
Abstract
Further study is needed regarding the intersection of community violence exposure, coping strategies, and health behaviors among young adult African American men and Hispanic/Latino men. This study did so in Lake County, Indiana, which contains multiple areas with disproportionate prevalence of violence relative to population size. Approximately 22 miles from Chicago, Lake County includes noteworthy mid-sized cities such as Gary, Hammond, and East Chicago. This study explored the perceptions of African American men and Hispanic/Latino men ages 18 to 25 regarding coping strategies and both healthy and health risk behaviors after directly witnessing or indirectly experiencing a violent act or event. We used aspects of social cognitive theory to design this community-based participatory research study. Thirteen males who self-identified as African American, Hispanic/Latino, or both, completed 34- to 80-minute, audio-recorded phone interviews. Audio recordings were transcribed, and NVivo 12 Windows was used by the research team (primary researchers and two coders) to complete transcript analysis. Findings from this study provided insight around African American men and Hispanic/Latino men regarding (a) witnessing violence directly or indirectly experiencing violence; (b) changes in everyday life experiences; (c) coping strategies that involved socio-emotional health, spiritual health, social health, and risky health behaviors; (d) rationales for not asking for help; (e) observations of significant others’ coping; (f) what to do differently in the future; (g) beliefs about mentors; and (h) beliefs about mental health providers. Delving into participants’ experiences revealed that African American men and Hispanic/Latino men in Lake County, Indiana chose to adopt a range of health risk and health positive strategies after directly witnessing or indirectly experiencing violence. Becoming knowledgeable about African American men’s and Hispanic/Latino men’s diverse coping strategies and health behaviors may help inform the community about how best to cocreate spaces that aim to alleviate the traumatic experience of having directly or indirectly experienced community violence.
Keywords
Young people across all communities—rural, urban, and suburban—in the United States are either directly or indirectly exposed to and affected by community violence and/or violent events in their lifetime (Finkelhor et al., 2009, 2015; So et al., 2021). Previous research has emphasized the importance of identifying and understanding the effect of trauma on young and emerging adult development (Price et al., 2019). By definition: Trauma occurs in the event of exposure to (1) actual or threatened death; (2) serious injury, or sexual violence by way of direct experience, observed witness; (3) learning of the traumatic event; or (4) repeated exposure to aversive details regarding the event. (Briere & Scott, 2014, p. 9; Griffith et al., 2019, p. 306)
Recent research by Lanfear et al. (2023) found that African American (56%) and Hispanic/Latino individuals (55%) growing up in the Midwest (specifically Chicago) were significantly more likely to have been exposed to direct and indirect community violence than their White counterparts (26%) by the age of 40. Similarly, studies have variously found that a majority of study respondents who reported losing someone from a violent event self-identified as a minority (African American or Hispanic) or a female or reported a lower socioeconomic status (Lynn-Whaley & Sugarmann, 2017; Rheingold et al., 2012; Turner et al., 2018). African American men and Hispanic/Latino men ages 18 to 25 who were exposed to community violence (violent injury/assault), either directly or indirectly, had experienced trauma (Griffith et al., 2019; Wolff et al., 2014). Indeed, trauma experienced by young African American men and Hispanic/Latino men due to community violence is a public health concern that warrants continued research (Listenbee et al., 2012; Pierre et al., 2020; Mrug et al., 2008).
How African American and Hispanic/Latino Men Cope with Violence
In the United States, males and persons ages 20 to 24 years had the highest homicide rates across all age groups (13.2 per 100,000 population; Sheats et al., 2022). Non-Hispanic Black/African American males (40.9 per 100,000 population) and Hispanic males (8.6 per 100,000 population) are proportionally more likely to be homicide victims compared to their White male counterparts (3.3 per 100,000 population; Sheats et al., 2022). This pattern also holds true for Lake County, Indiana, the site of this specific study, where most homicides occurred in the city of Gary (Reese, n.d.), and the victims were primarily African American males (79.8%) and Hispanic/Latino males (7.3%; Cross, 2018; Reese, 2019; U.S. Census Bureau, n.d.a).
African American men and Hispanic/Latino men are at a higher risk of engaging in unhealthy behaviors as a coping mechanism in response to community violence exposure (Arkin, 2015; Fowler et al., 2009). For example, for African American men ages 18 to 25, substance misuse was associated with exposure to direct victimization (childhood maltreatment, sexual victimization, and peer/sibling) and witnessing (indirect) victimization (Saadatmand et al., 2021). Furthermore, African American male adolescents report that “they [are] more likely to respond to victimization in the community by acting ‘tough’ or carrying a weapon for protection rather than feeling depressed” (Gaylord-Harden et al., 2011, p. 716 as cited in Bell & Jenkins, 1993). For Hispanic/Latino men between 18 and 25, adverse childhood experiences were significantly associated with substance use (cigarettes, marijuana, “hard” drugs, and binge drinking; Allem et al., 2015).
Due to stigma and cultural traditions, African American men and Hispanic/Latino men may be reluctant to seek mental health services as a constructive alternative and are more likely to suffer in silence or turn to behaviors that undermine health (hereafter, health risk behaviors) as a temporary solution (Gloria & Peregoy, 1996; Levant et al., 2011) after being exposed to violence. For example, they may engage in anger suppression and confrontation as ways of coping with overt and covert racial discrimination (Brondolo et al., 2009). The hypothesized causes of this reluctance may emerge from divergent sources. Specific examples include findings that some members of the African diaspora communities still consider mental health counseling taboo (Chang & Berk, 2009; Williamson, 2014). Somewhat differently, members of the Hispanic/Latino communities may avoid counseling outside of the family due to fears around bringing shame on their family unit (Gloria & Peregoy, 1996; Lee, 2014).
Nonclinical mentoring may function differently for young African American men and Hispanic/Latino men than formal counseling. Studies have suggested that youth mentoring programs may be associated with less frequent behavioral and emotional problems for young African American men and Hispanic/Latino men (Deutsch & Spencer, 2009; Pribnow, 2020; Sánchez et al., 2018). Several scholars have proposed that mentoring relationships may aid young African American men and Hispanic/Latino men socioemotionally, cognitively, and in terms of their identity and fostering healthy development—however, the precise nature of the mentoring (e.g., older adults or peers), mentorship structure, and intervention effect sizes are likely to vary (Jackson et al., 2014; Pribnow, 2020; Rhodes & DuBois, 2008; Sánchez et al., 2018; Santos et al., 2013). Yet, mentors may share an understanding and expertise in how to navigate professional roles or address racially sensitive issues (e.g., discrimination and prejudice). This literature suggests a need to further understand how mentorship might mitigate the influence of trauma among young African American men and Hispanic/Latino men and the nuances of how such mentorship might function. For example, while it remains unclear if the gender of the mentor is relevant in the mentor–mentee relationship, some evidence supports the importance of having a keen awareness of one’s own racial and ethnic identity and the impact it may have on the mentor-mentee relationship (Alvarez et al., 2009).
The literature cited above makes it clear that exposure to community violence can be traumatic, and that young African American men and Hispanic/Latino men may adapt to such exposure through adoption of health risk behaviors. Furthermore, there is some evidence that they may be disposed to avoid mental health services. However, a holistic understanding of how young African American men and Hispanic/Latino men cope after being exposed to violence remains elusive, especially if they are interested in confiding in a mentor or mental health provider.
Research Questions
While many important and nuanced differences exist between young African American men and Hispanic/Latino men, and each population deserves to be studied individually, important similarities also exist, as noted above. Moreover, because of the sensitive nature of dialog around coping strategies and health behaviors after being exposed to community violence, and because of the multiracial/ethnic dynamic in Lake County, the first author chose to include both groups of men for this study. Therefore, as part of that vital larger process to help further our understanding of how young and emerging adult (ages 18–25) young African American men and Hispanic/Latino men cope after directly witnessing or indirectly experiencing a violent act or event, this study aimed to generate knowledge related to two primary questions:
What healthy and health risk behaviors do young African American men and Hispanic/Latino men, aged 18 to 25, engage in after directly witnessing or indirectly experiencing a violent act or event?
To what extent do young African American men and Hispanic/Latino men ages 18 to 25 seek out mentors and mental health providers after directly witnessing or indirectly experiencing a violent act or event?
This study considers the first of these behaviors as internal coping activities and the second external coping activities.
Methods
Study Site
Our study site was Lake County, Indiana, which is located approximately 22 miles southeast of Chicago, Illinois. Lake County was chosen for this study due to the magnitude of community violence, specifically gun- and gang-related violence, relative to the population size in places within the county such as Gary, East Chicago, and Hammond, each of which have high percentages of African American male and Hispanic/Latino male residents. For example, in 2021, “firearms were used in 44 of Gary’s 48 homicides, 15 of Hammonds’ 16 cases, 12 of East Chicago’s 13 cases, five of Michigan City’s six cases, and all three of Merrillville’s confirmed homicides” (Reese, 2022, para. 4). In 2021, Hispanic/Latino individuals and non-Hispanic/Latino African Americans comprised 20.9% and 24.5% of the population in Lake County, respectively (U.S. Census Bureau, n.d.b).
Factors Studied
For our study, the personal factors of interest consisted of race, gender, age, education, having witnessed or indirectly experienced a violent act or event, and a cluster of attributes often associated with being masculine, namely being assertive, ambitious, or risk-taking (Mahalik et al., 2003; Wong & Wang, 2022). Behavioral factors included young African American men’s and Hispanic/Latino men’s positive coping strategies and negative coping strategies, as well as their healthy and risky behaviors. The environmental factors consisted of marital status, participants’ peer groups, family units, neighborhoods, social and broadcast media exposure, availability of community services (specifically a mentor or mental health provider), and socioeconomic status. Internal coping strategies included engaging in healthy behaviors, while external coping activities included seeking out a community mentor or mental health provider to share and process their perceptions and emotions after directly witnessing or indirectly experiencing a physically violent act or event. In principle, we treated having directly witnessed violence the same as being a victim. Indirectly experiencing violence was conceptualized as hearing or reading about a violent event in their community; or viewing depictions of such an event in print, visual, or social media; or attending a funeral; visiting a victim of violence in the hospital or at home; visiting the family of a victim of violence; seeing them in the store; or another interaction with a direct victim.
Approach
In this study, we used a qualitative, descriptive phenomenological design employing semistructured interviews to learn about the lived experiences (Bhattacharya, 2017; Finlay, 2009) of African American men and Hispanic/Latino men who directly witnessed or indirectly experienced violent acts in Lake County. Descriptive phenomenology provides an in-depth opportunity for the researcher to explore and analyze the meaning of lived experiences on individual perceptions, feelings, and judgments about a particular phenomenon (Creswell & Creswell, 2018; Patton, 2002; van Manen & van Manen, 2021).
Within that framework, our study focused on aspects of health behavioral science emphasizing “the systematic investigation of the multifactored nature unique to everyone’s decision-making process regarding their behavior” (Rovito, 2019, p. 258). Specifically, community violence exposure among minority males is a public health concern that warrants continued research (Listenbee et al., 2012; Pierre et al., 2020). Bowleg (2021) encouraged scholars and practitioners to adopt “intersectional public health lenses that embrace rather than obscure(s) the heterogeneity of people’s lived experiences” (Elnaiem, n.d., as cited in Bowleg 2021, p. 88). For example, men of color may experience and interface with the world by cycling through their various existing social identities (Wong et al., 2017). That is, men who self-identify as either African American/Black and/or Hispanic/Latino non-White may have multiple social identities (Wong et al., 2017) and at times experience conflict where one social identity is deemed more acceptable than the other based on the given circumstances (e.g., a male who self-identifies as being African American and a young man). “Individual experiences associated with their social identities (e.g., racism, acculturation, and ethnic identity) should be interrelated” (Cole, 2009, as cited in Wong et al., 2017, p. 269). The challenge for scholars/practitioners is how to intentionally make space to qualitatively study people who self-identify as either an African American/Black man or a Hispanic/Latino man, with current or previous lived experiences of directly witnessing or indirectly experiencing physical violent acts. This need led to the selection of a descriptive phenomenological approach to investigate African American/Black and Hispanic/Latino men’s coping strategies and health behaviors after being exposed to community violence.
Methodological Framework
Social cognitive theory (SCT) focuses on observing and learning from others along with positive and negative reinforcement behavior (Bandura, 1986) and suggests that personal, behavioral, and environmental factors are interrelated and impact one’s decision-making and overall behaviors, which is consistent with our broader a priori understanding of trauma. We used SCT to guide the development of the questionnaire to help identify the perceptions of how young African American men and Hispanic/Latino men behave after directly witnessing or indirectly experiencing a violent act or event, but use of SCT did not supplant our phenomenological approach in interpreting the data.
SCT was well-suited to guide the development of the questionnaires, because it allowed the primary investigator to construct interview questions focused on understanding African American men’s and Hispanic/Latino men’s self-efficacy, behavioral capability, and observational learning to better understand how intense stressors and perceived threats are managed. This, in turn, facilitated our interest in learning how African American men and Hispanic/Latino men cope after being exposed to community violence (Benight & Bandura, 2004). To share a specific example, self-efficacy is associated with humans’ ability to make logical decisions and ability to reason, as well as with their stress reactions and how they may cope during stressful and/or threatening situations (Benight & Bandura, 2004). With this in mind, we included one question in our semistructured interview guide, “What are your beliefs about having control over being able to cope in a healthy manner after being exposed to violence?” because of our expectation that subjects’ experiences with coping were associated with their trauma response.
Participants
Our study began in November 2021 and concluded in February 2022. Using a community-based participatory research orientation, this study involved a collaborative partnership with Holistic Evolution (HE), a community-based organization in Northwest Indiana. HE is a nonprofit membership organization that seeks to address the developmental needs of male youths of color by providing them with a mentor who has healthy beliefs and clear standards (HE, 2021). With the assistance of HE staff, a purposive and theoretical sampling process (Groenewald, 2004) was used to identify and engage community members (Patton, 2002). To be eligible, individuals had to (a) self-identify as being a African American man or Hispanic/Latino man, (b) be aged 18 or older, (c) currently or previously have lived experiences of directly witnessing or indirectly experiencing physical violent acts, and (d) currently live or previously have lived in Lake County, Indiana.
The first author (KADB) requested assistance from HE staff with introducing study goals to eligible participants. Multiple recruitment items such as a study information sheet, flyer, and recruitment email were disseminated. The study flyer was shared across the first author’s and HE’s social media platforms such as Twitter, Instagram, and Facebook. KADB also attended community events, passing out the study flyers and study information sheets. All procedures and materials were approved by an Institutional Review Board before the study began.
Procedure
Our semistructured interview guide consisted of open- and closed-ended questions that were administered by the first author (KADB) to interviewees. The interview guide focused on five key categories: (a) participants’ personal experience with direct or indirect exposure to community violence, (b) participants’ self-efficacy regarding their coping choices after exposure to violence, (c) participants’ behavioral capability regarding their coping choices after exposure to violence, (d) participants’ observational learning, and (e) participants’ perceptions regarding their willingness to talk with someone else (community mentors or mental health provider) after having directly witnessed or indirectly experienced a violent act in their community in Lake County.
Some African American men and Hispanic/Latino men do not like to talk about matters related to community violence, shootings, homicides, or related topics. Such reluctance is related to a “street code” of which community members, community-based researchers, and police officers are often aware (Kwak et al., 2019). Therefore, by the time we had reached theoretical saturation (Fusch & Ness, 2015; Saunders et al., 2018) by interviewing 13 individuals, an additional 12 interview attempts had been declined (e.g., 25 total individuals had been approached). Characteristics of the 13 participants are shown in Table 1. Data were collected through 34- to 80- min semistructured, audio-recorded interviews.
Study Participants’ Demographics.
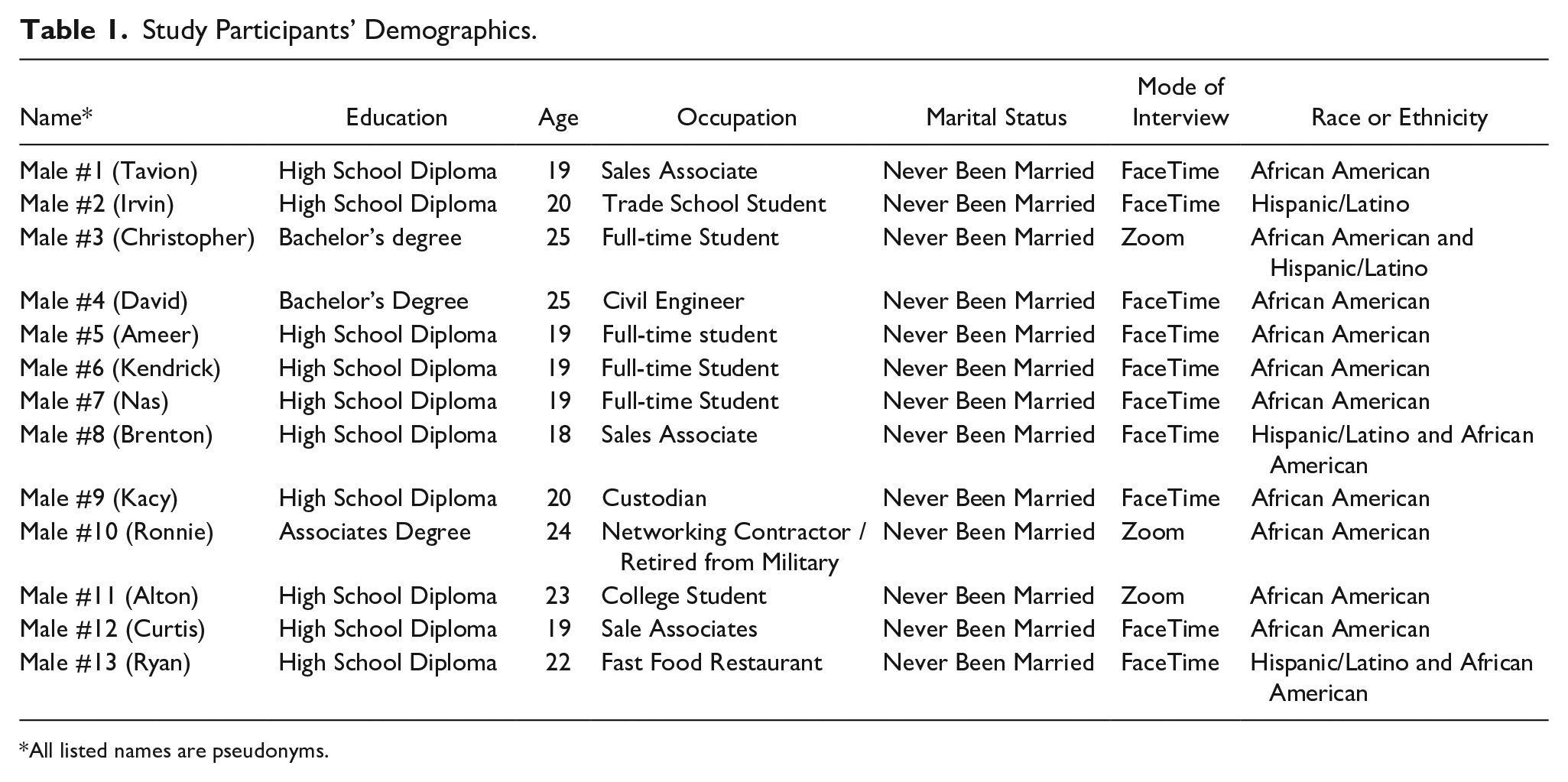
All listed names are pseudonyms.
KADB conducted all interviews. All participants received a study information sheet and informed consent was secured from all participants, along with their permission to be audio-recorded. Interviews were conducted via Zoom or by using the FaceTime app on cell phones. KADB texted or emailed participants first and then asked if they preferred to be interviewed via Zoom, phone, or FaceTime. All recordings were stored behind the university’s institutional firewall via OneDrive until transcribed. Each interview was transcribed verbatim by a vendor transcription service and then reviewed by the data collection lead and research team (Archibald et al., 2019). All participants were assigned pseudonyms to ensure confidentiality and offered a copy of their de-identified transcript.
Data Analysis
Based on the theoretical approach and constructs described above, data analysis consisted of a mix of deductive and inductive processes. For the deductive process, before the interviews began, we developed a codebook that included detailed definitions. For the inductive process, the data analysis was carried out by four researchers and consisted of an iterative process of reading and rereading the transcripts (Connelly, 2010). Two of the four researchers (KADB, CO, TN, and BW), who served as coders, were naïve to the study, thus helping to achieve internal reliability (Leung, 2015; Silverman, 2021).
NVivo (QSR International Pty Ltd, 2020) was used as the analysis platform, because it was a suitable and reputable tool for analyzing qualitative research data. Utilizing NVivo helped the first author with managing and organizing the data for the research team. While using NVivo, the research team initially coded the data using codebooks (Babchuk, 2019; Creswell & Guetterman, 2019). Upon coding the data, the research team identified the units of data that aligned with the research questions (Banchuk, 2019), highlighted all emergent data as new codes, then classified themes and subthemes appropriately (Creswell & Poth, 2018) across all interviews to validate the findings (Connelly, 2010), and finally developed interpretations of the data individually and collectively. We had four primary coders, all of whom are study authors and one of whom is a highly experienced qualitative methodology expert (CO) who did the circulation checking and confirmation using NVivo. Once all four coders agreed on all categorization and coding decisions, we moved forward. The first author held research team meetings to ensure member checking, review data (data triangulation and thick descriptions), and establish that all final coding decisions were credible and represented the content of the interviews accurately (Creswell & Poth, 2018; Nowell et al., 2017). For example, after finding that 11 out of the 13 participants discussed that they had observed others in their lives using psychoactive substances as a form of coping after being exposed to violence, we made the decision to incorporate “Risky Health Behaviors—Drug Abuse and Misuse” as a major results category.
Results
Witnessing Violence Directly or Indirectly Experiencing Violence
Participants shared their experiences about witnessing violence directly and indirectly in their communities. Across all 13 interviews, participants indicated that they had seen shootings, fights, robberies, and hit and runs. Hearing gunshots is common in some communities in Lake County as expressed by “ Kids can’t even be in this park without this park getting shot. . . It was times where I stayed up all night because I was worried about my brother. My brother was asleep right next to the window. . . I would literally stay up and watch him just to make sure he was okay because I didn’t want him getting hit by any stray bullets.
Participants also described how violence personally impacted them as they reflected on their friends/loved ones being killed by gun violence and the ongoing fear of being hit by stray bullets. I was 12 . . . I was on a basketball court playing basketball and I heard gunshots . . . I’m walking towards like where I heard the gunshots and everybody running back towards my way. And like they said, ... like, one of my homies got killed . . . And I end up going to where he got killed that way everybody was running from. And he was on the ground bleeding out, and I was just shocked. Like I was just looking at him.
Changes in Everyday Life Experiences
Participants reflected on how their lives changed after being exposed to community violence. Participants shared how they began to move differently, change friend circles, and stay on point (e.g., being vigilant and aware of surroundings). Participants described the essence of street smarts, which they referred to as survival skills related to the environment and acceptability of social cues (do’s and don’ts). As expressed by I got smarter. I got way smarter. Like, I got survival skills. . . I didn’t have a car. So, I was outside like, so I had elite survival skills. Cause I was walking everywhere. I was walking to other neighborhoods. . . I’m walking like 30 minutes to an hour every day, like outside. And it was just, I kept my head on the swift. Like I wasn’t walking with phones. Um, when I was catching a bus, I was like staying on point.
Participants suggested that violence is the norm in Lake County, and it can happen to anyone at any time, reflecting a perception that no one is safe. Overall, being exposed to violence directly or indirectly led most participants to adapt to their environment by incorporating survival strategies. As explained by I stopped doing a lot of hood stuff. I really think I changed I surrounded myself with. . . I was always the youngest. I used to always run around with the older guys and beat up people for no reason. . . but now I feel like what I need friends for, I always moved solo since that happened (gun violence) to my homie.
Social–Emotional Coping Strategies
Participants described multiple coping strategies after exposure to violence, such as crying, rapping, writing, and listening to calm music. “
When males described the idea of crying, some highlighted how it was an “angry cry,” or that they typically do not cry, but after hearing about the loss of loved ones (including close friends), they did
Spiritual Coping Strategies
Participants mentioned that praying and talking to their God was a priority in their life and helped them through challenging circumstances. As shared by God is above my family, my significant other. And He’s like, you would think we’re in a relationship. Like He’s, He’s my everything. . . there’s times where I woke up and I knew for a fact I was not going to have a good day at all. And know certain things took place and it’s like, thank God that I made it home. I made it home to like, you know, kiss my mom and tell her I love her kiss, my other sister or you know, so just kiss my significant other, you know, like that. . . I literally pray of the time because it’s like, He’s helped me through some of the craziest things.
Participants mentioned how they often prayed and kept God at the center of their hearts. They described how praying or simply talking to God served as a way of escape because they felt when they spoke to God, somebody was there listening to them genuinely. Well, I like to talk to God a lot and I know that He always will be there if I can’t talk to anybody else. So, as I talk to him and I say my prayers, I know that he’s going to talk back to me and He’s going to answer my prayer. . . So, it’s like, as I talk to Him, everything gets better.
Social Health Coping Strategies (Family, School, and Sports)
Participants also shared the coping strategies that involved sports and being involved with their family and friends as ways that they chose to cope. As described by
Many participants talked about how school was seen as a way out of their environment, and it served as an outlet to temporarily release and ignore the day to day realities of violence. As expressed by I’m going to be completely honest. It was the school system. Honestly, I seen it as a ticket out. . . I went to university at 17. I had graduated early, and I seen school as like a ticket off the hood. So that was what it really was. I was trying to get the best grades and trying to be like the smartest for person. . . like I had like friends who was older than me from the same environment that was from the hood. They went to school and their life got better. . . I was like, I’m going to go to school bro, school is the way out!
Most participants called their friends “brothers” and described regarding them with a familial kind of love. Some video games were also mentioned as a coping strategy among participants. “. . .Like seeing, like after, after all the violence stuff, stuff that happened, like I’ll probably like, you know, go chill out or something like that, go in my room, play the game or something. Like get my mind off the shit”-
Risky Health Behaviors (Drug Abuse and Misuse)
Participants described drugs such as marijuana, Percocet, Molly, Xanax, and ecstasy as ways to cope after being exposed to violence in Lake County. Drugs seemed to be both a positive and negative coping strategy for young African American and Hispanic/Latino men. Some participants described how drugs negatively impacted their bodies; as After seeing my baby cousin and seeing my sister and my niece in a casket, that’s when like. . . it sparked that drug use. . . I’ve done Percocets. I’ve done Molly. I’ve done ecstasy pills. I’ve done Xanax. . .When I was doing it, my body and just myself period was slowly deteriorate. . . I was slowly drifting away from everyone and, and I would just, I would go off of how I felt in the moment. Like, if I, like I said angry, I would do whatever. It didn’t matter to me. And I always heard like the words, like, man, you’re tripping, man. You bugging like what was wrong with you? Like, and people looked at me like, like I was crazy.
As typified by
I don’t care what nobody say. Smoking (marijuana) helps. I can merge smoking is how I graduated school early. . . Just doing my work before everybody and just be having fun. If I would not have smoked, I probably would’ve been fighting all the time. . .
Rationale for Not Asking for Help
Participants explained why asking for help was a challenge for them during times of trouble in their lives. The notion of “owing people” was a barrier that prevented some males from asking for help. As expressed by I feel like no matter who that person is, people help people so they can have somebody to owe. And I ain’t about to feel like I got to owe you just because you help me one time. So that’s why I don’t really look for no help from nobody. Because if I got to owe you to help me, I don’t need it.
Other participants discussed the importance of genuinely knowing the individuals who they would ask for help to avoid situations where deceptive people might manipulate them. Further, some participants stated how they felt like they would be wasting people’s time. In lieu of reaching out, some participants described how they typically stay to themselves and attempt to fix the situation or become consumed by it. As expressed by I never really went to people when I had to cope. It’s just like, I always want to stay by myself and try to fix 'em on my own. So, I’m that type of person to not say nothing. If something is bothering me and I’ll fix it on my own, or I just let it eat me up inside.
Observation of How Significant Others (e.g., Peers, Friends, Parents, Coaches, Teachers, etc.) Coped
Most participants stated that they did not learn coping strategies directly from their family and described how others in their lives decided to cope after being exposed to violence. Participants reported that they seldom witnessed people in their social circles talking about sensitive matters regarding violence outside of their homes. As
Drug and alcohol use and isolation were the most frequently described coping strategies used by significant others in participants’ lives. Participants shared that they witnessed their friends doing drugs include marijuana (weed), heroin, ecstasy, and other street drugs. Weed abuse, alcohol abuse, and just staying to themselves and, and planning on going farther than this place, trying to get out of this place. Because the only thing that’s here that most of, of I say is selling drugs, dying, or going to jail. There’s nothing else really here for us in Gary.
Things to Do Differently in the Future
Participants shared a variety of responses about what they would do differently in the future to cope. As If a doctor prescribes me Percocet, I will tell him no. Yeah. I will never take anything other than an ibuprofen. . .” Interviewer: “Like, what’s motivating this change for you?” “I want a house, like a nice house in a nice neighborhood. I want few cars. I want to, you know, have kids have, do normal things. I don’t want the big mansion or the like, I’m more simple. . . As a couple, as a family and me turning into a family man, I can’t do that while doing this. I can’t do that while steady popping pills.
Other participants described how violence is occurring everywhere and can happen to anyone, so it is important to adjust how they respond to and resolve violence when they experience it. As shared by
Beliefs About Having a Mentor
Most males had people who have been influential in their lives but who were not formally serving as mentors. Their unofficial mentors were members of their social networks, like their teachers or family members. As expressed by
When asked about the importance of having a mentor, participants shared that a mentor would help them make it through life and how it is impossible to make it in this society without having someone else to look up to or talk to for advice. Participants described mentors as someone who provides insight and guidance on their journey ahead, especially if they came from similar backgrounds. As expressed by
Beliefs About the Race or Gender of Mentors (Subtheme)
Participants shared mixed thoughts about whether the race or gender of a mentor mattered. Some participants indicated that seeing people who look like them in places they dreamed of is important. Other participants were concerned that mentors cannot help effectively if they do not share similarities. As shared by
Other participants felt that the race or gender of a mentor did not really matter because mentors had knowledge and wisdom that they lacked and desperately needed. As It’s not a racial thing for me. Since you are another color or you another race or religious or anything, you know, something. So it is like, you know some type of information that I don’t know. And if you’re older than me, you know, some type of wisdom or knowledge that I won’t know anyway. Right. So, I’m not going to put race or anything like that on a person just because, I mean, just to listen to somebody.
Beliefs About Seeing a Mental Health Provider
Across all 13 interviews, most participants were not interested in talking with a mental health provider. As expressed by
Some males indicated that their mental health was fine. In some cases, they addressed whether a mental health therapist could genuinely help them. The idea of a mental health provider being someone who may not know them intimately seemed to play a factor in whether males would take an interest in speaking with a therapist. Yeah, like if they were a mental health provider and I was close to them or I like got to know them, then I would probably talk. But other than that, like me just not knowing them and just get it to talking, it won’t happen.
Beliefs About the Race or Gender of Mental Health Providers (Subtheme)
As with mentors, participants shared mixed thoughts about whether the mental health providers’ race or gender mattered, specifically if it impacted their desire to share their thoughts and feelings as an external coping strategy. As I do have a like more of a natural comfort talking to women than I do to men. And I’ve noticed it along. I like if I’m in a room full of people, I don’t know. I’m going to go talk to a woman before I go talk to a man.
However, other participants indicated that the race or gender of a mental health provider is irrelevant if they are genuinely there to help. As If they’re genuinely there to help, then you should allow them to help. Because like the people that help me, they aren’t all African American or they are, they aren’t all male. But they all help in tremendous ways.
Discussion
The purpose of this study was to understand how young African American and Hispanic/Latino men cope after directly witnessing or indirectly experiencing exposure to violence, with a particular focus on internal and external coping strategies. Although exposure to violence was an eligibility criterion for participating, it is still notable that hearing gunshots in specific urban and underserved communities was perceived as the norm in Lake County, Indiana. Current study findings were consistent with the existing literature regarding young African American and Hispanic/Latino men in urban areas. Specifically, the lived experience of participants in our study was consistent with previous studies (Aisenberg et al., 2007; Elsaesser & Voisin, 2015; Lambert et al., 2012; Springer & Padgett, 2000), which reported that African American and Hispanic/Latino male adolescents residing in urban communities witness community violence, specifically shootings or stabbings (Gaylord-Harden, et al., 2017; Kataoka et al., 2003; Paxton, et al., 2004; Schwab-Stone et al., 1995).
Our study results are notable because they reflect a variety of dimensions in young African American and Hispanic/Latino men responses to being exposed to violence that are not readily identifiable through quantitative research. Moreover, unlike a grounded theory study of the coping styles and the type of community violence exposure experienced by African American adolescents residing within a high-violence community on Chicago’s southside (Voisin et al., 2011), current study results capture changes in everyday life experiences that young African American and Hispanic/Latino men ages 18 to 25 undergo.
Our study participants described a wide variety of changes in their everyday life experiences after being directly or indirectly exposed to violence, including changing their friend circles, moving differently in their community (e.g., vigilance), learning survival skills, and adapting to new ways of living life. Participants’ internal coping strategies were varied but primarily fell into four categories: socioemotional health, spiritual health, social health, and risky health behaviors. For socioemotional coping strategies, young African American and Hispanic/Latino men chose to write, rap, listen to calm music, or simply cry after being directly or indirectly exposed to violence. For spiritual health, they expressed that praying and talking to their God was a priority in their lives that helped them through challenging circumstances. These concepts are similar to those offered by Brady et al. (2008), who found that healthy and effective coping strategies for adolescents who were exposed to violence consisted of engaging in positive activities such as sports and prayer, with the ability to keep their mind focused on the positive factors in life such as practicing self-control, avoiding confrontation, and seeking advice from others.
For social health, most participants talked about school being a way out. This was both because it could provide an outlet to play basketball and other sports and because education was perceived as a ticket out of the hood and even gangs, in some respects. This finding was consistent with Voisin et al. (2011), who discovered that a main coping technique for African American men overcoming community violence exposure was to excel in school in hopes of being able to move out of their community. However, our results were generally inconsistent with findings from Bell and Jenkins (1993) and Rasmussen et al. (2004), which indicated that both African American men and Hispanic/Latino men reported using confrontational coping when responding to community violence. Notably, some of our participants indicated that drug use (marijuana, ecstasy, molly, Percocets, and Xanax) was a prominent go-to for males to numb themselves and cope with their painful realities and, in some cases, to avoid confrontations at school or their neighborhood.
Young African American and Hispanic/Latino men in our study described having a hard time asking for help when they needed it. Instead, they reported engaging in activities that were solitary or isolating (not talking, shutting down, playing video games, or avoiding friends). This finding was consistent with Brady et al. (2008), who found that ineffective coping strategies used by adolescents include attempting to withhold their true thoughts and feelings, choosing to isolate themselves intentionally, and refusing to acknowledge the truth of what they experience, while trying to forget about the situation that occurred. Relatedly, most of our study participants seldom witnessed people in their social networks seeking out a therapist. Consistent with SCT, one might speculate that young African American and Hispanic/Latino men who do not observe older males and peers engaging in this type of behavior will find it difficult to share their personal vulnerabilities with others when they need help.
Our participants, who had no other choice but to continue to live in violent communities, described knowing how to survive and make do in their circumstances, consistent with research finding that males may choose to suppress their emotions to cope with surviving and navigating unsafe environments (Cassidy & Stevenson, 2005; Gaylord-Harden et al., 2011). Sometimes, this was aided by psychoactive substances, but perception of risk was not uniform. In one case, a young male indicated that he would not take drugs like Percocet, even if a doctor prescribed them.
Finally, while the young African American and Hispanic/Latino men in our study were not always open to speaking with mental health providers, the majority of participants expressed the importance of having a mentor. Our findings are consistent with the literature considered through a community lens. Some members of the African diaspora communities still believe mental health counseling is taboo (Chang & Berk, 2009; Williamson, 2014). Additionally, some members of the Hispanic/Latino community may feel that engaging with mental health providers might bring shame to their family (Gloria & Peregoy, 1996; Lee, 2014). In contrast, when asked about their interest in having a mentor (even informally), the majority of participants agreed that having a mentor would help them learn, though some participants were not convinced that mentors could help them in their life.
It seems that participants had a realistic understanding of what a mentor entails and how a mentor could assist them. They also were able to distinguish mentors from mental health providers and, while open to having mentors in their lives, expressed clear disinterest in working with a mental health provider. For both mentors and mental health providers, participants shared mixed feelings about demographic characteristics. Some indicated that having a mentor or mental health provider who looks like them is essential, consistent with existing research findings that young African American and Hispanic/Latino men perceive counselors who look like them to be more credible (versus White counselors), because of their shared cultural heritage and values Steinfeldt et al., 2020; Sue & Zane, 1987). Conversely, other participants felt that demographic characteristics were irrelevant.
Limitations
The sample size and demographics were limitations of this study. That the sample size was relatively small (n = 13) and represented a subgroup of young African American and Hispanic/Latino men in Lake County, Indiana, was intentional, as theoretical saturation was achieved after hearing no more new information from the 13 interviews (Saunders et al., 2018; Fusch & Ness, 2015; Glaser & Strauss, 1967). At the same time, qualitative research is not necessarily designed to be generalizable, but rather to be generative and produce new ideas. In that sense, we believe that this study was successful. Another limitation was that the interviewer (KADB) was a community outsider. A researcher is considered an insider when they conduct research with a population to which they belong (Dwyer & Buckle, 2009; Kanuha, 2000). Although the lead researcher was older than age 18 and identified as African American with direct previous exposure to violence, they identify as neither a male nor a resident of Lake County.
Future Research
Future research should investigate factors that may influence whether young African American and Hispanic/Latino men reach out and ask for help from others, as well as their rationales for not seeking help from others, such as mental health providers and community mentors. Also, scholars should further examine how young African American and Hispanic/Latino men construe mentorship, what they may seek from a relationship with a mentor, and how mentors could facilitate access to mental health providers when needed. Additionally, research should examine whether and why young African American and Hispanic/Latino men are resistant to working with mental health providers and what messages regarding working with mental health providers would resonate with this population. Finally, to inform mental health resource development and dissemination for males, future research should attempt to definitively understand if race or gender of community mentors or mental health providers matter to young African American men and Hispanic/Latino men. In this study, it seemed like some of the participants were more comfortable opening up to women, yet we need more research to see if this is generally true.
Based on the findings in this study, we tentatively propose several recommendations for practice. Our findings suggest that mentors can serve as an intermediary between mental health professionals and African American men and Hispanic/Latino men after they are exposed to violence. For example, one might consider proactively equipping community mentors/mentor-like figures (parents, guardians, teachers, coaches, barbers, faith-based leaders, community health workers, and others) with mental health first aid training. Such training could serve both as a high-leverage community intervention and an opportunity for rigorous evaluation of benefits and costs.
Further, there is a known deficit in the number of mental health-care professionals throughout the United States and Indiana (Bureau of Health Workforce, 2022; Kaiser Family Foundation, 2022) with an additional nested lack of mental health professionals who are African American and Hispanic/Latino (American Psychological Association, 2022; Bernard et al., 2023). If strategies are identified to reliably facilitate connections between young African American men and Hispanic/Latino men and mental health professionals, then policymakers might conduct an intensive assessment of education/licensing requirements for mental health professionals in the state of Indiana to understand the barriers and gaps that may exist for people with marginalized identities who seek to become mental health professionals.
Conclusion
This study explored young African American and Hispanic/Latino men’s perceptions, coping strategies, and lifestyle changes after being exposed to community violence in Lake County, Indiana. Delving into participants’ experiences revealed the diverse and complex ways the participants chose to cope after directly witnessing or indirectly experiencing violence. This study serves as a valuable generative resource and, ideally, will contribute to the development of new approaches to better serve young African American and Hispanic/Latino men in similar circumstances. Finally, this study provided actionable information to local community organizations.
Footnotes
Acknowledgements
The authors would like to thank Ms. Esther J. Lewis, CEO of Holistic Evolution (HE) in Lake County, Indiana, for her partnership and for helping us recruit participants for this study. The authors would also like to acknowledge the participants’ investment of time and energy and their vulnerability in sharing their real-life experiences of being exposed to community violence directly or indirectly.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.