
Abstract
Prisons are saturated with trauma survivors; yet trauma has not been the focal point of corrections-based treatment. This is the first randomized controlled trial assessing the effectiveness of a Peer-facilitated trauma-specific intervention among men incarcerated for violent offenses (Exploring Trauma: A 6-Session Brief Intervention for Men). The sample consisted of 221 participants (131 treatment / 90 waitlisted control group). Independent t tests determined change over 6-8 weeks on anxiety, depression, mental health, current traumatic distress, and anger. Hypotheses were predominantly supported. Significant improvement was found for the intervention group compared with the waitlisted control group on 11 of the 13 trauma-related outcomes. The greatest effect sizes ranged from .46 for mental health functioning, .42 for trait anger composite, and .40 for anxiety. Support for the effectiveness of this brief intervention and capability of a Peer-facilitated model of delivery was demonstrated. Future research should replicate the methodology and incorporate records data and post-release outcomes.
Introduction
A growing body of research has linked histories of adverse childhood experiences (ACEs), substance use/dependence, and antisocial personality traits as precursors to violent and aggressive behavior by men, and as primary treatment needs to address to end the cycle of trauma and violence (Bonta et al., 2000; Burdon et al., 2004; Horwitz et al., 2001; Messina & Burdon, 2021; Messina & Schepps, 2021; Springer et al., 2007). Although, histories of trauma and abuse among justice-involved men may have previously been under-reported, more recent literature has revealed greater willingness to self-report ACEs (prior to age 18). Messina and Schepps (2021) found that among 624 incarcerated men, 67% revealed they had experienced verbal abuse prior to the age of 18; 64% revealed physical abuse; 50% emotional neglect; 33% physical neglect; and 29% sexual abuse. They also reported high rates of household dysfunction under the age of 18 including parental separation/divorce (71%); domestic violence (38%); substance use (64%); mental illness (32%); and 44% reported incarceration of a household member.
Childhood victimization is also reported to be correlated with adult violence and aggression. Further analysis from the sample revealed that the histories of victimization were significantly associated with adult perpetration of abuse. If the respondent suffered abuse as a child, he was three times more likely to perpetrate minor abuse (e.g., restraining, punching, kicking), severe abuse (e.g., choking, burning, stabbing), and intimidation (e.g., threatening harm or death) on others as an adult. If the respondent suffered sexual abuse as a child, he was 8 times more likely to perpetrate a sex crime as an adult (Messina & Schepps, 2021). People can be further negatively impacted by their own use of violence, referred to as perpetrator-induced trauma (MacNair, 2015). They can feel great shame and guilt over their own offending behavior, preventing motivation to access support. Although some studies have explored childhood adversity as a mediator of violence and aggression, additional research on treatment outcomes for trauma survivors is vital to determine if those with the most complex histories of trauma can be responsive to trauma-focused treatment.
The cumulative negative effects of ACEs include the increased likelihood of post-traumatic stress disorder (PTSD), depression, anxiety, substance use/dependence, criminal behavior, chronic health disorders, earlier death, and suicide ideation (Felitti et al., 1998; Greenfield & Marks, 2010; Holmes & Slap, 1998; Horwitz et al., 2001; Kubiak & Rose, 2007; Messina et al., 2007; Wolff & Shi, 2012). However, there is great hesitancy to open the proverbial “can of worms” and openly discuss trauma within the corrections-based programs (Messina & Schepps, 2021). Concerns about addressing histories of trauma include lack of custody staff to address the presumed disruptive behavior of participants with high levels of trauma and the high cost of mental health staff needed due to the potential re-traumatization or decompensation (Miller & Najavits, 2012; Najavits & Hien, 2013). Thus, histories of trauma and current traumatic distress are often unaddressed and corrections-based treatment focuses instead on treating substance use and reducing recidivism to increase public safety. Failing to appropriately address trauma is also failure to focus on the underlying needs of participants to reduce recidivism and increase their well-being.
Additionally, many debilitating predictive factors, such as the impact of lifelong trauma, are missing from the analytical models of treatment outcome studies, further impeding the availability of specialized treatment programs designed to address such factors (Baglivio et al., 2014; Meade & Steiner, 2013; Messina, 2022). Thus, it is difficult to rely on conclusions about the effectiveness of corrections-based treatment if the programs are not attending to the complex needs of those under their care. What has become clear from the literature is that traumatic experiences are highly prevalent, with victimization and perpetration overlapping and ongoing among incarcerated populations, with or without, substance use disorders (Henry, 2020a; Kubiak et al., 2017; Messina & Schepps, 2021; Wolff & Shi, 2012).
Pilot Studies on Trauma-Specific Treatment Outcomes 1
Recent pilot studies have begun to show the positive impact of a trauma-specific psychoeducational program implemented within the California Department of Corrections and Rehabilitation (CDCR) (Messina, 2022; Messina & Burdon, 2021). Exploring Trauma (ET): A Brief Intervention for Men (Covington & Rodriguez, 2016) was introduced to CDCR with the goal of reducing trauma-related mental health issues and the reoccurrence of violence in prison. The 6-session ET intervention is grounded in trauma theory, which posits that early trauma influences both perceptions of and reactions to life events (Herman, 1992; 1997; Kendall-Tackett, 2000). Trauma exposure, particularly early and ongoing, may result in repressed anger (Newman & Peterson, 1996; Springer et al., 2007). Anger from trauma is theorized to be confounded with emotional pain and often lacks healthy expression, leading to the continual repression of anger and pain, which may result in assaultive and violent behavior (Kubiak et al., 2017; Thomas, 2005).
The initial pilot studies implemented a trained Peer-facilitated model of program delivery assessing the program impact among 624 participants from two men’s prisons and varying levels of security risk classification, that is, medium to maximum security (Messina, 2022). Results from the pre- and post-intervention surveys demonstrated statistically significant improvement over 6–8 weeks among participants on 100% of the 19 mental health and anger outcomes measured. Effect sizes for psychological measures were small to moderate in size, with the largest impact on current traumatic distress, depression, and anxiety (Cohen’s d .54, .48, .46, respectively). The largest impact for anger and aggression included trait anger, that is, angry feelings/emotions, (Cohen’s d = .35); instrumental anger, that is, the outward expression of anger and control (Cohen’s d = .35); and physical aggression (Cohen’s d = .32). Quantitative analyses from programs at both women’s and men’s prisons demonstrated feasibility of the Peer-facilitated model of program delivery (Gajewski & Messina, 2021). Post-program feedback surveys from 1800 participants and focus group summaries from 44 participants and facilitators were compiled and analyzed using deductive thematic analysis. Participants’ feedback was overwhelmingly positive. They commented on their appreciation for the facilitators, the safety of small groups, the ability to discuss trauma without judgment, learning skills to address and control anger, gaining self-respect and empathy, and healing relationships and childhood wounds.
The second series of pilot studies assessed a trained Program Staff-facilitated model of the ET brief intervention for 186 participants residing in two maximum security housing units (SHUs), the highest security risk classification other than condemned housing. Results were consistent with the Peer-facilitated model of program delivery, as significant improvement was found for 100% of the 17 outcomes for the men housed in the SHU (Messina & Burdon, 2021).
The greatest impact was for psychological dysfunction, depression, current traumatic distress, and anxiety (Cohen’s d ranged from .54, .43, .41 respectively). The greatest impact for anger and aggression included physical aggression (Cohen’s d = .40); indirect aggression (Cohen’s d = .36); hostility (Cohen’s d = .38); and trait anger (Cohen’s d = .30). The consistent findings of the pilot research have demonstrated positive support for the feasibility and value of the ET intervention for those at all levels of risk classification, with trained Program Staff- or Peer-facilitated models of program delivery.
However, the pilot studies were limited in that they used a single group pretest–posttest design and did not include a comparison group of men who did not participate in ET. Although the sample sizes provided enough power to detect significant between subject change, and findings were consistent across prisons and samples, it is difficult to judge whether improvements were solely a product of participation in the ET program.
The goal of the current study is to create a more rigorous examination of the program by conducting an experimental study to further explore the effectiveness of the Peer-facilitated delivery of the ET brief intervention to reduce trauma-related mental health difficulties, anger, and violence among incarcerated populations. Given the emerging research reporting the results of incarcerated men’s willingness to discuss histories of abuse and to volunteer for the trauma-specific treatment, it is vital for corrections officials be informed about evidence-based treatment models and feasible models of treatment delivery. Based on the results of the pilot studies, it was hypothesized that 1) Participants in the ET intervention group would exhibit significant improvement on current psychological dysfunction and current traumatic distress compared with the waitlisted control group; and 2) Participants in the ET intervention group would exhibit significant improvement on the anger/aggression outcome measures compared with the waitlisted control group.
Methods
Procedures
This study employed a randomized controlled trial of a psychoeducational brief trauma intervention using a waitlisted control group design among incarcerated participants in a California medium security male prison. Procedures were reviewed and approved by the University of California, Los Angeles, Institutional Review Board, the DHHS Office for Human Research Protections, and the CDCR Research Advisory Committee. Enrollment for this study took place from July of 2017 and data collection ended in June 2019. A Federal Certificate of Confidentiality was also obtained, and all volunteers were given a unique study identification used by the research staff to link the pre- and post-surveys.
Sample Selection and Recruitment
The sample was selected from those incarcerated in a California prison housed on a security classification risk Level III yard. 2 All residents housed on this yard were eligible to volunteer for the program and research. A flyer with the name of the program, a description of the program length and content, the affiliated research plan, and the planned Peer-facilitation was posted in the housing units by the Program Coordinator. Any man could sign up to participate in the program if he did not have a schedule conflict (e.g., work); however, the program was offered for a morning group or an evening group to increase availability. The CDCR agreed that there would be no other eligibility criteria. There was no other formal recruitment and the opportunity quickly spread by “word of mouth” from participants.
Program disruption, breach of the rules of confidentiality, or missing two sessions were reason for being dropped from the program and was monitored throughout the study by the Program Coordinator. Decisions regarding dropping a participant were made by the Program Coordinator from reports from the Peer Facilitators, as Program Coordinators sat outside the door during program hours. No violations were reported.
Informed Consent
Research staff created a schedule (based on the sign-up sheets) to meet with 10–15 volunteers at a time to explain the purpose of the study, answer questions, and have those agreeing to participate sign the informed consent form. The research staff member read the IRB- approved consent form to the volunteers describing the randomization, the study goals, the measures used to protect the confidentiality of the participants’ data, and the voluntary nature of the study. Although there were no specific eligibility criteria, participants were required by the facility to complete five of the six sessions to attend graduation and receive a certificate of completion. They could participate in the program and decline to participate in the research with no penalty. The residents were informed that participation would not impact their recommendations for parole, parole status, or re-sentencing in any way. Participants were not compensated.
Randomization
In order to avoid adding to the workload of the facility assignment Lieutenant (the person in charge of program assignment and participant monitoring), the research director placed eligible volunteers with an even CDCR identification number into the treatment intervention group, and volunteers with an odd CDCR number onto the waitlisted control group (based on the result of a coin toss). Residents were not assigned CDCR numbers with any specificity. This was the simplest way to randomize participants fairly within the institution, and to monitor any randomization violations. This also allowed participation in the brief intervention for everyone who volunteered. Those from the waitlisted control group were offered the program after they completed their final survey, approximately 4-weeks after the intervention group 6-session rotation.
Peer Facilitators and the Program Coordinator
The ET program authors (Covington & Rodriguez, 2016) trained approximately 20 peers and the Program Coordinator to facilitate the intervention using the ET Facilitator’s Guide. The Program Coordinator was hired by the grantee 3 and was a retired CDCR Deputy Warden with a strong belief in program services and over 30 years of corrections experience. The Program Coordinator’s primary duties were to provide oversight of the facilitators and coordinate all aspects of program sign up, documentation of attendance, program schedules, program space, graduations, and organize time and space for research staff for data collection. The Program Coordinator was also available to peers and participants who needed any additional support.
Peer facilitators were interviewed at length by the institution, chosen, and later paired by the ET Program Coordinator. Criteria for the ET peer facilitator position included having social influence, having the ability to connect with other residents, previously holding positions as mentors, and being available during programming hours. All peer facilitators were required to graduate from ET as participants, led by the Program Coordinator, prior to facilitation. Groups were co-facilitated by the same team of peers twice a week during the 3-week cycle and multiple simultaneous groups were run on the facility yard. The Program Coordinator, custody officers, and other prison staff did not interrupt the groups or enter the group space except in case of an emergency. Privacy and confidentiality of the groups were fully supported by the institution; thus, 6 to 10 participants and two Peer-facilitators were occupying the program space alone during the two- hour group time with the Program Coordinator waiting outside.
The Peer-facilitators were residents serving life without parole or serving more than 10 years at the prison. They had previously graduated from the program. Thirty-one percent were serving sentences for homicide and 69% had served time in the SHUs. On average, the Peer-facilitators were 45.9 (sd = 7.83) and had been incarcerated an average of 20.9 years (sd= 10.28). Thirty-one percent of facilitators were White, 23% were Black, and 23% were Hispanic, 7% were multiracial, and 15% listed as “other.” Fifty-four percent had never been married.
Although none of the facilitators had graduated high school prior to incarceration, 38% had obtained a GED while in prison.
Participation and Follow up Rate
A total of 249 residents volunteered for the program and the research project. Of those, 221 completed both the pre- and post-survey (131 randomized to the ET intervention and 90 randomized to the waitlist control group), resulting in an 89% follow up rate. Research staff were not able to schedule six of the waitlisted control group members and 22 ET participants for the post-survey. Specific reasons for non-completion of the post-survey varied from institutional housing movement, prison lock down, refusal to participate or conflict with work hours. No demographic differences were found between those who remained in the analyses compared with those lost at follow up.
Program Description: Exploring Trauma
Exploring Trauma (ET) is a 6-session trauma-specific program designed for those who have experienced trauma associated with ACEs and adult victimization (Covington & Rodriguez, 2016). The ET brief intervention is a psychoeducational group program and emphasizes skill-building and grounding techniques. The curriculum specifically addresses trauma which occurred as a result of experiencing toxic stress, abuse, violence, and other adverse experiences. The session topics include: The Subject of Trauma; Exploring Trauma; Thinking, Feeling, and Acting; Beyond Guilt, Shame, and Anger; Healthy Relationships; Love and Endings. The program materials consist of a Facilitator’s Guide, a Participant’s Workbook for group-work, journaling, and homework. The Peer-facilitated program model that was delivered was comprised of six, two- hour group sessions delivered twice weekly (with some interruptions due to prison lock downs or other institutional restrictions). Based on the content focus on trauma and violence, the program was restricted to small, closed groups of 6–10 participants (i.e., no new participants entered during the 3-week cycle).
Measures
Self-report and attendance records data were collected for the study participants. Research staff provided the initial surveys at the facility prior to the ET program entry for the intervention group and at the time of consent for the control group. On average, the pre-survey was completed within 45 minutes. The post-survey took place after 4-weeks after completion of the 6-sessions of ET (approximately 3 weeks for the control group to begin their rotation into the program) and took approximately 45 minutes to complete. The research staff collected the surveys upon completion and left the facility with the surveys in a sealed envelope to ensure confidentiality of survey responses. After data entry, paper copies were kept in locked file cabinets at the research offices.
Self-Administered Surveys
Participants were given the surveys in small groups of 10–12 while proctored by a research staff member in a private room without custody staff present. The surveys and instructions were prepared at a sixth grade reading level and research staff answered any questions that arose. Standardized instruments included detailed questions about demographics, childhood and adult victimization and perpetration, mental health, substance use, and criminal justice involvement. The feasibility of these measures and procedures were previously found to be effective and valid among incarcerated populations (Kubiak et al., 2014; Messina, 2022; Messina et al., 2020; Messina & Burdon, 2021; Messina & Zwart, 2021)
Conflict Tactics Scales and the Abuse Behavior Inventory
To ascertain the level of victimization and perpetration of violence within the sample, a modified index of perpetration and victimization history was developed based on several of the items from the Conflict Tactics Scales (Straus, 1979; Straus et al., 1996) and the Abuse Behavior Inventory (Shepard & Campbell, 1992). Participants were asked to indicate whether they had ever been the victim or perpetrator of 15 different behaviors which were coded into four major categories: (1) minor physical abuse (three behaviors; pushed, hit, restrained), (2) severe physical abuse (four behaviors; choked, burned, beaten, shot/stabbed), (3) threats and intimidation (seven behaviors; threats of physical harm or death to self, children, family members, or friends), and (4) sexual abuse/assault (forced into an unwanted sex act).
For each behavior, participants were asked to indicate whether it had ever happened to them in their lives, or if they had ever engaged in the behavior. If the answer to either was yes, they were then asked to indicate whether: (1) It happened to them as a child before the age of 18; (2) It happened to them as an adult by a romantic partner; (3) It happened to them as an adult by someone other than a romantic partner; (4) They did it as an adult to a romantic partner; or (5) They did it as an adult to someone other than a romantic partner. Data were collapsed into frequencies relating to whether respondents were (1) victims as children, (2) victims as adults, or (3) perpetrators as adults of each major category of behavior. Cronbach’s alpha for the current sample resulted in .85 for minor abuse, .72 for severe abuse, and .83 for intimidation.
Patient health questionnaire – depression and anxiety subscales
The Patient Health Questionnaire (PHQ) Depression Subscale is a 9-item subscale that measures current (past 2 weeks) depressive symptomology (Kroenke & Spitzer, 2002; Spitzer et al., 1999). Participants report on the symptoms they have experienced in the preceding 2-week period. Responses are based on a 4-point Likert-type scale ranging from 0 (Not at all) to 3 (Nearly every day) and are summed into an overall symptom severity scale score that falls between 0 and 27. In a validation study of over 3000 participants (with a cut off score of 10 or greater), the sensitivity for major depression was 88%, with a specificity of 88%, and a positive likelihood ratio of 7:1 (Kroenke & Spitzer, 2002). The 7.1 ratio indicated patients with major depression were seven times more likely to have a PHQ depression score of 10 or greater than patients without major depression.
The PHQ Anxiety Subscale is a 6-item subscale that measures anxiety symptoms felt over the past 4 weeks (Spitzer et al., 1999). Responses are based on a 4-point Likert-type scale ranging from 0 (Not at all) to 3 (Nearly every day) and are summed into an overall symptom severity scale score that falls between 0 and 18. In a validation study of over 3000 participants the PHQ anxiety subscale had an overall accuracy of .91 (specificity .97, sensitivity .63) in detecting any anxiety disorder when compared with mental health professionals using the Primary Care Evaluation of Mental Disorders (Prime-MD) (Spitzer et al., 1999).
Trauma symptom checklist – 40
The Trauma Symptom Checklist – 40 (TSC-40) is a 40- item self-report measure of symptomatic distress in adults arising from childhood or adult traumatic experiences (Elliot & Briere, 1992). It measures aspects of PTSD as well as other symptoms found in some traumatized individuals. Respondents are asked to rate how often they have experienced each symptom in the last 2 months using a 4-point frequency rating scale ranging from 0 (Never) to 3 (Often). In addition to yielding a total score (ranging from 0 to 120), the TSC-40 has six subscales: Anxiety, Depression, Dissociation, Sexual Abuse Trauma Index, Sexual Problems, and Sleep Disturbances. Using data collected from a large sample (N = 2963) of professional women, Elliott and Briere (1992) determined that the TSC-40 has high internal consistency (alpha =.90). Elliott and Briere also showed that the scale discriminates between those who have and have not been abused as children. This difference held strongly for all subscales, as well as for the total scale.
Kessler psychological distress scale (K6)
The K6 is a six-item brief mental health scale validated nationally and internationally (Kessler et al., 2002, 2003). The K6 was used to screen for current (previous 4 weeks) symptoms indicative of serious mental illness. The K6 is designed to detect any past-year diagnosis of an Axis I disorder and a Global Assessment of Functioning score (GAF) of 60 or below. It has been found to have relatively high stability over time (e.g., r _ .52 across 12 years; Drapeau et al., 2010). Responses, based on a Likert-type scale, ranging from 0 (None of the time) to 4 (All of the time), were summed into an overall scale with scores ranging from 0 to 24 (higher scores indicating a poor state of mental health). Kessler et al., 2003 used a sample of 1000 respondents to assess scale validity. Cronbach’s alpha for the scale was 0.89. The K6 scale had good discrimination, with an AUC of 0.86. An overall cut score of 13 was used to distinguish those with serious mental illness, at this cut-off score, the sensitivity was 0.36, specificity was 0.96, and total classification accuracy was 0.92.
State-trait anger expression Inventory—2 (STAXI-2)
The STAXI-2 is a 57-item instrument used to measure the experience and intensity of anger as an emotional state (State Anger) and as an emotional trait (Trait Anger). The State Anger Composite Scale assesses the intensity of angry feelings as a temporary emotional state and the Trait Anger Composite Scale measures the intensity of anger as a constant component of personality (Spielberger, 1999). For the 15 State Anger items, participants rate the intensity of their emotions “right now” on a four point Likert scale ranging from 1 (Not at all) to 4 (Very much so). For the 10 Trait Anger items, participants rate how they “generally” feel on a four point Likert scale ranging from 1 (Almost never) to 4 (Almost always). For the 32 Anger Expression and Anger Control items, participants rated how they generally react in certain situations also on a four point Likert scale ranging from 1 (Almost never) to 4 (Almost always). In the American sample of 1900 subjects, the subscales showed decent internal consistency, varying from .82 to .75 (Spielberger, 1999). The test–retest reliability of this instrument has shown to be stable over time (Bishop & Quah, 1998; Jacobs et al., 1988).
Revised instrumental and expressive anger representation scales)
The Revised Instrumental and Expressive Representation Scales have 16 items with two sub-scales (instrumental and expressive) assessing anger expression (Campbell et al., 1999). Instrumental anger is a more outward expression of anger that is often used to control others. In contrast, expressive anger is characterized by holding in or suppressing anger until there is an ‘‘explosion’’ of emotion. In the first subscales, respondents answered the degree of agreement about eight items measuring instrumental anger, including “I believe that physical force is needed to get through to some people” and “If I hit someone and hurt them, they were asking for it.” The second subscales assessed expressive anger using eight items such as “During a physical fight I feel out of control” and “After a physical fight I feel drained and guilty.” Participants responded on a scale from 1 (Strongly Disagree) to 5 (Strongly Agree). Some items were reverse scored so that higher scores indicate stronger anger expression. The eight items from each subscale are summed with a range of 8–40 for each sub-scale. The validation study with over 405 men and women on the eight instrumental and eight expressive items (with a range of 8–40 for each sub-scale) revealed a Cronbach’s alpha for the revised eight item instrumental item scale was 0.80 and the revised eight item expressive scale was 0.62. The correlation between the revised instrument and expressive scale was −0.02, indicating near perfect independence.
Statistical Analyses
Initial analysis comparing the two groups at baseline included descriptive and inferential statistics based on the reported background characteristics of participants. Descriptive statistics included percentages, means, and measures of variance. Frequency tables were used to examine cell sizes for categorical variables and non-normality for continuous variables. The second stage of data analyses were designed to quantify the effectiveness of the ET brief intervention.
Independent-sample t-tests were conducted to assess changes in the main outcomes across time, allowing for the examination of mean change over time comparing the intervention group to the waitlisted control group. Cohen’s d was computed to determine the effect size of significant treatment effects (Sullivan, 2012). Paired-sample t tests were also conducted to assess changes in the outcomes across time for the treatment group (post-test scores minus pre-test scores), allowing for the examination of mean change over time per individual who participated in ET.
Results
Sample Descriptives
Demographics and History by Group.
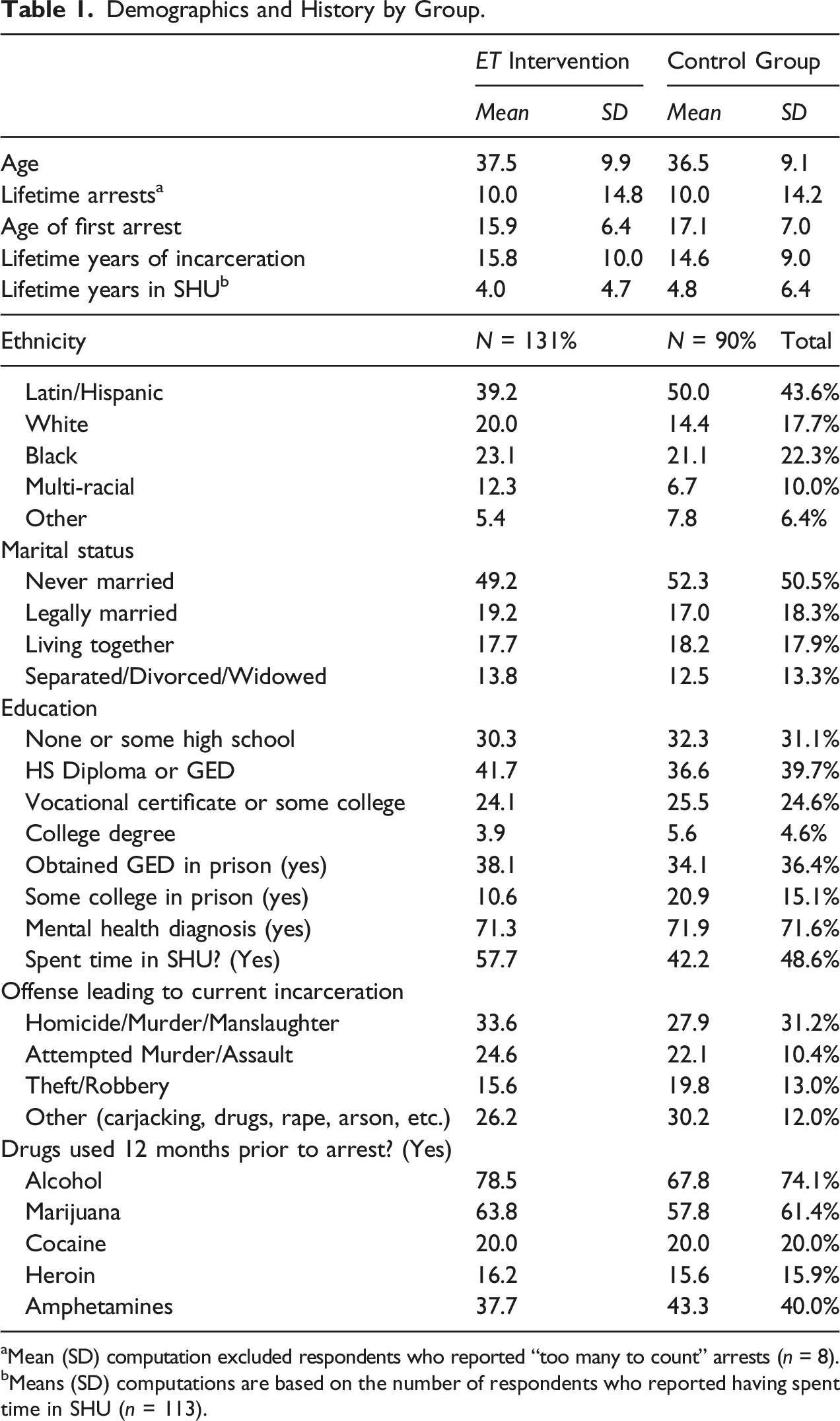
aMean (SD) computation excluded respondents who reported “too many to count” arrests (n = 8).
bMeans (SD) computations are based on the number of respondents who reported having spent time in SHU (n = 113).
On average, participants were 37.1 years old at the time of the baseline survey, were approximately 16.4 years old at time of first arrest, had been arrested approximately 10 times, and spent 15.3 years incarcerated. Respondents are predominantly Latino/Hispanic (44%) or Black (22%), and 10% listed the multi-racial category. Thus, of the 221 respondents who participated in the in the study, nearly 100% are people of color, exposing the disproportionate number of minorities incarcerated in the United States. Fifty-one percent have never been married. Thirty-one percent reported having no high school or some high school prior to incarceration and 40% reported having a high school diploma or GED prior to incarceration. Seventy-two percent reported being previously diagnosed with a mental health disorder. Participants were incarcerated for a variety of offenses with homicide, murder, manslaughter, attempted murder, and serious assault being the most common (55%), with 49% previously serving time in the SHU. A majority of respondents reported substantial substance use within the 12 months prior to incarceration, most frequently reporting alcohol (74%), marijuana (61%), and amphetamines (40%).
Prior to the age of 18, approximately 81% of the study participants reported that they had been victims of minor physical abuse, 79% reported being victims of severe physical abuse, 26% reported being victims of sexual abuse/assault, and 62% reported being victims of threats and intimidation. Regarding being the perpetrators of these behaviors as adults, 57% reported perpetrating minor physical abuse as an adult, 58% reported perpetrating severe physical abuse as an adult, 54% reported being the perpetrator of threats or intimidation as an adult, and 6% reported forcing sex on another.
Exploring Trauma Treatment Outcomes
Mean Change by Group.
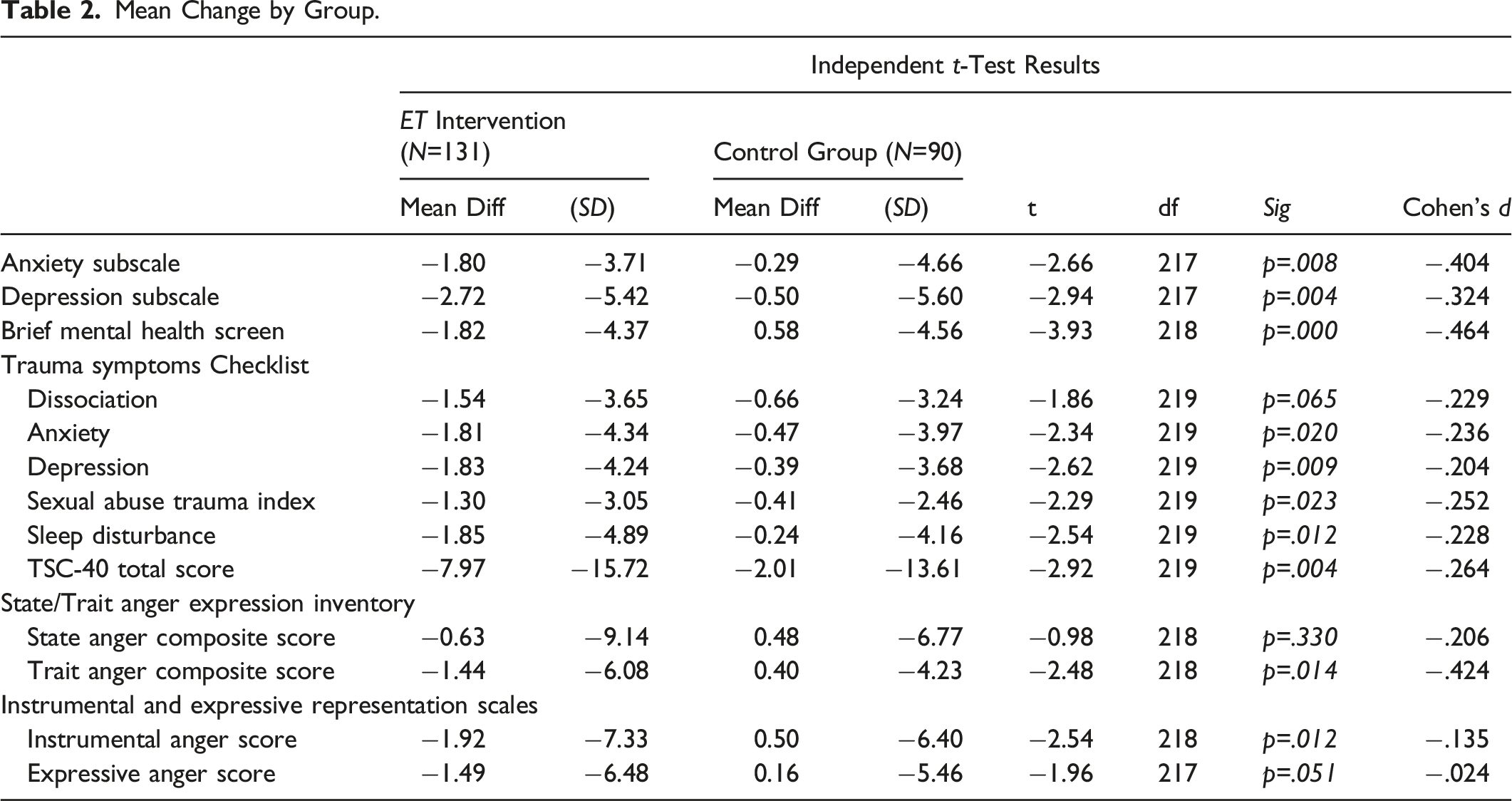
Hypothesis 2 regarding anger and aggression was predominantly supported, as findings showed that the ET participants had significantly lower mean scores than the control group on the trait anger composite score (i.e., angry emotions over time; t = 2.48; p =.014), the instrumental anger score (i.e., anger that erupts from repressed feelings; t = 2.53; p =.012), and the expressive anger score (i.e., anger used to manipulate or threaten; t = 1.96; p =.051). There were no significant differences between the two groups on the state anger composite score (i.e., angry feelings at a particular time).
When comparing the pre- and post-test mean change over time among the 131 ET participants, significant lower mean scores were found for anxiety (t = 3.50; p <.001), depression (t = 4.14; p <.001), psychological well-being (t = 3.01; p <.003), current traumatic distress (t = 3.96; p <.001), trait anger (t = 2.25; p <.03), and expressive anger (t = 2.08; p <.04). The instrumental anger score approached significance at p < .07 and the state anger composite score was not significantly different from pre-to post-intervention although mean change was in the predicted direction (Figure 1). Consort Flow Diagram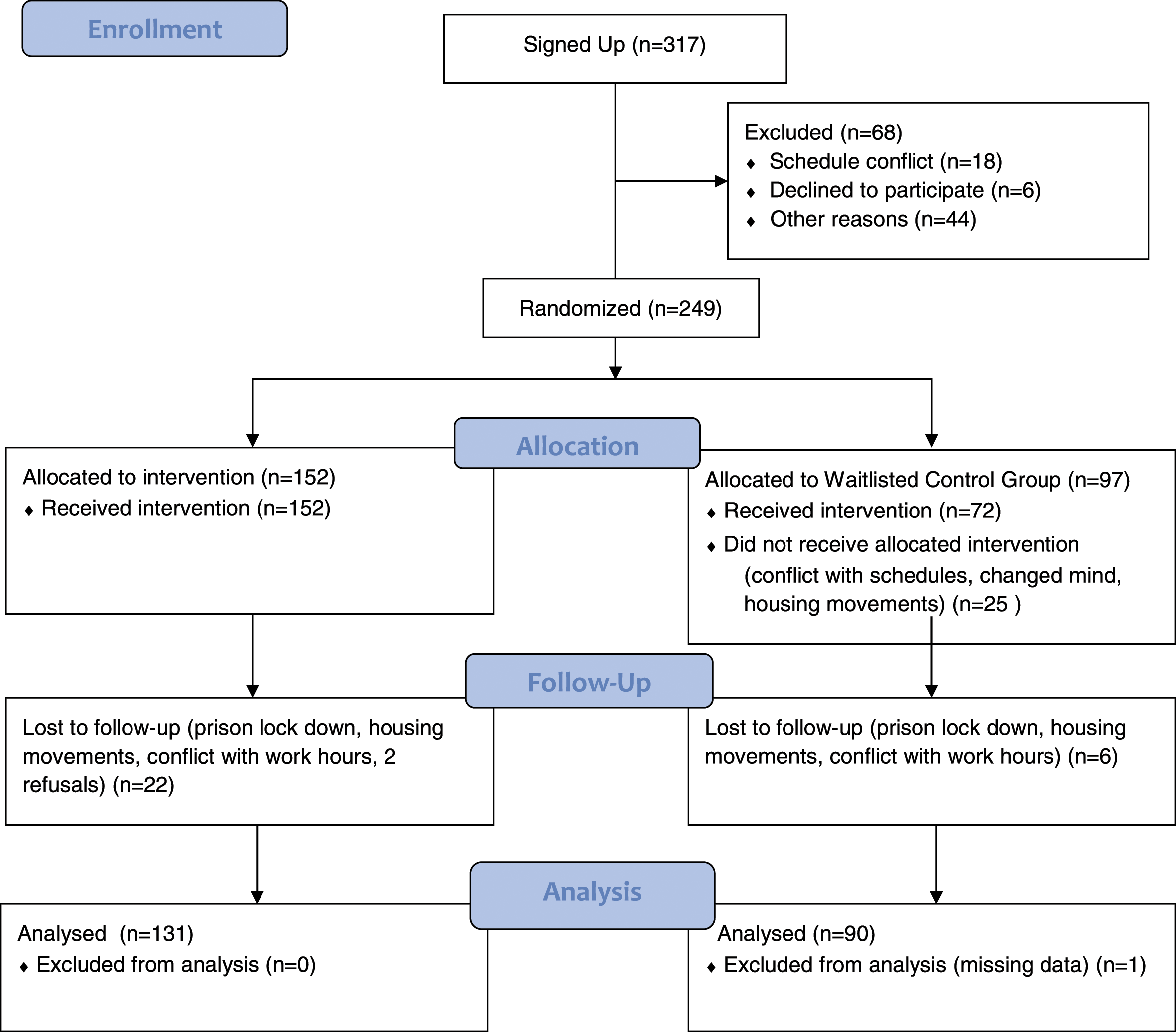
Discussion
The results from this experimental study substantiate the positive findings from the previous pilot studies among incarcerated populations at multiple levels of security risk classification (e.g., SHU, Levels, II, III, IV). This study confirmed that current trauma-related mental health problems and anger and aggression can be lessened and managed when appropriately addressed with a trauma-specific psychoeducational intervention. Thus, the intervention may help maintain security of the facility by decreasing anger and aggression among the participants and preventing worsening of mental health symptoms. This finding is a meaningful contribution to the literature given the crucial need to create a safe environment for both custody staff and residents. Reductions in precursors to violence ultimately result in reduced costs related to medical care, case reviews, legal action, and decreased trauma for staff and residents. The combined findings reported for ET and other supportive literature indicate that there is great potential for trauma-specific program services to be implemented among corrections populations.
Although statistically significant reductions in pre- and post-intervention mean differences were found in all but one of the outcomes measured favoring the treatment group, the effect sizes were not large. The greatest impact was on current symptoms of mental health impairment, anxiety, and trait anger (i.e., reductions in intensity of anger as a constant component of personality). Yet these are important areas of study, in that prison is a highly traumatic and violent environment, potentially more so for those with mental health issues. The degree to which these symptoms can be managed and diminished, particularly from a brief intervention, indicates a promising ability to enhance well-being and coping skills to manage feelings of anger.
Outcomes showing significant mean changes favoring the treatment group, albeit with lower effect sizes, such as current traumatic distress, suggests that participants may need more intensive trauma-specific interventions to manage current and ongoing trauma symptomology.
One outcome that deserves further exploration is the state anger composite scale assessing the intensity of angry feelings as a temporary emotional state versus the trait anger composite scale measuring the intensity of anger as a constant component of personality or a general emotion attached to anger. The trait anger composite significantly decreased for the treatment group compared with the waitlist control group, while there were no differences for the state anger composite scale. The state anger composite reflects an impact on angry feelings at a particular time, a temporary feeling, and the intensity of that emotion. This may be difficult to regulate in a highly volatile environment, such as prison, where a threat may necessitate or trigger an immediate reaction. The implication could also be that longer and more intensive trauma-specific interventions are needed to further address trauma-related anger and reactions.
This study contributes to the evidence supporting Peer-facilitated programming as an impactful and cost-effective model of delivery. The consistent outcomes from the current study and previous pilot studies, without any reported rule violations or peer misconduct indicated successful implementation of Peer-facilitation in prison. The research findings also provide evidence that those with histories of childhood maltreatment can be treated in a custody setting when the program content is addressing those histories with safety and appropriate material. A recent experimental study has also shown the successful implementation of a Peer-facilitated 20- session intensive violence prevention program for incarcerated women, that is, Beyond Violence (Covington, 2016; Messina & Calhoun, 2020). The ET program has also demonstrated positive results when facilitated by trained Program Coordinators in SHUs, where Peer-facilitation is not allowed (Messina & Burdon, 2021). The current findings are further applicable to corrections services as they indicate the efficacy of brief interventions as an additional cost-effective treatment opportunity for those in short-stay housing units (e.g., reception centers, SHUs, pre-release, etc.). Additionally, brief trauma-specific interventions can be used as a method of providing more immediate attention to clients on waiting lists for specialized programs or motivating an individual to begin to focus on behavior change and continue programming (Bagnall et al., 2015).
Strengths
This study employed the most rigorous evaluative methodology needed to determine if an intervention is evidence-based. By adding a randomized control group, without group violations and with a high follow up rate, study results increase the reliability and validity of the previous findings. ET is also a manualized intervention which creates standardization of delivery and the ability to monitor fidelity of facilitation. Peer-facilitators were trained by the program authors and program implementation had oversight by Program Coordinators (also trained by the program authors). Additionally, the Peer-facilitators delivered the intervention, and research staff administered the surveys, reducing the likelihood of social desirability bias. Finally, data elements were included to validate the trajectories of violence in the participant’s lives, both as victims and perpetrators. As the ET program was delivered to specifically address trauma among a population convicted of violent offenses, it was vital to determine that the intervention was efficacious for the target population. The results from the perpetration and victimization history surveys demonstrated the high prevalence of reported victimization and perpetration within the sample, and further indicated that these experiences were inextricably linked in this sample. In sum, the current study’s methodology resulted in a rigorous evaluation among the targeted population.
Limitations
Although this study had several methodological strengths, it also had limitations. The study sample may not be representative of male prison populations nationally. California’s recent policy changes enacted lengthy sentences for those convicted of violent offenses (e.g., crimes against persons involving force, use of a weapon, homicide, manslaughter, assault, and sex offenses) (Owen & Mobley, 2012). Yet, they are similar with regard to the high rates of trauma and substance use found nationally in justice-involved populations (Henry, 2020b). There is also the potential for a biased estimation resulting from sample attrition. There were some difficulties in scheduling follow up interviews with treatment participants beyond research staff control.
However, comparisons between the small percentage lost at follow-up did not show significant differences with those who completed the follow up surveys (89%). Finally, post-release outcomes were not obtained due to the lengthy sentences among the sample for serious violent crimes.
Policy Implications
While the prevalence of trauma and abuse are high among justice-involved populations, the opportunity for trauma-specific treatment is sparse. Historically, corrections-based treatment has focused on reducing recidivism and research has driven the direction of interventions toward that goal. It is difficult to draw conclusions about the effectiveness of corrections-based treatment if the programs are not attending to the full reality of the complex needs of those under their care. Currently, the most widely used framework for guiding correctional interventions is the Risk-Need-Responsivity model, positing that the most intensive treatment should be focused on those at the highest risk of recidivism (Andrews et al., 2011; Bonta et al., 2000). However, this study’s findings show that brief trauma-specific psychoeducational programs can also be used to effect change in participants’ behaviors and their understanding of the lifelong impact of ACEs.
The findings are applicable to corrections-based treatment services indicating the positive impact of Peer-facilitated delivery models and replicated findings from meta-analyses reporting the usefulness of Peer-facilitated substance use programs (Bagnall et al., 2015; Petosa & Smith, 2014). An expert symposium conducted on the efficacy of Peer-facilitated programs in prison concluded that peer facilitation can improve health outcomes, with a positive impact for both facilitators and participants (Woodall et al., 2015). However, the intensive peer training, program oversight, manualized curricula, and institutional support in this project likely added to the success of the program delivery. This study draws attention to the ability to openly discuss and appropriately address childhood abuse in corrections-based programs. As treatment services progress and potentially incorporate a trauma-lens, special provisions should be made for subsequent psychological counseling and support as needed for peers and participants.
Correctional organizations must become both trauma-informed and trauma-responsive to change the culture of the environment and recognize the unmet needs for both residents and staff (Covington & Bloom, 2018).
Future Research
Longitudinal studies assessing multiple treatment outcome measures, both during confinement and after release, are necessary to further examine the ET program impact. As a six- session brief intervention, ET may be an ideal curriculum for introductory programming, short-term housing programing, or pre-release programming. Additional rigorous studies are needed, and future research should also measure the sustainability of the benefits of trauma-specific programs, incorporate more qualitative measures to unravel the positive dynamics of peer-facilitation and the safety of small groups, include official rule violation records, and include post-release outcome measures (e.g., psychological wellbeing, education, housing, employment, and recidivism). The ET program continues to operate in the California SHUs and the general prison population within several California facilities. The ET program has been expanded to meet the needs of transgender and gender-diverse populations (i.e., Exploring Trauma Plus), which is also offered within multiple institutions in California.
Footnotes
Acknowledgments
This randomized controlled trial would not have been possible without the strong support and engagement of the California Department of Corrections and Rehabilitation (CDCR) Lead Administrators such as former FOPS Directors, Jay Virbel and Amy Miller, the Director and Deputy Director of the Department of Rehabilitative Programming, Brantley Choate and Kevin Hoffman, and the institutional staff at the California State Prison, Corcoran. We are especially grateful to Dr Covington and Rob Rodriguez, the authors of Exploring Trauma: A Brief Intervention for Men. We would like to acknowledge the following individuals for their support of and contributions to the project. Warden Ken Clark, Warden (Acting) Michael Sexton, Retired Warden Dave Davies, Chief Deputy Warden Martin Gamboa, Captain Chris Lesniak, Captain Raymond Juarez, Correctional Counselor III Shawn Rocha, Correctional Counselor II Josh Phelps, Correctional Counselor II Veronica Plata, Correctional Counselor III Juan Bugarin, Correctional Captain O’brian Bailey, PSA Ana Hernandez, Michael Tann (Retired Deputy Warden and EJS Program Coordinator), and Dr William Burdon (EJS Research Director). Finally, we are grateful to the men who facilitated the program and the participants who volunteered their time.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This pilot project was funded by the California Department of Corrections and Rehabilitation (CDCR), Department of Rehabilitative Programs (DRP), via the Innovative Grant Round III Long Term Offender Programs. CDCR contracted with Envisioning Justice Solutions, Inc. for the research component of the project. EJS provided a subcontract to the Center for Gender and Justice to provide the training and materials for the brief intervention.