
Abstract
Previous intimate partner violence research and social psychological theory have highlighted that ethnicity and level of harm are both factors that have the potential to influence bystander willingness to intervene in, as well as the acceptance of intimate partner violence between couples. Little research has been conducted on the general willingness of bystanders to intervene in, or the level of acceptance of coercive control. This is the first study to explore whether the likelihood of bystander willingness to intervene is influenced by participant gender, the ethnicity of the couple involved in a hypothetical scenario of coercive control, and by differing levels of abusive behavior. In this study, we also explored the influence of participants’ acceptance of coercive control. A semi-experimental design was used, utilizing an online community sample sourced through social media of 346 adult participants across Australia. The participants were randomly allocated to read a fictional coercive control scenario detailing either low or high harm instances of coercive control. Within the online survey the ethnicity of the couple was manipulated with participants’ randomly allocated to read a scenario about a couple with the same ethnicity as them (Australian of British or European descent) or a couple with Indian Australian ethnicity. The results showed the participants were significantly more willing to intervene in the coercive control scenario when the couple shared the same ethnicity as them. In response to the low harm scenarios, participants were significantly more accepting of coercive control if the couple were Indian Australian. However, males responding to high harm scenarios were more accepting of coercive control if the couple shared the same ethnic identity as them. The implications from these findings for theory and future bystander intervention programs are discussed.
Keywords
Introduction
Coercive control (CC) is a specific form of intimate partner violence (IPV) used by a perpetrator to control their partner/former partner. It is a systematic pattern of behavior involving intimidation, isolation, and fear-inducing violence or threats of violence to establish dominance over their victim (Crossman & Hardesty, 2018). The framework of CC captures the non-physical, enduring nature of abuse that erodes the victim’s self-esteem and personal life (Barlow & Walklate, 2021). Women who experienced CC reported higher frequencies of each form of IPV, and increased levels of danger compared to survivors of IPV who did not (Dichter et al., 2018). Furthermore, CC has been found to predict post-separation violence, sexual assault, and intimate partner homicide (Monckton Smith, 2020; Stark & Hester, 2019).
While the real-life implications of CC victimization have been documented, conducting research into bystander prevention and intervention strategies for CC has been challenging (Fenton et al., 2019). As the United Kingdom and Ireland are the only countries with current legislation against CC (Stark & Hester, 2019), and legislation varying between the states and territories in Australia (McMahon et al., 2019), there are inconsistencies in the criminalization of CC across countries. Furthermore, despite the implementation of CC legislation, difficulties for police and prosecution services arise due to issues in recognizing and responding to evidence of CC which hinders effective intervention (Lagdon et al., 2022).
Bystander Intervention Model
Previous research into bystander intervention in IPV has utilized the bystander intervention model (BIM) developed by Latane and Darley (1970), which outlines the process of intervention through five steps: (1) noticing the event, (2) identifying the event as an emergency, (3) assuming responsibility to act, (4) deciding how to intervene, and (5) implementing the chosen intervention (Weitzman et al., 2017). Additionally, Latane and Darley (1970) introduced the notion of the “bystander effect,” using the concepts of diffusion of responsibility, ambiguity, and group cohesiveness, to explain factors that may prevent individuals from effectively moving through the process of intervention. When in the presence of others, the responsibility of intervening becomes shared, with individuals often assuming another bystander will help, reducing the likelihood they intervene themselves (Latane & Darley, 1968). Additionally, bystanders are less likely to intervene in an ambiguous situation, whereby it is unclear that help is warranted or necessary (Latane & Darley, 1968). The need to behave in accordance with group and social norms can lead to group cohesiveness, subsequently in bystander situations when other observers do not react, the rest of the group take this as an indication that a response is not required (Rutkowski et al., 1983).
The utility of the BIM has been examined in previous research, particularly in situations of IPV or sexual assault. Katz et al. (2017) conducted a vignette study with 160 Caucasian United States (US) college students to investigate whether their willingness to intervene in an incapacitated sexual assault scenario differed if the potential victim was African American or of an unspecified racial background. They found that participants who were randomly assigned to read the scenario where the victim was African American, reported less intent to intervene, and felt less personal responsibility to intervene (Katz et al., 2017). But increasing the level of harm in an emergency situation has been found to increase the likelihood an individual will move through the steps of the BIM, ultimately enhancing willingness to intervene (Bennett et al., 2017; Fischer et al., 2006). However, little is known about the applicability of the BIM in instances of CC, and while people appear willing to intervene and help a victim in an IPV situation (Bennett et al., 2017) further research is necessary to investigate whether people would show a similar level of intent to intervene in a CC situation. Further research is also necessary on whether barriers to intervention that have been identified in IPV research are relevant to situations of CC.
The Influence of Social Factors on Willingness to Intervene
In previous IPV research (Katz et al., 2017), social factors such as ethnicity had a significant impact on an individual’s willingness to intervene. Research into whether the same effect on an individual’s willingness to intervene in a CC situation is warranted and would be an important step in informing bystander intervention programs. The social identity approach analyses the role of group membership and external situations in influencing the behavior and attitudes of individual members within a group (Hogg & Reid, 2006), and therefore provides an appropriate theoretical underpinning for the potential barrier social identities may play in willingness to intervene in CC.
Social identity theory (SIT) suggests that people gain part of their self-concept from their group memberships, with social identification being high in emotional and value significance to the individual (Hogg & Reid, 2006). Self-categorization theory furthers SIT by proposing that group identification creates norms and cognitive representations that prescribe ingroup behavior, resulting in those who do not fit within the scope of the ingroup being considered the “outgroup” (Turner & Onorato, 2010). The process of social categorization is based upon the use of prototypes, which conceptualizes groups by a vague set of key attributes associated with that particular group (Hogg & Reid, 2006). While these categorical representations of others are used to capture similarities among people in the same group, they are also used to accentuate differences between groups, often resulting in the depersonalization of others when they are viewed through the lens of their relevant group prototype (Turner & Onorato, 2010). The ingroup and outgroup demarcation has real-life consequences in that individuals afford different emotions and behaviors to ingroup and outgroup members (Xiao et al., 2016).
Additionally, ingroup favoritism emphasizes that individuals afford more positivity to the ingroup compared to the outgroup, particularly regarding helping behaviors (Brewer, 1999; Mower, 2015). Ethnicity has been found to be one main basis for ingroup identification, especially for minorities and migrants (Smeekes & Verkuyten, 2013). Consequently, there is the possibility that when an individual views someone from a different ethnic group to their own as an “outgroup” member, this may reduce their willingness to intervene in emergency situations such as CC.
Acceptance for CC
Attitudes toward IPV, such as the belief that IPV is a private matter, or acceptance of IPV, for example the perception of such behaviors as normative, are a key factor in reducing the likelihood of bystander intervention in IPV (Weitzman et al., 2017). Research has identified negative correlations between willingness to intervene in IPV against women (IPVAW) with acceptability for IPVAW, victim-blaming and hostile sexism (Gracia et al., 2018). Sociodemographic factors, such as gender, have been found to influence level of acceptance for IPV, with research identifying being female was predictive of lower acceptability in attitudes toward IPV (Herrero et al., 2017). Males have been found to be more likely to use a victim’s potential infidelity to blame her for victimization, as well as more willing to blame victims for remaining in an abusive relationship (Eigenberg & Policastro, 2016).
Cross-cultural differences in attitudes toward IPV have also been identified, with ethnic minority students in the United States showing higher acceptance of IPV, possibly a result of differences in cultural values and norms (Zark & Satyen, 2021). Given that CC is a specific form of IPV, it is likely that these factors would elicit similar effects on an individual’s attitudes toward CC. Additionally, research correlating the perception of acceptability and level of aggression in IPV vignettes uncovered that scenarios displaying lower levels of aggression were perceived as more acceptable (Ramsey, 2017). Therefore, if level of aggression can be equated to level of harm, where a high level of harm results from higher aggression, it is likely that manipulating the level of harm in a CC scenario would result in lower ratings of acceptance in a high harm situation and vice versa. Furthermore, while community attitudes are generally intolerant of IPV (Webster et al., 2018), further research is necessary to investigate whether there is a similar level of intolerance in community attitudes toward CC.
The Current Study
In the current study, a semi-experimental approach was used with participants randomly allocated to read a vignette detailing a hypothetical example of a CC scenario. Then to examine how likely participants would be to intervene in this scenario, the ethnic identity of the couple and the level of harm were manipulated across scenarios, to examine whether those variables significantly influenced respondent’s willingness to intervene in that situation and their acceptance for CC. Participants read a scenario about a couple with the same ethnic identity as them to ensure they were perceived as the ingroup, or a different ethnic identity so they were perceived as outgroup members. The level of harm was manipulated across scenarios to describe either a low or high harm incident of CC.
Willingness to Intervene
Previous research has highlighted strong correlations between age and gender in willingness to intervene, whereby older participants are more willing to intervene, and men are more likely to directly intervene in IPV; therefore, those variables will be controlled for in the analysis (Palmer et al., 2018; Wijaya et al., 2022).
Hypothesis 1: Participants will be more willing to intervene in CC if the couple involved shares the same ethnic identity as them, compared to if the couple has a different ethnic identity.
Hypothesis 2: Participants will be more willing to intervene if the scenario describes a higher level of harm (e.g., more aggressive) compared to a low harm scenario.
Acceptance for CC
As previous research has found that age influences acceptance for IPV (Sánchez-Prada et al., 2020), we controlled for age in the analysis.
Hypothesis 3: Males will be more accepting of CC compared to females.
Hypothesis 4: Participants who read the outgroup scenarios will be more accepting of CC in comparison to those who read the ingroup scenarios.
Hypothesis 5: Participants who read the low harm scenarios will be more accepting of CC compared to those who read the high harm scenarios.
Method
Participants
Participants were a community sample of Australian adults, aged over 18, who were citizens or residents of Australia and of British or European descent. Of the 346 participants included in the final sample, 103 identified as male, and 243 as female, with an age range of 17 to 77, M = 40.8, SD = 14.74. In terms of education, 56% of participants had attained an undergraduate degree or higher, 7.6% had completed year 10, 17.9% had completed year 12 and 18.5% had completed a TAFE or Trade apprenticeship. About half (53.8%) of participants stated that they were employed full time, 22.4% were part time or casually employed, 6.7% were students, 14.8% were retired or a primary caregiver, and 2.2% were unemployed.
Measures
Demographics of age, gender, ethnicity, education, region, and employment were collected. To investigate the influence of ethnic identity and level of harm on (1) willingness to intervene in and (2) acceptance for CC, participants were randomly allocated to read one of four vignettes describing a CC situation, which was based on a combination of victim survivor stories of CC sourced online and incorporating tactics specific to CC. The vignettes presented participants with a hypothetical story of a couple in a CC situation, with vignettes differing based upon the ethnicity of the couple or the level of harm of CC. The participants were asked to imagine the couple as people, who had been their neighbors for the last 5 years, to create some level of familiarity. The two different ethnic groups were British/European Australian, for the “ingroup” condition as this ethnic group matched that of the individual’s recruited for the study, and an Indian couple who had recently migrated to Australia for the “outgroup” condition. The low harm vignette details CC tactics of emotional abuse, financial abuse, social isolation, and technological monitoring, with the high harm vignette essentially identical to the low harm vignette, except for the addition of the threat of physical violence to increase the perceived level of harm. Therefore, the four vignettes were Australian-high harm, Australian-low harm, Indian-high harm, or Indian-low harm (please contact the corresponding author for examples of the vignettes used in this study). A manipulation check was used to ensure participants read the vignette thoroughly, with a question asking them to identify the names of the couple in the scenario and a second question asking whether a threat of physical violence was present to ensure participants were correctly identifying the level of harm.
Willingness to Intervene
Willingness to intervene was measured using an adapted scale from the measurement of the BIM for bullying and sexual harassment developed by Nickerson et al. (2014), based on Latane and Darley’s (1970) BIM. The Nickerson et al. (2014) scale was adapted by removing items not relevant to CC situations and rewording items to reflect the content of CC vignettes. The 13-item willingness to intervene scale used in this study asked participants to rate, on a scale from one “strongly disagree” to five “strongly agree,” whether they would intervene, for example item five “After reading about Raj and Priya/Jack and Amelia, I feel that I should intervene and help in this situation.” Item 13 was modified to match the level of harm of the vignette the scale followed. Therefore, the high harm conditions asked participants to respond to “I would not get involved myself, but I would involve someone else that is, the police, to stop Raj/Jack being domineering toward Priya/Amelia,” and in the low harm condition, relationships Australia was used as an example of an external resource for intervention instead of the Police. A mean composite score was created from all items, to indicate overall willingness to intervene on a scale of one to five, which displayed good internal reliability (Cronbach’s α = .79).
Acceptance of CC
An adapted version of the acceptability of IPVAW scale developed by Martín-Fernández et al. (2018) was used to measure acceptance of CC. Original items regarding physical or sexual violence were removed and only the items relating to CC were used in this study. The 12-item scale used asked participants to “please rate how acceptable or unacceptable you believe the following behaviors are for a man” from one “unacceptable” to five “acceptable,” to each item. An example of an item is (Item 4) “to set limits on where his partner goes.” A mean composite score was created from these items, whereby total acceptance for CC was represented on a scale of one to five, which demonstrated good internal reliability (Cronbach’s α = .89).
Procedure
The study was approved by a University Human Research Ethics Committee and the participants were recruited through social media. The study was advertised on social media platforms, specifically Facebook, Quora, and Reddit, with participants who had completed the survey being asked to share the survey on with others. This study was advertised to Australian residents of British or European descent to ensure the manipulation of ethnic group (ingroup vs. outgroup) across vignettes would be effective. The study was advertised as an investigation into people’s attitudes regarding couple relationships, and the behaviors they consider acceptable in response to a hypothetical scenario, to avoid priming participants on the fact this study was investigating CC. The chance to win one of four $25 shopping center vouchers was included as incentive to participate in the study. Participants were randomly allocated to one of the four vignettes, and subsequently asked questions for the manipulation checks to ensure participants had read and understood the scenario they were allocated to. Participants then completed the willingness to intervene scale followed by the acceptance for CC scale, with participants being reminded at the beginning of each scale they were not required to answer any questions they were not comfortable with. Finally, after completing both scales, participants were fully debriefed about the study and how they were randomly allocated to read different vignettes.
Results
Data Screening and Preliminary Analysis
Data analysis was completed using IBM SPSS Statistics (Version 28). There were 606 people who responded to the survey advertisement; however, after data screening and cleaning, the final sample comprised of 346 participants. Participants who did not identify as Australian of British or European descent were excluded (n = 63). Cases were removed where a substantial amount of missing data was observed (only demographics were answered, n = 168) and had failed to answer either of the manipulation checks correctly (n = 7). Eleven participants identified as LGBTQI+ or chose not to disclose gender and were excluded from analysis as the group size was too small to meet equal variance.
Data were screened which confirmed all responses were within the appropriate range. Preliminary analysis revealed a small significant negative correlation between acceptance for CC and willingness to intervene r = −.28, p < .001, indicating those who were more willing to intervene in the CC scenario were less accepting of CC, which was in the expected direction given the previously identified negative correlation between acceptance for IPV and willingness to intervene (Gracia et al., 2018).
Preliminary analysis was conducted to assess how willing participants were to intervene in the CC scenario and how accepting they were for the CC scenario across conditions. A one-sample t-test revealed that the mean willingness to intervene score (M = 3.9, SD = .53) combining all CC scenarios was significantly higher than the midpoint of scale at three t(355) = 31.85, p < .001, d = .53. A one-sample t-test comparing the mean acceptance score (M = 1.29, SD = .45) for CC combining all conditions to the midpoint of three found that acceptance was significantly lower than the midpoint t(351) = −71.73, p < .001, d = .45.
Willingness to Intervene
A 2 × 2 between-group ANCOVA was conducted to assess H1, whether the level of harm of CC and H2, whether the ethnicity of the protagonist (Australian vs. Indian) affected an individual’s willingness to intervene in a CC scenario, controlling for gender and age. A visual inspection of the data using histograms and inspection of descriptive statistics indicated the assumptions of normality for the ANCOVA were met. Levene’s test was not significant (p = .43), demonstrating the assumption for homogeneity of variance was met. Inspection of box plots of willingness to intervene split across conditions identified three potential outliers; however, upon inspection of z-scores and 5% trimmed means, these outliers were determined to have little influence on the mean score. 1 The point-biserial correlation between the covariates of age and gender was weak (r = .203, p < .001), and all covariates displayed reliability and were measured prior to the experimental manipulation. Visual inspections of scatterplots displayed a linear relationship between the dependent variable and all covariates, as well as homogeneity of all regression slopes.
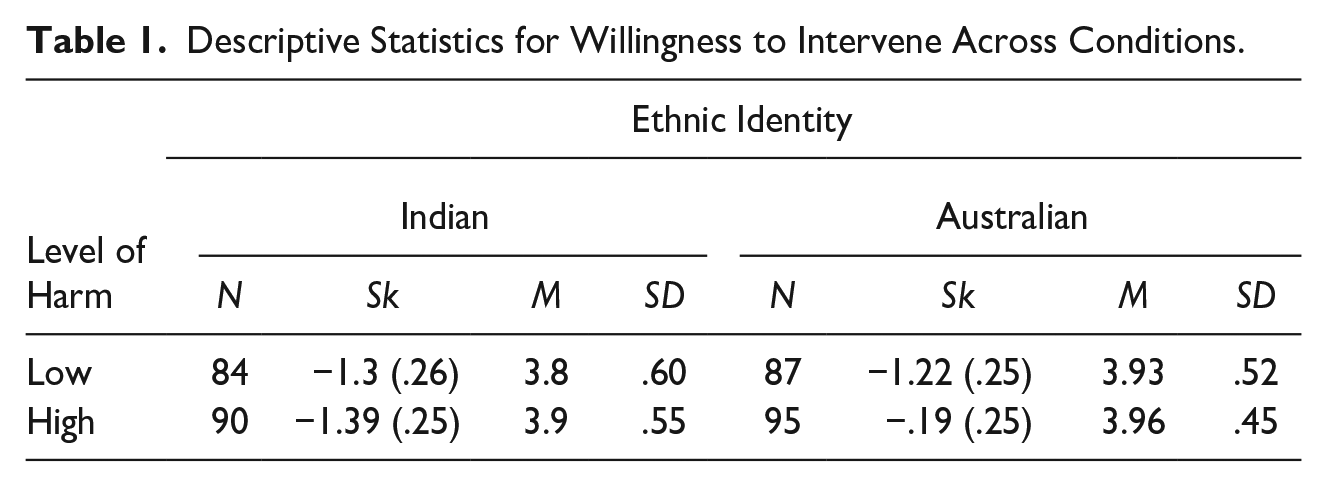
With a critical alpha set at α = .05 for all analyses, the ANCOVA showed a significant main effect of ethnicity on willingness to intervene F(1, 336) = 6.28, p = .013, with a small effect size (ηp2 = .018). Consistent with H1, these results indicate that participants who read the CC scenario involving an Indian Australian couple (M = 3.8) were significantly less likely to intervene than those who read the scenario involving the Australian couple of British/European descent (M = 3.95). However, contrary to H2, the main effect of level of harm was not statistically significant F(1, 336) = 1.59, p = .21, ηp2 = .005 (see Table 1 below for descriptive statistics).
Descriptive Statistics for Willingness to Intervene Across Conditions.
Acceptance for CC
A 2 × 2 × 2 between-group ANCOVA was performed to assess whether H3 gender, H4 ethnicity of the couple, and H5 the level of harm of CC affected the level of acceptance for CC, controlling for age. The assumption of normality was found to be violated after visual inspection of histograms, as the data were positively skewed. However, given the large sample size (n > 200), ANCOVAs are robust to violations of this assumption (Pallant, 2016), and given the expectation that acceptance for CC would be a positively skewed variable (assuming the general population would rate CC as unacceptable) the choice of ANCOVA for analysis was retained. A significant Levene’s test indicated the assumption of homogeneity of variance had been violated; however, given the size of the groups are relatively similar (largest/smallest = 1.05), and the robustness of ANCOVA against violations of this assumption, homogeneity of variance was assumed (Pallant, 2016). 2 Descriptive statistics for acceptance of CC are shown in Table 2.
Descriptive Statistics for Acceptance for Coercive Control Across Conditions.
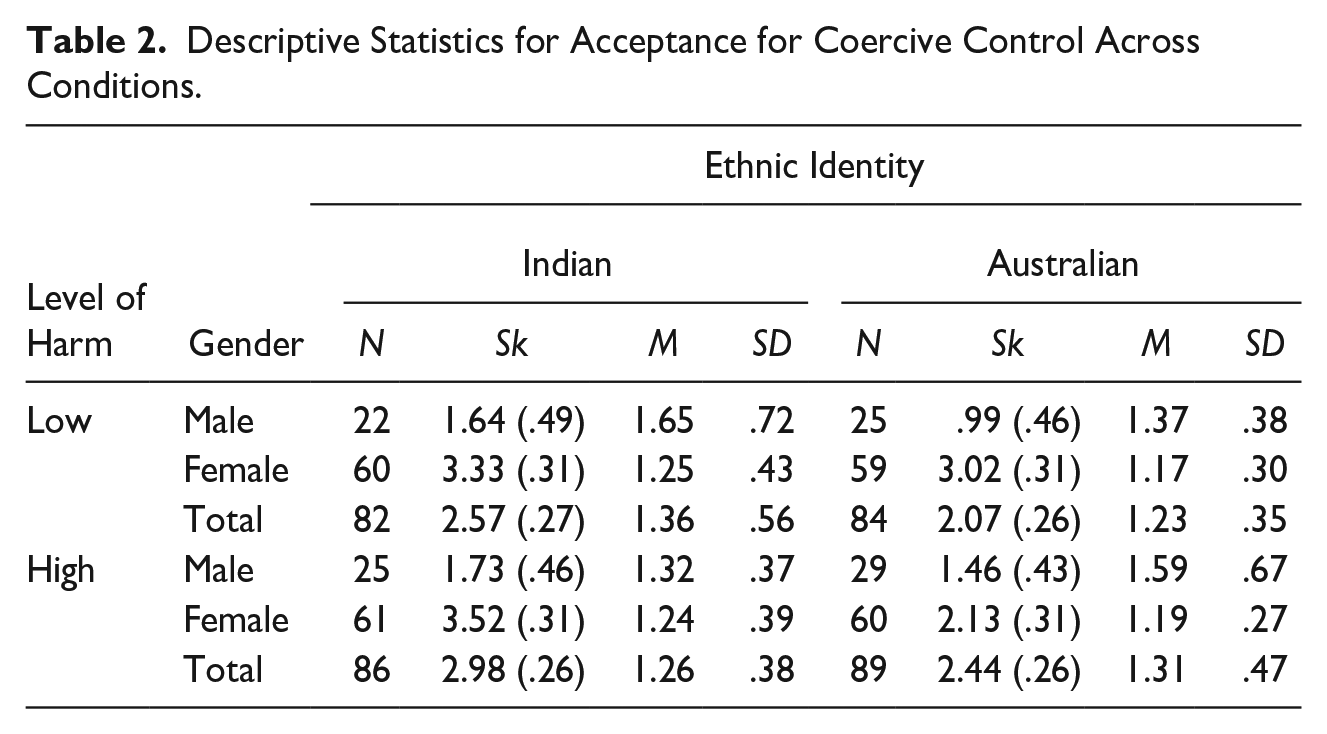
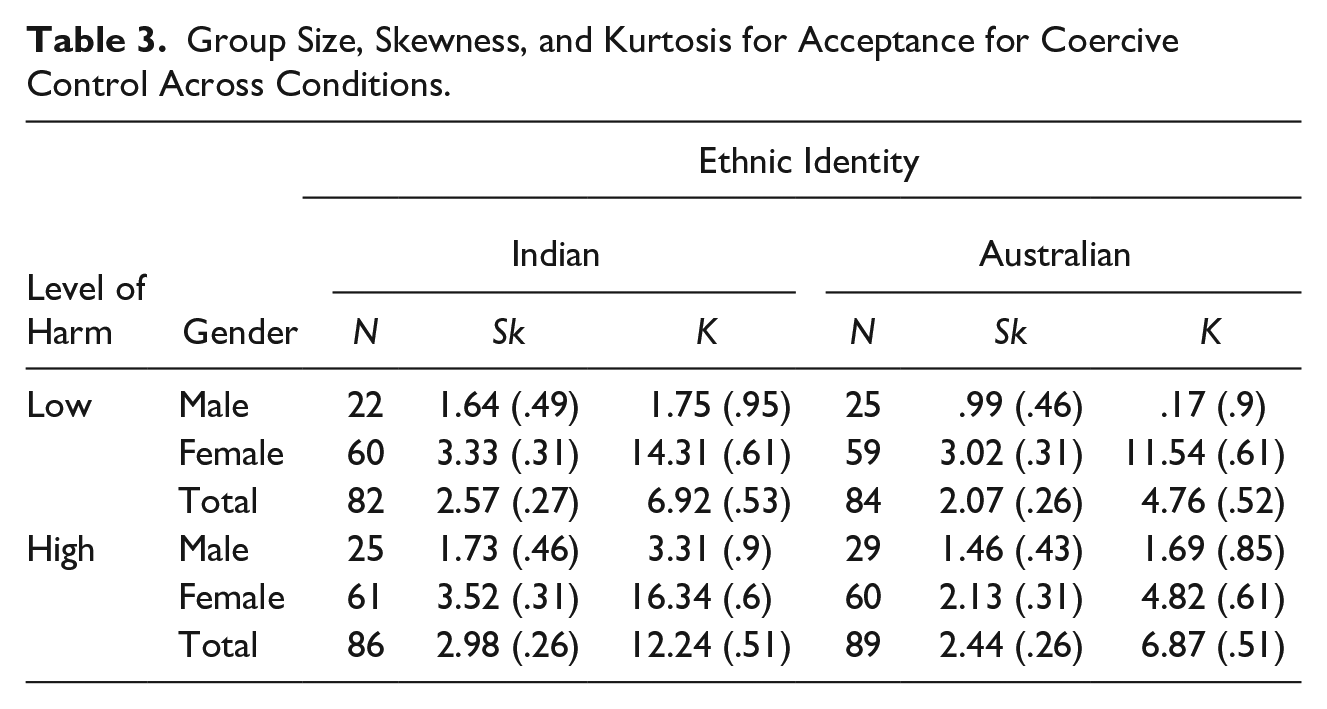
The ANCOVA revealed significant main effects of age 3 F(1, 332) = 10.17, p = .002, ηp2 = .03, and gender F(1, 332) = 21.35 p < .001, ηp2 = .06, indicating that those who were older were less accepting of CC, and consistent with H3, indicating that females were less accepting of CC. Significant interactions were identified between the level of harm and ethnicity variables F(1, 332) = 7.8 p = .006, ηp2 = .023, as well as a three-way interaction between gender, level of harm, and ethnicity F(1,332) = 7.13, p = .008, ηp2 = .021. Post hoc pairwise comparisons of the interaction between the level of harm and ethnicity showed that participants who read the low harm scenarios were significantly more accepting of CC if the couple were Indian compared to the Australian condition F(1,332) = 5.36, p = .021, which was consistent with H4. However, no significant results were found to support H5 (refer to Table 3).
Group Size, Skewness, and Kurtosis for Acceptance for Coercive Control Across Conditions.
Further ANCOVAs with the sample split by gender were conducted to analyze the three-way interaction between gender, level of harm, and ethnic identity. Through comparison of the ANCOVAs for the male and female sample, a significant interaction between level of harm and ethnic identity was found for the male sample F(1, 96) = 6.29, p = .014 (see Figure 1 below). Pairwise comparisons revealed the significant difference was found in the high harm condition, where males were more accepting of CC for the British/European couple compared to the Indian couple F(1, 96) = 3.68, p = .05, and no significant differences were found in the low harm condition F(1, 96) = 2.68, p = .105. However, this interaction was not present in the female sample F(1, 235) = .04, p = .836, where instead higher acceptance for CC was reported for those who had read about the Australian Indian couple (M = 1.25) compared to the Australian couple of British/European descent (M = 1.18), irrespective of whether they were allocated to the low or high harm condition, but the difference was not significant.
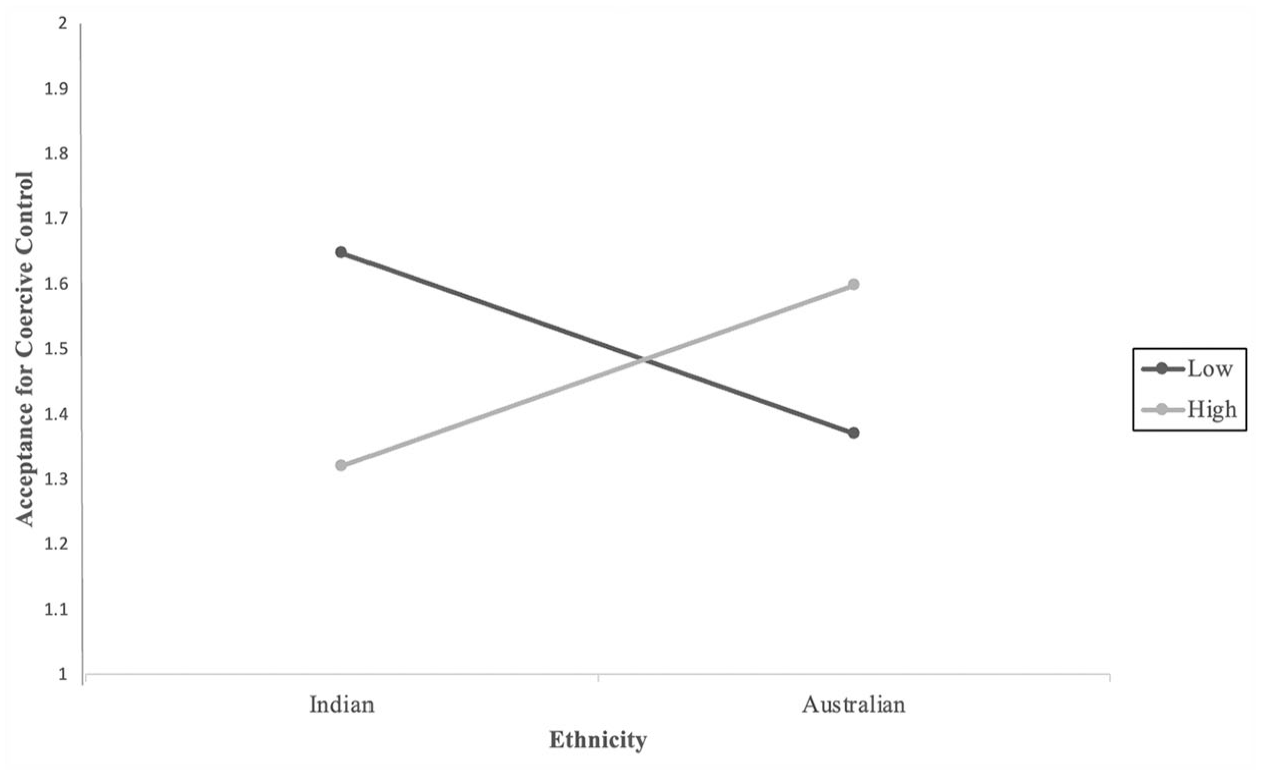
The interaction between level of harm and ethnicity on acceptance for CC for males.
Discussion
This study sought to assess whether differences in ethnicity and level of harm embedded in the scenario would influence levels of acceptance or willingness to intervene in CC. H1 was partially supported in that participants reported they were more willing to intervene in the CC vignette if the couple shared the same ethnic identity as them. No support for H2 was found, as there was no significant difference in willingness to intervene across the levels of harm. H3 was partially supported as males were more accepting of CC than females; however, the interactions between ethnic identity, level of harm, and gender revealed unexpected results with mixed support for the hypotheses. An interaction between level of harm and ethnic identity provided some support for H4, where participants were more accepting of CC if they had read the outgroup scenarios, in the low harm condition. However, no main effects were found for the level of harm, providing no support for H5. Conversely, for males, an interaction between level of harm and ethnic identity was present, where those who read the low harm scenario were more accepting of CC if the couple were Indian Australian; however, for the high harm scenarios, they were more accepting of CC if the couple were Australian of British/European descent.
While previous research has identified the utility of the BIM in predicting willingness to intervene in situations of IPV (Fischer et al., 2006), the findings from this study have highlighted the utility of BIMs to predict willingness to intervene, specifically for CC. Moreover, despite community attitudes being generally intolerant of IPV (Webster et al., 2018), no published research could be located that measured rates of acceptance toward behaviors specific to CC. Given that CC focuses on the non-physical aspects of abuse, such as social isolation, and technological monitoring (Harris & Woodlock, 2018), there was the potential that these behaviors could be perceived as more acceptable in comparison to acceptance rates for physical or sexual violence. However, results from this study found that most participants rated CC behaviors as unacceptable.
Factors Influencing Willingness to Intervene
Furthermore, by manipulating the ethnic identity of the couple involved in the CC scenarios, this study was able to detect the effect ethnic differences can have on an individual’s willingness to intervene. Similar to the Katz et al. (2017) findings revealing the influence of ethnicity on intent to intervene in a sexual assault scenario, the findings from this study showed that ethnicity may also act as a barrier to intervention in CC. These findings provide further support for the influence of SIT and subsequent ingroup favoritism, finding that individuals are significantly more likely to intervene in a CC scenario when the couple are perceived as ingroup members (Brewer, 1999; Mower, 2015).
However, no significant difference between the levels of harm on willingness to intervene in CC was identified, a surprising result given previous research highlighting that perceiving the situation as an emergency would increase willingness to intervene in line with the BIM (Fischer et al., 2006). The lack of difference in willingness to intervene across levels of harm may have occurred if participants perceived the scenarios similarly as emergencies warranting intervention, regardless of the inclusion of the threat of physical violence. However, while the differing levels of harm did not influence willingness to intervene in the manner that was expected, these results highlight that even without the threat of physical violence, participants identified the CC scenario as an emergency scenario that warranted intervention.
Factors Influencing Acceptance for CC
Regarding factors influencing acceptance for CC, this study identified a significant effect of gender. Previous research has identified associations between gender and acceptance for IPV, having found men were more approving of both female and male perpetrated IPV in comparison to females (Spencer et al., 2021). However, this study was able to uncover the influence of gender on acceptance specifically for CC, finding that men, while still rating CC behaviors as largely unacceptable, were significantly more accepting in comparison to females. Positive associations between acceptability of general violence and sexism, with acceptability of IPV have been identified, and as men have been found to be more likely to endorse sexism or violence (Herrero et al., 2017), it is possible these factors also contributed to males’ higher acceptance for CC.
Further differentiation in levels of acceptance for CC across genders was also identified, as the interaction between ethnicity and level of harm on acceptance varied between genders. For females, there was no interaction between ethnicity and level of harm on their level of acceptance for CC. Conversely, when looking at the effects of ethnicity and level of harm on acceptance of CC for males, an interaction between ethnicity and level of harm was uncovered. This interaction showed that males who read the low harm scenarios were more accepting of CC if the couple were Indian Australian (outgroup). This difference in acceptance could potentially be explained by SIT, as strong ingroup identification has been associated with intergroup differentiation and stereotypic perception (Kelly, 1993). Consequently, participants who read the outgroup scenarios may have rated the CC as somewhat more acceptable compared to the ingroup respondents, as they may have stereotyped those behaviors to be normative for the outgroup (Hagendoorn, 1993).
However, unexpectedly for males who read the high harm scenarios, they reported higher acceptance of CC if the couple were British/European Australian (ingroup) compared to the Indian Australian (outgroup) scenario. This was contrary to the hypothesis that participants would be more accepting of CC for the outgroup and low harm conditions. However, attribution theory may be of explanatory value for this finding, as it is possible that there was a preference for ingroup serving attributions, and less internal attributions for the negative acts of the ingroup were made when compared to the outgroup, due to ultimate attribution error (Hewstone, 1990). Consequently, participants may have overestimated the situational factors and underestimated the personal factors as causes for the CC behavior in the ingroup scenarios (Hewstone, 1990), subsequently rating those behaviors as more acceptable. Parallels between these findings can also be drawn with other research, as one study found that when other ingroup members behaved immorally, motivation to maintain a moral group image can result in increased threat and defensive behaviors, and that participants were more defensive in response to ingroup moral failure compared to the outgroup (van der Toorn et al., 2015). Additionally, individuals who strongly identify with their ingroup have been found to engage in morally disengaging perspective taking with the perpetrators (Li et al., 2020). Therefore, if participants did in fact regard the high harm CC scenario to be immoral behavior, or highly identified with the ingroup, there is the possibility that they responded defensively by rating those behaviors as more acceptable in the ingroup condition, and as less acceptable for the outgroup. Additionally, it is likely males made a greater distinction between the low and high levels of harm in the CC scenarios compared to females, given that the interaction was only found for male participants and not female participants.
Strengths and Limitations
This study was able to examine how willing participants were to intervene and accept a situation of CC, finding in preliminary analysis that participants reported high levels of willingness to intervene in CC and low levels of acceptance for CC. Furthermore, research investigating the impact of ethnic differences on IPV and CC outcomes has been scant to date, however this study was able to effectively apply social psychological theory to uncover the influence ethnicity can have on willingness to intervene in and acceptance for CC. Given the fast-growing migrant population in Australia, the general population is comprised from a range of groups from culturally and linguistically diverse backgrounds (Anthony et al., 2022). This study aimed to reflect the current composition of the Australian population, as Australians of European or British descent are currently in the majority and as such were used for the “ingroup” condition, and Indian ethnicity has been the fastest rising migrant group to Australia, making them one of the largest visible minority groups, therefore were chosen for the “outgroup” condition. As such, this study was able to assess, in lines with the current Australian population trends, how likely the majority are to intervene in a CC incident affecting members of a minority group, finding that ethnicity can act as a barrier where willingness to intervene is reduced and acceptance for CC is increased when the situation involves members of an ethnic outgroup. Ensuring participants who were not fully aware of the true nature of the study until after completion also contributes to the robustness of the findings, as this study avoided priming participants for a CC study, subsequently reducing any potential bias they may have had in their responses.
However, the findings from this study must be interpreted in light of its limitations. While one of the strengths of this study was its reflection of Australia’s population by focusing on Australians of European or British descent and Indian Australians, this resulted in the sample of the study being limited exclusively to participants who were Australian of British or European descent. This limits the generalizability of these findings to other ethnic groups, and further research should investigate whether the influence of ingroup favoritism would have the same effect on willingness to intervene for minority group members intervening in a CC scenario involving the majority group. While the survey was delivered in an anonymous online format, there is still the potential that social desirability bias may have influenced responses, especially as the social norms in Australia view IPV as unacceptable and warranting intervention (Webster et al., 2018). This study also yielded small effect sizes and was unable to find an effect of the level of harm on willingness to intervene or acceptance for CC, outside of the interaction between harm, gender, and culture found for acceptance for CC. Given that the low and high harm vignettes were essentially identical except for the addition of the threat of physical violence in the high harm scenario, it is likely the difference between the levels of harm embedded in the scenarios was not significant enough to elicit an effect. Future studies investigating the level of harm on these variables should increase the differentiation between the low and high harm scenarios to see if a difference in response would be found.
Implications for Bystander Intervention Programs
The findings from this study have highlighted the potential for effective bystander intervention in CC scenarios, due to the high willingness to intervene in and low acceptance for CC, as there are clear implications for these findings to inform future prevention and intervention strategies. Furthermore, this study has shown that ethnicity can act as a barrier to intervention in situations of CC, and that ethnicity may also influence respondents’ levels of acceptance for CC behavior. Additionally, uncovering that males are more accepting of CC behavior than females overall, and specifically from an ingroup member in a high harm situation, is pertinent to effective development of programs aiming to increase awareness and reduce acceptance of CC. These findings highlight the importance of tailoring bystander intervention programs for CC by gender. Additionally, bystander intervention programs need to focus on increasing willingness to intervene in and reducing acceptance for CC in ethnic groups other than one’s own.
Future Directions
The findings of this study have highlighted the role group identification based on ethnic identity can have on an individual’s willingness to intervene, and future research should investigate whether other factors that create a similar ingroup/outgroup dynamic, such as sexuality or religion would also influence willingness to intervene. Future research could utilize a social identification scale to examine whether the strength of ingroup identification has a moderating effect on the reduced willingness to intervene in the outgroup condition. While this study revealed an unexpected interaction between gender, level of harm, and ethnicity on acceptance for CC, future research should explore the effect ingroup serving bias may have on acceptance for forms of IPV other than CC. This study also revealed a significant effect of age on acceptance for CC, and future research should unpack the association between age and acceptance for CC.
Conclusion
By uncovering a general willingness to intervene in and low acceptance for CC, this study has made a unique contribution to IPV literature. Furthermore, the results of this study showed that differences in ethnicity can have an effect on reducing willingness to intervene in CC and increasing acceptance for CC. Participants were more willing to intervene in the situation, if the couple had the same ethnic identity as them. Participants who read low harm scenarios were more accepting of CC if the couple held a different ethnic identity to them, and males were more accepting of CC if the couple had the same ethnic identity as them and were involved in a high harm scenario. These findings should be considered in the development and application of future bystander intervention programs for CC.
Footnotes
Acknowledgements
We would like to thank the 357 participants who generously contributed their time to take part in our research, allowing us to gain further insight into bystander intervention in coercive control.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This project was supported by a small Betty Kitchener/University of Canberra Researcher Award given to the first author. The Betty Kitchener Endowment and University of Canberra staff who administered the funds were not involved in any part of this research including the data collection, analysis, and interpretation of the data.