
Abstract
Research focusing on the role of adverse childhood experience (ACE) of individuals involved in sexual homicide (SH) is scarce. Theoretical models of SH have postulated a connection between these adverse experiences and the development of internal risk factors. However, such assumptions have never been empirically tested. Therefore, the current research aims to identify how ACEs affect the development of personality disorders and problematic behaviors during adolescence, which constitute internal risk factors for the commission of SH. The sample comes from a database including 613 individuals involved in sexual crimes in Canada among which 60 committed a SH. Bivariate and multiple regression analyses were conducted to identify personality disorders and problematic behaviors during adolescence associated with the presence of ACEs. Next, path analysis was used to identify the direct and indirect relationships between ACEs, internal risk factors, and the commission of SH. Results showed that individuals who experienced ACEs were more likely to develop internal risk factors involved in the commission of SH. Moreover, findings suggest that the impact of these adverse experiences will differ, depending on whether the child has been victim of violence or if he/she has witnessed it.
Keywords
Introduction
The past two decades have seen an increase in the research on sexual homicide (SH). Due to the availability of larger databases, researchers have been able to test several hypotheses regarding SH and the offenders who perpetrate it (Beauregard & DeLisi, 2018; Chopin et al., 2020; DeLisi & Beauregard, 2018). However, most of these studies have focused on the crime-commission process adopted by these offenders, overlooking the various conceptual and developmental mechanisms that could lead some offenders to kill their victims during or following a sexual assault. Three theoretical models have been proposed over the years to explain SH include the motivational model (Burgess et al., 1986), the trauma control model (Hickey, 1997), and the integrated paraphilic model (Arrigo & Purcell, 2001; Purcell & Arrigo, 2006).
Largely influenced by the social learning perspective, all three models identify the presence of a criminogenic environment during childhood as the origin of SH. Moreover, an integrated conceptual framework combining social learning and routine activities theories have been proposed and partially supported (Chan, 2015; Chan et al., 2011). The presence of violence and abuse (physical, psychological, and sexual) in the family—whether witnessed or experienced directly by the individual—was believed to impede the child’s development, resulting in the adoption of antisocial methods for expressing their needs and hostility, and leading to social isolation (Chan, 2015; Chan et al., 2011; Hickey, 1997; Ressler et al., 1988). These adverse childhood experiences (ACEs) contribute to the development of a deviant behavioral learning process, which could result in the child internalizing deviant and aggressive attitudes that they have been exposed to over an extended period of time (Chan, 2015) as well as becoming socially isolated with low self-esteem (Arrigo & Purcell, 2001).
Following the unresolved trauma resulting from these ACEs, it was suggested that some individuals would retreat into a fantasy world, which is a socially acceptable way to cope with the feelings of helplessness and gain absolute control over their lives (Burgess et al., 1986). However, unable to cope with stressful situations, these individuals develop problematic behaviors in childhood, such as feelings of anger, low self-esteem, and social isolation, driving them to retreat into a world of deviant sexual fantasies (Arrigo & Purcell, 2001), which serves as a mechanism to regain control of their lives and achieve dominance, both of which are missing from their reality. Because of the over-reliance on their fantasy lives, the individuals are unable to develop prosocial bonds, which subsequently lead to the development of negative personality traits. This rich fantasy life of the offenders becomes increasingly ineffective at satisfying their needs, and the offenders begin to act out, adopting deviant and criminal behavior, escalating from such crimes as arson and animal abuse during childhood, to the commission of a SH in adulthood (Burgess et al., 1986)
Despite theoretically sound propositions, these models have not been tested empirically. Partly due to their complexity, researchers have been unable to investigate all the mechanisms involved in the commission of a SH. Nonetheless, it is possible to examine some of these mechanisms to better understand the origin of SH. Therefore, the current study examines how traumatic childhood experiences affect the development of personality disorders and problematic behaviors during adolescence, which constitute internal risk factors for the commission of a SH.
Developmental Sequela
The developmental psychopathology perspectives propose a framework to explain the relationship between ACEs during the early stages of human development and the emergence of subsequent disorders (Cicchetti & Banny, 2014; Levenson & Socia, 2016). This theoretical approach suggests that positive and negative experiences affect the dynamic interactions between affective and cognitive processing that shape the personality and behavioral adaptation patterns of individuals (Rutter & Sroufe, 2000). The development occurs as a succession of stages. Each stage of development includes a set of skills that will irrevocably condition the acquisition of skills in the next stage of development. When the normal acquisition of skills is disrupted by adverse experiences, the developmental process is impaired resulting in the cultivation of personality disorders and maladaptive behaviors (Cicchetti & Banny, 2014; Cicchetti et al., 2012; Rutter & Sroufe, 2000). Several studies document linkages between ACEs and both internalizing and externalizing disorders (see, e.g., Afifi et al., 2011; Chopin et al., 2022; Cicchetti & Banny, 2014; Cicchetti et al., 2012; Johnson et al., 1999; Luntz & Widom, 1994; Widom, 1998).
From this perspective, ACEs serve as precursors of personality pathology (Cicchetti & Banny, 2014). For example, Luntz and Widom (1994) indicated that being victimized and/or neglected during childhood impacted positively both the presence and the number of symptoms of antisocial personality disorder. Widom (1998) replicated this study with a larger sample and confirmed that the antisocial personality diagnosis was significantly associated with childhood victimization for both males and females. Similarly, Johnson et al. (1999) compared the prevalence of personality disorders among childhood victimized individuals and a control group of non-victimized individuals, showing that antisocial, borderline, narcissistic, and passive-aggressive personality disorders were more frequently found among individuals who had been abused or neglected during childhood. Cluster C personality disorders (i.e., avoidant, dependent, obsessive-compulsive) were more likely to be diagnosed in individuals who experienced childhood abuse or neglect (Johnson et al., 1999). More recent studies confirmed the existence of a significant relationship between negative childhood experiences—and their severity—and cluster B personality disorders (Afifi et al., 2011; Bohle & de Vogel, 2017). However, studies were unable to establish a link between the type of childhood victimization (i.e., emotional abuse/neglect, physical/sexual abuse) and the presence of Cluster A, B, and C personality disorders (Tyrka et al., 2009).
Other researchers examined the link between early ACEs and adult criminal offending. These studies showed that childhood victimization rates were significantly higher among incarcerated individuals than the general population (e.g., Dierkhising et al., 2013; Levenson et al., 2014), suggesting that individuals who have had traumatic experiences in their childhood were more likely to be involved in sexual offending (e.g., Drury et al., 2019; Krahé & Berger, 2017; Miley et al., 2020). Moreover, some studies identified a relationship between polyvictimization during childhood and the severity of sexual crimes perpetrated during adulthood (Finkelhor et al., 2007). These studies found that polyvictimization during childhood constitutes a risk factor for engaging in more severe sexual offending later in life. For instance, Leach et al. (2016) found that violent sexual and non-sexual assaults in adulthood were more likely to be associated with childhood polyvictimization, while King et al. (2019) found that individuals who were polyvictimized as children were more likely to commit completed rapes than those who were not. DeLisi and Beauregard (2018) demonstrated a clear relationship between traumatic childhood experiences and involvement in SH, showing that polyvictimized individuals and those who were exposed to several traumatic childhood experiences (i.e., witnesses) presented a significant higher probability of committing a SH.
SH Offenders and Personality Disorders
Although not explicitly specified, the theoretical models of SH suggested that in order to commit such a crime, offenders have to present some form of psychopathology ranging from various personality disorders (e.g., antisocial, borderline), to psychopathy to severe psychosis (Malmquist, 2007). The dominant personality feature often associated with SH has been psychopathy (e.g., Declercq et al., 2012; Myers et al., 2005). Porter et al. (2003) found that almost 85% of the SH offenders (SHOs) scored in the moderate-high range on the Psychopathy Checklist–revised (PCL-R; Hare, 1991). In addition, Firestone et al. (1998) found that SHOs presented significantly higher PCL-R scores—both on Factor 1 and 2—than a control group of incest offenders as well as they were more likely to be diagnosed with any personality disorder—and with antisocial personality disorder in particular. Despite these empirical findings, other studies raised some doubts as to the relationship between psychopathy and SH (see Langevin et al., 1988).
Different personality disorders are linked to the commission of a SH. Drawing on work by DeLisi and Wright (2014) who suggested that low self-control could partly explain SH, Healey and Beauregard (2017) tested one specific component of this concept—namely impulsivity—and found that it was significantly associated with SH, even after taking into account various crime characteristics. Among a different sample of SHOs, Meloy (2000) observed significant evidence of psychopathy and antisocial personality disorder in addition to higher levels of obsession, as well as moderate levels of formal thought disorder, which are compatible with a Borderline personality (see Gacono & Meloy, 1994; Meloy et al., 1997). Similarly, Schlesinger (2004) found that compulsive SHOs were usually psychopaths, whereas catathymic SHOs were more likely to present borderline and schizoid personality disorders. Hill et al. (2006) found that offenders with sexual sadism were more often diagnosed with personality disorders than the group without sexual sadism, such as antisocial, narcissistic, borderline, schizoid, and schizotypal personality disorders. Moreover, Proulx and Sauvêtre (2007) observed that when using the DSM-IV criteria, the most commonly diagnosed personality disorders among SHOs were antisocial, borderline, and narcissistic disorder. However, they also looked at the scores obtained on the MCMI and contrary to the clinical diagnoses, the psychometric instrument indicated a predominance of avoidant, dependent, and schizoid personality disorders among SHOs. According to Proulx and Sauvêtre (2007, p. 65), such discrepancy between clinical diagnoses and the psychometric results could be “a reflection of the fact that psychometric instruments evaluate the sexual murderer, while clinicians evaluate the crime itself.”
Given the discrepancies in the personality profiles associated with SH, Beauregard and DeLisi (2021) compared three groups of sex offenders—SHOs, non-violent, and violent sex offenders—and found that the personality profile of SHOs was comprised primarily of Schizoid and Borderline Personality Disorders and that the comorbidity between these three personality features presented unique personality dysfunction that facilitates the lethal sexual violence of SHOs compared to non-homicidal sex offenders.
Aim of Study
On one hand, theoretical models of SH have postulated a connection between ACEs, personality disorders, the adoption of problematic behaviors, and the commission of a SH. However, they lack empirical verification. On the other hand, empirical studies have examined the relationships between these same factors but individually, thus neglecting the potential relationships between all of these factors. Adopting an integrative and multifactorial perspective approach is imperative. Therefore, the current purpose is to identify the indirect links that exist between ACEs and SH. Specifically, we aim to identify how traumatic childhood experiences affect the development of personality disorders and problematic behaviors during adolescence that constitute internal risk factors for the commission of SH. This integrated approach would allow us to better understand the developmental dynamics associated with the commission of severe sexual crimes and help guide therapeutic approaches for clinicians working with child victims (e.g., identifying risk factors) or individuals involved in SH (e.g., understanding the developmental process from a therapeutic perspective).
Methodology
Sample
The sample used in this study comes from a prospective study on the recidivism of individuals involved in sexual crimes in Canada. The data collection took place in a federal penitentiary between 1994 and 2000. The database used in this study included 613 individuals who received a prison sentence of at least 2 years. The participation rate is considered as high with 93% of participants who agreed to participate. All participants signed a consent form mentioning that data collected would be used for research purpose only. In the sample, 553 individuals were convicted for non-lethal sexual crimes, while 60 were convicted for having perpetrated a SH. Because there is no legal definition of SH, the FBI definition by Ressler et al. (1988) was used. This definition states that to be considered as sexual, a homicide should include a least one of the following elements: (a) victim’s attire or lack of attire, (b) exposure of the sexual parts of the victim’s body, (c) sexual positioning of the body, (d) insertion of foreign objects into the victim’s cavities, (e) evidence of sexual intercourse (oral, anal, or vaginal), and (f) evidence of substitute sexual activity, interest, or sadistic fantasy.
Measures
Response variable
Previous studies identified that childhood victimization and polyvictimization constitute a risk factor for engaging in severe sexual offending later in life (DeLisi & Beauregard, 2018; King et al., 2019; Leach et al., 2016). We used two response variables (i.e., see the detailed distribution in Online Appendix 1) to operationalize the concept of ACEs: (1) childhood victimization and (2) exposure to victimization. In order to respect the causal order, we made sure for these two variables that the first traumatic event occurred before the age of 12. Childhood victimization (x̄ = 1.17, SD = 1.19, range = 0–5) is a count measure of victimization experiences occurring prior to age 12. These included the following four dichotomous items (no = 0, yes = 1): victim of psychological violence, victim of physical violence, victim of incest, and victim of sexual contact. Exposure to violence (x̄ = 1.31, SD = 1.35, range = 0–6) is a count measure of violence exposure occurring prior to age 12. This variable refers specifically to witnessing victimization and is different from victimization. These included the following six dichotomous items (no = 0, yes = 1): exposure to psychological violence, exposure to physical violence, exposure to pedophilia, exposure to rape, exposure to incest, and exposure to sexual violence.
Explanatory variables
Three types of explanatory variables were used: personality disorders, problematic behaviors during adolescence, and the crime lethal outcome.
The psychopathology developmental approach suggests an association between ACEs and the development of personality disorders (Cicchetti & Banny, 2014). Moreover, studies found an association between the presence of specific personality disorders among SHOs (Beauregard & DeLisi, 2021). To examine whether personality disorders may be related to ACEs and SH, we used 10 dichotomous variables (0 = absence; 1 = presence) divided into the three personality disorders cluster: Cluster A—Eccentric, Cluster B—Dramatic, and Cluster C—Anxious. The Eccentric cluster includes the following variables: (1) paranoid, (2) schizoid, and (3) schizotypal. The Dramatic cluster includes the following variables: (4) antisocial, (5) borderline, (6) histrionic, and (7) narcissistic. Finally, the Anxious cluster includes the following variables: (8) avoidant, (9) dependent, and (10) obsessive-compulsive.
All individuals included in our sample were referred to a psychologist. Before meeting with the psychologist, they were administered the Minnesota Multiphasic Personality Inventory-II (MMPI-II). Results to this test were made available to the psychologist before meeting with the offender. Through a structured clinical interview, the psychologist would reach his diagnosis using mainly the DSM-IV criteria, as well as the results to the MMPI-II and official information included in the correctional file. Unfortunately, scores to the PCL-R were not available for the purpose of this study.
Previous studies highlighted that individuals who engaged in problematic behaviors during adolescence were more likely to be involved in a SH (Beauregard & DeLisi, 2018). To determine whether problematic behaviors during adolescence may link ACEs, personality disorders, and SH, we used two continuous variables: (11) internalized problematic behaviors (x̄ = 2.09, SD = 1.79, range = 0–7) and (12) antisocial problematic behaviors (x̄ = 1.68, SD = 1.55, range = 0–6). To ensure temporal causality, we made sure to consider only behaviors that occurred between 12 and 17 years of age. To create these two variables, we conducted a factorial analysis with 13 dichotomous variables describing specific problematic behaviors that occurred during the individuals’ adolescence (see Online Appendix 2). According to the Cattell method, it appeared that the best solution consisted of regrouping the 13 variables in two dimensions (see Online Appendix 3). The variable of internalized problematic behaviors is a scale created from the following dichotomous variables: daydreaming, social isolation, enuresis, poor self-image, phobias, nightmares, and sleep disorders (Cronbach’s α = 0.75). The variable of antisocial problematic behaviors is a scale created from the following dichotomous variables: chronic lying, rebellious attitude, anger temperament, reckless behavior, running away, and auto mutilation (Cronbach’s α = 0.65). According to previous research suggesting an association between ACEs and the presence of alcohol/drug abuse during adolescence (Widom et al., 2006), we included the following variable as well: (13) alcohol/drug abuse during adolescence (i.e., DSM-IV diagnosis of a use having started between 12 and 18 years of age).
Finally, previous studies suggested an association between ACEs (DeLisi & Beauregard, 2018), personality disorders (Beauregard & DeLisi, 2021), and problematic behaviors during adolescence (Beauregard & DeLisi, 2018) with the commission of SHs. In order to examine the role of these three components on the commission of lethal sexual crimes, we used one dichotomous variable: (14) individual perpetrated a SH.
Procedure
Data were mainly collected through semi-structured interviews using a computerized questionnaire. The questionnaire included information on numerous aspects of the offender’s life and criminal activity including pre-, peri-, and post-crime behaviors, attitudes regarding their crimes, victimology, developmental factors, and psychiatric diagnoses. Self-reported information was corroborated with official psychiatric and behavioral history information in the offender’s institutional file. Inter-rater agreement was measured on the basis of 16 interviews (and consultation of official documentation) conducted jointly by two raters. Ratings were done independently following these interviews, which were conducted by one interviewer in the presence of the other. There was excellent agreement between raters (Cohen’s κ = 0.87). Moreover, all personality disorders were obtained from the psychologist in charge of the assessment of the offender using the DSM-IV.
Participants
Table 1 presents descriptive statistics of both response and explanatory variables that were used in this study. Individuals included in the sample experienced an average of 1.17 victimization events during their childhood and were exposed to an average of 1.48 victimization events in their lifetime. These individuals presented paranoid personality disorders in 6.70% of cases, schizoid in 1.63% of cases, and schizotypal in 0.16% of cases. For 32.46% of them an antisocial personality disorder was diagnosed, borderline for 15.82% of them, histrionic for 2.28% of them, and narcissistic for 22.19% of them. The diagnosis of avoidant personality was established for 20.72% of the individuals included in our sample, that of dependent personality for 44.05% of them, and obsessive compulsive for 3.10% of them. As to the problematic behaviors identified during adolescence, the individuals included in the sample had an average of 1.68 antisocial problematic behaviors and 2.09 internalized problematic behaviors. Moreover, 67.70% of them had a problematic use of alcohol and/or drugs during adolescence. Finally, 9.31% of them were involved in a SH.
Descriptive Statistics (N = 613).
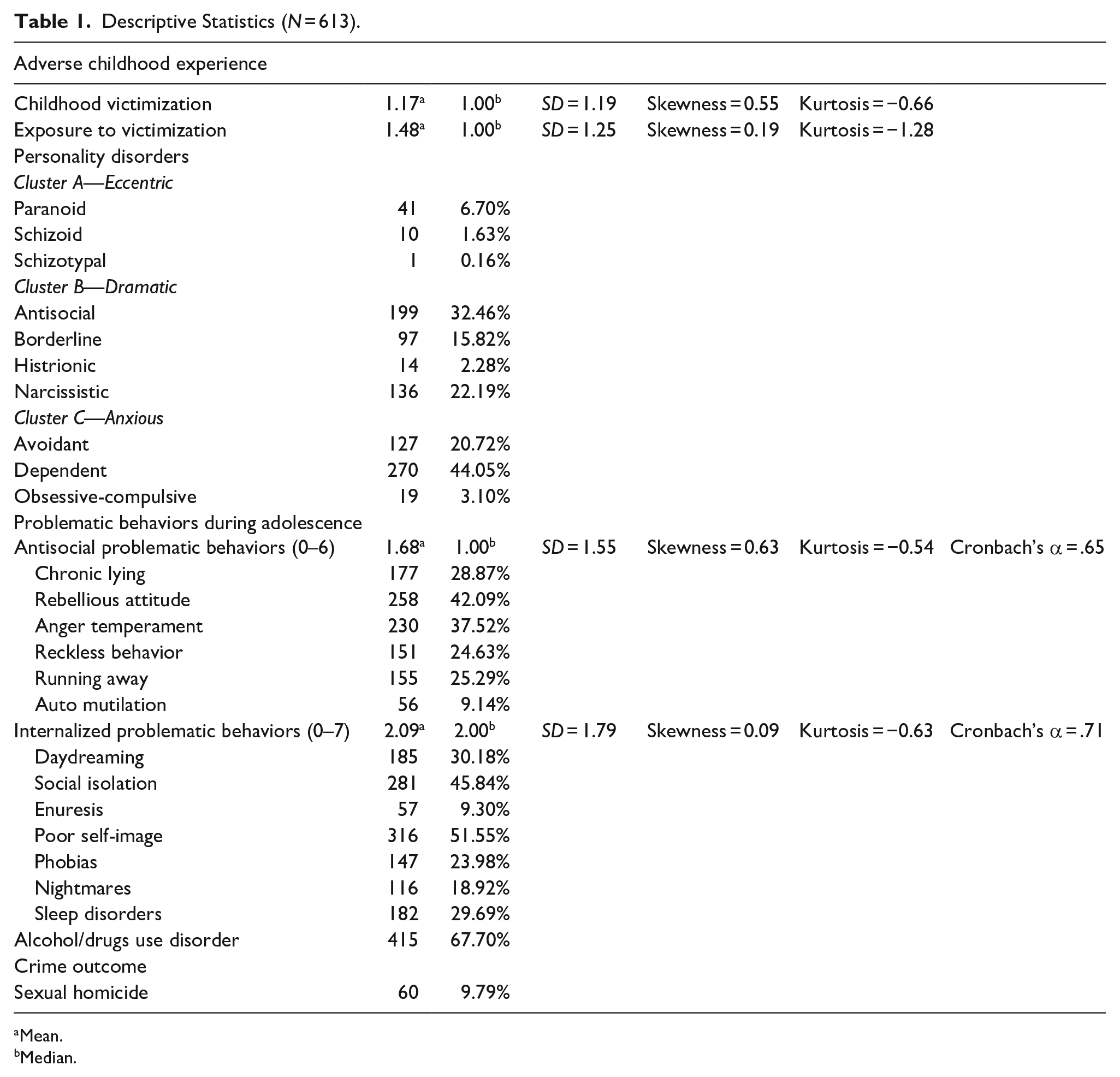
Mean.
Median.
Analytical Strategy
Following a psychopathological developmental approach, we specifically aimed to determine how ACEs may influence the development of personality disorders and problematic behaviors during adolescence, which are more likely to characterize individuals involved in SH. To explore the complexity of the interactions between these different components, we followed a three-step process. First, a bivariate comparison (i.e., analysis of variance) between the set of explanatory variables (i.e., personality disorders, problematic behaviors, SH) and the number of childhood victimization and exposure was conducted. Second, using only the significant variables at the bivariate level (Tabachnick & Fidell, 2019), we performed multiple linear regression analysis. The goal was to determine whether the number of different childhood victimization (i.e., polyvictimization) and exposure to victimization was associated with exploratory variables at the multivariate level. The regression method is often used for two main analyses: prediction and causal (Allison, 1999). In a prediction study, the goal is to develop a formula for making predictions about the response variable based on the observed values of the explanatory variables. For causal analysis, the explanatory variables are assumed to be causes of the response variable. Causal analysis was used in this study, in which childhood victimization variables represented the cause of explanatory variables. Finally, an exploratory path analysis was used to determine the direct and indirect associations between ACEs (i.e., childhood victimization and exposure to victimization) and the variables of interest. This exploratory model aimed to test the application of the developmental psychopathology theory to individuals involved in SH. Specifically, the goal was to determine whether ACEs were associated with the development of specific personality disorders, which would have shaped problematic behaviors during adolescence, leading to the commission of SH (see Figure 1). Standardized path coefficients (β) for both the direct and indirect effects were estimated using 2000 bootstrap samples. Goodness of fit was assessed with the maximum likelihood chi-squared statistic, the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMSR) (Hu & Bentler, 1999; Kline, 2015). A test for multicollinearity was conducted for the variables included in the multivariate analyses and results showed that the variance inflation factor did not exceed the 1.69 threshold, and the tolerance was above 0.59.
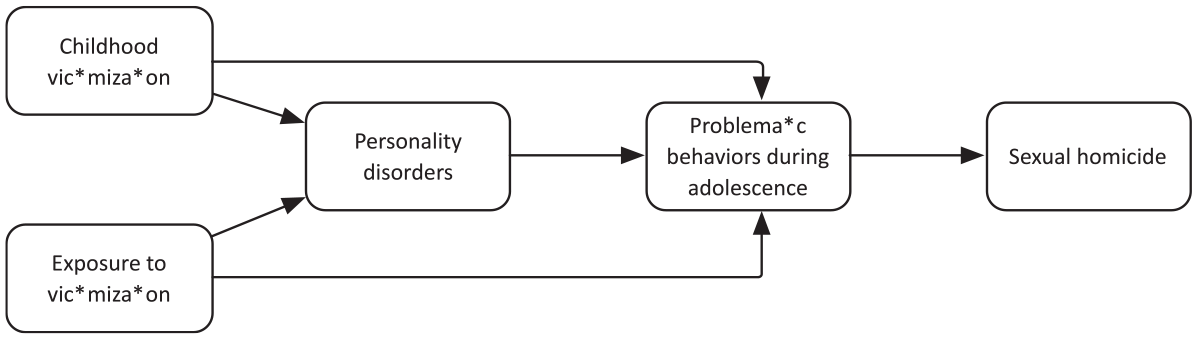
Proposed model.
Ethics
This study received ethical approval from the Research Ethics Board of the University of Montreal.
Results
Table 2 presents the results of the bivariate analyses. Results showed that individuals who have a diagnosis of antisocial, F(1,611) = 4.99, p = .026; borderline, F(1,611) = 18.10, p < .001; avoidant, F(1,611) = 9.28, p = .002; and dependent, F(1,611) = 9.14, p = .003, personality disorders were more likely to have experienced childhood victimization. Individuals who have had several internalized (Pearson’s r = 0.43, p < .001) and antisocial (Pearson’s r = 0.34, p < .001) behaviors during adolescence were more likely to have experienced childhood victimization. Those with a diagnosis of alcohol and/or drug use disorders, F(1,611) = 21.76, p < .001, as well as those involved in SH, F(1,611) = 9.52, p = .002, were more likely to have experienced childhood victimization. As to the exposure to violence, results showed that individuals who have a diagnosis of antisocial, F(1,611) = 12.06, p = .003; borderline, F(1,611) = 10.84, p = .001; and dependent, F(1,611) = 13.89, p < .001, personality disorders were more likely to have experienced exposure to victimization during childhood. Individuals who have had several internalized (Pearson’s r = 0.33, p < .001) and antisocial (Pearson’s r = 0.32, p < .001) behaviors during adolescence were more likely to have been exposed to victimization during childhood. Finally, individuals with a diagnosis of alcohol and/or drug use disorders, F(1,611) = 29.94, p < .001, as well as those involved in SH, F(1,611) = 15.04, p < .001, were more likely to have experienced exposure to victimization during childhood.
One-Way Analyses of Variance Comparing Means of Childhood Victimization and Exposure to Victimization During Childhood for Personality Disorders, Problematic Behaviors, and Crime Outcome Independent Variables (N = 613).
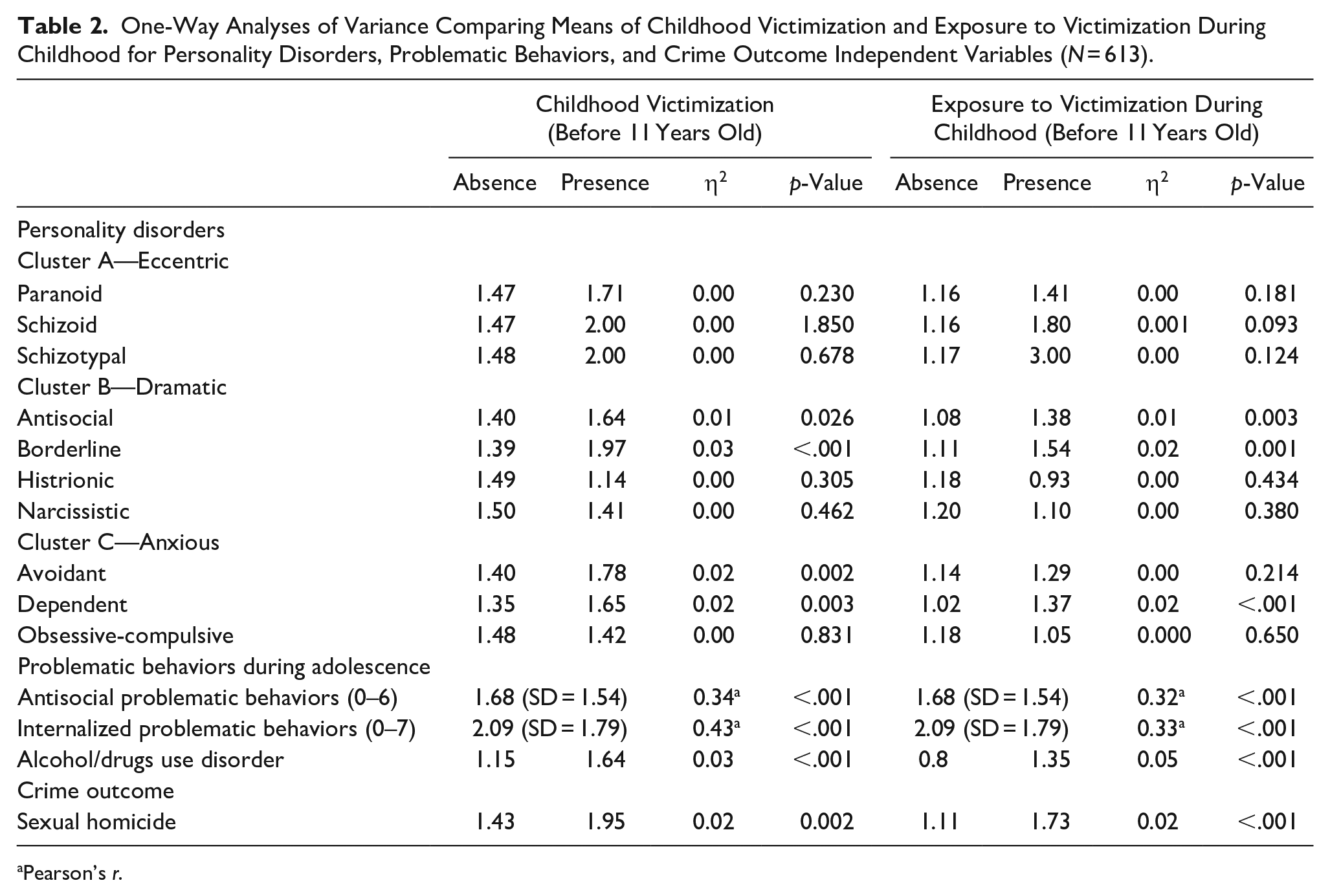
Pearson’s r.
Table 3 presents the results of the multiple linear regression analyses. In Model 1 related to childhood victimization, the combined explanatory power of explanatory variables explained half of the variance in childhood victimization as the regression coefficient R is .49, while the R2 is .24, and the adjusted R2 is .23. The multiple regression equation is significant at <.001 with an F-value of 23.87. The findings suggested that individuals who experienced childhood victimization were more likely to present borderline (β = .25, p = .042), avoidant (β = .24, p = .043), and dependent (β = .26, p = .005) personality disorders. They were also more likely to present antisocial (β = .15, p < .001) and internalized problematic behaviors (β = .21, p < .001) during adolescence. Finally, these individuals were more likely to commit a SH (β = .27, p = .006). In Model 2 related to exposure to victimization during childhood, the combined explanatory power of explanatory variables explained a bit less than half of the variance in exposure to victimization as the regression coefficient R was .45, while the R2 was .20, and the adjusted R2 was .19. The multiple regression equation was significant at <.001 with an F-value of 13.11. Individuals who were exposed to victimization during childhood were more likely to present antisocial (β = .26, p = .049) and dependent (β = .25, p < .001) personality disorders. They were also more likely to present antisocial (β = .13, p < .001), internalized problematic behaviors (β = .16, p < .001), and alcohol/drug disorders (β = .23, p = .023) during adolescence. Finally, these individuals were more likely to commit a SH (β = .58, p = .001).
Multiple Regression Models of Factors Associated With Childhood Victimization and Exposure to Victimization During Childhood (N = 613).
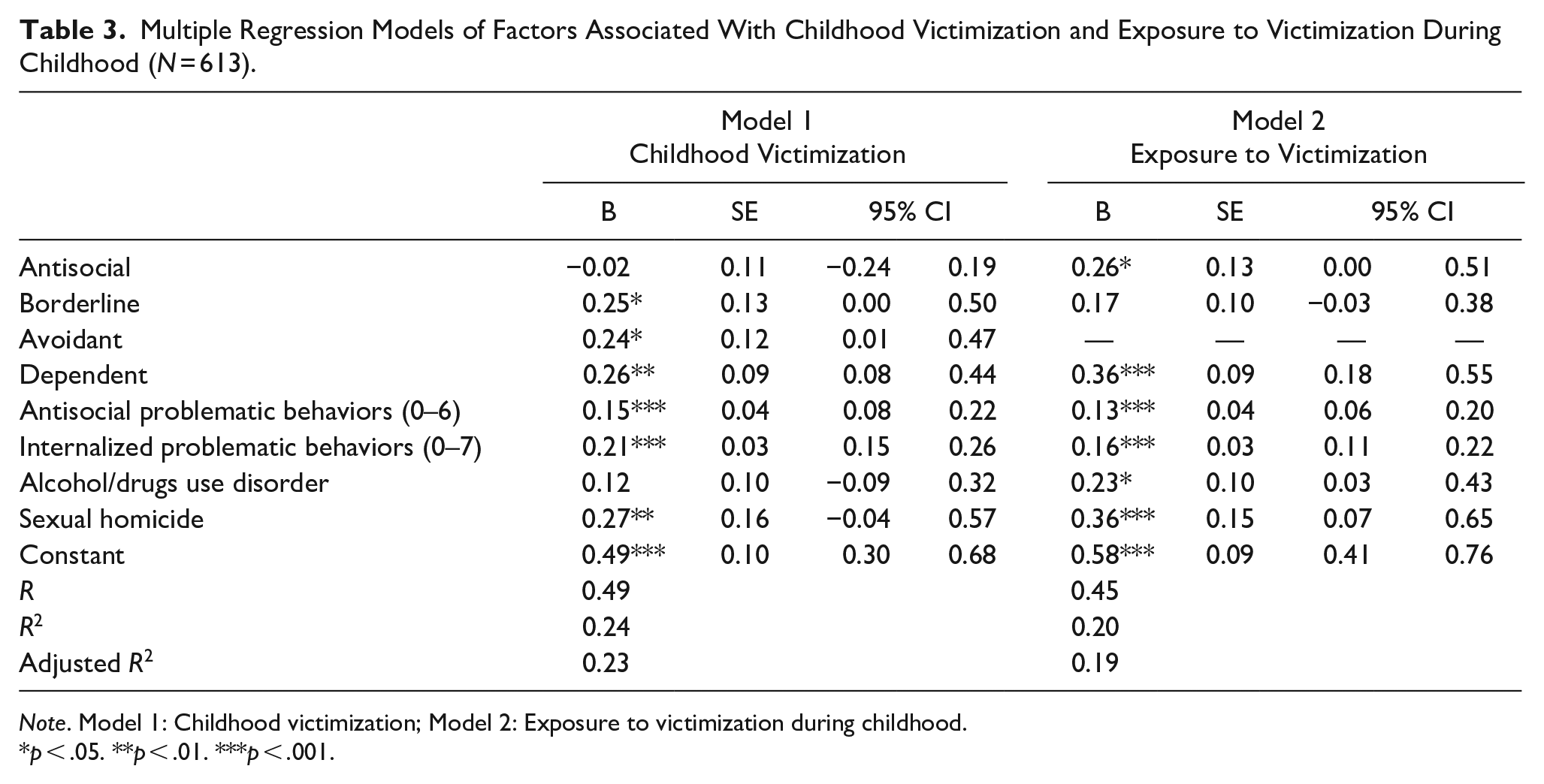
Note. Model 1: Childhood victimization; Model 2: Exposure to victimization during childhood.
p < .05. **p < .01. ***p < .001.
Table 4 and Figure 2 present findings of the path analysis. The goodness of fit statistics showed a satisfactory model with a χ2 (4) of 200.62 (p < .001), CFI of 0.93, RMSEA of 0.02, and SRMR of 0.07. The findings suggested a relationship between childhood victimization and borderline (β = .15, p = .006) as well as avoidant (β = .16, p = .003) personality disorders. As to the exposure to victimization, we observed a relationship with the diagnosis of dependent personality disorder (β = .12, p = .021). The presence of an antisocial disorder was significantly associated with the development of antisocial problematic behaviors (β = .35, p < .001) and the observation of alcohol/drugs use disorder during adolescence (β = .29, p < .001). The results suggested a significant relationship between the presence of a borderline disorder and the observation of antisocial (β = .20, p < .001) and internalized (β = .08, p = .031) problematic behaviors during adolescence. A relationship was also observed between the presence of an avoidant personality disorder and the observation of internalized problematic behaviors during adolescence (β = .17, p < .001). The path analysis suggested direct relationships between childhood victimization and the observation of antisocial (β = .20, p < .001) and internalized (β = .29, p = .031) problematic behaviors during adolescence. A similar association exists with exposure to victimization and the presence of both antisocial (β = .14, p = .003) and internalized (β = .13, p = .011) problematic behaviors during adolescence. Finally, we identified only one significant relationship between the observation of antisocial problematic behaviors during adolescence (β = .15, p < .001) and the commission of a SH.
Regression Weights of the Exploratory Path Analysis (N = 613).
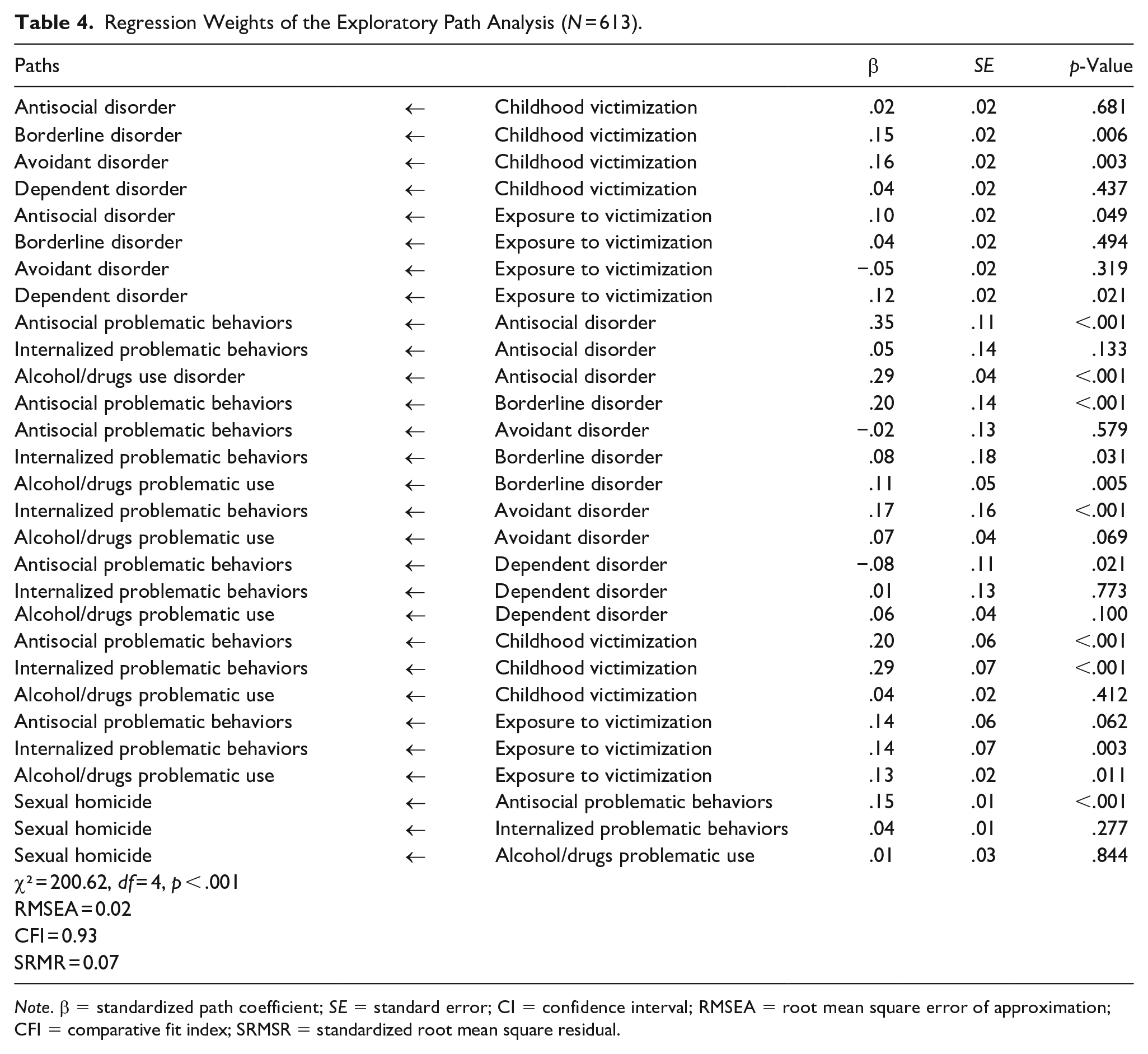
Note. β = standardized path coefficient; SE = standard error; CI = confidence interval; RMSEA = root mean square error of approximation; CFI = comparative fit index; SRMSR = standardized root mean square residual.
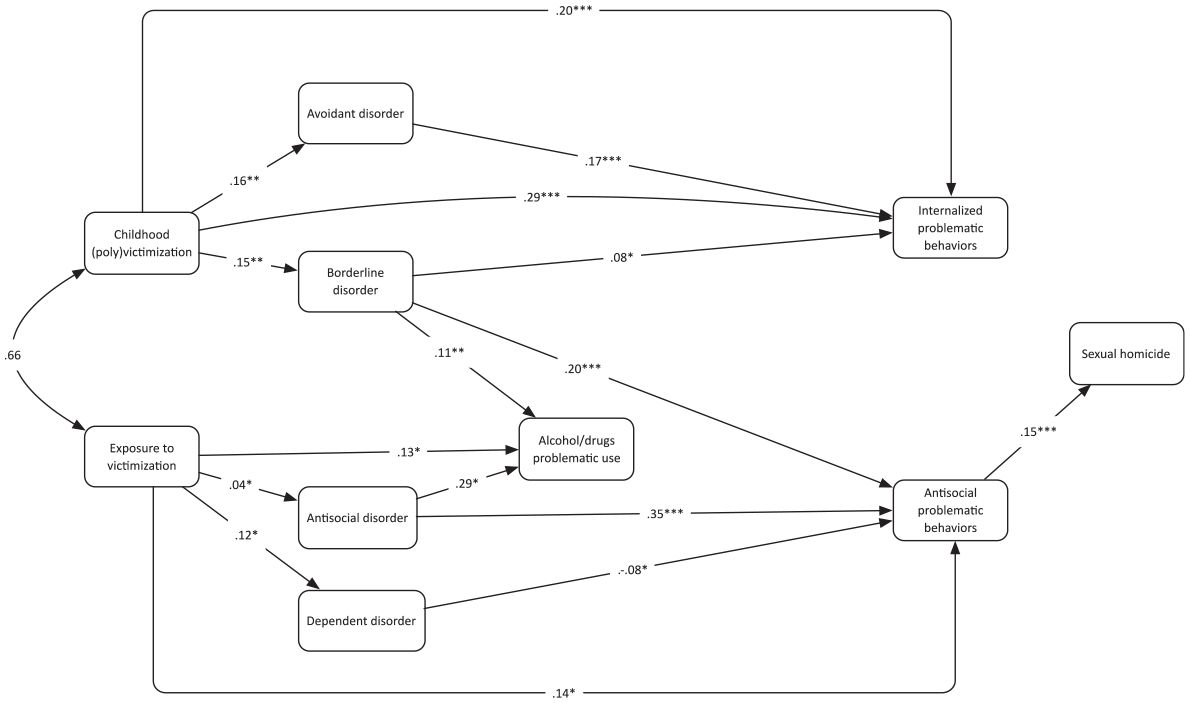
Exploratory path analysis (N = 613).
Discussion
Conceptual models of SH frequently invoke a social learning process whereby early life formative experiences play a major role in the development of personality pathology and diverse behavioral adaptations, some of which are extreme and culminate in crimes such as murder and rape. Unfortunately, prior studies have overlooked the commonalities in these perspectives (e.g., Burgess et al., 1986; Hickey, 1997; Purcell & Arrigo, 2006); the current study filled this void and several important themes emerged from the analyses.
First, although traumatic experiences and ACEs are almost universally seen as important risk factors for conduct problems and violence, their findings are highly variable as shown by our models that differentiate childhood victimization and exposure to victimization. Direct victimization or indirect victimization have different effects depending on the form of psychopathology in question, and its valence. Any adverse experience whether childhood victimization or exposure to victimization significantly impacts dependent personality, which makes sense given the sadness, withdrawal, and resignation associated with Cluster C personality disorders. Direct childhood victimization is significantly associated with avoidant personality disorder, which likely develop an enduring pattern of avoiding other people to mitigate the risk for abuse and borderline personality, which sets into motion an impulsive and unstable interpersonal style. Broader exposure to victimization is not associated with these two personality disorders. A diametric situation is seen for antisocial personality disorder where childhood victimization had null effects, but exposure to victimization had a significant positive effect. For highly externalizing, aggressive youth, being personally abused serves to inure them to violence and likely accelerate underlying anger and hostility that facilitates broadband involvement in offending. However, it is the ambient exposure to victimization, which implicates the settings in which they are reared that is predictive of this personality disorder adaptation. Collectively, these findings are consistent with other research that differentiated trauma events from reactions to the trauma events (DeLisi et al., 2021) to show the complexity of the relationship between ACEs and conduct problems.
Second, the exploratory path model made clear that childhood victimization and exposure to victimization foster an array of significant clinical and behavioral problems spanning personality disorders, which fundamentally impair adult functioning in family relationships, intimate relationships, and work responsibilities, problematic substance use, internalizing features, and externalizing features. These outcomes are common. Uncommon is any pathway to SH, an exceedingly rare event (Chan & Beauregard, 2016; Chan & Heide, 2009) even when considering the multitude of active offenders who have developmental histories that are conducive to lethal sexual violence. In our model, the only significant path toward SH was from antisocial problematic behaviors; thus it is very difficult to predict SH even among persons with numerous risk factors for it. Conceptual models for SH produce many false positives.
Third, we acknowledge that developmental sequela reflects greater nuance than our path model indicates and other important constructs are missing. For instance, an often-overlooked feature of ACEs is they are not unidirectional whereby youth are exclusively abused and neglected. In some cases, the specific behavioral features of the child elicit or evoke more hostile, abusive, and punitive responses from parents, teachers, and other peers. This concept is known as an evocative gene-environment correlation. In our clinical experiences, highly defiant and aggressive youth, who ultimately develop antisocial personality disorder and psychopathic features, are most likely to experience these reciprocal, multidirectional effects resulting from ACEs and other noxious environmental exposures. A missing variable that potentially puts this into context is homicidal ideation. Some SHOs experience homicidal ideation pervasively since early childhood (Meloy, 2000), and these acutely violent cognitions and the inappropriate behaviors that result from them (e.g., social isolation, animal cruelty, killing of animals, bullying of younger children, precocious sexual experimentation) likely increase parental abuse and neglect. Moreover, emerging research (e.g., Carbone et al., 2020; Heirigs, 2021) reveals that homicidal ideation is a potent risk factor for murder and other violent felonies and severe behavioral disorders, thus it could also be a key ingredient toward SH.
Fourth, keeping with multiplicity of conditions that arise from direct and indirect trauma exposure, so too is the psychological complexity of SHOs (Beauregard & DeLisi, 2021). Although it is intuitive to construe sexual murderers as simply psychopathic sexual sadists with antisocial personality disorder (and many are), the preponderance of them evinces multiple Cluster A, B, and C personality disorders that produce variegated associations with conduct problems. Some psychopathology facilitate internalizing features, some facilitate externalizing features, and some conditions facilitate both.
Diversity
This study examined the relationship between ACEs and the development of internal risk factors involved in SH. Diversity is specifically addressed in this research through two aspects. First, a plethora of research has been conducted on the relationship between ACEs and sexual offending during adulthood, but little research has examined SH, whose knowledge is based primarily on theoretical models. This study proposes a first empirical investigation of this issue. Second, it contributes to the generalizability of knowledge relating to the links between ACEs, internal risk factors, and the commission of violent sexual assaults. Most of the studies analyzing the relationship between ACEs and personality disorders have been realized with data from the United States and the use of Canadian data on this topic increases the external validity of existing results.
Conclusion
The prediction of a rare event such as SH is a challenging task. In fact, the current knowledge does not allow us to make these predictions without the risk of many false positives. However, the body of research on SH and the lethal outcome in sexual victimization all seems to agree with the fact that individuals who are at risk of committing serious sexual crimes have seen the sequela leading to this extreme form of violence beginning in childhood. Although such idea has been at the core of the various theoretical model of SH, only a few studies attempted to test this. The current study goes further by examining the complex sequela that may lead to SH, while taking into account the personality component. The findings suggest that the impact of ACEs will differ, depending on whether the child has been victim of violence or if he/she has witnessed it.
The results of this study allow for discussion of both theoretical and practical implications. Theories that suggested the presence of a developmental component in the explanation of SH were mainly based on clinical observations and lacked empirical validation. Our results contributed to validating the relevance of these models. Furthermore, this study not only establishes a link between traumatic childhood experiences and involvement in SH, but also allows to understand their impact on the development of subsequent internal risk factors. The proposed model allows to identify the causal complexity of the internal risk factor pathways involved in the commission of SHs. Beyond the empirical validation, this study proposes a new conceptual framework of internal risk factors following a developmental perspective that should be confronted with external risk factors.
As to the practical implications, these results suggest that early intervention—and prevention—should be a priority. The relationship between childhood victimization and the development of risk factors is probabilistic (Cicchetti & Banny, 2014) and it is important to increase the identification of children who have sustained different types of traumas in order to offer them appropriate psychological assistance. The objective is to reframe their affective and cognitive processing that may have been adversely affected by physical and psychological negative experiences. A special focus should be made on the relation to violence and sexuality as well as in the early diagnosis of personality disorders that will allow for appropriate management. Such an approach could allow for better monitoring of the multiplication of risk factors over time and thus contribute to reducing the likelihood of committing a crime. Finally, for individuals who have already committed a crime, the consideration of childhood trauma in the treatment process is fundamental. Known as trauma-informed care (Levenson et al., 2014), this practice allows for the integration of ACEs into more general cognitive behavioral therapy programs to increase the likelihood of reducing recidivism.
It is important to examine how these ACEs affect the development of personality as this may inform clinicians on how this is likely to impact these individuals in the future.
Although interesting and informative, this study is not without limitations. Despite the use of various precautions (e.g., triangulation of information), a lot of the information used in the current study is self-reported. Thus, we cannot exclude the possibility that some participants have exaggerated their childhood experiences to justify their offense. Moreover, given that personality disorders were assessed by different psychologists in correctional settings, it is not impossible that these diagnoses may have varied. Although this is unlikely considering the use of the DSM criteria, it is not possible to exclude it. Related to personality disorders, another limitation of the current study is the absence of a measure of psychopathy for this particular sample. Psychopathy has often been associated to SH and it was not possible to test this association here. Additionally, we did not have the opportunity to use a control group including individuals who have not committed sexual offences. Despite previous studies comparing the general population and incarcerated individuals have shown that a significant proportion of sexual offenders experienced victimization during childhood (Levenson & Socia, 2016), we acknowledge that our approach is based on probabilistic patterns and that not all individuals following this pattern will engage in sexual offending (Cicchetti & Banny, 2014). Finally, the number of SH cases included in this sample was limited, which may have prevented to reach the level of significance for some of the relationships explored.
Future studies should continue to examine the complex relationships between childhood victimization and its impact on the likelihood of committing acts of sexual violence later in life—particularly the most extreme one. One area that would require additional research is related to the specific relationship between childhood victimization and the development of deviant sexual interests. Combined with measures of psychopathy and sexual sadism, this information would represent a much-needed complement to this complex sequela leading to SH.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605221127199 – Supplemental material for Developmental Sequela for Sexual Homicide: Testing an Integrated Multi-Theoretical Model
Supplemental material, sj-docx-1-jiv-10.1177_08862605221127199 for Developmental Sequela for Sexual Homicide: Testing an Integrated Multi-Theoretical Model by Julien Chopin, Matt DeLisi and Eric Beauregard in Journal of Interpersonal Violence
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.