
Abstract
Many women and men experience intimate partner violence (IPV) during their lifetime. However, only relatively few people actually seek formal help after such an experience. The current study applied the mediated-moderation model of self-compassion and stigma that has previously been used to explain men’s help-seeking behavior for depressive symptoms. The current study analyzed whether conformity to masculinity ideologies (CMI), self-stigma, and self-compassion were related to women’s and men’s intention to seek formal help after IPV experiences. A cross-sectional online questionnaire study was conducted with 491 German-speaking participants (65.8% women/34.2% men; age: M = 36.1 years; SD = 14.2). Participants read three vignettes about experienced IPV and then indicated how likely they would be to seek medical or psychological help if they were in the main character’s situation. Additionally, the Conformity to Masculine Norms Inventory, Self-Stigma of Seeking Help Scale, and Self-Compassion Scale were used. Separate manifest path models for women and men revealed that strong CMI was linked to strong self-stigma in women and men. In turn, strong self-stigma was linked to weak intentions to seek formal help after IPV experiences. In men, strong self-compassion weakened (i.e., “buffered”) the link between CMI and self-stigma. However, direct associations between strong CMI and weak intentions to seek formal help remained, especially for those participants with strong self-compassion. The current study adds to the existing literature on associations between CMI, self-compassion, and self-stigma by showing that those links are also relevant in women. However, self-compassion might not always act as a “buffer” and mediators that explain links between strong CMI and weak intentions to seek formal help in people with strong self-compassion need to be found in future studies.
Keywords
Introduction
Intimate partner violence (IPV) is the intentional use of force or power against a current or former intimate partner and can be classified as physical violence (i.e., physical force that inflicts pain), psychological violence (i.e., behaviors intended to humiliate or control another individual), or sexual violence (i.e., any sexual act against a person using coercion or force) (WHO, 2010). A considerable proportion of the population is affected by IPV over their lifetime (WHO, 2021), whereby women are more often affected by IPV than men (e.g., Schlack et al., 2013). Even though many people experience IPV, only relatively few people actually seek psychological or medical help after such experiences (Martin et al., 2023). Women have been reported to more often seek help after experiences of IPV than men (e.g., Martin et al., 2023).
Past research on men’s reluctance to seek formal help focused on their conformity to masculinity ideologies (CMI) and self-stigma as barriers or self-compassion as potential facilitator (Booth et al., 2019; Cole & Ingram, 2020). The current study uses the IPV stigmatization model (Overstreet & Quinn, 2013) and a mediated-moderation model of self-compassion and stigma (Wong et al., 2019) to investigate whether CMI, self-stigma, and self-compassion were related to women’s and men’s intention to seek formal help after IPV experiences.
Women’s and Men’s Help-Seeking Behavior After IPV
Women experience IPV more often than men (Schlack et al., 2013). Therefore, the focus of many large-scale prevalence studies and reports concentrate on women’s IPV experiences (European Union, 2014; WHO, 2021). Globally, one in four women experiences physical and/or sexual violence from an intimate partner at least once in her lifetime (WHO, 2021). A large-scale study among women living in the European Union (EU) revealed that 22% of women living in Germany and 13% of women living in Austria had at least once experienced physical and/or sexual violence carried out by a current or past partner (European Union, 2014). Around 6% of women in Germany have experienced psychological violence perpetrated by their partners in the preceding 12 months (Lange et al., 2016).
A review of prevalence rates reported that 3% to 20% of men are affected by physical violence, 7% to 37% of men experience psychological violence, and 0% to 7% of men are targets of sexual violence committed by a current or previous partner (Kolbe & Büttner, 2020). In Germany, it has been reported that 1% of men had experienced physical violence exerted by a partner, and 3% had experienced psychological violence perpetrated by a partner within the past 12 months (Lange et al., 2016; Schlack et al., 2013).
Even though a substantial proportion of people experience IPV, people rarely seek psychological or medical help after such an experience (Martin et al., 2023). One study conducted in the United States reported that 55% of people who experienced physical, psychological, and/or sexual violence sought formal help after those experiences (Cho et al., 2020). In another U.S. study, 4% to 12% of participants reported that they had sought medical help after experiencing IPV, and 31% to 43% of participants said they had sought psychological help after experiencing IPV (Martin et al., 2023). Of the women who participated in a large-scale study in the EU, 15% to 22% reported that they had sought medical help after experiencing physical or sexual violence carried out by the current or past partner (European Union, 2014).
Many studies that compared women’s and men’s help-seeking behavior after experiences of IPV found that women are more likely than men to seek psychological or medical help after those experiences (e.g., Martin et al., 2023). For instance, in a study 29% of women as compared to 12% of men reported that they had sought medical help after experiencing physical and/or sexual violence committed by an intimate partner. Psychological help was sought by 35% of women and 16% of men after experiencing IPV (Ansara & Hindin, 2010). In Austria, it has been assessed that 21% of women and 20% of men who experience physical violence, 14% of women and 10% of men who experience psychological violence, and 11% of women and 5% of men who experience sexual violence seek medical help. Psychological help is sought out by 22% of women and 11% of men who sustain physical violence, 20% of women and 11% of men who experience psychological violence, and 16% of women and 3% of men who undergo sexual violence (Kapella et al., 2011).
Masculinity Ideologies, Self-Stigma, and Self-Compassion
The difference in women’s and men’s willingness to seek medical or psychological help is not only reported for help-seeking after IPV. Past research has consistently reported that men are overall less likely than women to seek medical or psychological help. One prominent explanation for men’s reduced willingness to seek formal help is men’s stronger CMI (Addis & Mahalik, 2003).
Masculinity ideologies are culturally defined standards or norms for male behavior (Pleck et al., 1993). Masculinity ideologies depict men as being confident, competent, successful, self-reliant, and as having high self-esteem. Additionally, men are expected to be physically strong and able to defend themselves. CMI often conflicts with seeking help for psychological or medical problems, especially if help-seeking necessitates the expression of fears, intimate emotions, or vulnerabilities (Addis & Mahalik, 2003).
Accordingly, men who are affected by IPV not only reported that they felt the experience of IPV conflicted with their ability to uphold masculinity ideologies (Hogan et al., 2022), but many men have also reported that they avoided or delayed seeking help after experiencing IPV because they attempted to conform to masculinity ideologies or because CMI felt like a barrier to help-seeking (Huntley et al., 2019).
One way in which CMI might influence help-seeking is the increased experience of self-stigma when seeking formal help (Arnocky & Vaillancourt, 2014). People who hold a stigma in relation to help-seeking have a poor opinion of people who need or seek help and perceive help-seeking to be something unacceptable. People with a strong self-stigma target those negative messages toward themselves in cases where they need or seek formal help (Vogel et al., 2006).
The IPV stigmatization model (Overstreet & Quinn, 2013) identifies self-stigma as an important barrier toward help-seeking after IPV experiences. The mediated-moderation model of self-compassion and stigma (Wong et al., 2019) incorporates the link between strong CMI and strong self-stigma in explaining men’s reluctance to seek formal help.
The mediated-moderation model of self-compassion and stigma (Wong et al., 2019) includes self-compassion, that is, the tendency to be kind toward oneself and take an understanding, nonjudgmental attitude toward one’s inadequacies and failures (Neff, 2003, 2023). Thereby, self-compassion is often seen as a “buffer” that might weaken the strong relationship between CMI and self-stigma (Heath et al., 2017; Wasylkiw & Clairo, 2018).
So far, the mediated-moderation model of self-compassion and stigma (Wong et al., 2019) has been applied to men, but not to women. However, women might also adhere to norms and standards described by masculinity ideologies (García-Sánchez et al., 2018; Zamarripa et al., 2003). Women’s CMI has been linked to stronger acceptance of IPV (McDermott et al., 2017). Furthermore, CMI in women was linked to a reduced willingness to seek formal help (McDermott et al., 2018). Thus, for women, too, self-stigma with regard to help-seeking can be a barrier to seeking formal help after IPV experiences (Alves-Costa et al., 2023; Lelaurain et al., 2017).
Aim of the Current Study
To date, most research on barriers to formal help-seeking after IPV experiences stems from North America, and more studies on this topic from the EU are needed (Lelaurain et al., 2017). The mediated-moderation model of self-compassion and stigma (Wong et al., 2019) has not been tested in women. Furthermore, the associations between CMI, self-stigma, self-compassion, and help-seeking intentions after IPV experiences have not been tested.
The current study addressed those gaps in the literature. Similar to previous studies on the links between men’s adherence to masculinity ideologies, self-stigma, and help-seeking for depression (Cole & Ingram, 2020; Mahalik & Rochlen, 2006), the current study used vignettes, that is, short depictions of hypothetical situations, to assess women’s and men’s intention to seek formal help after experiencing IPV. Thereby, the mediated-moderation model of self-compassion and stigma (Wong et al., 2019) was tested with regard to help-seeking after IPV experiences in a sample of German-speaking persons in the EU. Based on the model the following hypotheses were tested (see the figure in Supplemental Material S1):
Hypothesis 1 (H1): Strong CMI is linked to stronger self-stigma with regard to formal help-seeking after IPV experiences in women and men.
Hypothesis 2 (H2): Strong CMI and strong self-stigma are linked to reduced intentions to seek formal help after IPV experiences in women and men.
Hypothesis 3 (H3): Self-compassion weakens (i.e., “buffers”) the link between CMI and self-stigma in women and men.
Methods
Participants
For the analysis, responses from 491 participants were considered. The sociodemographic characteristics of the sample are shown in Table 1. Of the participants, 65.8% were women and 34.2% were men. On average, participants were 36.1 (SD = 14.2) years old. The majority of the participants had German nationality and identified as being heterosexual. Nearly half of the sample were single people and were employed in paid work. Similar numbers of participants had finished vocational training, had university entrance-level qualification, or had a university degree (Table 1).
Sociodemographic Description of the Sample.
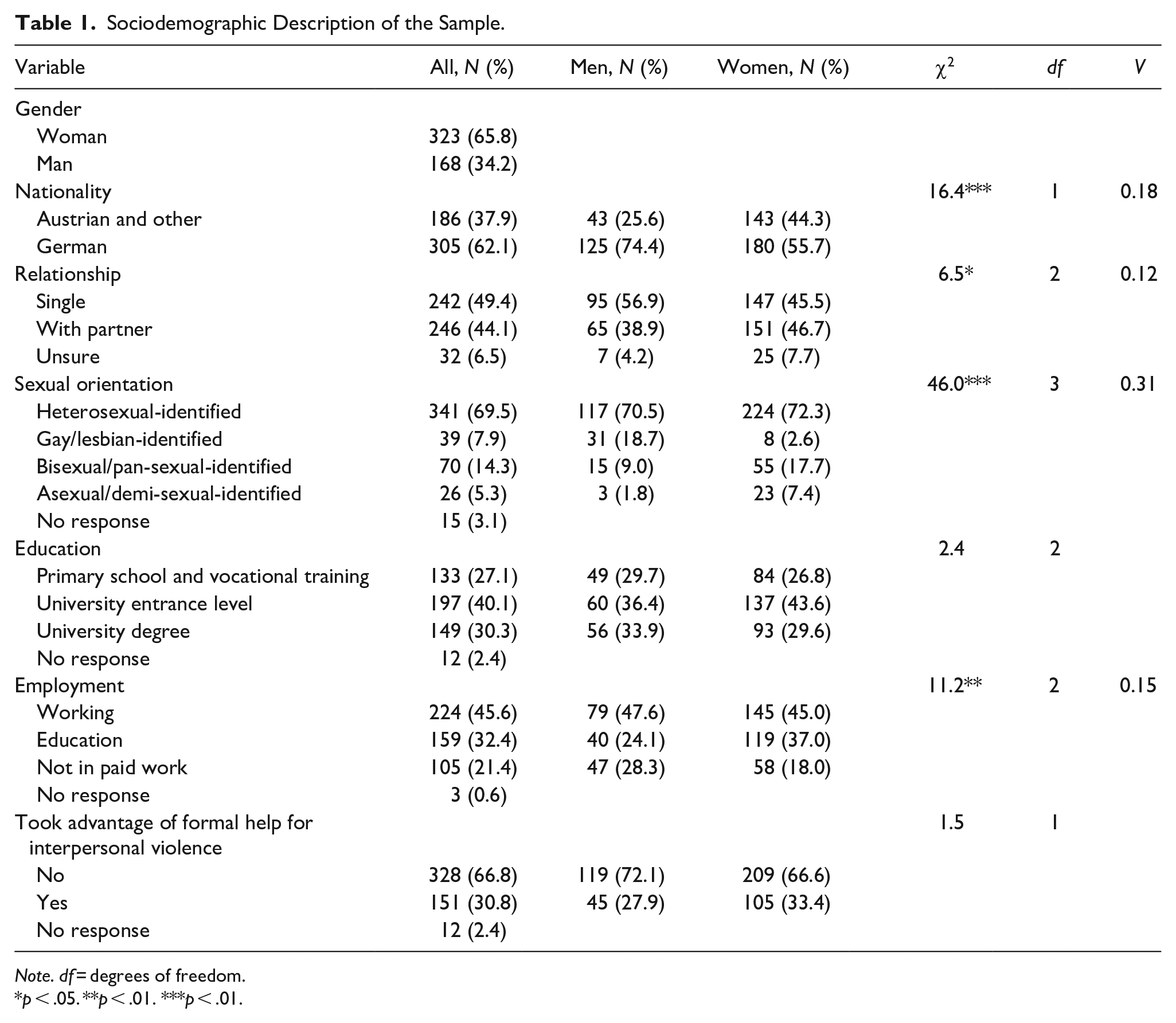
Note. df = degrees of freedom.
p < .05. **p < .01. ***p < .01.
Procedures
The study was conducted online from March 2021 to October 2021 and was hosted on SoSci: der onlineFragebogen (http://soscisurvey.de/). First, all students at an Austrian Medical University were invited by email to participate in the study. Second, the study was promoted with paid advertisement on Facebook. The paid advertisement targeted all persons over the age of 18 years living in Germany, Austria, and German-speaking regions of Italy. The email invitation and the paid advertisement informed that the current study was about help-seeking behaviors after having negative experiences. The link provided in the email invitation and the paid advertisement led to the first page of the questionnaire that more specifically revealed that the study’s purpose was to better understand help-seeking intentions after experiencing IPV.
Because women predominantly followed the invitation to participate, starting from June 2021 we targeted only men with the advertisement on Facebook. We halted recruitment after not receiving additional responses, while at the same time increasing the reach of the advertisement.
Participation in the study was voluntary and anonymous. Individuals did not receive any incentive for participating. Only after giving informed consent were participants able to access the questionnaire. The medical university’s Ethics Committee confirmed (on January 18, 2021) that under Austrian law the current study did not require formal approval by an Ethics Committee.
Measures
Sociodemographic information
Sociodemographic information was assessed with self-constructed questions about participants’ gender, age, sexual orientation, relationship status, highest level of education, employment, and nationality (Supplemental Material S2). For the analysis only participants who identified as women or men were considered because too few people with other identities participated. Because only few participants had Italian nationality (n = 33; 6.7%) and one participant (0.2%) had Turkish nationality, a new variable for nationality was formed, in which the two categories German nationality and Austrian and other nationalities were subsumed. A new variable for education was formed, in which secondary school (n = 61; 12.5%) and vocational training (n = 72; 14.7%) were summarized in one category. Finally, a new variable for employment was formed, in which the categories unemployed (n = 39; 7.9%), retired (n = 41; 8.4%), and parental leave (n = 8; 1.6%) were summarized in one new category, namely not in paid work.
Help-seeking intentions
The current study’s approach to assessing participants’ intention to seek formal help was informed by previous studies that assessed men’s potential responses when experiencing symptoms of depression (Cole & Ingram, 2020; Mahalik & Rochlen, 2006). Similar to the previous studies, the current study used vignettes, to describe a main character’s IPV experiences. Specifically, three vignettes, one about psychological, one about physical, and one about sexualized IPV, were presented (see all vignettes in the Supplemental Material S3).
The gender of the main character was identical to the participants’ indicated gender identity. After each vignette, participants were asked to imagine being in the described situation and to indicate how likely they would be to seek medical help or professional psychological help (Cole & Ingram, 2020). Because an uneven number of response categories was recommended, especially for questions where participants might be indecisive (Weijters et al., 2010), we used a 5-point Likert scale (1 = very unlikely; 5 = very likely) instead of the previously used 4-point Likert scale (Cole & Ingram, 2020; Mahalik & Rochlen, 2006). Mean scores across all responses were calculated. Higher scores indicated stronger intentions to formally seek help after IPV experiences. The previous study, which assessed formal help-seeking intentions of men for depressive symptoms, had an internal consistency of α = .92 (Cole & Ingram, 2020). In the current study, the internal consistency was α = .89 (Supplemental Material S4).
Self-constructed questions were used to ask participants whether they had sought medical help, psychological help, or other professional help at least once after own experiences of interpersonal violence (1 = no; 2 = yes). All participants who responded that they had used at least one formal help resource were coded as having availed themselves of formal help after experiences of interpersonal violence.
Conformity to masculinity ideologies
CMI was assessed with the 30-item short version of the Conformity to Masculine Norms Inventory (CMNI) (Mahalik et al., 2003). In comparison to the original version of the CMNI, theCMNI-30 items (CMNI-30) is considerably shorter, but still includes 10 of the original 11 scales. Furthermore, some items’ wording had been changed to improve item clarity and consistency (Levant et al., 2020). Participants were asked to respond on a 6-point Likert scale (1 = strongly disagree; 6 = strongly agree) whether statements describing behaviors or opinions that conform to masculinity ideologies apply to them. One example item read, “I will do anything to win.” The CMNI-30 has been validated only in men and has been shown to have satisfactory internal consistencies (most scales had α coefficients above .70) (Levant et al., 2020). For the current study, the German-language version of the CMNI-30 was used (Komlenac et al., 2023). A higher mean total score indicated stronger CMI with a satisfactory internal consistency in women and men (Supplemental Material S4; Ponterotto & Ruckdeschel, 2007).
Self-compassion
Self-compassion was measured with the German-language version (Hupfeld & Ruffieux, 2011) of the Self-Compassion Scale (SCD-D) (Neff, 2003). The questionnaire consists of statements describing possible reactions to difficult situations. Participants indicated on a 5-point Likert scale how often they reacted in the described manner (1 = almost never; 5 = almost always). For the current study, a scoring scheme, which summarized the 26 items in two scales, namely self-compassion and self-coldness, was used (Brenner et al., 2017). For this purpose, the self-coldness scale consisted of items assessing being self-judgmental, tending to feel alone, and being focused on and overwhelmed by negative emotions (e.g., “I’m intolerant and impatient towards those aspects of my personality I don’t like”). The Self-Compassion Scale measures the extent to which a person is kind to themselves, tries to balance and control upsetting emotions and realizes that other people share difficulties and negative feelings that are similar to one’s own (e.g., “I try to be understanding and patient towards those aspects of my personality I don’t like.”) (Brenner et al., 2017; Neff, 2003). The two scales, self-compassion and self-coldness, proved to have satisfactory internal consistencies (Coefficient omega hierarchical (ωH) >.84) (Brenner et al., 2017). In the current study, those scales also had satisfactory internal consistencies (αs >.90; Supplemental Material S4). Higher scores for self-compassion indicated higher levels of self-compassion, whereas higher scores for self-coldness indicated lower levels of self-coldness (Hupfeld & Ruffieux, 2011).
Self-Stigma of Seeking Help Scale
Self-stigma, hence the degree to which an individual’s self-esteem or self-worth is threatened by the prospect of needing professional help, was assessed with the Self-Stigma of Seeking Help Scale (SSOSH) (Vogel et al., 2006). For the current study, a revised seven-item version with satisfactory psychometric properties (αs = .87–.89) was used (Brenner et al., 2021). German-language items that were provided online were used (Vogel, 2020). In order to better assess self-stigma in relation to seeking medical help after experiences of interpersonal violence, the wording of items was changed. All phrases that referred to “psychological help” were changed to “medical help” or “physician.” Additionally, all phrases that referred to psychological problems were changed to “experiences of interpersonal violence” (e.g., “I would feel inadequate if I went to a physician for help after experiencing interpersonal violence.”). Participants were asked to indicate on a 5-point Likert scale their agreement or disagreement with the statements (1 = strongly disagree; 5 = strongly agree). In the current study, acceptable internal consistencies were obtained (Supplemental Material S4).
Lifetime experiences of violence
In order to measure cumulative lifetime experiences of interpersonal violence, the Cumulative Lifetime Violence Severity Scale was used (Scott-Storey et al., 2020). This scale assesses experiences of interpersonal violence during childhood (11 items) and adulthood (11 items). For each description of an experience of interpersonal violence (e.g., “Since the age of 18 I have been hit, kicked, slapped, burned, choked, or otherwise physically hurt by a caregiver or family member [other than a partner]”), participants indicated how often (1 = never; 5 = often) they had experienced such a situation. Additionally, they indicated how distressed they were (1 = not at all distressed; 5 = very distressed) by each experience of interpersonal violence they had at least rarely experienced. One mean score across all frequency and distress items was calculated for each participant, indicating the frequency and/or severity of cumulative lifetime experiences of interpersonal violence. The original Cumulative Lifetime Violence Severity Scale was validated in men and proved to have satisfactory internal consistencies (αs = .78–.86) (Scott-Storey et al., 2020). For the current study, all items were translated from English to German with the forth-and-back procedure (Brislin, 1970). The total score showed satisfactory internal consistencies (Supplemental Material S4).
Statistical Analysis
Descriptive statistics, chi-square tests, and t-tests were performed to determine average responses of participants and to compare responses between women and men. Correlation analyses were performed to calculate the bivariate relationships between the studied variables.
To test the current study’s hypotheses, two manifest path models, one for women and one for men, were calculated. Those models were calculated with the PROCESS macro (Hayes, 2018; https://www.processmacro.org) for SPSS. For the current analysis, SPSS for Windows, version 26.0 (IBM Corp., Armonk, NY, USA) was used. Model 10 of the PROCESS macro (Hayes, 2018) was chosen with bootstrap bias-corrected 95% confidence intervals (bootstrap sample was n = 5,000). Significant results were indicated when p ≤ .05 or when 95% confidence intervals did not include zero.
The calculated model is shown in the Supplemental Material S1. In each manifest path model, intention to seek formal help (variable Y) was predicted by self-stigma (mediator, variable M), and CMI (variable X). Self-coldness (variable W) and self-compassion (variable Z) were entered as moderators for the link between CMI and intention to seek formal help and the link between CMI and self-stigma. In all analyses, the control variables age, nationality, relationship status, sexual orientation, education, employment, own past formal help-seeking, and own experiences of interpersonal violence were considered.
In total, 1,265 persons gave informed consent and opened the online questionnaire. Of those participants, 704 participants were excluded because they gave wrong responses to two attention-check items (“Please select the response ‘Agree’”) (Huang et al., 2012). Furthermore, 23 participants stopped filling out the questionnaire before reaching the end. Two participants were excluded because they gave an unrealistic age (above3,232), and two participants indicated being younger than 18 years. Additionally, six participants did not reveal their age. There were too few nonbinary persons (n = 22; 4.2%), trans men (n = 4; 0.8%), inter* persons (n = 1; 0.2%), or people with a different gender (n = 6; 1.1%) to include them in the statistical analysis. Four people did not indicate their gender and could therefore not be included in the analysis. Ultimately, 491 responses were used for the analysis.
From previous research (Booth et al., 2019), links between CMI and self-stigma or links between self-stigma and intentions to seek formal help were expected to be medium in effect size (Cohen, 1992). For such effects to be detected in manifest path models with the use of bias-corrected bootstrap coefficients, a minimum sample size of n = 148 is suggested (Fritz & Mackinnon, 2007). In the current study, the sample size for women (n = 323) and for men (n = 168) satisfies this requirement.
Results
Descriptive Statistics
Overall, participants reported few incidents of own experiences of interpersonal violence (Supplemental Material S4). Nearly one-third of the participants reported having at least once sought out formal help after experiencing interpersonal violence (Table 1). After reading the vignettes about the main character experiencing different forms of IPV, participants reported that they would be moderately likely to seek formal help if they were in the main character’s situation (Supplemental Material S4).
In general, participants did rather not conform to masculinity ideologies, whereas men reported conforming to those ideologies more often than women (Supplemental Material S4). Participants reported moderate self-compassion and self-coldness. Thereby, women reported stronger self-coldness than men. Finally, the prospect of seeking medical help after experiences of interpersonal violence did rather not weaken participants’ sense of self-worth or self-esteem (Supplemental Material S4).
Correlations
All correlations between variables are reported in Supplemental Material S5. Participants with frequent and/or distressing experiences of interpersonal violence were more likely to have sought formal help after such experiences. Furthermore, having had frequent and/or distressing experiences of interpersonal violence was linked to stronger CMI, weaker self-compassion, stronger self-coldness, and stronger self-stigma.
Strong CMI was linked to weaker self-compassion and stronger self-coldness in women and men. Additionally, strong CMI correlated with strong self-stigma. Strong self-stigma was associated with weaker self-compassion and stronger self-coldness.
Help-seeking intentions after IPV experiences were stronger in older participants and those who had sought formal help after experiences of interpersonal violence in the past. Weak CMI, strong self-compassion, and weak self-coldness were linked to stronger intentions to seek formal help. Finally, strong self-stigma was associated with weaker intentions to seek formal help (Supplemental Material S5).
Mediation and Moderation Analysis
Women
All path coefficients of the manifest path model in women are reported in Table 2. Woman with German nationality and those who had experienced frequent and/or distressing experiences of interpersonal violence reported having stronger self-stigma than women with Austrian and other nationalities and women who had no or few experiences of interpersonal violence. Additionally, strong CMI and weak self-compassion were linked to strong self-stigma with regard to seeking medical help after experiences of interpersonal violence.
All Model Path Coefficients—Direct Associations.
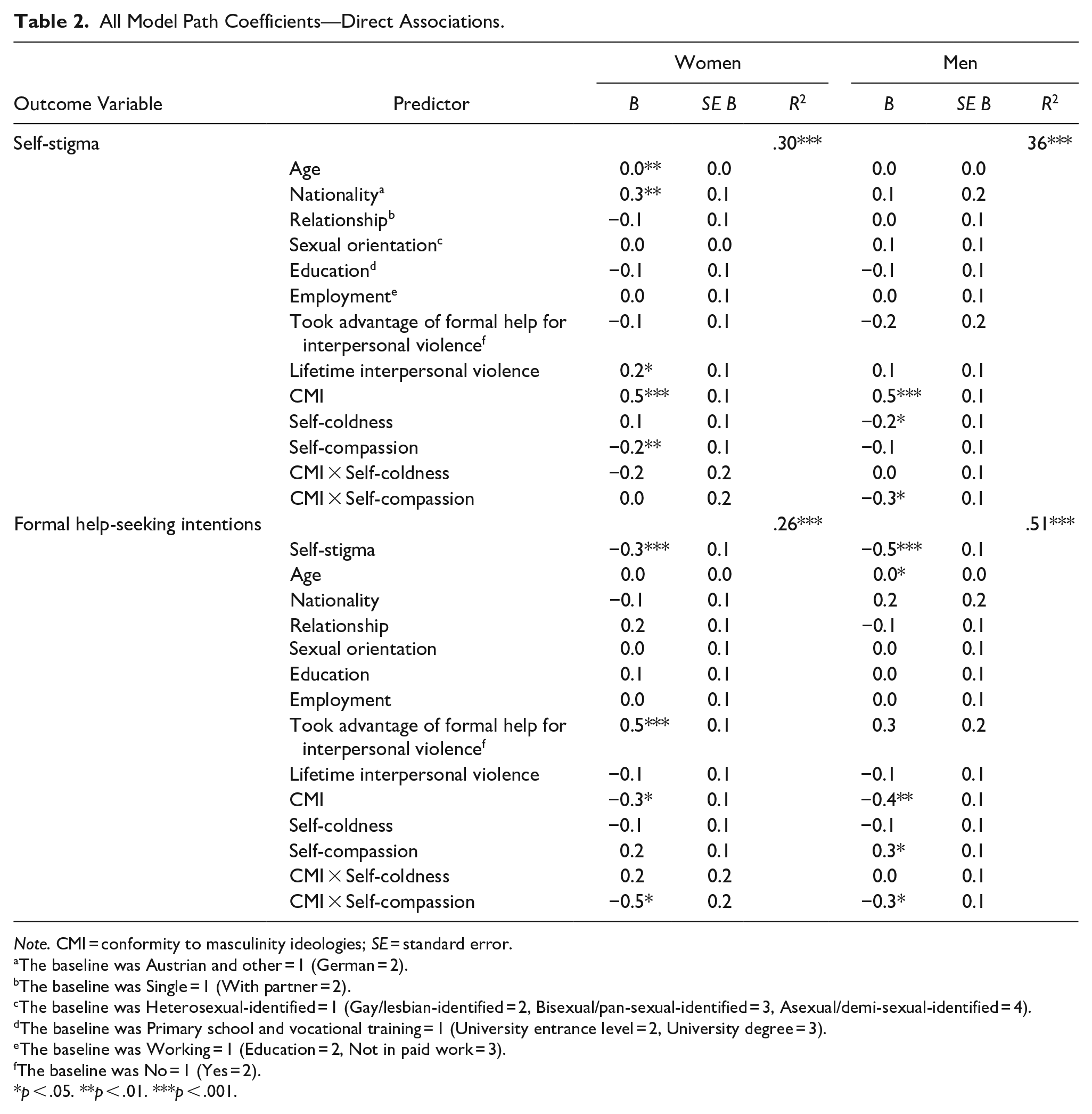
Note. CMI = conformity to masculinity ideologies; SE = standard error.
The baseline was Austrian and other = 1 (German = 2).
The baseline was Single = 1 (With partner = 2).
The baseline was Heterosexual-identified = 1 (Gay/lesbian-identified = 2, Bisexual/pan-sexual-identified = 3, Asexual/demi-sexual-identified = 4).
The baseline was Primary school and vocational training = 1 (University entrance level = 2, University degree = 3).
The baseline was Working = 1 (Education = 2, Not in paid work = 3).
The baseline was No = 1 (Yes = 2).
p < .05. **p < .01. ***p < .001.
Strong self-stigma in turn was linked to weaker intentions to seek formal help. Those women who took advantage of formal help in the past after experiencing interpersonal violence more often intended to seek formal help than women who did not seek help in the past. Self-compassion moderated the link between CMI and help-seeking intentions (Table 2). Strong CMI was especially linked to weaker intentions to seek formal help in women with strong self-compassion (bs = −0.8 to −0.5, ps = .012–.031). In women with weak self-compassion, CMI was not linked to the intention to seek help after IPV experiences (bs = 0.0–0.2, ps = .507–.800). Thereby, in women with weak CMI, those with strong self-compassion had stronger intentions to seek formal help than women with weak self-compassion (see figure in Supplemental Material S6). This difference between women with strong and weak self-compassion was not evident in women with strong CMI.
Finally, strong CMI was indirectly linked to weaker intentions to seek formal help after IPV experiences via self-stigma only in women with weak self-compassion and strong self-coldness. At other levels of self-coldness and self-compassion confidence intervals of indirect path coefficients included zero, thus were not significant (Supplemental Material S8).
Men
All path coefficients of the manifest path model in men are reported in Table 2. Men with strong self-coldness were more likely to have strong self-stigma than men with weak self-coldness. The significant interaction CMI × self-compassion indicated that strong CMI was especially linked to strong self-stigma in men with weak self-compassion (bs = 0.7–0.8, ps ≤ .001). In men with strong self-compassion, CMI was not linked to self-stigma (bs = 0.3–0.3, ps = .069–.275).
Strong self-stigma in turn was linked to weaker intentions to seek formal help. Self-compassion moderated the link between CMI and help-seeking intentions (Table 2). Strong CMI was especially linked to weaker intentions to seek formal help in men with strong self-compassion (bs = −0.7, ps = .002–.016). In men with weak self-compassion, CMI was not linked to the intention to seek help after IPV experiences (bs = −0.2 to −0.1, ps = .357–.360). Thereby, in men with weak CMI, those with stronger self-compassion had stronger intentions to seek formal help than men with weak self-compassion (see figure in Supplemental Material S7). This difference between men with strong and weak self-compassion was not evident in men with strong CMI.
Finally, strong CMI was indirectly linked to weaker intentions to seek formal help after IPV experiences via self-stigma only in men with weak self-compassion and strong self-coldness. At other levels of self-coldness and self-compassion confidence intervals of indirect path coefficients included zero, thus were not significant (Supplemental Material S9).
Discussion
The current study investigated barriers to and facilitators of formal help-seeking after IPV experiences in German-speaking women and men in the EU. Thereby, it was revealed that strong CMI was linked to stronger self-stigma with regard to formal help-seeking in women and men (H1). Strong self-stigma and strong CMI, in turn, were linked to weak intentions to seek psychological and/or medical help after IPV experiences (H2). Self-compassion was found to be a potential facilitator because strong self-compassion weakened (i.e., “buffered”) the link between CMI and self-stigma in women and men (H3).
Masculinity, Self-Stigma, and Help-Seeking
One explanation for people’s low willingness to seek psychological or medical help after IPV experiences (Martin et al., 2023) is people’s strong self-stigma with regard to help-seeking (Alves-Costa et al., 2023; Lelaurain et al., 2017). In line with the IPV stigmatization model (Overstreet & Quinn, 2013), in the current study especially those participants, who regarded needing or seeking help as something unacceptable or something that threatens their sense of self-worth (Vogel et al., 2006), had weaker intentions to seek formal help after IPV experiences. Thus, self-stigma can be seen as a barrier to formal help-seeking after IPV experiences.
The current study further revealed that CMI co-occurred with women’s and men’s strong self-stigma concerning formal help-seeking. People who try to conform to masculinity ideologies might perceive an incompatibility between being stoic, strong, independent, or invulnerable and needing help after IPV experiences, especially if help-seeking necessitates the expression of fears, intimate emotions, or admitting vulnerabilities (Addis & Mahalik, 2003). The current study’s results are in line with previous findings from qualitative studies. Many men have reported that they avoided or delayed seeking help after IPV experiences because they attempted to conform to masculinity ideologies or because CMI felt like a barrier to help-seeking (Huntley et al., 2019).
Previously, it has been shown that adherence to masculinity ideologies in women was linked to a reduced willingness to seek formal help for suicidal thoughts (McDermott et al., 2018). The current study adds that, similar to men, strong CMI in women is linked to strong self-stigma and in turn to low willingness to seek formal help after IPV experiences (Cole & Ingram, 2020). Thus, the current study adds support for the argument that it is relevant to understand how masculinity ideologies affect the lives of men and women (Whorley & Addis, 2006) and not to focus solely on men when studying masculinity ideologies.
Masculinity Ideologies and Self-Compassion
According to the mediated-moderation model of self-compassion and stigma (Wong et al., 2019), self-compassion, that is, being kind to oneself also when perceiving own inadequacies and failures (Neff, 2003), can weaken (i.e., “buffer”) the link between CMI and self-stigma. In line with the model, numerous studies have shown that self-compassion can moderate the association between CMI and self-stigma concerning help-seeking for psychological problems (Heath et al., 2017; Wasylkiw & Clairo, 2018). Thereby, in men with high levels of self-compassion the link between strong CMI and self-stigma for formal help-seeking was weaker than in men with high levels of self-compassion (Booth et al., 2019). The current study replicated those findings with regard to formal help-seeking after IPV experiences. Namely, only in men with weak self-compassion show strong CMI linked to strong self-stigma. The analysis of indirect path coefficients further revealed that strong CMI was linked to reduced intentions to seek formal help after IPV experiences via increased levels of self-stigma only in women and men with weak self-compassion and strong self-coldness.
The current study is unique in that it shows that strong self-compassion was linked to weaker self-stigma for formal help-seeking in women. Even though self-compassion is often discussed as “colliding” with the ability to conform to masculinity ideologies (Wasylkiw & Clairo, 2018) and most research on associations between self-compassion and self-stigma for formal help-seeking has focused on men (Heath et al., 2017; Wasylkiw & Clairo, 2018), on average, women and not men have lower levels of self-compassion (Yarnell et al., 2015). In the current study, this difference in levels of self-compassion between women and men also became evident. Therefore, the focus of research on the benefits of having high levels of self-compassion for formal help-seeking needs to shift to also include women. The current study revealed that having stronger self-compassion might go hand in hand with reduced self-stigma in women and men alike.
However, the analysis of direct links between CMI and intention to seek formal help revealed that self-compassion might not always act as a “buffer,” whereas in people with weak CMI strong self-compassion was linked to stronger intentions to seek formal help, this association was not evident in persons with strong CMI. Thus, CMI might be linked to reduced willingness to seek help, via other routes than self-stigma (e.g., devaluations and negative judgments of own needs for and use of formal help) (Wong et al., 2019). Other cognitive (e.g., appraisal strategies or benefit finding) and social (e.g., giving forgiveness or receiving social support) processes linked to self-compassion might mediate associations between CMI and intentions to seek formal help (Wong et al., 2019). Future studies that include cognitive and social processes are needed to explain the current study’s findings of direct links between strong CMI and weak intentions to seek formal help, which are especially prevalent in persons with strong self-compassion.
Implications
Similar to previous studies of the links between men’s CMI, self-stigma, and help-seeking for depression (Cole & Ingram, 2020; Mahalik & Rochlen, 2006), the current study shows that CMI was linked to reduced intentions to seek formal help after IPV experiences. Therefore, healthcare providers need to be sensitive to and understand consequences of cultural pressures to endorse and conform to masculinity ideologies (American Psychological Association, 2018). It has been recommended that the topic of masculinity ideologies and gender-sensitive treatment already be included in clinical practice training (Seidler et al., 2019) or medical education (Komlenac & Hochleitner, 2019). In this way, healthcare practitioners should become aware of their own gender-based attitudes and expectations. They should also be aware of and explore their patients’ endorsement of and CMI (Seidler et al., 2018). Healthcare practitioners may try to use their patients’ CMI to best advantage by reframing the healthcare situations in a way that promotes self-management, empowerment, accountability, and autonomy throughout treatment. In such healthcare settings, patients who strongly conform to masculinity ideologies might be able to utilize healthcare offers after experiencing IPV, whereas at the same time being able to maintain their sense of masculinity (Komlenac et al., 2020; Seidler et al., 2018).
The current study extends previous suggestions by fostering awareness for masculinity ideologies affecting the lives of men and women (Whorley & Addis, 2006). Even though, overall, women report lower levels of CMI (García-Sánchez et al., 2018; Zamarripa et al., 2003), women’s CMI is linked to women’s reduced willingness to seek formal help (McDermott et al., 2018). Therefore, it is recommended that patients’ endorsement of and CMI be explored in women and men and appropriate gender-sensitive approaches in clinical care be applied after IPV.
In addition to healthcare providers, other services such as social services or victim support organizations offer formal help to people who experience IPV. As is the case with healthcare services, a relatively small proportion of people seek out social services or victim support organizations after experiencing IPV (European Union, 2014). The current study’s findings and recommendations might be applicable to those services.
Because of the previous and current findings that self-compassion can weaken the association between CMI and self-stigma concerning help-seeking (Heath et al., 2017; Wasylkiw & Clairo, 2018), and self-compassion interventions might increase a person’s positive health behavior (Biber & Ellis, 2019). For instance, self-compassion interventions have been linked to higher levels of mindfulness and lower levels of self-criticism (Ferrari et al., 2019). Future studies are needed to develop strategies for how to target specific populations (e.g., adolescents, college students, clinicians, healthcare professionals, parents, and spouses) with such self-compassion interventions (e.g., workshops and online webpages) in order to help people access healthcare more easily when the need arises (e.g., after IPV experiences).
Limitations
The current study did not focus on participants’ actual help-seeking behavior, but provided participants with vignettes and assessed their intentions to seek formal help after IPV experiences. Vignettes seemed appropriate because they can model real-life decisions in specific contexts or situations. Additionally, vignettes are often used to study sensitive topics, they are nonpersonal and believed to elicit fewer socially desirable responses (Wallander, 2009).
The current study was conducted during the coronavirus disease 2019 (COVID-19) outbreak in Europe. On the one hand, an increased awareness for the importance of addressing mental health problems was evident during this period. On the other hand, many healthcare settings implemented infection-control measures by in part reducing outpatient appointments. Thus, increased awareness and higher demands for mental health services were not met with an increased availability of such services (Moreno et al., 2020). Some participants could have indicated no intent to seek formal help after IPV experiences because of the prospect of not easily receiving proper help during this time of high demand for psychological and medical health services.
The CMNI (Levant et al., 2020; Mahalik et al., 2003) and the Cumulative Lifetime Violence Severity Scale (Scott-Storey et al., 2020) were developed and originally validated for men only. The CMNI-46 proved to have at least partial metric invariance, indicating that factor loadings were similar across women and men (McDermott et al., 2018). However, further validation studies and stronger support for metric and scalar invariance are needed to increase the confidence that those scales measure similar constructs in women and men.
The cross-sectional study design precludes any conclusions of causality or the temporal order of found relationships. Future prospective, longitudinal, or experimental studies could address and prevent those limitations.
Lastly, some limitations of the current study’s sample need to be mentioned. One part of the current study’s results is based on a convenience sample of university students. Thus, the proportion of people with university entrance-level education and a university degree was relatively high in the current sample. Such a sample may significantly differ from other populations (Henrich et al., 2010). In general, studies with university students as participants find associations with larger effect sizes than studies with more general samples (Henrich et al., 2010). Finally, it was found to be difficult to recruit enough men for the current study. Some nonrespondents might especially uphold certain masculinity ideologies or be reluctant to seek help after undergoing IPV experiences (Näslindh-Ylispangar et al., 2008). Therefore, the reported intentions to seek help following IPV experiences might be an upper estimate, and the possibility to generalize results to a larger proportion of the population might be limited.
Conclusion
The current study revealed that self-compassion weakened (i.e., “buffered”) the strong link between high levels of CMI and high levels of self-stigma for seeking help after experiencing IPV. Self-compassion interventions might increase women’s and men’s positive health behavior including willingness to seek formal help after experiencing IPV (Neff, 2023). In contrast to previous studies about self-compassion and help-seeking that focused on men (Heath et al., 2017; Wasylkiw & Clairo, 2018), the current study highlights that especially women could benefit from such interventions, given that they reported lower levels of self-compassion in the current and previous studies (Yarnell et al., 2015).
The analysis of direct links between CMI and intention to seek formal help revealed that strong CMI was linked to a reduced intention to seek formal help, especially in persons with strong self-compassion. Namely, intentions to seek formal help did not differ among people with different levels of self-compassion when they strongly conformed to masculinity ideologies. In contrast, in people with weak CMI strong self-compassion were linked to stronger intentions to seek formal help. Future studies need to study other mediators in addition to self-stigma that might explain how CMI is linked to intention to seek formal help. In contrast to the route via self-stigma, for alternative routes, self-compassion might not act as a “buffer.”
Supplemental Material
sj-docx-1-jiv10.1177_08862605231169766 – Supplemental material for Not Always a “Buffer”: Self-Compassion as Moderator of the Link Between Masculinity Ideologies and Help-Seeking Intentions After Experiences of Intimate Partner Violence
Supplemental material, sj-docx-1-jiv10.1177_08862605231169766 for Not Always a “Buffer”: Self-Compassion as Moderator of the Link Between Masculinity Ideologies and Help-Seeking Intentions After Experiences of Intimate Partner Violence by Nikola Komlenac, Elisa Lamp, Franziska Maresch, Andreas Walther and Margarethe Hochleitner in Journal of Interpersonal Violence
Footnotes
Author contributions
NK, EL, FM, and MH designed the research. NK and MH collected the data. NK analyzed and interpreted the data. NK wrote the manuscript. AW critically commented the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This study was conducted as part of the second and third authors’ master’s theses.
Ethics Approval and Consent to Participate
The medical university’s Ethics Committee exempted the current study from full ethics review. The study was conducted in accordance with the Declaration of Helsinki (World Medical Association, 2013) and the APA standards (APA, 2002). All participants gave written informed consent.
Availability of Data and Materials
The datasets used and/or analyzed in the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.