
Abstract
Despite the well-documented link between child maltreatment (CM) and mental health, evidence suggests substantial variability in the post-traumatic sequelae of CM across cultures. The perceived acceptability of CM in one’s community might moderate the association between CM and mental health, but little research has been conducted on it so far. This study examined how the perceived acceptability of CM may influence the relationship between CM experiences and post-traumatic symptoms in individuals from four different continents and if the pattern of associations is the same across countries. We recruited a sample of 478 adults from Cameroon (n = 111), Canada (n = 137), Japan (n = 108), and Germany (n = 122). We administered online questionnaires and performed multiple group moderation analyses for total CM, neglect, physical abuse, emotional maltreatment, sexual abuse, and exposure to domestic violence (DV). A significant positive main effect of CM on post-traumatic symptoms was found in the overall sample and in Cameroon; in Germany, only neglect and emotional maltreatment were positively associated to post-traumatic symptoms. Moderation effects were identified; the perceived acceptability of neglect in Cameroon and Germany and of exposure to DV in Cameroon had a dampening effect on the relationship between CM experiences and post-traumatic symptoms. Our findings confirm that CM experiences entail long-term post-traumatic sequelae that can vary across cultures and CM subtypes and further our understanding of this issue by showing that the perceived acceptability of CM may be an understudied moderator.
Keywords
Introduction
Child maltreatment (CM), which includes physical abuse, sexual abuse, emotional maltreatment, neglect, and exposure to domestic violence (DV), is a global problem concerning over 25% of children around the world (García-Mollá et al., 2023). There is a well-documented link between CM and health, such as poor physical and mental health outcomes (Brown et al., 2022), a heightened risk of psychiatric disorders (Wong et al., 2022), and impaired social functioning (Pfaltz et al., 2022). However, evidence suggests substantial variability in the post-traumatic reactions associated with CM across cultures (Balsam et al., 2010; Mbagaya et al., 2013; Sebre et al., 2004; Shrestha et al., 2019). Recent research has focused on factors that may explain this variation. Some researchers emphasize that CM experiences are perceived differently across cultures (Moody et al., 2018; Wadji et al., 2023) and that this may impact post-traumatic adjustment. Beliefs about the social acceptability of certain parenting practices that may be considered CM may not only increase the likelihood of CM (Ganz et al., 2020; Klika et al., 2019) but also shape the meaning attributed to CM with consequences on adjustment (Deater-Deckard & Dodge, 1997). Drawing on the person-process-context-time model (Bronfenbrenner & Morris, 2006) within a developmental psychopathology perspective (Cicchetti & Toth, 1995) the mechanisms by which CM is associated with mental health can only be unraveled by considering the entanglement between the cultural context specificities and the individual attributes. CM survivors will likely integrate their own perception of what their community of reference considers acceptable in their appraisal of CM experiences, and this might affect mental health outcomes. However, very little work has been conducted on the perceived acceptability of CM as a factor that can moderate the association between CM and post-traumatic symptoms (Landsford et al., 2005). The current study aims to address this gap in the literature by examining how perceived acceptability of CM can moderate the relationship between CM experiences and post-traumatic symptoms in adults from four different continents.
Cultural Considerations in the Understanding of CM and Post-Traumatic Symptoms
Culture is a set of beliefs, attitudes, values, and standards of behavior shared within the confines of a country (Kolhatkar & Berkowitz, 2014; Taras et al., 2016). Culture influences how parents care for children and what parenting behaviors they consider acceptable (Bornstein, 2013). Consequently, there are substantial cultural differences across countries in child-rearing practices and beliefs (Raman & Hodes, 2012; Westby, 2007). For example, studies have pointed out that while in Cameroon child-rearing is considered a community task that emphasizes the values of obedience, respect for authority, and conformity to collectivity, in Germany it intensively relies on parents and aims at promoting the child’s self-determination, unicity, and assertive skills (Keller et al., 2005; Mugadza et al., 2019; Walper & Kreyenfeld, 2022). Additionally, while in Canada child-rearing practices emphasize children’s autonomy (Liu et al., 2005), in Japan they foster children’s dependence on indulgent care of their mother and moral rectitude, affected by the Confucian ideology (Nagase & Holloway, 2022).
Cultural values and practices also play important roles in shaping the definition and interpretation of CM. For example, behaviors that are considered harmful and neglectful in some Western countries, like the use of physical punishment or leaving infants and toddlers in the care of young siblings, may be considered acceptable elsewhere, in particular in Sub-Saharan Africa and South Asia (Pace et al., 2019; Ruiz-Casares et al., 2018). In addition, some cultures may be very permissive with children and place few demands on them, while others may sanction harsh disciplinary measures to control children. For example, in some Asian and African countries, it is a widespread practice to punish children’s misbehaviors by having them kneel on painful materials, like uncooked rice or gravel (Westby, 2007).
The experience and manifestation of trauma symptoms are also influenced by an individual’s social and cultural background (Schnyder et al., 2016). Culture can shape the subjective meaning of trauma, and this, in turn, can influence symptom expression as well as the magnitude of the impact of trauma on individuals (Harris et al., 2010). For example, a previous study that investigated the prevalence and psychopathological consequences of child physical abuse and neglect in Kenya, Zambia, and the Netherlands found, among other results, that post-traumatic symptoms mediated the relationship between physical abuse and other psychopathological sequelae (i.e., criminal tendencies, depressive symptoms, and borderline personality symptoms) in the Netherlands and in Kenya, while they did not mediate the relationship between neglect and other psychopathological sequelae in Kenya and Zambia (Mbagaya et al., 2013). The authors attributed this difference to the social norms endorsed by the participants from African countries, where widespread poverty may lead to interpret neglectful behaviors as being more normative, and hence less traumatic than in the Netherlands (Mbagaya et al., 2013). Taking culture into account is therefore important, as countries across the globe vary widely in their conceptualization of CM and trauma symptoms.
Perceived Acceptability of CM, CM Experiences, and Post-Traumatic Symptoms
Social norms indicate the mainstream attitudes, behaviors, and expectations that define the standards of acceptability shared within a community and ultimately shape the way people act (Xenitidou & Edmonds, 2014). Acceptability of CM is a strong predictor of CM perpetration (Bensley et al., 2004; Taylor et al., 2011). Thus, an important consequence of perceiving CM as acceptable is the heightened risk of engaging in maltreating parenting practices (Dempsey et al., 2018). Klika et al. (2019) provide a clear distinction between actual norms (i.e., behaviors and attitudes held by a majority of people in a community or group) and perceived norms (i.e., an individual’s perceptions of the beliefs, values, attitudes and/or behaviors within their community).
Few studies have examined cross-cultural differences in the association between perceived norms toward CM and psychological adjustment following CM experiences. The available literature mainly focuses on physical discipline and harsh punishment (Deater-Deckard & Dodge, 1997; Lansford et al., 2005, 2014). For example, Deater-Deckard and Dodge (1997) suggested that cultural normativeness (i.e., the extent to which a certain practice is considered acceptable in a culture) alters the meaning that children attribute to physical discipline, which in turn mediates their psychological adjustment. In a longitudinal study including six countries, Lansford et al. (2005) found that the reported normativeness of physical discipline differed across countries and that frequent use of physical discipline was less strongly associated with a child’s aggression and anxiety in conditions of greater perceived normativeness. The authors interpreted these findings in light of Rohner’s Parental Acceptance-Rejection Theory, now known as the Interpersonal Acceptance-Rejection Theory (Rohner, 2021). This theory posits that children’s psychological adjustment depends on their perceptions of their attachment figures’ acceptance or rejection. However, it should be noted that when more severe forms of physical abuse have been considered together with physical discipline, physical abuse was found to have even more detrimental effects on participants from cultural backgrounds more lenient toward CM (Lansford et al., 2002). Despite evidence suggesting that the normative cultural context in which CM takes place and its perceived acceptability can affect the strength or direction of the relationship between CM and post-traumatic symptoms (Deater-Deckard & Dodge, 1997; Lansford et al., 2005; Rohner, 2021), to date, little research has examined whether perceived norms toward CM (henceforth, perceived acceptability of CM) moderates the association between a variety of CM experiences and post-traumatic symptoms, and if the effect is the same across cultures and CM subtypes.
The Present Study
In the current study, adult samples were recruited from Cameroon, Canada, Japan, and Germany (i.e., four countries representing different continents, cultures, living standards, and gross national income) to examine cross-culturally: (a) the association between CM experiences and post-traumatic symptoms; and (b) if the perceived acceptability of CM and its several subtypes moderate the associations between experiences of CM and post-traumatic symptoms. In line with past studies (Lansford et al., 2005) and Rohner’s Acceptance-Rejection Theory (Rohner, 2021), we expect that (a) the experience of CM will be associated with trauma-related symptoms and that (b) perceived acceptability of CM will exert a moderating effect on this relationship. Also, we expect that (c) the main effects and moderation patterns will vary across cultures and CM subtypes.
Methods
Participants
Participants were recruited online across Cameroon (n = 111), Canada (n = 137), Japan (n = 108), and Germany (n = 122). Inclusion criteria consisted of being above 18 years of age and residing in one of the target countries. A final sample of 478 adults (from 18 to 84 years old, M = 37.42, SD = 13.88) participated in the study.
Procedure
In Cameroon, Canada, and Germany, ads were posted on social media (Facebook, Instagram, and LinkedIn) and circulated across the personal and professional networks of the investigators. Participation was further incentivized with a reimbursement of 10 CHF for internet expenses in Cameroon and with two prize draws of $ 50 CAD each (and the equivalent in €) in Canada and Germany. In Japan, both a panel survey through a survey company and a snowball sampling through flyers distributed in several physical locations (e.g., hospitals and universities) were conducted. No incentive strategy was adopted in Japan in line with local ethical guidelines. Data was collected anonymously online using Qualtrics. Participants were given the chance to choose the language they felt the most comfortable with, among English, French, German, and Japanese. At first, participants had to confirm their adherence to the inclusion criteria and provide their e-consent. They were informed about free local psychological support helplines to contact in case of psychological distress evoked by the survey. These procedures were approved by the Institutional Research Ethics Boards of all institutions involved. The study was part of a research subtheme aimed at identifying the socioemotional consequences of CM, implemented within the Global Collaboration on Traumatic Stress, a network of researchers and clinicians working together worldwide on topics related to traumatic stress.
Instruments
Sociodemographic Information
The sociodemographic questionnaire consisted of twelve items documenting age, gender, relational status, number of children, ethnicity, education, occupation, and physical disabilities.
CM Experiences
Experiences of CM were assessed through a composite self-report measure made of 24 items derived from three questionnaires, introduced by the prompt “Before the age of 18, have you ever experienced one of the following…” Experiences of neglect were documented through five yes/no items from the ISPCAN Child Abuse Screening Tool (Dunne et al., 2009; Zolotor et al., 2009). An example of an item is, “Were you made to wear clothes that were dirty, torn, or inappropriate for the season when your parent(s) or caretaker(s) could afford otherwise?.” One point was attributed to all affirmative answers (range = 0–5; α = .68 in the current sample). The Early Trauma Inventory Self-Report-Short Form (Bremner, et al., 2007) was used to assess physical abuse (five yes/no items, score range = 0–5), emotional maltreatment (five yes/no items, score range = 0–5), and sexual abuse (six yes/no items, score range = 0–6). Examples of items are “Were you ever slapped in the face with an open hand by a parent or caregiver?” (physical abuse), “Were you often put down or ridiculed by a parent or caregiver?” (emotional maltreatment), “Were you ever touched in an intimate or private part of your body (ex. breast, thigh, genitals) in a way that surprised you or made you feel uncomfortable?” (sexual abuse). Internal consistencies of these subscales ranged from α = .73 to .85. A three-item adaptation of the Revised Conflict Tactics Scales 2 (CTS2) (Straus et al., 1996) was used to assess exposure to DV. An example of an item is “Prior to your 18th birthday, was your parent or step-parent sometimes, often, or very often kicked, bitten, hit with a fist, or hit with something hard?.” Scores ranged from 0 to 3 (α = .89). In addition to sum scores for each subscale, a total sum score inclusive of all CM subtypes was calculated (range from 0 to 24; α = .88). Existing translations were used for all items assessing CM experiences.
Perceived Acceptability of CM
Twenty-four items about perceived acceptability of CM were derived from the instruments used to assess CM experiences and back-translated into French, German, and Japanese. Participants were asked to rate on a five-point Likert scale (1 = never acceptable to 5 = always acceptable) how acceptable would most people in their community find a variety of behaviors that may be considered as neglect, physical abuse, emotional maltreatment, sexual abuse, and exposure to DV. Examples of items are “When caregivers can afford it, how acceptable is it that children have to wear clothes that are dirty, torn, or inappropriate for the season?” (neglect), “. . .Children are being slapped in the face with an open hand by a parent or caregiver?” (physical abuse), or “. . .Children are being put down or ridiculed by a parent or caregiver?” (emotional maltreatment). A mean score (range 1–5) was calculated for each subtype of CM and for the totality of CM behaviors (henceforth, total CM). Lower scores indicated lower levels of perceived acceptability of CM. The Cronbach’s alphas ranged from .84 to .96.
Post-Traumatic Symptoms
The presence of post-traumatic symptoms was assessed with the Global Psychotrauma Screen (GPS; Olff, 2020), available in the four languages of the study. The GPS is made of 22 yes/no items designed to identify trauma symptoms following potentially traumatic experiences (GPS symptoms subscale: 17 items), and the protective factors influencing the course of symptoms (GPS risk and protective factors subscale: 5 items). Items are introduced by the prompt: “please think about the event or experience that currently affects you the most,” followed by two items specifying when it occurred (ranging from “last month” to “when I was a child or below 18 years of age”) and which nature(s) better characterize it (i.e., physical violence, sexual violence, emotional abuse, serious injury, life-threatening event, sudden death of a loved one, coronavirus, either personally experienced or happened to someone else). The present study will focus only on the 17 items of the GPS symptoms subscale, which explores a variety of symptom domains within the past month, including classic post-traumatic stress disorder (PTSD) symptoms (e.g., re-experiencing, avoidance, arousal), disturbances in self-organization as part of complex PTSD, anxiety, depression, sleep problems, self-harm, dissociation, other physical, emotional, or social problems and substance abuse. An example of an item is “in the past month, have you had nightmares about the past traumatic life event(s) you have experienced or thought about the event(s) when you did not want to?.” One point was attributed to every positive answer and summed up in a total score ranging from 0 to 17, with higher scores suggesting higher overall symptomology. Preliminary studies suggest a GPS symptom score of 8 as a sensitive cut-off for probable PTSD (Frewen et al., 2021). The Cronbach’s alpha of the GPS symptoms subscale in the current sample was .91.
Data Analyses
Preliminary descriptive and correlational analyses were conducted with IBM SPSS Statistics, version 27.0 (IBM Corp. Released 2020). Spearman’s rho test was used to calculate the correlation coefficients since most of the variables did not have a normal distribution. Listwise deletion was applied in case of missing data.
Moderation analysis and multiple group moderation analyses were conducted with the statistical software MPlus, version 8.8 (Muthén & Muthén, 2017). The Full Information Maximum Likelihood procedure was used to deal with missing data. The moderation effect of the perceived acceptability of CM on the relation between CM experiences and post-traumatic symptoms was examined for total CM behaviors first and then for each subtype of CM. The effect of age, gender, and year of education was controlled for. First, we tested the moderation in the complete sample; then, we conducted multiple group moderation analyses to examine whether any differences in the models were observable depending on the country of residence. Provided that variables were mostly non-normally distributed, the MLR estimator option was privileged for maximum likelihood estimation with robust standard errors. Since the assumption of multivariate normality was not met and provided the large sample size, the chi-square test of model fit has not been reported, and incremental indices of model fit have been used (Bentler & Bonnet, 1980; Hooper et al., 2008). The absolute index Root Mean Square Error of Approximation (RMSEA) has been reported in the following sections. Graphs were plotted with IBM SPSS statistics version 27.
Results
Sociodemographic Characteristics
The sociodemographic characteristics by country and for the complete sample are reported in Table 1. Participants differed significantly across countries for all the sociodemographic variables. Pairwise comparisons highlighted that the mean age in Germany was significantly lower than in the other three countries, while in Japan it was significantly higher. Canada and Germany had a higher percentage of female respondents as compared to Cameroon and Japan, where the percentage of female and male respondents was not significantly different.
Sociodemographic Characteristics of the Participants of the Four Target Countries and of the Complete Sample.

Note. SD = standard deviation.
The value refers to the Pearson chi-square test conducted on categorical variables.
Descriptive Statistics
Descriptive statistics for the four countries and the complete sample are shown in Table 2. Overall, 77.8% of the complete sample reported experiencing at least one form of CM. Participants reported having been exposed at an average of 4.74 (SD = 4.74) maltreating behaviors during their childhood over the 24 forms of ill-treatment that were assessed by the questionnaires. The most reported subtype of CM was physical abuse (61.0%), followed by emotional maltreatment (56.2%), neglect (43.0%), sexual abuse (24.4%), and exposure to DV (17.1%). Overall, the total perceived acceptability of CM behaviors was relatively low (M = 1.39; SD = 0.54; i.e., between almost never acceptable to sometimes acceptable). Details on the perceived acceptability of each subtype of CM are reported in Table 2. Participants responded to the GPS by reporting to a similar extent events that occurred within the last year (33.8%), more than a year earlier (33.6%), and in childhood (32.7%). Seventy-six percent of the participants reported suffering from at least one post-traumatic symptom, with a mean score of 5.46 (SD = 4.86). Correlation coefficients in the complete sample and by country are reported in the supplementary material.
Descriptive Statistics for CM Experiences, Perceived Acceptability of CM and Post-Traumatic Symptoms in the Four Target Countries and in the Complete Sample.
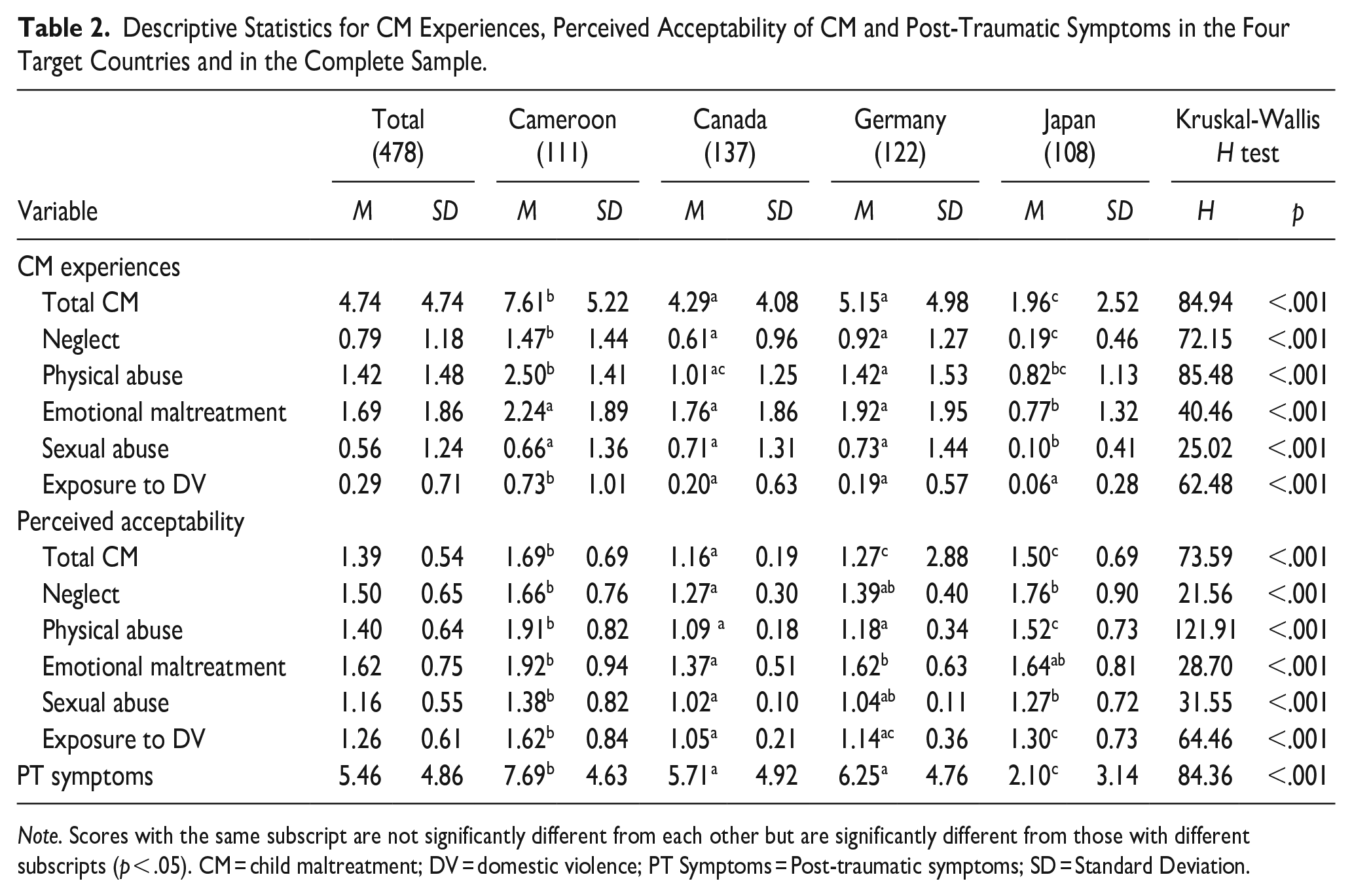
Note. Scores with the same subscript are not significantly different from each other but are significantly different from those with different subscripts (p < .05). CM = child maltreatment; DV = domestic violence; PT Symptoms = Post-traumatic symptoms; SD = Standard Deviation.
Moderation Analysis
When fitting the moderation models for the complete sample and the multigroup moderation models across countries, the incremental indices of fit were satisfactory for total CM (complete sample: RMSEA = 0.06; TLI = 0.94; multiple groups: RMSEA = 0.04; TLI = 0.96), emotional maltreatment (complete sample: RMSEA = 0.04; TLI = 0.98; multiple groups: RMSEA = 0.01; TLI = 0.99), and exposure to DV (complete sample: RMSEA = 0.04; TLI = 0.93; multiple groups: RMSEA = 0.02; TLI = 0.95). For neglect (complete sample: RMSEA = 0.07; TLI = 0.89; multiple groups: RMSEA = 0.06; TLI = 0.83), physical abuse (complete sample: RMSEA = 0.09; TLI = 0.80; multiple groups: RMSEA = 0.08; TLI = 0.72) and sexual abuse (complete sample: RMSEA = 0.06; TLI = 0.84; multiple groups: RMSEA = 0.09; TLI = 0.03) the incremental indices were below the suggested cutoff scores of acceptability (Hair et al., 2010). Given that incremental fit indices for models pertaining to neglect (complete sample and multiple groups) and physical and sexual abuse (complete sample only) were close to the cutoff score with acceptable RMSEA indices (Hu & Bentler, 1999), these models will be presented. Multiple group moderation models with physical and sexual abuse have been discarded.
Main Effect of CM Experiences
In line with our first hypothesis, CM experiences were associated with increased post-traumatic symptoms in the complete sample (β = .66; p < .001), regardless of the specific subtype (neglect: β = 2.41; p < .001; physical abuse: β = 1.14; p < .001; emotional maltreatment: β = 1.31; p < .001; sexual abuse: β = .99; p < .001; exposure to DV: β = .44; p = .003). Furthermore, in line with our third hypothesis, focusing only on the CM experiences whose multiple group moderation model fit the data, country-specific findings emerged.
Results showed that in Cameroon, total CM (β = 1.01; p = .001), neglect (β = 2.76; p < .001), emotional maltreatment (β = 1.47; p = .001), and exposure to DV (β = −.87; p = .008) were associated to greater post-traumatic symptoms. In Germany, neglect and emotional maltreatment were positively associated to post-traumatic symptoms (total of CM: β = .87; p = .001; neglect: β = 4.23; p < .001; emotional maltreatment: β = 2.38; p < .001). In Canada and Japan no significant main effect of the CM experiences on trauma symptoms emerged.
Moderation Effects
When looking at the complete sample, results of the moderation effects showed that only the perceived acceptability of neglect moderated the relationship between the experience of neglect and post-traumatic symptoms (β = −.40; p = .025), partially confirming our second hypothesis. The perceived acceptability of neglect had a dampening effect on the positive relationship between experiences of neglect and post-traumatic symptoms (see Figure 1). At lower levels of perceived acceptability of neglect, an increase in exposure to neglect was associated with heightened post-traumatic symptoms as compared to mean and high levels of perceived acceptability.
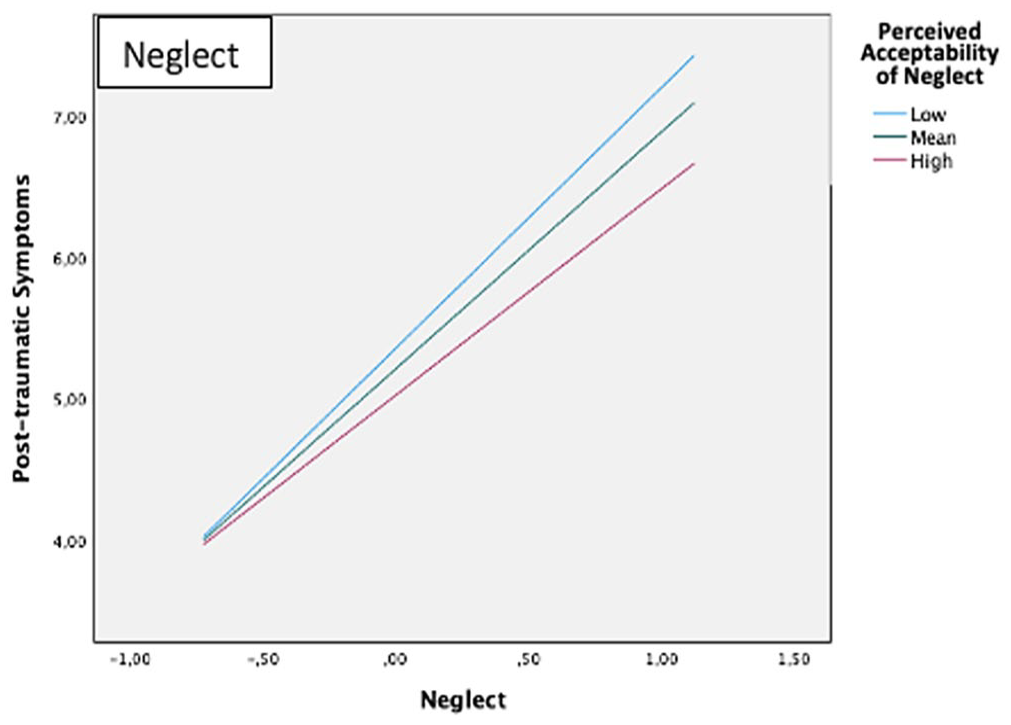
Significant moderation effect of perceived acceptability of neglect on post-traumatic symptoms in the complete sample.
As expected according to hypothesis 3, country-specific findings also emerged with regard to moderation effects for the CM experiences that satisfied multigroup model fit. In Cameroon, the association between the overall exposure to CM and post-traumatic symptoms depended on the perceived acceptability of CM (β = −.28; p < .001): at high levels of perceived acceptability, the effect of the CM experiences on post-traumatic symptoms was weaker than at moderate and low levels.
When unpacking CM in its subtypes, the Cameroonian participants suffered more post-traumatic symptoms at higher levels of neglect (β = −.87; p = .008) and exposure to DV (β = −.87; p = .008), but only if they perceived each of these forms of ill-treatment as less acceptable in their community. A graphical representation of results is presented in Figure 2.
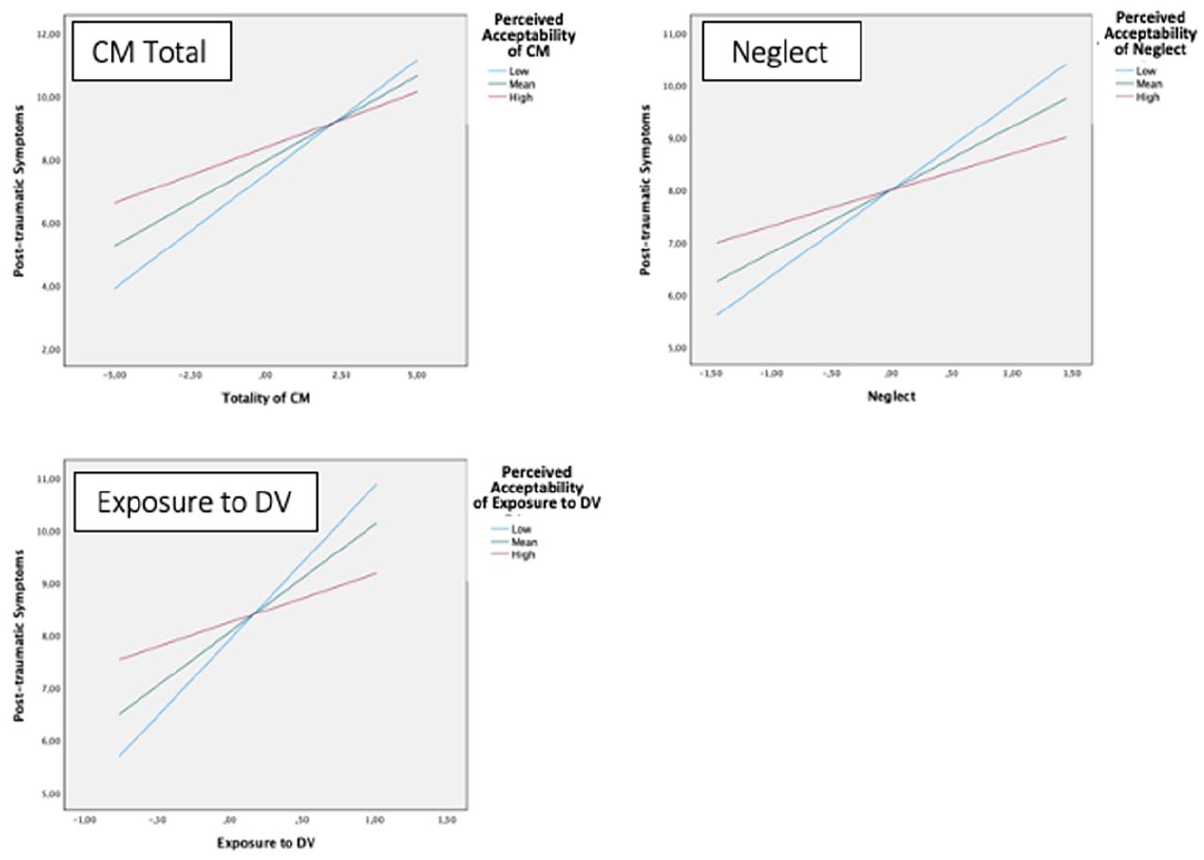
Significant moderation effect of perceived acceptability of CM total, neglect, and exposure to DV on post-traumatic symptoms in Cameroon.
In Germany, only perceived acceptability of neglect was found to moderate the relationship between experiences of neglect and post-traumatic symptoms (β = −1.45; p = .019). As represented in Figure 3, when the perceived acceptability of neglect was low, participants with higher experience of neglect during childhood reported more post-traumatic symptoms as compared to when it was perceived as more acceptable. In Canada and in Japan, no significant moderation effect emerged for any of the CM experiences.
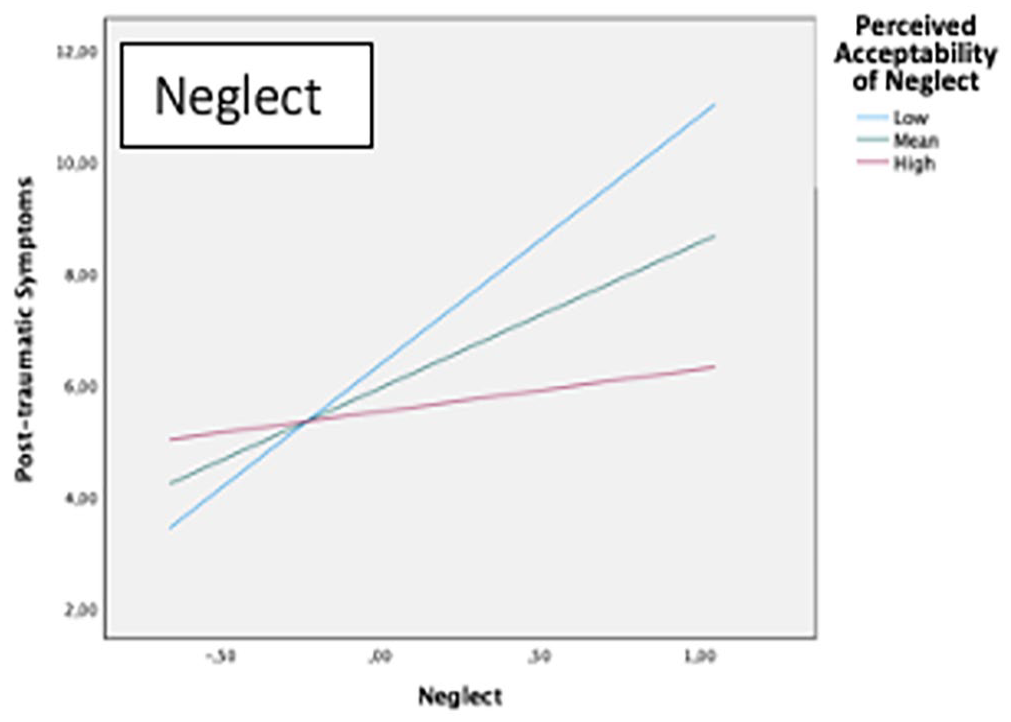
Significant moderation effect of perceived acceptability of neglect on post-traumatic symptoms in Germany.
Discussion
This cross-cultural study aimed at exploring the moderation effects of the acceptability of CM and CM subtypes in the association between CM experiences and post-traumatic symptoms in adults from Cameroon, Canada, Germany, and Japan. Our findings show that beyond the main effect of CM in its different forms on post-traumatic symptoms across cultures, country-specific differences exist. Moreover, perceived social norms about CM (i.e., perceived acceptability of CM) moderated the relationship between CM experiences and post-traumatic symptoms, but not uniformly across cultures and with nuances depending on CM subtypes.
The Impact of CM Experiences on Adults’ Post-Traumatic Symptoms Across Countries
Results confirm previous well-documented evidence that all forms of CM are associated with post-traumatic symptoms, highlighting the need to take action against CM. However, this association varies widely across countries and CM subtypes. It is only in Cameroon that all CM subtypes were associated with post-traumatic symptoms. In Germany, only neglect and emotional maltreatment were associated with post-traumatic symptoms, while, surprisingly, in Canada and in Japan, CM experiences were not associated with post-traumatic symptoms. Further investigations are needed to understand these findings, which are inconsistent with extant evidence and may be statistical artifacts due to statistical power for subgroup analyses or low variability in some scores (e.g., Fujiwara et al., 2010; Klinger-König et al., 2022; Van Vugt et al., 2014). However, previous evidence highlighted cultural variations in the psychological sequelae of different CM subtypes. For example, a cross-cultural study in Kenya, Zambia, and the Netherlands found that childhood neglect was associated with adverse psychological outcomes in university students in the three countries, while the psychological sequelae of physical abuse were associated with psychopathological aftermaths only in the two African countries (Mbagaya et al., 2013). Moreover, it should be noted that cross-cultural differences exist in the expression of post-traumatic symptoms, which may help explain our findings and further stress the need for culturally sensitive means of measuring and identifying CM and trauma reactions (Hinton & Lewis-Fernandez, 2011). For example, in Japan, the stigma and self-stigma associated with trauma might hinder its disclosure (Schnyder et al., 2016), making it more difficult to identify.
The Moderating Effect of the Perceived Acceptability of CM
Moderation effects showed that a lower perceived acceptability of neglect was associated with greater post-traumatic symptoms for survivors in the overall sample and in Germany and Cameroon; the same moderation pattern was also found for exposure to DV in Cameroon. The direction of these findings is in line with the results from Lansford and colleagues’ cross-cultural study on the moderating role of cultural normativeness on children’s adjustment to physical discipline (Lansford et al., 2005). Rohner’s Interpersonal Acceptance-Rejection Theory might help to interpret this pattern of results (Rohner, 2021). The perception of a CM behavior as more acceptable by the community might help survivors, for better or for worse, to make sense of their experience with less feelings of rejection (Rohner, 2021) or stigmatization (e.g., Hofmann et al., 2010). Interestingly, in the complete sample, this pattern was only significant for neglect, suggesting a variability across CM subtypes.
Neglect is different from other CM subtypes since it consists in the omission of adequate caring practices rather than the commission of abusive behaviors (Music, 2017). It is the caregivers’ chronic failure to meet children’s physical and emotional needs (Music, 2017) that may be driven by indifference toward the child according to Rohner (2021). However, neglectful behaviors are often exacerbated by other stressful life conditions, such as unemployment, social deprivation, poverty, or economic crisis (Music, 2017), rather than by indifference (Rohner, 2021). This might lead neglect survivors to appraise their experience in the light of higher perceived acceptability of neglect due to other underlying reasons rather than in the light of a rejection against them. This interpretation might help buffer the effects of neglect.
The non-significant findings observed with physical abuse and emotional maltreatment are in line with previous evidence showing that the dampening effect of perceived acceptability observed on the relationship between CM experiences and psychological adjustment occurs only with milder physical discipline (Lansford et al., 2014) and verbally aggressive behaviors (e.g., yelling; Ali et al., 2019). However, when more severe physically and emotionally abusive experiences are considered, CM experiences result in similar long-term detrimental effects cross-culturally and even more severe effects on survivors from cultural backgrounds that endorse more lenient norms toward CM (Lansford et al., 2002).
Besides CM subtypes, cultural specificities were identified that warrant further exploration. In the case of neglect, in Cameroon, some country-specific factors, like the country’s income or level of poverty (Akmatov, 2011) or child-rearing practices that rely less on adult surveillance (Ruiz-Casares et al., 2018), might contribute to a perception that some experiences that would be considered neglectful elsewhere are more acceptable. These assumptions would be in line with Mbagaya and colleagues’ speculations (2013), who suggested that the cultural variability in the post-traumatic sequelae observed among Kenyan, Zambian, and Dutch survivors of neglect might be attributed to differences in the appraisal of the neglectful experience.
In this study, a moderating effect emerged in Cameroon for exposure to DV. This finding is consistent with Fosco et al. (2007) who stressed the need for a deeper consideration of the cultural beliefs underlying exposure to DV. The authors postulate that survivors living in communities that endorse DV may be less likely to consider themselves abused, appraise the experience as less upsetting, and feel less distressed (Fosco et al., 2007). However, these findings are far from suggesting that higher perceived acceptability of DV—or any CM subtype—is desirable. Indeed, when people perceive exposure to DV as more acceptable in their community, they might be more likely to legitimate aggression within relationships (Fosco et al., 2007), and thus increase the risk of perpetuation of DV, which exerts its detrimental effects by inducing feelings of fear, guilt, or powerlessness in the child (Fosco et al., 2007; Kubeka, 2008). Furthermore, the negative outcomes of exposure to DV are likely to be exacerbated by collateral experiences of neglect connected to the deleterious impacts of DV on the abused caregiver (Kubeka, 2008). Indeed, studies with mothers who suffer from DV have consistently found that feelings of depression and powerlessness related to the abusive situation affect their parenting behaviors so that they tend to be less warm and often distant from their children, and this contributes to a strained mother-child relationship (Levendosky & Graham-Bermann, 2001). Hence, conclusions need to be drawn carefully about the implications of these findings for policies and practice, remembering that all CM experiences entail negative outcomes on mental health.
Limitations
The current study has limitations to consider. First, the convenience samples from the four participating countries presented some baseline differences in terms of some sociodemographic characteristics that make comparisons more difficult to interpret and the generalization of results to the whole country’s population impossible. Including more countries and more representative samples would be an important avenue for future research. Second, the cross-sectional nature of the study does not allow to draw causal conclusions on the obtained results. Third, the study’s findings might be subject to a self-report bias. Also, CM experiences were assessed retrospectively, which increases the likelihood of recall bias. Fourth, perceived social norms were assessed with a non-validated questionnaire; validation studies are needed. Fifth, not all moderating models reached the cutoff for satisfactory fit, resulting in an inability to interpret multigroup models with some CM subtypes. Finally, the number of statistical analyses conducted may have inflated the risk of Type 1 error. Replication studies are needed.
Implications
Our findings do not suggest that being more accepting of CM behaviors is desirable. Exposure to CM predicts negative health outcomes both in our study and in previous ones (e.g., Lansford et al., 2005), and social norms toward CM predict perpetration of CM (Bensley et al., 2004; Taylor et al., 2011). This evidence highlights the need to discourage social norms that endorse violence and CM, with the aim to eradicate this important social problem. Schools, mass media, advocacy campaigns, and policymakers should promote alternative social norms and policies that endorse the culture of non-violence, where survivors are neither blamed nor rejected. This would provide survivors with alternative attributional interpretations of their experience while hindering the transmission of social norms that tolerate or justify violence.
Nowadays, several social norms campaigns have been implemented to promote behavioral changes and to prevent destructive behaviors, such as alcohol consumption and abuse, smoking, sexual assault, and CM (e.g., Berkowitz, 2010, Ottley et al., 2022). These campaigns have usually provided normative feedback to communities, groups, and individuals to correct misperceptions that influence behaviors (Berkowitz, 2010). However, for them to be effective, cultural sensitivity as well as awareness about the specificity of CM in all its manifestations are required. The current study provides interesting insights in this regard.
Evidence about the attenuating role of the perceived acceptability on the effects of neglect on post-traumatic symptoms suggests that neglect should be combated by providing material support to vulnerable communities as well as with policies aimed at reducing disparities, promote social welfare, and reinforce parental skills. Again, cultural sensitivity is crucial.
Finally, our findings inform mental health and childcare practitioners of the weight of the perceived acceptability of certain CM practices on the post-traumatic outcomes for CM survivors of different cultures, highlighting the need for tailored culturally sensitive interventions that take into account the specificities of CM subtypes.
Future Directions
Our findings suggest that perceived acceptability of CM might play a protective role in post-traumatic symptoms in some countries for some CM subtypes. Further studies are needed to replicate our findings and investigate the determinants of social norms on mental health across different cultures, in order to develop effective interventions to promote mental health in CM survivors without normalizing CM. Future studies should aim to increase the sample size and representativity for each participating country and to involve further countries representative of all regions of the world, like Central and South America, Eastern Europe, Northern Africa, the Middle East, and Australia.
Future studies might consider measures of interpersonal acceptance-rejection to gain a deeper understanding of the impact of perceived cultural norms on mental health. Also, the dimensions of culture that might drive the moderating effect of the perceived acceptability of CM on the relationship between CM experiences and post-traumatic symptoms need to be further investigated. For example, cultural dimensions like the predominantly collectivistic/individualistic or interdependent/independent orientation of the participating countries should be considered. For example, in collectivistic cultures that prioritize group harmony and tend to exclude people who do not align with social norms (Schnyder et al., 2016), the perceived acceptability of CM might have a different impact on post-traumatic symptoms, as compared to individualistic cultures. Moreover, it might be worthwhile to investigate the relation between the perceived acceptability of different CM subtypes and social support of CM survivors, as social support has been found to be protective against post-traumatic outcomes in some cultures (Hansford & Jobson, 2022). Finally, future studies should consider a prospective longitudinal design for a better understanding of the temporal dynamics between social norms, CM experiences, and post-traumatic symptoms.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605241234348 – Supplemental material for Perceived Acceptability of Child Maltreatment as a Moderator of the Association Between Experiences of Child Maltreatment and Post-Traumatic Symptoms: A Cross-Cultural Study
Supplemental material, sj-docx-1-jiv-10.1177_08862605241234348 for Perceived Acceptability of Child Maltreatment as a Moderator of the Association Between Experiences of Child Maltreatment and Post-Traumatic Symptoms: A Cross-Cultural Study by Eleonora Bartoli, Dany Laure Wadji, Misari Oe, Polly Cheng, Chantal Martin-Soelch, Monique C. Pfaltz and Rachel Langevin in Journal of Interpersonal Violence
Footnotes
Acknowledgments and credits
We wish to thank the participants without whom this project would not have been possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This project was supported by the Internal Social Sciences and Humanities Development Grants of McGill University. Dr. Langevin is supported by a Chercheur-Boursier Junior 1 Award from the Fonds de recherche du Québec—Santé (#310809) and a William Dawson Scholar Award from McGill University. M.Sc. Wadji was supported by a doctoral scholarship funded by the Swiss Government Excellence Scholarships (2018.0801, 2018) and the Swiss National Science Foundation (SNSF) (P1FRP1_199872, 2021). She is now supported by a Postdoc. Mobility fellowship from the SNSF (P500PS_214332, 2023). M. Sc. Bartoli is supported by a doctoral scholarship funded by the German Studienstiftung des deutschen Volkes (2019–2023).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.