
Abstract
In North Dakota (ND), American Indian women are more likely to be exposed to adverse childhood experiences (ACEs) and interpersonal violence, and receive late prenatal care (PNC) compared to other racial groups. In a sample of 1,849 (weighted n = 26,348) women from the 2017 to 2019 North Dakota Pregnancy Risk Assessment Monitoring System, we performed a series of logistic regression models to estimate odds ratios (OR) and 95% confidence intervals (95% CI) for AI and Other Racial Identity women compared to White women regarding risk of late PNC (initiated after week 13) and dissatisfaction of PNC timing. Models were adjusted for interpersonal violence (from husband/partner, family member, someone outside of family, ex-husband/partner, or any) to determine if violence accounts for racial/ethnic disparities in PNC. AI women experienced two-fold higher risk of late PNC (OR: 2.25, 95% CI: 1.55, 3.26) and dissatisfaction of PNC timing (OR: 2.34, 95% CI: 1.61, 3.40) than White women. In the analyses for the association between joint ACEs (Higher: ≥4; Lower: <4)/Race and PNC outcomes, odds of late PNC were two-fold among AI women with Higher ACEs (OR: 2.35, 95% CI: 1.41, 3.94) and Lower ACEs (OR: 2.73, 95% CI: 1.69, 4.41), compared to White women with Lower ACEs. Results were similar for dissatisfaction of PNC timing. Accounting for violence did not significantly change odds ratios in any analyses. Thus, interpersonal violence surrounding pregnancy does not explain racial disparities in PNC in ND. To understand disparities in PNC among AI women, risk factors like historic trauma and systemic oppression should be examined.
Keywords
Background
Access to early prenatal care (PNC) is associated with decreased risk of adverse fetal and infant outcomes (e.g., preterm birth, low birth weight, and neonatal mortality) and adverse maternal outcomes (e.g., mental health, hypertensive disorders) (Heaman et al., 2019; Holcomb et al., 2021; Mackay et al., 2001; Vintzileos et al., 2002). In 2018, 77% of pregnant women in the United States initiated PNC in the first trimester; however, American Indian women had lower prevalence (65%) of first trimester PNC than other racial/ethnic groups: (Non-Hispanic Black 67.1%; Hispanic 72.7%; Non-Hispanic Asian 81.8%; Non-Hispanic White 82.5%) (U.S. Department of Health and Human Services, n.d.). In an analysis of 2017 to 2018 North Dakota Pregnancy Risk Assessment Monitoring System (ND PRAMS) data, American Indian women had two-fold higher odds of late PNC compared to White women, despite controlling for sociodemographic and medical factors (Sebens & Williams, 2022). Given the American Indian population is the second largest racial/ethnic group in North Dakota (ND) (U.S. Census Bureau, 2022), and rurality presents a challenge for accessing PNC (Gjesfjeld & Jung, 2011), further investigation into determinants of racial/ethnic disparities in PNC specific to ND is warranted to reduce inequities, particularly among American Indian women (Holcomb et al., 2021). Our current study investigates interpersonal violence in the context of Adverse Childhood Experiences (ACEs) as a potential contributor to racial disparities in PNC access and satisfaction. This study will also provide interpersonal violence prevalence rates among pregnant American Indian women in ND—data that is currently not available.
Interpersonal Violence
Interpersonal violence is the intentional use of physical force or power against other persons, including physical, sexual, or psychological violence as well as deprivation and neglect. Types of interpersonal violence include family and partner violence as well as community violence (Mercy et al., 2017). This study uses the broad definition of interpersonal violence to remain inclusive of the harms inflicted by all perpetrators of pregnancy-related violence (e.g., partners, ex-partners, family, and others), while recognizing that intimate partner violence (IPV) is the most prevalent type of interpersonal violence against women.
In the U.S., 59 million women (48%) have experienced sexual violence, physical violence, and/or stalking by an intimate partner in their lifetime (Leemis et al., 2022). Additionally, 58% of American Indian women have experienced violence from an intimate partner, the second-highest rate only to multiracial women (64%) (Leemis et al., 2022). ND has one of the lowest rates of reported IPV in the country with approximately 30% of women experiencing IPV in their lifetimes (National Coalition Against Domestic Violence, 2023); however, estimates for American Indian women were unavailable (Smith et al., 2017). Furthermore, CAWS ND, the statewide sexual and domestic violence coalition, reported an increasing number of new victims of domestic violence during the COVID-19 pandemic, serving 4,674 new cases in 2020, 5,417 in 2021, and 6,128 in 2022 (National Coalition Against Domestic Violence, 2023). Violence surrounding pregnancy is particularly important, as IPV is the largest contributor of homicide in the prenatal and postpartum periods (Campbell et al., 2021; Wallace et al., 2021). Over 8% of women experience IPV in the 12 months before pregnancy and 5% of women experience IPV during pregnancy (Scribano et al., 2012). In ND, 3% of new victims of domestic violence were pregnant (North Dakota Council on Abused Women’s Services, 2020).
Exposure to IPV may increase difficulty in accessing healthcare, including PNC, often due to the perpetrators’ power and control in the relationship, thus, exposure to IPV prior to pregnancy may increase risk for late PNC (Cha & Masho, 2013; Taillieu & Brownridge, 2010). A 2018 meta-analysis of 31 U.S. and international studies reported that women who experienced IPV prior to and during pregnancy were more likely to receive no (OR: 2.62, 95% CI: 1.55, 4.42) or late PNC (OR: 1.81, 95% CI: 1.48, 2.23) (Jamieson, 2018). A study of 104 rural Appalachian women reported that 48% of women who experienced IPV surrounding pregnancy did not receive PNC in the first trimester, compared to 35% of women who did not experience any IPV (Bailey & Daugherty, 2007). A cross-sectional study conducted in Mumbai, India found pregnant women who experienced violence were half as likely to receive PNC in the first trimester (OR: 0.49, 95% CI: 0.24–0.95) (Silverman et al., 2016).
Two additional studies explore the association between pregnancy-related IPV and late or inadequate PNC. A 2002 qualitative study among 30 midwestern, urban Native American women found that all eight women who received inadequate PNC experienced physical or sexual abuse from a current intimate partner (Bohn, 2002). A 2013 cross-sectional study utilizing 2004 to 2008 national PRAMS data found that women who experienced preconception and/or prenatal IPV were 20% less likely to receive adequate PNC than women who did not experience any IPV; however, preconception IPV alone was only found to have borderline statistical significance with PNC inadequacy (OR: 1.2, 95% CI: 1.0, 1.4) (Cha & Masho, 2013).
Adverse Childhood Experiences
Adverse Childhood Experiences (ACEs) include experiences of abuse, household challenges, and neglect that occur during childhood. Like interpersonal violence, ACEs are associated with adverse health and behavior outcomes in children and adults, including chronic disease, substance use, mental illness, and early death (Felitti et al., 1998; Gilgoff et al., 2020; Warne et al., 2017). Additionally, there is a dose-response effect with each additional ACE, and those with four or more ACEs are more likely to have worse health outcomes than those with fewer ACEs (Giovanelli et al., 2016; Hughes et al., 2017). Prevalence of ACEs vary by race/ethnicity, with nearly 64% of Black children and 52% of Hispanic children experiencing at least one ACE, compared to 42% of White Non-Hispanic children (Bethell et al., 2017). American Indian populations are often excluded from these analyses or grouped in with other races/ethnicities (Richards et al., 2021); however, data suggest American Indian populations experience more ACEs on average compared to other racial/ethnic groups. For example, American Indian children in the Northern Plains (including ND) were more likely to experience 2 or more ACEs compared to American Indian children in other parts of the country (Kenney & Singh, 2016; Richards et al., 2021; Warne et al., 2017).
Individuals with multiple ACEs have an increased risk of experiencing IPV as adults (Navarro et al., 2022; Whitfield et al., 2003). This association may be due to the negative impact of ACEs on social, emotional, and cognitive development, as well as poor mental health and coping skills. Additionally, exposure to violence as a child may normalize violent behaviors, making it more likely that children exposed to ACEs are more likely to engage in and be victimized by violence in adulthood (Navarro et al., 2022). Furthermore, research on ACEs and the association with healthcare access is currently mixed. Studies by Chartier et al. and Finestone et al. indicated that because individuals with ACEs are more likely to experience health issues, they may be more likely to utilize healthcare services in adulthood (Chartier et al., 2007, 2010; Finestone et al., 2000). Alternatively, Alcalá et al. reported that ACEs were associated with lower odds of healthcare utilization in the previous year (Alcalá et al., 2018). Among pregnant women, exposure to ACEs may have severe health implications for the mother and the infant including maternal mental illness, low infant birth weight, and preterm birth (Christiaens et al., 2015); however, the association between ACEs and PNC access remains unexplored. Given the strong evidence linking ACEs and poor pregnancy outcomes, and PNC being a key determinant of pregnancy outcomes, pregnant women with high ACEs may be less likely to receive timely PNC. Considering IPV in the context of ACEs may provide greater insight into disparities in PNC utilization, particularly among American Indian women.
Current Study
American Indians are more likely to experience ACEs and interpersonal violence, but less likely to receive PNC in the first trimester, compared to White women. Additionally, ACEs are associated with experiencing interpersonal violence in adulthood. Given these disparities, we used ND PRAMS data to examine whether interpersonal violence in the 12 months prior to pregnancy contributes to racial disparities in PNC, overall and in the context of ACEs. Due to the complexity of contributing factors to racial/ethnic disparities in perinatal outcomes (Gadson et al., 2017), we hypothesized that interpersonal violence before pregnancy partially accounts for racial disparities in PNC utilization among pregnant American Indian women in ND. Additionally, we hypothesized that adjusting for interpersonal violence will lead to a greater reduction in PNC access disparities among pregnant women with higher ACEs.
Materials and Methods
Data for 4,297 women were obtained from the 2017 to 2019 ND PRAMS. PRAMS collects state-specific data on the demographics, experiences, and outcomes of pregnant women before, during, and after pregnancy. Participants were excluded from analysis if they had missing data on covariates or on trimester of PNC initiation, satisfaction with timing of PNC initiation, and preconception violence (excluded n = 2,448), resulting in an analytic sample of 1,849 women. Sample weights account for stratified survey design, noncoverage and nonresponse, and give unbiased estimates of population parameters. Sample weights are applied in analysis to obtain estimates reflective of the number of people that recently gave birth in ND that each ND PRAMS participant represents. Therefore, the weighted analytic sample included 26,348 women, with each of the 1,849 women included in the analytic sample representing approximately 14 women who recently gave birth in ND. More detailed information on PRAMS methodology is available online (Centers for Disease Control and Prevention, 2023).
Race & Ethnicity
Race/ethnicity was self-reported by participants in the ND PRAMS survey. Categories include American Indian (American Indian/Alaska Native alone or biracial American Indian-White), White (White alone), and Other Racial Identities (other race/ethnicity; includes Black, Asian, Hispanic [all races], and other/unknown). Low birth rates in ND among other races and ethnicities during 2017 to 2019 did not allow for separate race/ethnicity estimates.
Prenatal Care Access
Women who had their first PNC visit in the first trimester (by week 12 or month 3) were identified as having “early PNC,” while those who initiated PNC after the first trimester or not at all were identified as having “late PNC.” For PNC timing satisfaction, women reported yes or no to the question “did you get prenatal care as early in your pregnancy as you wanted?” Women who reported “yes” were categorized as “satisfied with PNC timing” and women who reported “no” were categorized as “dissatisfied with PNC timing.”
Interpersonal Violence
Participants self-reported yes or no to the question, “In the 12 months before you got pregnant with your new baby, did [a husband/partner, family member, someone outside of their family, or an ex-husband/partner] push, hit, slap, kick, choke, or physically hurt you in any other way?” Separate variables were created for each abuser: husband/partner, family member, someone outside of their family, or an ex-husband/partner. An “Any exposure to violence” variable was created to capture any “yes” responses to interpersonal violence experienced in the 12 months before pregnancy.
Adverse Childhood Experiences
Participants reported yes or no to the ten questions sourced from the Adverse Childhood Experiences (ACEs) Questionnaire (Felitti et al., 1998) regarding potentially traumatic experiences of abuse, household challenges, and neglect before the age of 18. Aligning with previous ACE studies, if participants reported yes to four or more ACEs, they were categorized in the “Higher ACEs” group, while women with less than four were categorized in the “Lower ACEs” group (Anda et al., 2005; Giovanelli et al., 2016).
Joint ACEs/Race Variable
A joint exposure variable was created by combining racial identity (American Indian, White, or Other Racial Identities) with ACEs level (Higher or Lower): American Indian with Higher ACEs, Other Racial Identities with Higher ACEs, White with Higher ACEs, American Indian with Lower ACEs, Other Racial Identities with Lower ACEs, and the reference group, White with Lower ACEs.
Confounding
Confounders were identified based on prior literature. Sociodemographic factors represent resource access, in which those who are young, unmarried, have low income, no health insurance, or who live far from healthcare facilities have more difficulty obtaining care (Aved et al., 1993; Cha & Masho, 2013; Holcomb et al., 2021; Sebens & Williams, 2022). Confounders included annual income (≤$40,000, > $40,000; based on the sample median), Medicaid status prior to pregnancy (has Medicaid, has other health insurance, or has no health insurance), rurality (rural or urban residence), maternal age in years (<20, 20–35, >35), maternal education (≤high school, > high school), and marital status (married, other). Medical conditions and health behaviors may motivate persons to access PNC to ensure the health of their pregnancy (Cha & Masho, 2013; Sebens & Williams, 2022). Medical and health behavioral confounders included substance use before pregnancy (yes or no to any smoking, alcohol, e-cigarettes, marijuana), pre-existing chronic disease (yes or no to any diabetes, hypertension, depression), pregnancy intention (wanted now, wanted later or never), and pre-pregnancy BMI (<25, ≥25).
Statistical Analysis
Descriptive statistics including weighted percentages and frequencies were generated to assess the distribution of covariate characteristics among the sample. Weighted percentages and frequencies of interpersonal violence before pregnancy experienced by race/ethnicity are summarized overall and by ACE level. A series of logistic regression models were performed to estimate unadjusted and adjusted odds ratios (OR) and 95% confidence intervals (95% CI) for both late PNC and dissatisfaction of PNC timing among American Indian and Other Racial Identity women compared to White women. Model 1 provides the unadjusted estimate for the association between race/ethnicity and PNC outcomes. Model 2 includes confounders and ACEs. Models 3 to 7 were adjusted for confounders, ACEs, and one of the interpersonal violence variables (model 3: any violence, model 4: violence from husband/partner, model 5: violence from other family member, model 6: violence from other, and model 7: violence from an ex-husband/partner). To determine if accounting for interpersonal violence in the models results in a meaningful change in the OR for American Indian or Other Racial Identities, we compared ORs from adjusted models to preceding models (e.g., Model 2 compared to Model 1; Violence models compared to Model 2; Percent Change Equation: ([Model 2 OR-Model Including Violence Variable OR]/Model 2 OR)*100%). If the change in OR is 10% or greater, this will be considered a meaningful change in the observed disparity.
A second series of models were fit to estimate OR and 95% CIs for the association between the joint ACEs/Race variable and PNC outcomes. This series of models was similar to Models 1 to 7 as described above, without including race/ethnicity or ACEs as separate variables. This joint-exposure approach allows us to consider the additive effects of racial identity and ACEs, such that the co-occurrence of both variables may result in a different risk profile than other combinations of both variables (Knol et al., 2011). All statistical analyses were conducted using SAS On Demand for Academics (SAS Institute Inc., Cary, NC, USA) using proc survey commands and survey weights to account for complex survey design and nonresponse. This work was approved by the University of North Dakota Institutional Review Board.
Results
Prevalence of outcomes and covariates for the overall sample and by race/ethnicity are included in Table 1. Ninety-two percent of White women received PNC in the first trimester, compared to 79% of women of Other Racial Identities and 71% of American Indian women (p < 0.01). Only 73% of American Indian women were satisfied with the timing of PNC received, compared to 85% of women of Other Racial Identities, and 91% of White women (p < 0.01). Thirty-three percent of American Indian women also reported four or more ACEs compared to 19% of White women, and 11% of women of Other Racial Identities (p < 0.01). American Indian women in the sample were more likely to be younger, unmarried, live in rural areas, have lower incomes, have a chronic disease, be overweight, and have achieved a lower education level than White and Other Racial Identity women. White women had the highest prevalence of substance use before pregnancy, and typically, had higher incomes and education levels (Table 1).
Weighted Percent (and Frequency) of Outcomes and Demographic Factors by Race/Rthnicity in ND PRAMS (2017–2019) (Weighted n = 26,348).
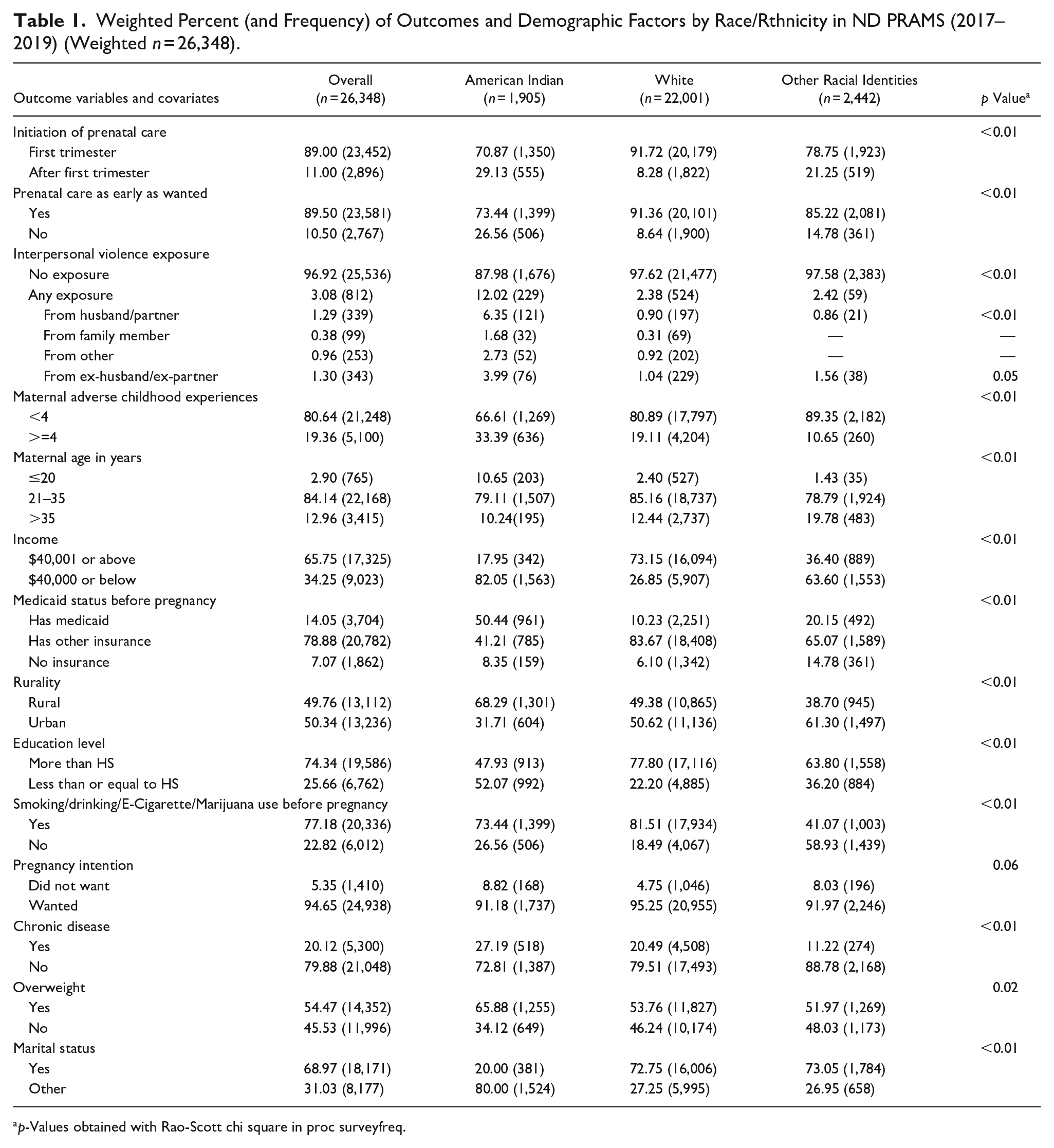
p-Values obtained with Rao-Scott chi square in proc surveyfreq.
Table 2 provides interpersonal violence prevalence among racial/ethnic groups, stratified by ACEs level. Overall, 3% of pregnant women in the sample experienced any interpersonal violence in the year before pregnancy. Violence from ex-husband/ex-partner and husband/partner were most prevalent in the overall sample, followed by violence from someone outside of the family, and from a family member. American Indian women experienced the highest overall prevalence of interpersonal violence at 12.02%, approximately 5 times the prevalence among White women (2.38%) and among Other Racial Identity women (2.42%). Women in the Higher ACEs group (8.80%) had a 5-fold higher prevalence of interpersonal violence experienced than those in the Lower ACEs group (1.71%). 23% of American Indian women in the Higher ACEs group experienced interpersonal violence from any source, compared to 6.3% of American Indian women in the Lower ACEs group.
Weighted Percent (and Frequency) of Violence Before Pregnancy Experienced by Race/Ethnicity with ACEs Level Stratification (Weighted n = 26,348).
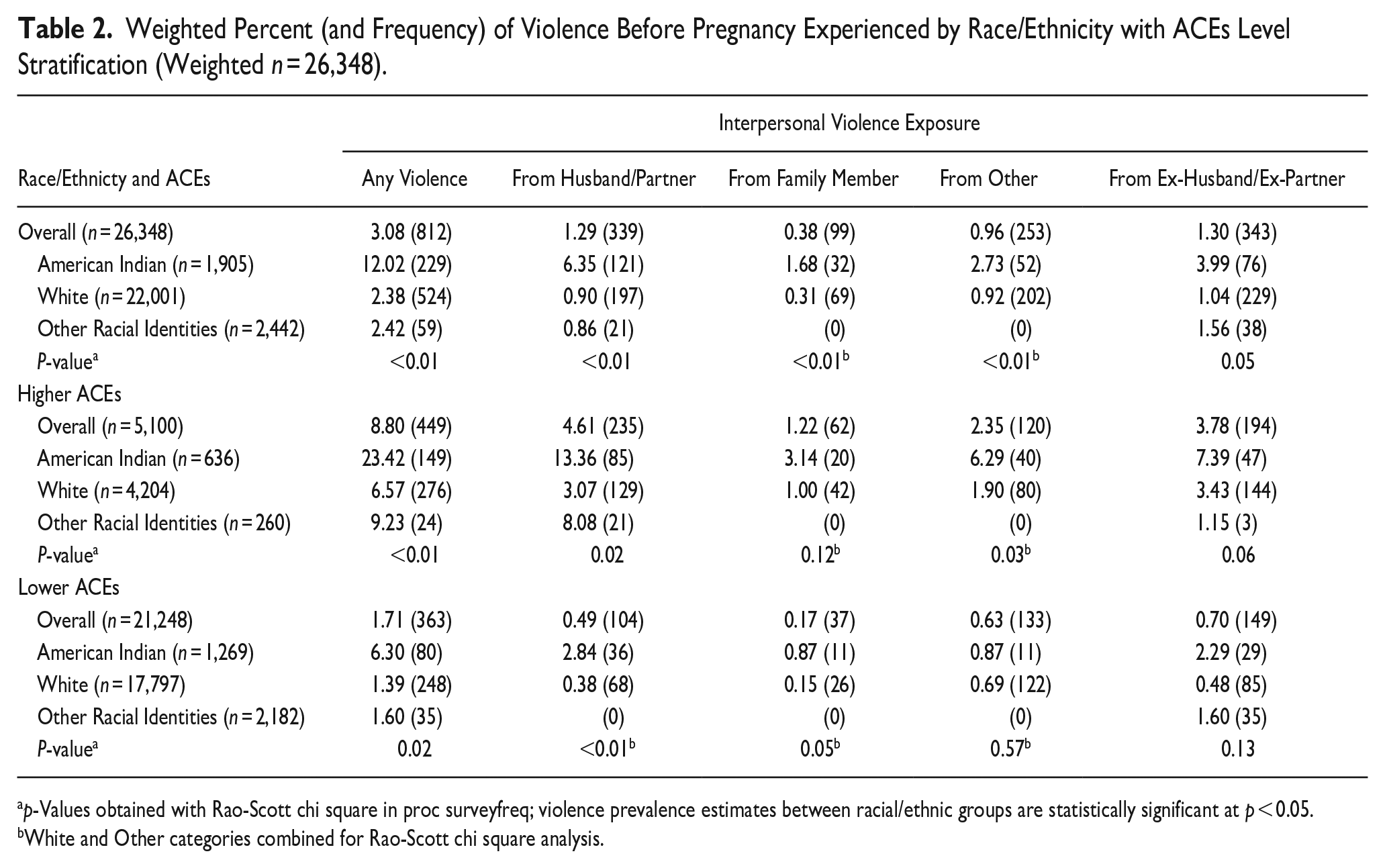
p-Values obtained with Rao-Scott chi square in proc surveyfreq; violence prevalence estimates between racial/ethnic groups are statistically significant at p < 0.05.
White and Other categories combined for Rao-Scott chi square analysis.
Hypothesis 1
Table 3a includes the logistic regression results for late PNC. In the unadjusted model with race/ethnicity as the main predictor, compared to White women, American Indian women were 356% (OR: 4.56, 95% CI: 3.43, 6.05) more likely to receive late PNC. Women of Other Racial Identities were 199% (OR: 2.99, 95% CI: 1.75, 5.12) more likely to receive late PNC. After accounting for maternal sociodemographic factors, health factors, and ACEs (Model 2), the odds decreased by 51% for American Indian women and 17% for women of Other Racial Identities, but the odds of receiving late PNC remained two times higher among American Indian women (OR: 2.25, 95% CI: 1.55, 3.26) and women of Other Racial Identities (OR: 2.47, 95% CI: 1.36, 4.48) compared to White women. After adjusting for any interpersonal violence experienced before pregnancy, the odds of receiving late PNC among American Indian women decreased by 3.1% (OR: 2.18, 95% CI: 1.50, 3.18), and odds among women of Other Racial Identities decreased by 1.2% (OR: 2.44, 95% CI: 1.34, 4.45). Inclusion of the abuser-specific variables did not meaningfully change estimates for either racial/ethnic group.
Odds Ratio and 95% Confidence Intervals for the Association Between Interpersonal Violence Before Pregnancy and Late Prenatal Care Initiation—ND PRAMS 2017 to 2019 (Weighted n = 26,348).
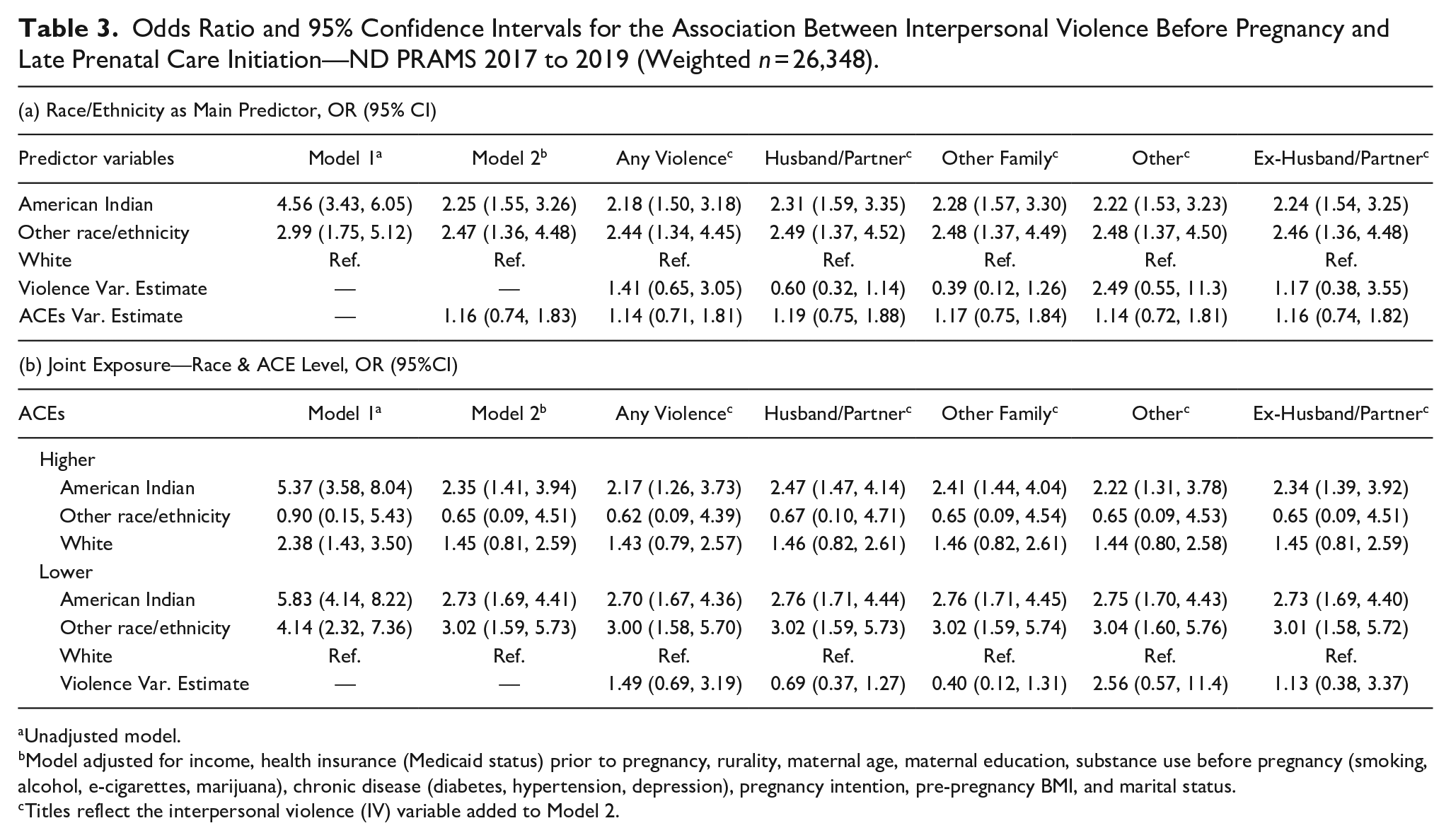
Unadjusted model.
Model adjusted for income, health insurance (Medicaid status) prior to pregnancy, rurality, maternal age, maternal education, substance use before pregnancy (smoking, alcohol, e-cigarettes, marijuana), chronic disease (diabetes, hypertension, depression), pregnancy intention, pre-pregnancy BMI, and marital status.
Titles reflect the interpersonal violence (IV) variable added to Model 2.
Table 4a includes logistic regression results for dissatisfaction of timing of PNC initiation. In the unadjusted model with race/ethnicity as the main predictor, compared to White women, American Indian women were 282% (OR: 3.82, 95% CI: 3.89, 5.05) and women of Other Racial Identities were 84% (OR: 1.84, 95% CI: 1.00, 3.38) more likely to be dissatisfied with the timing of PNC initiation. After adjusting for maternal sociodemographic factors, health factors, and ACEs (Model 2), the disparity was eliminated for women of Other Racial Identities (OR: 1.69, 95% CI: 0.91, 3.13) and the odds for American Indian women decreased by 39%, but remained more than two times significantly higher (OR: 2.34, 95% CI: 1.61, 3.40) than the odds among White women. Inclusion of any interpersonal violence variables did not meaningfully change estimates for either American Indian or Other Racial Identity women. Our first hypothesis was unsupported, as adjusting for interpersonal violence did not significantly decrease disparities in PNC utilization among pregnant American Indian women in ND.
Odds Ratio and 95% Confidence Intervals for the Association Between Interpersonal Violence Before Pregnancy and Dissatisfaction with Timing of Prenatal Care Initiation—ND PRAMS 2017 to 2019 (Weighted n = 26,348).
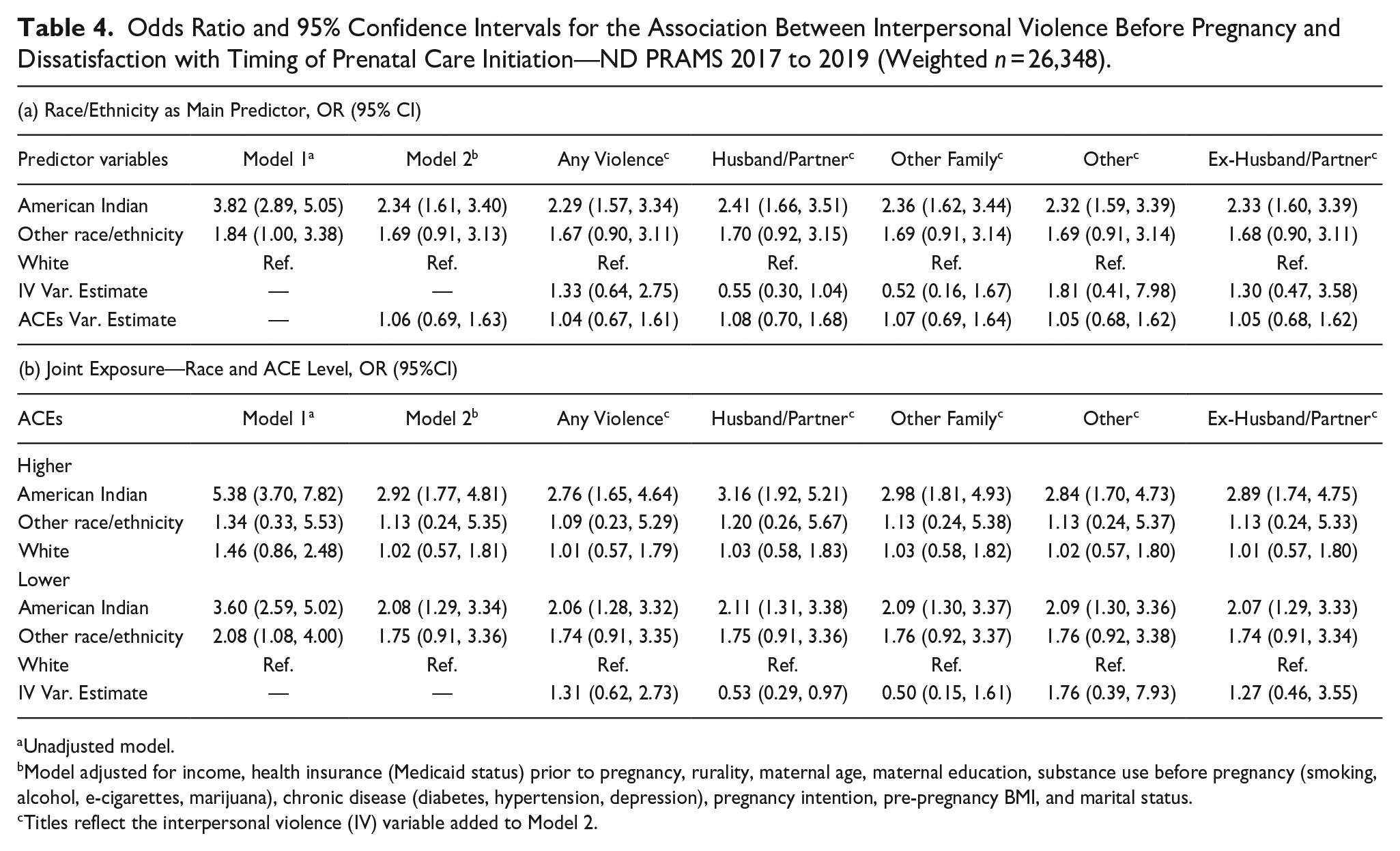
Unadjusted model.
Model adjusted for income, health insurance (Medicaid status) prior to pregnancy, rurality, maternal age, maternal education, substance use before pregnancy (smoking, alcohol, e-cigarettes, marijuana), chronic disease (diabetes, hypertension, depression), pregnancy intention, pre-pregnancy BMI, and marital status.
Titles reflect the interpersonal violence (IV) variable added to Model 2.
Hypothesis 2
In the joint exposure unadjusted model in Table 3b, American Indian women with both lower ACEs (OR: 5.83, 95% CI: 4.14, 8.22) and higher ACEs (OR: 5.37, 95% CI: 3.58, 8.04) and Other Racial Identity women with lower ACEs (OR: 4.14, 95% CI: 2.32, 7.36) were significantly more likely to receive late PNC, while Other Racial Identity women with Higher ACEs did not significantly differ from White women with Lower ACEs. Adjusting for maternal sociodemographic and health factors (model 2) reduced the odds of receiving late PNC among American Indian women with Higher ACEs by 56% (OR: 2.35, 95% CI: 1.41, 3.94), and among American Indian women with Lower ACEs by 53% (OR: 2.73, 95% CI: 1.69, 4.41). Additionally, the odds of late PNC among women of Other Racial Identities with Lower ACEs decreased by 27% (OR: 3.02, 95% CI: 1.59, 5.73). After adjusting for any interpersonal violence before pregnancy, the odds of late PNC decreased for American Indian women with Higher ACEs by 7.6% (OR: 2.17, 95% CI: 1.26, 3.73) and slightly decreased for both American Indian women with Lower ACEs (OR: 2.70, 95% CI: 1.67, 4.36) and women of Other Racial Identities with Lower ACEs (OR: 3.00, 95% CI: 1.58, 5.70).
In the unadjusted joint exposure model on Table 4b, compared to the odds of PNC dissatisfaction among White women with Lower ACEs, American Indian women with Higher ACEs were 438% (OR: 5.38, 95% CI: 3.70, 7.82), American Indian women with Lower ACEs were 260% (OR: 3.60, 95% CI: 2.59, 5.02), and women of Other Racial Identities with Lower ACEs were 108% (OR: 2.08, 95% CI: 1.08, 4.00) more likely to be dissatisfied with the timing of PNC initiation. Upon adjusting for maternal sociodemographic and health factors (model 2), the disparity in satisfaction with timing of PNC initiation was eliminated for Other Racial Identity women with Lower ACES and reduced for American Indian women with Higher ACEs by 46% (OR: 2.92, 95% CI: 1.77, 4.81), and reduced for American Indian women with Lower ACEs by 42% (OR: 2.08, 95% CI: 1.29, 3.36). After adjusting for any violence before pregnancy, the odds of not receiving PNC when wanted among American Indian women with Higher ACEs decreased by 5.5% (OR: 2.76, 95% CI: 1.65, 4.64) and decreased by less than 1% among American Indian women with Lower ACEs (OR: 2.06, 95% CI: 1.28, 3.32). Our second hypothesis was partially supported, as the two-fold PNC utilization disparity remains, but a greater reduction in disparities among American Indian women with Higher ACEs was exhibited.
Discussion
In this analysis of PNC among a diverse population of women in ND, we hypothesized that exposure to interpersonal violence would partially account for racial disparities in PNC access. The first hypothesis was not supported as interpersonal violence did not meaningfully change observed racial disparities. We also hypothesized that accounting for interpersonal violence will lead to a greater reduction in PNC access disparities among pregnant women with a higher level of ACEs. Our second hypothesis was partially supported as disparities in PNC were partly mitigated among American Indian women with higher ACEs, yet a two-fold higher risk for late PNC and dissatisfaction with timing of PNC initiation remain.
The lack of effect when adjusting for interpersonal violence is unexpected, given the disparate experience of interpersonal violence by race in the sample and prior literature that suggests that interpersonal violence may inhibit early access to PNC (Bailey & Daugherty, 2007; Bohn, 2002; Jamieson, 2018; Silverman et al., 2016). Using National PRAMS data, Cha & Masho (2013) found a significant association between preconception and/or prenatal IPV and inadequacy of PNC, based on the Adequacy of Prenatal Care Utilization (APNCU) index (Kotelchuck, 1994), which considers PNC initiation and the frequency of visits. This study also found a borderline association between preconception violence and PNC inadequacy. However, even though our study used similar data collection methods and analyses, our findings do not suggest a relationship between interpersonal violence, including IPV, before pregnancy and the timing of PNC initiation among our sample of pregnant ND women. There are several distinctions between our study and the Cha and Masho study potentially contributing to this difference. First, our study included ACEs within analysis, while the Cha and Masho study did not account for ACEs. As those with higher ACEs are more likely to experience violence in adulthood (Gilgoff et al., 2020), this may partially explain differences in findings. Second, despite both studies using PRAMS data, samples are different in terms of geography and racial/ethnic makeup, as we used only ND PRAMS data (n = 1,849) while Cha and Masho used national PRAMS data (n = 202,367). The purpose of our study to examine disparities in PNC between American Indian and White women necessitated the use of a dataset that oversamples American Indian women, which ND PRAMS allows for. Furthermore, the national PRAMS dataset likely has greater variability in violence exposures compared to ND PRAMS, as ND has one of the lowest rates of reported IPV in the country (National Coalition Against Domestic Violence, 2023). Third, we defined early PNC as care received in the third month or earlier while Cha & Masho defined adequate care as PNC that begins by the fourth month and receipt of 80% to 109% of expected visits, thus the differing outcome variables may not have the same relationship with a similar exposure. Lastly, our models specified maternal race/ethnicity as the main predictor, while the Cha and Masho models were specified for IPV as the main predictor, potentially accounting for differences in the observed effect of interpersonal violence.
Results of the current study may be explained by a non-monotonic, or individualized, response to being in a violent situation when pregnant. Abuse often alternates between four stages: a period where issues and tension build, a period in which violence is enacted, a period where the abuser apologizes for or minimizes the violence, and a calm period in which violence stops and the victim may believe it will not happen again. This cycle, alongside fear of repercussions, is one of the reasons why women do not report intimate partner violence or leave the relationship (Rakovec-Felser, 2014). For example, qualitative data from 142 women with a history of IPV found that only half of the women reported their abuse to a healthcare provider, and two-thirds of those women only disclosed because their healthcare provider asked (Morse et al., 2012). Due to the complex and cyclical nature of violent intimate relationships, some pregnant women may avoid PNC settings out of fear of disclosing their experiences with interpersonal violence (Mccloskey et al., 2007). Additionally, abusive partners may be monitoring or controlling PNC appointment attendance (O’Doherty et al., 2015). For these women, PNC may be delayed or avoided altogether. Alternatively, given that interpersonal violence is associated with a myriad of health consequences for both the mother and infant (Heaman et al., 2019; Holcomb et al., 2021; Mackay et al., 2001; Vintzileos et al., 2002), some pregnant women may seek PNC as a preventive measure. Regarding PNC access, the behaviors of pregnant women experiencing interpersonal violence, particularly from an intimate partner, may be more difficult to predict than originally expected with these quantitative data.
From our knowledge, our study is the first to look at racial disparities in PNC access in the context of ACEs. The ACEs variable is not associated with late PNC in any model; however, given the disparate distribution of ACEs by race and the elevated prevalence of interpersonal violence among those with higher ACEs, analyses for the joint race/ACE level were performed. While overall differences in racial disparity estimates among ACE groups were not statistically significant, there are noteworthy observations. American Indian women with a higher level of ACEs had slightly lower odds of receiving late PNC, but higher odds of being dissatisfied with PNC timing than American Indian women with a lower level of ACEs. Other Racial Identity women with a lower level of ACEs had higher odds of both receiving late PNC and being dissatisfied with PNC timing than Other Racial Identity women with a higher level of ACEs.
Sebens and Williams (2022) reported that lack of health insurance, money, transportation, and childcare; being too busy; and wanting to keep pregnancy a secret were all significant (p < 0.05) barriers to PNC in ND, for all of which American Indian women report a higher prevalence than White women. However, small sample sizes for the self-reported barriers to PNC in ND PRAMS limit analysis to bivariate associations (Sebens & Williams, 2022). Additionally, a qualitative study interviewed 58 American Indian women in the Northern Plains regarding their perceptions of PNC, identifying communication difficulties with physicians, long wait times for appointments, and feeling uncomfortable seeing a male physician as barriers that inhibit American Indian women from seeking timely and continuous PNC (Hanson, 2012). Furthermore, many American Indians in ND live in very rural areas where there are higher rates of inadequate PNC and limited healthcare services and providers, forcing residents to travel long distances for care (Baldwin et al., 2013). While our regression models were adjusted for health insurance status, rurality, and income, other significant barriers to care likely contribute to racial disparities in PNC access and should be further explored to understand the magnitude of their impact. Data considerations like mixed methods data and increased sample size may allow for more rigorous investigation of barriers to PNC. Additionally, interpersonal violence and ACEs are just some forms of adversity that American Indian and Other Racial Identity women face. These factors do not account for historical trauma and systemic oppression that have led minority women to experience reduced economic opportunity and disparities in health and healthcare access in the U.S (Moon et al., 2015). While our study findings show that interpersonal violence and ACEs are not primary contributors to racial disparities in PNC access in ND, this is not to say that interpersonal violence and ACEs do not contribute to other poor health and behavior outcomes surrounding pregnancy (Alhusen et al., 2015; Wajid et al., 2020). It is likely that unmeasured confounders related to systemic oppression greatly contribute to the racial disparities in PNC access, and more research is necessary to identify key factors.
Strengths
This study has several strengths. First, it contributes to a limited collection of research on pregnant American Indian women in ND, particularly regarding ACEs, interpersonal violence, and PNC access. This is especially notable given the very high rates of maternal and infant mortality for American Indian women. Next, while other studies have found an association between IPV and inadequate PNC, our study examined interpersonal violence through an expanded lens, included analyses by race, and explored these associations in the context of ACEs. This study provides ACE and interpersonal violence prevalence estimates for pregnant women in ND and focused on American Indian women. Next, the design of this study oversampled American Indian women, allowing for the analysis to better represent this population of pregnant women in ND. The greater inclusion of American Indian women is important for ameliorating maternal/infant health disparities and for centering American Indian culture. Additionally, PNC access is a timely topic, as the COVID-19 pandemic led to the expansion of telemedicine, which has the potential to impact PNC outcomes (Pflugeisen & Mou, 2017), especially among American Indian and rural populations.
Limitations
These results should be considered in the context of its limitations. First, over 90% of those who were excluded from analysis had missing demographic data, while other excluded participants were primarily American Indian (68%) and had an annual household income less than $40,000 (85%). Additionally, ND has limited racial and ethnic diversity, so the sample of women of Other Racial Identities is small, leading to wide confidence intervals. Furthermore, as data are self-reported, social desirability bias and recall bias both likely contribute to underestimates of true exposure to interpersonal violence. Only severe instances of interpersonal violence may be reported; thus, interpersonal violence prevalence in this sample is likely conservative. Next, while other states in the Midwest may be similar, the results of this study can only be generalized to pregnant women in ND. Lastly, while historic trauma and systemic oppression may contribute to observed racial disparities in this analysis, ND PRAMS does not collect data relevant to those constructs. Future data collection efforts should incorporate historic trauma and systemic oppression to understand how these constructs may contribute to disparities facing American Indian populations.
While more research is necessary to explore the relationship between interpersonal violence and racial disparities in PNC access in the context of ACEs, as well as the experience of violence around pregnancy and its potential health impacts for both mothers and infants, interpersonal violence and ACEs should be screened for during annual health check-ups and at PNC appointments. In addition to screening, healthcare providers should receive training on how to identify, respond to, and provide safety planning and resources to pregnant women experiencing interpersonal violence (Macedo et al., 2018). Furthermore, additional support is needed for programs and services that address barriers to PNC among American Indian women in ND (i.e. financial assistance, childcare, transportation, health insurance screening).
Conclusion
This study did not find evidence that adverse childhood experiences or interpersonal violence experienced before pregnancy contributes to racial disparities in PNC access in ND, particularly among American Indian women. To fully understand why these disparities exist, we may need longitudinal data and to consider additional risk factors associated with historical trauma and systemic oppression. It may be that interpersonal violence and ACE exposure were confounded with historical trauma in our sample. Additionally, other health and behavior outcomes should be explored among American Indian women who have adverse childhood experiences and/or are exposed to interpersonal violence surrounding pregnancy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Research reported in this publication was supported by the National Institute Of General Medical Sciences of the National Institutes of Health under Award Number P20GM139759. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This project was supported by funding from the North Dakota Department of Health and the Centers for Disease Control and Prevention (G21.255—COVID-19 Health Disparities).