
Abstract
Lesbian, gay, bisexual, queer, and other sexual minority (LGBQ+) young adults report similar or higher rates of intimate partner violence (IPV) perpetration than their heterosexual peers. Elevated IPV risk among LGBQ+ young adults may be attributable to experiencing heterosexist discrimination and internalized homophobia. In addition, LGBQ+ people report disproportionate posttraumatic stress disorder (PTSD) symptoms, alcohol use, and IPV perpetration in dating relationships. Thus, this study explored which combinations of IPV risk factors (i.e., experiencing heterosexist discrimination, internalized homophobia, PTSD symptoms, alcohol use) related to forms of IPV perpetration, inclusive of psychological, physical, and sexual forms, in a sample of 342 LGBQ+ young adults. Internalized homophobia was related to psychological IPV perpetration at high and medium levels of PTSD symptoms and only high levels of alcohol use. PTSD symptoms and alcohol use interacted to predict psychological IPV perpetration; and PTSD symptoms related to increased psychological IPV perpetration at high and medium, but not low, alcohol use levels. Alcohol use was positively related to physical IPV perpetration. No other risk factors or interactions were significantly related to physical or sexual IPV perpetration. Results were consistent with prior findings that linked internalized homophobia, alcohol use, and PTSD symptoms to IPV perpetration and highlight the interacting nature of these IPV perpetration risk factors. Comprehensive IPV interventions with LGBQ+ young adults should evaluate the impact of simultaneously targeting these multiple IPV risk factors considering their interacting contributions to IPV perpetration risk. More research is needed to examine the temporal relations between minority stress, PTSD symptoms, alcohol use, and IPV perpetration.
Intimate partner violence (IPV)—defined as physical, sexual, and psychological aggression toward current or former dating or romantic partners—is highly prevalent and associated with myriad psychological and physical health problems among young adults, including severe injury, substance use, and depressive symptoms (Exner-Cortens et al., 2013; Plichta, 2004). Despite most studies on IPV etiology focusing on heterosexual people, sexual minority young adults perpetrate IPV at equal or greater rates (between 26% and 61%) than their heterosexual counterparts (between 29% and 35%; Edwards et al., 2015; Messinger, 2011; Walters et al., 2013). Furthermore, sexual minority individuals report similar risk factors for IPV (e.g., alcohol use) yet also face unique risk factors for IPV (Rollè et al., 2018). That is, according to minority stress theory, lesbian, gay, bisexual, queer, and other sexual minority
Sexual Minority Stress and IPV Perpetration
Risk factors, such as trauma and alcohol use, have been established as predictors of IPV perpetration across all populations (Hahn et al., 2015; McKinney et al., 2010). However, given the unique stressors experienced by LGBQ+ individuals, these risk factors may be especially pronounced. Brooks (1981) proposed that the severity of this psychosocial stress depends on the cumulative intensity and frequency of one’s exposure to life stressors, such as sexual identity-related stressors (e.g., heterosexist discrimination), internalization of stress, general life stressors (e.g., low socioeconomic status), and access to protective factors. Building from this framework, Meyer (2003) posited that mental health disparities derive from the overall experience of holding a non-heterosexual sexual identity coupled with exposure to distal (e.g., experiencing heterosexist discrimination) and proximal (e.g., internalized homophobia) sexual identity-related stressors. Minority stress theory is supported by several studies demonstrating associations between minority stressors and mental health problems, health risk behavior (e.g., alcohol use), and IPV among LGBQ+ individuals (e.g., Edwards & Sylaska, 2013; Goldbach et al., 2014; Lewis et al., 2012; Rendina et al., 2017). However, few studies have simultaneously considered interacting relations between minority stress, mental health, health risk behavior, and IPV perpetration, and even fewer studies have examined associations between these risk factors across forms of IPV perpetration.
Studies testing associations between sexual minority stress constructs and IPV perpetration have mixed findings, particularly in the relation between experiencing heterosexist discrimination and IPV perpetration. Although some research found no direct associations between heterosexist discrimination and IPV perpetration (Balsam & Szymanski, 2005; Edwards & Sylaska, 2013), others have supported this association (e.g., Longobardi & Badenes-Ribera, 2017; Stephenson & Finneran, 2017; Sutter et al., 2019; Swann et al., 2022). Studies demonstrating direct associations between heterosexist discrimination and IPV perpetration suggested that this association may be moderated by poor mental health, substance use problems, or other minority stressors (e.g., internalized homophobia; Stephenson & Finneran, 2017; Swann et al., 2022). Inconsistencies across studies highlight a need to further investigate the relation between experiencing heterosexist discrimination and IPV perpetration, as such mixed evidence suggests that heterosexist discrimination may not be independently related to IPV perpetration or may only be related to certain forms of IPV perpetration. Heterosexist discrimination may co-occur with PTSD symptoms and alcohol use (Kalb et al., 2018; Veldhuis et al., 2022), which are also risk factors for IPV perpetration (Bandermann & Szymanski, 2014; Lawrence & Taft, 2013; Roberts et al., 2010). Thus, co-occurring elevations in heterosexist discrimination and these IPV risk factors may synergistically associate with IPV perpetration among sexual minority people.
There is increasing evidence that links internalized homophobia to IPV perpetration over and above the effects of experiencing heterosexist discrimination (Edwards & Sylaska, 2013; Lewis et al., 2017). Heterosexist discrimination because of one’s sexual identity can occur in several forms, including being denied job opportunities, facing rejection, experiencing verbal harassment, and being physically assaulted. Internalized homophobia is a consequence of living in a heterosexist, discriminatory culture where LGBQ+ people direct these negative societal attitudes inward (Meyer, 1995), which may manifest in holding more negative attitudes toward LGBQ+ people broadly, disconnecting from the LGBQ+ community, and having greater discomfort accepting and disclosing their sexual identity to others (Theodore et al., 2013). LGBQ+ people who direct anti-LGBQ+ attitudes toward themselves may then project this negative self-concept onto romantic partners via IPV perpetration, as supported by a meta-analysis demonstrating a small global association between internalized homophobia and increased IPV perpetration across forms (Badenes-Ribera et al., 2019). However, this meta-analysis noted that the association between internalized homophobia and IPV perpetration across studies is often small or not statistically significant; therefore, there may be other factors that exacerbate this relation. For example, internalized homophobia may co-occur with prior experiences of discrimination and other IPV risk factors such as alcohol use and PTSD symptoms (Amadio & Chung, 2004; Straub et al., 2018). Furthermore, despite heterosexist discrimination and internalized homophobia often being studied in isolation, these stressors could also interact to predict IPV perpetration risk. For example, individuals with higher internalized homophobia may appraise experiences of heterosexist discrimination differently than those with lower internalized homophobia and, consequently, experience more distress. Further investigation of the interactions between minority stressors and other related IPV risk factors is needed to identify who is at the highest risk for IPV perpetration.
Trauma Among Sexual Minority People
Sexual minority individuals report equal or higher rates of PTSD symptoms compared to their heterosexual peers (Alessi et al., 2013; Roberts et al., 2010), which may stem from disproportionate exposure to traumatic stressors across contexts (Andersen & Blosnich, 2013). Within familial contexts, LGBQ+ people report higher rates of ACEs (e.g., physical abuse, neglect, verbal aggression) compared to heterosexual individuals (Baams, 2018; McLaughlin et al., 2012). Increased caregiver-to-child aggression reported among LGBQ+ youth could be attributed to caregivers who disapprove of gender-nonconforming behavior reacting with aggression after observing their children engage in such behavior (Andersen & Blosnich, 2013; Roberts et al., 2012). This aggression and hostility can also occur after LGBQ+ youth disclose their sexual identity to their parents (Rothman et al., 2012). In severe cases, caregivers of LGBQ+ youth can withdraw financial support and/or expel their children from their home after learning of their child’s sexual identity, which likely explains the over-representation of sexual minority identities among homeless youth (Durso & Gates, 2012; Willoughby et al., 2006).
Consistent with the intergenerational transmission of violence theory, childhood maltreatment is associated with increased IPV perpetration in young adulthood and PTSD symptoms may explain this relation (Faulkner et al., 2014; Goncy et al., 2021; McLaughlin et al., 2012; White & Widom, 2003). Several mechanisms could explain the relationship between PTSD symptoms and IPV perpetration, including elevated anger, alcohol use, and emotion dysregulation (Simpson et al., 2022; Taft et al., 2007). LGBQ+ youth are also more vulnerable to peer victimization and heterosexist hate crimes (Friedman et al., 2011; Scheer & Antebi-Gruszka, 2019) which are, in turn, related to increased PTSD symptoms and substance misuse among LGBQ+ youth and adults (Collier et al., 2013; Newcomb et al., 2012). Given that sexual minority stressors can manifest in disproportionate exposure to adverse experiences (e.g., childhood maltreatment, peer victimization) across life contexts, a trauma-informed lens should be applied to ascertain the link between sexual minority stress and IPV perpetration etiology. Although disproportionate exposure to stress and adversity is inherently harmful to the well-being of LGBQ+ people, the risk for IPV perpetration could be exacerbated by how these individuals cope with minority stress and/or PTSD symptoms, with the greatest risk being among those who use more maladaptive coping strategies (e.g., alcohol use) in tandem with elevated minority stress and/or PTSD symptoms.
Alcohol Use and IPV Perpetration
The link between alcohol use and IPV perpetration across its forms is well-supported in the empirical literature. Compared to other drugs, alcohol is the most strongly associated with violence (McKinney et al., 2010) and thus is commonly used among those who perpetrate IPV. In addition to alcohol’s direct cognitive effects on impulsive and aggressive behavior (Heinz et al., 2011), alcohol myopia theory suggests that when consuming alcohol, one’s attention narrows to the most salient factors in their environment. The individual has less information to utilize when making decisions, resulting in a higher likelihood of impulsive behavior (Steele & Josephs, 1990). This narrowing of attention and increase in impulsive behavior is a suggested mechanism for increased aggression (Giancola et al., 2010). Given the significant vulnerabilities of those with LGBQ+ identities due to minority stress and disproportionate exposure to adverse experiences, it is likely that there may be an increased effect of alcohol myopic facilitation in this population that contributes to potential increases in IPV perpetration.
Alcohol use may also co-occur with PTSD symptoms to predict IPV perpetration. Co-occurring alcohol use and PTSD symptoms are often explained through the self-medication model, which posits that individuals use alcohol to manage distress associated with traumatic experiences (Khantzian, 2003). Prior daily diary and ecological momentary assessment studies supported the self-medication model, such that greater PTSD symptoms predicted increased alcohol use on the same day and the following day (Lane et al., 2019; Simpson et al., 2014). Another daily diary study showed that, in addition to alcohol use, individuals with more distal PTSD symptoms had increased odds of psychological and physical IPV perpetration (Moore et al., 2011). Thus, it is possible that combined elevations in both PTSD symptoms and alcohol use, as well as sexual minority stress and alcohol use, may put individuals at greater risk for IPV perpetration over and above independent associations.
The Current Study
We tested whether experiencing heterosexist discrimination, internalized homophobia, PTSD symptoms, alcohol use, and interactions between each risk factor were related to increased psychological, physical, and sexual IPV perpetration among LGBQ+ young adults. In this study, we focused only on predictors of IPV perpetration because IPV in dating relationships is often bidirectional (Langhinrichsen-Rohling et al., 2012). We also only examined predictors of IPV perpetration to avoid assigning blame for violence to victims of IPV. We did this while controlling for the effects of several empirically supported correlates of IPV: age, ACEs, relationship length, and cohabitation status (Manning et al., 2018; Rickert et al., 2002). We also accounted for whether individuals held a trans/nonbinary identity, as sexual minority individuals with trans/nonbinary identities may experience sexual minority stress differently than their cisgender peers and there may be differences in IPV across gender (e.g., Bosco et al., 2022). We hypothesized that, across each two-way interaction (alcohol use × PTSD symptoms, PTSD symptoms × heterosexist discrimination, heterosexist discrimination × alcohol use, internalized homophobia × heterosexist discrimination, internalized homophobia × PTSD symptoms, and internalized homophobia × alcohol use), individuals with high levels in each combination would be at the greatest risk for IPV perpetration across forms relative to those with low levels in each combination.
Method
Participants
For sample demographics and identities, see Table 1. We recruited a sample of 342 young adults (i.e., between ages 18 and 25) in dating relationships for at least 1 month who identified as a sexual minority (i.e., lesbian, gay, bisexual, queer, pansexual, asexual, same-gender loving, or another non-heterosexual identity), had a minimum of two contact days (in person or virtually) weekly with their partner, were not fearful of their partner, and reported that they drank alcohol within the past month. We only included participants who were not fearful of their partner due to ethical concerns raised during the study’s development. In addition, we only included participants who drank alcohol within the past month as the larger study aimed to examine associations between alcohol use and IPV perpetration. The mean age of participants was 21.42 (SD = 2.02) years and 79.01% of participants were enrolled in college or graduate school. Among participants, 39.94% identified as bisexual, 19.24% lesbian, 13.41% gay, 11.95% queer, 11.66% pansexual, 0.87% asexual, and 2.62% identified as another sexual identity (e.g., same-gender loving, demisexual), were unsure of their sexual identity or did not use labels for their sexual identity. Most participants identified as women (60.23% total; 58.48% cisgender women; 1.75% transgender women), followed by men (28.65% total; 19.88% cisgender men; 8.77% transgender men) and genderqueer/gender non-conforming people (16.33%). In addition, 7.29% of participants self-described their gender identity and, among these, indicated that they were nonbinary, agender, demigirl, gender fluid, transmasculine, and transfeminine people. Most participants (78.94%) reported that their sex was assigned female at birth and the remaining were assigned male at birth (20.76%). The sample’s racial identity makeup was 87.76% White, 7.00% Asian American, 6.71% Black/African American, 5.83% Multiracial, 2.62% American Indian or Alaska Native, 0.58% Middle Eastern, and 1.75% other racial/ethnic identity (e.g., Hispanic/Latino, Mixed Caribbean). Finally, 8.45% indicated that their ethnicity was Hispanic or Latino. Notably, participants could select multiple gender and racial/ethnic identities to describe themselves; therefore, the total percentages of these identities in this sample were greater than 100%. Specifically, 10.53% of respondents selected multiple racial identities and 11.11% selected multiple gender identities. The mean relationship length was 18.74 months (SD = 17.99), 34.99% of participants reported that they live with their romantic partner, and 9.60% of participants reported that they were in a non-exclusive relationship. Across participants, 50.3% reported that they shared the same gender as their partner and 48.83% reported being in a relationship with a man, 37.13% with a woman, and 14.04% with a nonbinary/gender-expansive person.
Participant Sociodemographic Characteristics and Identities.
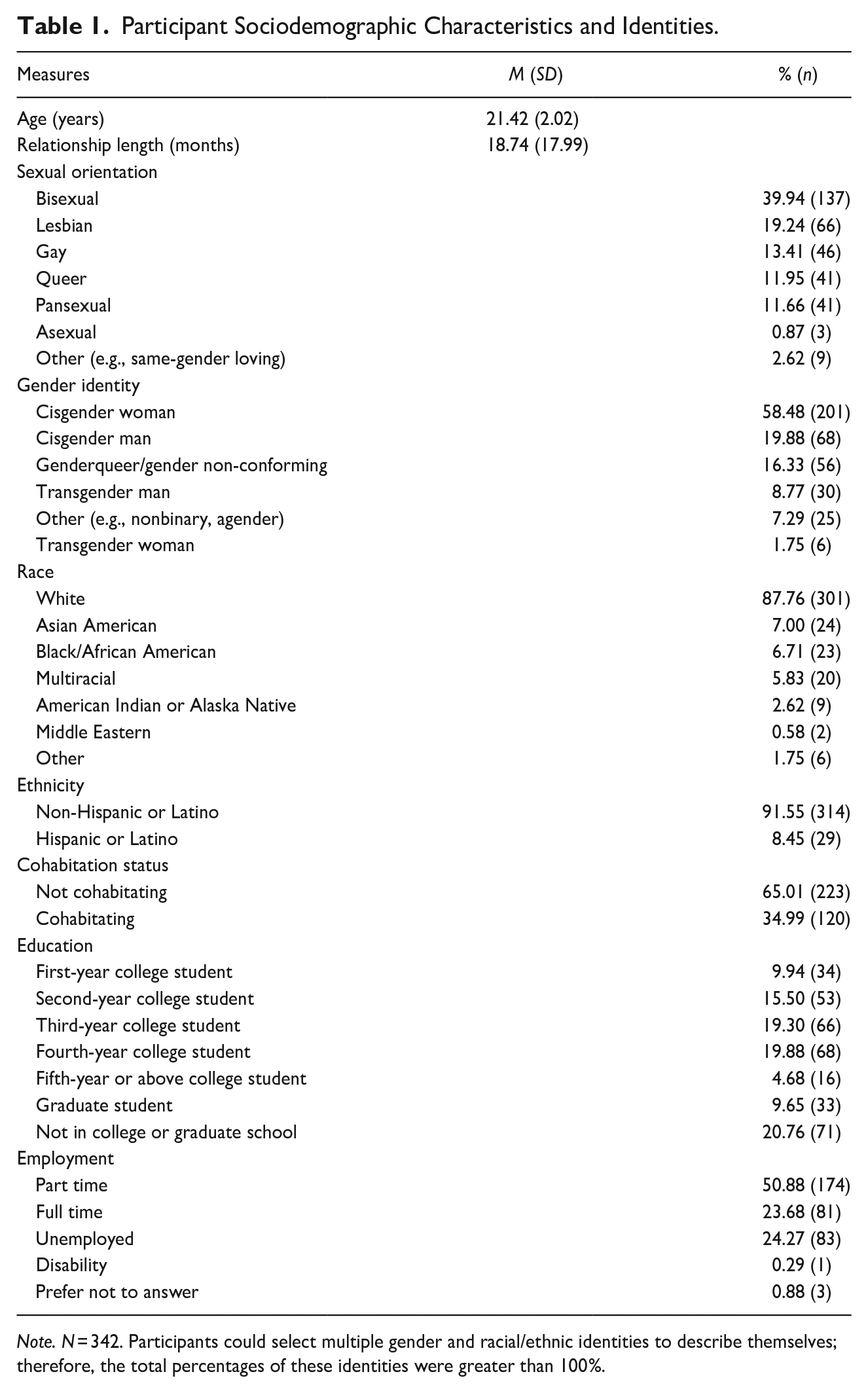
Note. N = 342. Participants could select multiple gender and racial/ethnic identities to describe themselves; therefore, the total percentages of these identities were greater than 100%.
Procedures
Study procedures were approved by the Institutional Review Board at the penultimate author’s institution. Participants agreed to participate in a larger prospective study and data for the present study are from a 2-hour baseline session where participants completed a survey. After participating, participants could either choose to receive monetary compensation or research credit in their psychology course. We recruited participants via psychology research pools at affiliated universities, flyers posted at community businesses (e.g., coffee shops), on social media (e.g., Facebook, Reddit), at LGBTQ+ Pride festivals, and through partnerships with university-affiliated Pride centers. The participants who were recruited via community events were screened for eligibility at the event, whereas those who saw the flyer completed the screener using a QR code that redirected them to a link to the screener on Qualtrics.com. This online screener assessed eligibility criteria (e.g., identifying as a sexual minority, had a minimum of two contact days weekly with their partner, were not fearful of their partner, and reported that they drank alcohol within the past month). We contacted prospective participants who screened eligible to complete the study’s baseline assessment at one of the affiliated universities—a large midwestern university or a large southeastern university. Participants could also complete the baseline assessment online via Zoom or Google Meet with study staff. During the baseline session, participants completed an online survey with a research assistant available, either in-person or online, to answer questions about the survey. All participants were provided with a list of local and national resources for IPV, substance use, LGBTQ+ support, and mental health.
Measures
Demographics
Participants reported their age, race, ethnicity, gender identity, sexual identity, relationship length (in months), and cohabitation status. We measured gender identity and sexual orientation by asking participants to select from a list of identities or to provide an alternate self-identification. Participants were also asked to select the sex that was listed on their birth certificate.
IPV perpetration
To measure IPV perpetration, we used the 50-item Conflict in Adolescent Dating Relationships Inventory (CADRI; Wolfe et al., 2001). Participants rated the frequency of perpetrating a specific conflict tactic within the past year (0 = this never happened; 6 = more than 20 times in the past 12 months). Furthermore, participants who had perpetrated IPV before, yet not in the last year, could select an option (7 = not in the past 12 months, but it did happen before) that assessed lifetime IPV prevalence. Of note, we tested study hypotheses using only past-year IPV total scores for each subscale; thus, participants who endorsed a lifetime history of IPV perpetration, but not in the last year, were scored as 0 for the present study. Participants with multiple partners were instructed to respond to items thinking about all their partners combined. Although the CADRI assessed IPV perpetration across several unique forms (e.g., relational aggression), we used only the verbal/emotional, physical, and sexual perpetration subscales to measure psychological, physical, and sexual IPV perpetration, respectively. Consistent with prior studies (e.g., Cunningham et al., 2013; Grocott et al., 2023), we modified the CADRI response choices to match the Revised Conflict Tactics Scale (Straus et al., 1996) by summing the midpoints, when needed, of each response category that participants selected (e.g., we coded answer choices “3–5 times in the past 12 months” as 4 and “more than 20 times in the past 12 months” as 25). Higher scores indicated greater IPV perpetration. The CADRI is widely used among adolescents and young adults, has performed similarly in other samples, and has well-documented psychometric properties (Cascardi et al., 2019; Shorey et al., 2019; Wolfe et al., 2001). Similar to other studies on IPV, numerous participants reported never perpetrating IPV and/or only perpetrating singular IPV tactics within a subscale (e.g., Haynes et al., 2018). This response style can restrict internal consistency; therefore, we did not calculate internal consistency, as it would poorly reflect the psychometric properties of the CADRI (Ryan, 2013).
Adverse childhood experiences
We used the 14-item ACE scale, which includes items that assess several forms of childhood adversity experienced prior to age 18 (Finkelhor et al., 2015). Each item assessed a single ACE and respondents rated whether (0 = no, 1 = yes) they experienced each ACE. A total score (0–14) was calculated by summing the dichotomous responses. The items used in the revised ACE scale have demonstrated strong psychometric properties (Finkelhor et al., 2005) and had acceptable internal consistency in this study (α = .78).
Heterosexist discrimination
The Heterosexist Harassment, Rejection, and Discrimination Scale (HHRDS; Szymanski, 2006) is a 14-item measure of heterosexist harassment, rejection, and discrimination experiences within the past year among sexual minority people. Each item is rated on a 6-point Likert scale, with 1 = the event has never happened to you, and 6 = the event happened almost all the time (more than 70% of the time) within the past year. We summed responses to each item to create a total heterosexist discrimination score. As the original HHRDS was created for women (Szymanski, 2006), we used an adapted version of the HHRDS that changes the word lesbian to lesbian/gay/bisexual person to be more gender inclusive (Katz-Wise et al., 2017). The adapted HHRDS evidenced strong internal consistency, measurement invariance, and factorial validity among diverse samples of LGBQ+ people (Denton et al., 2014; Feinstein et al., 2023; Smith et al., 2020). In this sample, the HHRDS had good internal consistency (α = .87).
Internalized homophobia
We adopted the Multi-Axial Gay Men’s Inventory-Men’s Short Version (MAGI-MSV; Theodore et al., 2013) to create an inclusive measure of internalized homophobia (IHS). The 14-item MAGI-MSV was originally validated among a sample of gay men and demonstrated strong psychometric properties across four factors (Theodore et al., 2013). For this study, we changed items to be more inclusive of numerous LGBQ+ identities and retained 12 items across three factors. These same 12 items were used in prior research assessing associations between IPV and internalized homophobia (Edwards et al., 2021). These three factors included LGBQ+ identity self-assurance and worth (e.g., “Whenever I think about my sexual orientation, I feel depressed”), public appearance of LGBQ+ identity (e.g., “Some gay man/lesbian women/bisexual individuals flaunt their sexual orientation too much”), and maladaptive measures to eliminate LGBQ+ identity (e.g., “Over the past 2 years, I have considered getting professional help to change my sexual orientation”). All IHS items were summed to create a total score of internalized homophobia. The IHS had good internal consistency in this sample (α = .86).
PTSD symptoms
PTSD symptoms were assessed using the PTSD Checklist for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (PCL-5; Weathers et al., 2013). The PCL-5 uses 20 items to assess the past month’s PTSD symptom severity after a stressful experience. Respondents rated each item on a 5-point Likert scale (0 = not at all, 4 = extremely). Responses to each item are then totaled to create a total symptom severity scale (range = 0–80), with higher scores indicating more severe PTSD symptoms. A PCL-5 cutoff score of 31 or higher reflects clinically significant PTSD symptoms (Ashbaugh et al., 2016). The PCL-5 has demonstrated strong internal consistency, convergent validity, and discriminant validity among several populations, including trauma-exposed college students and veterans (Blevins et al., 2015; Wortmann et al., 2016). In the current sample, the PCL-5 had excellent internal consistency (α = .94).
Alcohol use
Alcohol use was measured using the Alcohol Use Disorders Identification Test—Consumption items (AUDIT-C; Bush et al., 1998) which uses three items to measure alcohol use in the past year. Participants rated how often they had a drink containing alcohol in the past year (0 = never, 4 = four or more times a week), how many drinks they had on a typical day drinking in the past year (0 = none, 4 = 10 or more drinks), and how often they had six or more drinks per occasion in the past year (0 = never, 4 = daily or almost daily). Responses were summed to create a total score that ranged from 0 to 12, with higher scores indicating greater alcohol use. When screening for alcohol misuse, an AUDIT-C cutoff score of 5 or higher is recommended across gender (Bradley et al., 2007). The AUDIT-C effectively screened for alcohol use disorders and alcohol misuse among a national sample (Dawson et al., 2005). In our sample, the AUDIT-C demonstrated questionable internal consistency (α = .65). However, Cronbach’s alpha is often lower for short measures such as the AUDIT-C and the psychometric properties of the AUDIT-C are well-supported in prior studies (Bush et al., 1998; Tavakol & Dennick, 2011).
Data Analytic Strategy
Descriptive statistics and correlation analyses were conducted using SPSS Version 27.0. Study hypotheses were tested using Mplus Version 8.8, which allowed us to simultaneously regress all forms of IPV perpetration on each predictor variable. First, we ran a model testing the main effects between each predictor and the form of IPV perpetration (Model 1). Prior to running the second model that included interaction terms, we mean-centered heterosexist discrimination, internalized homophobia, PTSD symptoms, and alcohol use to account for issues of multicollinearity. We then created six interaction terms among the predictor variables (PTSD symptoms × alcohol use, PTSD symptoms × heterosexist discrimination, heterosexist discrimination × alcohol use, internalized homophobia × PTSD symptoms, internalized homophobia × heterosexist discrimination, and internalized homophobia × alcohol use). Next, we ran a second model that included all main effects and each interaction term (Model 2). Consistent with conventional approaches to interpreting interactions between continuous variables (Cohen & Cohen, 1983), we examined the effects of each variable at ±1 SD from the mean of the moderator. If no interactions were significant for a given outcome variable, we interpreted the main effects model. We tested these models using maximum likelihood with robust standard error estimation, which is robust to non-normally distributed outcome variables such as IPV perpetration. Models are considered to have acceptable model fit when the comparative fit index and Tucker–Lewis index values are above .90 and the root mean square error of approximation values are below .08 (Brown, 2015). However, both models were fully saturated, meaning that we estimated an equal number of parameters as there were values to be fitted, which resulted in a perfect model fit. Thus, we did not report model fit indices.
Results
Descriptive Statistics
For bivariate correlations, means, and standard deviations among study variables, see Table 2.
Bivariate Correlations, Means, and Standard Deviation of Study Variables.
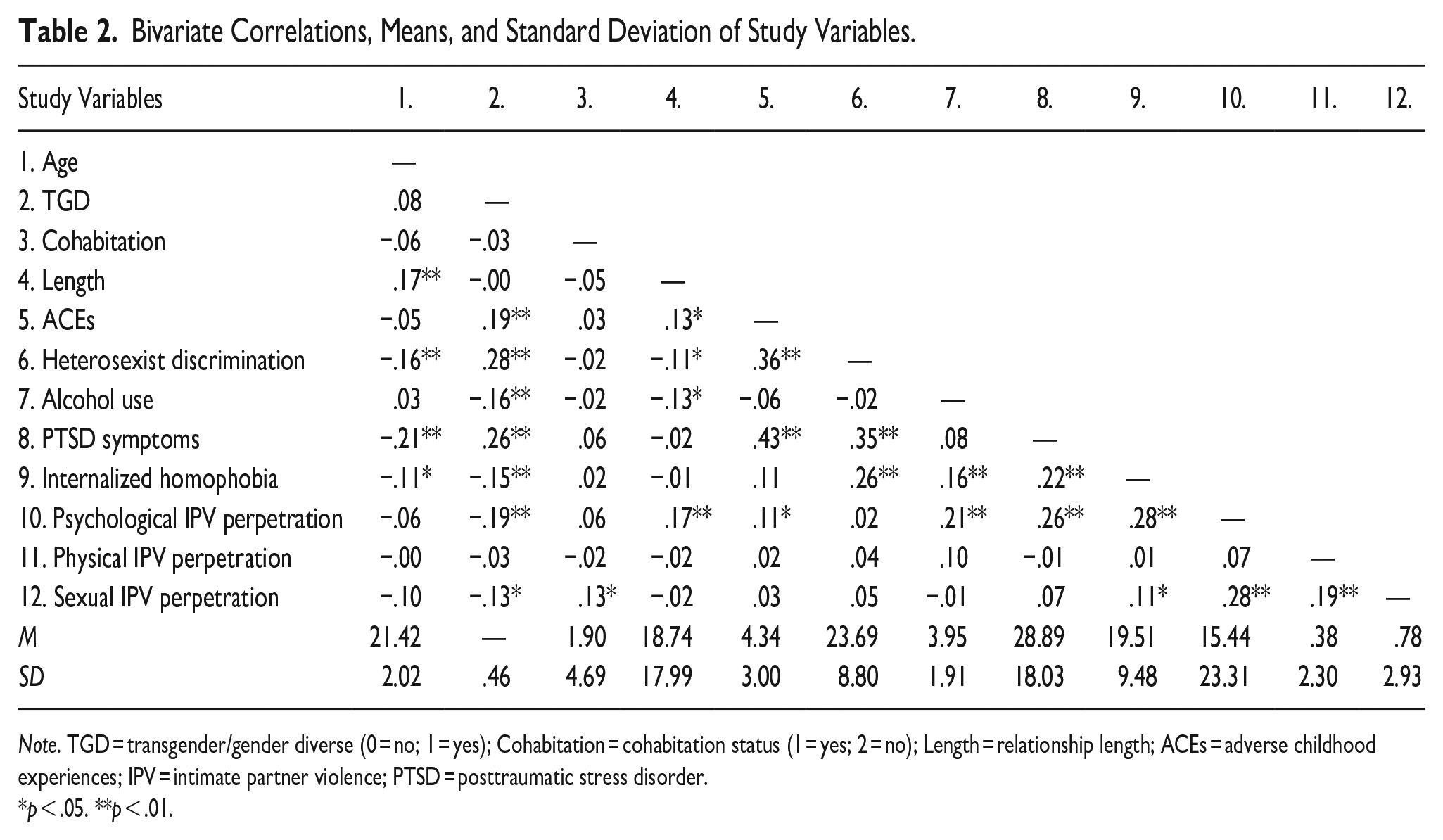
Note. TGD = transgender/gender diverse (0 = no; 1 = yes); Cohabitation = cohabitation status (1 = yes; 2 = no); Length = relationship length; ACEs = adverse childhood experiences; IPV = intimate partner violence; PTSD = posttraumatic stress disorder.
p < .05. **p < .01.
Participants reported experiencing, on average, four ACEs before age 18 (M = 4.35, SD = 3.00). In this sample, 91.49% of participants reported experiencing at least one ACE; the most endorsed ACE was experiencing feelings of loneliness and rejection (72.30%). The least endorsed ACE was having a household member go to prison (8.70%). Experiencing heterosexist discrimination was also highly prevalent in this sample, with 93.27% of participants endorsing at least one instance of past-year heterosexist discrimination. The most endorsed item on the HHRDS was hearing an anti-LGBQ+ remark from a family member (78.10%), whereas the least endorsed item was being denied job opportunities due to one’s sexual identity (5.60%).
Nearly all participants (97.38%) endorsed at least one PTSD symptom and 45.19% had a PCL-5 score of 31 or higher, reflecting clinically significant PTSD symptoms. Clinically significant alcohol misuse (i.e., an AUDIT-C score of 5 or more) was endorsed by 29.74% of participants. Perpetrating psychological IPV at least once was the most common form of past-year IPV perpetration among participants (86.01%), followed by sexual (22.74%) and physical (8.16%) IPV perpetration.
Regression and Moderation Analyses
Path analysis results for Model 1 and Model 2 are presented in Table 3. In Model 2, the results of a two-way interaction between alcohol use and PTSD symptoms revealed that the interaction term significantly predicted psychological IPV perpetration, but no other forms of IPV perpetration. PTSD symptoms positively related to psychological IPV perpetration at high (B = .57, SE = .13, p < .001) and medium (B = .33, SE = .08, p < .001), but not low (B = −.09, SE = .10, p = .39) levels of alcohol use. The interactions between internalized homophobia and PTSD symptoms, as well as between internalized homophobia and alcohol use, were also significantly related to psychological IPV perpetration. Internalized homophobia was positively related to psychological IPV perpetration at high (B = .58, SE = .12, p < .001) and medium (B = .33, SE = .08, p < .001), but not low (B = .07, SE = .11, p = .51) levels of PTSD symptoms. Internalized homophobia was also positively related to psychological IPV perpetration at high (B = 2.12, SE = .65, p = .001) but not medium (B = .99, SE = .62, p = .11) or low (B = −.14, SE = .87, p = .87) levels of alcohol use. Alcohol use was positively related to physical IPV perpetration (β = .11, SE = .05, p = .02). No other hypothesized direct effects or interactions for other forms of IPV perpetration were statistically significant.
Regression Estimates for Moderation Model.
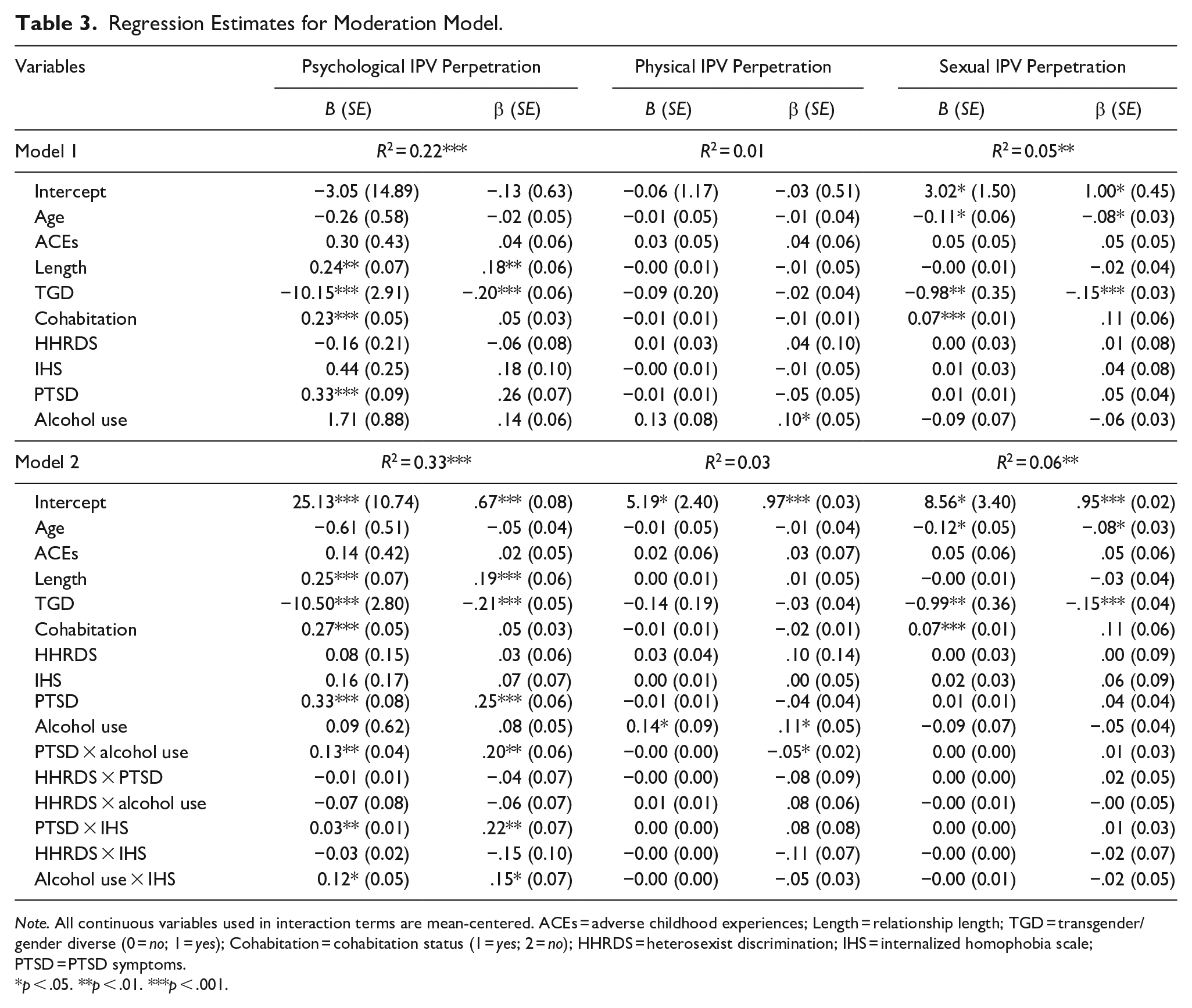
Note. All continuous variables used in interaction terms are mean-centered. ACEs = adverse childhood experiences; Length = relationship length; TGD = transgender/gender diverse (0 = no; 1 = yes); Cohabitation = cohabitation status (1 = yes; 2 = no); HHRDS = heterosexist discrimination; IHS = internalized homophobia scale; PTSD = PTSD symptoms.
p < .05. **p < .01. ***p < .001.
Discussion
This study provided a preliminary investigation into interactions between heterosexist discrimination, internalized homophobia, PTSD symptoms, and alcohol use to predict IPV perpetration in LGBQ+ young adults. In alignment with expectations, alcohol use significantly moderated the association between PTSD symptoms and psychological IPV perpetration, such that PTSD symptoms predicted increased psychological IPV perpetration at medium and high levels of alcohol use. Furthermore, the relation between internalized homophobia and psychological IPV perpetration was moderated by alcohol use and PTSD symptoms, with internalized homophobia being related to psychological IPV perpetration at medium and high levels of PTSD symptoms and high levels of alcohol use.
The moderating effect of alcohol use on the relationship between PTSD symptoms and psychological IPV perpetration, as well as between internalized homophobia and psychological IPV perpetration, is consistent with self-medication and alcohol myopia theories of IPV etiology. Specifically, these data indicate that alcohol use may be an important psychological IPV perpetration risk factor as evidenced by the higher effect sizes of PTSD symptoms and internalized homophobia on psychological IPV perpetration at high levels of alcohol use. Although there was a small, significant association between alcohol use and physical IPV perpetration, our study was not consistent with prior studies that also linked alcohol use to sexual IPV perpetration. In addition, no other hypothesized interactions or direct effects were significantly related to physical and sexual IPV perpetration. Failure to replicate these findings could be attributed to the low prevalence of sexual and physical IPV perpetration in the sample, as this limited our ability to capture variability in these constructs. These low prevalence rates in the current sample relative to national estimates may reflect our use of a less representative sample of LGBQ+ young adults, our inclusion criterion of participants not being fearful of their partners, or socially desirable responses to perpetration items.
Another notable finding was the interaction between PTSD symptoms and internalized homophobia as they related to psychological IPV perpetration. This finding underscores the notion that co-occurring elevations in mental disorder symptoms and minority stress may contribute to IPV perpetration risk. Specifically, our study demonstrated that the relation between internalized homophobia and psychological IPV perpetration was contingent on having at least a moderate level of PTSD symptoms and this association strengthened as PTSD symptoms increased. Prior empirical work has suggested that the development of internalized homophobia may often be a consequence of living in non-affirming environments and/or facing adverse experiences (e.g., discrimination, childhood maltreatment) associated with one’s LGBQ+ identity (Gold et al., 2011; Meyer, 1995), all of which may also contribute to elevations in PTSD symptoms. In turn, specific features of PTSD symptoms that are often associated with IPV perpetration (e.g., anger, hypervigilance) may specifically exacerbate this relation. Our findings were also consistent with prior research that linked internalized homophobia to internalizing mental health problems (e.g., Newcomb & Mustanski, 2010). Further investigation of the associations between internalized homophobia, PTSD symptoms, and IPV perpetration is needed.
Although study results did not support any associations between heterosexist discrimination and IPV perpetration, this does not refute the deleterious effect of experiencing discrimination on the mental health of LGBQ+ young adults. Rather, PTSD symptoms, internalized homophobia, and alcohol use merely explained more variability in psychological IPV perpetration outcomes than heterosexist discrimination. Considering that heterosexist discrimination was moderately correlated with PTSD symptoms and internalized homophobia, these mechanisms could mediate the relation between experiencing heterosexist discrimination and IPV perpetration. However, this study’s cross-sectional design prevented us from testing these mediating associations. In addition, our study’s cross-sectional design prohibited us from inferring causality and the temporal associations between these constructs. Future longitudinal studies should investigate the temporal relations between minority stress, PTSD symptoms, alcohol use, and IPV perpetration.
Clinical and Policy Implications
Study results highlight key mechanisms, likely exacerbated by experiencing minority stress, that should be targeted for IPV prevention among LGBQ+ young adults. These findings are consistent with prior recommendations by Edwards et al. (2020) for IPV prevention programs, which include simultaneously combatting structural stigma while providing LGBQ+ people with adaptive coping resources for minority stress. In particular, these findings suggest that IPV prevention programs should focus on reducing alcohol use among LGBQ+ individuals with internalized homophobia and PTSD symptoms. Furthermore, because alcohol use and the presence of PTSD symptoms accounted for a large portion of variability relative to heterosexist discrimination, addressing both alcohol use and trauma through intervention may be especially important for this population. Research in comorbid treatment development suggests that targeting both PTSD symptoms and alcohol use simultaneously is highly efficacious yet underutilized by clinicians (Buckheit et al., 2022). Considering the elevated risk for trauma and alcohol use in LGBQ+ individuals, especially in the presence of internalized homophobia, a multifaceted approach to treatment and early intervention is necessary.
Limitations and Future Directions
Several limitations should be considered when interpreting these findings. First, PTSD symptoms were assessed without determining an index trauma event prior to completing the PCL-5. Future studies on the relation between PTSD symptoms and IPV perpetration should identify the specific index trauma participants refer to when completing the PCL-5. It is possible that ACEs could underlie the development of PTSD symptoms and potentially increase the risk for minority stress, alcohol use, and, in turn, IPV perpetration. Therefore, future longitudinal studies should investigate the mediating effects of minority stress, PTSD symptoms, and alcohol use between ACEs and IPV perpetration. In addition, nearly 10% of participants were in non-exclusive relationships. These individuals in non-exclusive relationships may have reported violence related to multiple partners, which may make their experiences less comparable to those in exclusive relationships. Furthermore, the inclusion criterion that participants were not fearful of their partners may have led to truncated scores and, consequently, nonsignificant findings between risk factors and sexual and physical IPV perpetration. This inclusion criterion may also have limited the generalizability of study findings to other LGBQ+ young adults in dating relationships. Next, this study found several significant associations between covariates and each form of IPV perpetration. Notably, our findings suggested that people with trans/gender-expansive identities were less likely to perpetrate sexual and physical IPV relative to cisgender individuals. Future studies with LGBTQ+ individuals could consider the influence of these covariates on IPV risk.
Furthermore, this sample had a limited representation of LGBQ+ people of color and was primarily comprised of college-educated LGBQ+ young adults, which hinders the generalizability of study findings. Future research should investigate these associations with more diverse samples of LGBQ+ people and consider the risk for trauma exposure and minority stress through the lens of intersectionality (i.e., among people who hold multiple minoritized identities). For instance, given that racial minorities tend to experience significant racism that exacerbates coping (Meyer et al., 2008) as well as discrimination from within sexual minority communities (Balsam et al., 2011), and bi+ (i.e., bisexual, pansexual, queer) people tend to experience the highest rates of alcohol use (Shokoohi et al., 2022) and trauma relative to other sexual minorities (Alessi et al., 2013; Roberts et al., 2010), it is likely that examining trauma exposure and minority stress with a more diverse sample through an intersectional framework would reveal a more nuanced understanding of study variables. Although our sample had a diverse representation of sexual and gender identities, our sample size resulted in limited statistical power to test differences across these subgroups. More research is needed investigating subgroup differences across sexual, racial/ethnic, and gender identities considering the heterogeneous experiences of LGBQ+ people.
Conclusion
This study aimed to identify which combinations of risk factors related to IPV perpetration in a sample of LGBQ+ young adults. We found that PTSD symptoms interacted with alcohol use to predict psychological IPV perpetration at high and medium levels. Internalized homophobia was related to psychological IPV perpetration at high and medium levels of PTSD symptoms and only high levels of alcohol use. These findings were consistent with extant research linking PTSD symptoms, alcohol use, and internalized homophobia to IPV perpetration. These interactions highlight the need for comprehensive prevention and clinical intervention for LGBQ+ young adults that target these multiple risk factors. Future research may aim to investigate the temporal relationship between these risk factors to develop more specialized interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: Research reported in this publication was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under Award Number R01AA027248. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.