
Abstract
In contrast to adults, there is considerably less research on childhood or adolescent exposure to sexual harassment (CAESH), its lasting psychological correlates, and whether such experiences should be included in definitions of childhood sexual abuse. The current study examined the prevalence and symptomatic sequels of unwanted flirting, being “checked out” sexually, unwanted sexual attention, sexual comments, propositions, and related noncontact behaviors that occurred before age 18, as well as the multivariate relationship between CAESH and contact child sexual abuse (C-CSA) in a diverse online sample of 528 individuals. CAESH was very common, with over 95% of women and 64% of men reporting at least one experience of noncontact sexual harassment before age 18. When childhood sexual abuse was operationalized as the presence of either C-CSA or a total CAESH score of 18 or higher (corresponding to an average score of “3–5 times” prior to age 18), the prevalence was 67% for women and 26% for men, more than three times higher than C-CSA alone. This expanded definition was associated with significantly more anxiety, depression, and posttraumatic stress relative to C-CSA alone. These results suggest that CAESH is a significant source of symptoms in adults and support the emerging perspective that childhood sexual abuse may be best understood as including both contact and noncontact events.
Sexual aggression against women and children is common in North American society. Current estimates suggest that around 20% of adult women and approximately 4%–7% of men experience sexual assault or rape in their lifetime (Elliott et al., 2004; Sorenson et al., 1987; Tjaden & Thoennes, 2000) and over 25% of children and adolescents report sexual abuse or sexual assault—especially girls and adolescent women but also boys and adolescent men (Finkelhor et al., 2014). These forms of contact sexual maltreatment have been associated with subsequent psychological difficulties, ranging from anxiety, depression, and posttraumatic stress to substance abuse, somatic responses, and low self-esteem (Dworkin et al., 2017; Hailes et al., 2019).
Sexual maltreatment does not appear to have to involve physical contact in order to be traumatic, however. For example, studies indicate that substantial numbers of adult women and, to a lesser extent, adult men experience sexual harassment (see a systematic review by Karami et al., 2021), defined by the U.S. Equal Employment Opportunity Commission as “unwelcome sexual advances, request for sexual favors, and other verbal and physical conduct of a sexual nature” (U.S. Department of the Interior, n.d.). Although such behaviors may include physical acts such as grabbing or touching a person without their permission, sexual harassment generally focuses on nonphysical behaviors, demands, or comments. These behaviors, which are not limited to the workplace, are associated with a range of symptomatic outcomes (Karami et al., 2021; Willness et al., 2007).
Often reflecting attempts to devalue or exploit women and girls (Fitzgerald & Cortina, 2018), noncontact sexual harassment can be considered part of a sexual aggression continuum or “continuum of harm,” ranging from inappropriate gestures, salacious statements, unwanted sexual attention, and sexual propositions, to physical acts such as sexual abuse, assaults, and rape (Kelly, 1987; McCloskey, 1997). Although noncontact sexual aggression and harassment is widely documented in adults, there are fewer studies or discussions of such behavior against children and youth (Landolt et al., 2016). Instead, the focus of many (but not all) studies, policy statements, and laws regarding sexual maltreatment of children tends to be on “sexual activity,” especially contact sexual victimization (e.g., Briere et al., 2020; Finkelhor et al., 2014; Violato & Genius, 1993). This is despite the fact that many of the behaviors described in the literature as sexual harassment (e.g., sexual propositions, sexual comments or gestures, and unwanted sexual attention) when occurring during childhood or adolescence may be considered noncontact forms of sexual abuse (Mathews & Collin-Vézina, 2019; Zolotor et al., 2009). In fact, not viewing early sexual harassment as a potential form of child sexual abuse may lead to an underestimation of the actual amount of sexual maltreatment experienced by children and adolescents and may underestimate the deleterious nature of such experiences above and beyond contact victimization (Mathews & Collin-Vézina, 2019).
In the present study, we examined childhood and adolescent exposure to sexual harassment (CAESH) in a diverse, online sample, and the association of such maltreatment with participants’ current reports of psychological symptoms. We hypothesized that (a) CAESH would be associated with later adult symptoms of anxiety, depression, and posttraumatic stress, and (b) a definition of childhood sexual abuse that included contact child sexual abuse (C-CSA) and elevated CAESH scores would be more prevalent and more associated with symptomatology than contact sexual abuse alone.
Methods
Procedures
Participants were asked to complete an anonymous online survey on “the links between various life experiences, discrimination, and psychological symptoms” using one of two online data recruitment sites for psychology research: Psychological Research on the Net and Social Psychology Network. These websites are housed in the U.S.; however, English speakers from other countries also can access them and we did not code the nationality of respondents in this study. Nine participants also were recruited through Mechanical Turk (MTurk). In return for their involvement, individuals were given the opportunity to enter a draw for one of 10 Amazon gift cards and the Mturk participants were reimbursed for their participation.
Participants were provided with an informed consent form, after which the questionnaire became available for completion. Participants could discontinue participation at any time or leave questions blank without losing their reimbursement or ability to enter the draw, and received an explanation of the purpose of the study along with resources they could access if they became distressed. This study was approved by the University of Victoria’s Institutional Review Board.
Participants
Participants were English-speaking individuals, aged 19 or older (the age of majority in the Canadian province where this study was initiated). Of 823 individuals who completed some portion of the questionnaire, 295 (38.8%) were screened out because they responded to less than half of items or were under age 19, leaving 528 participants.
When this sample was compared to a subsample of individuals for whom there were at least some demographic data but who were screened out for skipping most other items, logistic regression analysis found no differences based on race, gender, or LGBTQ+ identity. However, completers were older (M = 27.38, SD = 10.84) than noncompleters (M = 24.13, SD = 10.36), p < .001), total equation: X2 (8, N = 818) = 33.22, p < .001.
In the final sample, 389 participants (73.7%) identified as female, 122 (23.1%) as male, and 33 (6.4%) as nonbinary. The mean age was 27.48 years (SD = 11.08) and racial identity was 338 (64.3%) White, 43 (8.2%) Black or African American/Canadian, 45 (8.6%) Hispanic/Latinx, 43 (8.2%) Asian American or Canadian, 3 (0.6%) Native Hawaiian, 3 (0.6%) American or Canadian Indigenous people, and 51 (9.7%) “other or mixed” race. A total of 338 participants (64.3%) described themselves as heterosexual, 43 (8.1%) as gay or lesbian, 102 (19.3%) as bisexual, 20 (3.8%) as asexual or no orientation, and 21 (4.0%) as “other” orientation. This sample was also used in a recent study of police aggression against marginalized people (Briere & Runtz, 2024), using different variables beyond demographics.
Subgroups Analyses and Missing Data Management
Before analyses were conducted, the data were randomly split into two nonoverlapping subsamples (ns = 265 and 263) using the SPSS 28 random number procedure: the first to develop the CAESH and the second to cross-validate subsample 1 results and to examine the relationship between CAESH and symptomatology. The use of separate development and validation samples is recommended in modern measure development (e.g., Boateng et al., 2018), including as a way to address overestimation of model performance and reduced generalizability that can occur when a measure is developed and tested using a single, nonreplicated sample (Smith et al., 2014).
Discriminant analysis of study variables indicated no differences between development and validation subsamples, N = 528, X2(7) = 4.95, p = .667. Linear interpolation was used to replace missing values, which ranged from 0% (age) to 14.5% (Generalized Anxiety Disorder-7 [GAD-7]; Spitzer et al., 2006), and modal response were used to replace missing data for nominal-dichotomous variables. Because the number of participants identifying as nonbinary in subsamples 1 and 2 were small (n = 7 [2.6%] and n = 9 [3.4%], respectively), analyses that included gender were limited to those identifying as male or female.
Measures
Contact Childhood Sexual Abuse
C-CSA was determined based on participants’ responses to the dichotomously scored childhood sexual abuse item of the Adverse Childhood Experiences Scale (ACES; Felitti et al., 1998), that is, “Did an adult or person at least 5 years older than you ever touch or fondle you or have you touch their body in a sexual way, or try to or actually have oral, anal, or vaginal sex with you?” ACE items and the total scale have been used in numerous studies (e.g., Hughes et al., 2017; Sahle et al., 2022) and have been shown to be valid measures of childhood adversities. In the total sample, 14.7% (n = 57) of women and 9.0% (n = 11) of men reported C-CSA on the ACES. See Table 1 for descriptive data on C-CSA and the other variables used in this study.
Descriptive Statistics for Study Variables in Full Sample.
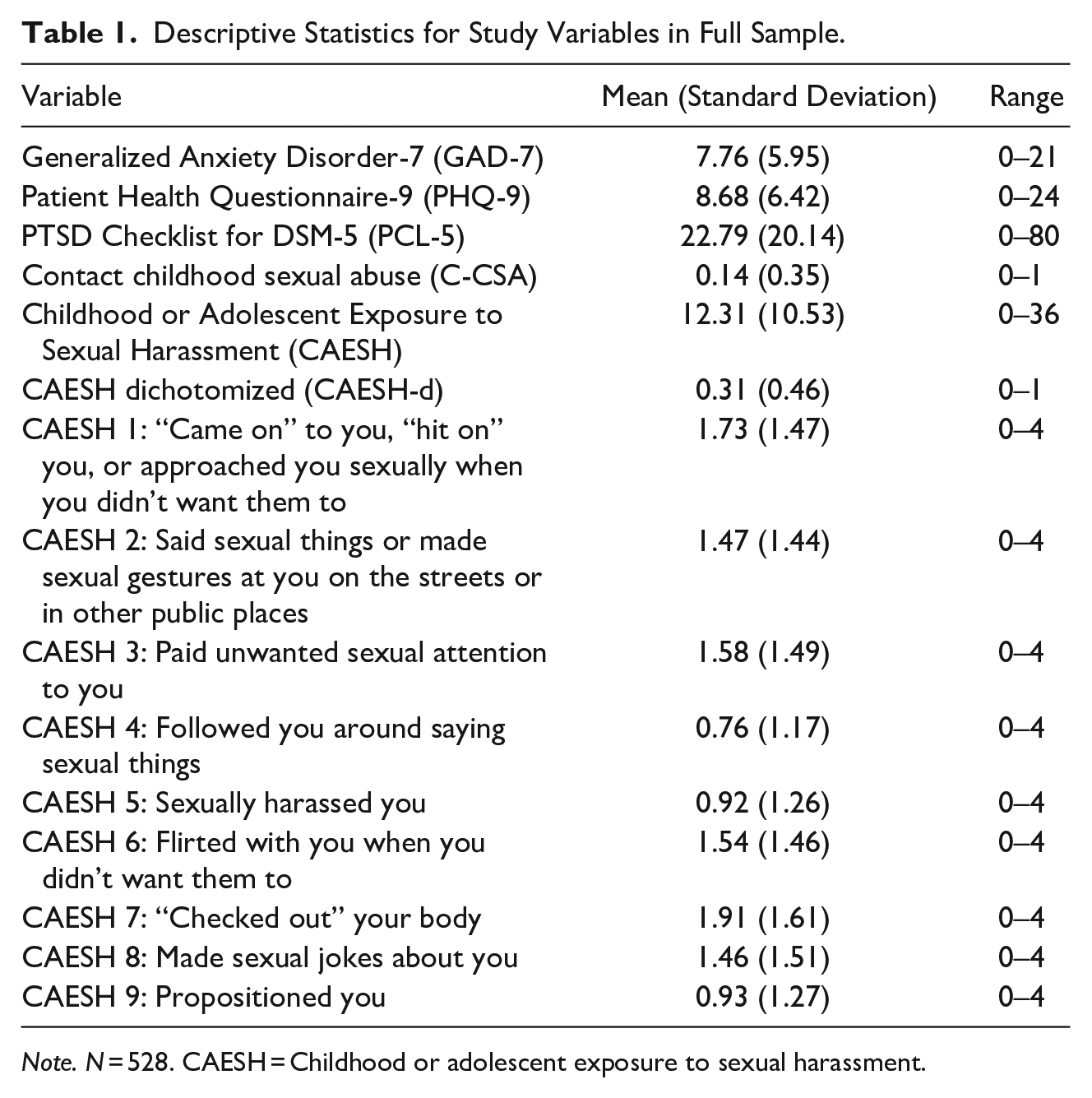
Note. N = 528. CAESH = Childhood or adolescent exposure to sexual harassment.
Childhood or Adolescent Exposure to Sexual Harassment
The CAESH was developed for the present study. A list of nine types of noncontact sexual harassment was generated by the authors following a review of the relevant literature and based on clinical experience. Participants were asked “In your life, how often have people done the following things” (a) before age 18 and (b) at age 18 or older (data not used in current study), including being “hit on” or approached sexually; exposed to sexual comments or gestures in public places; unwanted sexual attention; sexual harassment; unwanted flirting; having one’s body “checked out” sexually; being propositioned; and being the target of sexual jokes, rated on a scale ranging from 0 (“never”) to 4 (“more than 10 times”). See Table 1 for item wording. Following a principal factors analysis in subsample 1, these items were summed to create a nine-item unit-weighted scale: CAESH.
CSA/CAESH
In order to test the prevalence and predictive validity of a variable that included information on both contact and noncontact child sexual abuse, CAESH scores were dichotomized at 18 or higher, corresponding to an average score of 2 (“3–5 times”) or higher (CAESH-d). If participants endorsed C-CSA, CAESH-d, or both, they were categorized as having been sexually abused in childhood on a new dichotomous variable, CSA/CAESH.
Anxiety and Depression
Symptoms of anxiety and depression were assessed based on the sums of participants’ scores on the seven-item GAD-7 and the nine-item Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001). Both measures are psychometrically valid and reliable and are widely used in research and clinical practice (Kroenke et al., 2016). The GAD-7 and PHQ-9 were internally consistent in the current study (α = .93 and .92, respectively).
Posttraumatic Stress
Posttraumatic stress was indexed by the sum of items on the generic version of the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 1993), anchored on “problems that people sometimes have in response to a very stressful experience.” Beyond its use to screen for a PTSD diagnosis, the PCL-5 is widely used as a continuous measure of posttraumatic stress (e.g., Blevins et al., 2015; Wortmann et al., 2016). The PCL-5 was internally consistent in the current study, α = .96.
Aims
Aims of this study in subsample 1 were to (a) develop the CAESH and determine its factor structure and internal consistency, (b) evaluate associations between CAESH and participant sex and age, and (c) determine the prevalence of CSA/CAESH relative to C-CSA alone.
In subsample 2, we sought to (d) cross-validate the factor structure and internal consistency of the CAESH found in Subsample 1, and (e) assess the incremental validity of the combined CSA/CAESH variable in the prediction of anxiety, depression, and posttraumatic stress. Aim 5 was tested using hierarchical multiple regression analyses: C-CSA was entered at step 1 to determine its relationship to symptomatology without consideration of CSA/CAESH, and CSA/CAESH was added at step 2 to assess its unique association with symptoms controlling for C-CSA. The R2 associated with entry of variables at step 2 indicates the proportion of variance associated with CSA/CAESH above-and-beyond that associated with C-CSA.
Results
Aims 1: Factor Analysis and Internal Consistency in Subsample 1
A principal axis exploratory factor analysis of CAESH items in subsample 1 yielded a single factor based both on Kaiser’s (1960) eigenvalue <1 criterion and a scree plot that broke at one factor, accounting for 67.78% of item variance (see Table 2 for factor loadings). The resultant nine-item scale was internally consistent (α = .94).
Principle Factor Matrix for Childhood and Adolescent Exposure to Sexual Harassment Scale in Subsample 1.
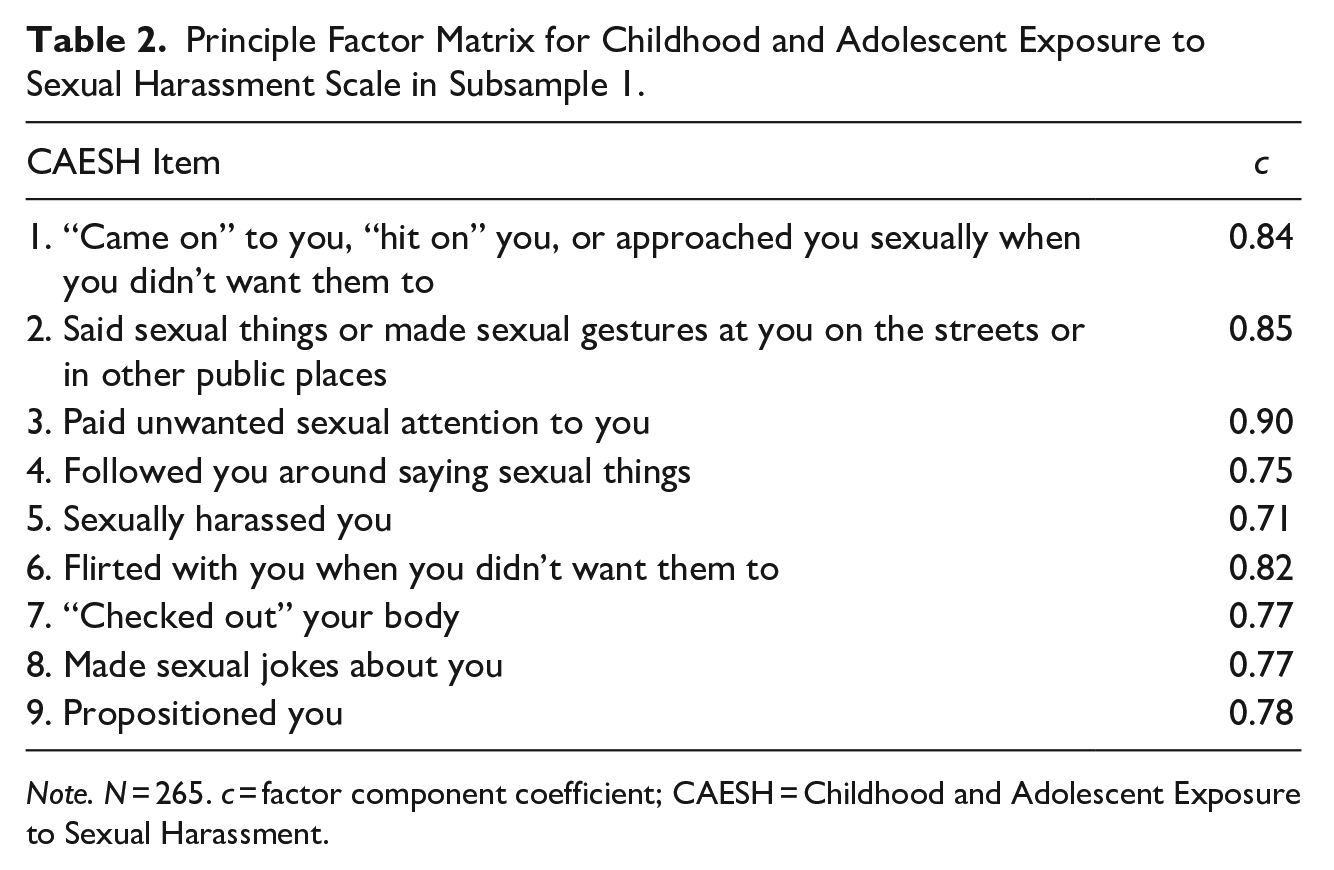
Note. N = 265. c = factor component coefficient; CAESH = Childhood and Adolescent Exposure to Sexual Harassment.
Aim 2: Associations with Sex, Age, and C-CSA in Subsample 1
As presented in Table 3, multiple regression analysis in subsample 1 indicated that self-reported female sex and a history of C-CSA, but not age, were associated with higher rates of CAESH, adjusted R2 = .18, F(3,254) = 20.05, p < .001. A post hoc t-test of the significant sex effect revealed that those identifying as female reported nearly three times higher CAESH (n = 184; M = 15.03, SD = 10.55) than did those identifying as male (n = 69; M = 5.47, SD = 5.97), t(251) = 6.34, p < .001, Cohen’s d = .98 (Cohen & Cohen, 1975). In total, 95.1% (n = 195) of females and 64.2% (n = 34) of males in subsample 1 endorsed at least one or two experience of CAESH prior to age 18, and 58.0% (n = 85 and 5.7%, (n = 3) respectively, endorsed 3 -5 times or more.
Multiple Regression of Age, Sex, and Contact Childhood Sexual Abuse (C-CSA) on Child and Adolescent Exposure to Sexual Harassment (CAESH) Scores in Subsample 1.
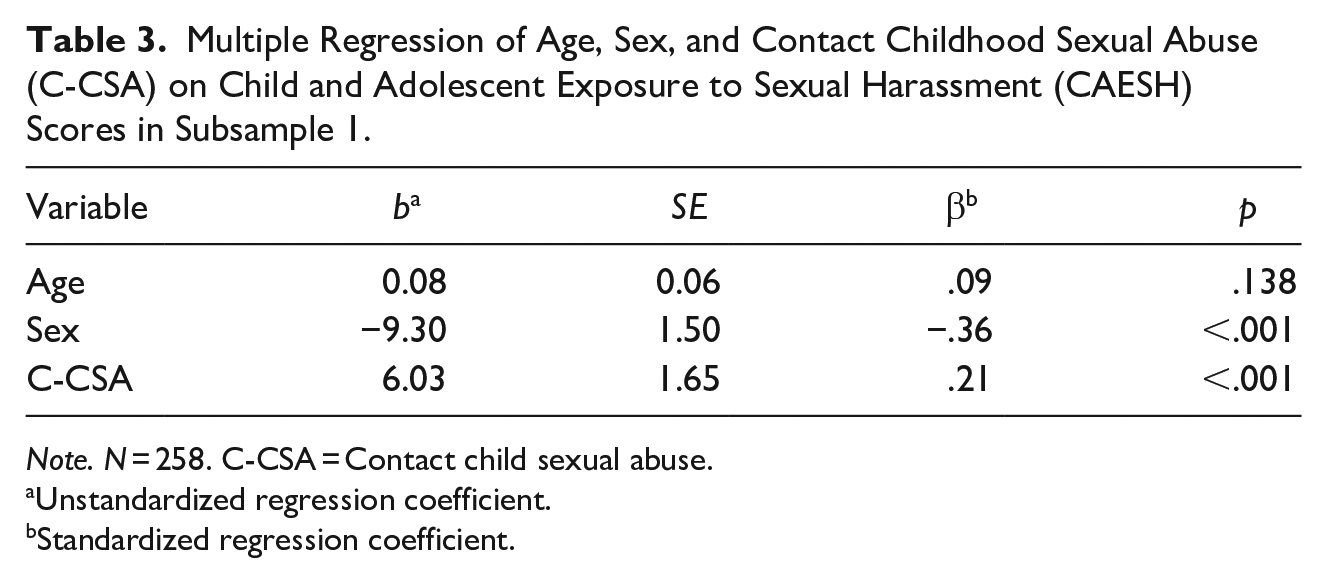
Note. N = 258. C-CSA = Contact child sexual abuse.
Unstandardized regression coefficient.
Standardized regression coefficient.
Aim 3: Prevalence of C-CSA and CSA/CAESH in Subsample 1
When the definition of childhood sexual abuse was modified to include either a CAESH score of 18 or higher or self-reported contact sexual victimization (CSA/CAESH), prevalence rates increased substantially (68.3% of women and 30.2% of men) relative to C-CSA alone (18.0% of women and 7.5% of men).
Aim 4: Cross validation in Subsample 2
Cross validation of the subsample 1 CAESH factor structure and internal consistency in subsample 2 revealed equivalent results, with the same variables loading on the same factors, accounting for 69.55% of item variance, and equivalent internal consistency (α = .94). Subsample 2 factor analysis results are available from the first author.
Aim 5: Incremental Prediction in Subsample 2
As presented in Table 4, hierarchical multiple regression analyses in subsample 2 indicated that although C-CSA was related to depression and posttraumatic stress at Step 1, these associations were no longer significant once CSA/CAESH was entered at Step 2. In contrast, CSA/CAESH was a significant incremental predictor of anxiety, depression, and posttraumatic stress after controlling for C-CSA, accounting for significant additional symptom variance (R2 = .05, .02, and .05, respectively).
Hierarchical Multiple Regression Analyses Predicting Anxiety, Depression, and Posttraumatic Stress as a Function of Contact Child Sexual Abuse (C-CSA) and CSA/CAESH in Subsample 2.
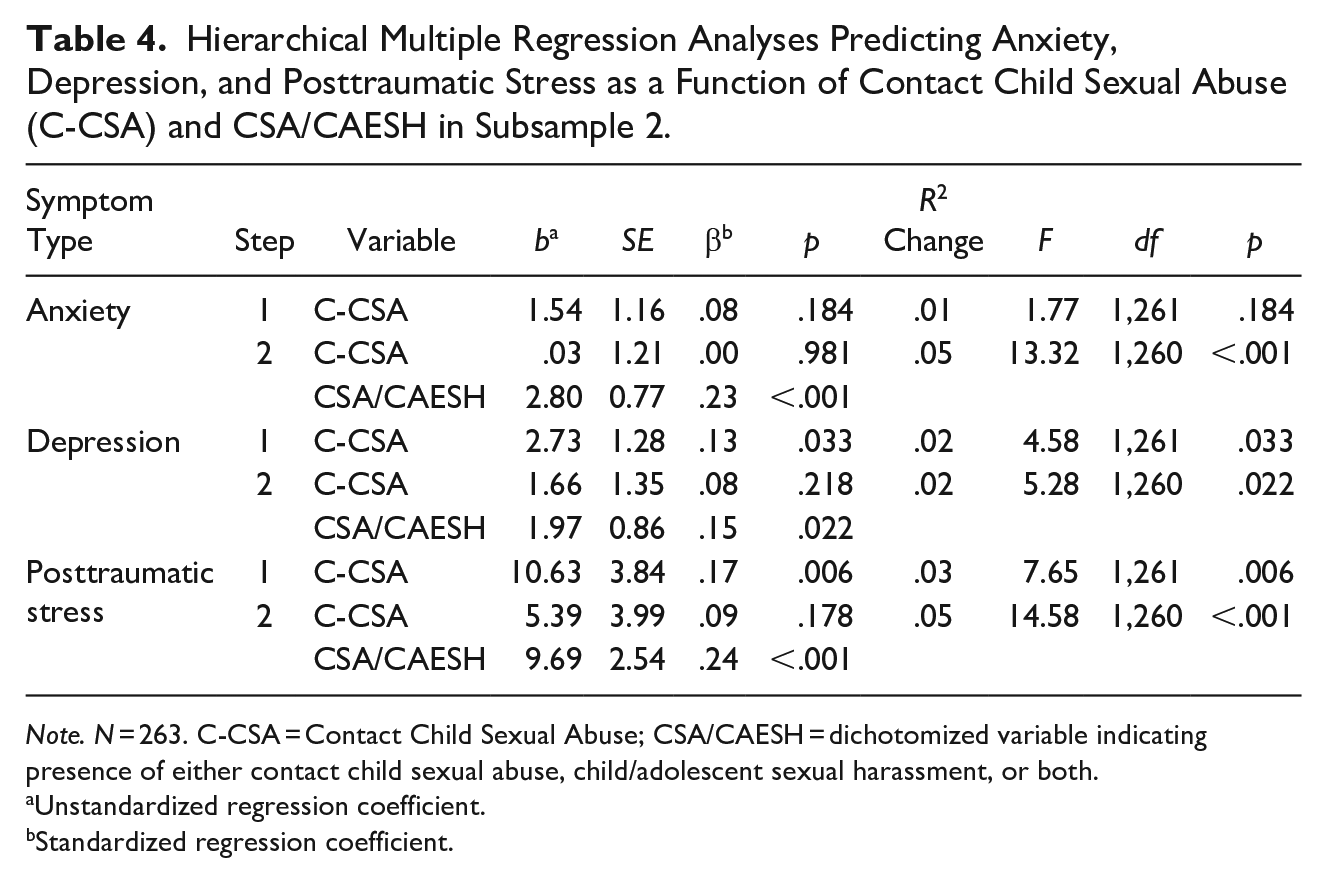
Note. N = 263. C-CSA = Contact Child Sexual Abuse; CSA/CAESH = dichotomized variable indicating presence of either contact child sexual abuse, child/adolescent sexual harassment, or both.
Unstandardized regression coefficient.
Standardized regression coefficient.
Discussion
To the extent that they are generalizable, these results highlight the prevalence and potential impacts of sexual harassment of children and adolescents in North American society. When the usual definition of childhood sexual abuse was modified to reflect either a CAESH score of 18 or higher or contact sexual victimization, or both, prevalence rates increased from 18.0% of women and 7.5% of men for C-CSA to 68.3% of women and 30.2% of men for CSA/CAESH. Importantly, the reported frequency of CAESH-d in this study was based on the decision to dichotomize CAESH at three to five times or more across CAESH items. Were CAESH scores to be dichotomized at one to two times or more, the prevalence of contact and noncontact sexual abuse would have been even higher, with 95% of women and 64% of men reported at least one to two experiences of CAESH prior to adulthood. Conversely, setting the cut-off for CAESH-d at a higher level (e.g., 4–10 times or higher) would reduce the reported prevalence rate, although running the risk of normalizing otherwise significant levels of sexual harassment of children or adolescents.
Although some researchers suggest that childhood sexual abuse should include noncontact child sexual victimization (e.g., Landolt et al, 2016; Mathews & Collin-Vézina, 2019), most studies (including many of those by the first and second authors of this study) have included only contact sexual maltreatment (e.g., being touched, fondled, or experiencing attempted or actual oral, anal, or vaginal intercourse at the hands of an older person) in their definition of sexual abuse. The current results suggest that calls to include noncontact experiences in definitions of childhood sexual abuse may be clinically appropriate, since a more inclusive definition (e.g., CSA/CAESH) predicted significantly more variance in psychological symptoms than did C-CSA alone.
Limitations
Because the participants for this study were recruited via the Internet, the generalizability of these findings should be considered. Fortunately, a number of studies in major journals suggest that web-based research can generate reliable and valid results (e.g., Buchanan & Scofield, 2018). Further, the pattern of associations reported here are consistent with the literature, and missing values were not associated with background variables, except that older participants were more likely to complete the questionnaire. The online nature of this sample may, in fact, mitigate concerns about representativeness, since it resulted in higher numbers of non-White and LGBTQ+ participants than is often found in similar research.
Participants in this study, by definition, had access to the Internet, potentially limiting the generalizability of these findings to those with access to a computer. Further, like most studies in this area, the current data were based on retrospective self-reporting, which may have introduced variability associated with imperfect memory for past events and the limitations of self-assessed psychological symptoms.
Although the ACES C-CSA rates in the present study are in general agreement with other studies (e.g., Finkelhor, 1994), Dolson et al. (2021) note that the ACES sexual abuse item does not include sexual contact by someone less than 5 years older than the child—a scenario that is included in other research definitions (e.g., Finkelhor, 1994). In the same vein, although the ACES sexual abuse item refers to actions by “a parent or adult in the household,” the CAESH specifies anyone (i.e., “people”), regardless of age. It is likely that the gap between C-CSA and CSA/CAESH endorsements found here would be smaller were Finkelhor and colleagues’ definition used instead of Felitti et al.’s, since it would include sexual abuse experiences with people less than 5 years younger than the survivor. Given the relatively narrow focus of the ACES definition, future researchers might consider using Finkelhor and colleagues’ C-CSA definition when calculating CSA/CAESH, since it is likely to capture instances of C-CSA not tapped by the ACES sexual abuse item.
Implications
This research suggests that childhood and adolescent sexual harassment is widely prevalent and psychologically impactful in the general population, highlighting the importance of identifying early experiences of sexual harassment and the appropriateness of broadening discussions of child sexual victimization to include noncontact experiences. Viewing CAESH as a form of childhood sexual abuse, with its own unique and overlapping effects, would likely increase reported prevalence rates and might broaden or increase the known psychological effects of childhood sexual victimization cited in the literature.
Alternatively, researchers and others may choose to study CAESH as separate from C-CSA, just as sexual harassment in adults is often considered a form of sexual victimization that is related to, but not the same as, sexual assault. The fact that 95% women reported at least once instance of noncontact sexual harassment in childhood or adolescence suggests that the lived experience of most people identifying as female includes negative sexualization and inappropriate sexual interactions early in life, above-and-beyond any additional experiences of C-CSA. These findings are consistent with a substantial literature on gender differences in sexual victimization rates across the lifespan (e.g., Hines et al, 2012; Rees et al., 2011; Silove et al., 2017), and extends these findings specifically to childhood sexual harassment.
The clinical implications of these results include the need to identify and prevent CAESH as early as possible, as well as the value of specialized treatment approaches to CAESH-related difficulties. Although sexual harassment was common among those exposed to contact childhood sexual victimization in the present study and thus might be addressed in some instances of sexual-abuse-focused therapy, CAESH appears to have independent contributions to, at minimum, subsequent anxiety and depression, and posttraumatic stress. As a result, clinical attention should be considered not only when C-CSA is reported, but also if CAESH is present, with or without C-CSA. In the latter case, additional or different clinical issues may arise when at least some of the survivor’s abuse was noncontact in nature, sometimes deemed as less serious than contact victimization, and the perpetrator was potentially a peer or other nonadult.
Conclusion
The current findings suggest that noncontact sexual harassment of children and adolescents is common and associated with significant psychological harm, whether in isolation or in combination with experiences of contact sexual abuse. Because many instances of CAESH, although associated with psychological distress, likely go undisclosed or are discounted as less significant than other forms of childhood sexual abuse, further research and treatment approaches to this relatively neglected form of sexual victimization are indicated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.