
Abstract
The objectives of this study were to measure the prevalence of mental distress and to explore the relationship between violence against women (VAW), social support, self-esteem, and mental distress in women in Riyadh, Saudi Arabia. A questionnaire-guided, cross-sectional, interview-based study was conducted with 1,932 women, in primary healthcare centers. Around 29% reported moderate to severe distress levels, whereas 40% of women reported lifetime exposure to at least one type of violence. Linear regression analysis found that VAW was positively associated with mental distress with a unit increase associated with a 0.13 (0.58, 1.15) increase in distress level, whereas, for both social support and self-esteem, a unit increase in violence was associated with −0.23 (−0.47, −0.32) and −0.22 (−0.49, −0.33) unit decrease in the mental distress. Structural equation modeling found that violence had direct significant negative effects on social support (β = −.156, p < .001) and self-esteem (β = −.135, p < .001). Both social support (β = −.266, p < .001) and self-esteem (β = −.183, p < .001) had direct significant negative effects on distress. VAW exerted a direct significant positive effect on distress (β = .171, p < .001) as well as an indirect effect (β = .068, p < .001). Both social support (β = .044, p < .001) and self-esteem (β = .025, p < .001) were significant mediators of the effect of violence on mental distress. VAW can lead to mental distress and low self-esteem. Identification, counseling, and social support for women are important to improve their self-confidence and reduce the adverse effects of violence.
Background
Violence Against Women and Mental Health
Mental or psychological distress refers to emotional suffering and maladaptive psychological functioning as a result of experiencing stressful events (Abeloff et al., 2000; Drapeau et al., 2012). Systematic review and meta-analysis have reported that a significant percentage of women exposed to intimate partner violence (IPV) suffer from major depressive disorder, elevated depressive symptoms, and postpartum depression (ranging from 9% to 28%) (Bacchus et al., 2018). A bidirectional relationship exists between violence and depression (Oram et al., 2017; Sousa et al., 2021); abused women were 1.76 (1.26–2.44) times more likely to report mental disorders, whereas depressed women were 1.72 (1.28–2.31) more likely to be abused. In addition, IPV was associated with a 2.19 (1.39–3.45) times increase in postpartum depression (Avdibegovic et al., 2017).
Mental distress stimulates physiological changes (van den Heuvel et al., 2018), leading to devastating physical health. However, in the context of victimization, individuals’ inner and external resources play a varying role in causing mental distress (Turner et al., 2017). Hence, consideration should be given to the effect of violence on women’s mental distress, particularly the mechanism by which violence leads to psychological (mental) distress and the mediating role of inner and external resources, such as social support and self-esteem.
Pearlin’s theory assumes that a high level of stress exposure predicts a higher level of psychological distress (Pearlin et al., 1981). Stressful life events impact individuals’ self-concept, such as self-esteem and psychosocial resources. These two aspects work as mediators (intervening factors) between stressful events (such as violence) and mental distress which is the stress outcome (Avison et al., 2009; Pearlin et al., 1981). It means that stressors play a role in developing mental distress, while self-concept and social resources explain the mechanism in developing the intensity of this outcome. According to this theory, the stressor is conceptualized to be a difficult chronic strain in an individual’s life (Pearlin & Bierman, 2013; Pearlin & Skaff, 1995). These life events could be victimization experience which has chronic nature. Thus, Pearlin’s theory of psychological distress is used in this current study as a theoretical framework. Based on this, we hypothesized that violence against women (VAW) predicts higher-level mental distress directly and indirectly through the mediating effects of social support and self-esteem. It means VAW suggest a lower level of social support and self-esteem, and both of these predict mental distress.
The pooled estimated prevalence of any type of VAW in Arab countries was reported to be 73% (Hawcroft et al., 2019). Prevalence estimation may not be accurate due to societal acceptance, attitude, and justification for violence, whereas this attitude is lower in North America compared with sub-Saharan Africa (Ibala et al., 2021; Schwab-Reese & Renner, 2017). The lifetime prevalence in Saudi Arabia for VAW is around 40%, which is slightly higher than the global prevalence (Abolfotouh & Almuneef, 2020). Like elsewhere, violence in Arab countries is shaped by early childhood experiences, marital conflict, and socioeconomic, community, and cultural factors (Alhalal et al., 2021). Social support from family and friends is crucial for women in the context of domestic violence (Afifi et al., 2011; Bohlaiga, 2014) as they tend to avoid seeking outside help (Afifi et al., 2011; Barnawi, 2017) except with few that prefer to turn to informal sources of support (Alzahrani et al., 2016). These women also experienced adverse mental health outcomes such as posttraumatic stress disorder, depression symptoms (Alhalal, 2016), anxiety, panic attacks (Alhabib, 2011), and suicidal thoughts (Eldoseri et al., 2014). It means women who experience violence might feel themselves emotionally overwhelmed.
Outcomes of VAW
Research in the area of VAW has substantially shown the negative effects of violence on women’s health such as abortion, premature labor, hypertension, diabetes, and restricted daily activity, and on mental health outcomes such as depression, anxiety, memory, and sleep problems (Bonomi et al., 2009; Moulding et al., 2021; Park et al., 2017). A study of more than 3,000 women showed that women victimized by IPV were at higher risk of having medical, psychosocial/mental, and female reproductive problems compared with never abused women (Bonomi et al., 2009). Another survey of 600 IPV-victimized women reported that 90% claimed poor psychological well-being and 52% were diagnosed with mental illnesses (Moulding et al., 2021). The authors concluded that the impact of IPV on women’s mental health undermines her status as a person and a citizen, and focuses only on the mental illness. A study by Al Serkal (2014) found that emotional distress, suicidal thoughts, and suicidal attempts were reported to be higher among victims of IPV compared with non-victimized women. A study of a cohort of more than 20,000 women reported that women who are victims of IPV have lower scores on the quality-of-life scale and higher prevalence of mental distress compared with women who are exposed to violence from strangers (30% vs. 12%) (Hisasue et al., 2020).
Psychological distress could be the beginning of mental health issues, such as anxiety and depression. The American Psychological Association defines psychological distress as “a set of painful mental and physical symptoms that are associated with normal fluctuations of mood in most people” (American Psychological Association, 2022). It includes depression, anxiety, and somatic symptoms (Kessler et al., 2003). Women experience high mental distress when involved in a violent relationship (Vilariño et al., 2018; Williams & Frieze, 2005). However, it was found that only psychological type of violence predicts women’s mental distress (Hill et al., 2007). The way in which violence affects women’s mental distress has not been extensively examined. In addition, the relationship between VAW and mental distress as maladaptive functioning and outcome should be understood in different cultural contexts (Bryant-Davis, 2019). Among Arab women, including Saudi Arabia, the impact of violence on women’s mental distress has not been examined.
Social Support and Self-Esteem
Social support is considered a protective factor against violence. Women subjected to violence usually suffer from low self-esteem and low social support leading to depression, which may cause a lack of interest and increase the chances of re-victimization (Duru et al., 2019). In a study on IPV-associated mental health adverse outcomes, it was found that young victimized mothers aged 16 to 25 who perceived less social support were more likely to have high anxiety symptoms (Choi et al., 2021). Similar to social support, low self-esteem is recognized as a risk factor for IPV victimization (Papadakaki et al., 2009). A meta-analysis of 80 longitudinal studies showed that low self-esteem served as a risk factor for depression and anxiety, while anxiety was found to have a reciprocal relation with self-esteem, depression had less effect on self-esteem (Sowislo & Orth, 2013). It is proven that self-esteem is high during adolescence and tends to decline during old age (Orth et al., 2012). In a longitudinal study with 213 individuals, the authors reported a reciprocal association between self-esteem and social support, where high self-esteem at age 36 predicted high social support 6 years later, that is, at age 42, and vice versa (Kinnunen et al., 2008). Hence, for better mental health, adequate social support should be made available, especially during childhood and middle age to maintain high self-esteem.
Mental disorders including anxiety disorders and nicotine and alcohol abuse are found to be higher among women victimized by IPV (An et al., 2019). A large study established the association between smoking and excessive drinking with low self-esteem (Szinay et al., 2019). Similarly, a large meta-analysis of 53 longitudinal studies of subjects aged between 4 and 76 years from multi-ethnic backgrounds reported that individual perception of social relationships is strongly influenced by self-esteem (Harris & Orth., 2020). Hence, both low self-esteem and social support, directly and indirectly, impact the effect violence has on causing distress among IPV victims.
Few studies are available on self-esteem, self-efficacy; and social support from Saudi Arabia; however, many of these were conducted among university-going female students, with context to academic achievements, empowerment, or physical appearance (Aldhahi et al., 2022; Al-Qahtani et al., 2021). A large-scale study conducted on 15 universities in Saudi Arabia found that around 70% of the women scored high on the self-esteem scale. It was concluded that both self-esteem and self-efficacy are important for women’s empowerment (Al-Qahtani et al., 2021). The research on social support in Saudi Arabia is in its preliminary stages. Studies have measured social support in the context of menopausal aged women and found that a lack of emotional and tangible support was associated with poor quality of life (AlQuaiz et al., 2017). Although the local culture and traditions emphasize social relationships, still, there is a significant percentage of women with inadequate or lack of support (Abdel-Khalek et al., 2013).
VAW in Saudi Arabia
The Saudi government has recently passed a law in protecting women against violence (Ministry of Social Affairs, 2017). In terms of attitude toward the issue, 80.5% see violence as a private family issue and 49% of married women believe that they should follow their husbands’ orders (Eldoseri et al., 2014). A systematic review revealed that 34.3% to 57.7% of Saudi women experience violence during their lifetimes (Kazzaz et al., 2019), yet limited information is available on the role of mediating factors such as social support and self-esteem in women exposed to violence. The purpose of this study was to measure mental distress and to test the hypothesized model in which social support and self-esteem mediate the association between VAW and mental distress in women in Saudi Arabia.
Methods
Study Design and Setting
A cross-sectional survey was conducted with Saudi women using a simple random sampling strategy. A total of 18 primary healthcare centers (PHCCs) were randomly selected from a list of 105 PHCCs belonging to five administrative regions of Riyadh City. In addition, 13 private institutes were also approached and included in the study to represent working women. The study was approved by the Institutional Review Board (E-12-658) and Institutional Review Board of the Ministry of Health, Dammam (IRB ID MOH0151), Saudi Arabia.
Sampling Methods
Prior to data collection, rigorous efforts were put in to advertise the study in both public and private settings using posters, pamphlets, and announcements. On average, the data collection team spent 2 weeks in each of the selected PHCCs to include all eligible participants. The inclusion criteria were all Saudi, Arabic-speaking, and non-pregnant women, whereas we excluded women with gross mental incapacity. All females visiting the PHCC and fulfilling the inclusion criteria were approached and invited to participate. Written informed consent was taken from each woman. The refusal rate was around 10%. Initially, more than 2,000 women gave consent to participate; however, 68 forms were discarded due to incompletion, and 1,932 participants were included in the analysis. The sample comprised of both young (46% were <40 years) and middle-aged population (30% were >50%). Among 1,932 participants, around 7% (n = 139) were unmarried, 75% were currently married, and around 8% were divorced. Polygamy was reported by 20% of women, with only 2% mentioning the husband having more than two wives.
Data Collection Procedure
A team of five female data collectors conducted the questionnaire-based interviews in Arabic with each of the women separately. Separate rooms were arranged for conducting the interviews in each of the selected PHCC and the private offices. It was ensured that privacy is maintained during the interviews. The data collectors were trained on developing rapport with the participant, explaining to her the reason and importance of the study, satisfying her apprehensions related to confidentiality, and making them comfortable in answering all types of questions. Each interview took around 20 to 25 minutes. Informed and signed consent was obtained from each participant.
Safety Protocol
The safety and well-being of the participants were ensured at each stage. The participants who reported violence were given the contact number of the National Family Safety Program (NFSP), which is a national program aiming to serve the victims of abuse, and the national hotline for reporting violence under the family protection department at the Ministry of Human Resources and Social Development (Ministry of Social Affairs, 2017). All participants were asked to follow up with their family physician. The helpline for reporting violence has workers available 24/7. The NFSP and the social protection department not only provide social support but also provide legal and judicial support to the victims. The safety and well-being of the participants were also ensured, and participants with K-10 of ≥25 were asked to follow-up with their family physician or psychologist in PHCC.
Measurements
The structured questionnaire comprised of sociodemographic profile, reproductive health questions, in addition to the questionnaires on VAW, mental distress, social support, and self-esteem.
WHO Questionnaire on VAW
We utilized the violence-related questions from the WHO Multi-country Study on Women’s Health and Domestic Violence (World Health Organization [WHO], 2005). The questionnaire has been translated and utilized (including the Arabic version) in many countries across the world. For the married women, the questions referred to any violence by their husband and for the unmarried, the questions referred to violence by the woman’s father or brother. In total, the questionnaire comprised 19 items covering different types of violence, namely, controlling behavior, emotional, physical, and sexual violence. Controlling behavior comprises questions of husband-imposed restrictions on whom she met and where she went. The emotional violence included questions on threatening, insulting, and scaring. Physical violence included all types of physical abuse actions ranging from slapping to kicking, beating, and burning. Sexual abuse inquired about forceful or humiliating sexual actions. Frequency for each item was measured using the Likert scale (all of the time [many times], most of the time [few times], a sometime, bit of the time [rarely], and never). Separate and total scores were computed for the violence and its type. The Cronbach’s alpha for the questionnaire was .85.
Kessler Psychological Distress Scale (K-10)
Mental distress was measured using a validated, pre-tested 10-item questionnaire (Kessler et al., 2003). The K-10 comprises questions on anxiety such as feeling nervous and restless and questions on depression such as feeling hopeless and worthless. The total score was calculated for each participant by adding all the responses. According to the scoring protocol, participants with scores <20 denote no distress, scores ranging between 20 and 24 are considered as mild distress, scores between 25 and 29 are moderate distress, and scores ≥30 as severe mental distress. The Cronbach’s alpha value for the scale was .88.
Rosenberg Self-Esteem Scale
Self-esteem was measured using the Rosenberg self-esteem scale (RSES) (Rosenberg et al., 1995). It was previously translated into Arabic language and utilized by multiple studies (Abdel-Khalek, 2016; ALAhmari et al., 2019). RSES comprises 10 questions with positive and negative statements related to self-esteem. Positively worded questions ask about self-worth, success, feeling proud, and satisfied, whereas negative questions are phrased to ask about failures, disrespect, and feeling useless. The responses are graded using the Likert scale, with totally disagree as 1 to totally agree as 4. The responses are added to obtain a total score ranging from 10 to 40, with high scores indicating high self-esteem. The Cronbach’s alpha value for the scale was 0.80.
Social Support Survey Scale (4S)
Social support survey scale was utilized to measure social support (Sherbourne & Stewart, 1991). The scale comprises four questions, two measuring emotional support and the rest measuring tangible support. Emotional support inquires whether someone is available to listen to you or talk to you, whereas tangible support inquires about any help available for doing household chores or taking her to the doctor. Responses were measured using the Likert scale ranging from 1 to 5, with social support available all the time ranked as 5 and no support available as 1. The Cronbach’s alpha for the social support items was .83
Statistical Analysis
Descriptive data are presented by calculating the means (standard deviation) for the continuous and frequency percentages for the categorical variables. The univariate and hierarchical linear regression analyses were conducted to identify the significant factors associated with mental distress. The factors significant in univariate analysis were entered into the multivariate model. The p<.05 was taken as significant.
Using MPLUS version 8, structural equation modeling (SEM) with the maximum likelihood method of estimation was conducted to test the hypothesized model. SEM is an advanced regression technique that estimates the linear causal relationships between the observed and latent variables, including both direct and indirect (mediating) effects (Kline, 2011). In the analysis, both violence and social support were latent variables, while self-esteem and mental distress were treated as observed variables. Social support and self-esteem were allowed to be correlated. In this model, we account for the effect of women’s age, marital status, and education. To determine whether the model fits the data, we used fitting indices, which were the root-mean-squared error of approximation (RMSEA), standardized root-mean-squared residual (SRMR), comparative fit index (CFI), Tucker–Lewis Index (TLI), and chi-squared. Standardized (β) and unstandardized path (B) coefficients were reported to compare the strength of paths within models and across the models.
Results
Table 1 is showing the sociodemographic characteristics of the 1,932 women, having a mean age of 43.91 (±10.98) years, ranging from 30 to 75 years. Univariate analysis found that age, education, and occupation were significantly associated with mental distress.
Association between Socio-Demographic, Anthropometric, and Health-Related Characteristics of Women with Mental Distress in Riyadh City, Saudi Arabia (N = 1,932).
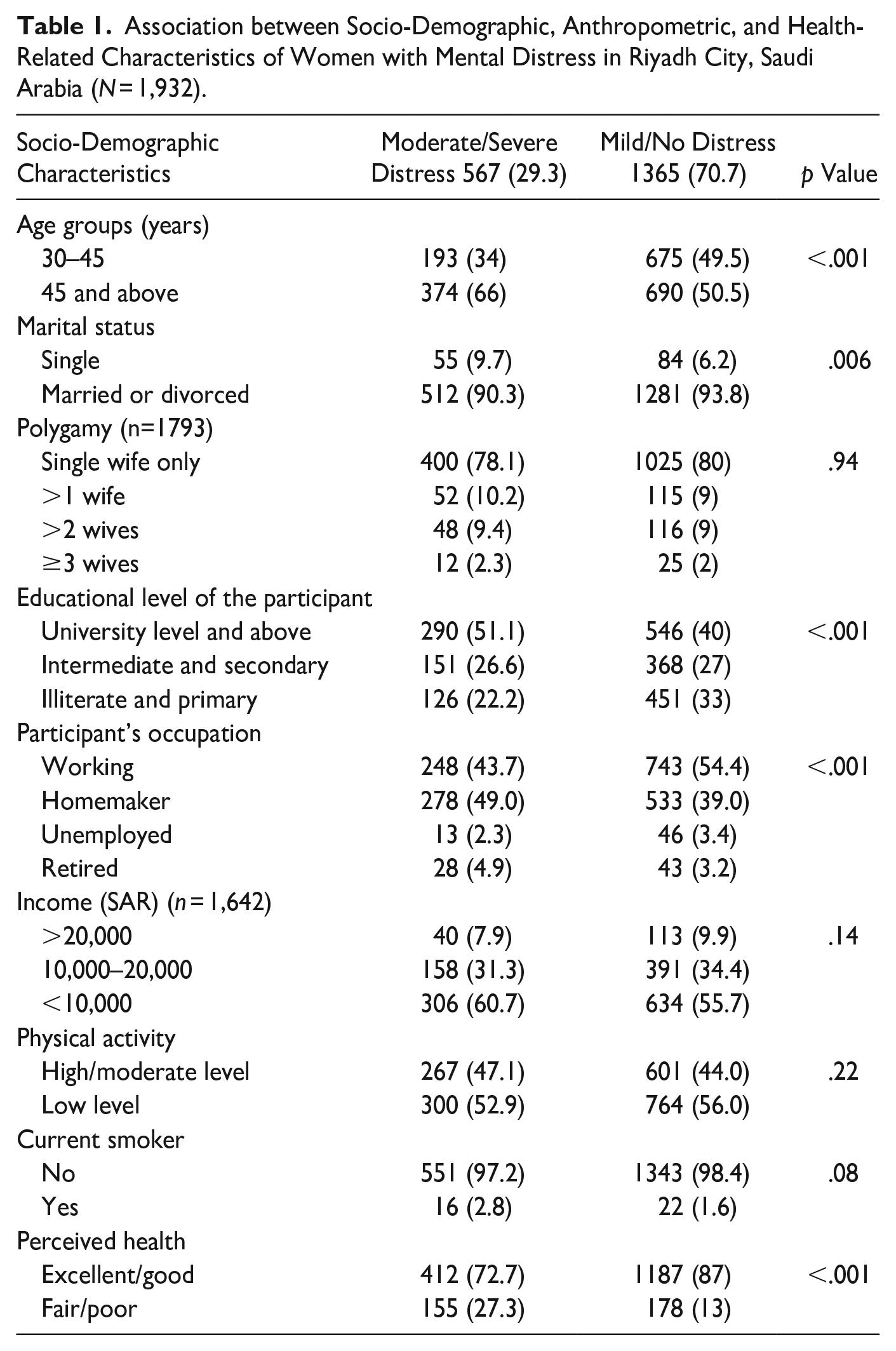
Table 2 is showing the reported frequency of mental distress (K-10) items. Women ≥45 years, single in status, with high education level, and housewives were more distressed as compared to their counterparts. The average K-10 scores were 21.46 (±7.49), indicating mild mental distress. Categorical data found that 45% (n = 872) were without distress (scores <20), whereas among the remaining 25.5% (n = 493), 13.7% (n = 264), and 15.7% (n = 303) were suffering from mild, moderate, and severe distress, respectively. Around 7% (n = 130) of women reported that they felt like hurting themselves and wished they were dead. Similarly, women perceiving their health status as poor were showing high distress levels (p < .001).
Frequency of Women Reporting Mental Distress Symptoms in Riyadh City, Saudi Arabia (N = 1,932).
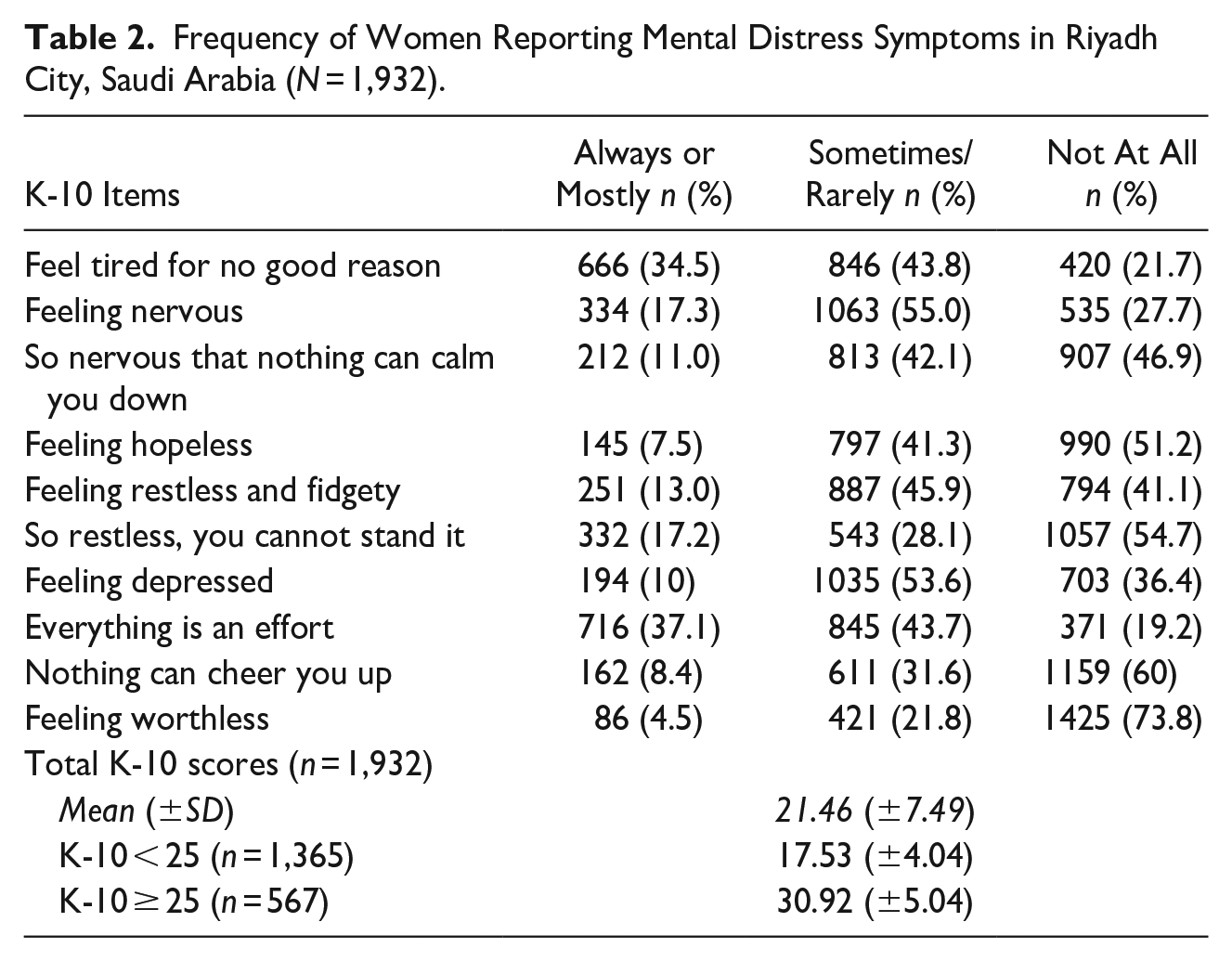
Table 3 is showing the reported frequency of violence and its type. The lifetime prevalence for any type of violence was reported by 40.6% of women (n = 784). 93% of women in our study were married, and they were referred to VAW by a male spouse member, whereas 7% of unmarried women reported violence by male members like their father or elder brother. Descriptive analysis found that controlling behavior was the most frequent type, reported by 38% of women, specifically, to take permission before seeking health care was reported by 16.8% (n = 324). Around 8% and 5.4% reported that their spouses blamed them for disobeying and not completing the household work, respectively.
Prevalence of Domestic Violence Reported by Women in Riyadh, Saudi Arabia (N = 1932).
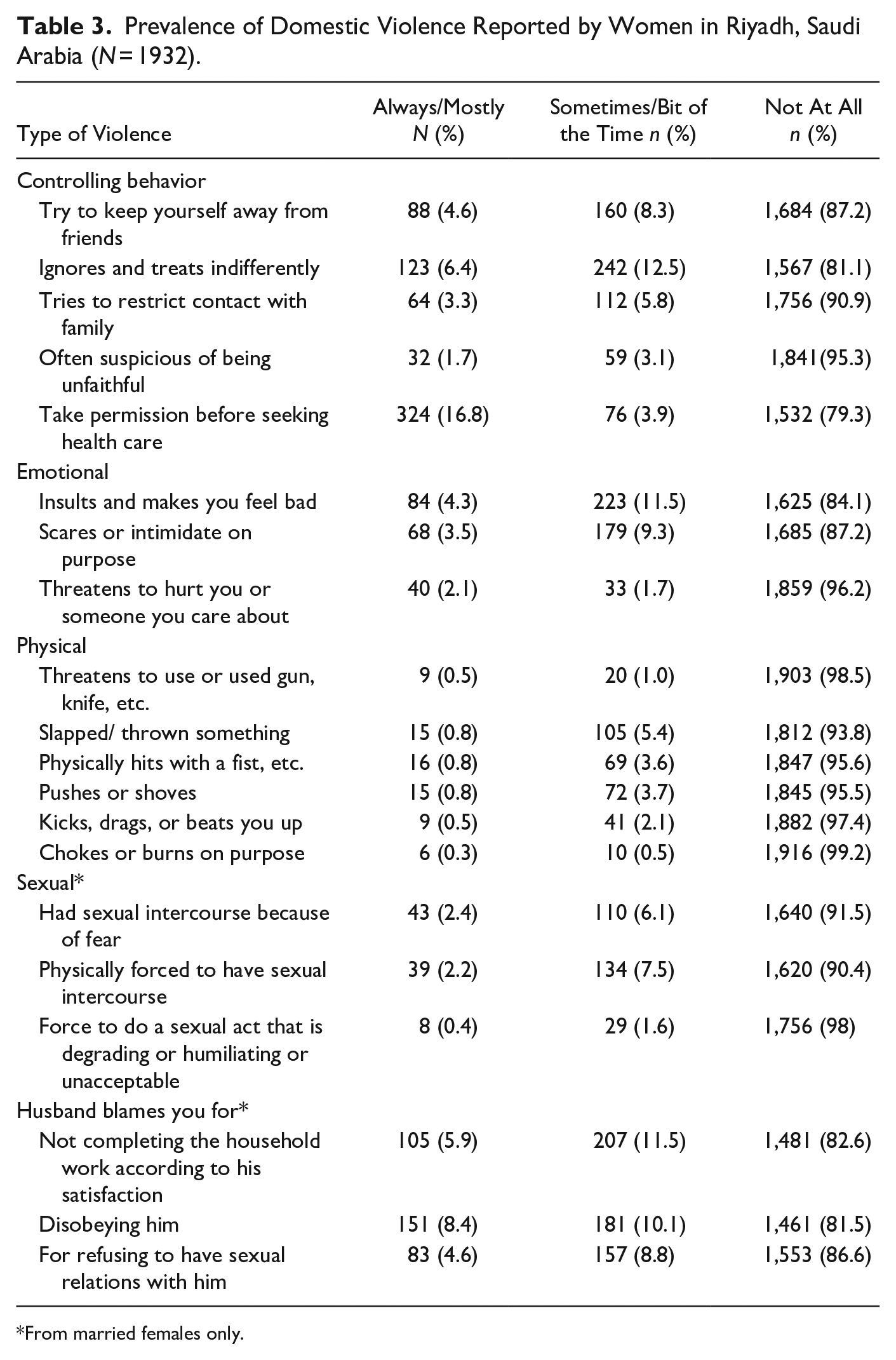
From married females only.
The average self-esteem scores were 21.53 (±3.96), with 22.5% (n = 434) women having scores >15, whereas 5% (n = 97) had scores <15. Pearson correlation coefficient “r” found that mental distress scores were significantly negatively correlated with age (r = −0.24, p < .001) and self-esteem (r = −0.26, p < .001). Similarly, a positive correlation was observed between mental distress and lack of emotional (r = .26, p < .001) and lack of tangible support (r = 0.26, p < .001).
Bivariate Association
Pearson correlation value between total self-esteem scores and violence was r = −0.12 (p < .001). Among different types of violence, there was a moderate and significant correlation between emotional abuse and self-esteem (r = −0.12, p < .001) and controlling behavior and self-esteem (r = −0.11, p < .001), whereas the correlation between self-esteem and sexual violence (r = −.09, p < .001) and physical violence (r = −0.08, p < .001) were significant but weak.
Hierarchical Linear Regression
Table 4 is showing the hierarchical linear regression analysis. The univariate analysis identified that age, education, and occupation were significantly associated with mental distress; however, education and occupation were correlated with each other (r = 0.30). Hence, we adjusted for age and education in the final model.
Univariate and Hierarchical Linear Regression Analysis Showing Association between Domestic Violence, Social Support, and Self-Esteem with Mental Distress in Women in Riyadh City, Saudi Arabia.
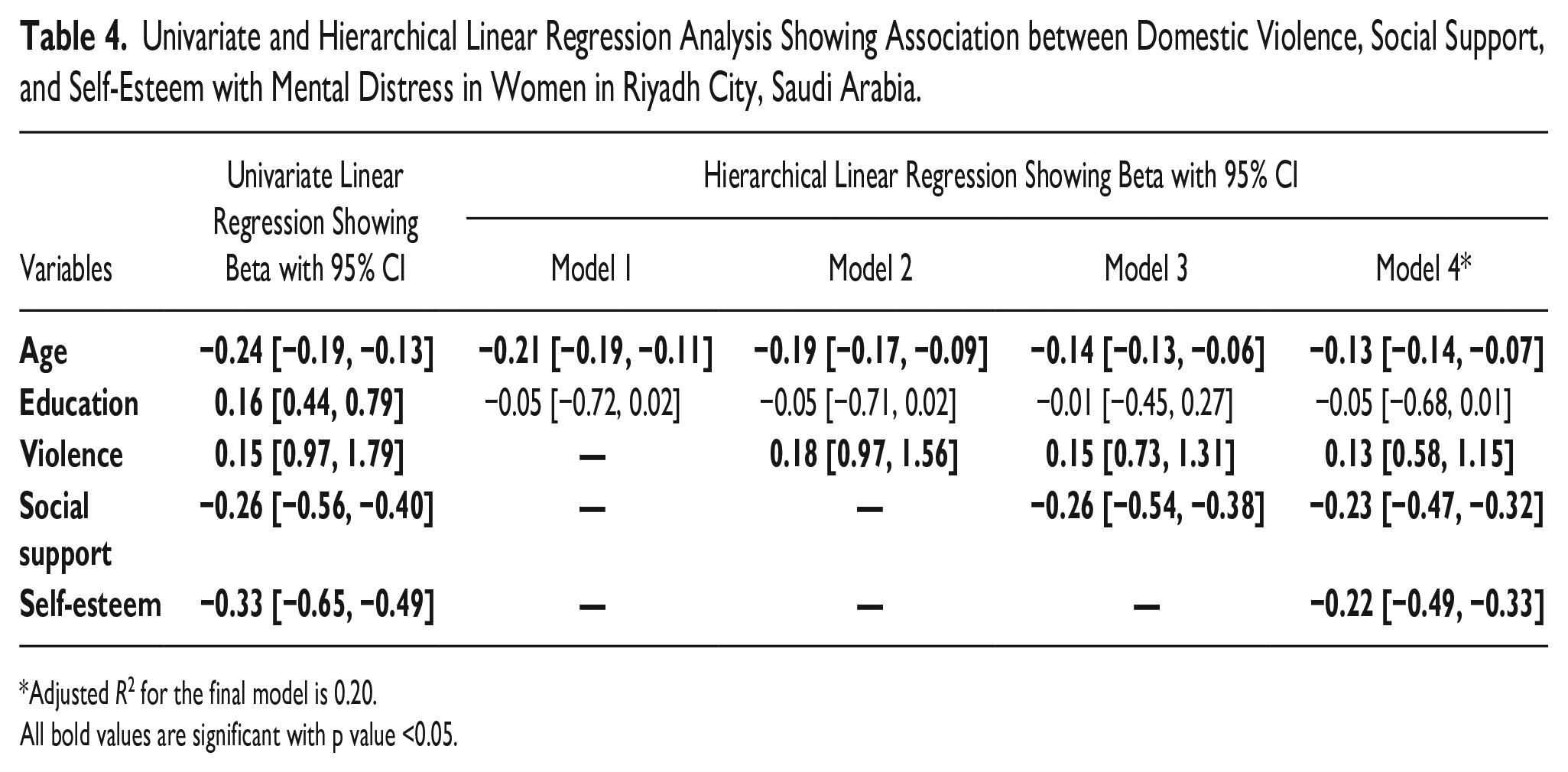
Adjusted R2 for the final model is 0.20.
All bold values are significant with p value <0.05.
In the multivariate model, the sociodemographic variables, age and education, were entered in the first step, followed by violence, social support, and self-esteem in subsequent models. The final model shows that a unit increase in age is significantly associated with a −0.13 (1.14, −0.07) unit decrease in distress scores. A unit increase in violence was associated with a 0.13 (0.58, 1.15) increase in distress level. Both a unit increase in social support and self-esteem were associated with −0.23 (0.47, 0.32) and −0.22 (−0.49, −0.33) unit decrease in the mental distress scores.
Structural Equation Modeling for Hypothesized Model
Standardized factor loadings for the latent measures (violence and social support) were statistically significant with magnitude ranging from 0.636 to 0.954. Controlling for women’s age and education, the model showed an excellent fit with the data (Figure 1), χ2 (26) = 75.44, CFI = 0.989, TLI = 0.982, RMSEA = 0.031 (90% CI [0.023–0.040]), and SRMR = 0.015. Standardized regression coefficients (β) and unstandardized coefficients (B) for each path are reported in Table 5. The model was adjusted for age, marital status, and education. Both marital status and education were not significant.
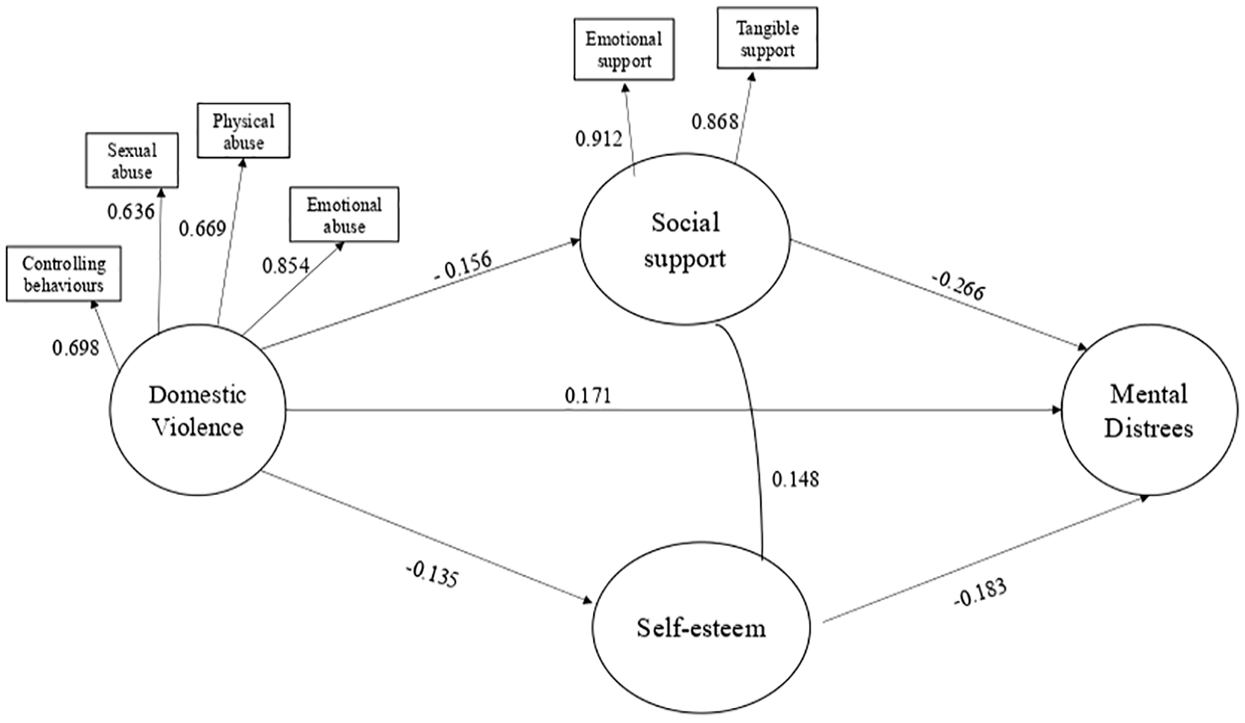
Structural equation model with manifest variables, latent variables, measures, and standardized path coefficients for violence against women, social support, self-esteem, and mental distress in Riyadh, Saudi Arabia.
Standardized Regression Coefficients (β) and Unstandardized Coefficients (B) for Violence and Social Support, Self-Esteem, and Mental Distress in Riyadh, Saudi Arabia (N = 1,932).
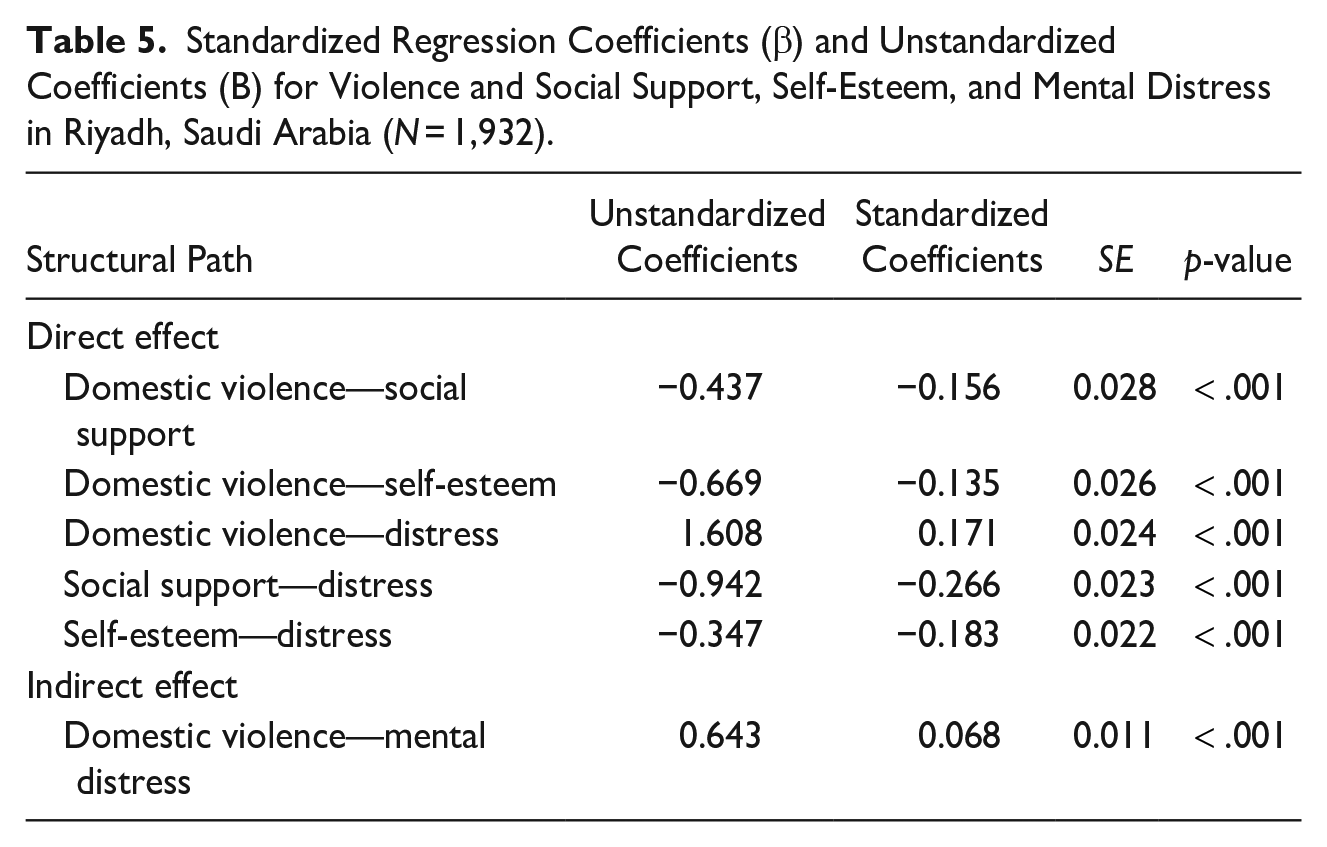
Looking specifically at the model, violence had significant direct negative effects on social support (β = −.156, p < .001) and self-esteem (β = −.135, p < .001). Social support had significant negative direct effects on mental distress (β = −.266, p < .001). Self-esteem had significant negative direct effects on mental distress (β = −.183, p < .001). VAW exerted a direct significant positive effect on mental distress (β = .171, p < .001) as well as an indirect effect (β = .068, p < .001). Both social support (β = .044, p < .001) and self-esteem (β = .025, p < .001) were significant mediators of the effect of violence on mental distress.
Discussion
The study results demonstrate the negative effect of violence on mental distress, along with the mediating role of social support and self-esteem. The effect of violence on distress was measured using violence as a latent variable with four types of abuse (controlling behaviors, sexual abuse, physical abuse, and emotional abuse). In comparison to physical and sexual violence, we found that controlling behavior was the most common type of violence in Saudi Arabia. Controlling behavior, also referred to as “coercive control,” is common among couples with abusive partners. Controlling behavior, in general, refers to targeting and dominating another individual in a negative way (Oram et al., 2017). Controlling behavior is not a single act, infection, it is a spectrum, where on one end there are subtle, unconscious actions and on the other end full blown abuse. In a traditional Arab family, the head of the family is a male member, and he is the decision-maker (Al-Khraif et al., 2020). Although the decisions may be for the woman’s betterment; however, they are taken independently without involving the woman.
Moreover, the culture of having more than one wife (polygamy) is associated with VAW, especially controlling behavior and emotional abuse (Alquaiz et al, 2021). This is the prevailing patriarchal issue of the system where the husband wants to demonstrate controlling behaviour to continue the hold over women and to avoid any conflicts between the wives and justify it for the betterment of women.
In contrast to physical/sexual abuse, both controlling behavior and emotional abuse comprise subtle verbal actions; however, they have a significant effect on mental health in the form of distress, helplessness, and depression (Oram et al., 2017). In terms of evaluating the impact of controlling behavior on mental health, it is also important to assess how the women are being addressed. If the way of communication is humiliating, especially in front of others this may damage the self-respect and self-esteem of the women. Receiving commands rather than advice or suggestions has an impact on recipients’ mental health.
Unfortunately, less attention is given to nonphysical types of violence, whereas physical and sexual abuse cases are dealt with on priority basis (WHO, 2021). A survey conducted in Middle East and South Asia by the WHO reports that half of the women consider verbal and emotional violence as a “normal act” (WHO, 2020) and ignore it. However, Arab women also have a strong anxiety temperament, and any exposure to even nonphysical forms of violence may trigger strong behavioral and physiological responses (Almiş et al., 2018). The impact of controlling behavior on mental health can differ based on the way orders are conveyed to women (e.g., in the presence of others, in a humiliating manner) which is a concern. Receiving commands rather than advice or suggestions has an impact on recipients’ mental health.
Reporting for physical and sexual abuse was low and can be explained on the basis of several steps taken in support of women’s rights and safety (National Family and Safety Program, 2021). Male members, subjecting women to physical violence are considered disrespectful individuals, by all cultures and communities (Mead & Kelty, 2021). The reporting of sexual abuse was low, which may be due to under-reporting or cultural differences as no court law is available to punish the perpetrators. Although, the religion, Islam, has explicitly forbidden to use of any sort of emotional or physical force pertaining to the sexual relationship between the married couple; however, marital rape (forceful intercourse by the spouse) is not defined as abuse (Deosthali et al., 2021).
Previous research studies have found a strong association between social support and life satisfaction and mental health (Kong & You, 2013; Yan et al., 2020). Social support varies among different cultures. In Saudi society, the collective culture prevails, with the majority of support coming from the mother, sisters, aunts, and even the extended family, especially for young women. This culture may reflect the level of trust and comfort which exists between family members (AlQuaiz et al, 2017). The woman has the right to ask for emotional or tangible support, and it is the responsibility and social obligation of the rest of the family to provide it. This is one of the major reasons that till now, no formal social support groups are available in Saudi Arabia. However, with the nuclear family system emerging everywhere, social support groups may prove to be a good preventive strategy against mental distress (Al-Khraif et al., 2020).
Our results are in support of previous studies that have reported the majority of Saudi women report high self-esteem (Kazi, 2021; Al-Qahtani et al., 2021). One of the major reasons for high self-esteem may be the availability of social support from families and friends (Kazi, 2021). Saudi Arabia has a collectivistic culture and families are close to each other. In addition, women are protected by the male members of the family which further boosts their self-esteem (Kazi, 2021). Women with high self-esteem are found to be more cooperative, flexible, and engaged in positive relationships, leading to better quality of life (Tian 2016). Besides social support, other important factors for high self-esteem in Saudi women are getting married and having children, which helps her in achieving a sense of completeness and also fulfilling multiple roles as a daughter, wife, and mother (Bint-e-Tahir 2015).
The availability of social support helps in accomplishing social roles and responsibilities, which further improves self-efficacy and self-esteem (Kazi, 2021). Our results are supporting the sociometer theory, proving that both self-esteem and social support complement each other (Leary, 2003; Trzesniewski et al., 2003). Women who were exposed to violence described themselves as being sad and lonely and scored higher in dimensions of deprivation and aggression and lower incorporation and production. This weakens her social support causing her loneliness and lack of confidence in her decisions and simultaneously a feeling of worthlessness leading to further mental distress (Costa & Gomes, 2018; Duru et al., 2019).
Age was negatively associated with mental distress, which can be explained on the basis of the positive role of social support. In western cultures, sending the elderly to the old age home is one of the reasons for depression. In Saudi culture, usually, older people receive more attention, care, and support. Someone from the family members is available to pay attention and take care of the elderly, which may explain the low level of distress among old-aged women. Mental distress was severe among women exposed to multiple types of violence compared to those subjected to one type, thus emphasizing early detection and provision of social support to prevent re-victimization (Yu et al. 2019; Dostanic et al. 2021). A previous study has concluded that intense negative emotion can put victimized women at risk of re-victimization, mental distress, and as an obstacle to help-seeking behavior (Avdibegovic et al., 2017).
Summary and Conclusion
A significant percentage of women suffer from VAW (especially controlling behavior) and mental distress. The study has established a strong association between VAW and mental distress, with the mediating effect of social support and self-esteem, thus emphasizing the importance of social support and protection.
The protection from violence and abuse law in Saudi Arabia has emphasized in addition to the short-term response to VAW, to consider the long-term rehabilitation and prevention of re-victimization (nfsp.org.sa). However, in reality, more emphasis is put on responding to acute cases of VAW and the management of short-term consequences. Long-term side effects such as mental distress or low self-esteem have received less emphasis due to various factors such as the scarce number of psychiatric centers and professionals, cultures, and attitude of society about mental health issues (Koenig et al., 2014).
It is observed that in collectivistic cultures, like Saudi Arabia, social support for women varies, especially before and after marriage. Women have to fulfill several roles and responsibilities as a mother, daughter, and wife. Before marriage, she is supported by family and friends, whereas afterwards, it is mostly from her spouse, in-laws, and children. However, due to recent changes in the society set up, people prefer a nuclear family structure; hence, there is a decline in family connectivity (Moghadam 2004), which may lead to social problems, mental distress, and poor quality of life. In addition, recently, more women are joining the workforce, hence to balance between work and home life, they need both formal and informal social support. A depressed woman cannot take care of her children, family, and job and can increase the burden on the limited mental healthcare services.
VAW is associated with distress, loneliness, and lack of confidence; hence, social support and self-esteem are important to negate the adverse effect of violence on the mental health of women and re-victimization. Different types of social support interventions prove to be effective in reducing IPV incidence and improving the physical and mental health outcomes of IPV survivors and there is no difference between remote interventions desired effect compared with face-to-face interventions (Ogbe et al. 2020). Awareness and availability of social support groups can help in decreasing stress and improving the connectedness and self-esteem of women (Sullivan 2012; Alquaiz et al. 2021). The volunteers can provide information and guide victims usually by arranging in-person visits or phone calls in addition to increasing awareness about VAW and its consequences at the community level (Ogbe et al. 2020). It is recommended that social support groups should be formally available to provide protection, counseling, and support in carrying out day-to-day tasks.
Our study included a good sample size thus supporting the robust results. In addition, all the questionnaires/scales on violence, self-esteem, distress, and social support were validated and previously utilized by researchers. However, we have some limitations in our study. Saudi Arabia has a unique culture; hence, the results can only be generalized to countries with highly patriarchal structures, similar to that of Saudi Arabia, where women feel compelled to obey their husbands, and men can have more than one wife (Al-Khraif et al., 2020). Economic abuse is an important type of violence; however, we are not able to comment as we did not inquire about it. Recently, more Saudi women have joined the main workforce; hence, it will be important and interesting to explore it in future research studies. We are also limited in generalizing our results to women who are exposed to IPV (other than their husband), as the Saudi culture does not support couples having extramarital relationships. We included unmarried women who may be subjected to violence by their father or brother; however, the percentage was very less (7%) as compared to married women.
To achieve long-lasting and sustainable results, it is important to include family members and friends in providing support. Longitudinal studies conducted under real-life scenarios can enable us to study the effect of various factors including violence, social support, and self-esteem on the mental health of women. Long-term follow-up, provision of mental health, and raising awareness about the long-term effect of violence on victims of abuse are very crucial.
Footnotes
Authors Contribution Statements
JAQ contributed to conception and design of the study, supervision, writing, reviewing, and approval of final draft; AK contributed to acquisition, analysis, and interpretation of the data, manuscript writing, reviewing, and approval of final draft; JAM contributed to data collection, write up, review, and approval of the final draft; EA contributed to the analysis, interpretation of the analysis, manuscript writing, and approval of the final draft manuscript; MA contributed to the conception, design, review for intellectual feedback, and approval of final draft; YH contributed toward data collection, cleaning, write-up, and reviewing the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by the Deanship of Scientific Research, Research chairs program, King Saud University, Riyadh, Kingdom of Saudi Arabia.
Ethics Approval
The study was approved by the Institutional Review Board, King Saud University (E-12-658) and Institutional Review Board of the Ministry of Health, Dammam (IRB ID MOH0151), Saudi Arabia.
Consent
Informed consent was obtained from all individual participants included in the study.
Data,Materials,and code availability
The datasets generated during and analyzed during the current study are not publicly available due to confidential reasons but are available from the corresponding author on reasonable request.