
Abstract
Limited knowledge exists concerning the prevalence and drivers of intimate partner violence (IPV) against Afghan women and its association with child morbidity and mortality in Afghanistan. The study used data from the 2015 Afghanistan Demographic and Health Survey (ADHS 2015). The prevalence and associated sociodemographic factors of IPV were described by analyzing the data from Afghan women aged 15 to 49 years selected for the IPV module in ADHS 2015 (n = 24,070) whose children under 5 (n = 22,927) were included in the further analysis to estimate the morbidity and mortality of children and its association with IPV. It appeared that more than half of the Afghan women aged 15 to 49 years experienced IPV in the past year. Illiteracy (odds ratio [OR] = 1.69; 95% CI: 1.19, 2.39), living in rural areas (OR = 1.47; [1.19, 1.82]) being from the Pashtun, Tajik, Uzbek, and Pashai ethnic backgrounds were associated with a higher risk of IPV exposure. In general, the likelihood of child mortality within the first 5 years was higher among children born to mothers exposed to IPV, particularly physical and sexual even after adjustment for sociodemographic inequalities, the number of antenatal care, and marriage age. In addition, the odds of diarrhea, acute respiratory infection, and fever in the past 2 weeks were significantly higher among the children of victimized mothers in both adjusted and unadjusted models. Moreover, low birth weight and small birth size were more likely to be observed among the children of a mother who either experienced sexual or physical violence. The findings emphasized the elevated risk of morbidity and mortality among children under 5 born to mothers exposed to IPV and incorporating IPV screening into maternity and child care could reduce these adverse outcomes among Afghan women.
Introduction
Intimate partner violence (IPV) against women is a serious public health issue with vital human rights implications. IPV is defined as physical, emotional, and sexual violence (SV) as well as spousal controlling behavior (Dadras, Nakayama, et al., 2022) and is the most common form of violence against women that has recently received enormous international recognition due to the obvious violation of women’s rights, particularly in the developing world (World Health Organization [WHO], 2021b). IPV is a widespread issue in conflict and postconflict contexts such as Afghanistan. It has been reported that almost half of the Afghan women aged 15 to 49 years have once been the victim of spousal violence in their lifetime (Gibbs et al., 2018; Nijhowne & Oates, 2008; Stark & Ager, 2011). Several factors such as poverty, illiteracy, child marriage, patriarchal norms, and longstanding conflict could increase the risk of IPV exposure (Gibbs et al., 2018; Krug, 2002; United Nations Development Programme, 2015); however, their decompositional contribution to the IPV incidence could vary across different contexts. Meanwhile, limited knowledge exists concerning the sociodemographic inequalities that could instigate spousal violence against Afghan women; thus, further studies are warranted.
In addition to the harmful consequences of IPV on women’s health, several adverse health outcomes have been documented among the children of victimized women (Bacchus et al., 2004; Sabarwal et al., 2012). It has been shown that children who witness IPV may experience more emotional and behavioral distress such as anxiety, depression, low self-esteem, nightmares, poor school performance, risky behavior, and physical health issues (Carlson, 2000). Additionally, they are more likely to suffer from IPV in later life (Ellsberg et al., 1999; Jewkes et al., 2003). IPV has been also linked to low birth weight, under-immunization, malnutrition, and a higher risk of infectious disease in early life (Nasir & Hyder, 2003; Paul & Mondal, 2021; Sabarwal et al., 2012; Ziaei et al., 2014). It has also been shown that IPV could lead to higher morbidity and mortality among children under 5 years in several settings (Ackerson & Subramanian, 2009; Asling-Monemi et al., 2008; Garoma et al., 2012), but the results are controversial as a variety of sociocultural, economical, and environmental factors could influence this association. For example, a study in Bangladesh found no association between IPV and children under 5 mortality (Asling-Monemi et al., 2008), whereas other studies from India observed higher mortality and mortality among children under 5 (Ackerson & Subramanian, 2009; Paul & Mondal, 2021).
Afghanistan is one the countries with the highest mortality rate of children under 5 in the world, and an estimated 55% of children died under the age of 5 years in 2020 (World Bank, 2020). The leading causes of death among children under 5 in Afghanistan include pneumonia, diarrhea, and preterm birth complications (WHO, 2021a). Despite the high prevalence of violence against women in Afghanistan (Dadras, Nakayama, et al., 2022) and its potential association with childhood mortality and morbidities, there is no previous report of such findings in Afghanistan. Therefore in this study, first, we aimed to explore the prevalence of IPV and the impact that different types of IPV could have on the mortality and morbidity of children under 5 born to mothers who experienced such violence in a nationally representative sample of children under 5 in Afghanistan. Additionally, since previous studies suggested that adverse child outcomes could be prevented by appropriate antenatal care (ANC) and regular monitoring of fetus growth in the womb during pregnancy (Doku & Neupane, 2017; Kuhnt & Vollmer, 2017), we further examined the impact that adequate ANC could have on the association of IPV with children morbidity and mortality. Besides, early age at marriage (<18 years) is documented as a potential reason for higher adverse child outcomes (Hossain et al., 2022; Paul, 2020; Raj et al., 2010) and thus, we further adjusted for the mother’s age at marriage to account for such effect, if any.
Methods
Study Design in ADHS (2015)
This cross-sectional study analyzed the data for a sample of Afghan women aged 15 to 49 years old, who were selected for the IPV module in the Afghanistan Demographic and Health Survey (ADHS) in 2015 as well as their children under 5 years. ADHS is a nationally representative survey implemented by the Central Statistics Organization in collaboration with the Afghanistan Ministry of Public Health and funded by the United States Agency for International Development.
Study Population and Sampling in ADHS (2015)
ADHS (2015) gathered data for women aged 15 to 49 years and their children aged less than 5 years old. A stratified two-stage cluster sampling was applied to estimate the key indicators at the national level, in urban and rural areas, and for each of the 34 provinces in Afghanistan. The sampling included 950 clusters (enumeration areas from the previous national census) including 260 urban and 690 rural areas. In the second stage, through an equal probability systematic selection process, 25,650 households were selected within 950 clusters. Sampling weights were applied to obtain a representative estimate at the national level. A sample of the women aged 15 to 49 years (n = 29,641) who were either permanent residents of the selected households or visitors who stayed in the households the night before the survey were recruited after informed consent. The women were interviewed about all births in the past 5 years, the sample from which data were derived in the present study. Following the World Health Organization’s guidelines for the ethical collection of information on domestic violence, only one eligible woman per household was randomly selected for this module; the module was not implemented if privacy could not be obtained (WHO, 2001).
Measurement and Scales
A standard Demographic and Health Survey (DHS) questionnaire gathered data on sociodemography, health status, and access to health services from all eligible women and their children under 5. This includes women’s and children’s demographic characteristics, household information, family planning, fertility preferences, women’s and children’s health, sexually transmitted diseases, marriage, sexual behavior, and domestic violence (Dadras & Chapman, 2017). However, for the current study, our primary interest was questions related to IPV of married women aged 15 to 49 years and morbidity and mortality indicators of children under 5 years.
Independent Variables
Exposure to IPV was measured using a modified version of the Conflict Tactic Scale (Straus et al., 1996), in which any experiences of different types of IPV during the past 12 months were explored. Physical violence (PV) was defined as being slapped, kicked, bitten, pushed, punched, choked, burnt on purpose, or assaulted using a knife or other weapons. SV was defined as forced sexual intercourse, degrading or humiliating sexual acts, or engaging in sexual intercourse out of fear. Emotional violence (EV) was described as exposure to verbal abuse or insults, made to feel bad about oneself, belittled in front of other people, scared or intimidated, threatened with violence, or confronted with threats of harm. The responses were dichotomized into 1 = “yes” and 0 = “no.”
Outcomes of Interest
Eight indicators concerning the morbidity and mortality of children under 5 whose data were available in ADHS (2015) were selected as follows:
The morbidity indices included five indicators: (a) diarrhea in the past 2 weeks, (b) acute respiratory infection (ARI) in the past 2 weeks (i.e., whether the child had suffered from a cough and rapid breathing in the last 2 weeks), (c) fever in the past 2 weeks, (d) very small or small size at birth (“very small or smaller than average” vs. “average or larger”), and (e) low birth weight (birth weight < 2500 g). Due to the large proportion of birth at home (46.27%) and lack of reliable records, there were 18,874 missing cases out of 22,927 live birth; however, including the size at birth increased the validity of estimation; as for those with missing birth weight, birth size could be an appropriate proxy variable to indicate the birth weight.
The mortality indicators included three indicators: (a) child mortality was defined as the death of a child before the age of 5 years (0 to 59 months), (b) infant mortality was defined as death within the first year of life, and (c) neonatal mortality was defined as death within the first month of life.
Covariates
Covariates included the sociodemographic characteristics of births to young women aged 15 to 49 years consisting of maternal and child factors. Maternal demographic included age (continuous in years), education (no education, primary, secondary, or higher), place of residence (rural or urban), wealth index (poor, middle, or rich), ethnicity (Pashtun, Tajik, Hazara, Uzbek, Turkman, Nuristani, Baloch, Pashai, or other), age at marriage (<18 or ≥18), and the number of ANC visits (<4 times or ≥4). Child-specific demographics included age (continuous in years) and sex (male or female).
Statistical Analysis
To estimate the prevalence of IPV and its associated sociodemographic factors among married women aged 15 to 49 years, the analysis included the women aged 15 to 49 years who were selected for the IPV module in ADHS (2015) (n = 24,070), and to estimate the morbidity and mortality of children and its association with IPV, the children born in the past 5 years by married women aged 15 to 49 years, who were selected for IPV module were included (n = 22,927). Since we have a large dataset and less than 10% of cases had missing data for included variables, the missing data were treated case-wise (Langkamp et al., 2010) assuming data are completely missing at random across the dataset.
The descriptive statistics described the distribution of women’s sociodemographic characteristics (Table 1) and estimated the prevalence of different types of IPV (Table 2). Binary logistic regression was employed to estimate the odds of IPV across different sociodemographic characteristics (Table 1), as well as the odds of morbidity and mortality across the different types of IPV, before and after adjustment for maternal and child’s sociodemographic factors (Table 3). Adjusted models for diarrhea, ARI, and fever outcomes included only the living children under 5 years and accounted for the age of child, sex of child, maternal age, maternal education, place of residence, wealth index, and ethnicity. Adjusted models for child mortality indices, low birth size, and low birth weight included all the births in the past 5 years and accounted for sex of child, maternal age, maternal education, place of residence, wealth index, and ethnicity.
The Distribution of Sociodemographic Characteristics and Their Association With IPV.
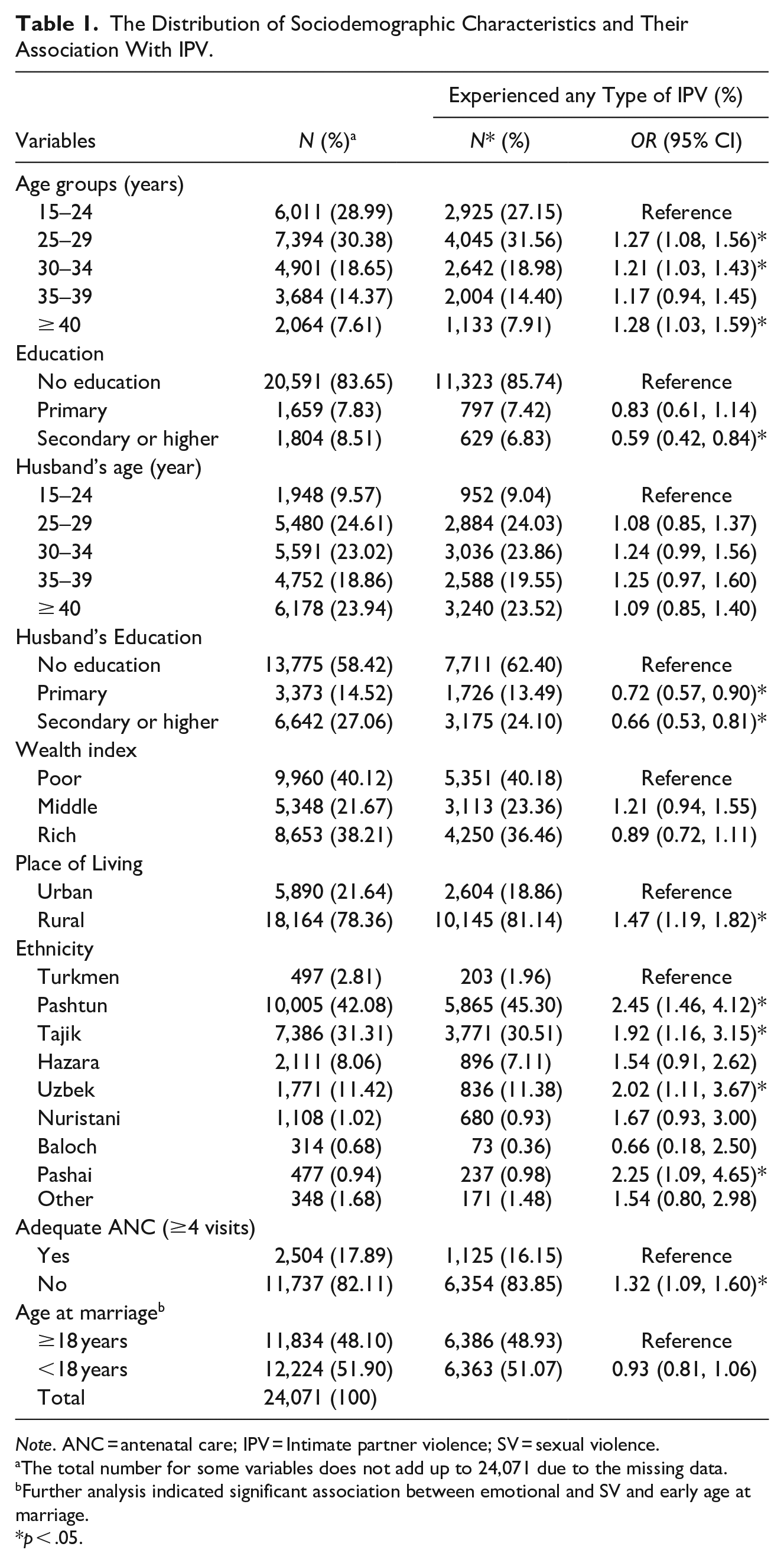
Note. ANC = antenatal care; IPV = Intimate partner violence; SV = sexual violence.
The total number for some variables does not add up to 24,071 due to the missing data.
Further analysis indicated significant association between emotional and SV and early age at marriage.
p < .05.
Prevalence of the Different Components of Spousal Violence.
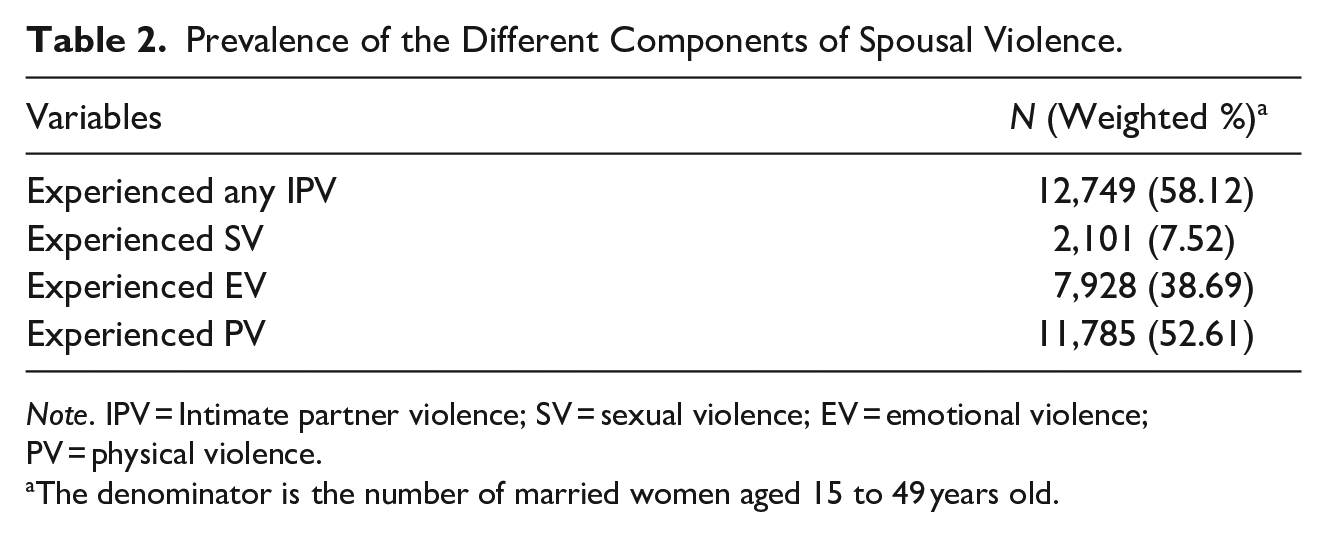
Note. IPV = Intimate partner violence; SV = sexual violence; EV = emotional violence; PV = physical violence.
The denominator is the number of married women aged 15 to 49 years old.
The Prevalence and Association of Child Morbidity and Mortality, Birth Weight and Size With Different Types of IPV.
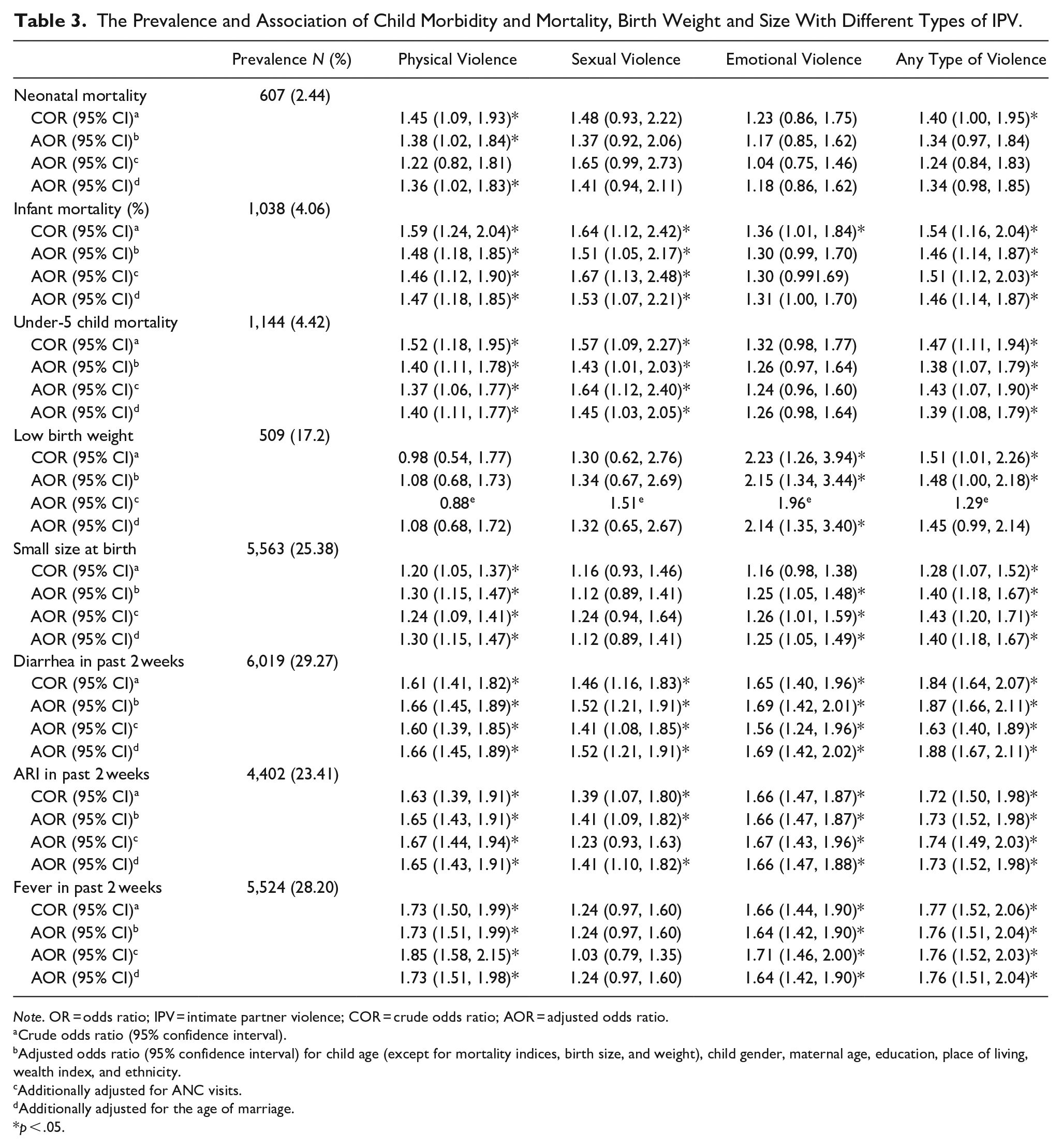
Note. OR = odds ratio; IPV = intimate partner violence; COR = crude odds ratio; AOR = adjusted odds ratio.
Crude odds ratio (95% confidence interval).
Adjusted odds ratio (95% confidence interval) for child age (except for mortality indices, birth size, and weight), child gender, maternal age, education, place of living, wealth index, and ethnicity.
Additionally adjusted for ANC visits.
Additionally adjusted for the age of marriage.
p < .05.
In addition to the mentioned covariates, a separate model was built to account for the impact of antenatal visits, examining the effect of IPV type on child morbidity and mortality indices beyond the attributable influence of sociodemographic inequalities, including the inadequate number of antenatal visits during pregnancy. Given the current evidence indicating lower age at marriage could increase the risk of maternal and child morbidity and mortality (Gortzak-Uzan et al., 2001; Olausson et al., 1999); therefore, additional models accounted for the effect of maternal age at marriage (Table 3).
All the analyses were performed using STATA version 14, and sampling weight and design were defined and accounted for using the STATA command “svy” in all analyses. Results were presented as OR and adjusted odds ratio (AOR) with 95% confidence intervals (95% CI). A p-value < .05 was considered to be statistically significant.
Ethical Consideration
The data used in this study could be accessed upon a reasonable request from the DHS website and are publicly available. The ethical necessities for data collection were sought and assured by the institutions that commissioned, funded, or managed the surveys. All DHS are reviewed and approved by ICF International and Institutional Review Board of Ministry of Health in the target country to ensure that the protocols comply with the U.S. Department of Health and Human Services regulations for the protection of human subjects. Therefore, this study did not require further ethical approval.
Results
Sociodemographic Characteristics of Married Women Aged 15 to 49 Years, Selected for IPV Module in ADHS (2015)
As Table 1 illustrated, the majority of married women (30.38%) selected for the IPV module were in the 25 to 29 years age group, and less than 10% were in the age group ≥40 years. Approximately two-thirds of these women were illiterate and living in rural areas and were either from Pashtun or Tajik ethnic backgrounds. Almost half of the husbands were in the age group 25 to 35, and more than half of them had no education. More or less, 40% of women belonged to either poor (40.12%) or rich (38.12%) households. More than half of these women married at ages less than 18 years as a minor, and less than one-fifth received adequate ANC (≥4 visits) during their last pregnancy.
The Association Between the Sociodemographic Attributes and IPV Among Married Women Aged 15 to 49 years, Selected for the IPV Module in ADHS (2015)
Approximately a quarter (27.15%) of married women aged 15 to 49 years who experienced IPV were from the age group 15 to 24 years, indicating that older age groups are more likely to experience spousal violence compared to this age group (Table 1). In addition, there was a higher level of illiteracy in both women who experienced IPV (85.74%), and their husbands (62.40%); and husbands (OR: 0.66; 95% CI: 0.53, 0.81) and wives (OR: 0.59; [0.42, 0.84]) of higher education were less likely to engage in the violent experience. More than two-thirds of women with IPV experience were living in rural areas (81.14%), and it appeared that living in rural areas could substantially increase the likelihood of IPV (OR = 1.47; [1.19, 1.82]). There was no significant association between the household economic status and exposure to IPV, and the majority of women in both groups belonged to either poor or rich households. Almost three-quarters of women with IPV experience were from Pashtun (45.50%) or Tajik (30.51%) ethnic backgrounds, and Pashtun (OR = 2.45; [1.46, 4.12]), Tajik (OR = 1.92; 2.45; [1.16, 3.15]), Uzbek (OR = 2.02; [1.11, 3.67]), and Pashai (OR = 2.25; [1.09, 4.65]) ethnic groups were more likely to suffer from IPV compared to the reference group (Turkmen). It appeared that IPV is more prevalent among those who had inadequate ANC (83.85%), and those with inadequate ANC are more likely to be a victim of partner violence (OR = 1.32; [1.09, 1.60]). There was no significant association between the age of marriage and IPV among women selected for the IPV module in ADHS (2015)
The Prevalence and Association of Different Types of IPV With Morbidity and Mortality of Children Under-5 Born to Married Women Aged 15 to 49 Years, Selected for the IPV Module in ADHS (2015)
More than half (58.12%) of the married women aged 15 to 49 years suffered from spousal violence at least once in the past 12 months. The prevalence of PV, EV, and SV was 52.61%, 38.69%, and 7.52%, respectively, in married women aged 15 to 49 years in the study sample.
The neonatal mortality rate of births to married women aged 15 to 49 was 2.44%. It appeared only the babies of women who suffered from PV are more likely to die within the first month of life, before (COR] = 1.45; 95% CI: 1.09, 1.93) and after (AOR = 1.38; [1.02, 1.84]) adjustment or sociodemographic inequalities and maternal age at marriage. However, this association disappeared after adjustment for the number of ANC visits (AOR = 1.22; [0.82, 1.81]). There was also a significant association between neonatal mortality and experiencing any type of spousal violence in the unadjusted model (COR = 1.40; [1.00, 1.95]), which became insignificant in adjusted models.
The overall infant mortality rate was 4.06%, and the odds of dying in the first year of life were significantly higher among the children born to mothers who suffered from any type of spousal violence (physical, emotional, or sexual). Adjusting for sociodemographic inequalities, maternal age at marriage, and the number of ANC visits did not change the strength of this association except for EV, which became insignificant in adjusted models (Table 3).
The mortality rate was 4.42% among the children under-5 born to women aged 15 to 49 years included in this study. Except for EV (COR = 1.32; 95% CI: 0.98, 1.77), there was a significant association between exposure to all types of IPV and children under-5 mortality in both unadjusted and adjusted models (Table 3).
Approximately 17.2% of the children under 5 born to mothers aged 15 to 49, who were selected for the IPV module in ADHS (2015) suffered from low birth weight (<2,500 g). Although the odds of low birth weight were significantly higher among the babies born to mothers who suffered from any type of IPV in both adjusted and unadjusted models, it only remains significant among those with a mother who endured EV in extended analysis. Moreover, the calculation of standard errors was not possible in the model adjusted for the number of ANC visits because of the stratum with a single sampling unit.
Almost a quarter (25.38%) of the babies were reported by mothers to be either small or very small at the time of birth, and except for SV, the babies of mothers with other spousal violent experiences (physical and emotional) were more likely to be small/very small at birth in adjusted models (Table 3).
The prevalence of diarrhea, ARI, and fever in the past 2 weeks was 29.27%, 23.41%, and 28.20% among the children under 5 born to married women aged 15 to 49 years, selected for the IPV module in ADHS (2015). The children under 5, whose mothers suffered from at least one type of spousal violence, were more likely to suffer from these morbidities in both adjusted and unadjusted models (Table 3), except for fever in children of mothers with SV experience (AOR and COR = 1.24; p > .05)
Discussion
The findings indicated that more than half of the married women aged 15 to 49 years in Afghanistan experienced at least one type of spousal violence in their lifetime; with PV being the lead, followed by EV and SV. Similar findings have been documented in previous studies in Afghanistan (Dadras, Nakayama, et al., 2022) and the UNICEF reports (UNICEF, 2021). Not surprisingly, in a country where child marriage is a rampant practice (Dadras, Khampaya, et al., 2022) and gender cultural norms encourage violence against women and girls, the risk of IPV exposure is expected to be high. Consistent rates have been observed in similar settings with common roots and cultures such as Pakistan (Ali et al., 2015; Murshid & Critelli, 2020). Despite enormous efforts and human rights advocacy in the last decades, Afghan women are still experiencing spousal violence in several manners and are in dire need of support to be empowered in order to overcome the obstacles and be represented and treated more equally in Afghan society.
In this study, women of older age groups were more likely to suffer from spousal violence compared to the youngest age group (15 to 24 years), regardless of their husband’s age. This could be either due to the higher women empowerment of young women as a result of higher education and enhanced awareness of their rights that prevent IPV (Dadras, 2022), or the fear of bitter consequences sustained by an abusive partner and not willing to participate in the survey, either need to be addressed in future studies. It has been shown that most young Afghan brides are accompanied by their husbands or family members to the facilities in which the survey had been conducted and disclosure of a violent exposure experience could be fearful and threatening for them and thus, they do rather avoid participating in the survey (Dadras et al., 2020, 2021). This study also found that women with lower literacy were more prone to partner violence. These findings are in line with previous studies in which education has been noted as a key predictor of spousal violence against women (Alebel et al., 2018; Dadras, Nakayama, et al., 2022; Weitzman, 2018). It also appeared that living in rural areas could increase the likelihood of IPV regardless of the socioeconomic status and marriage age of our study participants. This has been attributed to the lower education and poverty in rural areas (Dadras, Nakayama, et al., 2022; Moffitt et al., 2020), even though no association was observed between socioeconomic status and IPV exposure in our study. Therefore, providing safety nets and shelter for the victims abandoned or fleeing the violence in remote underprivileged areas is vital to ensure the physical and mental health integrity of the survivors. It is crucial for healthcare providers to be aware of the potential risks associated with IPV and to take steps to screen and intervene when appropriate in order to help prevent further harm.
Another notable finding in this study was the higher likelihood of experiencing spousal violence among those who had less access to ANC, reflecting upon the strong association between adequate access to maternity care and the chance of IPV exposure in Afghan women. It has been shown that the majority of Afghan women, who are exposed to spousal violence, lack the authority to make decisions and are unable to negotiate their reproductive needs as a result of the husband’s abusive power (Dadras, Nakayama, et al., 2022). Although it is an obvious violation of women’s rights, it has been ignored for several years. This has been dismantling all the efforts that have been made by women’s rights advocates to empower Afghan women for decades and are mainly rooted in the man-dominant values and norms of Afghan society that approve the proxy decision-making by men in the household concerning the reproductive needs of women cohabited with them. Given the recent turn of power and provoked antifeminism activities of the incumbent government, a strong and sustainable human rights campaign engaging all relevant stakeholders is a need to mitigate the current situation and ensure the safety and health integrity of Afghan women and their offspring.
A growing body of literature demonstrated that IPV in man-dominant societies could interfere with women’s ability to meet basic reproductive needs and could harm the health of newborns and living children (Bair-Merritt et al., 2006; Barnett et al., 2021; Silverman et al., 2006b). Several parameters, such as child immunization and exclusive breastfeeding, could be influenced by IPV, and the mothers who experience IPV may not be able to fully meet the nutritional and developmental needs of the newborn; thus, this could compromise the health of the child and lead to irreversible adverse outcomes and long-term morbidities and even death (Ariyo & Jiang, 2021; Bair-Merritt et al., 2006; Silverman et al., 2006a). Likewise in our study, the children under 5 born to mothers exposed to spousal violence were more likely to suffer from early death, low birth weight, and morbidities such as diarrhea, ARI, and fever in the last 2 weeks. However, adjustment for the number of ANC received during pregnancy diminished some of these associations. This emphasizes the key role of adequate maternity care in shaping the offspring’s health, and the programs and intervention should be directed more toward enhancing access to maternity care for women who experience IPV through sustainable and secure measures by which the women could be protected from further harm. Moreover, it has been suggested that the nutrition of women and their children could significantly be influenced by IPV; literature indicates poor food-seeking behaviors and limited access to nutritional supplements among victims owing to the abusive behavior of their husbands, and this may lead to malnutrition in women and thus their children (Desta et al., 2021; Ferdos & Rahman, 2018; Ziaei et al., 2014). In addition, maternal malnutrition may lead to low birth weight and smaller size at birth, which increase the mortality and morbidity of the newborn (Chai et al., 2016; Mondal & Paul, 2020). Despite all available evidence reflecting upon the potential reasons for higher morbidity and mortality among the children of women who experience IPV, the sequence of events and exact mechanisms are yet to be investigated in future studies and should be a priority for research funding institutes to maintain the efforts bringing insight into the potential mechanisms through which IPV could threaten the health of mother and child. Meanwhile, the policy and interventions should target the underlying causes of child mortality and morbidity in Afghanistan and adapt to the needs of Afghan women and children to reduce the adverse impact of IPV on child health. More importantly, screening for IPV as an important predictor of child morbidity and mortality should be incorporated into maternity and child care programs in Afghanistan, and necessary protective measures and sheltering for victims should be established in a safe environment through international collaboration and human rights advocacy.
Limitations
The findings of the present study should be interpreted in light of several limitations. The sociocultural sensitive concerns and gender-based inequalities existing in Afghan society bring about a substantial fear of disclosure among women who experience IPV; therefore, there is an elevated risk of nonparticipation and socially desirable responses that could bias the results toward null and underestimation of IPV prevalence, particularly among more vulnerable and underprivileged groups. In addition, the cross-sectional design of the study limits the ability to draw causal inferences between IPV and child morbidity and mortality. Including only the households in which husbands and wives were currently living together may have led to excluding the severe case of IPV that have been expelled or abandoned by their husbands as well as those who fled from the household and lived in alternate facilities and shelters; this could also push our results toward the null. Finally, assessing the children’s nutritional status was not possible based on the collected data from mothers; it is well known that nutritional deficiency compromised the child’s immune system and increases the vulnerability to microbial infection manifesting as diarrhea, ARI, and feverish illnesses (Ackerson & Subramanian, 2008; Al-Zangabila et al., 2021; Khan et al., 2019). Future studies should focus on these nutritional deficiencies and underlying reasons to address the potential adverse health outcomes. Despite all these shortcomings, there are some strengths to this study. First and foremost, to the best of our knowledge, it is the first study that addressed the impact that IPV could have on morbidity and mortality among children under 5. Moreover, unlike previous studies (Ahmed et al., 2006; Jejeebhoy, 1998; Rico et al., 2011), we separated the study population into two groups: first, all the women aged 15 to 49 years who were selected for the IPV module to estimate the IPV prevalence and its sociodemographic factors; and second, the children born to these women to estimate the prevalence of child morbidity and mortality indices and to examine its association with IPV exposure. However, previous studies suffered from selection bias as they only included women who had a child in the past 5 years and this could bias the estimation of IPV and its associated factors (Ferdousy & Matin, 2015; Silverman et al., 2009).
Conclusion
The findings emphasized the elevated risk of morbidity and mortality among children under 5 born by mothers aged 15 to 49 years who were exposed to IPV in Afghanistan. A high rate of spousal violence was observed among Afghan women driven mainly by illiteracy, particularly in rural areas. This calls for immediate action, formulating interventions and protective measures to reduce IPV among Afghan women. Incorporating the screening for IPV in maternity and childcare could be the first and foremost step in achieving this goal. Furthermore, women’s right advocate and campaigns should strive to communicate the message to the international community and health organizations and engage all stakeholders to develop policies and interventions providing the necessary support for women who experience IPV by implementing the appropriate protective measures, expanding the safety net, and providing shelter for fleeing or abandoned victim in a safe and secure environment. Further studies are recommended to advance the knowledge concerning the potential mechanisms through which IPV could affect the child’s and mother’s health.
Footnotes
Acknowledgements
We would like to express our utmost gratitude to the librarians at the library of the University of Bergen for providing technical support to prepare and submit this manuscript.
Authors’ Contribution
Both OD, MH, and FD wrote the research protocol and contributed to the data analysis and writing the manuscript.
Author’s Note
Omid Dadras is also affiliated to Western Norway University of Applied Sciences, Bergen, Norway.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The study was performed in accordance with relevant guidelines and regulations (U.S. Department of Health and Human Services regulations for the protection of human subjects). In addition, this survey was approved by the Institutional Review Board (IRB) of the Afghanistan Ministry of Health (MoH). An informed verbal and written consent was obtained from all the participants/guardians/parents before the interview. We also sought permission from the DHS website and filled out a request to access and download the data. Therefore, further ethical approval to use the data is not necessary.
Availability of Data and Material
The DHS questionnaire that collected the data in Afghanistan’s demographic and health survey in 2015 could be downloaded from DHS’s official website (![]() ). The dataset (ADHS, 2015) that was used in this study could be available upon a reasonable request by a registered user and with permission from the DHS website.
). The dataset (ADHS, 2015) that was used in this study could be available upon a reasonable request by a registered user and with permission from the DHS website.