
Abstract
Background: Despite a robust consensus regarding the potentially negative implications of childhood sexual abuse (CSA), research investigating risk and protective factors—particularly among well-functioning young adults—is scant. Dissociation is one of the major maladaptive outcomes of CSA. Nevertheless, CSA explains only about 10% of the variance of dissociation. Possibly, this modest effect size is due to protective factors moderating the relation between CSA and dissociative symptoms. One such factor may be the extent to which one has succeeded in developing a clear and coherent sense of who they are. Objective: We aimed to explore whether self-concept clarity (SCC) moderates the relationship between CSA and dissociation (Model 1), and an alternative hypothesis, whereby CSA may moderate the relationship between SCC and dissociation (Model 2). Participants and Setting: This was tested among 65 well-functioning young women drawn from an earlier study that intentionally oversampled CSA survivors. Methods: We included data from survivors of CSA by a known perpetrator (n = 35) and women with no sexual trauma (n = 30). Results: Findings were consistent with both Model 1 and Model 2, but only when depersonalization-derealization, namely detachment, was considered. Simple effects analyses revealed that CSA was related to depersonalization-derealization only under low SCC levels (Model 1), and SCC was negatively related to depersonalization-derealization only in the CSA group (Model 2). Conclusions: Findings suggest that SCC is a protective factor, buffering the association between CSA and detachment (depersonalization-derealization) symptoms. Clinical implications are discussed.
Childhood sexual abuse (CSA), a powerful and widespread traumatic stressor, has been associated with potentially negative short and long-term implications pertaining to different domains of development, as well as to physical and psychological wellbeing (Dunn et al., 2018; Fergusson et al., 2013). Worldwide studies point to CSA rates as high as two to four out of every 10 women, demonstrated in both clinical (i.e., individuals experiencing significant psychopathological symptoms) and nonclinical samples, including well-functioning individuals and college students (e.g., Filipas & Ullman, 2006; Finkelhor et al., 2005; Lev-Wiesel et al., 2018). Nevertheless, studies exploring risk and resilience among CSA survivors have focused mostly on at-risk or clinical samples, with very few studies (Godbout et al., 2014) addressing the implications of CSA among well-functioning young women, namely, female survivors of CSA who are functioning well psychologically, socially, and occupationally. Focusing on the latter is needed as it may broaden the understanding of the potential impact of CSA on larger parts of the population. Moreover, it may facilitate the identification of resilience factors, as a larger variability is expected to be found within such factors among well-functioning individuals. This is especially important as, despite a strong consensus regarding the implications of CSA, there is a need to further identify potential risk and protective factors (Dunn et al., 2018).
One of the most significant outcomes associated with CSA is dissociation (Vonderlin et al., 2018). Dissociation is regarded as a stress-related symptom usually reported by individuals exposed to adversities (Dalenberg et al., 2012). It has been described by Spiegel et al. (2011) as a disruption and/or discontinuity of typically integrated aspects of psychological functioning and mental processing, including consciousness, memory, identity, as well as cognition, and affect. Holmes et al. (2005) suggest that because the term dissociation has been used to describe a wide variety of processes and phenomena, it would be valuable to distinguish between two separate processes: detachment and compartmentalization. As per Holmes et al. (2005), detachment is defined as an altered state of consciousness characterized by a sense of separation from the self (i.e., depersonalization) or the world (i.e., derealization) that seemingly occurs in response to an overwhelming fear, and in chronic conditions, due to environmental or intra-personal triggers. Compartmentalization refers to the inability to deliberately control actions or cognitive processes that would normally be amenable to such control (e.g., dissociative amnesia and unexplained neurological symptoms characteristic of conversion). It seems that in such situations, the affected process or information remains intact despite being inaccessible—it becomes compartmentalized (Holmes et al., 2005).
Dissociation has been identified as one of the most potent and recognized psychological processes associated with childhood trauma and specifically CSA. Thus, CSA predicts dissociation over and above non-specific predictors such as general psychopathology or parental dysfunction (Chiu et al., 2015; Vonderlin et al., 2018). Moreover, studies have identified dissociation as a significant risk factor not only highly correlated with CSA (Vonderlin et al., 2018), but also as a meaningful mediator in the association between CSA and psychological symptoms, as well as revictimization (e.g., Ensink et al., 2017; Messman-Moore & Long, 2003). Although trauma is considered to be a major cause of dissociation among a large array of populations (for review see: Dalenberg et al., 2012), it explains only about 10% of the variance in dissociative experiences (as can be inferred by an average effect size of .31 for sexual abuse samples, and .32 for the overall weighted r estimate reviewed in Dalenberg et al., 2012). Nonetheless, according to the authors, the statistical significance of the overall weighted rs indeed support the consistency of the trauma–dissociation link across samples, whereas the heterogeneity of the effect size suggests the presence of mediators or moderators presumably affecting the strength, but not the presence of the trauma–dissociation association (Dalenberg et al., 2012). In line with this suggestion, it is important to identify protective factors (moderators) that may attenuate the impact of CSA on dissociation. The current study aims to shed light on the association between CSA and dissociation among well-functioning individuals by focusing on the potentially protective role of self-concept clarity (SCC).
Self-concept clarity refers to a positive and consistent self-perception as well as to the coherence of an individual’s identity, the level of confidence about one’s attributes, and the consistency and stability of these attributes across circumstances and roles (Campbell et al., 1996; Stinson et al., 2008). Growing attention has been given to the role of SCC in the onset and development of psychopathology. Studies have shown that low levels of SCC were associated with poor psychological adjustment and functioning whereas high levels of SCC were related to adaptive psychological adjustment and functioning (for review see: Cicero, 2017). Low SCC has been linked to diverse psychological difficulties, including depression, anxiety, autism, schizophrenia, and post-traumatic stress disorder (Binsale, 2017). Specifically in the context of childhood trauma, SCC mediated the association between childhood adversities, including CSA, and diverse mental health outcomes: suicidal behavior, depression, loneliness, perceived stress, and life distress (Wong et al., 2019). Similarly, SCC and dissociation mediated the associations between emotional or physical abuse or neglect and psychosis (Evans et al., 2015). Moreover, low SCC was suggested as the mechanism through which childhood trauma results in adulthood psychopathology (Cicero, 2017).
High SCC has been shown to play a significant protective role against the emergence of psychopathology and has been associated with higher levels of psychological adjustment and subjective wellbeing (e.g., Campbell et al., 2003; Ritchie et al., 2011), and lower levels of psychological distress among young adults (Schiller et al., 2016). As a longitudinal protective factor, SCC buffered the effect of low self-esteem on depressive symptoms two years later, in a study exemplifying the positive contribution of a cohesive and stable self-perception (self-esteem and SCC) in the face of life stress (Lee-Flynn et al., 2011). In another study, SCC was not only negatively associated with depression after a 1-year interval, but it also buffered the impact of the vulnerability factor “silencing the self” on depressive symptoms. Specifically, silencing the self was positively associated with depressive symptoms only when SCC was low (Peleg-Sagy & Shahar, 2015).
These findings highlight the potentially protective role of SCC in ameliorating the negative impact of stress and other self-related vulnerability factors on psychopathology. Hasson-Ohayon et al. (2016) suggest that SCC may play a key role in the development and maintenance of a coherent, positive, and non-stigmatized sense of self among individuals diagnosed with serious mental illness, which may in itself promote resilience. The subjective perception of stability, consistency, and coherency in the self-concept may serve as a protective factor as it may reduce internal conflicts in the face of stress (Chiu et al., 2017). Another possible reason for the aforementioned findings has been given by Smith et al. (1996), showing that individuals with higher levels of SCC tend to display more adaptive coping styles, whereas individuals with low levels of SCC tend to rely on more passive coping styles (e.g., mental and/or behavioral disengagement, denial, and substance abuse).
In the context of CSA, individuals with low SCC may exhibit more passive coping strategies exemplified in higher levels of dissociative experiences, whereas individuals with high levels of SCC may demonstrate lower levels of dissociation. Support for this notion can be found in a study testing whether self-concept organization differs among individuals with different levels of dissociation proneness, showing that dissociation proneness was associated with decreases in SCC (Chiu et al., 2017). This proximity between dissociation and SCC raises the question of whether they are distinct concepts or whether they both reflect the same psychological construct. Since dissociation includes additional features, other than altered self-perception, it has been argued that low levels of SCC are an intrinsic part of dissociation (Chiu et al., 2017; Evans et al., 2015). We suggest that these concepts are indeed closely connected and relevant for a mutual exploration, but also that they are distinct psychological concepts, as will be elaborated below.
Of the three broad categories comprising the self, namely, content, process, and structure (Stopa, 2009), SCC is located within the category of content—that is, the specific information about the self, and structure—that is, the way in which information about the self is organized (Binsale, 2017). Dissociation, on the other hand, seems to be a process, since it involves alterations of attention and awareness towards one’s mental processes, sometimes as a strategic defense mechanism in the face of overwhelming emotion (Spiegel et al., 2011). Another distinction between the concepts pertains to the different aspects of self-unity reflected by SCC versus dissociation. Specifically, it has been suggested that SCC relates to the conceptual self, that is, what one believes about oneself, whereas dissociation relates to the phenomenological experience of the self, that is, one’s subjective experience of being (Holm & Thomsen, 2018). Chiu et al. (2017) suggest that future studies should clarify the interrelationships between the structures of self-concept, traumatization, and the altered sense of self in dissociative disorders. Nevertheless, to the best of our knowledge, the role of SCC in understanding the relationship between CSA and dissociation has yet to be tested, paving the way to the current study.
More specifically, we focused on young adulthood because it represents a period in identity development where there is an increasing interest and motivation to define one’s self (Arnett, 2000). This developmental period has been identified in both theory and research as particularly challenging, as young individuals are expected by society to immerse themselves in diverse experiences, from which they might potentially extract a coherent life story (Bauer & McAdams, 2004). As discussed herein, a central aspect of establishing one’s identity is securing a coherent, clear, and positive sense of self, a process that might be compromised by various life stressors, including a history of childhood trauma.
The Current Study
In the current study, we aimed to unveil the potentially intervening role of SCC in the association between CSA and dissociation. Based on the above literature review, we theorized that a clear, well-defined self-concept may constitute a resilience factor associated with lower levels of dissociative symptoms, even in the presence of a traumatic background. In contrast, a blurred self-concept may serve as a vulnerability factor. We relied on the idea that a self-concept which remains stable across life events and situations may help to coherently weave an individual’s past trauma into their personal narrative and enable them to deal with their trauma-related emotions by using defenses or coping mechanisms which are more adaptive than dissociation. Indeed, an unintegrated self-concept is related to dissociation (Lutz & Ross, 2003) and low levels of SCC are associated with maladaptive coping with stressors (Willis & Burnett, 2016) and childhood traumas (Cicero, 2017). Thus, we expected that the association between CSA and dissociation will only be significant among individuals with low SCC, but not among individuals with high SCC. In line with the notion of distinguishing between the two separate processes comprising dissociation, we aimed to test this model (henceforth Model 1) both in terms of detachment and in terms of compartmentalization processes (Holmes et al., 2005).
Additionally, we examined whether the link between SCC and dissociation is dependent upon the existence of CSA. As mentioned earlier, both low SCC and high dissociation are manifested in poor consolidation of the self, but we presume they are not identical constructs. We propose that dissociation reflects disintegration of the self in a more basic, perceptual, less conscious level, or as suggested by Holm and Thomsen (2018), at a phenomenological level. Chiu et al. (2017) suggest that individuals with dissociation proneness have a unique self-concept structure characterized by low clarity and polarized evaluations of self-aspects, but which is insufficient for the emergence of dissociative identity symptoms. Therefore, they suggested a stress-diathesis model, in which childhood traumatization may interact with this characteristic structure and result in dissociative symptoms. Our alternative model (Model 2) aimed to investigate a similar question, as we examined whether a history of childhood abuse may be a trigger that causes a blurred self-concept to escalate into dissociation, whereas in the absence of childhood abuse, such incoherent self-concept will not be deteriorated to the point of dissociation. We thus hypothesized that SCC will be associated with dissociation only among CSA survivors, but not among non-traumatized individuals. Finally, we examined Model 1 and Model 2 among young adult females, including CSA survivors who had been sexually abused by a familiar perpetrator and women who reported the absence of any sexual trauma.
Methods
Participants And Procedure
Sixty-five high-functioning young adult female subjects (Mage = 25.59, SD age = 3.89) participated in the study, 35 of them reporting a history of childhood sexual abuse (CSA) and 30 of them reporting no such history. The sample was drawn from a larger project focusing on the implications of childhood experiences on young adults’ well-being [masked for review]. Participants were sought via announcements on websites and internet forums for CSA survivors, bulletin boards posted throughout universities, rape crisis centers, public psychological service clinics, therapists’ clinics, and service centers for sexually abused women. General inclusion criteria for the study were as follows: (a) young adult female aged 18–39; (b) for those with a history of CSA, the abuse had to have involved a known, nonpeer perpetrator, as assessed using multiple measures (as detailed in the Measures section below); and (c) being engaged in a meaningful romantic relationship (with a partner either of different or same sex and/or gender) for at least 1 month within the past 3 months. In order to sample well-functioning individuals, participants completed a screening questionnaire at the beginning of the study, addressing their functioning on occupational, educational, physical, social, romantic, and psychological aspects. Then, one of the first authors (DL), a clinical psychologist, screened individuals according to their level of functioning, based on the Global Assessment of Functioning (GAF) Scale from the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV TR; American Psychiatric Association, 2000). Exclusion criteria therefore included currently severe psychological symptoms or current hospitalization in an inpatient psychiatric ward. Assessment was conducted using self-report questionnaires administered by email or in person, according to the participant’s preference. Upon completion of the surveys, the participants were financially compensated with $40 for their time.
The sample was ethnically and demographically varied, including participants from different geographical areas (urban and rural regions), with various financial statuses, occupations, and different kinds of religious practices. The majority of the sample (91%) described their sexual orientation as heterosexual. There were no significant differences between participants with and without a history of CSA in age (t(55) = 1.20, ns; M = 26.10, SD = 4.68 for CSA; M = 24.99, SD = 2.64 for non-CSA) and years of education (t(62) = 1.14, ns; M = 13.77, SD = 1.99 for CSA; M = 13.28, SD = 1.36 for non-CSA). The study was approved by the Ethics Committee of the Department of Psychology at [masked for review].
This study included two phases with 99 participants in the first and 65 in the second. Since SCC was assessed only in the second phase, participants who dropped out before this phase were not included in the present investigation. In order to support the validity of our results rather than the possibility that drop-out influenced them, we also ran analyses on the full sample of 99 participants, while imputing their SCC missing values using multiple imputations (Sterne et al., 2009). Specifically, the SCC missing data were imputed five times, with values which were sampled from their predictive distribution based on the observed data, to generate five complete and different possible data sets. Then, we applied our regression models on the five imputed datasets and observed pooled estimates derived from all possibilities. Our findings remained the same using the pooled estimates as well as in all individual datasets, suggesting that results did not seem to be affected by drop-out.
Measures
Child sexual abuse was assessed using three questionnaires: the Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998), the sexual Experiences Survey–Short Form Victimization Revised (SES-SFV; Koss et al., 2007; Koss & Gidycz, 1985), and the Post-Traumatic Stress Diagnostic Scale–Part I (PDS; Foa, 1995). The CTQ is a 28-item retrospective self-report questionnaire. Individuals are asked to indicate on a 5-point Likert scale how often (1 =never, 5 =frequently) they experienced certain events as children or as adolescents. These items yield five different subscales of childhood trauma: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect (Bernstein & Fink, 1998). The CTQ has been found to be valid for use in clinical and nonclinical populations (Scher et al., 2001) and demonstrated a strong convergence with the Childhood Trauma Interview (Bernstein & Fink, 1998). In this study, only the sexual abuse subscale was used, ranging from a minimum of 5 (replying never in all five items assessing sexual abuse) to a maximum of 25. Internal consistency was: Cronbach’s α = .95. Participants scoring 6 and above were further examined to meet study criteria for CSA, namely, whether the perpetrator was both known and not a peer. In cases where participants scored higher than 6, but also reported on different measures that the abuse was perpetrated by either a nonfamiliar person or a peer, or during adulthood, they were omitted from the study. Also, only participants who scored five on the levels of sexual abuse subscale were included as non-CSA participants; The SES-SFV is a shortened, modified version of the Sexual Experiences Survey (Koss & Gidycz, 1985). Participants were asked if they had ever (as children, adolescent, or adults) undergone any of 11 sexual experiences, their age at the time, the perpetrator relationship (stranger, acquaintance, and family member), and the frequency of the experience (four categories: none, once, few, and many). The SES-SFV was also used to gain additional information regarding the age when the abuse began and ended, its frequency, and the perpetrator’s relationship to the survivor. Data collected using this questionnaire were employed for screening for both the CSA survivors or the non-CSA participants. The latter group included only women scoring zero on the SES-SFV, indicating the absence of any form of sexual trauma. In this sample Cronbach’s α = .84; The PDS (Foa, 1995) asks respondents to read through a list of traumatic events and checkmark any event they had witnessed or experienced. Only women who checked the events “sexually assaulted or abused by a familiar perpetrator” or “engaged in a sexual relationship with someone more than 5 years older” (in this case, a clarification was initiated to assess whether the relationship was considered as sexual abuse) were included in the sample as CSA survivors. In this sample, Cronbach’s α = .94. Based on the described criteria, participants were assigned to a binary CSA dummy variable: (a) non-CSA and (b) CSA survivors.
Means, Standard Deviations, Skewness, Kurtosis, and Zero-Order Correlations Between Dissociative experiences and Self-Concept Clarity.
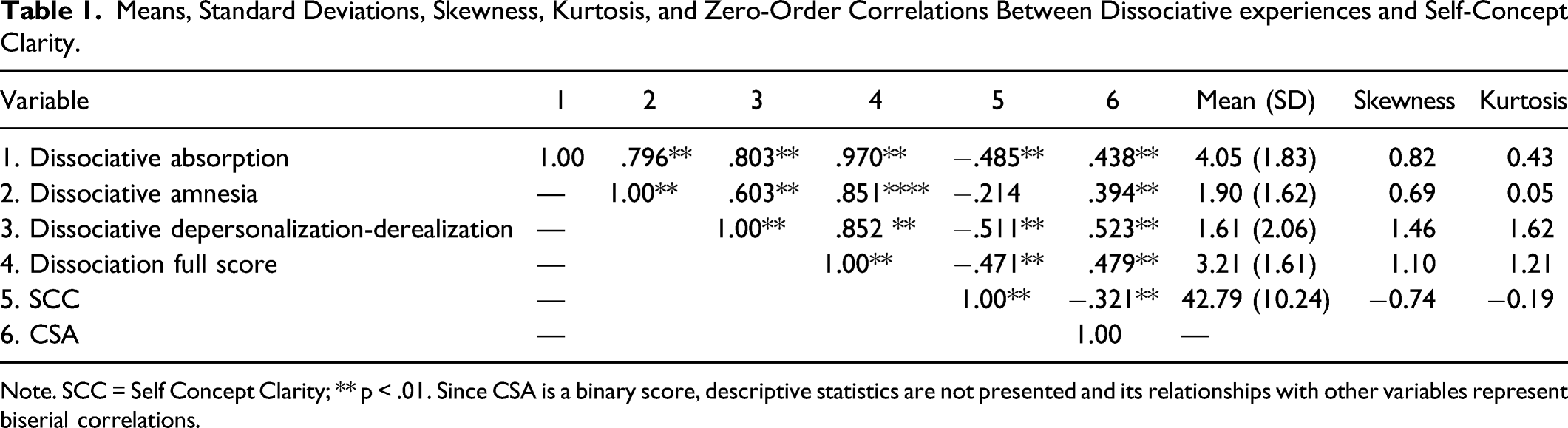
Note. SCC = Self Concept Clarity; ** p < .01. Since CSA is a binary score, descriptive statistics are not presented and its relationships with other variables represent biserial correlations.
Self-Concept Clarity was assessed using a 12-item, 5-point Likert scale (SCC; Campbell et al., 1996). Each item is related to perceived consistency and clarity of sense of self. From the scale’s 12 items, 10 are reverse-keyed (e.g., “Sometimes I think I know other people better than I know myself”) while the remaining two are not (e.g., ‘‘In general, I have a clear sense of who I am’’). The negative items are reverse-scored, and a total score is calculated as a sum of all the items, so a higher score indicates higher SCC. The questionnaire is reported to have good internal consistency and test-retest reliability (Campbell et al., 1996). In this sample, Cronbach’s α = .89.
Data Analysis
All analyses were performed using SPSS. First, we attenuated the possible influence of outliers as suggested by Tabachnick, Fidell, and Ullman (2007). We standardized the dissociation and SCC variables and inspected their histograms; any score of over Z = 3.29 or under Z = −3.29 that was not attached to the rest of the distribution was changed to a less extreme score (specifically, a single unit above or below the edge of the distribution, respectively). Next, we analyzed the data using linear regression models, assessing the role of SCC as a possible moderator (Model 1) between CSA (operationalized as the binary/group variable) and dissociation (manifested by each of the dissociative variables), as well as the role of CSA as a moderator (Model 2) of the relationship between SCC and dissociation. SCC was centered beforehand. Since the sample was modest and the dissociative variables were not normally distributed, analyses were carried out using bootstrapping (based on 1000 re-samples and bias corrected and accelerated confidence intervals). Hypothesis testing based on bootstrapping means that it is not necessary to assume a normal-shaped distribution of variables.
Results
Means, Standard Deviations, and Zero-Order Correlations
Table 1 presents descriptive statistics of all study variables. All the dissociative variables were not distributed normally among our participants, and thus transformed with a square root transformation to acceptable limits of ±2 for skewness and kurtosis (Gravetter & Wallnau, 2014). The transformed variables were used in all analyses. The lack of normality in the raw dissociative variables supports our decision to use the bootstrapping method for our hypothesis testing. Self-concept clarity was distributed normally. Also, as shown in Table 1, CSA was positively related to all subscales of dissociation, and negatively linked to SCC. Self-concept clarity was significantly associated with depersonalization-derealization, absorption, and with the total score of dissociation, but not with amnesia.
Hierarchical Multiple Regression Models
Hierarchical multiple regression model, predicting subtypes of dissociative experiences (dissociative depersonalization-derealization, dissociative amnesia, and dissociative absorption).
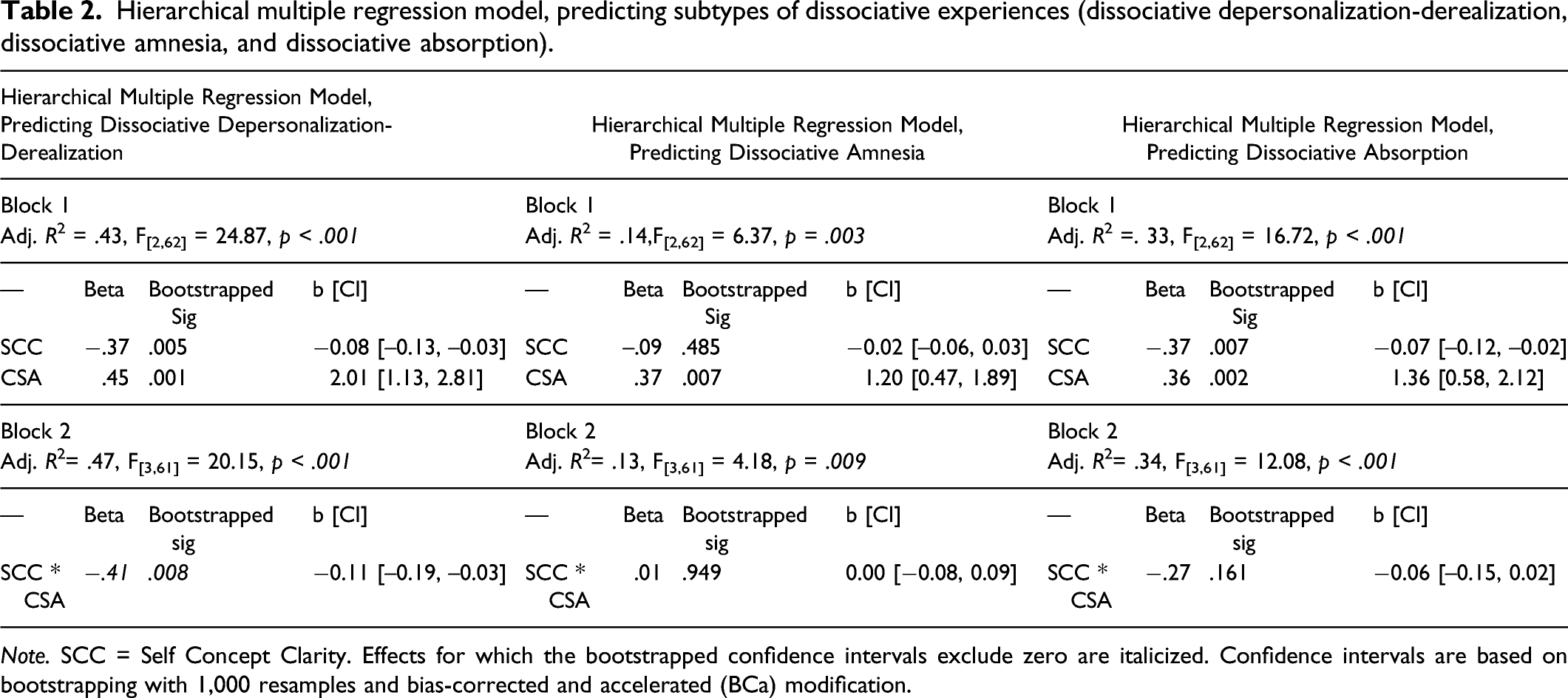
Note. SCC = Self Concept Clarity. Effects for which the bootstrapped confidence intervals exclude zero are italicized. Confidence intervals are based on bootstrapping with 1,000 resamples and bias-corrected and accelerated (BCa) modification.
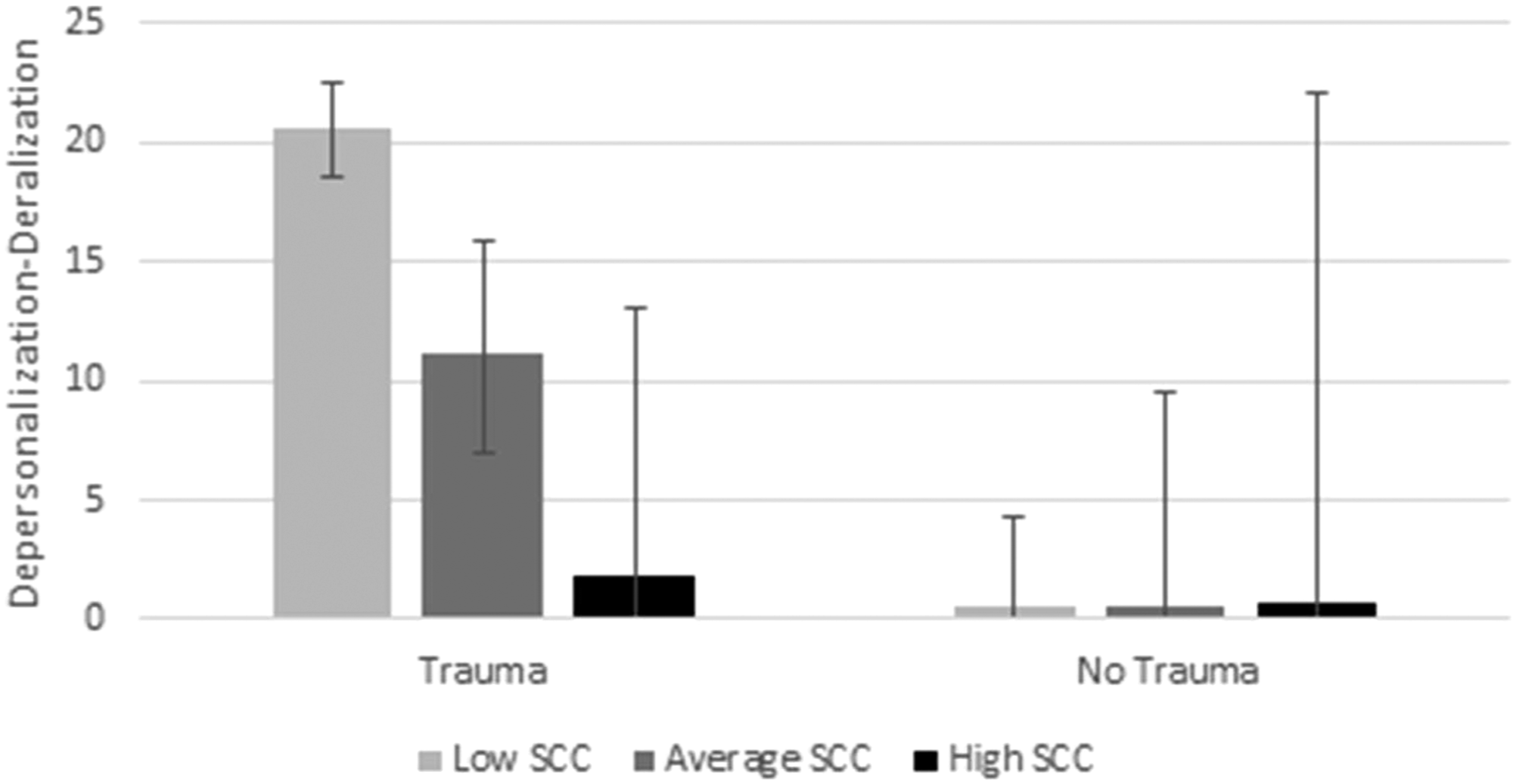
Simple effects analyses examining the hypothesis of Model 1.
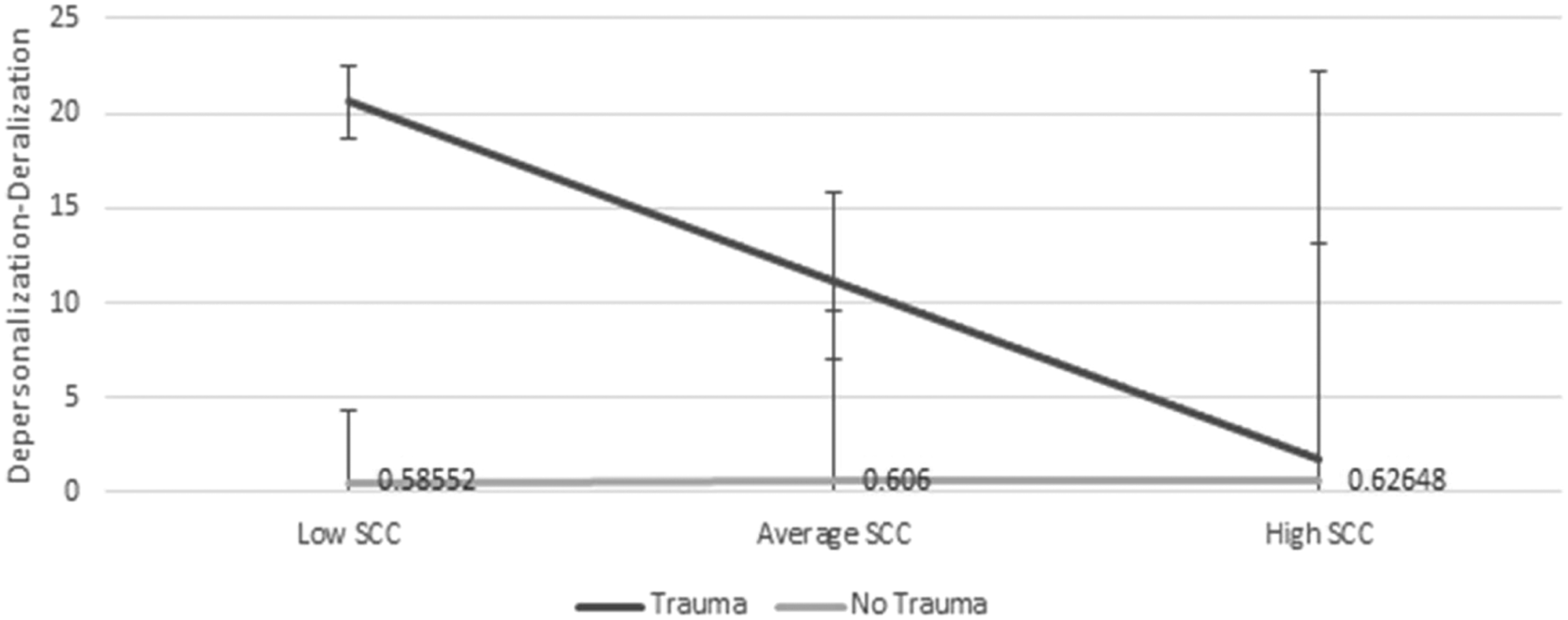
Simple slopes analyses examining the hypothesis of Model 2.
Contrary to our hypotheses, in the regression models predicting the two other dissociative variables, namely, dissociative amnesia and dissociative absorption, no interactions emerged between CSA and SCC.
Discussion
The aim of the current study was to investigate the interplay between CSA, SCC, and dissociation, in a sample of otherwise well-functioning young women, comprising survivors of CSA by a known perpetrator and women who reported never having been exposed to sexual trauma. Our main objective was to examine whether SCC may be a factor which intervenes with the emergence of dissociative symptoms among individuals that deal with a history of CSA (Model 1). More specifically, we investigated whether high levels of SCC constitute a resilience factor against the development of dissociation (or in other words, whether low levels of SCC are a risk factor strengthening the trauma-dissociation relationship). Additionally, we tested an alternative model, examining whether having a history of CSA may be the factor that determines whether low SCC will be associated with dissociation (Model 2). The hypotheses of this study were partially supported.
Specifically, SCC did not moderate the relationship between CSA and amnesia (compartmentalization) or absorption, but it did moderate the association between CSA and depersonalization-derealization, reflecting detachment. The lack of findings involving compartmentalization (dissociative amnesia) in our sample may, to some degree, stem from an inadequacy of the amnesia subscale of the DES. Previous studies have suggested that this subscale is less suitable for investigations of correlations between dissociative experiences and psychopathological symptoms (e.g., Soffer-Dudek et al., 2015; Spindler & Elklit, 2003). Also, the DES amnesia subscale may have limited validity when used in nonclinical samples such as ours, as Spindler and Elklit (2003) noted it had an inferior internal consistency when compared to the other DES subscales. Alternatively, the results may reflect a true difference between the dissociative functions. These results are congruent with the notion of Holmes et al. (2005) that depersonalization-derealization (detachment) represents a statistically separable factor from amnesia (compartmentalization) in the DES, even though in practice they might often be highly correlated.
Regarding the absorption subscale, the lack of findings might be, at least partially, the result of a lack of statistical power, given our small sample size. But it may also express a qualitative difference between absorption and depersonalization-derealization, concerning their affinity to trauma. Previous work had indicated that absorption is strongly related to psychopathology, but not necessarily as a consequence of trauma (Soffer-Dudek & Somer, 2021). It has been related to other types of pathologies, such as obsessive-compulsive symptoms (Soffer-Dudek, 2019). Depersonalization-derealization, on the other hand, represents a more extreme manifestation of dissociation, which is intrinsically associated with trauma: peritraumatic dissociation is characterized by depersonalization and derealization (Marmar et al., 2004), and episodes of depersonalization and derealization are a central element in the diagnosis of Acute Stress Disorder (Cardeña & Carlson, 2011). In other words, both depersonalization-derealization and absorption are associated with a lowered clarity of the concept of self, but the former is more relevant to traumatic stressors.
Our results support the notion that a consistent and coherent self-perception may act as a resilience factor buffering the tendency to detach, even in the presence of a history of a potent traumatic stressor such as CSA. As discussed herein, it is plausible that a stable, consistent, and coherent self-concept may reduce internal conflicts in the face of stress (Chiu et al., 2017), thereby allowing CSA survivors to deal with stressful situations without feeling emotionally overwhelmed in a way that may lead them to dissociate from their selves (depersonalization) or from the external reality (derealization).
In contrast, among CSA survivors with a blurred self-concept, their self-perception may not be able to prevent them from turning to detachment mechanisms. Low-SCC individuals may feel that their self-beliefs are unstable, or even worse, that different aspects of their personality are conflicted with each other, leaving them with a sense of a lack of unity within their self-concept (Campbell et al., 2003; Holm & Thomsen, 2018). In the face of stress, this can potentially translate into increased reliance on detachment from oneself and reality, as a strategic defense mechanism in the face of overwhelming emotion (Spiegel et al., 2011). Indeed, dissociation has been conceptualized as a defense toward negative emotions and a response to traumatic events (Spiegel et al., 2011; van Der Kolk & Fisler, 1995). Similarly, as suggested by Smith et al. (1996), SCC is not only an intra-psychic process as described above, but rather, it also manifests in the coping strategies chosen by individuals. Thus, while individuals with high levels of SCC tend to display more adaptive coping styles, those with low levels of SCC tend to rely on more passive ones, including dissociation (Chiu et al., 2017). Thereby, dissociative detachment may be regarded as a passive coping style used among some CSA survivors with low SCC, but it is unlikely to manifest among those with high levels of SCC.
This is the first study exemplifying the moderating role of SCC in the association between CSA and detachment. Our findings join previous ones in attesting to the protective role of high SCC in buffering the onset and development of psychopathology (e.g., Lee-Flynn et al., 2011; Peleg-Sagy & Shahar, 2015; Schiller et al., 2016). Current findings shed more light on existing knowledge regarding SCC, by demonstrating its moderating role in the specific context of dissociative detachment, a standalone pathology but also a powerful risk factor for further psychopathology among CSA survivors (Vonderlin et al., 2018). Moreover, our results contribute to a better understanding of the interplay between CSA and dissociation. Although CSA is considered to be a major cause of dissociation, it explains only a relatively small portion of its variance (Dalenberg et al., 2012). Our findings suggest that SCC may explain a part of this unexplained variance. These findings corroborate the stress-diathesis model introduced by Chiu et al. (2017) which explained dissociative symptomology as a result of an interaction between childhood traumatization (i.e., stress) and a specific structure of self, characterized by low SCC (i.e., diathesis).
Likewise, our findings demonstrate that under low levels of SCC, individuals are more likely to be vulnerable to detachment, a potent and recognized psychological process associated with symptomatic distress. Thus, given that dissociation is a widely demonstrated risk factor for psychopathology among CSA survivors, it can be argued that our findings are also consistent with outcomes showing that low levels of SCC were not only correlated with psychological maladaptation, but also mediated the association between childhood adversities and diverse mental health difficulties (Evans et al., 2015; Wong et al., 2019).
We also found, consistent with Model 2, that a history of CSA moderated the association between SCC and depersonalization-derealization. Thus, SCC was negatively significantly related to depersonalization-derealization, only among individuals with a history of CSA, but not among individuals reporting no sexual trauma. Our hypothesis that CSA may serve as a catalyst that exacerbates low SCC to the point of dissociation was only partially supported, as this pattern was significant specifically regarding detachment, but not for compartmentalization nor absorption. As noted above, we suggest that significant findings were found only in the context of depersonalization-derealization, because these dissociative experiences are most relevant to the type of population reviewed in this study.
In addition, our findings support our proposition that SCC and detachment, although related, pertain to different constructs. Although these two constructs share some conceptual similarity, they are not inseparably related, as demonstrated by the fact that their relation is dependent on whether there was a history of CSA or not. These findings are inconsistent with previous studies suggesting that low SCC is an intrinsic part of dissociation (Chiu et al., 2017; Evans et al., 2015). This difference may stem from several factors. First, the current study employed a moderation analysis, whereas both other studies probed only main effects. In other words, they did not probe whether trauma explained systematic variance in the dissociation-SCC relationship. Second, we focused on high-functioning CSA survivors and controls, whereas Chiu et al. (2017) focused on undergraduate students and Evans et al. (2015) on individuals with psychosis compared to controls. These different samples and methods of analyses make it difficult to directly compare the studies and raise a need for further research. Additional support obtained in our study for the separateness of SCC and dissociation pertains to findings showing that there are certain aspects of dissociation that are not related to SCC, as demonstrated in the non-significant link between SCC and amnesia (compartmentalization). However, none of the aforementioned findings, in our study or the other two studies mentioned, provides conclusive evidence about the overlap or distinction of SCC and dissociation. Such evidence can only be obtained with factor analytic studies based on large samples, hopefully utilized in future research.
Most studies in this field are based on clinical samples, leaving room to further investigate the implications of CSA, especially in terms of identifying potential risk and protective factors (Dunn et al., 2018). Focusing on this population has enabled us to identify SCC as a potential resilience factor in the association between CSA and detachment. Such knowledge can potentially be generalized to more vulnerable populations as well.
Limitations
Findings of this study should be considered within the following methodological limitations. First, the sample focused only on women and sample size was modest. To generalize our results to CSA survivors in general, it is important to replicate them with a larger, cross-cultural, sample that will include both men and women. Second, our study focused on participants that had met the criteria of being well-functioning individuals, thereby, the ability to generalize these findings to more diverse populations with a history of CSA may be limited. Notably, however, we chose to focus on this population given its relative marginalization in the literature on CSA, but we also recognize the resulting limitations. Third, even though earlier studies have attested to the accuracy and reliability of recall among survivors of childhood maltreatment (Dube et al., 2004) and CSA in particular (Barnes et al., 2009), shared method variance and reporting biases may nonetheless be present in our study. Thereby, additional assessment methods (e.g., interviews) should be included in future research. Moreover, missing SCC data in this sample was handled using multiple imputations, which predicts missing values based on existing observed data and random imputations. Although many regard this method of dealing with missing data as the gold standard, it does not guarantee full certainty regarding the true values of the missing data. Using a different technique for estimating the absent values could have resulted in different findings. Finally, tracking central variables via additional waves of assessments would enhance the study design, enable a better understanding of the interplay between all study variables, and allow for the examination of directional effects. It is also important to examine these subjects in a more representative sample, thus allowing to consider aspects of diversity.
Implications
Findings of this study may contribute to the understanding of the psychological dynamics accruing in the context of CSA and have important implications for the assessment and treatment of individuals with a history of CSA. Understanding how CSA transmits its harmful consequences and identifying resilience in this regard is essential for designing prevention and intervention programs. In this study we were able to identify SCC as a potential resilience factor. Our findings suggest that SCC is a protective factor against dissociative experiences of depersonalization and derealization (detachment), which are common in the general population (Hunter et al., 2004) but are severely underdiagnosed (Michal et al., 2016). Self-concept clarity was not found as a resilience factor regarding other types of dissociative experiences, that is, compartmentalization or absorption. This differentiation has important clinical implications, as it emphasizes that although various dissociative experiences are closely related, they do not constitute a single component. Understanding the specificity of dissociative processes is highly clinically relevant, as it assists the therapist in getting closer to the patient’s authentic experience, thereby promoting a better therapeutic alliance and allowing more efficiency in targeting specific areas of difficulty and need (Chefetz & Bromberg, 2004).
Psychopathology, dissociation, and SCC should be routinely assessed when sexually abused women consult for treatment. To reduce psychopathology, professionals might benefit from addressing SCC and dissociation, using targeted therapeutic interventions, especially those enhancing mentalization regarding self and others (Ensink et al., 2017) as well as interventions involving focus on attention and perception—found to be effective in reducing depersonalization and derealization (e.g., Donnelly & Neziroglu, 2010; Schweden et al., 2020). The current findings suggest that detachment may be approached in therapy through the concept of self. Arguably, building and strengthening the coherence of a survivor’s personal narrative of autobiographical events and their relation to the present-day self-concept across situations may reduce the tendency to detach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Israel Foundations Trustees (Doctoral Grant 29).