
Abstract
Limited qualitative research has been conducted to understand the experiences of victims of sexual harassment or assault (SHA) when a bystander intervenes. Even less research has focused on the consequences of bystander actions from the victim’s perspective, particularly regarding the aggressor’s subsequent behavior toward the victim and occurrence of verbal or physical harm to those involved. This qualitative study aimed to address these limitations with the following research questions: (a) what strategies did victims of SHA identify bystanders use when intervening? (b) what strategies were present when the aggressor’s behavior was stopped, paused, or continued toward the victim? and (c) what strategies were present when verbal or physical harm occurred to someone involved? Adult women between the ages of 18 to 30 (N = 25, college student = 80%) were interviewed about one situation of bystander intervention during SHA since the age of 16 years. Findings suggest that victims identified direct, distance, distract, delegate, and proximity strategies by bystanders. Most participants reported that the aggressor’s behavior stopped or paused following bystander action, and in these cases, at least one distance or direct strategy was reportedly used most frequently. Approximately, 24% and 8% of participants reported verbal or physical harm, respectively, to at least one party. Direct and distance strategies were most frequently mentioned in experiences of SHA that involved harm. When the aggressor’s behavior continued (i.e., was not altered during the event) despite bystander actions, strategies most frequently reported included distract, delegate, and proximity. Together, results suggest that bystander intervention training programs and future research may be needed to understand under what contexts certain strategies successfully prevent or thwart SHA while maintaining emotional and physical safety for those involved.
Introduction
According to RAINN (n.d.), women and individuals who identify as a gender minority experience sexual violence at a particularly high rate. A recent national study suggested that individuals between the ages of 18 and 29, regardless of college status, were more likely to endorse sexual harassment and assault compared to those above the age of 30 (Mumford et al., 2020). Research suggests that this can occur within social events (e.g., parties and bars), wherein bystanders who could help are most often present before a sexual assault (Banyard et al., 2004; Haikalis et al., 2018). Despite lower prevalence rates of bystander presence for sexual assault compared to other types of violence, these witnesses may experience higher rates of threats or incidences of physical harm, which highlights the need to better understand how bystanders can be helpful while maintaining safety (Hamby et al., 2016). Further, few studies have focused on the potential impact of bystander behavior on the aggressor’s actions. The present study aimed to address these limitations using a qualitative approach to better understand victim’s 1 experiences of unwanted sexual behavior while others are present as it relates to (a) the identified bystander intervention strategies, (b) the presence of these strategies based on the aggressor’s subsequent actions, and (c) the presence of strategies related to verbal and physical harm to those involved.
Bystanders have a range of opportunities to intervene to stop sexual violence (McMahon & Banyard, 2012). A bystander can intervene before, during, and/or after a sexual assault has occurred. Behaviors that a bystander may notice during these timepoints are seeing someone isolate the victim while intoxicated (before), walking in on an ongoing rape (during), and/or supporting a victim in reporting an instance of sexual assault (after). The most common timepoint for bystanders to be present is before a sexual assault (Banyard et al., 2004; Haikalis et al., 2018), which includes sexually harassing behaviors (see Fitzgerald et al., 1995 for overview). Further, helping behavior before or during a sexual assault is the only timepoints in which a bystander can prevent or thwart an ongoing situation by reducing or discontinuing instances of sexual assault.
To help someone before or during an experience of sexual assault, bystanders need to have knowledge of how to intervene when they witness unwanted sexual advances. Programs are used to educate potential bystanders on some available strategies to help someone experiencing unwanted sexual behaviors (e.g., the Green Dot; Edwards, 2009). These strategies include direct (i.e., interrupting the situation), distraction (i.e., attempting to change attention to allow the victim to remove themselves from the interaction), and delegation (i.e., sending someone else to disrupt the situation) methods. In a study examining hypothetical responses for bystander action (McMahon et al., 2013), most bystanders stated that they would engage in indirect interventions (59%), particularly distraction, while only 34% indicated that they would use direct methods like assertive communication. Less frequently, participants endorsed that they would delegate to another individual (11%). Among 150 participants who reported on their own intervention strategies during an instance of sexual assault (Moschella et al., 2018), bystanders reported using direct, distraction and delegation methods plus an additional two strategies: diffusion and distance. Diffuse strategies are defined as actions to calm down the involved parties, such as “breaking up the situation by telling the parties to relax or calm down,” (p. 3218), and distance strategies involved physically separating the individuals in some way (Moschella et al., 2018). Bystanders in this study often used more than one strategy to intervene, with the most frequently used strategies being distance (42.7%), direct (42.0%) and distract (26.7%).
A much-needed line of research involves examining what happens after someone engages in bystander actions for sexual assault. A recent study that utilized videos of interpersonal disputes in public, real-life situations wherein a bystander intervened found that 12 of 337 (3.6%) non-escalatory bystanders (i.e., non-aggressive) experienced physical harm (Liebst et al., 2021). Escalatory bystander intervention behaviors (e.g., punching and weapon use) increased risk of physical harm when someone intervened (Liebst et al., 2018). Consequences of bystander intervention are important to consider because they influence whether the helping bystander and those who witnessed the bystander intervention will intervene in a future sexual assault or harassment situation. Active bystanders, or bystanders who intervene, often experience mixed emotions (i.e., both negative and positive) after the intervention (Witte et al., 2017), and bystanders who experience adverse consequences report less intent to intervene in the future (Banyard et al., 2007, 2019). Unfortunately, bystanders of sexual violence—compared to other forms of interpersonal violence—may be at greater risk of experiencing physical harm when intervening (Hamby et al., 2016), and fear of physical harm can be a barrier to bystander intervention (e.g., Exner & Cummings, 2011). Notably, seeing others engage in bystander intervention may be the most consistent predictor of whether a bystander will attempt to prevent a sexual assault (Palmer, 2016). Seeing someone else get hurt while trying to intervene may deter inactive bystanders from becoming active ones in the future.
Few studies have examined bystander actions from the perspective of the victim, which is an important endeavor for several reasons. First, research suggests that the most common barrier to helping behavior for sexual assault is undetected risk (Kania & Cale, 2021). As such, bystanders may have a more difficult time detecting non-consent among less overt sexual violence (e.g., unwanted sexual touching). Further, the existing studies reveal important findings. Specifically, the consequences of bystander intervention (i.e., physical harm and threat to the safety of the bystander during the intervention or as a direct consequence from the intervention) may negatively impact the mental health of victims (e.g., trauma symptoms) following such occurrences (Hamby et al., 2016). Second, bystander presence alone may not be enough to influence mental health outcomes (Hamby et al., 2016). Third, the helpfulness of bystander intervention strategies is largely dependent on the context of the situation (McMahon, 2022). Thus, these lines of research converge to indicate that victim perspectives are needed to understand bystander intervention across a range of sexual violence risks to prevent further harm from occurring. Further, more exploration is needed to determine how bystanders may safely intervene and in what contexts specific bystander strategies are more effective than other bystander strategies for those experiencing sexual harassment or assault (SHA).
One way of conceptualizing helpfulness to the person experiencing SHA is to consider the subsequent behavior of the aggressor toward the victim when someone intervenes before or during a sexual assault, which we refer to as effectiveness. In public situations of interpersonal conflicts, analyzed video footage of 52 disputes suggests that physical interventions decreased the likelihood that the aggressor’s behavior would continue while nonphysical expressions of disapproval did not influence outcomes (Ejbye-Ernst, 2023). Specific to sexual assault, findings suggest that the incidence of victimization and perpetration of sexual assault is lower on college campuses with bystander intervention training programs (Coker et al., 2015). However, more research is needed to understand if these changes are related to bystander actions to prevent or stop sexual assault. To our knowledge, only one study provides information about bystander-helping behavior as it relates to stopping the behavior of aggressors involved in a sexually problematic situation (Moschella et al., 2018). In this study, approximately 13% of participants indicated that the behavior of the aggressors involved in the situation stopped following their intervention. Notably, the participants were not directly asked to indicate whether anyone’s behavior was stopped following their intervention. Thus, the possible impact on aggressor behavior was measured indirectly and spontaneously based on the participant’s report. Perhaps the effectiveness of bystander intervention would be different if participants were directly prompted to provide information about the impact of the bystander’s actions on the aggressor’s behavior.
In a recent study by Bridges and Colleagues (2021), participants were asked to provide how they would respond as a bystander to an alcohol-involved sexual assault depicted in a vignette. These authors obtained five expert witnesses’ quality of bystander intervention, which was conceptualized as the likelihood that certain bystander actions would prevent sexual assault incidences and/or harmful outcomes based on the strategies identified from responses (i.e., “do nothing,” “engage others,” “verbally intervene,” “physically intervene,” “ambiguous,” and “other,” p. 327). Distance strategies were rated as most likely to prevent the incidence of sexual assault and harmful outcomes, followed by verbal confrontation and getting peers involved. The strategy rated as least likely to prevent sexual assault and harmful outcomes was not engaging and getting help from authority figures. Though these findings are informative, this study was based on expert coding of likelihood of these outcomes and an alcohol-involved vignette rather than examining participants’ personal experiences of victimization, helping behaviors, and outcomes. Thus, more research is needed to understand the impact of bystander helping on outcomes related to sexual assault and potential harm to those involved.
Due to limited research on effective bystander actions, subsequent aggressor behavior, and safety of the bystander, aggressor, and self from the perspective of the individuals helped during SHA, the present study was treated as exploratory. Consistent with McMahon (2022), victim perspectives are centered as they are the individuals who are at-risk of harm and may be most impacted by whether bystander interventions can thwart aggressors’ behavior and consequences of actions. Moreover, a qualitative approach was utilized to understand the lived experiences of survivors in their own words and allow additional inquiry into the experience they shared. The present study addressed three research questions:
What strategies were identified by those experiencing SHA when a bystander intervened?
What bystander intervention strategies were mentioned in the experiences when the aggressor’s behavior was described to continue, pause, or stop toward the victim?
What bystander intervention strategies were mentioned in the experiences when there was a reported instance of physical or verbal harm to the victim, aggressor, and/or bystander?
Method
Like previous research examining bystander intervention from the perspective of bystanders (e.g., McMahon, 2022), interviews were conducted at the incident-specific level while focusing on the victims’ experiences of SHA. The data collection started shortly after the onset of the COVID-19 pandemic (August 2020 to March 2022), when many public spaces were restricted and there was less social contact. Institutional Review Board approval was obtained prior to recruitment and data collection.
Participants and Procedure
Participants (N = 25; 80% college students; 96% female) were recruited from the university and surrounding community using a range of methods (e.g., advertisements in college courses, email announcements, and social media). Prospective participants completed an online eligibility screening and were asked to provide their email addresses if they were interested in participating in a follow-up study about their experience of bystander intervention for SHA. The researcher contacted those who provided their emails to schedule a virtual semi-structured interview through WebEx. Eligibility was verbally confirmed with participants prior to starting the interview, which included gender identity of female or gender minority, current age of 18 to 30, and having prior experience of SHA after the age of 16 during which they perceived someone tried to help them. Older than age 16 was chosen in efforts to capture experiences where a person can legally provide sexual consent in most states in the United States (Office of the Assistant Secretary for Planning and Evaluation, 2004).
The semi-structured interviews were primarily conducted by a cisgender female studying clinical psychology as a doctoral student; however, two interviews were conducted by gender nonbinary person who was a post-baccalaureate research assistant. Informed consent was verbally discussed with each participant, which included direct mention of voluntary participation. Participants were asked to provide consent for the interview to be audio and video recorded. Following consent, participants were guided through a semi-structured interview (see below). At the conclusion of the interview, all participants completed a guided relaxation exercise to reduce potential residual distress. They were also provided with a list of mental health and crisis resources during the debriefing phase at the end of the study. College students who participated in the interview were able to choose between additional research credit or a $20 Amazon e-gift card. Those recruited from other methods received the $20 e-gift card compensation.
Measures
Participants also completed demographic questionnaires (e.g., current age, gender identity, race, and sexual orientation) prior to participating in the interview as part of a screening survey. Participants then completed a semi-structured interview, which included structured questions and flexibility for follow-up inquiries (Whiting, 2008). Initial creation of interview questions was guided by Burn’s (2009) application of the bystander intervention model to sexual assault (Latané & Darley, 1970). Specifically, participants were asked to describe (a) what happened between the participant and the aggressor (noticed event), (b) what they believe the bystander noticed that let them know the situation was unwanted or distressing (risk detection), (c) what they perceived led the bystander to intervene (perceived responsibility), (d) why they think the bystander chose the strategy they did (decide to act), and (e) what the bystander did to intervene (choose strategy). For the purposes of this study, participants were asked additional questions regarding whether the aggressor’s behavior stopped after the bystander intervened and to whom, if any, verbal or physical harm occurred.
Data Analytic Approach
Undergraduate research assistants transcribed the interviews, which were reviewed by a second member of the team for accuracy. Two doctoral students in clinical psychology with expertise in sexual assault research analyzed the transcripts using a hybrid coding approach involving deductive and inductive procedures (Fereday & Muir-Cochrane, 2006; described below). The initial codebook was developed prior to reviewing the data. First, the two coders independently read through each transcript to become familiar with the participants’ experiences. Then, the two coders reviewed a subsample of transcripts (n = 4) with the initial codebook and made adaptations for clarity until there was consistency in the coding (83% agreement). The revised codebook was used for the remainder of the coding process. The two coders reviewed a subset of transcripts each week and met to discuss their coding until all transcripts were reviewed (93% agreement). For the coding process, coders read through the transcripts again independently with special attention to the specific questions of interest; however, coders considered the totality of the transcript when coding the data to ensure our codes encompassed the full experience of the participants. The coders discussed the discrepancies for a subset of transcripts each week until they reached consensus. Final codes were imported into NVivo (Lumivero, 2023) for descriptive analyses.
Deductive procedures were used to identify the presence of bystander strategies, effectiveness levels, and verbal or physical harm, all of which were developed a priori. First, coders assessed for the presence of specific bystander strategies based on Moschella and Colleagues (2018) identification of five helping behaviors (i.e., direct, distance, distract, delegate, and diffuse; 0 = not present, 1 = present) plus a “new strategy” code for those not captured. Second, the effectiveness levels were analyzed and defined based on potential impact on aggressor behavior. Entirely effective was defined as the aggressor’s behavior being stopped toward the victim throughout the remainder of the situation following bystander intervention, while entirely ineffective was characterized by a continuation of SHA toward the victim despite bystander intervention. Temporarily effective was conceptualized as an aggressor pausing engagement in SHA for a brief amount of time before continuing that behavior during the same event toward the same victim. Lastly, coders examined the presence of verbal and physical harm occurring to the bystander, victim, and/or aggressor. Each effectiveness level was coded once (0 = not present, 1 = present). Verbal harm was defined as suspected or known emotional, verbal, or threat of harm during or immediately following bystander intervention, which can include behaviors such as calling someone demeaning names, threatening their social status (i.e., spreading lies), and/or threatening to harm someone. Physical harm was defined as suspected or known physical harm to someone involved regardless of severity (e.g., bruises and physical fights). Physical or verbal harm was coded (0 = not present, 1 = present) for victim, aggressor, and bystander.
The inductive process revealed an additional bystander strategy not captured a priori. The two coders discussed the participants’ responses coded as a new strategy to agree upon a label and description of the additional strategy.
Positionality
The primary author of the paper was responsible for conceptualizing the study, interviewing most participants, coding the transcripts, and interpreting the outcomes of the present study. She is a young adult, White, cisgender female, who grew up in a southern state in the United States and currently studies clinical psychology as a graduate student in a predominately White, southern institution. She has been researching the experiences of sexual assault victims for 4 years and has been providing therapy to individuals who have experienced domestic and/or sexual violence. Her demographic background likely increased her ability to establish rapport more easily with the participants during the interviews due to the similarities of herself and the participants. Her personal experiences contributed to the study being designed and analyzed from a perspective that intentionally avoided blaming potential victims of SHA for their experiences. As such, the aims of the study did not inquire about the actions of the victim; instead, focusing on the aggressor’s actions to emphasize their accountability. Relatedly, she also brought a research and clinical perspective to the data being collected and had to be mindful of the duties and expectations from each perspective.
Two other authors participated in the data collection or analysis phase of the study. One coauthor who completed some interviews with participants is a young adult, White, nonbinary person who grew up in a southern state in the United States. This research assistant went through training with the graduate student wherein they watched prerecorded examples of the interview protocol and completed a mock interview that was reviewed by the graduate student. They were also given the opportunity to ask any other questions. They had prior experience working on psychological research examining the effects of alcohol on bystander intervention as an undergraduate research assistant as well as experience working with survivors of abuse. Another coauthor assisted with coding the data and analyzing the new strategies that emerged with the first author. She is a young adult, Asian, cisgender female, who grew up in a southern state in the United States and currently studies clinical psychology as a graduate student in a predominately White, southern institution. She has had experience providing therapy to trauma-exposed veteran populations, which included military sexual trauma. Additionally, the author has experience and familiarity with literature pertinent to sexual violence.
Results
A total of 32 participants were interviewed for the present study. Seven transcripts were excluded due to an intervention occurring after an assault had taken place (n = 4), lack of clarity about the details of one specific event (n = 1), lack of clarity about whether a bystander’s action was intentional (n = 1), and the event occurring before the age of 16 (n = 1). An overview of demographic characteristics of the analytic sample (n = 25) can be found in Table 1. The frequency of interventions that occurred at different time points (i.e., pre-assault, low risk, pre-assault, high risk, and mid-assault) with examples is provided in Table 2. A sample size of 25 is among the most common sample sizes in qualitative research (Mason, 2010) and is comparable to a recent study (McMahon, 2022) with similar methodology and variables as this one (N = 33).
Participant Demographics (N = 25).
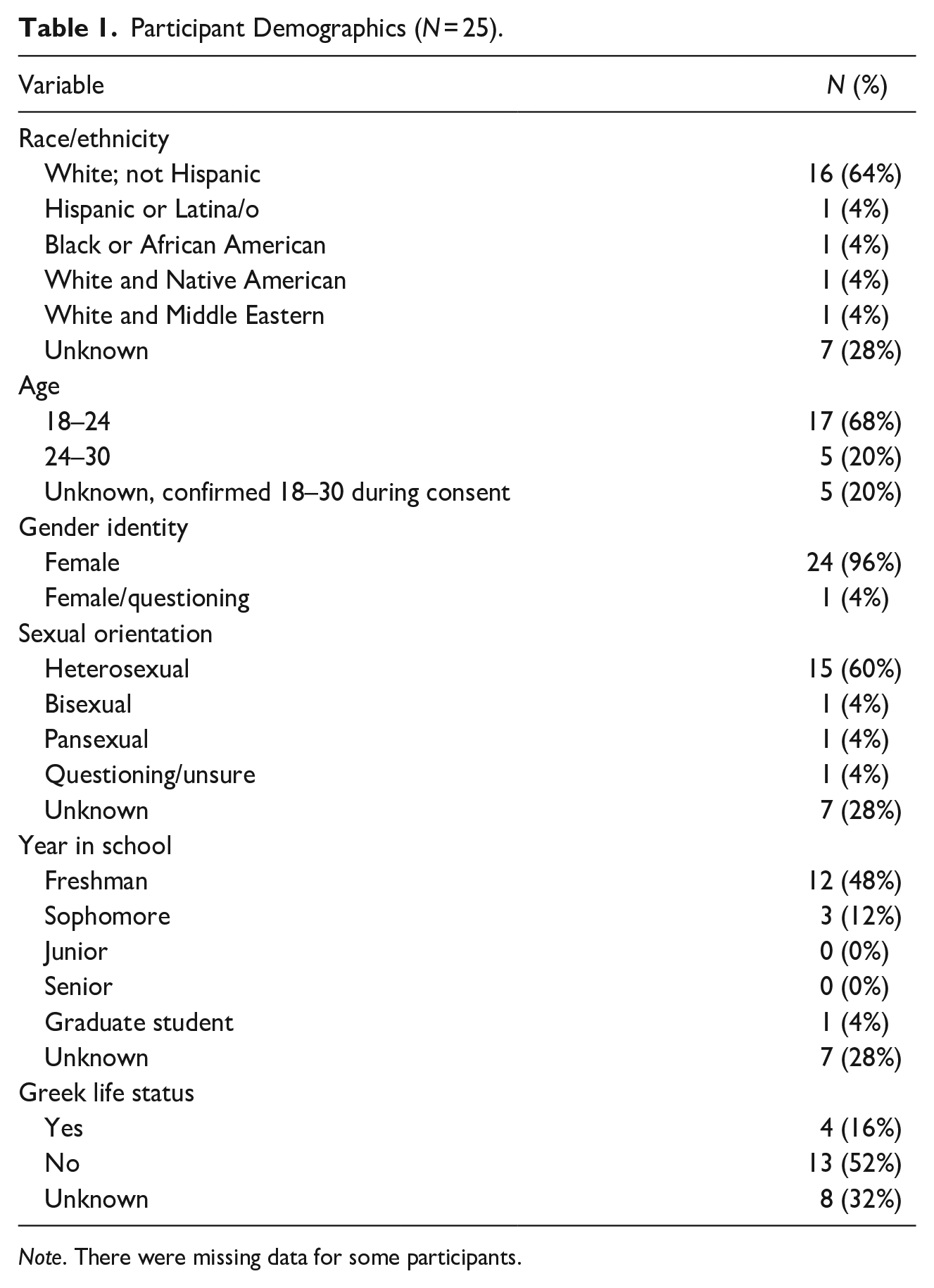
Note. There were missing data for some participants.
Frequency of Bystander Intervention Time Point and Example Behaviors.
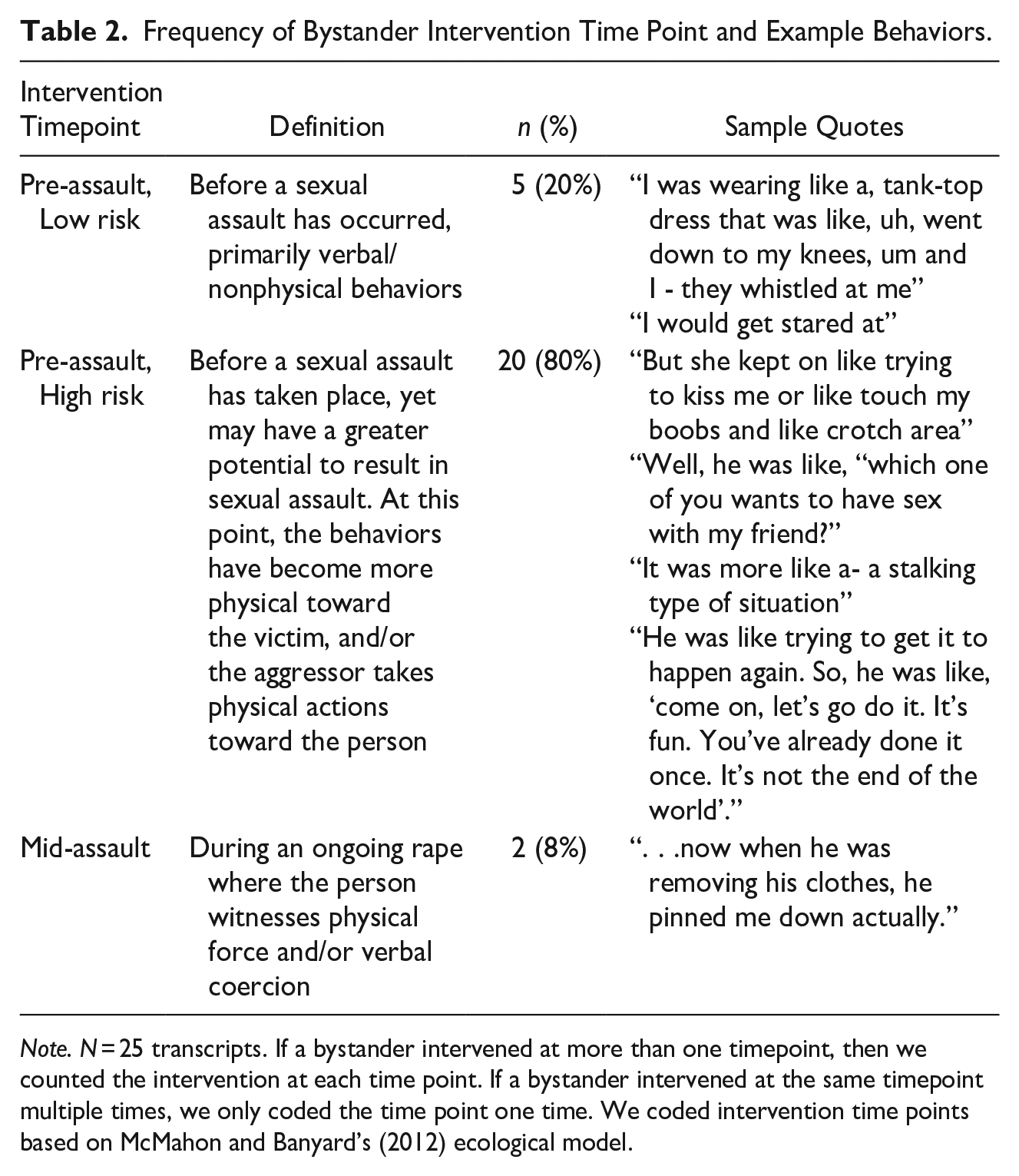
Note. N = 25 transcripts. If a bystander intervened at more than one timepoint, then we counted the intervention at each time point. If a bystander intervened at the same timepoint multiple times, we only coded the time point one time. We coded intervention time points based on McMahon and Banyard’s (2012) ecological model.
Identified Bystander Intervention Strategies by Victims
Participants described five bystander intervention strategies: distance (n = 18), direct (n = 12), distract (n = 8), delegate (n = 1), as well as a strategy not previously articulated in the bystander intervention scholarly field to our knowledge, which was conceptualized as proximity (n = 5) (described below). Table 3 provides an overview of the updated definitions for bystander intervention strategies that were identified by participants.
Strategies and Descriptions Based on Results from Present Study.
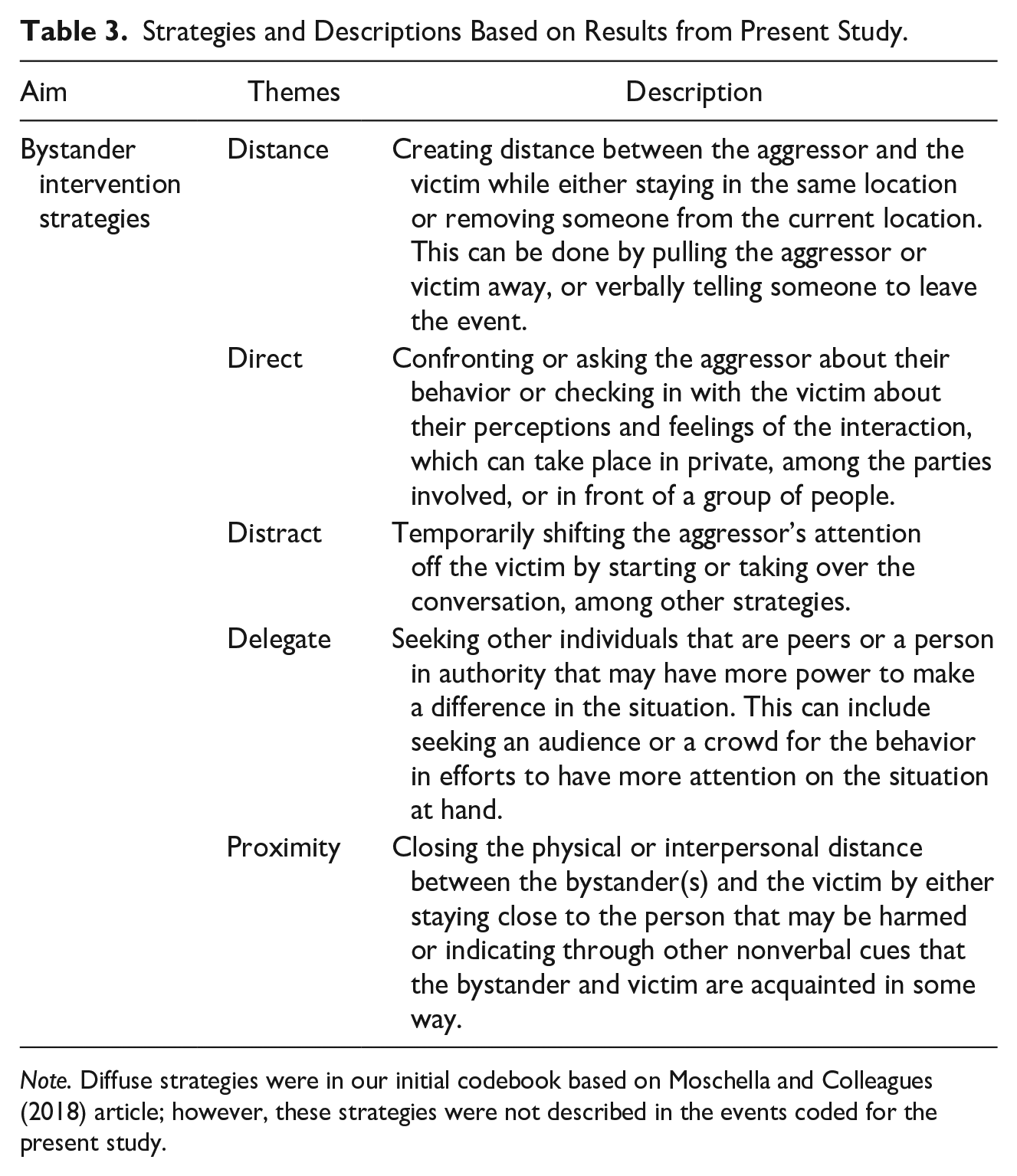
Note. Diffuse strategies were in our initial codebook based on Moschella and Colleagues (2018) article; however, these strategies were not described in the events coded for the present study.
Most participants (n = 15; 60%) described that the bystander used multiple strategies, which seemed to occur in combination or at multiple timepoints during an ongoing situation. The maximum number of strategies used in a single event was three (n = 4). Across the 15 events where multiple strategies were used, the most frequently co-mentioned strategies in an event were direct and distance (n = 10).
Strategy 1: Distance
Participants described a few different ways that the bystander used a distance strategy. First, some participants indicated that bystander(s) created space between the victim and the aggressor while staying in the same location, which was often done by removing the victim from the aggressor’s immediate grasp or space. For example, one participant reported “So, what BYSTANDER did- okay, so I was like frozen up and BYSTANDER like. . . grabbed me [laughs] and like pulled me towards BYSTANDER. . .” and another participant stated “BYSTANDER immediately stood up and. . . came and . . .grabbed me and . . .pulled me. . . And then went to the bathroom and BYSTANDER was talking me through it.” However, there were also times where the bystander attempted to create distance between the two parties involved by removing the aggressor from the situation. This was exemplified when one participant noted “. . . the third time was trying to get AGGRESSOR away from me, not me away from AGGRESSOR.”
Second, some participants indicated that bystanders tried to get them to leave the area of the aggressor entirely while other times the bystander would try to get the aggressor away from the area. For example, one participant reported that a bystander “put herself between them and me, and then like pushed me into the store” and another stated, “BYSTANDER was like, ‘dude, chill’, like kept pushin’ AGGRESSOR away. . .” Similarly, when instances occurred in a public location, bystanders tried to separate the individuals by telling the victim that she did not need to go back into the space that the perpetrator was in. One participant stated the bystander said “okay, yeah, you don’t need to come in this room anymore,” while another participant was informed that “. . .AGGRESSOR [was] staring [her] down, and that [they needed] to not walk by there again.”
Third, some participants indicated that the bystander(s) tried to create a physical barrier between the victim and the aggressor. As an example, one participant noted “. . . BYSTANDERS [tried] to like create a wall, so I could, um, stand behind BYSTANDERS so AGGRESSOR couldn’t see me,” and another stated that “. . . BYSTANDER physically like created like a barrier.” There were also times where the bystander would sit in between the aggressor and victim to create a tiny amount of space, such as “. . .then BYSTANDER sat in between me and AGGRESSOR.”
In one instance, the bystander indicated that she could swap places with the victim, which was upsetting to the victim: “And BYSTANDER was like, ‘well, just switch spots with me’, and I was like, ‘switch spots with you? Then, AGGRESSOR’S gonna just do it to you’. And BYSTANDER was like, ‘well, I don’t care if AGGRESSOR does it to me. I’m single.’”
Strategy 2: Direct
Direct strategies included a few different subsets of behaviors that involved addressing the aggressor’s behavior or checking in about the victim’s perception of the event, which either occurred solely between the people involved or in front of a group. The latter was reflected when a participant reported: BYSTANDER addressed AGGRESSOR in front of the entire room and was like you don’t do that, that’s not allowed, like I think it’s time that you and your friend leave and, um, he’s never made that advance again but it was [a] really uncomfortable experience.
In another instance, the bystander addressed the behavior in front of the immediate parties involved and provided an explanation of the inappropriateness of their actions: . . .as soon as BYSTANDER saw it happen, um, they walked over and they told the person like, “go away. That was not okay, um. Do not do this again. It’s very disrespectful,” and “it made me very uncomfortable, and it’s a violation of my personal space and my body.”
Other bystanders also addressed the aggressor directly by telling the individual to stop without providing an explanation of what was wrong with the behavior, such as when one participant reported the bystander “. . .told AGGRESSOR to stop,” and another stated “. . . BYSTANDER. . . says like, ‘dude, what are you talking about like just stop’.” In other instances, the bystander questioned the aggressor’s actions, such as “. . . asking the person, confronting the person, asking him, ‘why are you doing this?’”
One participant described multiple bystanders asking the victim about their perceptions/feelings about the situation: “BYSTANDERS were like. . . constantly asking how I was feeling and like discussing how AGGRESSOR’s actions were bizarre.”
Lastly, there were instances where direct strategies alongside other types of strategies were implemented, such as in the following quote where a distance strategy occurred following a direct approach: So, um, as soon as BYSTANDER saw it happen, um, they walked over and they told AGGRESSOR like, “go away. . .” And then, they helped me gather my things and they gathered their things and we left to the library, so we were in a different- a completely different environment than where, you know, they had just grabbed my bottom, and so that way I was able to be away from everyone and just me and my friend talked one on one about what just happened, how I was feeling, what I wanted to do, and we just sat there until it was time to go to class.
Strategy 3: Distract
Distract strategies focused on providing a temporary shift in attention from the event. In one example, the participant described that the bystander continuously shifted the aggressor’s attention, such as: BYSTANDER would say things like- like, “AGGRESSOR come and catch me,” . . . “try to catch me,” and then things like, “come here. Let me show you this.” And like, “Oh, look at” . . . “. . .You’re in this picture.” And . . .would be like, “oh, come and sit on this couch.”
In other instances, the bystander(s) were described as taking over the conversation between the victim and aggressor. One participant stated “. . .sometimes like answering those questions or just kind of like trying to hint that he should leave,” and another reported “. . .BYSTANDER came up and, um, started talking to me, so that it was not just me having this conversation with AGGRESSOR.”
Lastly, another participant reported that the bystander tried to physically create a distraction: “BYSTANDER tried to like grab one of their. . . shoulder. Like, just to say like, ‘hey’, I believe.”
Strategy 4: Delegate
One person reported the use of delegation strategies, which involved getting a group of individuals together to help. This was mentioned in the following response: “. . .BYSTANDER now went to call out the other crowd.” Notably, other strategies were reportedly implemented prior to this one when others could not adequately address the aggressor’s behavior.
Strategy 5: Proximity
Proximity strategies were conceptualized as enclosing physical or interpersonal distance between the bystander and the victim, which seemed to be in efforts to indicate that the victim was not alone and to assert their presence or relationship with the victim. In other words, participants mentioned that bystanders tended to stay close to them physically or engaged in actions that showed the aggressor that the bystanders were romantically or emotionally connected to the victim. These strategies were distinct from distance due to the emphasis on staying near the victim or aggressor (i.e., proximity) rather than creating distance between the parties (i.e., distance). For example, a few participants stated that the bystander(s) stayed near them in the situation, such as “. . . didn’t like leave me like alone by myself” and “. . .BYSTANDER showed up and was like, ‘yeah, no. You guys are staying here. . .’”
Another participant described a bystander coming into the space where the event was happening as an intervention: “. . .BYSTANDER helped just by having his presence there.” For interpersonal closeness, one strategy appeared to indicate that the bystander was affiliated with the victim, such as when a participant reported “BYSTANDER. . . put his arm around me and stuff to be like, ‘okay, we’re together’.”
Aggressor Behavior and Strategies Present
Overall, almost all the participants reported that the aggressor’s behavior was stopped for the remainder of the situation immediately following at least one bystander intervention strategy or co-occurring bystander interventions (84% of all events). Five of the events (20%) included at least one intervention that paused the aggressor’s behavior, and five events (20%) contained at least one strategy that did not alter the aggressor’s behavior immediately after intervention.
Table 4 provides the frequency of each effectiveness level based on the presence of each strategy in the event. Of the events that ended with the aggressor’s behavior stopping at the event-level (effective), the majority involved at least one distance strategy, nearly half included at least one direct strategy, and nearly 29% mentioned a distract strategy. Mentions of proximity and delegation strategies were less common in events in which the aggressor’s behavior stopped. Of the reported instances with at least one strategy described as pausing the aggressor’s behavior for a short length of time prior to re-engaging in SHA toward the same participant (temporarily effective), all involved at least one distance strategy; 40% involved direct, distract, and/or proximity strategies, while none involved delegation. Within the accounts where an aggressor’s behavior was described as continuing regardless of the bystander intervention (ineffective), 60% involved direct and/or distract strategies, 40% involved proximity, and 20% reported distance or delegate.
Presence of Strategies and Effectiveness.
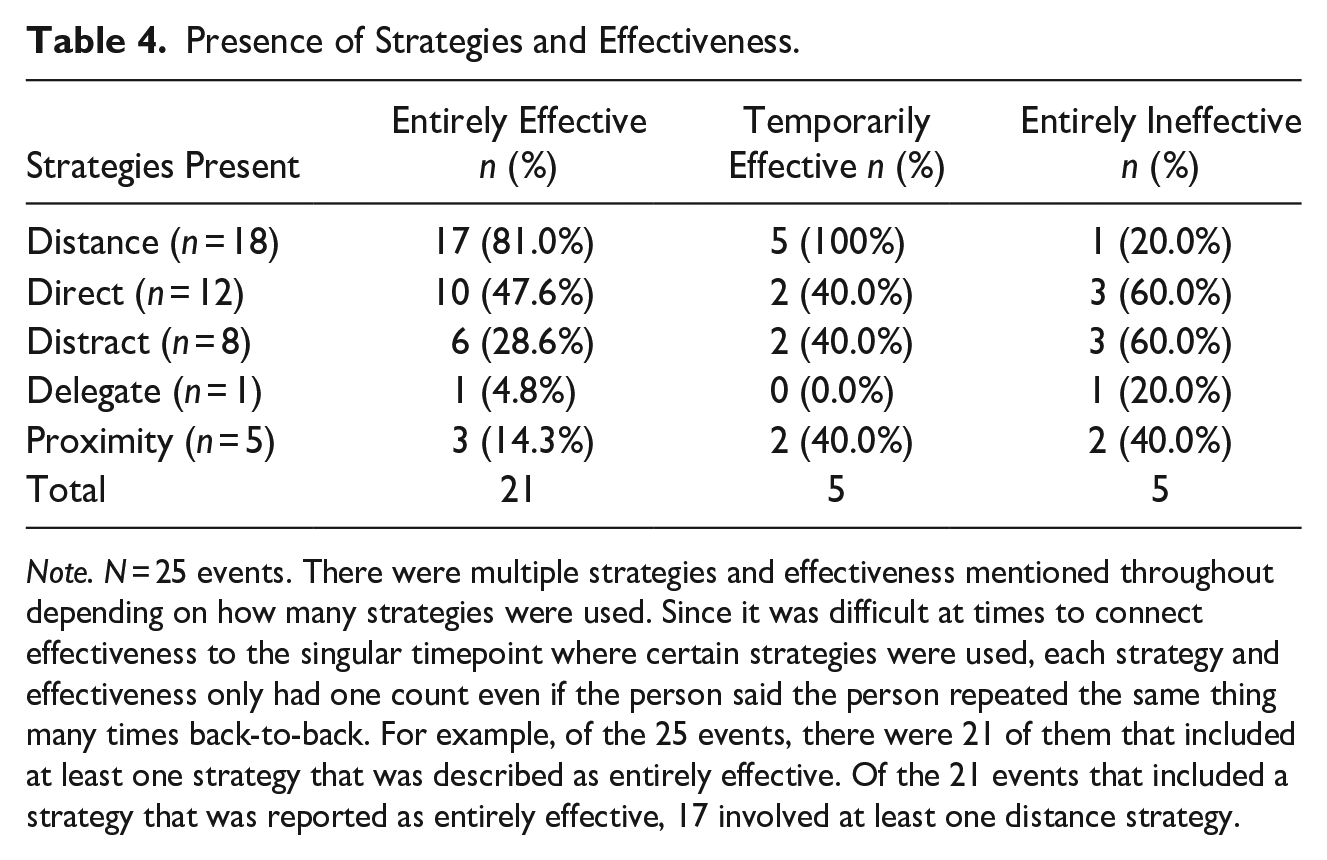
Note. N = 25 events. There were multiple strategies and effectiveness mentioned throughout depending on how many strategies were used. Since it was difficult at times to connect effectiveness to the singular timepoint where certain strategies were used, each strategy and effectiveness only had one count even if the person said the person repeated the same thing many times back-to-back. For example, of the 25 events, there were 21 of them that included at least one strategy that was described as entirely effective. Of the 21 events that included a strategy that was reported as entirely effective, 17 involved at least one distance strategy.
Entirely Effective
Most of the experiences ultimately ended in the aggressor’s behavior stopping toward the victim. The aggressor’s behavior was described as stopping when the victim was out of reach or grasp from the aggressor, which could be while in the same space or when they left that location. For example, one participant stated “AGGRESSOR stopped with me, ‘cause AGGRESSOR couldn’t reach me anymore. . . I think. . .it was really just that I was the most convenient person,” while others stated “. . .AGGRESSOR stopped that long enough to where like I can leave,” and “. . .I never had any other classes with AGGRESSOR or like lunch with AGGRESSOR, so it stopped then.”
Participants also mentioned that the behavior was stopped potentially due to other external reasons like the passage of time, such as “. . . because at that point it was getting close to like bedtime,” or “. . .we were only there for an extra 30 minutes and then we left. So, I didn’t see AGGRESSOR there.”
At other times, the participant stated that the behavior was stopped out of internal reactions (i.e., emotions) based off attention from other people or the presence of certain individuals. For example, one participant stated that “AGGRESSOR actually feared. . .there’s a crowd. . .also the shame,” and another reported “AGGRESSOR’s step-dad scares him more than. . .mom, does.” Other participants indicated that the behavior discontinued for an extended period of time, such as “. . .for like a year AGGRESSOR didn’t reach out,” or “Um, with me it stopped for the rest of like. . .since I’ve known AGGRESSOR.”
Temporarily Effective
Temporary effectiveness is exemplified by the following quote from a participant: The first time I think it was just that there was someone else present, ya know. Someone else is witnessing this. . . The second time the BYSTANDER tried to intervene or like the third whole incident, umm, I think it was more. . . the physical intervention, because AGGRESSOR didn’t see BYSTANDER coming.
Similarly, another participant described that the aggressor’s behavior was temporarily paused while in the presence of the bystander: . . .I think that while BYSTANDER was there uh the AGGRESSOR didn’t feel like she could get away with doing it again, but then as soon as BYSTANDER left I think AGGRESSOR was like, oh okay that person is gone, the other two didn’t intervene when I was starting these behaviors so like I can continue them now.
Another participant had a similar experience, in which she stated “Temporarily. Like AGGRESSOR stopped for the rest of the class, but then like when the next class. . . like nobody said anything, then AGGRESSOR would do it again until they said something.”
At other times, the participant reported that the aggressor paused their behavior temporarily due to being distracted by other things or people. As an example, one participant reported that the aggressor found another person to talk to before returning to her. This person described this experience as “kind of playing hide and seek” wherein she would continuously change locations after the bystander intervened once the aggressor continuously showed up.
Entirely Ineffective
In each of these instances, the perpetrator’s behavior was described as continuing regardless of the bystander’s intervention by saying that “AGGRESSOR didn’t stop,” or “it just continued.” Other participants expressed hope that the aggressor’s behavior would stop in the future, such as “You know hopefully it stopped for—I mean, well like, potential victims but, um, not for me.”
Lastly, one participant described difficulty saying whether the behavior stopped: It’s hard to say whether it deferred AGGRESSOR at all because, you know, we were standing there for a little bit, AGGRESSOR was still staring and then it wasn’t- it wasn’t for a little bit that we moved to the next area and that’s whenever AGGRESSOR moved with us.
Verbal or Physical Harm and Strategies Present
In the 25 experiences shared, six (24%) of them included behaviors that were consistent with verbal or physical harm, and all six involved an instance of verbal harm. Verbal harm primarily occurred to aggressor (n = 3) and victim (n = 2), followed by bystanders (n = 1). However, physical harm occurred in two (8%) of the 25 experiences, both of which also included verbal harm. Table 5 shows the frequency of verbal and physical harm to each party involved and the strategies present within the experiences.
Presence of Strategies and Verbal/Physical Harm.
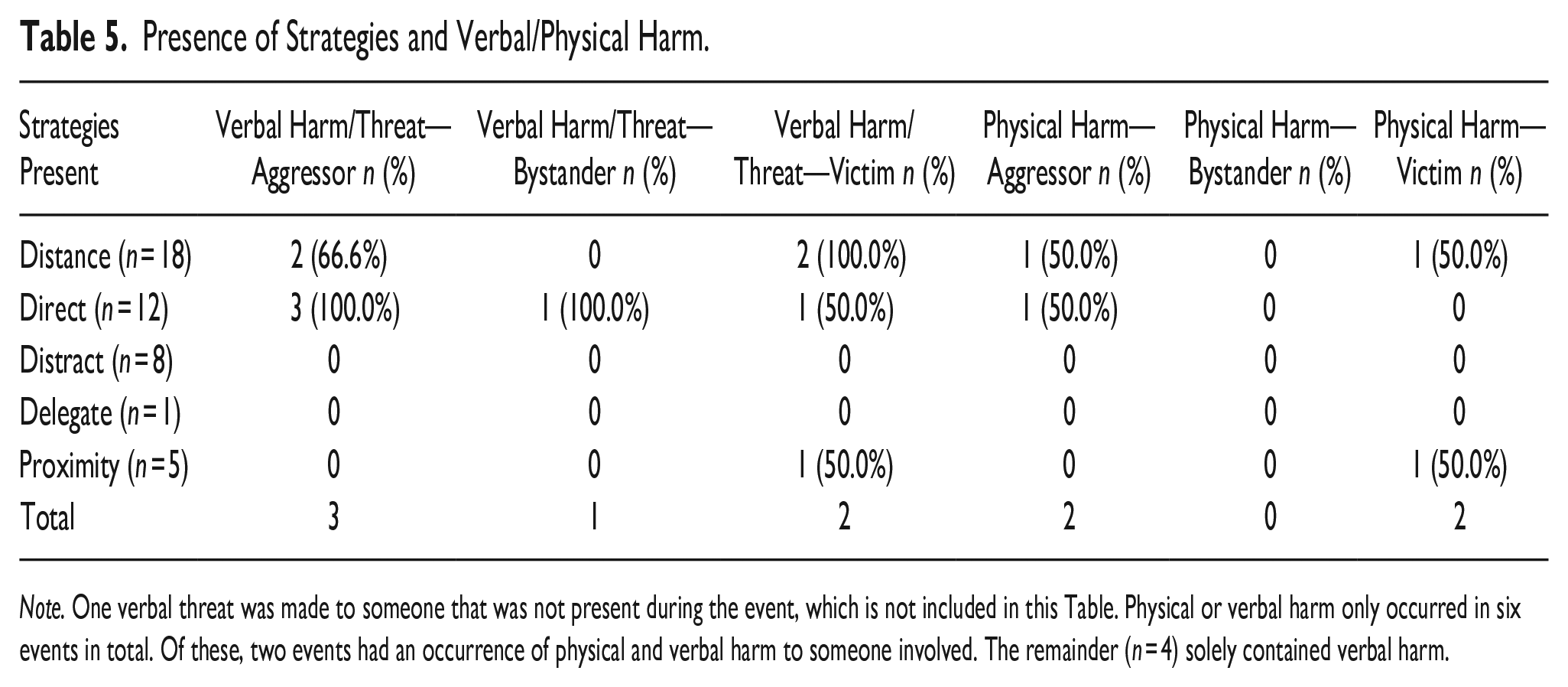
Note. One verbal threat was made to someone that was not present during the event, which is not included in this Table. Physical or verbal harm only occurred in six events in total. Of these, two events had an occurrence of physical and verbal harm to someone involved. The remainder (n = 4) solely contained verbal harm.
Verbal Threat/Harm
One participant reported that the perpetrator was being threatening by “ranting and cursing and calling me a bit**,” while another participant reported, “I don’t wanna cuss on here, but like asking why I was being a B word and like- . . . Constantly like getting closer and closer to me as I was backing up.” Another participant indicated that the bystander and aggressor were threatening each other: “Like, one was like, ‘oh, get out of my face before I do this’, and then the other one was like ‘well I’ll do this if you do this’. You know like- just bickering back and forth kind of.” In another instance, the aggressor was the only person threatened when the bystander reportedly stated, “don’t do that again or like next time I won’t be so nice.” In a unique instance, the aggressor threatened harm to a person that was not present during the incident: AGGRESSOR like, at one point . . . was like, “I’m going to burn this and like throw it into his”—I don’t know AGGRESSOR was just making dumb threats and trying to be funny cause she was like, “he doesn’t deserve you,” you know all that stuff.
Another bystander was described as directly threatening the aggressor when the participant stated, “BYSTANDER was gonna beat him, um, if he ever found out AGGRESSOR laid a hand on me. . .again.”
Physical Threat/Harm
There were only two reported instances of physical harm described by participants. One participant mentioned that they experienced physical harm during a bystander intervention: I ended up with a pretty good bruise all the way around my arm. It wasn’t like a handprint or anything. It was just kind of- AGGRESSOR was grabbing at me, not necessarily grabbing and like squeezing, umm. Except for that third time, AGGRESSOR really got ahold of me, umm, but I mean other than that, I just ended up with a pretty good bruise on my arm.
Another participant suspected that the aggressor may have been physically hurt due to the presence of physical objects during the intervention: Um well because BYSTANDER physically moved AGGRESSOR and in doing so, the AGGRESSOR hit her arm against the corner of my desk. So, I imagine that probably resulted in a bruise, but I never heard anything about it.
Discussion
We used a qualitative approach to better understand bystander intervention strategies used in SHA situations and intervention consequences from the perspective of the victim who experienced the SHA while another person was present and took action to help. Findings provide information about what strategies bystanders used to help the victim in instances of SHA, which intervention strategies were present based on the aggressor’s subsequent actions, and the extent to which the instances included verbal and physical harm to those involved.
The first aim was to determine bystander intervention strategies identified by victims of SHA. Of the identified five strategies, four of the strategies (i.e., distance, distract, direct, and delegate) were consistent with previous research on self-reported bystander helping actions (Moschella et al., 2018) and one new strategy (i.e., proximity) emerged from the data. The majority of the 25 events involved at least one distance (n = 18) strategy, followed by direct (n = 12), distract (n = 8), proximity (n = 5), and delegate (n = 1). To our knowledge, the proximity strategy is not described in previous research examining bystander intervention for SHA. However, 20% of the victim’s events included mention of this strategy, indicating proximity may be a relevant strategy to consider in future bystander intervention programming. Further, this strategy can be incorporated into future research efforts examining effectiveness of different interventions as it relates to instance rates of sexual assault (i.e., does staying close to the victim protect against SHA?).
Unlike previous research (Moschella et al., 2018), none of the victims mentioned diffuse strategies (i.e., calming down the parties involved) as a bystander action during SHA. This may have occurred for several reasons: (a) participants did not experience these strategies as helpful or designed to interrupt ongoing problematic actions, (b) these strategies were overlooked when recalling the experience, or (c) these strategies were not used by bystanders in the types of participant situations. Further, diffuse strategies may not be used commonly in the experiences within this study because participants may view this strategy as invalidating. While emotional support is viewed as helpful (McMahon, 2022), diffusion operates differently in that there is the potential underlying message that the emotional discomfort experienced by the victim must be minimized for SHA intervention to be effective.
The second aim was to understand the aggressor’s behavior in terms of whether their actions were stopped, paused, or continued following bystander intervention, and the presence of certain strategies in the experience of SHA based on these outcomes. Our study revealed that the aggressor’s behavior ultimately discontinued toward the victim at the event-level following at least one bystander intervention in 84% of the experiences. To our knowledge, the only study that has attempted to look at the relationship between bystander intervention strategy and the thwarting of behavior of parties involved was conducted by Moschella and Colleagues (2018), in which 12.7% of respondents spontaneously reported that the behaviors were stopped. It is suspected that these discrepant findings resulted from methodological differences; specifically, the present study was interview-based rather than survey-based, and interviewers directly asked about the behavior of the aggressor being altered while the other study did not prompt for this information. Further, the other study consolidated the behavior of all parties, while our focus examined victims’ perceptions of the aggressor’s behavior.
Moschella and Colleagues (2018) found that the parties involved stopped their behaviors most frequently when a distract or diffuse strategy was reported, followed by direct, distance, and delegate strategies. On the contrary, our findings suggested that when the aggressor’s behavior was stopped, the most frequently reported strategies were distance, direct, distract, proximity, and delegate strategies—and not diffuse strategies. This is consistent with findings in the study conducted by Bridges and Colleagues (2021) in which distance and verbal confrontation (i.e., distance and direct in the current study) were rated as most likely to prevent sexual assault and harm. Of note, the strategies that were mentioned least often when the aggressor’s behavior was stopped were also identified least often by participants in the present study. Thus, it is impossible to determine whether the differences in effectiveness rates occurred due to the infrequent use of such strategies or true behavioral outcomes from the selected intervention strategies. The current findings suggest that distance strategies, which frequently involved removing the victim from the immediate vicinity of the aggressor or leaving the situation where the aggressor was present altogether, may be most helpful in discontinuing the behavior of the aggressor. Direct strategies were present in half of the experiences in which the aggressor’s behavior was stopped entirely at the event-level, which often involved confronting the aggressor about their actions or checking in with the victim about their consent and comfort within the event. Thus, it is possible that discussion of problematic behaviors may be able to alter the aggressor’s behavior while bystanders are present and helping.
Among the events that included the presence of distance strategies, 36.8% involved the bystander removing the victim (n = 6) or the aggressor (n = 1) from the situation entirely. Essentially, this means that these bystanders prompted and encouraged the person being harmed to leave the situation entirely or asked the aggressor to leave the space. This resulted in the halting of the perpetrator’s behavior toward the victim. Therefore, it is possible that the effectiveness rate would be lower when bystanders utilize distance strategies while remaining in the same location (e.g., moving to another part of the same room) as opposed to leaving the situation entirely.
The last study’s aim was to examine rates of verbal and physical harm, and which strategies were present. Overall, most events (about 76%) did not involve verbal or physical harm to anyone involved. Reports of verbal or physical harm usually involved verbal or physical harm to more than one person. Given the relatively small number of instances of harm in the study, it is beyond the scope of the study to ascertain whether there are patterns related to harm and implementation of a specific bystander strategy. While direct and distance strategies were mentioned the most when harm was present, these strategies were also the most frequently mentioned overall. Of note, physical and verbal harm occurred least frequently to bystanders, which contrasts with findings by Hamby and Colleagues (2016) suggesting bystanders of sexual violence may be at increased rate of harm compared to other forms of violence.
Limitations
A major limitation of the present findings is that qualitative research does not allow for causal explanations; therefore, this study cannot conclude whether the behavior was stopped, altered, or continued due to the specific strategies reportedly used by the bystanders. As such, there are no causal conclusions or specific recommendations regarding which strategies were able to stop aggressor’s behavior in the moment. Further, the two coders only coded for whether the strategy was present once during the experience or not at all. Thus, these results do not capture the specific number of interventions that were used at multiple timepoints or when a bystander engaged in two strategies at the same time. Similarly, there was a disproportionate mention of certain strategies (i.e., distance, distract, and direct) over others (i.e., proximity and delegate), which makes it difficult to conclude whether these strategies were less prevalent when the aggressor’s behavior was stopped due to limited use or identification of those strategies. Future research would benefit from recruiting a larger and more diverse group of victims of SHA to replicate and extend the present findings. Observational or experimental research may be helpful in drawing more specific conclusions.
Another limitation is that participants in this study recognized that a bystander tried to help them. Due to the victim observing their help, it is possible that there were (a) other strategies that went undetected, or (b) other people who attempted to help the victim who were not noticed. These are also participants who seemed to want help, and most believed that the aggressor’s behavior stopped because of the intervention from the bystander; however, it is possible that these situations were thwarted for other reasons unspecific to the intervention and strategies. Future research could consider addressing these limitations, perhaps by including both the bystander and victim in an interview to compare their perspectives. Studies could also more broadly recruit victims of SHA that believe the situation was thwarted and ask their perceptions as to why to gain a better understanding of options to stop sexual assault within and outside of bystander intervention strategies. In addition, as few people reported that the intervention did not work to stop the SHA, it is difficult to understand whether the strategies associated with a thwarted SHA are similar or different from the strategies that tend to be present when intervention appears to be ineffective. It is possible that victims of SHA in which bystander intervention was ineffective may be less likely to perceive it as help and therefore be less likely to volunteer for our study. Recruitment of individuals who experienced SHA with others present who could possibly intervene could provide a wider range of bystander intervention strategies and effectiveness.
There are also strengths of the present study. To our knowledge, this is the first study to examine identified bystander intervention strategies from the perspective of the victim of SHA, and to examine how bystander intervention can impact aggressor’s behavior and verbal threat/harm, as well as physical harm to those involved. Further, we employed a semi-structured interview procedure to allow participants to share their experiences in their own words prior to guiding them throughout the interview process to center victims’ voices. The research questions were framed using non-judgmental language and allowed victims to share their experiences through their own worldview with minimal directive input from the interviewers aside from the standard interview questions. Moreover, interviewers intentionally avoided asking questions directly about the victim’s behavior to avoid victim-blaming language. We also had two coders with expertise in sexual assault research code the data, which allowed the two coders to discuss the discrepancies and come to an agreement on the various codes. This also provided multiple perspectives on coding the data, which can increase confidence in the findings of the present study. Further, this research did not restrict aggressor gender or focus exclusively on cisgender females (though this was the population that participated), which was done in efforts to include a more diverse group of individuals.
Future Directions
Future researchers can consider multiple avenues to further extend the present findings. First, recruitment of a larger and more diverse sample may be able to capture more and potentially different experiences with bystander intervention strategies, which could allow for more specific conclusions about the various strategies, effectiveness levels, and harm as a result. Bystanders may be less likely to intervene or to intervene in a certain way for fear of their own safety due to aspects of their own identity (e.g., gender, race, sexual orientation, and disability). There may also be hesitancy based on the aggressor’s identity (e.g., it might be riskier to use certain strategies if you’re a woman of color intervening with a white male aggressor; see Cole and Duncan (2022) for a review of bystander interventions through an intersectional lens). Further, some research suggests that White female bystanders may be less likely to intervene for Black female victims when at risk for alcohol-involved sexual assault (Katz et al., 2017) and bystanders are less likely to intervene among gay men (Katz et al., 2015); thus, bystanders may intervene later in the continuum for victims with certain characteristics. Unfortunately, we did not ask about such characteristics and cannot ascertain this information. Second, it may be helpful to delineate the strategies that successfully thwart SHA while maintaining safety, and the specific contextual features that may play a role in such outcomes. Third, it is unclear how the identification of bystander intervention may influence victims’ future behavior. For example, a few participants in this study mentioned that they did not want to make a “big deal” out of a small situation and suggested that bystander intervention confirmed that their experience was problematic. This seemed to validate participants’ perceptions of events, and at times, encouraged advocacy for oneself. Considering the importance of emotional validation for victims (McMahon, 2022), this identification of help from a bystander may be important to confirm one’s perceptions that SHA is problematic. Relatedly, future research could examine how these different outcomes of bystander intervention impact mental health outcomes among victims.
Prevention Implications
The results of the present study have important implications for bystander intervention training programs to prevent and thwart SHA. First, our findings suggest that bystanders may need to be persistent and use a variety of strategies in their efforts to stop an ongoing sexual assault considering that over half of the participants used a combination of strategies. Second, the strategies selected by bystanders to intervene may have differing implications for whether the aggressor’s behavior is stopped, as well as whether an instance of physical or verbal harm occurs. Thus, bystander education programs that emphasize strategies for intervention may want to consider the interaction of strategies and the goals of the victim on effectiveness. For example, many participants in the present study eventually left the situation, which discontinued the aggressor’s behavior. Thus, different strategies may be effective depending on whether the victim wants to stay in the same location despite experiencing SHA. Though there is variability in the presence of strategies and potential consequences, these findings also suggest that bystander intervention may be relatively effective and safe for bystanders given that the aggressor’s behavior was stopped toward the victim and the bystander was unharmed in most experiences. Nonetheless, there was still some rate of verbal and physical harm, so prevention programs can use this information to help bystanders consider how to keep themselves safe and weigh the pros and cons of helping. Importantly, some victims of SHA spontaneously reported that the same aggressor sexually assaulted them at a later time when bystanders were not present, suggesting that bystander action in one event may not extend to another situation if intervention does not occur again. Thus, bystander prevention programs may want to consider how bystanders can use their interventions to promote long-term behavior change and understand how these findings may vary among different aggressor-victim-bystander groupings based on personal characteristics. Ultimately, bystander intervention training programs need to be inclusive and cognizant of power and privilege when teaching community members how to help in a way that is safe and effective.
Footnotes
Acknowledgements
Thank you to the 2021 to 2022 Bridges Fellowship program at the University of Arkansas for supporting this research. This paper was based on the first author’s master’s thesis. I would like to express gratitude to Angie Wallace, Nikita Britto, and Morgan Wilson who helped with transcribing the interviews.
Authors’ note
Portions of this paper were presented at the 2023 International Conference on Sexual Assault, Domestic Violence, and Fighting for Change, Chicago, IL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by the Howell’s grant [2010.04S] University of Arkansas.