
Abstract
Intergenerational continuity of child maltreatment (CM) is a well-documented phenomenon of concern; however, its effects on the child’s level of exposure to CM, as well as subsequent trauma exposure and adult functioning remain undocumented. The present study aimed to further explore the intergenerational effects of CM by comparing emerging adults (EA; ages 18–25) on their exposure to CM, adult victimization, and psychological functioning according to their mother’s CM histories. One hundred and eighty-five mothers and their EA completed independently an online survey measuring sociodemographics, material deprivation, CM, adult victimization, and psychological functioning. The participating dyads (primarily White and female-identifying) were recruited online through social media, universities, and advertisements in non-profit organizations throughout Canada. Findings revealed that maternal histories of CM were associated with increased neglectful and physically abusive acts endured in childhood for maltreated EA. Maternal histories of CM, regardless of the EA’ victimization status, were associated with a higher EA’ number of adulthood interpersonal—but not non-interpersonal—traumas experienced. While a maternal history of CM was a risk factor for intimate partner violence (IPV) in maltreated EA, it was protective for non-maltreated EA. Maltreated EA with maltreated versus non-maltreated mothers presented more psychological difficulties, but only if they also reported material deprivation. Practitioners working with children at-risk or exposed to CM should document parents’ histories of CM and take that into account in their assessments and intervention practices. This study also provides further evidence to support social policies targeting the family system as a whole.
Keywords
Child maltreatment (CM) consists of the experience of physical, sexual, and emotional abuse, neglect, as well as exposure to intimate partner violence (IPV) before the age of 18. It can lead to severe acute injury and harmful long-term outcomes for survivors, such as harmful substance use (Mandavia et al., 2016), mental health (Lindert et al., 2014), and relationships issues (Nguyen et al., 2017). Past studies have identified that a parent’s history of CM is a potent risk factor for CM experiences among their children, regardless of their involvement as perpetrators; a concept known as intergenerational continuity of CM (Langevin et al., 2021; Widom et al., 2015). Indeed, prevalence estimates of intergenerational continuity of CM range from 7 to 88% depending on the studies’ methodologies (e.g., study design, types of CM examined) (Langevin et al., 2021). Despite the well-documented phenomenon of concern, the effects of intergenerational continuity or parental histories of CM on the child’s level of exposure to CM, as well as subsequent trauma exposure and adult functioning remain undocumented. As such, the present dyadic study aimed to add depth to our understanding of intergenerational patterns of CM by examining the associations between maternal histories of CM and their emerging adults’ (EA) level of exposure to various types of CM, revictimization/adulthood adverse experiences, and psychological functioning.
Processes Involved in Intergenerational Continuity
A systematic review of theoretical models explaining the intergenerational continuity of CM revealed that the impact of CM on mental health (e.g., posttraumatic stress, emotion regulation) and relationships (e.g., attachment, support networks), and the subsequent impact of these factors on the parenting role (e.g., attitudes, practices) are central to intergenerational victimization processes (Marshall et al., 2022). Empirical studies further support these theorized associations (Langevin et al., 2021). For example, studies demonstrated that the presence of posttraumatic stress symptoms in survivors of child sexual abuse increases the risk of second generation’s sexual abuse (Baril & Tourigny, 2016; Trickett et al., 2011). More generally, for both parents, emotional dysregulation has been associated with child abuse potential (Miragoli et al., 2020). Unfortunately, mental health difficulties and emotional dysregulation can reduce psychological capacity in parenting (Rutherford et al., 2015). For instance, parents with CM histories and mental health difficulties were likely to respond negatively to ambiguous cues from their children (Berlin et al., 2011). All in all, these negative impacts of CM on mental health and parenting appear to make children more vulnerable to victimization (Baril & Tourigny, 2016; Langevin, Gagné, et al., 2023) by (re)creating familial environments that might be more conducive to abuse and neglect (Noll et al., 2017). These dynamics could also result in higher levels of CM exposure for maltreated children in the CM continuity versus discontinuity trajectories (where CM does not continue intergenerationally), but this remains to be explored.
Moreover, intergenerational continuity of CM should be understood within the greater socioecological contexts. Ecological risk factors such as socioeconomic risk, lack of social support, and stressful life events have been found to maintain cycles of CM (St-Laurent et al., 2019). The accumulation of these risk factors is unfortunately not racially and culturally neutral. Black, Indigenous, and Hispanic communities are at higher risk for CM because of systemic discrimination, where marginalized communities face higher odds of few economic resources, neighborhood violence, and barriers to preventative resources (Drake et al., 2011; Luken et al., 2021; Roberts et al., 2011). Overall, many factors participate in maintaining victimization across generations; however, fortunately, a maternal history of CM is not deterministic of child victimization status as many families break cycles of violence and display patterns of discontinuity.
Intergenerational Effects of Child Maltreatment
The child sexual abuse literature demonstrates that a mother’s history of childhood sexual abuse is associated with increased difficulties in maltreated (Langevin, Hébert, et al., 2022), but also non-maltreated children (Borelli et al., 2019). For instance, in studies examining abuse continuity, mothers’ own child sexual abuse histories were associated with higher mental health symptoms, such as internalizing, externalizing, and dissociation symptoms, in abused children (Langevin, Hébert, et al., 2022). In addition, children with a sexually abused mother, no matter their own victimization history, were at greater risk of presenting internalizing and externalizing symptoms (Borelli et al., 2019). Many factors can contribute to these increased mental health symptoms in both continuity and discontinuity trajectories such as vicarious learning (Thompson, 2013), parenting (Grunsfeld, 2018), or heritability (Roth et al., 2014). However, studies examining the intergenerational effects of CM are mostly conducted with children and it is unclear whether these mental health difficulties persist into adulthood, and if so, in what form. Emotional dysregulation would be important to examine given its highly supported association with CM (e.g., Bonet et al., 2020) and its central role to many adulthood psychopathologies (Aldao et al., 2010). Similarly, trauma symptoms and general psychological distress (e.g., anxiety, depression symptoms) that are well documented as consequences of CM should be examined (e.g., Gallo et al., 2018; Lindert et al., 2014). Examining CM types, beyond sexual abuse, would help gain a better understanding of the links between maternal histories of CM and their children’s psychological functioning in adulthood.
Revictimization
In addition to examining psychological functioning as an intergenerational outcome of CM, understanding revictimization outcomes can have invaluable implications for prevention initiatives. The revictimization of CM survivors is a well-documented phenomenon (Walker et al., 2019; Widom et al., 2008). A recent meta-analysis of 80 studies estimated a mean prevalence of sexual revictimization in CSA survivors of 47.9% (Walker et al., 2019). In fact, all types of CM have been associated with increased risk for lifetime revictimization (Widom et al., 2008), and this is particularly the case for marginalized communities in terms of frequency and severity of the revictimization (López & Yeater, 2021; Pittenger et al., 2018). Unsurprisingly, Balsam et al. (2011) determined that revictimization can lead to dire outcomes such as higher levels of psychological distress, suicidality, alcohol use, and self-harm behaviors compared to those with no revictimization and those with no victimization histories. While we know maternal histories of CM are associated with increased risks of CM for the second generation, no studies have examined the potential role of maternal CM in second generation’s adulthood interpersonal and non-interpersonal (re)victimization.
Current Study
The present study aimed to further our understanding of the intergenerational effects of CM by examining the effects of mothers’ histories of CM on EA’: (1) level of exposure to five types of CM, (2) adult interpersonal and non-interpersonal adverse life events (including IPV victimization), and (3) on psychological functioning (psychological distress, emotional dysregulation, posttraumatic stress symptoms), while accounting for material deprivation. Although we focused primarily on individual-level risk factors within this study, material deprivation was accounted for as a contextual risk factor associated with early CM and intergenerational continuity of CM (Langevin, Gagné, et al., 2023; van IJzendoorn et al., 2010), and with many mental health outcomes (Belle, 1990).
Our study addressed many gaps in the literature on intergenerational continuity of CM including the lack of studies comparing the dosage of CM in maltreated EA with and without maltreated mothers, examining the role of maternal histories of CM in adult (re)victimization, and documenting the association between maternal histories of CM and the psychological functioning of EA. A dyadic approach, where data was collected from both the mother and their EA, was selected to increase the probability of accurate and complete reports of CM for both generations. Including EA for the second generation allowed for the documentation of the complete age range for CM and minimized recall bias in the second generation. Moreover, a sharp increase in mental health concerns is seen in emerging adulthood (Solmi et al., 2021). An additional argument for the inclusion of an EA sample is the fact that long lasting and more serious intimate relationships emerge in this developmental period, which can lead to an upcoming entry into parenthood (Arnett et al., 2014; Weisskirch, 2018). These particularities of emerging adulthood, in combination with the variables of interest in the current study, highlight the relevance of focusing on this developmental period. Within our Canadian sample, we hypothesized that: (1) a history of CM in mothers will be associated with greater levels of exposure to CM in maltreated EA; (2) a history of CM in mothers will be associated with greater exposure to adult (re)victimization experiences, especially of interpersonal nature and for maltreated EA; and (3) a history of CM in mothers will be associated with greater psychological difficulties in EA with and without a history of CM. We expected material deprivation to interact with CM to create greater psychological difficulties among maltreated EA living in precarious conditions (Putnam et al., 2013).
Method
Participants
Participants were mother-EA (18–25 years old) dyads from across Canada. Individually, mothers (M = 51.16 years old, SD = 5.82) and EA (90% female-identifying; M = 20.87, SD = 2.17) completed an online survey. Initially, the sample included 409 mothers and 809 EA; measures were put in place to screen out careless responses. Participants were excluded if they did not provide a valid identification number (n = 39), completed less than 75% of the survey (n = 36), answered “no” to a question that asked directly whether their data should be considered valid (n = 38), were duplicate responses (n = 68), did not meet the age criterion (n = 68), did not answer at least 3/5 directed questions correctly (n = 121), and completed the survey in less than half the modal time (n = 17). Our final sample included 253 mothers, 578 EA, and 185 complete dyads. This study only included the complete dyads that were divided in four groups based on the reported CM history of both members of the dyads: CM Both (both EA and mothers reported experiencing at least one form of CM; n = 78), CM EA (only the EA reported experiencing CM; n = 37), CM Mothers (only the mothers reported experiencing CM; n = 27), and No CM (none reported experiencing CM; n = 43). The majority of EA were female-identifying (90%), White (67%), and university-educated (51%). While there is a clear gender imbalance in the sample compared to the Canadian population, the percentage of White-identifying and university-educated participants appear similar to population-wide estimates from the 2016 census revealing that 25% of Canadians are from visible minorities and 54% have a postsecondary education (Statistics Canada, 2017). About half of EA documented material deprivation. Other sociodemographic characteristics and CM histories of the participants are presented in Table 1.
Sociodemographic Characteristics of the Emerging Adult.
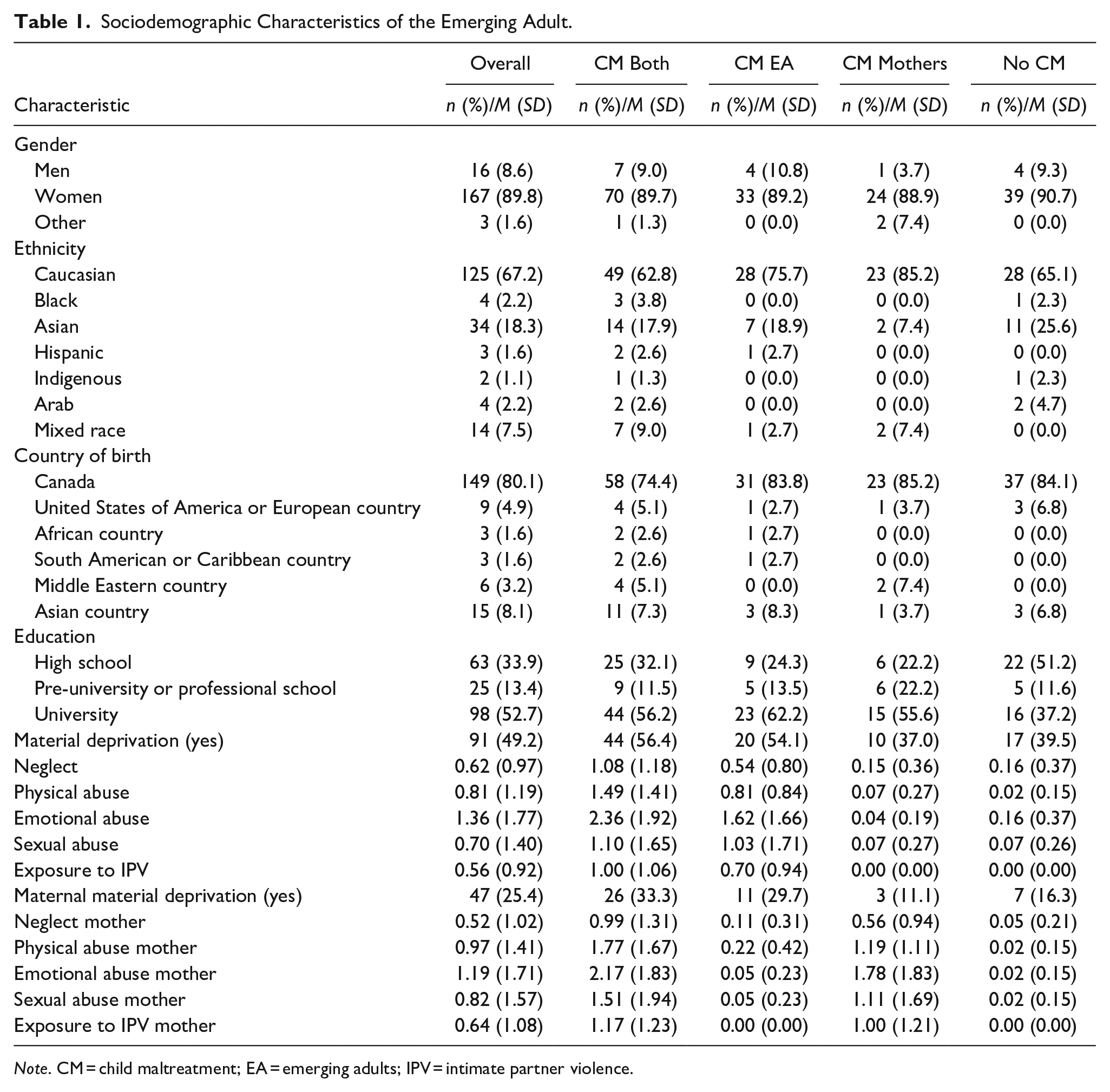
Note. CM = child maltreatment; EA = emerging adults; IPV = intimate partner violence.
Procedures
The participating dyads were recruited online through social media, universities, and advertisements in non-profit organizations throughout Canada. Study advertisements indicated the intent to investigate child adversity, relationships, and emotions. English and French-speaking individuals were included, and the survey was done via a secure survey platform. Participants were directed to a consent form first and encouraged providing the email address of their mother or EA child. The other member of the dyad then received an email briefly describing the project with a link to the consent form; an alphanumeric code was used to identify dyads. Mothers and EA were told not to discuss their answers together. All participants were entered into a draw for a chance to win an iPad, and members of complete dyads each received a $5 e-gift card. Procedures were approved by the McGill University Research Ethics Board.
Measures
Child maltreatment
Each member of the dyad self-reported their CM histories before 18 using “yes” or “no” answers. Physical/supervisory neglect was measured using the ISPCAN Child Abuse Screening Tool (ICAST; five items) (Dunne et al., 2009). A sample item is: “Have you ever not been given food to eat and/or drink even though your parent(s) or caretaker(s) could afford it?.” The ICAST was field-tested and internal consistencies were adequate (α = .61 to .82) (Dunne et al., 2009). The Early Trauma Inventory Self-Report—Short Form (ETI-SR-SF) (Bremner et al., 2007) was used to assess physical (five items), sexual (six items), and emotional abuse (five items). An example of questions is: “Before the age of 18, were you ever pushed or shoved by a parent or caregiver?.” The ETI-SR has shown adequate internal consistencies for measuring CM types in the development sample (α = .78 to .90) (Bremner et al., 2007). Exposure to IPV was measured using modified items from the Short-Revised Conflict Tactics Scales (CTS2S; three items) (Straus & Douglas, 2004), which documents exposure to psychological (one item; e.g., harsh criticism, destroying belongings) and physical (two items; e.g., shoving, kicking, throwing things at the partner) IPV. An example of an item is: “Have you ever seen your mother or father kick, punch, or beat up their partner?.” All CM types, except for sexual abuse, must have occurred within a caregiver-child relationship to be considered (no matter if the participating mother was the perpetrator or not) in order to avoid violence experienced outside of the caregiver-child relationship to be counted as CM (e.g., sibling victimization, peer-victimization). Count scores were computed to reflect the number of neglectful or abusive acts reported for each category of CM (which ranged from 0–3 to 0–6). In the current sample, internal consistency coefficients were adequate (α = .73 to .90). EA neglect had lower but acceptable internal consistency (α = .67).
To create intergenerational trajectories of CM, a dichotomous score for each CM type was calculated and participants were considered maltreated if they answered yes to at least one item in one CM type. This was done after carefully reviewing the frequencies of endorsement for each CM item and after excluding items that were highly endorsed and reflected more minor or unclear acts of abuse or neglect. One item per CM type, except for exposure to IPV, was deleted in that process: “Have you ever been hurt or injured because no adult was supervising you?” (neglect), “Were you ever slapped in the face with an open hand by a parent or caregiver?” (physical abuse), “Were you ever touched in an intimate or private part of your body (e.g. breast, thigh, genitals) in a way that surprised you or made you feel uncomfortable?” (sexual abuse), and “Did your parents or caregivers often fail to understand you or your needs?” (emotional abuse).
Adversity in adulthood
Exposure to interpersonal traumas and non-interpersonal adverse life events in adulthood were documented using the Life Events Checklist for DSM-5 (LEC; Weathers et al., 2013). EA reported their exposure (as a witness or a victim) to 16 potentially traumatic life events using a yes to no format. The interpersonal traumas count score (0–5) included five items documenting exposure to physical/sexual assaults and captivity (e.g., “Assault with a weapon [for example, being shot, stabbed, threatened with a knife, gun, bomb]”). The non-interpersonal adverse life events count score (0–11) included 11 items covering exposure to events such as serious accidents/injuries, fire, natural catastrophes, and transportation accidents.
Three subscales from the CTS2S (Straus & Douglas, 2004) were used to document the frequency of EA’ psychological (two items), physical (two items), and sexual (two items) IPV victimization in the past year; the negotiation and injury scales were not included in the present study. When compared to the full version of the CTS2, the CTS2S has been found to have adequate construct and concurrent validities (r = .65 to .89) (Straus & Douglas, 2004). Participants were asked to rate how many times they were subjected to various violent acts in the past year on a scale ranging from 0 = not in the past year to 6 = more than 20 times. In accordance with Straus and Douglas’s guidelines (2004), count scores were calculated for each form of IPV by summing the mid-points for each response choice. Internal consistency coefficients for each form of IPV ranged from α = .65 to .86.
Psychological functioning
Posttraumatic stress symptoms were documented using the 20-item PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013) that assessed symptoms of reexperiencing, avoidance, negative alterations in cognitions and mood, and hyperarousal (e.g., “In the past month, how much were you bothered by: repeated, disturbing, and unwanted memories of the stressful experience?”). EA recorded their answers on a 5-point Likert-type scale (0 = not at all, to 4 = extremely). In the current study, the PTSD checklist total sum score ranging from 0 to 80 was used (α = .95).
To assess the severity of their emotional dysregulation, EA completed the 18-item Difficulties in Emotional Regulation Scale (DERS—18; Victor & Klonsky, 2016), which includes six subscales with three items each: Awareness, Acceptance, Impulsivity, Strategies, Goal, and Clarity. Examples of items are: “When I’m upset, I acknowledge my emotions” (awareness) and “When I’m upset, I believe that I will remain that way for a long time” (strategies). Answers were recorded on a 5-point Likert-type scale (1 = almost never, 5 = almost always) and summed to create a total score where higher scores reflect higher dysregulation. The DERS-18 had good internal consistencies in the development sample (α = .77 to .90) and is a reliable and valid measure of emotional dysregulation (Victor & Klonsky 2016). In the current study, the total score for emotional dysregulation was used (α = .84).
EA’ general level of psychological distress was assessed using the Psychiatric Symptom Index (PSI; Préville et al., 1992), a validated 14-item self-report measure used to assess symptoms of irritability, depression, anxiety, and cognitive difficulties in the last week (e.g., “Did you feel bored or have little interest in things?”). Participants rated their symptoms on a 4-point Likert-type scale (0 = never to 3 = very often). A global score of psychological distress, ranging from 0 to 100, was calculated. Internal consistency for the total score was α = .89.
Sociodemographic characteristics
EA reported on their demographic characteristics (e.g., age, ethnicity, education). Mothers and EA completed the Canadian Survey of Economic Well-Being—Index of Material Deprivation (Statistics Canada, 2013), a 17-item measure assessing one’s ability to afford basic necessities. This survey is an appropriate measure for most of the Canadian population (Rheault & Crespo, 2015). Participants answered in a yes/no format to statements such as “Can you afford to pay your bills on time?.” A dichotomous score was created whereas participants that answered no to at least one item received a score of 1 = deprivation; other participants received a score of 0 = no deprivation.
Analytic Strategy
IBM Statistical Package for Social Sciences (SPSS) was used for statistical analyses. Preliminary analyses were conducted to identify outliers (changed for the closest non-outlier score), potentially relevant covariates to include in the models, and to determine if the assumptions were met to conduct a MANCOVA with psychological functioning variables. The mean/variance ratios were examined to select Poisson or negative binomial regressions for the analyses pertaining to CM histories and adversity in adulthood. For these analyses, the count scores for the different CM subtypes reported by EA were used.
Results
Preliminary Analyses
Six univariate outliers were brought to their closest within trajectory non-outlier score on psychological functioning outcomes. One EA was deleted due to outlier scores on more than one dependent variable. No multivariate outliers were identified. All assumptions were met to conduct a MANCOVA. Due to extremely low counts in our sample, the CTS2S physical IPV scale was not tested further for trajectory differences; only psychological and sexual IPV scores were examined. Table 2 presents the correlations between the main variables. All correlations were positive and significant (r = .158 to .559), except for the non-significant correlations of sexual abuse and emotional dysregulation with non-interpersonal adverse events in adulthood. Posttraumatic stress symptoms, emotional dysregulation, and psychological distress were highly correlated with one another (r = .580–.716). Chi-square analyses revealed no significant differences between EA based on intergenerational trajectories of CM for gender, education, ethnicity, and material deprivation. Maternal material deprivation was almost significant (χ2(3) = 7.75, p = .051) and was used as a covariate for analyses pertaining to CM. EA material deprivation was also kept as a covariate for analyses related to adversity in adulthood and psychological functioning. Descriptive statistics can be found in Tables 1 and 5.
Correlations Between Dependent Variables.
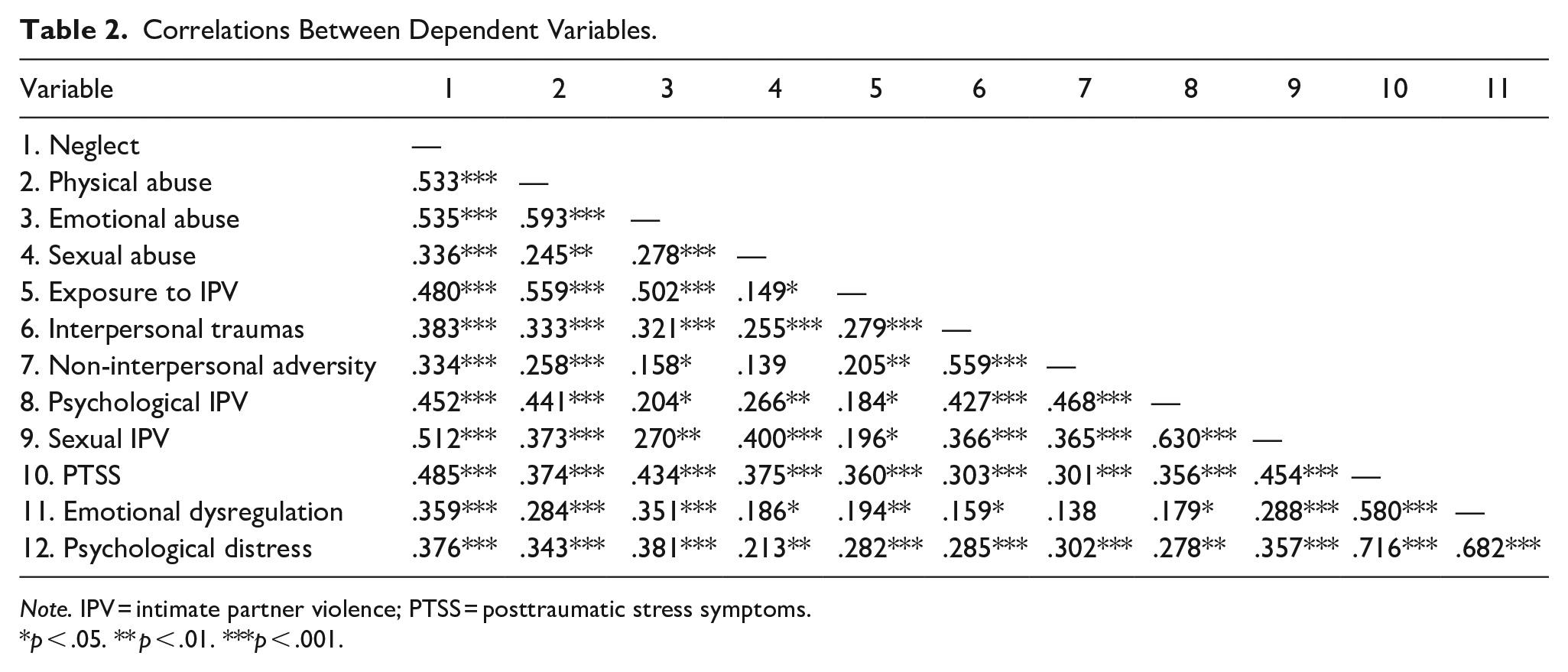
Note. IPV = intimate partner violence; PTSS = posttraumatic stress symptoms.
p < .05. ** p < .01. ***p < .001.
Child Maltreatment History
To address hypothesis 1, Poisson regressions (neglect, exposure to IPV) and negative binomial regressions (physical, sexual, and emotional abuse) were used to compare the CM Both and CM EA trajectories on levels of exposure to CM (count scores) in EA, while controlling for the presence of maternal material deprivation (Table 3). Results showed that being a member of CM Both versus CM EA was associated with almost doubled (Exp(B) = 1.97) counts of exposure to neglectful acts in childhood for maltreated EA. Similarly, count scores of physical abuse were 1.80 times higher in the CM Both compared to the CM EA trajectory. Material deprivation was not significant for these CM types. Thus, a maternal history of CM was associated with increasing numbers of neglectful and physically abusive acts endured by EA maltreated in childhood. Conversely, the amount of exposure to IPV (count scores) was not associated with the intergenerational trajectory of CM but was with material deprivation. The exposure to IPV was 1.72 times greater for EA from deprived compared to non-deprived familial environments. Finally, the amount of exposure to emotional and sexual abuse (count scores) was similar across the two intergenerational trajectories (CM Both vs. CM EA) and deprivation groups. See Figure 1 for a visual representation.
Poisson and Negative Binomial Regressions for CM Variables (n = 115).
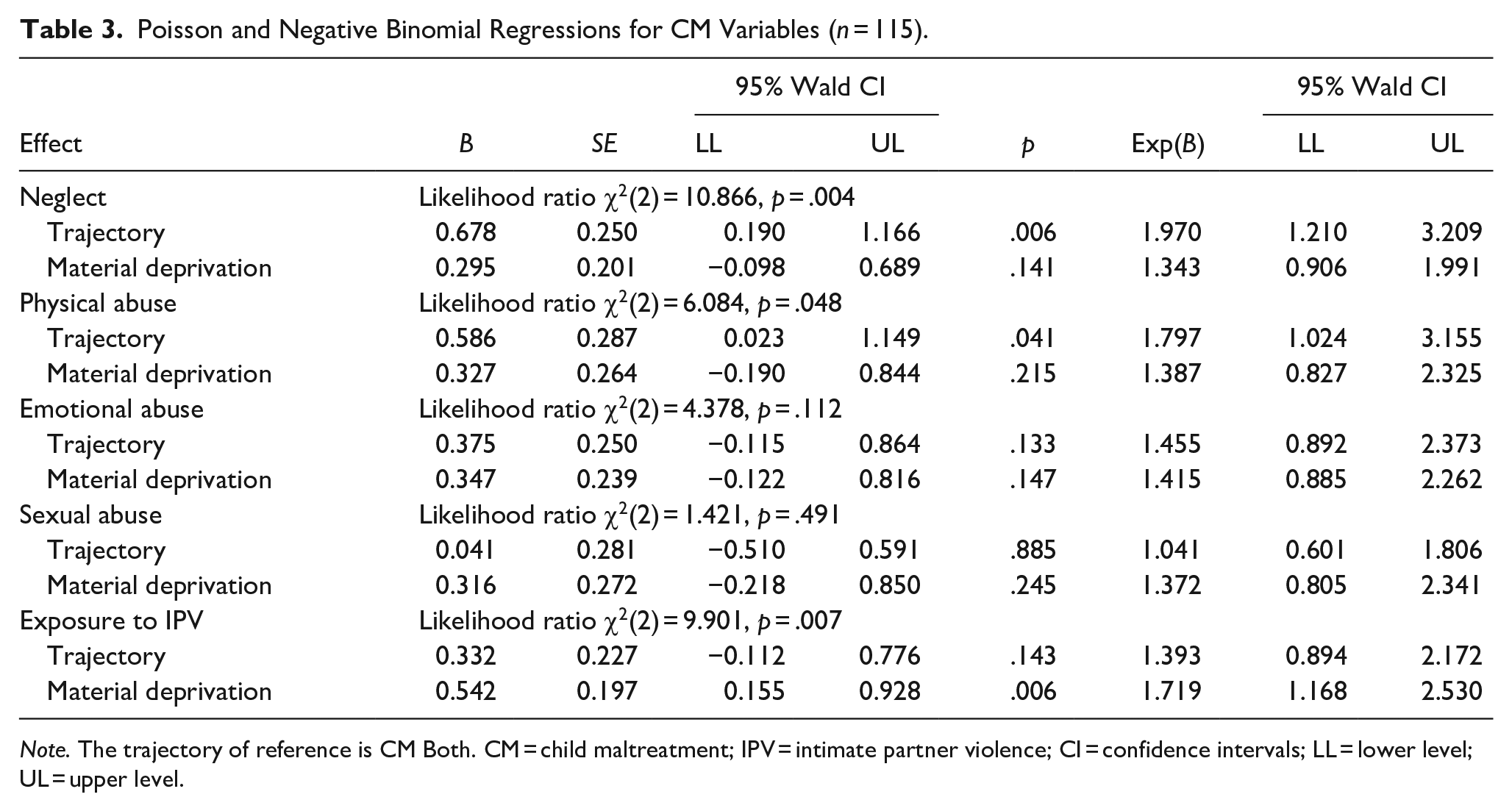
Note. The trajectory of reference is CM Both. CM = child maltreatment; IPV = intimate partner violence; CI = confidence intervals; LL = lower level; UL = upper level.
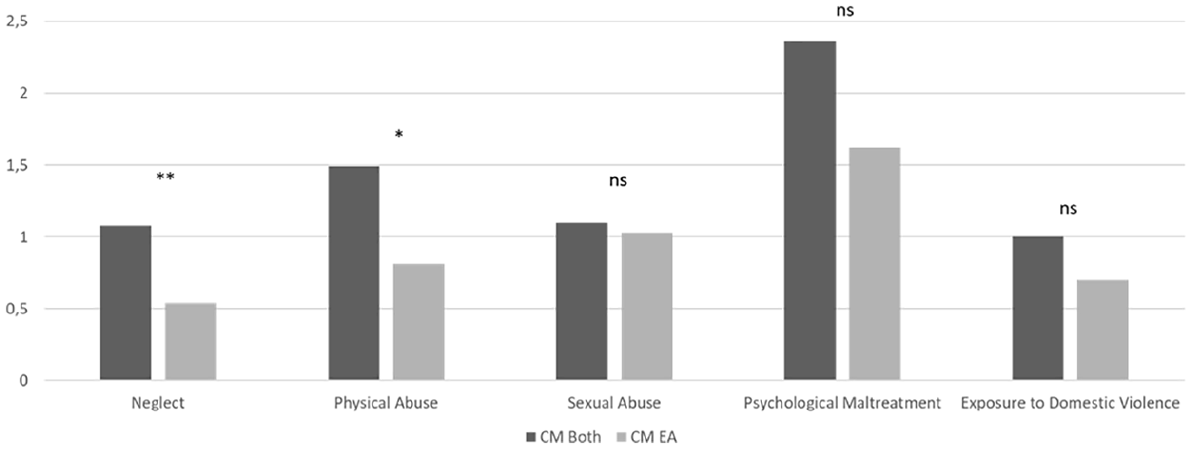
Differences in CM count scores for EA in the CM Both versus CM EA groups.
Adversity in Adulthood
To explore hypothesis 2 (see Figure 2 for a visual representation), Poisson regressions (interpersonal trauma) and negative binomial regressions (non-interpersonal adverse life events, IPV) were used to compare EA from the four trajectories on their levels of exposure to adversity in adulthood (count scores) while controlling for the presence of material deprivation (Table 4). Only comparisons between CM Both and CM EA (both groups with maltreated EA), and between CM Mothers and No CM trajectories (both groups with non-maltreated young adults) are presented here as these reflect the relevance of maternal histories of CM, hence of intergenerational trajectories of abuse.
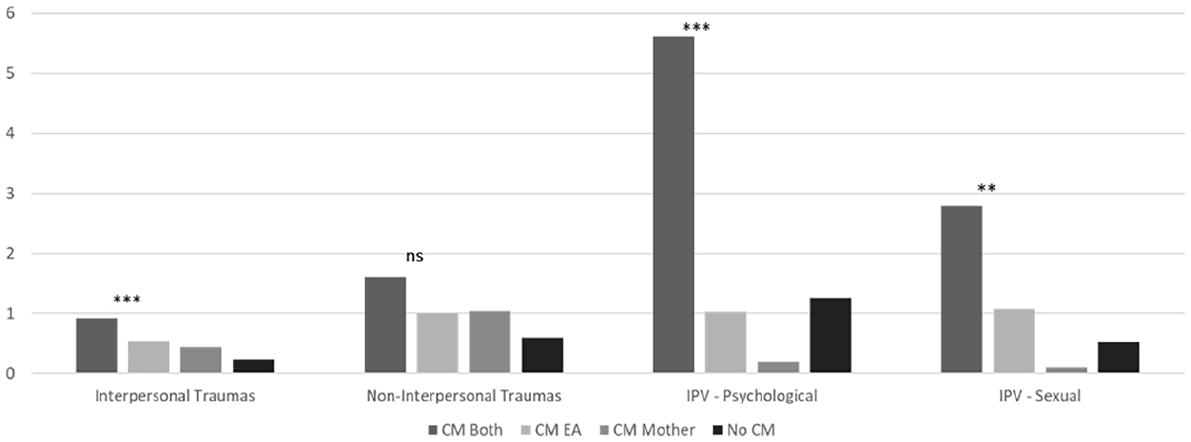
Group differences in count scores of adversity in adulthood.
Poisson and Negative Binomial Regressions for Adversity in Adulthood Variables.
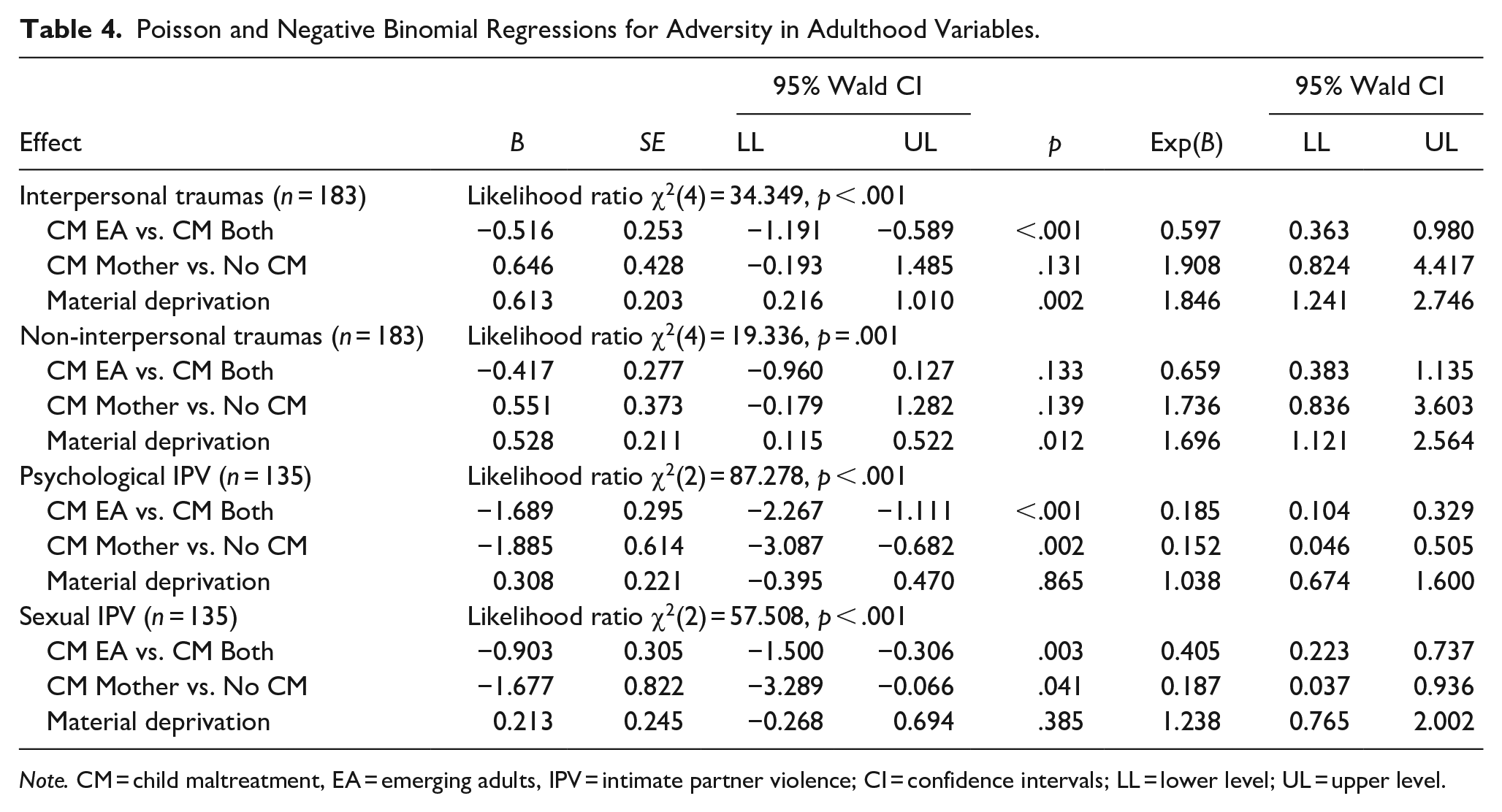
Note. CM = child maltreatment, EA = emerging adults, IPV = intimate partner violence; CI = confidence intervals; LL = lower level; UL = upper level.
The number of interpersonal traumas reported was significantly related to the presence of material deprivation (Exp(B) = 1.85) and to the intergenerational trajectory of CM. Specifically, EA from the CM EA trajectory reported fewer experiences of interpersonal trauma in adulthood than those from the CM Both (Exp(B) = 0.60); EA in the CM Mother trajectory reported almost twice as many experiences of interpersonal trauma in adulthood than young adults in the No CM trajectory (Exp(B) = 1.91). Thus, the presence of maternal histories of CM appeared to be associated with increased numbers of interpersonal traumas experienced in adulthood by EA. Conversely, no difference was found between CM EA and CM Both or between CM Mother and the No CM trajectories for EA’ experiences of non-interpersonal adverse life events in adulthood. However, material deprivation was related to a higher number of other adverse events experienced (Exp(B) = 1.70).
The number of reported experiences of psychological IPV in the past year was significantly related to the intergenerational trajectory of CM, but not to material deprivation. Specifically, EA from the CM EA trajectory reported fewer experiences of psychological IPV in the past year than those from the CM Both (Exp(B) = 0.19). EA in the CM Mother trajectory reported fewer experiences of psychological IPV in the past year than EA in the No CM trajectory (Exp(B) = 0.15). Similarly, the number of reported experiences of sexual IPV in the past year was significantly related to the intergenerational trajectory of CM, but not to material deprivation. EA from the CM EA trajectory reported fewer experiences of sexual IPV in the past year than those from the CM Both (Exp(B) = 0.41). Furthermore, EA in the CM Mother trajectory reported fewer experiences of sexual IPV in the past year than EA in the No CM trajectory (Exp(B) = 0.19). Overall, these results tend to indicate that EA with a history of CM are at risk of experiencing more frequent acts of psychological and sexual IPV if their mother is also a survivor of CM. However, a history of CM in mothers is associated with lower count scores of psychological and sexual IPV in dyads with non-maltreated EA, thus in cases of discontinuity of CM between generations.
Psychological Functioning
To address hypothesis 3, a MANCOVA was used to compare the four intergenerational trajectories of CM on EA’ psychological functioning (psychological distress, emotion dysregulation, posttraumatic stress symptoms). EA material deprivation was added as a covariate and the trajectory × deprivation interaction was tested. Only pairwise comparisons between CM EA and CM Both and between CM Mother and No CM trajectories are reported. Results are presented in Table 5.
Means, Standard Deviations, and MANCOVA Results for Psychological Functioning.
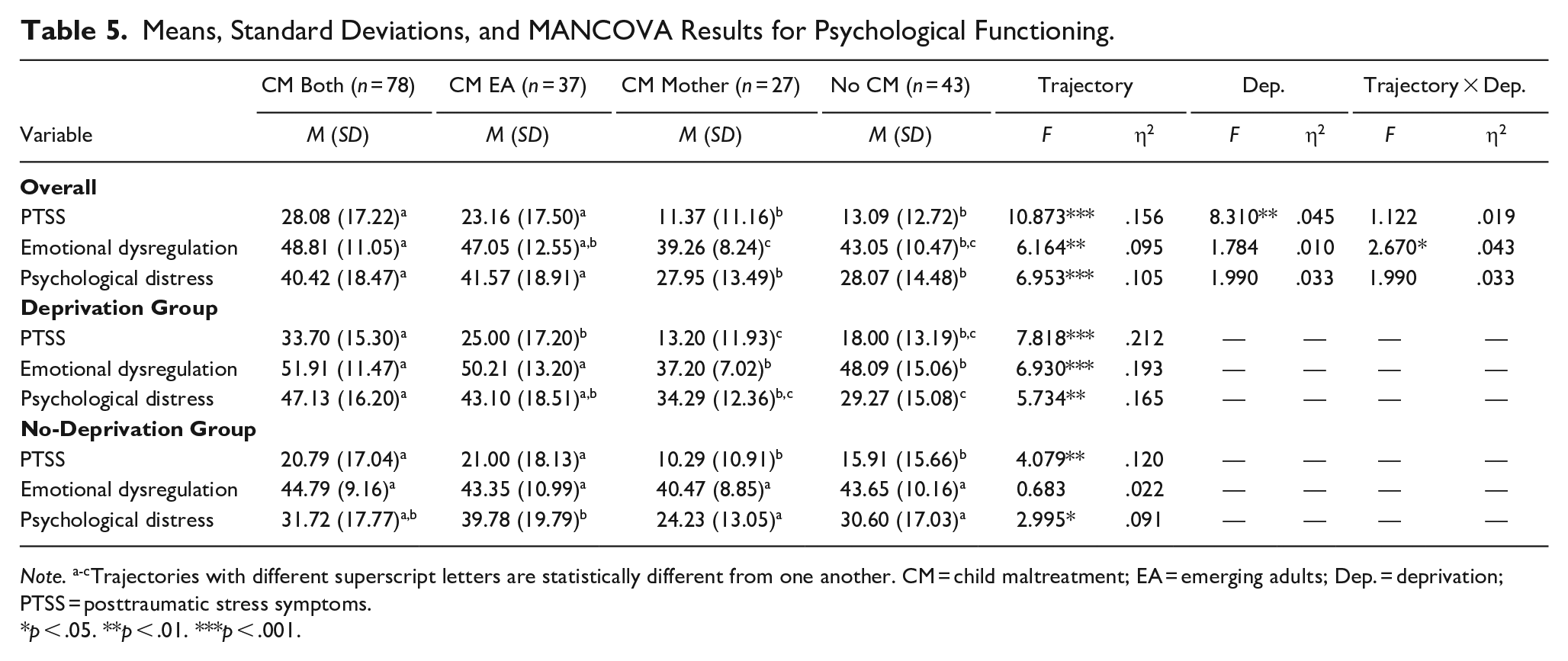
Note. a-cTrajectories with different superscript letters are statistically different from one another. CM = child maltreatment; EA = emerging adults; Dep. = deprivation; PTSS = posttraumatic stress symptoms.
p < .05. **p < .01. ***p < .001.
Pillai’s Trace multivariate test indicated a significant main effect of the trajectory (F (9, 531) = 4.679, p < .001; η2 = .073) and of material deprivation (F (3, 175) = 3.632, p = .014; η2 = .059), as well as a significant trajectory × deprivation interaction (F (9, 531) = 2.153, p = .024; η2 = .035). Tests of between subject effects revealed a significant trajectory difference on all dependent variables, while the main effect of material deprivation was only significant for posttraumatic stress symptoms and psychological distress. Conversely, the trajectory × deprivation interaction term was significant for emotional dysregulation only. No significant difference emerged between EA from the CM EA and CM Both trajectories and between EA from the CM Mother and the No CM trajectories in the pairwise comparisons. However, EA reporting material deprivation had higher scores of posttraumatic stress symptoms (Mdep. = 22.48; Mn-dep. = 15.49) and psychological distress (Mdep. = 38.45; Mn-dep. = 30.75) than EA without material deprivation. The examination of the interaction plot for emotional dysregulation indicated that for both trajectories including maltreated EA (CM Both and CM EA), material deprivation was associated with increased scores of dysregulation while scores of dysregulation for non-maltreated EA (CM Mother and No CM) appeared similar in the deprived and non-deprived groups.
To explore further the trajectory × deprivation interaction, separate MANCOVAs were run for each trajectory with material deprivation as the independent variable. In the CM Both trajectory, Pillai’s Trace multivariate test indicated a significant main effect of deprivation (F (3, 74) = 5.620, p = .001; η2 = .186), and between-subject effects revealed significant associations for posttraumatic stress symptoms (F (1, 76) = 12.365, p = .001; η2 = .140), emotional dysregulation (F (1, 76) = 8.760, p = .004; η2 = .103), and psychological distress (F (1, 76) = 15.947, p < .001; η2 = .173). In CM Both, deprived EA reported higher levels of posttraumatic stress symptoms (Mdep. = 33.74; Mn-dep. = 20.79), emotional dysregulation (Mdep. = 51.91; Mn-dep. = 44.79), and psychological distress (Mdep. = 47.13; Mn-dep. = 31.72) than non-deprived EA. In the other three trajectories (CM Mother, CM EA, No CM), Pillai’s Trace multivariate test indicated a non-significant effect of material deprivation (all ps > .05). Hence, material deprivation appeared associated with EA’ psychological functioning only for dyads where both mothers and EA have been maltreated in childhood.
Discussion
This study compared EA’ amount of exposure to maltreating and neglectful acts in childhood and to adverse events in adulthood based on their membership to distinct mother-EA trajectories of CM while accounting for material deprivation. Their psychological functioning was also compared. In a sample of primarily White female-identifying mother-EA dyads, our findings partially supported hypothesis 1 and suggested that a maternal history of CM was associated with greater numbers of neglectful and physically abusive acts endured in childhood for maltreated EA, but not with the numbers of sexually and emotionally abusive acts sustained, or with the amount of exposure to IPV. These findings enhance our understanding of intergenerational trajectories of CM by suggesting that a maternal history of CM might not only be associated with an increased risk of CM in the next generation (Langevin et al., 2021; van IJzendoorn et al., 2010), but might also be associated with increases in the amount of exposure to CM, especially for physical abuse and neglect. Theoretical models of intergenerational continuity of CM emphasize the enduring negative impacts that all types of CM have on mental health and on individuals’ ability to form safe, stable, secure, and nurturing relationships, and the subsequent implications for the caregiving context (Marshall et al., 2022; Noll et al., 2017). In addition, financial and housing insecurity as well as social service inaccessibility (both experienced disproportionally by marginalized communities) can increase parenting stress and affect parent to child relations (Luken et al., 2021; Roberts et al., 2011). The long-term impacts of CM and the associated familial contextual factors could explain why a maternal history of CM was associated with an increase in the levels of exposure to CM in EA. However, findings were only significant for some types of CM, emphasizing the importance of adopting a fine-grained approach instead of using a broad category of CM when investigating such associations. Intergenerational trajectories of child sexual abuse and exposure to IPV are somewhat distinct from other intergenerational patterns as they often involve victim-to-victim cycles wherein the abused parent is not the perpetrator of the child’s abuse (Baril & Tourigny, 2016; Marshall et al., 2022). This might partly explain our findings. Furthermore, child sexual abuse is a unique type of CM, as it does not necessarily involve an intrafamilial perpetrator. Future studies should explore the associations between maternal histories of CM and EA’ intra versus extrafamilial histories of sexual abuse. Moreover, maternal histories of CM were not associated with the amount of exposure to emotional abuse in EA. Past studies have found associations between emotional abuse and primary caregivers’ history of CM, mental health problems, and substance use (e.g., Chamberland et al., 2012). However, it is quite possible that while there is an increased risk of emotional abuse for children of maltreated mothers, the risk for more severe exposure is not greater based on maternal CM. Anyhow, additional studies are needed to gain a clearer understanding of the specific patterns of associations with CM types uncovered in the present study, especially in more diverse samples.
Regarding adversity in adulthood, our findings partially supported hypothesis 2 by indicating that the presence of maternal histories of CM, regardless of the victimization status histories of the EA, was associated with an increase in EA’ number of interpersonal traumas experienced in adulthood. Conversely, no difference was found for non-interpersonal adverse life events. This is in line with the “single generation” literature showing increased risk of interpersonal revictimization for victims of CM (Widom et al., 2008), but advances our knowledge by highlighting that this increased risk might surpass generations. Vulnerability to interpersonal victimization appears to be transferred to the next generation and various mechanisms could be at play in this transfer, including vicarious learning, heritability, and environmental factors. As such, a longitudinal twin study (Fisher et al., 2015) reported significant but modest heritability for maltreatment and neglect, crime, and peer and siblings victimization in their sample. However, victimization experiences appeared to be more strongly explained by nonshared risky environments than by heritable characteristics (Fisher et al., 2015). Again, the long-lasting impacts of CM on mental health, relationships, parenting, and the parenting context, could explain this transfer of risk from mothers to EA (Marshall et al., 2022), but studies directly exploring mechanisms of transfer in diverse populations are needed to confirm these hypothesized pathways.
Similarly, our results showed that EA with a history of CM were at risk of experiencing more frequent acts of psychological and sexual IPV when their mother was also a survivor of CM. However, non-maltreated EA seemed to benefit from the protective effect of having a mother that survived CM, but that was able to interrupt intergenerational cycles of CM. Indeed, non-maltreated EA were less likely to experience sexual and psychological IPV if their mother reported a history of CM (CM Mother vs. No CM). According to Langevin et al.’s (2021) review, some parental factors protecting against the intergenerational continuity have been identified in the literature including being older, having participated in therapy, greater self-control, positive and supportive relationships in childhood and adulthood, and effective communication with children. Some of these factors could also play a role in the prevention of dating violence victimization in EA (Hébert et al., 2019; Kaukinen, 2014). Furthermore, overcoming a history of CM and breaking intergenerational cycles mean demonstrating resilience (Schelbe & Geiger, 2017) and could even lead to posttraumatic growth for some mothers (Joseph & Linley, 2006). These (acquired) strengths, that could have helped maltreated mothers prevent CM of their children, could also be related to the modeling of positive intimate relationships, and to the development of an increased ability to identify risky situations and act accordingly to, potentially, prevent second generation’s IPV victimization (Schelbe & Geiger, 2017; Spencer et al., 2020). For instance, positive posttraumatic changes could include explicit parenting efforts to minimize harmful relational conflict (Fava et al., 2016), which can in turn reduce the risk for their children to perceive aggression as justifiable in intimate relationships (Collins et al., 2009). Nevertheless, given the characteristics of our sample, it is possible that this finding is more relevant for female-identifying EA compared to other genders. In addition, resources promoting resilience and post-traumatic growth may be more limited to marginalized communities. Further research is needed to explore the generalizability of this protective effect.
Contrary to hypothesis 3, results were less clear regarding the association of intergenerational trajectories of CM in mother to EA dyads and EA’ posttraumatic stress symptoms, emotional dysregulation, and psychological distress; the greater exposure to physical abuse and neglect in childhood and to interpersonal traumas in adulthood for EA with a maltreated mother was not related to greater psychological difficulties. Indeed, no difference emerged between maltreated EA or between non-maltreated EA as a function of the maternal history of CM in pairwise comparisons. Yet, past studies have identified that maltreated and non-maltreated children of maltreated mothers presented greater behavior problems than children of non-maltreated mothers, and that a history of maternal child sexual abuse was associated with greater behavior problems and dissociation in sexually abused children (Borelli et al., 2019; Langevin, Hébert, et al., 2022). However, these studies included children and their findings might not hold with adult populations. It is also possible that additional mediating and moderating factors, such as adulthood revictimization (Balsam et al., 2011), participation in therapy (Van der Put et al., 2018), or the presence of supportive relationships (Folger et al., 2013) would need to be included to clarify under which conditions a maternal history of CM might impact EA’ psychological functioning (Afifi & MacMillan, 2011; Yoon et al., 2019). In line with this hypothesis, the trajectory × deprivation interaction was significant and further exploration revealed that maltreated EA with maltreated mothers (CM Both) living in contexts of material deprivation reported greater psychological difficulties than those not living in such contexts. Material deprivation was not significant in the other three trajectories. This finding once again emphasized the importance of socioeconomic contexts in understanding mental health outcomes for maltreated individuals (Zielinski & Bradshaw, 2006). It aligns with the concept of synergistic effects of multiple forms of adversity brought forward by Putnam et al. (2013) showing that the cumulative impact of two or more types of adversity on complex adult psychopathology is greater than the sum of their individual effects. Indeed, the EA in our sample showing the worst mental health outcomes were characterized by three layers of adversity: having a mother with a history of CM, having their own history of CM, and living in socioeconomically disadvantaged contexts. As racial minorities are disproportionally affected by poor socioeconomic conditions, as well as social marginalization and discrimination, there are most likely additional layers of adversity exacerbating mental health concerns in racialized communities (Lanktree et al., 2012). Future studies could examine minority stress as another factor affecting families with intergenerational occurrences of CM.
Finally, material deprivation alone was significant in some of our analyses with higher levels of deprivation related to increased exposure to IPV in childhood as well as to interpersonal traumas and non-interpersonal adverse life events exposure in adulthood. Results also revealed higher scores of posttraumatic stress symptoms and psychological distress for EA living in a financially difficult situation. These findings are in line with past studies highlighting that socioeconomic disadvantage is a risk factor for exposure to adverse life events including CM (Conrad-Hiebner & Byram, 2020; van IJzendoorn et al., 2010), and for negative mental health outcomes such as depression, anxiety, and posttraumatic stress (Belle, 1990; Ridley et al., 2020).
Limitations and Implications
This innovative study provided highly relevant information on the associations between maternal histories of CM and trauma exposure and psychological functioning in EA with and without a history of CM. It had several strengths, including a dyadic design, a respectable sample size, the use of validated measures, the consideration for material deprivation, and a rigorous statistical approach. Notwithstanding these contributions, some limitations should be mentioned. First, the cross-sectional design did not allow to ascertain the directionality of the effects. Second, as the current study primarily recruited from Canadian universities and colleges, the convenience sample had low diversity in terms of gender, income (and material deprivation), education, and cultural backgrounds; limiting the generalizability of study findings. Third, the exclusion of fathers additionally limited the scope of our findings. Fourth, while the total sample size was respectable, some intergenerational trajectories had low counts of participants. Finally, the use of retrospective and short self-report measures of CM, measures that did not allow to identify who perpetrated the maltreatment, was not without limitations. Retrospective self-reports can introduce bias; short measures restrict the sensitivity; not knowing the perpetrator’s identity limits our ability to describe the intergenerational dynamics present for our mother-EA dyads. The cut-off of one positive item to be included in the CM category resulted in high counts of participants considered maltreated even after excluding highly endorsed items. Future studies should replicate our findings while filling some of these gaps by using prospective longitudinal designs, recruiting a larger more diverse and representative sample of the population, including fathers/parents from non-heteronormative or gender conforming families and using a combination of self- and official reports of CM. Since marginalized communities can be at greater likelihood to experience intergenerational patterns of CM due to systemic discrimination and less preventative and harm reduction resources, future studies should intentionally recruit samples with greater representation of the population as a whole. Qualitative or mixed methods studies could be valuable in providing an in-depth understanding of the mechanisms underlying different CM trajectories. Furthermore, clarifying some of the findings would be important, such as understanding why the amount of exposure did only differ for physical abuse and neglect. Uncovering pathways involved in the association between parental histories of CM and EA’ CM, adulthood victimization, and psychological functioning using path models with mediators and moderators would also be necessary. Factors such as parents’ relationship functioning, mental health, parenting, and neurobiology would be relevant to examine (Langevin et al., 2021; Marshall et al., 2022).
While our findings should be confirmed through replication with methodologically strong designs and diverse samples, some practical and policy implications are worth mentioning. Practitioners working with children at-risk or exposed to CM should document parents’ histories of CM and take that into account in their assessments and intervention practices. Targeting parents themselves might be appropriate in some cases to interrupt intergenerational cycles of CM and protect the next generation not only against CM, but also against IPV victimization. However, social policies targeting the family system and placing families at the heart of their interventions instead of focusing on individuals (parent or adolescent/EA) seems promising. Furthermore, as a parental history of CM appears to be associated with a greater risk of adulthood interpersonal victimization in EA, universal or targeted validated prevention programs could be offered to parents and adolescents to help them escape this transfer of risk and foster positive intimate relationships as soon as they emerge (e.g., Crooks et al., 2019). To conclude, given the important role of material deprivation, public policies and community resources fighting poverty and offering affordable high-quality therapeutic services to young victims of CM or new parents with a history of CM could be invaluable vectors of intergenerational resilience.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported by grants from the Social Sciences and Humanities Research Council of Canada and the Fonds de recherche du Québec—Société & Culture obtained by Dr. Langevin. Audrey Kern received a doctoral scholarship from the Fonds de recherche du Québec—Santé. We wish to thank the participating families without whom this project would not have been possible.