
Abstract
Self-stigma is the internalization of widespread and negative attitudes around a devalued attribute. Being a victim of intimate partner violence (IPV) is a stigmatized identity, with IPV self-stigma is a potential barrier to help seeking. The lack of an IPV self-stigma scale limits current measurement of this latent trait; this study sought to fill this gap. We developed the IPV Internalized Self-stigma Scale (IPVIS) by revising existing self-stigma and devaluation/discrimination measures and adding new items to fill perceived gaps. Using an online survey, a diverse sample (N = 455, M = 39.51, SD = 12.03) with various relationship types (e.g., heterosexual, same-sex), IPV circumstances (e.g., male or female perpetrators/victims) and different gender and sexual identities was recruited. Participants first completed the item pool (44-items), followed by measures of IPV, anxiety, depression, social health, and self-efficacy with data analyzed using a multi-model approach (e.g., factor analysis, item response theory [IRT]). Factor analyses revealed one dominant factor; IRT analyses further refined the unidimensional item set. The final 11 items had high internal consistency, ω = .90, 95% CI [0.89, 0.91], and were highly informative with moderate to high discrimination levels. The IPVIS demonstrated measurement invariance by demographics, showing no differential item functioning by age groups, sex, residence (urban/suburban/rural), ethnicity (European/Caucasian vs. others), or relationship status (partnered/unpartnered). Initial validity examination revealed significant correlations between the IPVIS and related measures (e.g., depression, anxiety, social health). The IPVIS is suitable for research and has widespread clinical applicability. To the best of our knowledge, the IPVIS is the first scale developed that assesses IPV self-stigma inclusive of a diverse range of clients/participants, relationship types, and IPV circumstances.
Keywords
Intimate partner violence (IPV) can occur in any intimate relationship and is a pattern of behavior (i.e., physical, sexual, psychological, coercive) by a previous or current partner that causes harm (WHO, 2021). Approximately 30% of women and 20% to 30% of men experience physical or sexual violence (Breiding et al., 2014; Costa et al., 2015; Desmarais et al., 2012). In same-sex relationships and the LGBTQI+ community, the incidence of IPV is comparable, if not higher, than for female–male partnerships (Fedele et al., 2022; Gehring & Vaske, 2017). While these estimates are concerning, concealment of IPV can be common (Kennedy & Prock, 2018). Indeed, a recent Australian report estimated that less than 50% of women who have experienced IPV sought help (AIHW, 2019), suggesting that certain barriers to disclosure may exist.
One such barrier to IPV disclosure and help seeking is stigma, a phenomenon identified by Goffman (1963) whereby an individual is rejected by society due to possessing a so-called discredited attribute. Stigma can exist individually and at societal and institutional levels (Morris et al., 2018). At an individual level, when a person internalizes widespread and pervasive stereotypes and myths around the devalued attribute, this is conceptualized as self-stigma (Overstreet & Quinn, 2013). Self-stigma occurs when the person becomes aware of stereotypes and then agrees with those stereotypes (Bonfils et al., 2018). This type of stigma can also be anticipated in that the “discredited person” may expect the stigma believing that they will experience adverse social outcomes if they disclose their predicament. Therefore, stigma can compound the afflicted person’s problem and, in some instances, outweigh it (Morris et al., 2018).
While there is a plethora of research on self-stigma in connection with other maladies (e.g., mental illness, HIV), few have considered IPV (Crowe et al., 2019). Dominant and widespread stereotypes portray IPV victims as trapped, weak, and responsible for their situation, and gendered views of IPV (i.e., only women experience IPV at the hands of men, see Hine et al., 2020; Leung, 2019, for examples) have been common. These victim-blaming and gendered views mean many IPV victims are not afforded a legitimate victim status (Meyer, 2016). According to Christie (1986), people respond adversely to those struck by circumstances perceived as being within their control to handle. Many IPV victims are not seen as “ideal victims” as people believe they have the power to change their situation (e.g., why don’t they just leave?). Given that victim-blaming is associated with IPV stigma (Crowe et al., 2019), it is reasonable to conclude that being a victim of IPV is a stigmatized identity (Meyer, 2016).
Studies into IPV and stigma are scarce and limited by their methodology. For instance, Overstreet et al. (2017) examined stigma centrality (the importance/meaning of IPV to oneself) and IPV concealment finding that the more an individual internalizes stigma, the less likely they are to disclose IPV with the association (between centrality and concealment) a function of centrality. However, the stigma measure adapted for their study was not IPV-specific and lacked evidence of validity. Fedele et al. (2022) noted that stigma consciousness contributed to poorer mental health in 209 individuals who identified as women and had been sexually or psychologically victimized in a relationship with a woman. However, they examined the experience of stigma as a component of minority stress using a measure of anticipated stigma. Few studies have considered self-stigma (internalized and anticipated stigma) which is a significant knowledge gap in the literature.
Self-stigma is prevalent in sufferers of various psychiatric disorders (e.g., posttraumatic stress, bipolar) and is related to poorer social health (e.g., support, isolation), increased depression, anxiety, perceived labeling and secrecy, and less empowerment and self-efficacy (Bonfils et al., 2018; Boyd et al., 2003; Brown et al., 2010; Howland et al., 2016). However, a common limitation of the various studies is the adaptation of the Internalized Stigma of Mental Illness Scale (ISMIS) (Boyd et al., 2003) to the target group (e.g., Brown et al., 2010). Research requires demonstrably valid measurement and while these modifications may seem minor, the scale’s validity and reliability cannot be assumed to generalize to its various adaptions/revisions.
IPV research is also sometimes limited by a gendered view, that is heterosexual relationships with women as victims and men as perpetrators. While this focus has emanated from societal/cultural perceptions, increasingly, it is acknowledged that this is a narrow view of IPV (Gehring & Vaske, 2017). It is generally acknowledged that predominantly women are victims and men perpetrators of IPV (CDC, 2022). However, IPV can occur in any relationship, is sometimes perpetrated by women, and may be more prevalent in same-sex relationships (Hardesty et al., 2011). Previous gendered views may mean individuals from marginalized groups such as male victims and the LGBTIQ+ community may be less likely to disclose IPV (Fedele et al., 2022; Hart, 2019). Therefore, an inclusive and gender-neutral scale is critical to ensure widespread applicability to identify barriers to disclosure.
To address this gap in the literature, Crowe et al. (2019) used classical test theory to develop the 20-item IPV Internalized Stigma Scale (IPVSS). The IPVSS assesses the broader experience of stigma by including internalized, anticipated, and perpetrator stigma and isolation. While internalized and anticipated stigma are well established in the literature, perpetrator stigma, the authors say, is a new concept that relates to the stigma the survivor experiences from the perpetrator of the abuse, which is distinct to the abuse perpetrated. Also, isolation is an outcome related to experience of stigma. The IPVSS is a clinical scale for IPV survivors who have left an abusive relationship at least 6 months previously. Initial examination of the IPVSS showed that the internalized stigma subscale had low to moderate correlations with IPV, depression, fear of negative evaluation and psychological maltreatment of women (rs = .18–.47). Anticipated and perpetrator stigma correlated with fear of negative evaluation and psychological maltreatment of women (rs = .15–.42) but did not show meaningful associations with depression or IPV. Isolation had moderate correlations with all included measures except depression. The IPVSS is a broader assessment of IPV stigma intended for use with those who are not currently experiencing IPV. However, assessing IPV self-stigma in individuals who are still in an abusive relationship is necessary for identifying barriers to help seeking. While, identifying IPV self-stigma in individuals who have previously left an abusive relationship enables understanding of the impact of self-stigma which has been previously linked to self-blame and poor mental health (Crowe et al., 2019; Murray et al., 2018); an assessment for those in a current or previous abusive relationship provides more focused information on how IPV victims internalize or anticipate stigma. This understanding is essential when assessing the impact of IPV self-stigma in regard to help-seeking behaviors and interventions aimed at improving mental and social health.
Employing a multi-model approach using IRT and factor analyses, this project aimed to develop a scale that assesses internalized and anticipated stigma in IPV victims who are still in or have been in an abusive relationship. We chose a congeneric measurement model, based on previous stigma measurement studies that found scale items were inequivalent indicators of the latent trait. We also included an initial assessment of concurrent validity. A new, psychometrically sound scale that assesses IPV internalized stigma would help fill a gap in the IPV field and improve future research and support efforts.
Method
Procedure
Following institutional ethics approval (H20367), recruitment occurred via a dedicated Facebook page using paid advertising and first-year psychology students who participated for course credit. Participants were directed to the Lime Survey platform, where they were asked to provide informed consent. The survey was open to individuals over 18 years, in a current or previous relationship and who resided in Australia. Participants were incentivized by the opportunity to win one of two AUD50.00 gift cards. Only some scales were randomized as the nature of the main study’s aims was not conducive to complete randomization (i.e., scales relating to a larger item pool were not randomized).
Of the 653 individuals who visited the survey site, 67 did not meet the eligibility criteria or complete any questions beyond the first item. Further data cleansing for spurious responses (i.e., straight-lining and unrealistic completion time) resulted in an additional 137 responses removed. The final sample contained 449 participants. Over 80% of cases had complete data (83.52%) and Little’s MCAR test did not indicate evidence against an MCAR assumption. This finding suggests that substantially accurate results may be obtained by replacing the missing values using a validated algorithm. We used expectation maximization, which is a recommended single-input method for data of this nature (Dong & Peng, 2013).
Participants
As shown in Table 1, the majority of participants (M = 39.51, SD = 12.03, age-range = 18–73) were partnered, identified as female, Caucasian/white European and resided in suburban communities. Over half of the participants indicated they were experiencing moderate to severe financial stress and had completed tertiary education. Nearly 60% were heterosexual. While online recruitment using social media may be biased toward younger samples, this was not evident in this sample which was broadly representative of Australian adults.
Participant Demographics
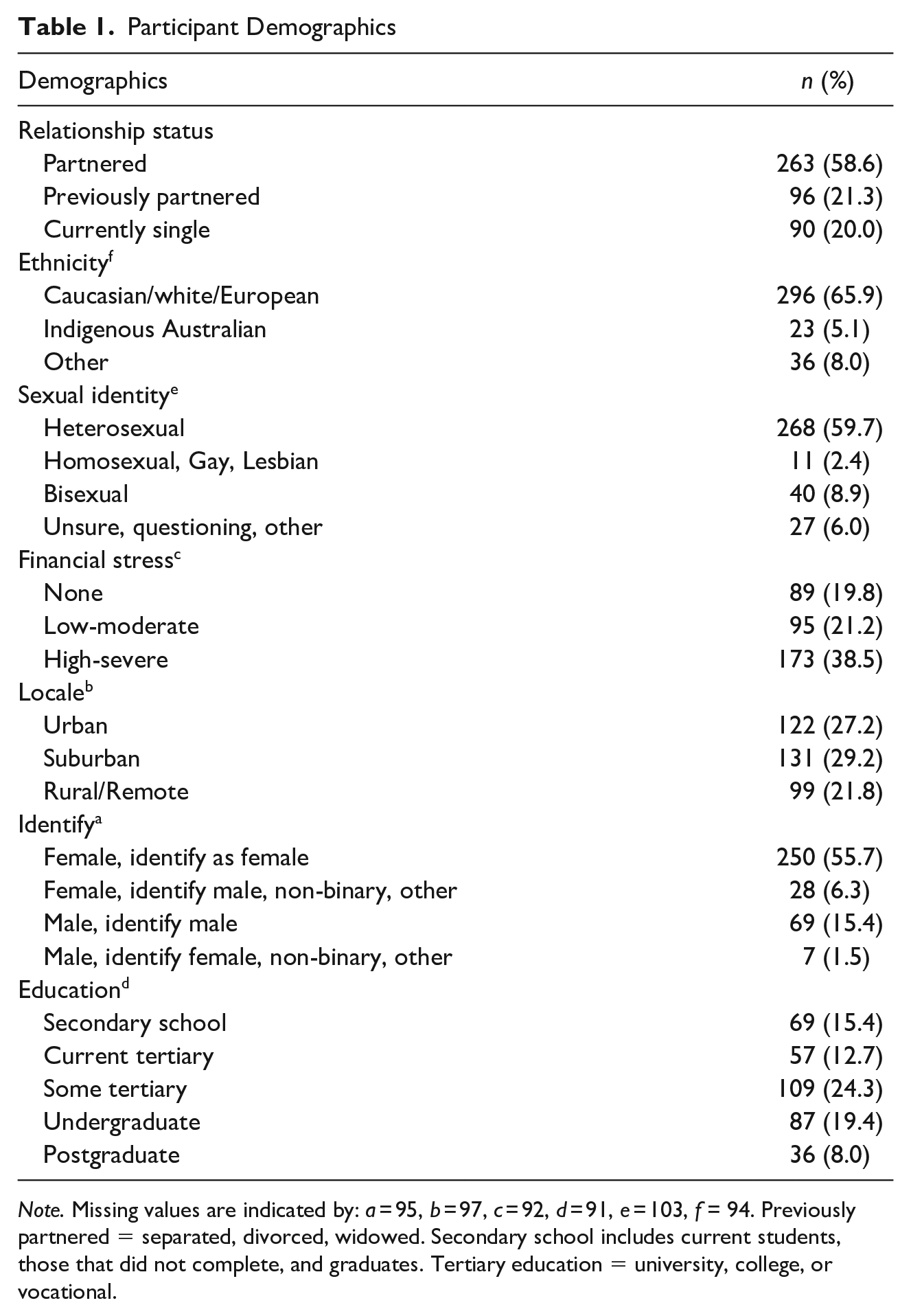
Note. Missing values are indicated by: a = 95, b = 97, c = 92, d = 91, e = 103, f = 94. Previously partnered = separated, divorced, widowed. Secondary school includes current students, those that did not complete, and graduates. Tertiary education = university, college, or vocational.
Item Pool
We derived the item pool by revising items from scales in the public domain and adding additional items based on a theoretical and empirical literature review. The ISMIS (Boyd et al., 2003) is a 29-item measure of internalized stigma that is commonly adapted for other “maladies.” Subscales assess alienation, stereotype endorsement, discrimination, social withdrawal, and stigma resistance. The Devaluation-Discrimination Scale (Link et al., 1991) is also a 29-item scale that measures the extent to which a person believes they will be devalued or discriminated against. The scale has four subscales: Devaluation-Discrimination, Secrecy, Education, and Withdrawal.
The 58 items from the above scales were revised for clarity, conciseness, and inclusiveness consistent with best practices for item development (DeVellis, 2016). Nineteen items were considered redundant, and five new items filled perceived gaps. In addition, all reverse-scored items were unreversed as they require higher verbal/linguistic abilities to comprehend (potentially limiting external validity) and contribute to poorer psychometric properties (Suárez Álvarez et al., 2018). Finally, items were scored on a 5-point scale from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate greater IPV self-stigma. Supplemental Table S1 presents the final item pool and the revisions, additions, and deletions to all items initially included in the item pool.
Materials
Composite Abuse Scale (Revised)-Short Form (CASR-SF)
This 15-item scale assesses the occurrence and frequency of physical, sexual, and psychological IPV (Ford-Gilboe et al., 2016). Items are rated from 1 (Never) to 5 (Daily/Almost daily). Higher scores indicate a greater frequency of abuse. The CASR-SF strongly correlates with coercive control, r = .51 (Ford-Gilboe et al., 2016). For this study, the internal consistency was ω = .96.
Social Health
The following scales from the Patient-Reported Outcomes Measurement Information Systems (PROMIS) assessed social health. All scales consisted of 6-items scored from 1 (Never) to 5 (Always). The PROMIS item banks pertaining to the social health scales have high correlations with similar social functioning scales (rs = .57–.76). All scales showed good internal consistency (Cella et al., 2010).
Informational, Emotional, and Instrumental Support
Informational support relates to the perceived availability of supportive, helpful information or advice (e.g., Other people help me get information when I have a problem). Emotional support relates to the perception of being cared for and valued (e.g., I have someone to talk with when I have a bad day). Instrumental support is the perception of having assistance available to help perform tasks (e.g., Is someone available to help you if you need it?). Higher scores indicate more support. For this study, the internal consistency was ω = .96 (informational), .97 (emotional), .97 (instrumental).
Companionship and Social Isolation
Companionship assesses the perception of having someone to share in social activities (e.g., Do you have someone with whom to relax?) Social isolation assessed an individual’s connectedness with others (e.g., I feel left out). For this study, the social isolation measure was reverse-scored; therefore, higher scores indicated less social isolation. For the current study, internal consistency was ω = .95 and .93, respectively.
Ability to Participate in Social Roles and Activities
This scale assessed the ability to perform one’s social roles and activities (e.g., I have to limit the things I do for fun with others). For this study, the items were reverse-scored; higher scores indicated a greater ability to participate. For the current study, ω = .90.
PROMIS Anxiety v1.0–8a
This 8-item scale focuses on fear (e.g., feelings of panic), anxious misery (e.g., dread), hyperarousal (e.g., tension, nervousness), and somatic symptoms related to anxious arousal (Cella et al., 2010). Items are rated from 1(Never) to 5 (Always). Higher scores indicate greater anxiety levels. The anxiety scale has strong correlations with similar anxiety measures, r = .75 (Cella et al., 2010). For this study, ω = .95.
PROMIS Emotional Distress Depression Scale v1.0–8a
The 8-item depression scale focuses on aspects of depression such as negative mood, self-criticism, worthlessness and negative affect (Cella et al., 2010). Items are rated from 1 (Never) to 5 (Always). Higher scores indicate greater depression. The depression scale has strong correlations with other measures of depression, rs = .72–.83 (Pilkonis et al., 2014). For this study, ω = .97.
General Self-Efficacy Scale
This 10-item scale assessed the belief in one’s general competence (Schwarzer & Jerusalem, 1995). Items include “I can remain calm when facing difficulties because I can rely on my coping abilities” and scored from 1 (Not at all true) to 4 (Exactly true). Higher scores indicate greater self-efficacy. For the current study, ω = .80.
Demographic Information
Participants provided demographic information on age, relationship status, biological and gender identity (e.g., biological male, identify as male), sexual identity (e.g., heterosexual, bisexual, questioning), residential location (urban, suburban, rural/remote), ethnic identity, indigeneity, current financial situation (i.e., “are you [or your family] currently experiencing any financial stress or problems?”) and education.
Data Analyses
The study conducted iterative factor analysis, bifactor analysis, hierarchical cluster and IRT analyses to determine the strongest and most informative set of items forming a valid measure of the latent trait—IPV self-stigma. This approach included conceptual IPV models (see Overstreet & Quinn, 2013) and measurement theory to guide analyses and interpretations. The R psych package was used for minimum residual factor analysis using direct oblimin rotation, which produces an unweighted least squares solution robust to skewed data (Flora et al., 2012). Hierarchical clustering indicated the ideal cluster number and included the root mean square residual (RMSR) as an estimate of model error. Bifactor analysis determined general factor saturation and additional group factor variance (Revelle, 2021). Internal consistency was estimated with McDonald’s ω, which is a less biased estimate than Cronbach’s alpha (Zinbarg et al., 2005). To test the unidimensional model fit, we utilized multiple model fit diagnostics. These included the Tucker Lewis index of factorability (TLI), explained common variance (ECV) and the root mean square error of approximation (RMSEA) (Asparouhov & Muthén, 2009; Xia & Yang, 2019). The IRT analyses followed expert recommendations (Embretson & Reise, 2000), including first determining the most appropriate model to fit the data and then evaluating items on discrimination/slope (a), information functions, and coverage of latent trait levels (theta). We also tested for lack of equivalence in measurement across demographic groupings through differential item functioning (DIF). We determined the graded response model (GRM; Samejima, 2004) was the best fit for this data over Rasch or classical test theory models, as it allows for variance in item discrimination and response formats, partly evidenced through variations in factor loadings. Scale development analyses used R 4.1.1 (R Core Team, 2021) packages: ltm (Rizopoulos, 2006); psych (Revelle, 2021); lordif (Choi et al., 2011); and coefficientalpha (Zhang & Yuan, 2016). Convergent validity was examined using SPSS v.28 (IBM Corp.).
Results
Our main goal was to develop a valid measure of IPV self-stigma, following best practices (DeVellis, 2016; Embretson & Reise, 2000; Gorsuch, 1983). We first conducted hierarchical cluster analysis, exploratory factor analysis and exploratory bifactor analysis with the full 44-item pool. Results showed a single cluster, with cluster fit = 0.82, RMSR = 0.08. However, most items had low cluster loadings (range = 0.10–0.69). Factor analysis also revealed one dominant factor with low communalities and loadings, TLI = 0.70, RMSEA = 0.07. Bifactor analysis indicated a single factor, again with primarily low factor loadings and communalities, ECV = 0.69, RMSEA = 0.05.
After finding consistent evidence of unidimensionality, we conducted GRM analyses. First, we compared a constrained model (all items have equal discrimination) with an unconstrained model. Results showed that the unconstrained model was a better fit, with less information loss, p < .001. We next removed the items with the poorest fit, one by one, and repeated analyses until all tests revealed an item set with consistently sound item and scale properties. The final 11 items assessing IPV self-stigma (the IPV Internalised Stigma Scale) are presented in Table 2.
The IPV Internalized Stigma Scale Cluster, Factor, and Bifactor Analysis.
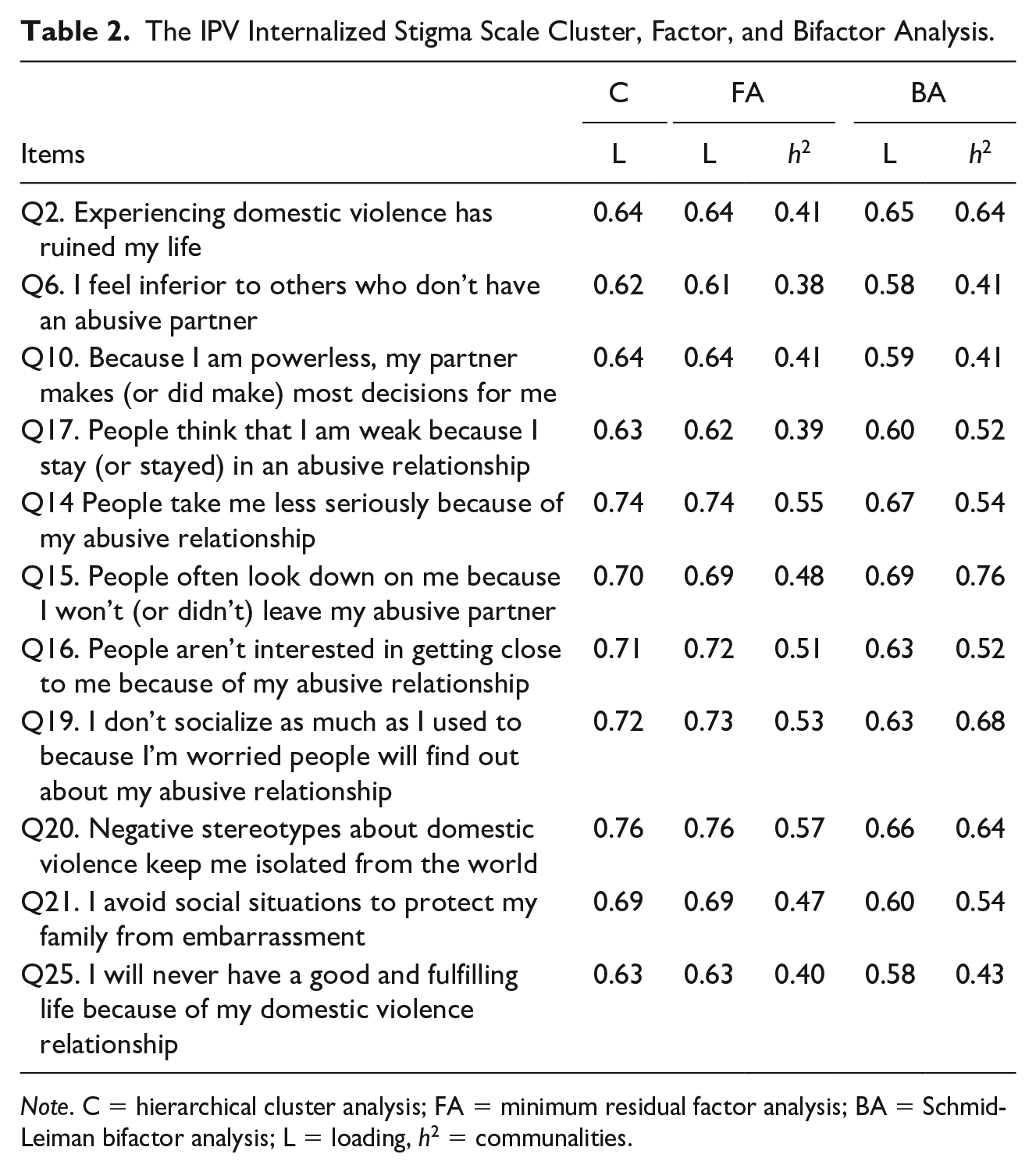
Note. C = hierarchical cluster analysis; FA = minimum residual factor analysis; BA = Schmid-Leiman bifactor analysis; L = loading, h2 = communalities.
Internal consistency was high, ω = .90, 95% CI [0.89, 0.91]. Cluster analysis showed cluster fit = 0.90, RMSR = 0.05. For factor analysis, TLI = 0.89, RMSEA = 0.10. Bifactor analysis showed, ECV = 0.71, RMSEA = 0.05. Figure 1 illustrates bifactor and hierarchical cluster models, respectively.
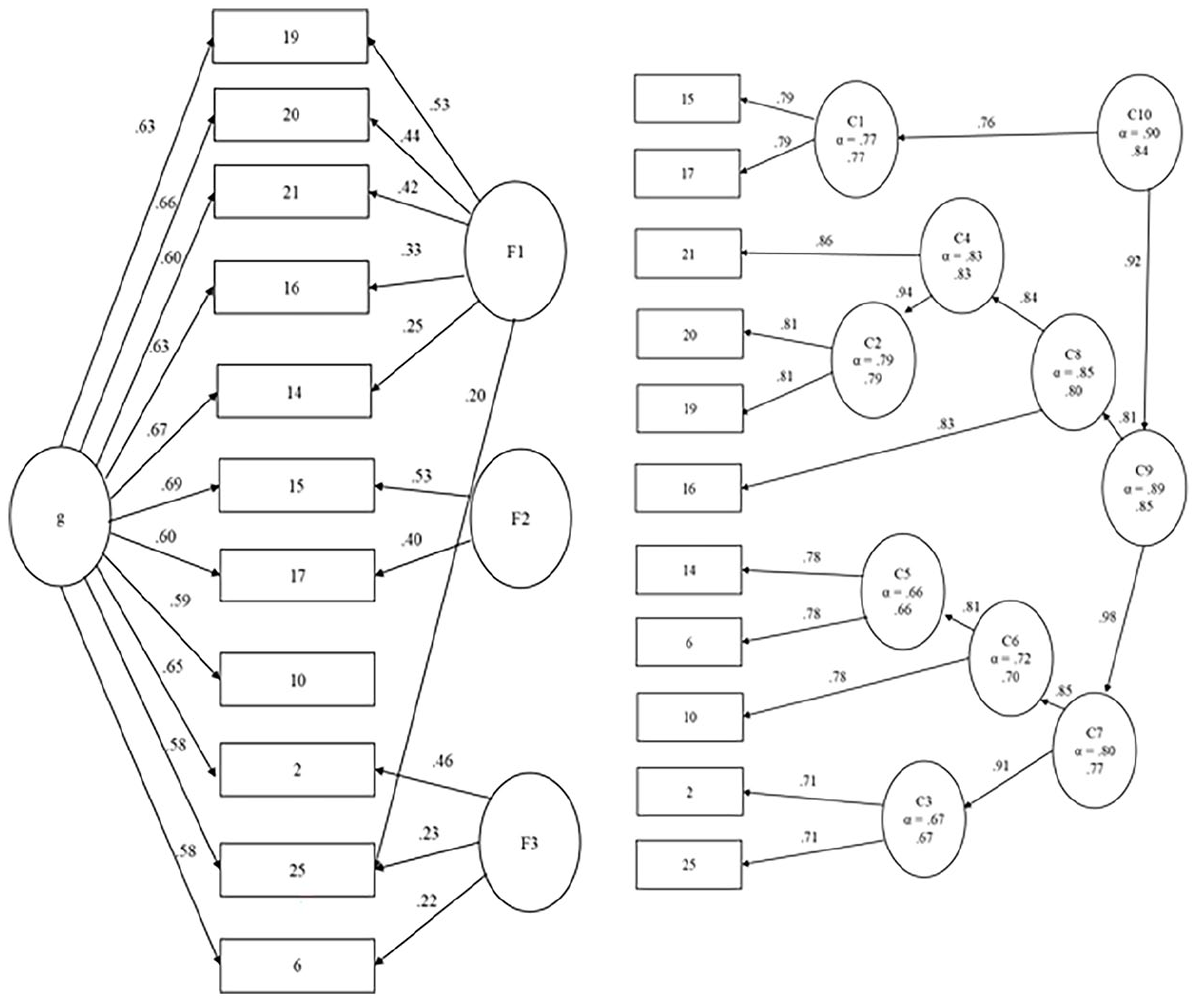
Bifactor and hierarchical cluster models of the IPV Internalized Stigma Scale.
Table 3 shows the item discrimination levels across theta (quantification of the latent trait) and item information functions. Results indicated that all items had moderate to high discrimination levels, a > 1.70. Results also demonstrated variation in the amount of latent trait information captured by each item, highlighting the value of using ability scores over sum scores.
Graded Response Model Analyses of the IPV Internalized Stigma Scale Items.
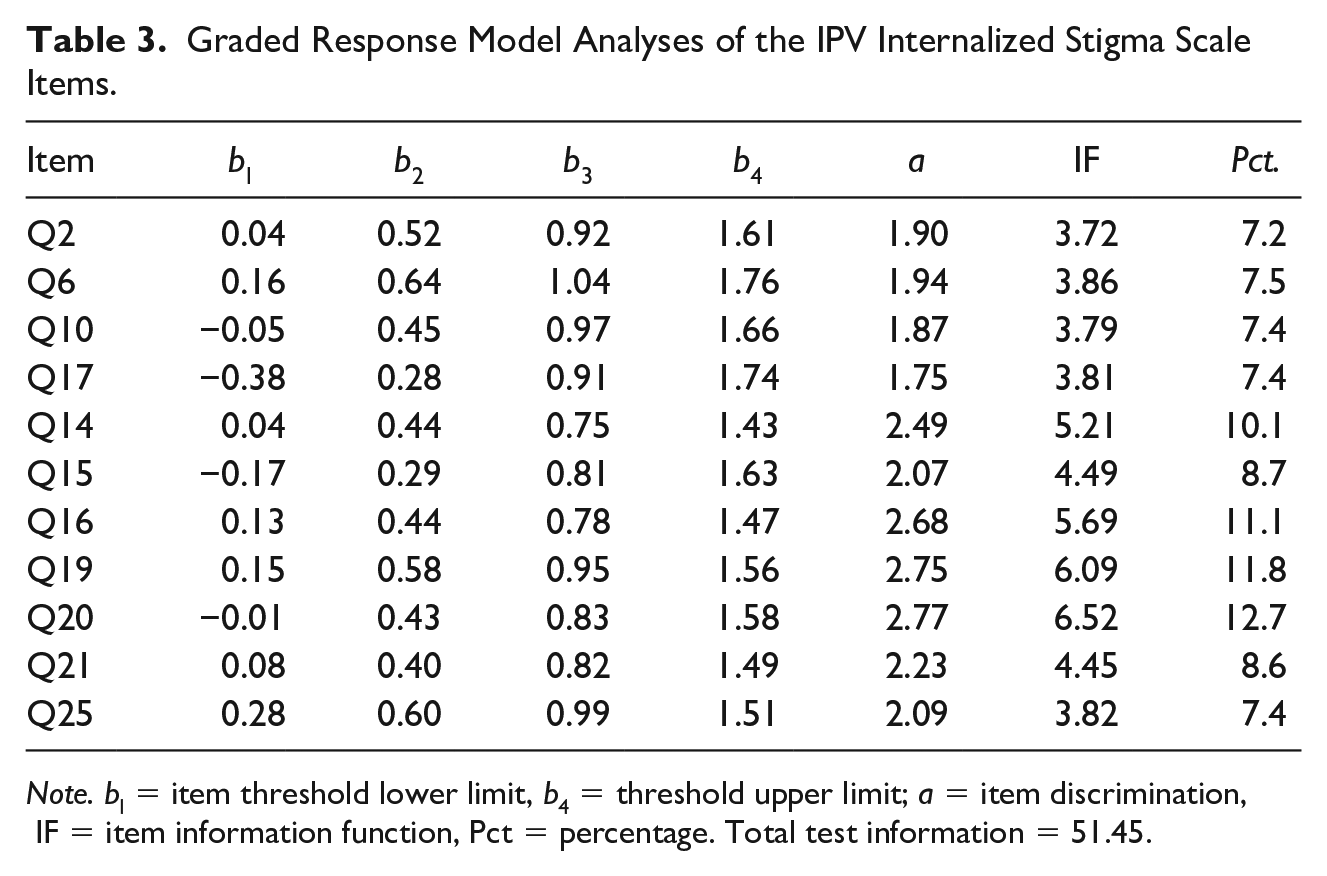
Note. bl = item threshold lower limit, b4 = threshold upper limit; a = item discrimination, IF = item information function, Pct = percentage. Total test information = 51.45.
The total test and item information diagnostics showed that the scale captures more information at higher levels of the trait, indicated by greater coverage above theta at zero. The individual item information details (b values) cluster around a moderate-high level of theta and illustrate how a few items capture information at very low or high levels. Item response characteristics indicate the range and peak levels of theta that each response on the item covers. These IRT outcomes provide information on item monotonicity (i.e., each response discriminates at increasing levels of theta) which helps validate the response set. Results showed that the mid-point responses (i.e., 3) were under-endorsed, indicating that five response points may be too many. However, item responses were appropriately ordered and cannot definitively point to the weakness being a neutral mid-point or the number of responses, as the overall results support monotonicity for all items.
Differential Item Functioning
Checking for invariance across relevant grouping variables (e.g., age, sex) is a crucial but often neglected step in scale development and validation (Embretson & Reise, 2000). We used the lordif package to conduct DIF checks by age groups (18–37, 38–56, 57+; 18–38 vs. 40+ years), sex (female/male), residence (urban/suburban/rural), ethnicity (European/Caucasian vs. others), relationship status (partnered vs. not). Sex and ethnicity were collapsed into binary variables necessary for this analysis. IRT-based DIF checks showed no DIF for any examined groups, all ΔR2 < .02.
Validity
To examine the concurrent validity of the IPV Internalized Self-stigma Scale (IPVIS), we used measures previously associated with IPV self-stigma. As expected (see Table 4), significant correlations between depression and anxiety indicated that those scoring highly on the IPVIS had greater depression and anxiety. Positive correlations between the IPVIS and self-efficacy indicate that those with more internalized stigma had less perceived efficacy. Higher scores on the IPVIS were also linked to less social support and companionship and greater social isolation.
Pearson’s Correlations: IPV Internalised Stigma Scale and Related Measures.
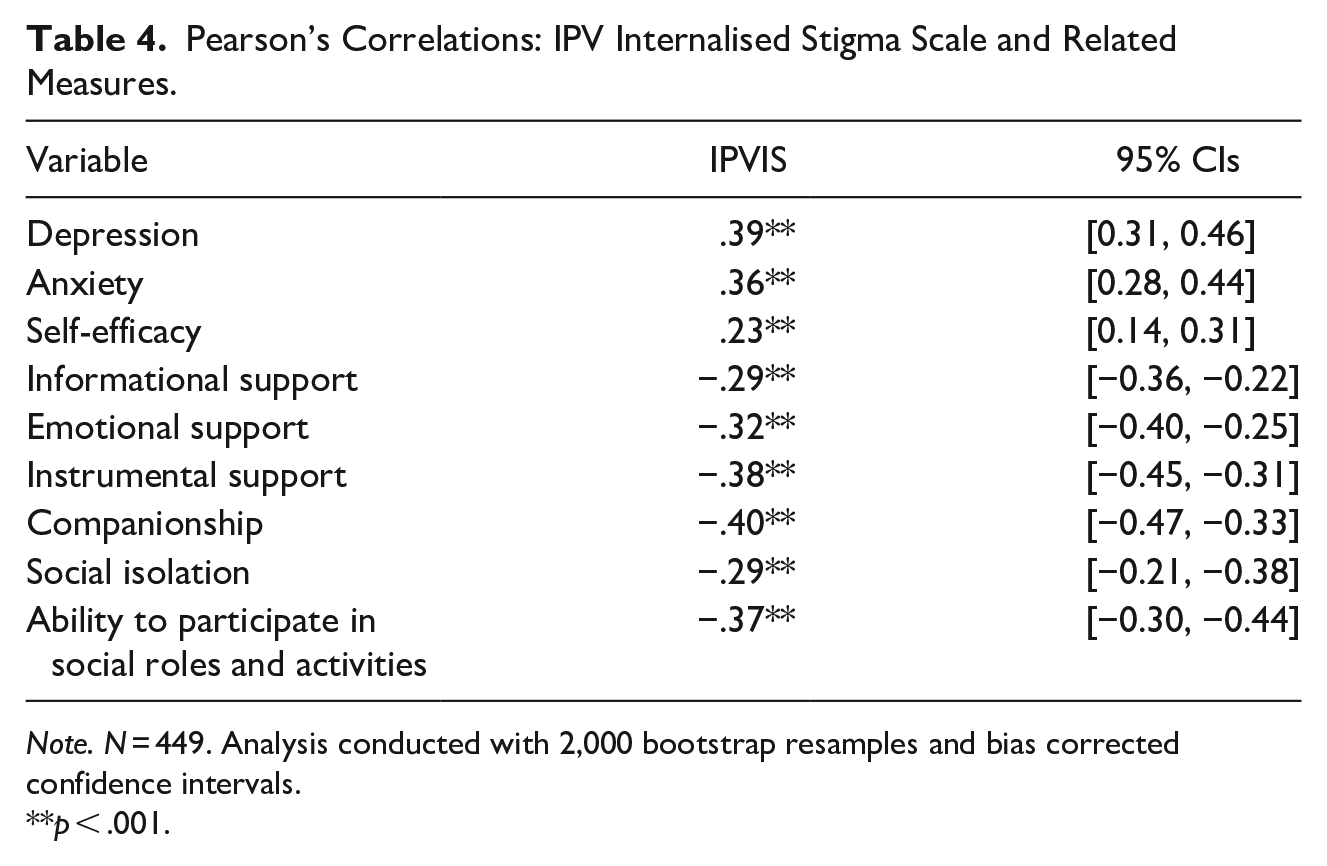
Note. N = 449. Analysis conducted with 2,000 bootstrap resamples and bias corrected confidence intervals.
p < .001.
Consistent with Smith et al.’s (2000) recommendations, we examined associations between the IPVIS with the full version of the revised ISMIS to confirm similar content coverage. To avoid autocorrelation, we only included the remaining 16 items of the ISMIS, that is, items not included in the IPVIS. While this may underestimate the association between the two instruments, it provides a means of assessing the overlapping variance between the scales, an important step in assessing validity in short-form development. The IPVIS correlated very strongly with the 16 items from the ISMIS, indicating similar content coverage, r(449) = .86, p < .0001.
Discussion
This study developed a measure of IPV self-stigma using items adapted from existing measures and additional items based on an empirical and theoretical review. The initial psychometric evaluation of the IPVIS indicates that the scale is suitable for research and clinical use with any individual in a current abusive relationship or who has left such a relationship. To the best of our knowledge, the IPVIS is the first scale developed that assesses IPV self-stigma that is inclusive of a diverse range of clients or participants in any type of relationship.
This study adopted a comprehensive multi-model approach to scale development, ensuring that the final set of items comprised a valid measurement of the latent trait—IPV self-stigma. This is a key strength of this study. The congeneric model approach, as opposed to classical test theory, provided finer details and additional information on the performance of the items and the scale overall (Flake et al., 2017). All items demonstrated moderate to high discrimination levels confirming that each item is tapping into meaningful facets of the latent trait. Moreover, the scale’s unidimensionality is a fundamental requirement for the validity of latent trait measures (Embretson & Reise, 2000).
The IPVIS can be used with diverse individuals, an important consideration for clinicians and researchers. Scales should be free of “systematic demographic subgroup bias” (Harvey & Hammer, 1999, p. 368) and the DIF provided evidence that the items performed consistently, independent of personal characteristics (i.e., age, sex, area of residence, ethnicity, and relationship status). Therefore, using the IPVIS, valid comparisons can be made across different groups for research purposes. Researchers can use the IPVIS to assess the latent trait, IPV self-stigma, to advance current knowledge in this understudied area (Crowe et al., 2019). For example, the scale can be used to examine the association between IPV self-stigma and adverse outcomes such as mental and social health addressing limitations of previous studies (e.g., Bonfils et al., 2018; Boyd et al., 2003; Brown et al., 2010; Howland et al., 2016).
In clinical settings, this measurement invariance ensures that the scale has widespread applicability for various relationship types (e.g., heterosexual, same-sex), IPV circumstances (e.g., male or female perpetrators or victims) and individuals (i.e., a diverse range of gender and sexual identity). The scale can be used to identify if self-stigma is a barrier to disclosure and help seeking by assessing the extent that an individual has internalized and anticipated stigma. For instance, scale items related to “being weak for staying in an abusive relationship” and “feeling looked down upon” tap into dominant and pervasive stereotypes that may be accepted as true (i.e., internalized stigma). Scale items that relate to anticipating adverse reactions (e.g., people not interested in getting close because of the abusive relationship) tap into anticipated stigma. This information can contribute to more targeted interventions aimed at addressing widespread and erroneous stereotypes. Given that IPV self-stigma has been identified as a barrier to help seeking (Overstreet & Quinn, 2013), this is an important area for research and clinical intervention. Also, the scale length (11-items) is suited to busy clinical settings. Supplemental Appendix contains the full scale and scoring guidelines.
Limitations and Future Directions
This study has many strengths, but it is not without limitations. We succeeded in obtaining a rather large and diverse sample that included IPV victims and those not victimized, providing suitable diversity for the topic of assessment. The scale development analyses were also varied and thorough, providing a large amount of information on the facets and measurement characteristics of IPV self-stigma. There remains, however, the need to examine temporal factors in IPVIS assessment through test-retest reliability and longitudinal study. Additional samples are also required, that are more ethnically diverse and also cover adolescents, as IPV is not restricted to those aged 18 and above.
Conclusion
The IPVIS is suitable for a diverse range of clients or participants in any relationship type for use in various settings. The inclusiveness of this scale overcomes previous limitations in the area of IPV that adopted gendered views of IPV. Moreover, the scale is suitable for screening IPV victims that are currently in an abusive relationship or who have previously been in one. This screening is essential to addressing barriers to support, as highlighted by Robinson and Spilsbury (2008). The items in the IPVIS perform consistently across personal characteristics, which ensures that the scale has widespread application which is an important consideration. The scale also taps into anticipated and internalized stigma, two aspects that help understand reasons for IPV concealment. Taken together, the IPVIS has been developed using a comprehensive approach to test development and has shown promising psychometric properties. The IPVIS is suitable for assessing IPV self-stigma in research and clinical settings.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605231162653 – Supplemental material for Development and Psychometric Evaluation of the IPV Internalized Stigma Scale
Supplemental material, sj-docx-1-jiv-10.1177_08862605231162653 for Development and Psychometric Evaluation of the IPV Internalized Stigma Scale by Robyn Brunton and Keith M. Harris in Journal of Interpersonal Violence
Supplemental Material
sj-docx-2-jiv-10.1177_08862605231162653 – Supplemental material for Development and Psychometric Evaluation of the IPV Internalized Stigma Scale
Supplemental material, sj-docx-2-jiv-10.1177_08862605231162653 for Development and Psychometric Evaluation of the IPV Internalized Stigma Scale by Robyn Brunton and Keith M. Harris in Journal of Interpersonal Violence
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.