves as seeing the world differently. These worldviews served parents to anticipate the environments, people, and systems that could be beneficial or detrimental to their child’s healing. However, it also contributed to the hypervigilance, overprotectiveness, and stress felt by the parents.
Gateway to Decentralization: Child Functioning Improves
For parents to have the opportunity to decentralize the child’s trauma from their lives, they had to perceive their child’s functioning as improving (e.g., “She’s now doing really good. She’s in university. She’s—she’s got a good life.”). This was illustrated by positive statements on their child’s well-being, behaviors, emotions, and interactions. In essence, this is the moment that the purpose of centralization is achieved.
Decentralization
Once parents felt that their child’s functioning had improved, decentralization became possible for parents. This process exists on a spectrum and was ongoing for most participants. During this phase parents begin to focus on life beyond the trauma. For example, their identity, behaviors, views, functioning, and relationships become informed by other experiences, although the trauma remains a piece of the parent’s life. In other words, the trauma is no longer central to the parent’s life. Indicators of decentralization were represented by a defocusing of the trauma in any of the areas of centralization (e.g., self-functioning, relationships, identity, etc.).
Discussion
The purpose of our study was to understand parents’ experience of centering their child’s interpersonal traumatic event in their lives post-disclosure. The resulting model of vicarious event centrality is the first to illustrate how and why the traumatic event informed parents’ lives post-disclosure. Moreover, it is only the second study to document vicarious event centrality. We expanded upon Cummings’ (2018) Protecting and Healing theory by understanding how the trauma informed parents’ lives beyond their parenting strategies. Through the three phases of Centralization, Decentralization Gateway, and Decentralization, the child’s interpersonal traumatic event moved from being the main informer of parents’ identity, functioning, worldview, parenting behaviors, relationships, and view of their child’s functioning, to one of many experiences that informed parents’ lives. Consistent with the Protecting and Healing theory, centralization aided in protecting and healing the child, and decentralization only became possible once healing was perceived to have occurred for the child (i.e., Decentralization Gateway). Descriptively, the domains of parents’ lives informed by the traumatic event (e.g., identity and worldviews) have overlapped with previous research on caregivers of child survivors (see Table 1).
Vicarious Event Centrality
Developed with direct trauma survivors, Berntsen and Rubin (2006) described that a traumatic experience can be a momentous event that subsequently influences identity, lifestory, and everyday experiences for the survivor. Berntsen and Rubin (2006) conceptualized event centrality through the lens of autobiographical memory; specifically, the salience of the traumatic event in autobiographical memory makes it an easily accessible reference point for understanding oneself, the world, and daily life. Similar to Berntsen and Rubin’s (2006) finding in direct trauma survivors, our study found that the trauma became central to the cognitive organization of the life and identity of the parent post-disclosure. More precisely, parents saw their child’s trauma as a turning point in their lifestory that informed their views on themselves (e.g., identity, behaviors, and functioning), others (e.g., relationships and child functioning), and the world. Considering parents were not direct survivors of the trauma, they only had an episodic memory of the disclosure rather than the traumatic event itself. Nonetheless, our study illustrates that a loved one’s traumatic event can become a salient autobiographical memory in one’s own lifestory, supporting previous research that event centrality can occur for loved ones indirectly exposed to a traumatic event (Greenblatt-Kimron et al., 2021).
Our study is the first to examine event centrality in a population of parents exposed to their child’s interpersonal trauma. Despite researchers previously finding that parents’ beliefs, relationships, and behaviors were influenced by their child’s experience of trauma (e.g., Cummings, 2018; Fuller, 2016; Kilroy et al., 2014; McElvaney & Nixon, 2020; Sparks & Stoppa, 2022), the term event centrality was not used. One possible explanation is that the construct of event centrality was not referenced in previous research in parents due to the researchers’ theoretical sensitivity to the construct (Birks & Mills, 2015). To make this construct more explicit in research, we suggest that future researchers in this area use the term vicarious event centrality. It is hoped that by doing so, researchers in the vicarious trauma area become attuned to the potential applicability of this construct to their research.
Berntsen and Rubin (2006) focus on the idea that the centering a traumatic memory in the life script is maladaptive, and subsequent research has supported an association between event centrality and negative mental health (Gehrt et al., 2018). This present study does not debate this finding, as parents relayed that their child’s trauma negatively impacted their own functioning (e.g., hypervigilance and worries). However, similar to research illustrating that event centrality is related to both PTSD and post-traumatic growth (Boals & Schuettler, 2011; Groleau et al., 2013; Schuettler & Boals, 2011), parents in our study retrospectively communicated that centering their lives around the child’s trauma was also adaptive. They found that this promoted their child’s recovery, which subsequently allowed for parents to decentralize the trauma from their own lives. An understanding of the adaptiveness of event centrality in helping parents focus on child recovery is presented below in the context of cognitive-constructive and attachment theories of trauma.
Cognitive-constructive theories of trauma suggest that individuals construct their reality based on the meaning they have extrapolated from events (McCann et al., 1988). For instance, accommodation describes how new experiences can result in changes to existing schemas (i.e., beliefs) to accommodate the new information (Payne et al., 2007). Thus, when events are traumatic, this can alter the framework of one’s beliefs about the world, self, and others (i.e., schemas) which subsequently impacts functioning (McCann et al., 1988). Our study supports that parents’ schemas about the self, others, and the world are informed by their child’s trauma, and that this can contribute to negative functioning (e.g., hypervigilance). Conversely, these schematic changes may serve a protective function through helping parents adapt their lives accordingly to protect and heal their child. For example, since they believed that their child’s functioning was negatively impacted by the trauma, parents tailored their parenting behaviors to promote the child’s healing. This supports previous researchers who found that caregivers who did not access mental health support for their child after CSA were those who believed this support was not necessary because they did not perceive their child as exhibiting behavioral symptoms (Fong et al., 2016). Thus, our study continues to add to the research base that illustrates that event centrality may be both maladaptive and adaptive.
Another possible explanation for the adaptiveness of event centrality comes from attachment theory. From an attachment theory lens, a child’s well-being is related to having a secure attachment with its primary caregivers (Bowlby, 1988; Lieberman, 2004; Malik et al., 2021). A secure attachment is achieved through the parent being consistently responsive and available to the child’s needs, which enables the child to internalize that they are loveable, safe, supported, and capable to interact with the others and the world (Bolen, 2000; Bowlby, 1988). Although attachment was not examined in this study, centering the trauma may have allowed parents to adaptively reorganize their lives to prioritize and respond to their child’s needs, promoting a secure attachment and subsequent healing. In fact, Cummings (2018) noted that one of the positive outcomes of parents focusing their parenting behaviors on protecting and healing the child from a trauma was an increase in the level of communication, intimacy, and support amongst family members, perhaps illustrating that a secure attachment was achieved. It may be helpful for future research to further understand the relationship between vicarious event centrality and attachment.
Protecting and Healing Theory
This study expanded upon Cummings’ (2018) Protecting and Healing theory by adding the understanding of how and why the child’s trauma informed parents’ lives beyond their parenting strategies. There are overlaps between our model of Vicarious Event Centralization and Decentralization and the Protecting and Healing theory that warrant further discussion.
Cummings (2018) found that during the phase of destabilization, parents’ expectations of the world, self, and others were altered by the trauma disclosure, which prompted parents’ lives to become exclusively focused on the trauma and on protecting and healing the child through various parenting behaviors (e.g., searching for the right thing to do and padding the child). Given our results, vicarious event centrality provides a helpful lens through which to view this destabilization. That is, our results add theoretical sensitivity to this model and demonstrate how parents’ experiences of destabilization can be explained by vicarious event centralization.
In the phase Recalibration, Cummings (2018) found that parents reached a tipping point where their efforts to protect and heal the child began to take effect. Parents regained stability by increasing attention to life beyond the trauma. This tipping point subprocess described in Recalibration parallels our Decentralization Gateway. The Decentralization process in this current study may also add to the understanding of the regaining stability subprocess described in Cummings (2018). Not only did parents start to focus on life outside of the trauma (e.g., regaining stability), but our study illustrates that parents then used these experiences to inform their behaviors, functioning, relationships, identity, and worldview. In other words, the trauma moved from being the main informer of their lives to one of the many experiences that informed their understanding of themselves, daily life, others, and the world.
In the Protecting and Healing theory, the final phase, Stabilization, is represented by experiencing thriving recovery whereby parents experience post-traumatic growth in the areas of familial intimacy, communication, emotional intelligence, and support. Based on the conceptual overlap between our Decentralization phase and the subprocess of Cummings (2018) regaining stability, it appears that parents must be at least in the process of decentering the trauma from their lives in order to reach thriving recovery. Future research would benefit from understanding how centralization and decentralization is related to post-traumatic gains in wellness and growth.
Implications
There are several practical implications from the Centralization and Decentralization model that can help inform service providers working with families who have experienced trauma. First, this study supports that parents are affected by their child’s trauma and thus require unique services to address their needs. Previous researchers have found that parents of CSA survivors highlight mental health services as necessary to help them cope with their experiences (Fong et al., 2020; Van Toledo & Seymour, 2016). However, parents continue to experience multiple barriers to such services (e.g., financial, personal, and accessibility barriers; Van Teldo & Seymour, 2016). Thus, this study supports that there must be a continued effort to remove barriers for parents’ access to services. Furthermore, our study can help mental health professionals validate the variety of ways that trauma has come to influence parents’ lives.
Second, the Vicarious Event Centralization and Decentralization model helps practitioners to understand the post-trauma experience for parents and target areas likely to increase recovery. For example, Cummings (2018) notes that practitioners might be too quick to ease client suffering, undermining the necessary experience of destabilization for recovery. Similarly, our study illustrates that parents centering the trauma in their lives may be an adaptive mechanism that promotes child recovery, which in turn allows parents to begin to decentralize the trauma and to move toward thriving recovery (Cummings, 2018). Recently, researchers have tested interventions aimed at decentering a traumatic event to ameliorate symptoms of PTSD (e.g., Boals & Murrell, 2016); however, these studies were performed with direct survivors of trauma. This current study illustrates that parents’ experiences of centralization are uniquely important to foster the child’s healing, and thus the aforementioned benefit of decentering a traumatic event for direct survivors may not generalize to parents who were vicariously traumatized. Nonetheless, it is possible that once the child has begun to recover, it would be helpful for the clinician to aid in decentering the trauma.
Third, an important target for intervention with parents may be those who have centralized the child’s trauma but have become stuck in this phase as they continue to perceive that their child is not recovering. It is unclear at this point whether this accurately represents the child’s functioning, as we only collected data from parents themselves. Therefore, it may be the case that parents may need help with attending to indicators of well-being in their child. For example, previous researchers have illustrated that parents’ report of their child’s PTSD symptomology paralleled their self-reported secondary traumatization symptomology, but that this relationship was not present when comparing their symptomology to their child’s report of PTSD symptomology (Mangold et al., 2022). Nonetheless, if it is the case that the child continues to not show any recovery despite parental centralization, it may be an indicator for the family to receive services to promote the child’s recovery.
Future Directions
From a research perspective, the high prevalence rate of children who experience trauma and the potential for negative outcomes for the child and parent necessitates further research in this area (Cyr et al., 2016, 2018; Finkelhor et al., 2013; Hailes et al., 2019; Norman et al., 2012). As previously discussed, this is the first study to examine vicarious event centrality in parents of child interpersonal trauma victims. Thus, future research would benefit from examining this construct using a quantitative or mixed-methods approach, to determine exactly how parents perform on measures of event centrality (Berntsen & Rubin, 2006). Furthermore, this may then suggest a need to tailor the measure for vicarious experiences and to examine its psychometric properties. As well, exploring event centrality in other vicariously traumatized populations (e.g., spouses, siblings, friends, and professionals) would be helpful to expand the foundation of research on vicarious event centrality. Furthermore, the aim of this study was not to directly explore how the experience of vicarious event centrality related to post-traumatic growth; however, based on previous research illustrating that event centrality is related to post-traumatic growth (e.g., Groleau et al., 2013) and that post-traumatic growth can occur for parents of child interpersonal trauma victims (Cummings, 2018), further understanding of this relationship is warranted. Both the Protecting and Healing model and our model presented here examined parental experiences stemming from a range of trauma types. While this demonstrates the commonality of parental experiences across forms of child trauma, future research might benefit from more homogeneity.
Limitations
One limitation of this study is that most participants identified as Caucasian; hence, the applicability of this model to ethnically and racially diverse populations should be considered with caution (Alegria et al., 2010). Second, the children who were victimized did not take part in this study; in other words, we did not collect data on the child’s experience post-trauma. Consequently, the Decentralization Gateway currently represents the perception by parents that their child has started to recover without data on the child’s self-reported recovery. Furthermore, examining the relationships between vicarious event centrality, traumatization, and growth was beyond the scope of this study. Currently, there is debate about the directionality of the relationship between event centrality and traumatization (e.g., Berntsen & Rubin, 2006; Greenblatt-Kimron et al., 2021) and about how event centrality is related to both PTSD and post-traumatic growth (e.g., Gehrt et al., 2018; Groleau et al., 2013). Researchers examining these three constructs would help to understand these relationships and be the first to do so in a sample of vicariously exposed parents. Lastly, participants willingly volunteered to participate in our study and may differ from those who did not volunteer (Robinson, 2014).
Conclusion
This study is the first to illustrate that parents centralize their child’s trauma in a myriad of ways post-disclosure and that this process may adaptively promote the child’s protection and healing. We found that decentralization of the trauma for parents was uniquely tied to their child’s recovery, similar to findings that parents can only access post-traumatic gains and growth once their child has experienced recovery (Cummings, 2018). This model provides a framework for future research to continue to examine vicarious event centrality in this population and how it may relate to post-trauma experiences of traumatization and recovery. Furthermore, it may help health professionals validate parental experiences of centering their child’s trauma in their lives.
Footnotes
Author Note
This work was completed as part of the doctoral dissertation of Whitney Willcott-Benoit.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by funding from the Centre for Forensic Behavioral Sciences and Justice Studies at the University of Saskatchewan and the Social Sciences and Humanities Research Council of Canada, awarded to the first author, as well as funding from the Centre for Forensic Behavioral Science and Justice Studies awarded to the second author.