
Abstract
Up to 32% of adults have experienced some form of childhood maltreatment (CM). Research has shown that these early childhood experiences are associated with a variety of interpersonal difficulties in adult sexual and romantic relationships. Polusny and Follette have suggested that these negative long-term effects are the result of emotional avoidance strategies that individuals use to cope with thoughts, feelings, and memories associated with CM. The present study tested this theorized mediational model with a sample of 150 participants, all of whom were currently in long-term relationships. Participants completed questionnaires designed to assess the severity of CM, fear of their own emotions, and a task designed to assess their accuracy at identifying emotions. Additionally, participants completed a variety of measures assessing the quality of their sexual and romantic relationships. These measures assessed their satisfaction, their communication, and the extent of problems in each domain. Our results showed that higher levels of CM were associated with lower satisfaction with communication and more problems in both the romantic and sexual domains. In regard to our mediational hypothesis, we found partial support showing that fear of one’s own emotions and emotion recognition mediated some of these associations. Our findings suggest that treatments targeting affective processes may be particularly important for helping victims of CM.
Childhood maltreatment (CM), defined by the World Health Organization to include all forms of physical and/or emotional ill-treatment, sexual abuse, neglect, negligence, and exploitation (World Health Organization, 2022), is recognized as a major global health issue by the World Health Organization (Krug et al., 2002). There is ample evidence demonstrating that different forms of abuse and maltreatment (physical abuse, sexual abuse, physical neglect, emotional neglect, and emotional abuse) frequently co-occur, and these domains may be best conceptualized as a single factor representing CM (see discussion by Donget al., 2004; Keyes et al., 2012). Based on these findings, the current study will be using a broad definition of CM and conceptualizing different forms of CM as different facets of CM.
In the United States, over 4.1 million incidents of childhood abuse or neglect were reported in 2016 (U.S. Department of Health & Human Services, 2020). Furthermore, the number of reported cases most likely underestimates the true prevalence of maltreatment, since many cases of childhood abuse and neglect go unreported (Gilbert et al., 2009). Compared to individuals who have never experienced CM, victims of CM are more likely to have a variety of mental health issues, such as mood disorders (Afifi et al., 2014; Fergusson et al., 2008), anxiety disorders (Afifi et al., 2014; Fergusson et al., 2008), and alcohol or drug use disorders (Afifi et al., 2014; Bulik et al., 2001; Fergusson et al., 2008). Furthermore, some reports have suggested that more than half of individuals with chronic mental health issues have experienced some form of CM (Bryer et al., 1987). Thus, the wide-ranging physical and mental health outcomes of CM have been well-documented. There is also evidence to suggest that the link between CM and interpersonal functioning may be explained by symptoms of depression and anxiety (Huh et al., 2014). The overall goal of the current study is to investigate the emotional mechanisms that underlie the association between CM severity and interpersonal outcomes.
CM and Interpersonal Functioning
Taking this broad definition, one of the most consistent findings is that CM is associated with a variety of interpersonal difficulties (see reviews by Goff & Smith, 2005; Leonard & Follette, 2002; Rumstein-McKean, & Hunsley, 2001). In an early review of the literature, Browne and Finkelhor (1986) found that victims of childhood sexual abuse commonly reported feeling fear, hostility, and distrust of others. Later work showed that survivors of CM rated their relationships as more poorly adjusted (Feinauer et al., 1996), tend to report less emotional trust in their romantic partners, and are more likely to view their partners as less reliable (DiLilio & Long, 1999).
One domain within relationships that has received considerable attention is how CM, and childhood sexual abuse in particular, affects sexual relationships. Childhood sexual abuse has been linked to a wide range of sexual difficulties and lower sexual satisfaction (see reviews by Leonard & Follette, 2002; Rumstein-McKean & Hunsley, 2001), although there are some studies that have failed to show this association (e.g., Alexander & Lupfer, 1987; Greenwald et al., 1990). In one of the most widely cited review articles that has investigated the reasons for the discrepant findings, Roberto Maniglio (2009) noted that methodological differences across the studies contributed to the inconsistencies in the findings. Further, the author conducted his own independent review of existing review articles and found that the preponderance of evidence suggests that survivors of childhood sexual abuse are significantly more likely to experience a wide range of medical, psychological, behavioral, and psychological disorders.
Theoretical Work Emotional Avoidance As a Sequelae of CM
Polusny and Follette (1995) proposed a theoretical model highlighting the importance of emotional avoidance in explaining these long-term negative effects associated with CM. According to this theory, children are often unable to escape an abusive situation and so they will often engage in dissociation and emotional suppression to cope with traumatic experiences. The theory further suggests that similar strategies are used after the incident to cope with memories, thoughts, and feelings following CM.
Although the emotional avoidance strategies of dissociation, emotional numbness, and emotional blunting may be initially necessary and adaptive because they allow the child to cope with adverse experiences that threaten their physical and psychological boundaries, they may pose significant relational challenges as the child transitions into adulthood (Bartlett et al., 2020). The coping strategies that may have been necessary for survival at one stage can make it difficult to form healthy relationships characterized by reciprocity, mutuality, trust, openness, and vulnerability. For example, Leitenberg et al., (1992) found that survivors of childhood sexual assault rated emotional suppression and denial as the most helpful strategies for coping, despite the fact that these strategies were significantly associated with poorer psychological functioning.
Polusny and Follette’s (1995) theory focuses specifically on how emotional avoidance is related to how an individual processes and experiences sexual interactions in adulthood since sexual stimuli have become associated with thoughts or flashbacks about previous sexual abuse. Despite this theory primarily focusing on sexual outcomes, it can be extended to broader relationship processes since intimacy and closeness could lead to feelings of vulnerability which could trigger similar feelings. However, it is also possible that the sexual domain may show unique effects because it can be closely tied to traumatic experiences. For this reason, the current study will include both measures of sexual quality and measures of general relationship quality.
The Influence of CM on How Emotions are Processed
Consistent with Polusny and Follette’s (1995) theory, research has shown that experiences of CM can fundamentally alter the way emotional information is processed (Mojjal et al., 2021). Studies have demonstrated that individuals who have experienced CM tend to report greater deficits in cognitive functioning (i.e., memory, executive control; Pechtel & Pizzagalli, 2011), processes that are known to develop across the first two decades of life (Casey et al., 1997). In addition to deficits in cognitive functioning, CM has been associated with a range of difficulties in processing emotional stimuli and experiences. For example, CM has been shown to be associated with increased negative affect and emotion dysregulation (Pechtel & Pizzagalli, 2011; Tottenham & Sheridan, 2010). Behavioral studies have also shown that victims of CM are more likely to interpret positive emotions as ambiguous, they have more difficulty disengaging from emotional stimuli, and they have more difficulty understanding and expressing emotions (Shields & Cicchetti, 2001; Tottenham & Sheridan, 2010). At the same time, there is evidence to suggest that abused children may be able to recognize anger using less sensory input as compared to children who have not experienced abuse (Pollak & Sinha, 2002). The authors reasoned that physically abused children, by virtue of great exposure to anger, may have facilitated access to representations of anger.
It is possible that these emotional processing difficulties can explain the long-term negative effects observed in the interpersonal functioning of individuals who have experienced CM (Walker et al., 2009). In relationships, expressing and sharing emotions promotes intimacy and communicates feelings about a partner and the status of the relationship (e.g., Keltner & Kring, 1998). Furthermore, identifying emotions also plays an important role in communication. For example, recognizing expressions of sadness or hurt are important in order to identify when a partner is in need of social support (Kennedy-Moore & Watson, 1999). Additionally, Walker and Colleagues (2009) have shown that emotional flooding during conflict partially accounts for lower levels of romantic satisfaction. Finally, emotional suppression is related to less closeness with others, less reception of social support in times of need, and less satisfying relationships (Gross & John, 2003).
A Focus on CM Severity
A number of past studies have compared individuals who had experienced CM to control groups on emotional processes [author masked]. In the current study, we extended the past work by focusing on how levels of CM, rather than absence/presence of CM, is associated with disruptions in emotional processes.
Investigating Different Indices of Interpersonal Functioning
In the current study, we extend past work by examining three key indices of interpersonal functioning, rather than focus exclusively on relationship quality. In addition to relationship quality, assessed through measures of relationship satisfaction and sexual satisfaction, we asked participants to rate the quality of sexual and nonsexual communication in their romantic relationship and also asked them to rate the extent to which a variety of commonly endorsed sexual and relationship issues are a problem in their relationship. Example of relationship problems included: not getting enough time together and disagreements around household chores. Example of sexual problems included: not showing interest in having sex and not initiating sexual activity.
Here onward, sexual and nonsexual communication are jointly referred to as the communication outcome, relationship and sexual problems are referred to as the problem outcome, and relationship and sexual satisfaction is referred to as the satisfaction outcome. 1 These three domains represent key indices of relationship functioning that are conceptually related, but also distinct from each other. Satisfaction was chosen since it is one of the most widely used metric for examining the quality of the sexual and romantic relationship and it has been shown to predict divorce (e.g., Gottman, & Levenson, 2000). Communication was chosen because it is a key mechanism by which individuals express and respond to each other’s needs and foster closeness, intimacy, acceptance and safety in their relationship (e.g., MacNeil & Byers, 2009). We also examined sexual and relationship problems that commonly occur in romantic relationships, such as making decisions about household chores or engaging in sexual experimentation. For each of the three outcomes, we examined sexual and nonsexual domains separately. The rationale for distinguishing between sexual and nonsexual domains is that CM would be expected to disrupt an individual’s capacity to build and foster intimacy, and the sexual aspect of a romantic relationship is one of the most intimate aspects of a romantic relationship. As a result, the sexual domain may be particularly impacted by a history of CM.
Emotional Processes as Mechanisms of the Association Between CM and Interpersonal Functioning
A major goal of our study was to investigate the emotional mechanisms that underlie the association between levels of CM and interpersonal functioning. Specifically, we tested the theory put forward by Polusny and Follette (1995) by investigating the role of two mechanisms. The first mechanism is the fear of one’s own emotions, an individual difference variable that is conceptually tied to the experiential avoidance of emotional states. The fear of one’s own emotions is viewed as a more primary mechanism and avoidance is conceptualized as a secondary coping process that represents an effort to cope with the fear that has been activated. We assessed participants’ fear of their positive and negative emotions using the Affective Control Scale (ACS; Williams et al., 1997). Although the scale was originally designed for panic disorder, it has been shown to be a valid assessment of fear of a range of different emotions. As an example, it has been shown to be related to military service-related post-traumatic stress disorder (PTSD) symptoms (Price et al., 2006).
We also tested a second mechanism, emotion recognition. We examined whether deficits in recognizing emotions in others are one of the mechanisms by which CM leads to problems in interpersonal functioning. Previous studies have shown that children with a history of CM have more difficulty identifying ambiguous faces (e.g., Gibb et al., 2009; Pollak & Kistler, 2002). Furthermore, adults who have post-traumatic stress disorder related to CM had reduced accuracy when identifying emotions in faces (Nazarov et al., 2014). However, the study on adults was based on individuals who had a diagnosis of PTSD related to their CM, which is only a minority of individuals who experience CM (Ackerman et al., 1998; Copeland et al., 2007). Therefore, it is currently unclear if the effect found would replicate in a general sample. Finally, these studies were unable to identify how this emotional processing deficit impacted the sexual and romantic relationship.
The Current Study
The overall goals of the current study were to examine whether: (a) increased severity of CM was associated with greater fear of own emotions and weaker emotion recognition skills; (b) whether performance on these emotional measures mediated the association between levels of CM and negative sexual outcomes in relationships. Our key predictor variable was CM severity.
In our first two hypotheses, we predicted that greater CM severity would predict greater fear of one’s own emotions (Hypothesis 1) and weaker emotion recognition skills (Hypothesis 2). We then examined the association between CM severity and each domain of interpersonal functioning, starting with communication. We predicted that CM severity would predict worse sexual and relationship communication (Hypothesis 3) and that this association would be mediated by fear of own emotions (Hypothesis 4) and by emotion recognition skills (Hypothesis 5). We then investigated the association between CM severity and satisfaction and predicted the great CM severity would be associated with lower relationship and sexual satisfaction (Hypothesis 6) and that these associations would be mediated by fear of own emotions (Hypothesis 7) and emotion recognition skills (Hypothesis 8). In our final set of hypotheses, we examined the outcome of relationship and sexual problems. It is inevitable that couples will face challenges and areas of conflict in their relationship, especially over time (e.g., discrepancies in desire, or different preferences). By understanding the perceived intensity of these problems, we can gain better insight into how CM affects adult romantic relationships. We predicted that higher levels of CM will be associated with greater endorsement of problems in both the sexual and nonsexual domains (Hypothesis 9). We hypothesized that both the fear of one’s own emotions (Hypothesis 10) and emotion recognition (Hypothesis 11) will mediate the effect of CM levels on interpersonal functioning.
We focused on individuals in long-term relationships, operationalized as partners who had been together for at least 1 year. We focused on long-term relationships, rather than casual relationships or the early stage of a relationship, because we reasoned that long-term relationships represent a context where problems with developing and fostering intimacy would most likely emerge, once the initial excitement phase of a relationship was over.
Method
Participants
Participants were recruited through TurkPrime using their prime panels. This service uses a variety of online platforms to collect the entire sample of survey data. In order to participate, participants were required to be at least 19 years old, and they were required to have been in a relationship for at least 1 year. Participants were asked to respond to a single-item measure asking about their experiences with childhood abuse, (“Prior to the age of 18 did you experience any instances of childhood physical or sexual abuse?”). As our goal was to examine how CM levels are associated with relationship and sexual outcomes, only participants who reported experiences of childhood abuse and who met the other study criteria were invited to participate in our study. The sample consisted of 175 individuals. However, 25 participants were excluded from the analyses because they either answered four or more of the seven validity questions incorrectly (e.g., “Please select 7 for this question”), or they completed the survey in under 10 min.
As a result, our final sample consisted of 150 individuals (44 cisgender men, 105 cisgender women, and 1 non-binary). The average age of the sample was 45.21 years old (SD = 15.33, range: 19–80). Individuals reported that they had been in their current relationship for an average of 18.5 years (SD = 15.89, range: 1.08–62.83 years). In regard to sexual orientation, 88.7% of the sample identified as heterosexual, 1.3% identified as gay or lesbian, and 9.3% identified as bisexual. The ethnic background of our sample was as follows: 113 participants (~75%) self-identified as White, 12 participants (~8%) self-identified as Hispanic, 10 participants (~7%) self-identified as South Asian descent, 6 participants (~4%) self-identified as Black, and the remaining participants did not answer this question.
Measures
CM Scale
This measure includes 19 questions that assess the intensity of five types of CM before the age of 17 (physical neglect, physical abuse, emotional neglect, emotional abuse, and sexual abuse) (Keyes et al., 2012). The scale includes five questions related to physical neglect, three questions about emotional abuse, two questions focused on physical abuse, five questions related to sexual abuse, and five questions about emotional neglect. This questionnaire asks participants to respond on a scale ranging from 1 (never) to 5 (very often). The questions designed to measure emotional neglect were reverse coded. Sample items included: “I felt there was someone in my family who wanted me to be a success,” and “How often did a parent or other adult living in your home push, grab, shove, slap or hit you?” Reliabilities for the subscales were all high ranging from α = .91 for the physical neglect subscale to α = .90 for the sexual abuse subscale. For our analyses, an average score of all items on the CM was computed.
Affective Control Scale
This scale is a 42-item self-report measure that assesses a participant’s fear of emotions and attempts to control emotional experiences (Williams et al., 1997). The scale includes four subscales related to specific emotional experiences: depression/sadness, anxiety, anger, and happiness/positive affect. For each item, participants responded on a seven-point Likert scale ranging from 1 (Strongly Disagree) to 7 (Strongly Agree). The scale has previously been shown to have a high internal consistency (α = .94 for the overall scale score) and good test-retest reliability over several weeks (r = .78; Williams et al., 1997). The present study found similarly high levels of internal consistency for the scale (α = .95). For this study the results were analyzed with the averaged scale score.
Reading the Mind in the Eyes Test
This test was used to assess accuracy at recognizing emotions when being shown pictures of eyes. The test includes 37 items (one test item and 36 scored items) with each item showing a picture of eyes (Baron-Cohen et al., 2001). Around each set of eyes are four emotion words (e.g., playful, comforting, irritated, bored). For each item participants are asked to identify which of the four words best reflects the emotions conveyed in the picture of the eyes. Participants scores on this task were based on the percentage of correct responses given. Although this measure was originally developed to test individual differences in mentalizing, it is now considered to be a measure that assesses explicit emotion labeling (Oakley et al., 2016). A meta-analytic investigation of the measure by Kittel and Colleagues (2022) demonstrated that the measure is significantly associated with other measures of emotion perception.
Quality of Relationship Index
This scale is a six-item measure that was administered to assess relationship satisfaction. The first part of the measure includes items such as “My relationship with my partner makes me happy” and participants rated it from 1 to 7 with 1 being very strongly disagree and 7 being very strongly agree (Norton, 1983). The second part of the measure is an item that asks the participant to rate how happy they are in the relationship on a scale of 1 (very unhappy) to 10 (very happy). Due to the difference in scale, all items were standardized before averaging. The scale showed a high degree of reliability (α = .97).
The Global Measure of Sexual Satisfaction
This scale is a five-item measure that was used to assess the overall sexual satisfaction of participants. For this questionnaire, participants were shown a Likert scale with word pairs on each end and then asked to rate how they would describe their sexual relationship based on these word pairs (Lawrance & Byers, 1995). The following word pairs are used in the measure: Bad-Good, Unpleasant-Pleasant, Negative-Positive, Unsatisfying-Satisfying, Worthless-Valuable. The scale had excellent reliability (α = .95).
Relationship Problems Questionnaire
This scale asks participants to rate their own relationship on 28 common relationship problems. For each item participants rated how much the issue is a problem in their relationship, and they were also asked to rate how anxious they would be discussing each problem with their partner (Rehman et al., 2017). For each question, participants responded on a seven-point Likert scale ranging from 1 (not at all) to 7 (very much so). An example of an item from this scale would be “How much time to spend together versus apart” or “Housework/chores.” These items showed a high level of reliability (α = .97).
Sexual Problems Questionnaire
This 25-item measure asks participants to rate the extent to which a variety of sexual issues are a problem in his or her relationships on a scale from 1 (not at all) to 7 (very much so) (Rehman et al., 2017). The scale includes items relating to common sexual issues (e.g., “Frequency of sexual relations,” “Showing interest in having sex,” “Exploring passions/experimentation”). The scale was found to have excellent reliability (α = .97).
Dyadic Sexual Communication Scale (DSC)
The DSC Scale includes 13-items, rated on a six-point scale (ranging from strongly disagree to strongly agree), designed to assess the quality of sexual communication in a relationship (Catania, 1998). The scale includes seven items assessing communication problems, for example: “My partner rarely responds when I want to talk about our sex life.” In addition to these items, the scale has six items designed to assess constructive communication, for example: “My partner has no difficulty in talking to me about his or her sexual feeling and desires.” For our analyses these six items were reverse coded to create a measure that reflects poor sexual communication. The overall reliability of this measure was found to be good (α = .77).
Dyadic Communication Scale
The Dyadic Communication Scale was adapted from the DSC to measure couples’ satisfaction with their communication in general (Catania, 1998). This adaptation involved removing references to the sexual aspects of communication. As a result, the scale included 13-items, again rated on a six-point scale. Similar to the DSC, it included seven items assessing communication problems (“My partner and I never seem to resolve our disagreements.”), and six items assessing constructive communication (“Even when angry with me, my partner is able to appreciate my views”). Once again, the six items assessing constructive communication were reverse coded. Reliability estimates for this scale were also found to be acceptable (α = .70).
Procedure
All study measures and procedures were reviewed and approved by the university’s research ethics board. Participants were first asked to complete a brief screening questionnaire to assess their eligibility to take part in the study. Participants who reported experiences of childhood abuse and who met the other study criteria were invited to participate in our study.
Participants who consented to the study, and who passed a captcha question, were then given a series of questionnaires related to their demographics, measures assessing emotional processes, their experience with abuse, and their current relationship (all described above). Questionnaires in this survey were randomized, with the exception of the Reading the Mind in the Eyes Test and the demographics questionnaire which were always presented last. These two questionnaires were placed at the end to ensure that the final questions participants completed were not directly inquiring about traumatic experiences. All participants received remuneration for completing the survey. However, TurkPrime was unable to specify how participants were paid since payment differed based on the different sites used for recruitment.
Results
Analytic Plan
All analyses were conducted using Mplus (Version 7, Muthén & Muthén, 2012) and all variables were standardized prior to analysis. In order to address our primary questions for this study, we used two mediation models (one with ACS score, and the other with the emotion recognition measure), for each of our three domains of interpersonal functioning (communication, satisfaction, and problems). The zero-order correlation matrix for all variables in this study is shown in Table 1 and the descriptive information of key study variables is presented in Table 2.
Zero-Order Correlations Between Sexual and Relationship Variables, Emotion Variables, and CM.
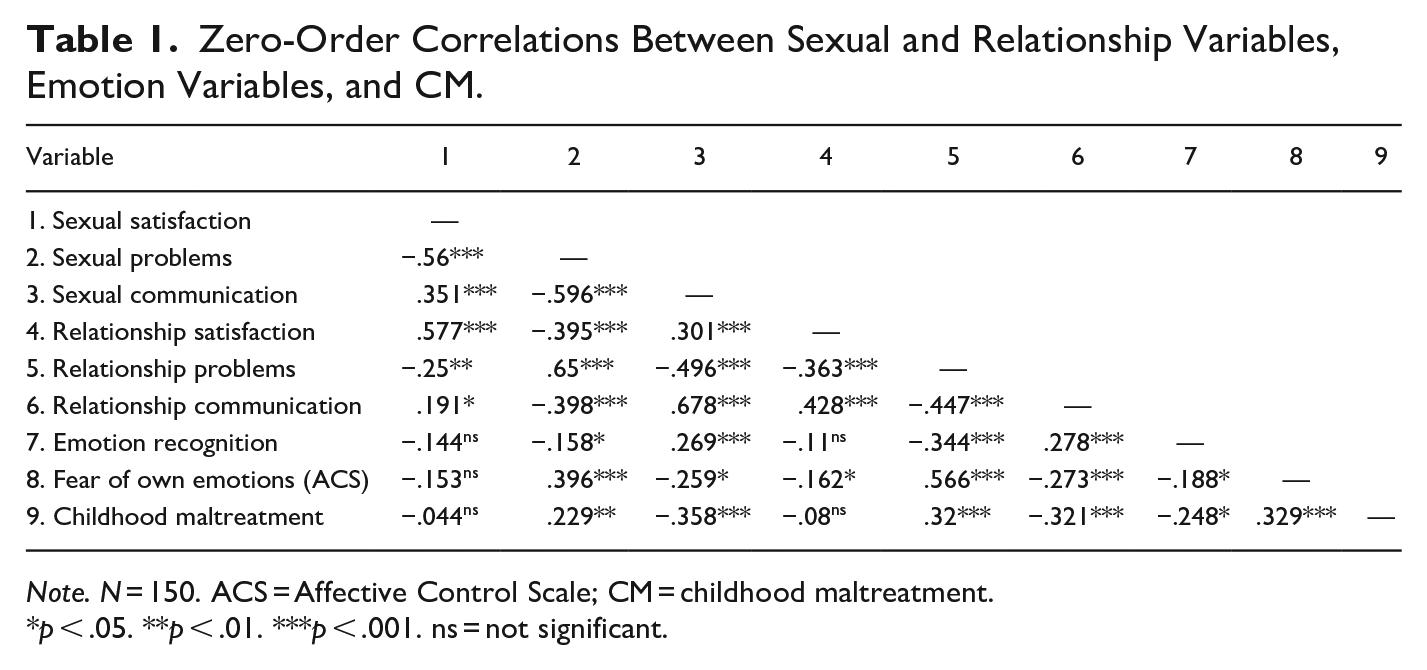
Note. N = 150. ACS = Affective Control Scale; CM = childhood maltreatment.
p < .05. **p < .01. ***p < .001. ns = not significant.
Descriptive Statistics of Key Study Variables.
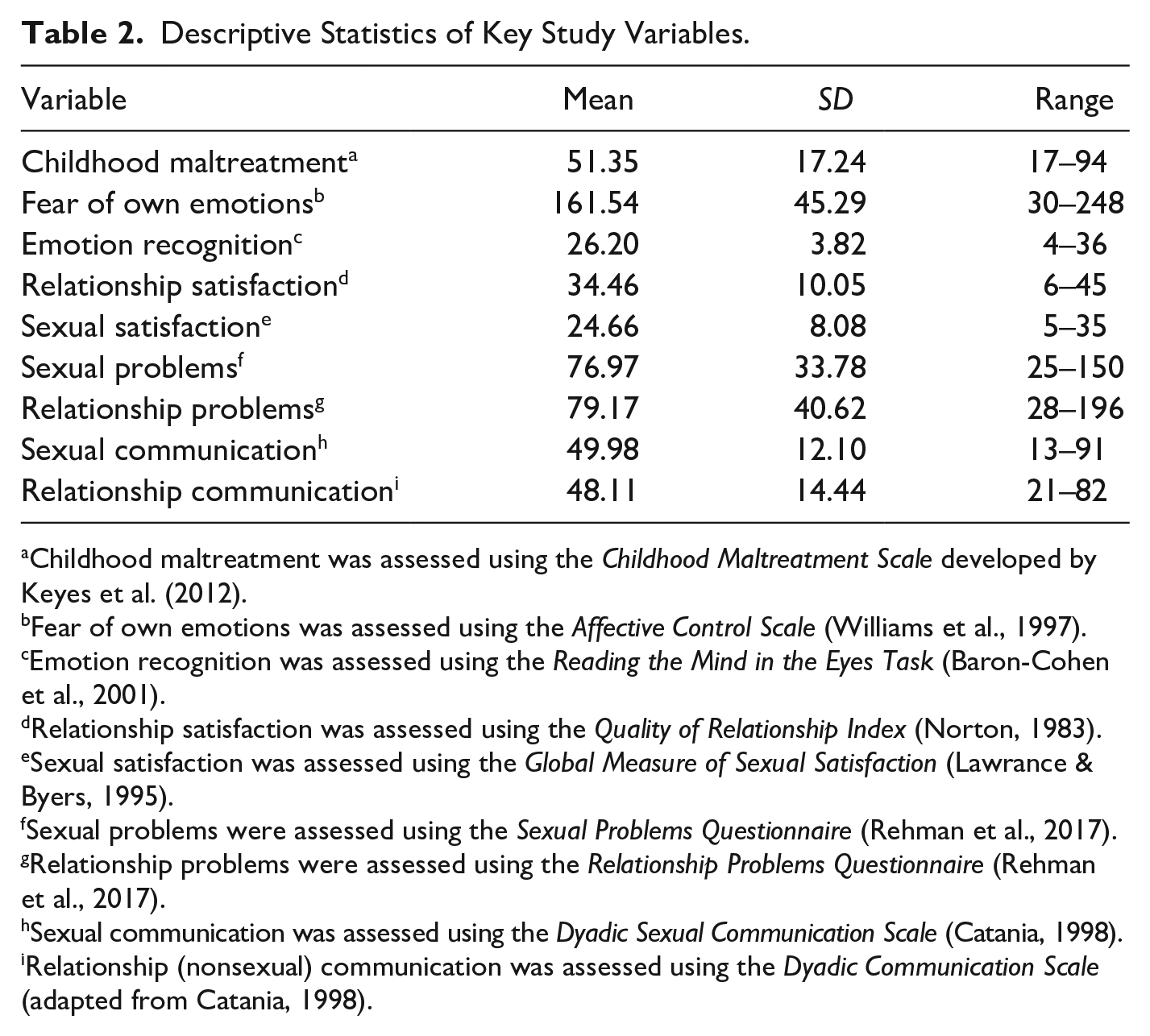
Childhood maltreatment was assessed using the Childhood Maltreatment Scale developed by Keyes et al. (2012).
Fear of own emotions was assessed using the Affective Control Scale (Williams et al., 1997).
Emotion recognition was assessed using the Reading the Mind in the Eyes Task (Baron-Cohen et al., 2001).
Relationship satisfaction was assessed using the Quality of Relationship Index (Norton, 1983).
Sexual satisfaction was assessed using the Global Measure of Sexual Satisfaction (Lawrance & Byers, 1995).
Sexual problems were assessed using the Sexual Problems Questionnaire (Rehman et al., 2017).
Relationship problems were assessed using the Relationship Problems Questionnaire (Rehman et al., 2017).
Sexual communication was assessed using the Dyadic Sexual Communication Scale (Catania, 1998).
Relationship (nonsexual) communication was assessed using the Dyadic Communication Scale (adapted from Catania, 1998).
Hypotheses 1 and 2: CM Severity Predicting Fear of Own Emotions and Emotion Recognition Skills
As an initial step, we examined the association between CM levels and (a) fear of own emotions, and (b) emotion recognition skills. We found that higher levels of CM were related to increased fear of one’s own emotions, as measured by the ACS (r = .33, SE = 0.07, p < .001). Similarly, our results suggested that higher levels of CM predicted decreased emotion recognition (r = −.25, SE = 0.08, p = .002).
CM and Interpersonal Functioning
We then examined the relationship between CM levels and the three indices of interpersonal functioning that were assessed in our study: communication. satisfaction, and problems. We examined models for both the sexual domain and the relationship in general. For each domain, we also examined whether the fear of one’s emotions and emotional recognition deficits served as a mechanism between CM and each index of interpersonal functioning.
Hypotheses 3 to 5: Emotional Processes Mediating the Link Between CM Severity and Communication
Higher levels of CM significantly predicted worse communication in both the sexual domain (β = −.36, SE = 0.07, p < .001) and the relationship domain (β = −.32, SE = 0.07, p < .001). Following these analyses, we then added ACS as a mediator of the effects for both sexual and relationship communication. The results of this mediation model are shown in Figure 1. This model showed that ACS significantly predicted lower relationship communication (β = −.19, SE = 0.08, p = .018), and sexual communication (β = −.16, SE = 0.08, p = .045). As a result, the model had a significant indirect effect for relationship communication (β = .06, SE = 0.03, p = .038) but nonsignificant effects for sexual communication (β = .05, SE = 0.03, p = .07). For both relationship and sexual communication, the direct effect of CM severity remained (sexual: β = .31, SE = 0.08, p < .001; relationship: β = .26, SE = 0.08, p = .001), suggesting that fear of own emotions does not fully account for the impact of CM severity on sexual or relationship communication.
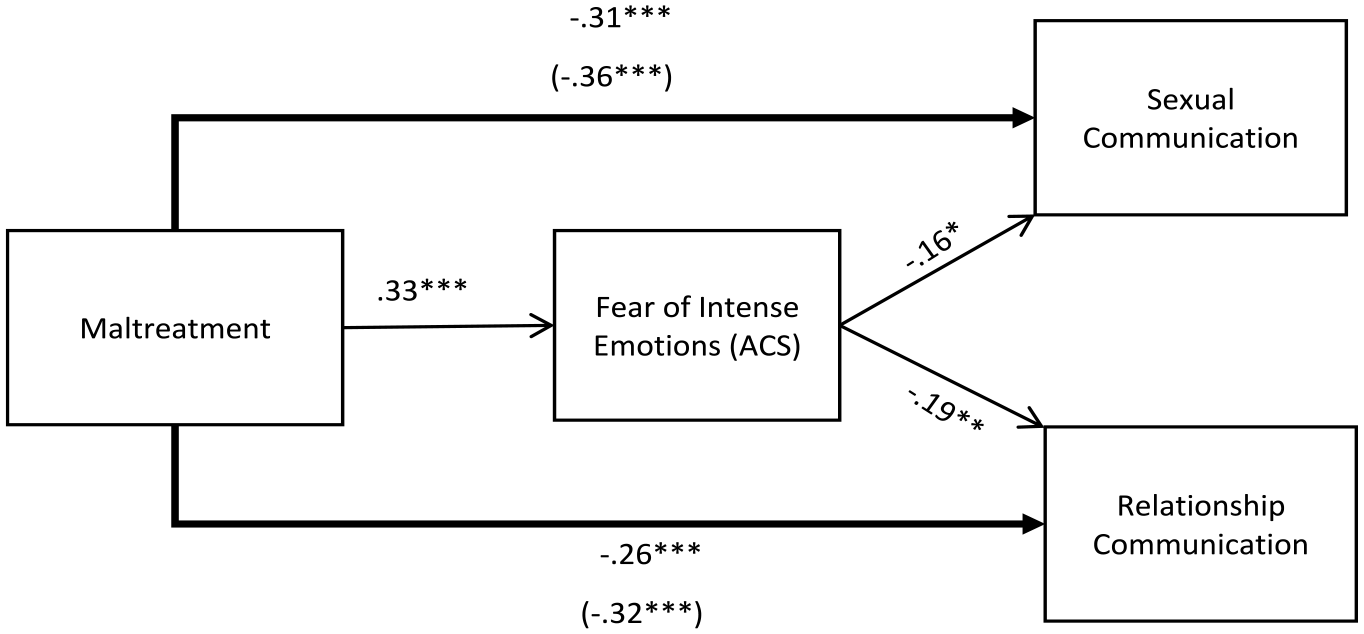
Standardized path coefficients for the mediation model. The standardized relationship between maltreatment and both communication domains is shown in parentheses.
We then tested another mediation model for emotion recognition. The results of this mediational analysis are shown in Figure 2. Emotion recognition was found to significantly predict better sexual communication (β = .19, SE = 0.08, p = .012), and better relationship communication (β = .21, SE = 0.08, p = .006). The total indirect effect was found to be significant for relationship communication (β = .05, SE = 0.03, p = .041) and sexual communication (β = .05, SE = 0.02, p = .05). Finally, the direct effect of CM severity remained significant for both sexual (β = .31, SE = 0.07, p < .001) and relationship communication (β = .27, SE = 0.08, p < .001), again suggesting that emotion recognition only partially accounts for the impact of CM severity on sexual or relationship communication.
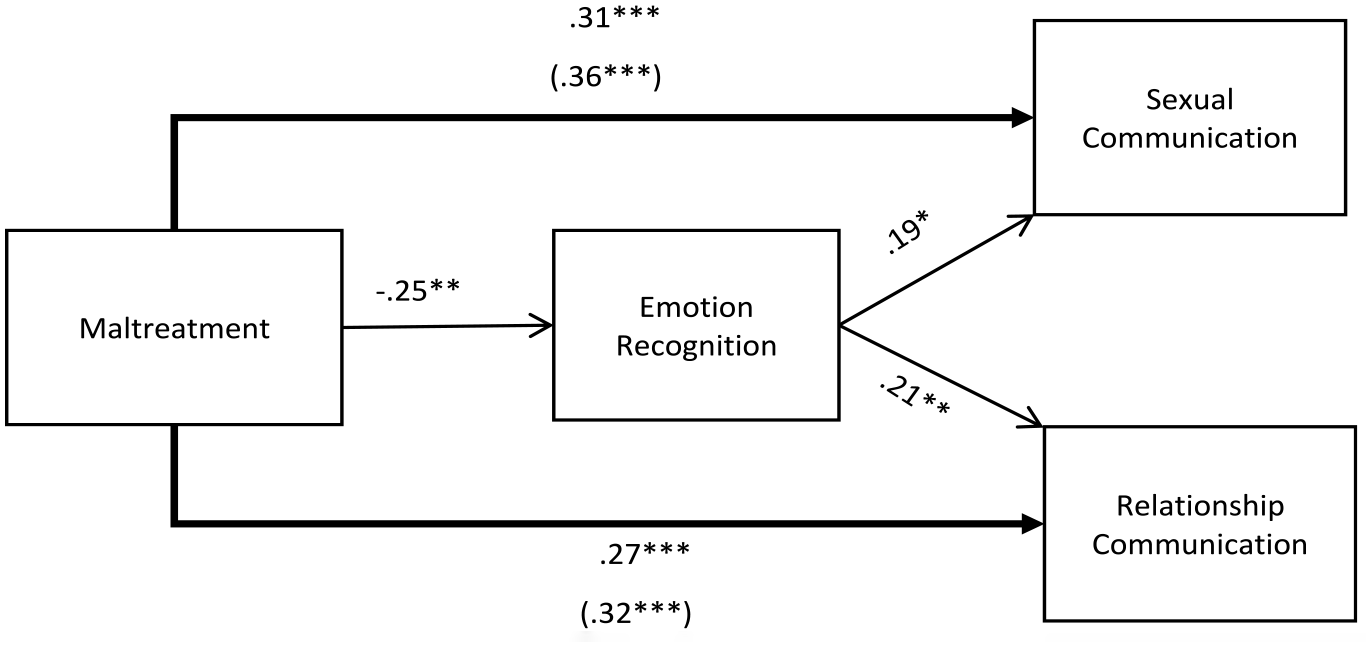
Standardized path coefficients for the mediation model. The standardized relationship between maltreatment and both domains of communication are shown in parentheses.
Hypotheses 6 to 8: Emotional Processes Mediating the Link Between CM Severity and Satisfaction
We did not find that CM levels predicted sexual satisfaction (β = .003, SE = 0.02, p = .082) or relationship satisfaction (β = −.019, SE = 0.02, p = .22). Because there was no direct effect, we did not conduct our planned mediation analyses.
Hypotheses 9 to 11: Emotional Processes Mediating the Link Between CM Severity and Problems
Finally, we examined the effect of levels of CM on perceptions of sexual and relationship problems. Consistent with our other results, higher levels of CM were significantly associated with perceiving more sexual problems (β = .23, SE = 0.08, p = .003) and relationship problems (β = .32, SE = 0.07, p < .001).
We then conducted mediational analyses using the participants’ ACS scores. Our results, shown in Figure 3, suggested that ACS scores predicted more sexual problems (β = .36, SE = 0.07, p < .001) and relationship problems (β = .52, SE = 0.06, p < .001). The indirect effect of ACS was found to significantly mediate the effect of CM severity on sexual problems (β = .12, SE = 0.04, p = .001), and it significantly mediated the effect on relationship problems (β = .17, SE = 0.04, p < .001). In this model, the direct effect remained significant for relationship problems (β = .15, SE = 0.07, p = .031), suggesting partial mediation. However, the direct effect for sexual problems was no longer significant (β = .11, SE = 0.07, p = .157).
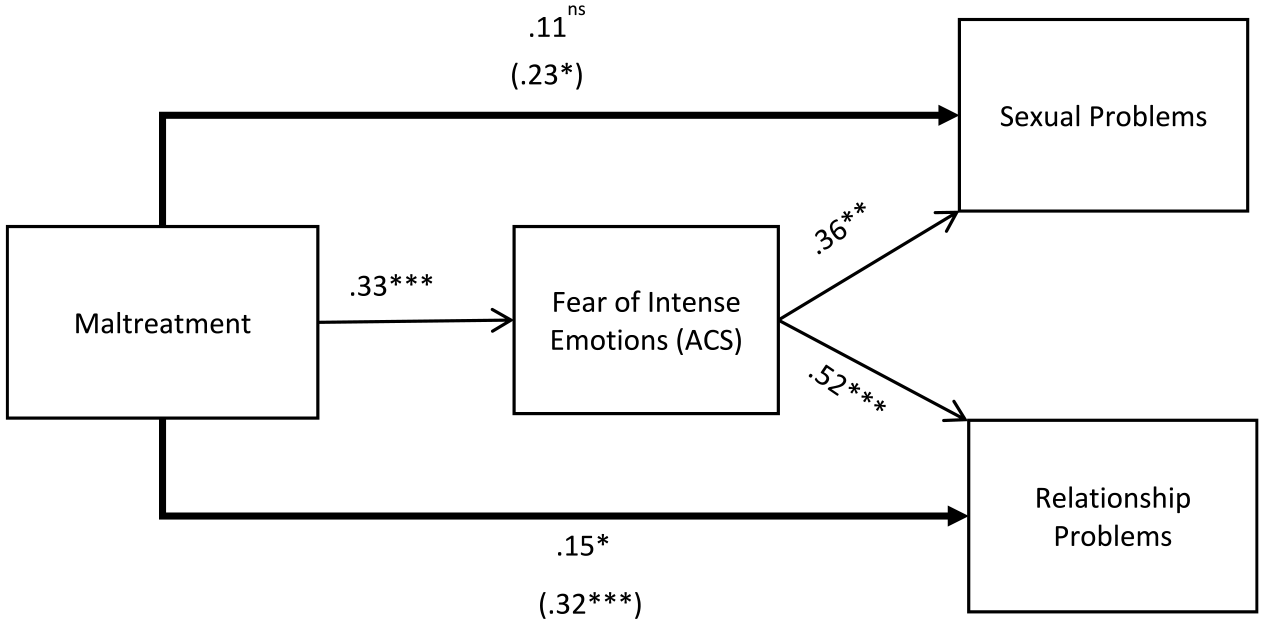
Standardized path coefficients for the mediation model. The standardized relationship between maltreatment and both domains of problems are shown in parentheses.
After examining ACS, we examined the effect of emotion recognition on sexual and relationship problems (shown in Figure 4). We did not find a significant relationship between emotion recognition and sexual problems (β = −.11, SE = 0.08, p = .194); however, emotion recognition was significantly related to less relationship problems (β = −.23, SE = 0.07, p = .001). Because the path for the sexual domain was not significant, we only examined the indirect effect for relationship problems. The indirect path for relationship problems was found to be significant (β = .07, SE = 0.03, p = .016). Taking this mediator into account, the direct effect of CM levels on relationship problems remained significant (relationship: β = .25, SE = 0.08, p = .001), suggesting a partial mediation of the direct effect.
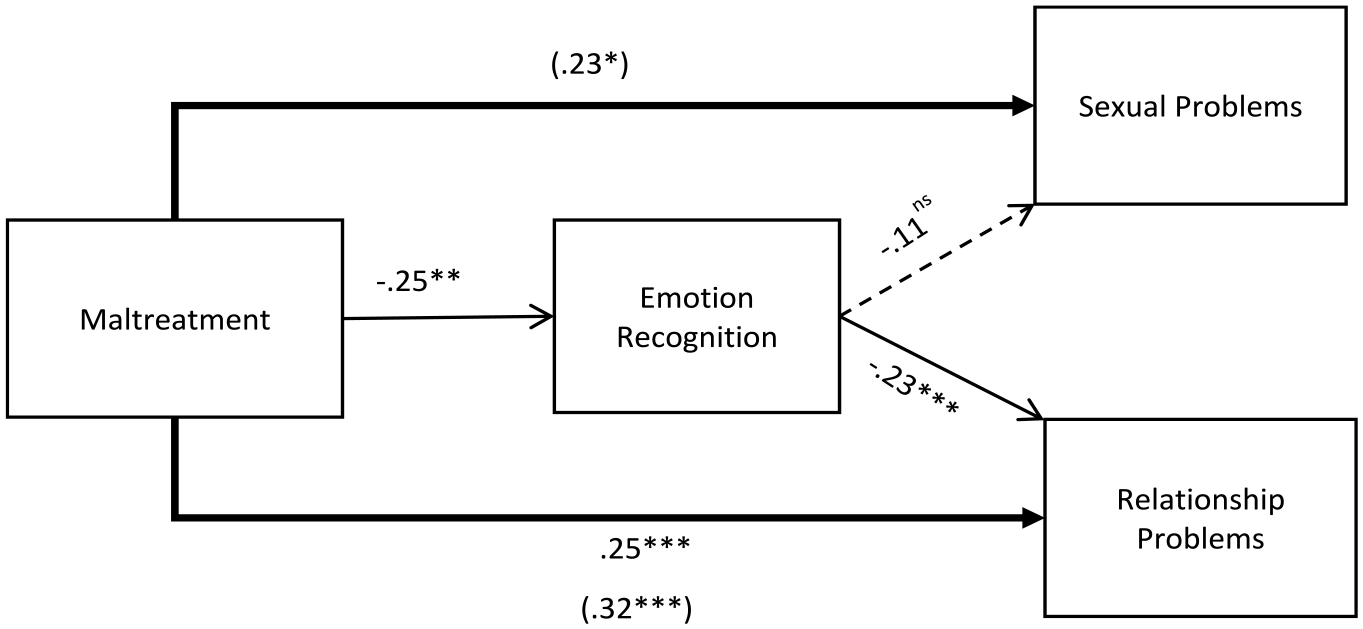
Standardized path coefficients for the mediation model. The standardized relationship between maltreatment and both domains of problems are shown in parentheses. Because the mediation model was not tested for sexual problems only the direct relationship between maltreatment and sexual problems is shown.
Discussion
One of the primary goals of this research was to replicate previous work showing that higher levels of CM are associated with lower interpersonal functioning (e.g., DiLilio and Long 1999; Leonard & Follette, 2002). We assessed three domains of interpersonal functioning: satisfaction, communication, and problems. Within each of these domains, we distinguished between sexual and nonsexual aspects of the relationship. While the domains of satisfaction and communication have been investigated in past research on CM and interpersonal functioning, we extended past research by also examining whether CM levels predict sexual and nonsexual problems in adult relationships.
Surprisingly, our results did not replicate previous findings for either sexual or relationship satisfaction. Although there have been many studies to show this link (Leonard & Follette, 2002; Rumstein-McKean, & Hunsley, 2001; Stephenson et al., 2014), there have been some studies that have not found this association in the past (for example, Alexander & Lupfer, 1987; Greenwald et al., 1990). One reason our results may differ from previous studies was that we used a dimensional measure of CM. Many of the studies have examined this question by comparing people who have and who have not experienced CM. It is possible that having experienced any CM affects future relationship satisfaction, rather than there being a linear relationship based on CM severity. It is also possible that different types of CM relate differently to relationship and sexual satisfaction.
Although we were unable to replicate the findings with the satisfaction measures, our results did suggest that higher CM levels are associated with less satisfaction with communication in both domains, replicating previous work. We also extended previous findings to show that CM levels are associated with endorsing a higher number of sexual and relationship problems. Importantly, these effects were all in the small to medium range for both domains. These results support previous findings that many survivors of CM display resilience and may not exhibit significant negative effects as a result of their experiences (Kendall-Tackett et al., 1993; Lynskey & Fergusson, 1997). Our results also underscore the importance of including multiple indicators of interpersonal functioning. Even when global impressions of the quality of the sexual and general relationship are not associated with levels of CM, as our results suggested, we found that other aspects of interpersonal functioning, specifically communication and problems, were associated with CM levels.
The second key goal of the current study was to test the theory put forward by Polusny and Follette (1995). Consistent with the predictions that would follow from this theory, we examined whether fear of own emotions and emotion recognition difficulties are responsible for the interpersonal difficulties associated with CM. Although this theory was proposed several decades ago, there has been little research that directly tested emotional avoidance as a mechanism (Walker et al., 2009). For this study we included two measures to test this theory, the first being a self-report questionnaire about fear of one’s own emotions, and the second was an emotion recognition task which allowed us to measure performance on an emotionally focused task. Our initial result showed that CM severity was associated with both fear of own emotions and weaker emotion recognition skills. This link adds to the evidence seen in children that CM is associated with decreased emotional processing. Furthermore, these results are consistent with other studies showing that these emotional processing difficulties continue into adulthood (e.g., Nazarov et al., 2014; Walker et al., 2009).
In regard to the mediation hypothesis, our results found partial support for Polusny and Follette’s (1995) theory. Specifically, our results suggested that fear of one’s own emotions partially explains why CM is associated with lower satisfaction with overall relationship communication, but not why CM levels are associated with satisfaction with sexual communication. Emotion recognition partially mediated the association between CM levels and satisfaction with sexual and nonsexual communication. In examining the association between CM, sexual and relationship problems, and emotional functioning, our results supported Polusny and Follette’s (1995) theory. Anxiety about emotions mediated the association between levels of CM and both relationship and sexual problems. The results for emotion recognition only replicated this effect for relationship problems, suggesting that difficulties with emotion recognition did not play as large of a role for sexual issues. Importantly, these findings generally found only partial mediation, suggesting there are likely additional mechanisms that could explain part of this association.
Treatment Implications
If replicated, these results provide insight into the psychological treatment for individuals with a history of CM. Our results suggest a mechanism that can be targeted in therapy. Specifically, addressing the individual’s fear of their own emotions may help improve communication and reduce the areas of conflict in a relationship.
There are a variety of treatment approaches which could help address these concerns. Our findings suggest that approaches like Emotion-focused therapy (Mlotek & Paivio, 2017) that emphasize identifying emotional experiences, differentiating between different emotional states, understanding why certain emotional experiences may be disallowed, and developing a capacity for experiencing and tolerating disavowed emotional states may be particularly beneficial for individuals who have experiences of CM. The foundational principles of Emotion-focused therapy suggest that trauma and abuse can lead an individual to lose connection with the adaptive functions of emotions. For instance, healthy anger signals to a person that the self has experienced a violation and guides the individual toward developing boundaries to protect themselves. However, individuals with CM may have had to suppress their own emotional state in order to maintain a connection with an attachment figure, leading to suppression and avoidance of certain emotional states. In the safety of the therapeutic relationship, individuals can begin to examine which emotions may have become disallowed, as a result of their developmental experiences, and how their constricted emotional response is influencing their current psychological and interpersonal functioning.
Limitations and Future Research
The first limitation is that the current study used a cross-sectional design, which limits what we can claim about the directionality of the mediation. However, it seems unlikely that relationship difficulties could affect the type of emotional processes that were investigated in the current study. Emotional avoidance and difficulties with emotion recognition are conceptualized as more primary processes and are viewed as more stable individual difference variables, as compared to relationship difficulties (Gross & Hen, 2004). However, future research using a longitudinal design could provide more support for this directionality, while also providing valuable insight about the evolution of the relationship and the development of problems over time. Ideally, this research could follow couples through multiple stages of their relationship, ranging from the formation of the relationship and extending to long-term outcomes. There also needs to be a comprehensive assessment of the range of emotional regulation difficulties in order to tease apart which aspects of emotion regulation explain greater variance in interpersonal outcomes. For example, recent research demonstrates that CM is also associated with reduced expressive flexibility, the ability to flexibly control emotional expression according to situational demands (Pițur & Miu, 2020). It is also important to note that because mental health diagnoses were not assessed in our study, the results could be due to comorbid mental health problems that survivors are experiencing. The current study was also limited because it was unable to examine the romantic partner’s perception. Relationships are by their very nature dyadic and partners of individuals with CM have rarely been included in research (Rumstein-McKean & Hunsley, 2001). A final limitation that we would like to note is that participants had to self-select as having experienced physical or sexual abuse to be included in our study. The rationale for this decision is that we wanted to focus on levels of CMA, rather than comparing groups on presence/absence of CMA. However, this inclusion criteria may have led to a lower sampling of individuals whose experiences of CMA consisted only of emotional abuse or physical or emotional neglect and the observed pattern of results may not generalize to such groups. In future work investigating emotional processes in CMA, it would be advisable to use broader inclusion criteria to ensure that findings generalize to a full spectrum of CMA experiences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported in part by funding from the Social Sciences and Humanities Research Council.