
Abstract
It has long been established that bullying has many negative impacts on the mental health of adolescents. Young people who are victimized by bullying may cope by drawing on available assets to protect themselves from harm. One such asset with ancient roots but with the potential for contemporary application is the concept of spiritual health—the idea that the connections in our lives (whether to ourselves, others, nature, or something transcendent) affect our well-being. In this study, we examined 12,593 Canadians aged 11–15 years to determine the effects of being victimized by bullying on their mental health, as measured by frequent subjective health complaints. We then explored whether strong spiritual health connections were effect modifiers that buffer such negative pathways, thereby acting as protective health assets. Data were obtained from the 2017/18 Canadian Health Behaviour in School-aged Children study. Generalized linear regression models were used to estimate associations and evaluate effect modification in different age and gender groups. Approximately 21% of participants reported being victimized by bullying. Strength of “connections to self” (i.e., a sense of meaning/purpose or joy and happiness in one’s life) was found to act as an effect modifier, but in girls alone. Contrary to expectations of a buffering effect, the strongest associations between victimization and frequent health complaints were identified for girls with high connections to self. Relative risks for poor mental health among these highly self-connected girls were 1.63 [95% CI: 1.26–2.12] and 1.25 [1.06–1.47] for younger and older girls, respectively. We interpreted this unexpected finding in light of cognitive theories of trauma, which suggest that adverse events may lead to worse health outcomes among those who place particular value on their world being meaningful, controllable or benevolent. Implications for clinical intervention and health promotion are considered.
Introduction
Bullying among young people is a global public health concern. Almost one in three students experiences some form of bullying victimization each month worldwide (United Nations Educational, Scientific and Cultural Organization, 2019) and this victimization has known consequences on their health. Bullied adolescents are at risk of internalizing problems such as depression, loneliness, anxiety, and low self-esteem (Hawker & Boulton, 2000). These patterns follow young people throughout the life course, with students who are bullied showing an increased long-term risk of depression up to 36 years after victimization (Ttofi et al., 2011). Victimization through bullying is also linked to physical symptoms, including headaches, stomach aches or sleeping difficulties (Due et al., 2005). Meta-analyses of both cross-sectional and longitudinal studies have demonstrated that bullied youth are at significantly increased risk of health complaints compared to non-bullied youth (Gini & Pozzoli, 2013). The clear adverse health impacts of this type of violence necessitate the development of interventions that are based upon a variety of different types of evidence.
One strategy that can be used to minimize the effects of bullying is to employ an “asset-based” approach, which draws upon strengths both within and external to children to help them develop in the healthiest possible manner, even in the face of adversity (Benson et al., 2007). Fostering protective health assets can help young people by buffering (moderating) the effects of exposure to adversity—such as bullying—on the risk of negative health outcomes (Kia-Keating et al., 2011). Few population-level studies have explored individual assets among populations of children who are victims of bullying. A U.S. study found that a strong “meaning in life” attenuated the association between bullying victimization and suicidal ideation in adolescent boys (Henry et al., 2014). In a similar study, García-Moya reported that among Spanish adolescents with a weaker sense of coherence, bullying was more strongly associated with psychosomatic symptoms when compared to those adolescents with a stronger sense of coherence (García-Moya et al., 2014).
One protective health asset with ancient roots but with the potential for contemporary application is spiritual health (Fisher, 2011; Miller & Thoresen, 2003). Spiritual health has long been studied in relation to perceptions of well-being and is integral in many indigenous traditions (King et al., 2009; Montenegro & Stephens, 2006; Tse et al., 2005) and holistic models of health (King & Benson, 2006). Inspired by these traditions, many have argued for the inclusion of spiritual health as a fourth domain in the World Health Organization’s (WHO) definition of health (Chirico, 2016; Vader, 2006).
Spiritual health is a difficult concept to define. One framework released in the 1970s by the National Interfaith Coalition (1975) has since provided a foundation for the study of adolescent spirituality as a multidimensional concept (Gomez & Fisher, 2003; Hay & Nye, 2006; Michaelson, Brooks, et al., 2016) that is distinct from formal religiosity (Hay & Nye, 2006). We adopt the following working definition:
Spiritual health is a dimension of health that entails a condition of spiritual well-being. This is a way of being that involves some capacity for awareness of the sacred qualities of life experiences and is characterized by connections in four domains: (1) self, (2) others, (3) nature, and (4) a sense of mystery or larger meaning to life, or whatever one considers to be ultimate. (Michaelson, Brooks, et al., 2016).
This definition focuses on the effects of connections that are both within (connections to self, measured through the reporting of a sense of meaning/purpose or joy in one’s life) and external (connections with others, to nature, and with the “transcendent”) to children (Michaelson, Brooks, et al., 2016).
Spiritual health is associated with self-reported health and well-being in young people (Brooks et al., 2018; Holder et al., 2010; Lerner et al., 2011). The spiritual health domains have also been established as a possible determinant of positive mental health in cross-national samples of students (Brooks et al., 2018; Michaelson, Brooks, et al., 2016; Michaelson et al., 2019). While the exact mechanisms by which these domains could act as protective health assets are not yet fully understood, the protective effects provided by a strong sense of spiritual health have been hypothesized to be mediated by the influence of mindfulness and emotional self-regulation on stress responses (Aldwin et al., 2014; Levenson & Aldwin, 2013).
The strength of associations between specific spiritual health connections and health have varied between studies; effects seem to depend on the outcome measure, individual domain, and demographically by age or gender. Cross-nationally, girls reported a heightened importance of these connections in their lives, and all children reported a decline in spiritual health with increased age (Michaelson, Brooks, et al., 2016; Michaelson, Trothen, et al., 2016). Prior studies have found that some of the spiritual health domains have stronger associations with positive health outcomes in girls than in boys (Brooks et al., 2018; Michaelson et al., 2019).
While spiritual health appears to act as a moderately strong asset that fosters health within the general adolescent population, we hypothesize that it may confer an even stronger protective benefit to youth at increased risk of poor mental health outcomes. Protective health assets must be studied within specific “at-risk” populations as assets may operate differently in particular contexts (Brooks & Kendall, 2013; Morgan & Ziglio, 2017). Evidence can then inform public health interventions that are appropriately targeted to such populations. While spiritual health has been established as an asset in general populations of adolescents, no published studies to date have focused on its protective effects among those who have been victimized by bullying-related violence.
In the current analysis, we had a novel opportunity to conduct a national study examining the association between bullying and subjective health complaints, as one specific indicator of poor internalizing mental health (Bohman et al., 2012; Campo, 2012). Our primary goal was to explore whether or not stronger indications of spiritual health connections act as effect modifiers to buffer the strength of relationships between bullying and impaired mental health. As a secondary objective, we proposed to explore if spiritual health connections moderated relationships between specific subtypes of bullying and mental health. This secondary objective was inspired by studies that have found that the health effects of bullying vary depending on if the aggression involved is direct or indirect (Baldry, 2004; Låftman et al., 2013), electronic (Låftman et al., 2013), or if multiple subtypes of victimization are experienced simultaneously (Waasdorp & Bradshaw, 2015; Wang et al., 2010). Thus, we hypothesized that such relationships may also vary between subgroups defined by their self-reported level of spiritual health. Finally, variations in the direction and strength of these relationships between age and gender groups were also investigated. Our hope was to provide foundational information in support of preventive interventions, clinically, educationally, and at the population level.
Methods
Data Source
Data were obtained from the 2017/18 (cycle 8) Canadian Health Behaviour in School-aged Children study (HBSC) (Freeman et al., 2016). HBSC is a cross-sectional survey conducted every four years in collaboration with the World Health Organization (Inchley et al., 2016). Participating HBSC countries follow an international protocol to ensure that data collection is consistent and quality controlled (Inchley et al., 2016). The Canadian HBSC involves an anonymous and self-completed school-based survey that is representative of the experiences of preadolescent and adolescent children in grades 6 to 10 (approximate ages 11 to 15 years; Freeman et al., 2016). Canadian students in grades 9 and 10 complete an extended questionnaire that is consistent with their experiences and literacy levels. Consent (active or passive depending on the practices within individual school boards) was obtained from the participating pupils, their parents/guardians, and participating schools.
Ethics. The Canadian HBSC survey has been granted ethics approval from the General Research Ethics Board at Queen’s University, as well as the Health Canada and Public Health Agency of Canada Research Ethics Board. This analysis was also approved by the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (HSREB).
Sample
Within each Canadian province (n = 10) and territory (n = 2; Nunavut did not participate), a list of eligible school jurisdictions was created and organized by school language, type of school board, and the population sizes of the school and its surrounding community (Freeman et al., 2016). Students excluded due to the Canadian sampling protocol (approximately 8% of the population (MacLeod & Hasan, 2017)) were those in private schools, home schools, schools on First Nation reserves, and youth who were incarcerated. A multistage cluster sample (individuals nested within classes, schools, and then school boards) was then drawn for participant accrual (Freeman et al., 2016). All consenting students present on the date of the survey were included, and the achieved sample size was 21,745 students from 287 schools. The participation rate was 75% at the individual student level.
Further exclusion criteria were applied for this analysis (Figure 1): (a) young people who identified as “bully-victims” as they are known to be at particularly high risk of psychosocial consequences compared to those only involved in perpetration or victimization of bullying alone (Craig et al., 2009; Juvonen & Graham, 2014); (b) students with a nonbinary gender or who reported intellectual or physical disabilities as small cell sizes posed a potential risk of re-identification, a risk precluded by our existing ethics agreements.
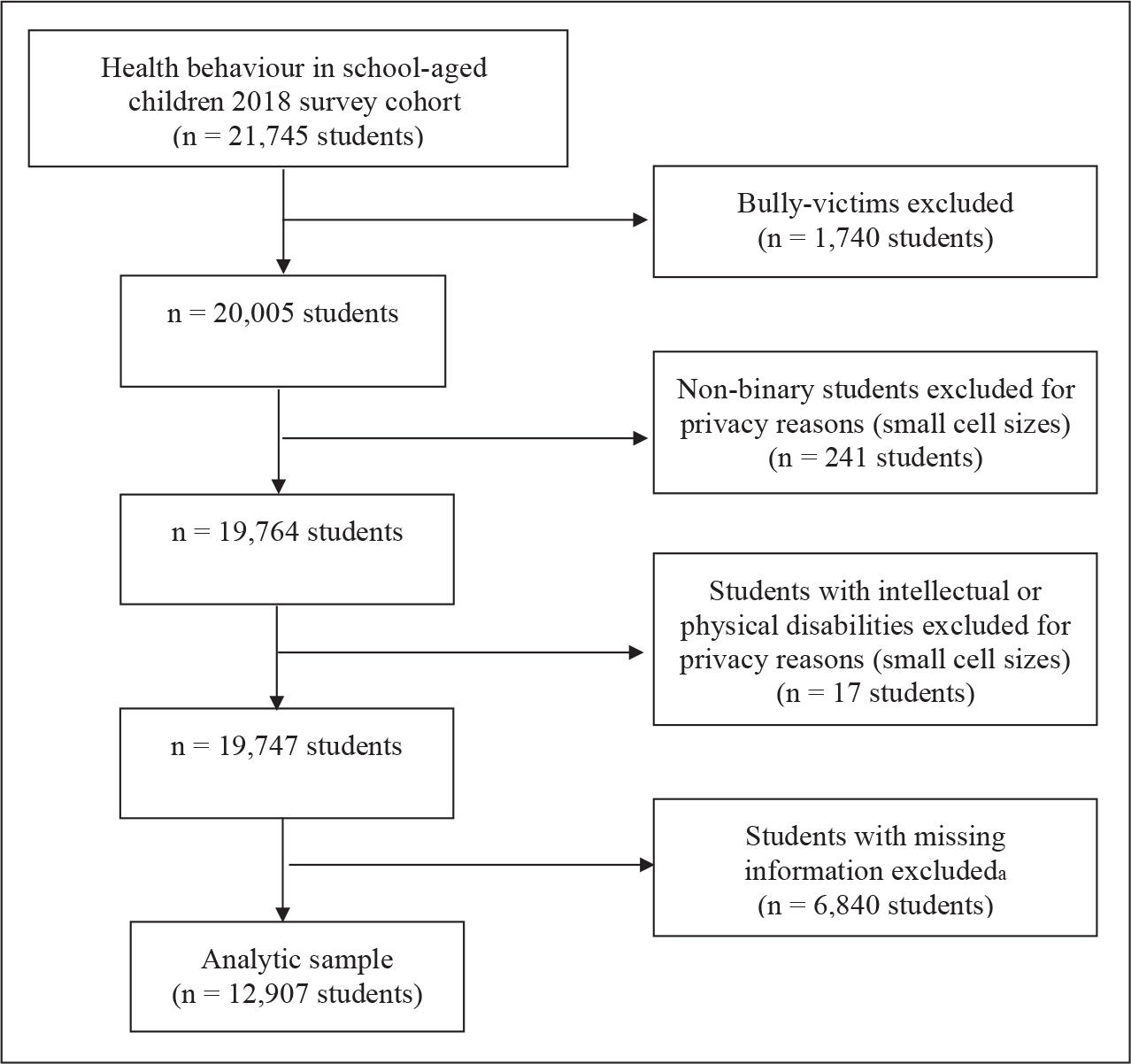
Note. All sample frequencies are weighted to ensure provincial and territorial representativeness by grade.
Measures
The primary relationship under study was the association between victimization by bullying and the reporting of frequent subjective health complaints related to internalizing mental health symptoms (Bohman et al., 2012; Campo, 2012). The four domains of spiritual health were examined as potential effect modifiers of this association. Based on precedent, we also examined student grade (as a proxy for age) and gender as possible effect modifiers (Gini & Pozzoli, 2013; Michaelson, Brooks, et al., 2016; Michaelson et al., 2019) while controlling for potential confounders.
Victimization by bullying. The frequency of victimization by any form of bullying at school in the past couple of months was reported by students. Responses were dichotomized as “bullied” (“2 or 3 times a month” or more often) or “not bullied.” The use of this cut point is supported theoretically as repeated incidents of targeted aggression are required according to the widely accepted Olweus definition of bullying (Solberg & Olweus, 2003). The two identified groups are known to differ on psychosocial adjustment variables (Solberg & Olweus, 2003). Subtypes of victimization, including direct (physical or verbal abuse), indirect (social exclusion, gossiping/spreading rumors), or cyber, were also identified according to the above cut point (Supplementary Table 1).
Epidemiological Description of Analytic Student Sample for Included Model Covariates, Stratified by Gender.
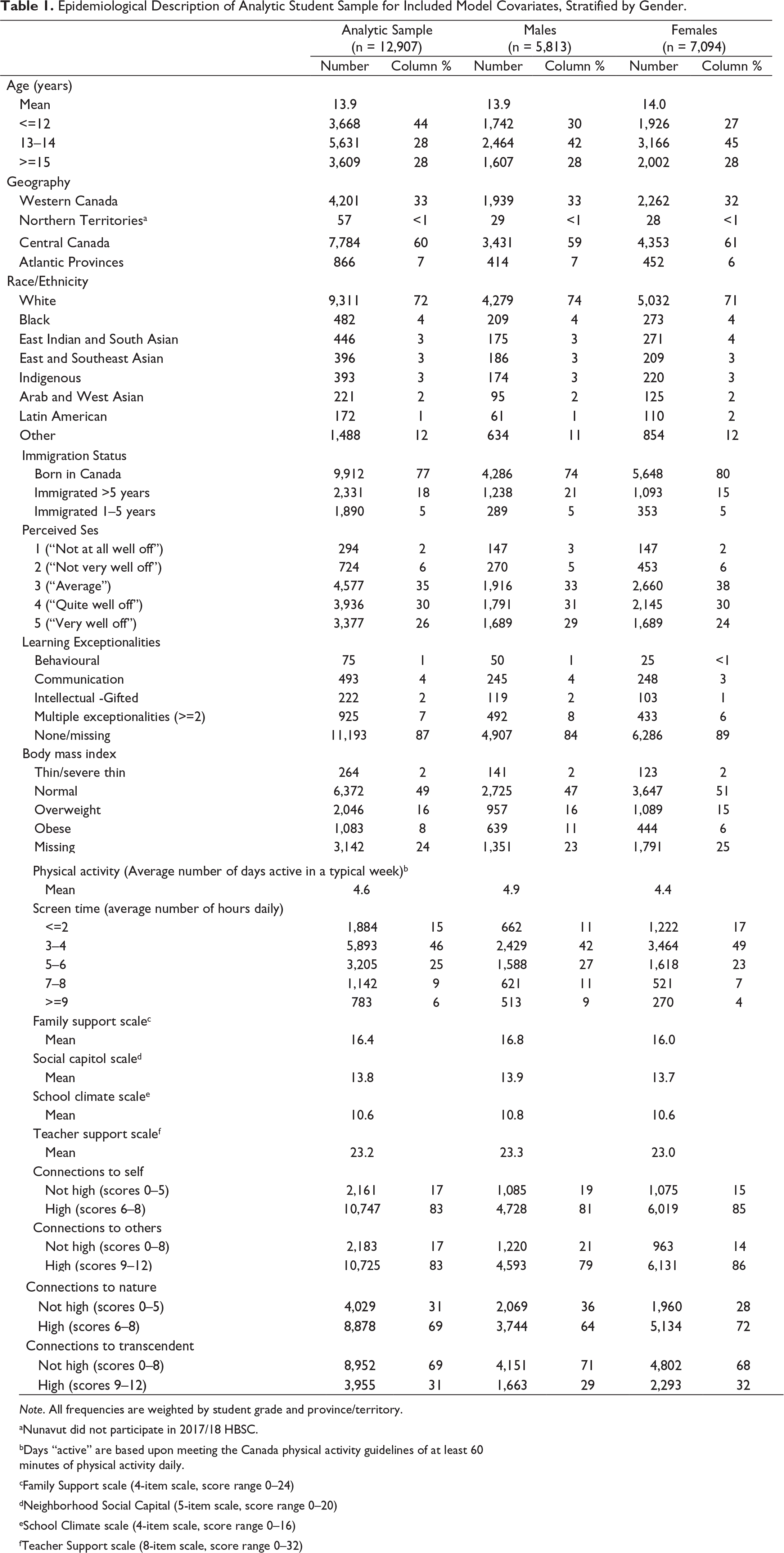
Note. All frequencies are weighted by student grade and province/territory.
aNunavut did not participate in 2017/18 HBSC.
bDays “active” are based upon meeting the Canada physical activity guidelines of at least 60 minutes of physical activity daily.
cFamily Support scale (4-item scale, score range 0–24)
dNeighborhood Social Capital (5-item scale, score range 0–20)
eSchool Climate scale (4-item scale, score range 0–16)
fTeacher Support scale (8-item scale, score range 0–32)
Subjective health complaints. Our primary outcome was poor mental health, which was measured using a subjective health complaints scale previously verified for construct validity and reliability (Freeman et al., 2016; Haugland & Wold, 2001). This scale included eight items describing the frequency (range 0—“rarely or never” to 4—“about every day”) of psychological symptoms (“feeling low [depressed],” “irritability or bad temper,” “feeling nervous,” “difficulties getting to sleep”) and somatic symptoms known to relate to psychological distress (“headache,” “stomachache,” “backache,” “feeling dizzy”). This scale represents a nonclinical measure of mental health and well-being with a long history of use in population health research (Currie et al., 2014). Responses were summed to produce a composite scale (range 0 to 32), with high scores representing the most frequent reports of symptoms. This scale has shown good internal consistency (α = 0.84) and test-retest reliability for the scale as a whole (r = 0.79), as well as for single psychological and somatic complaints (range r = 0.61 to r = 0.75 (Freeman et al., 2016; Haugland & Wold, 2001). Responses were categorized into tertiles (33.42% high, 33.23% medium, 33.34% low), with individuals in the highest tertile of scores designating a “high” number of health complaints. This allowed the comparison of students with many complaints with those who had relatively minor problems. This approach is consistent with past research (Freeman et al., 2016) and created roughly even groups, despite a heavily right-skewed distribution of scores.
Effect modifiers. Connections describing the four domains of spiritual health (self, others, nature, and the transcendent) were measured via the HBSC Spiritual Health Scale (Supplementary Table 2), a validated adaptation (Michaelson, Brooks, et al., 2016) of an existing instrument created for older adolescents and young adults (Gomez & Fisher, 2003). Students answered using a series of items describing the connections using a 5-point Likert-type scale ranging from 1 (“not at all important”) to 5 (“very important”). Consistent with confirmatory factor analyses that demonstrate that a four-domain model best represents spiritual health measures (Shaver et al., 2020), we created ordinal scores for each domain by summing corresponding domain items (score range 0–8 for self and nature, 0–12 for others and transcendent). We then transformed each domain into a binary variable consisting of “high” (cut point of scores >5 for self and nature, scores >9 for others and transcendent) versus “low” connections. Gender (male vs. female) and grade (6–8 vs. 9–10) as a social proxy for student age were also examined as potential effect modifiers, in both our primary associations of interest and with confounders.
Relative Risk (RR) Estimates for the Association Between Exposure to Bullying Victimization and High Subjective Health Complaints, Estimated by Strength of Spiritual Health (SH) Connections, Gender, and Grade.
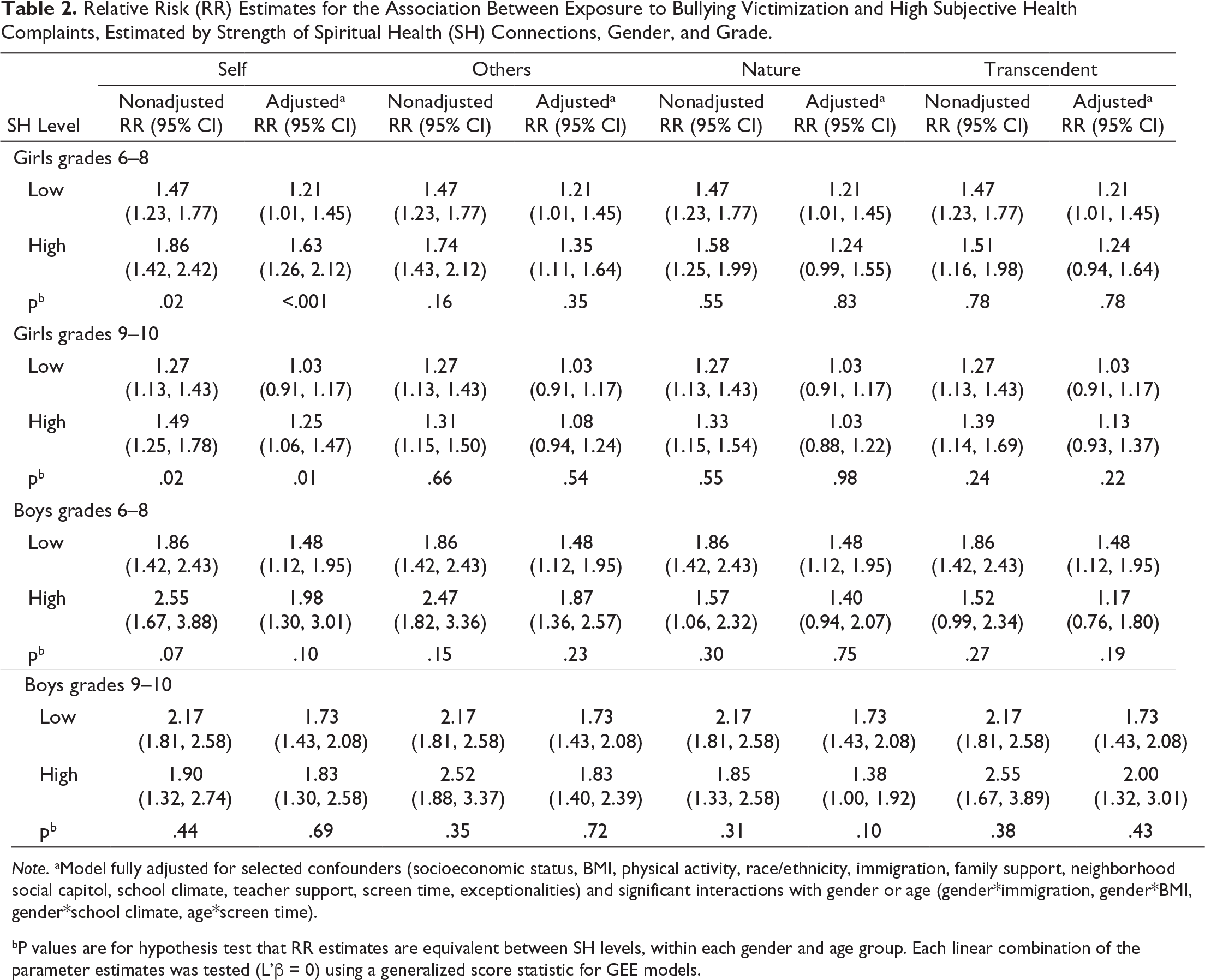
Note. aModel fully adjusted for selected confounders (socioeconomic status, BMI, physical activity, race/ethnicity, immigration, family support, neighborhood social capitol, school climate, teacher support, screen time, exceptionalities) and significant interactions with gender or age (gender*immigration, gender*BMI, gender*school climate, age*screen time).
bP values are for hypothesis test that RR estimates are equivalent between SH levels, within each gender and age group. Each linear combination of the parameter estimates was tested (L’β = 0) using a generalized score statistic for GEE models.
Confounders. Confounders were informed by past etiological literature based on (a) their association as likely causal risk factors for mental health outcomes, (b) their association with bullying victimization, and (c) not being on the causal pathway that links bullying victimization to mental health. These included perceived socioeconomic status (“how well off do you think your family is?”, with responses ranging from 0 [“very well off”] to 4 [“not at all well off”] (Currie et al., 2014; Karvonen & Rahkonen, 2011), sources of social support measured using previously developed HBSC scales, including Family Support (α = 0.91), Peer Support (α = 0.92), Neighborhood Social Capital (α = 0.78), School Climate (α =0.78) (Freeman et al., 2016), and Teacher Support (α = 0.82) (Currie et al., 2014), ethnicity (groups based on 2016 Canadian Census of Population) (Statistics Canada, 2017), body mass index (weight classes determined using WHO growth charts) (World Health Organization, 2007), immigration background (born in Canada, immigrated >5 years or immigrated 1–5 years ago), screen time (average number of daily hours) (Currie et al., 2014), physical inactivity (average number of days per week meeting recommended physical activity guidelines (Tremblay et al., 2011), and exceptionalities (based on Ontario Ministry of Education classification) (Ontario Ministry of Education, 2011). Information on the HBSC survey measurement of these items is available from the authors, upon request.
Minimal Detectable Differences
A simulation analysis was conducted using R software version 3.6.0 (R Core Team, 2019) to determine the smallest detectable multiplicative effect modification that any of the spiritual health domains could have on our associations of interest (relative risk ratio [RRR] = RR for high spiritual health/RR for low spiritual health), accounting for clustering (design effect of 1.2). A range of potential RRRs was examined for each age and gender grouping. One thousand data sets were generated for every potential RRR, with each simulated data set containing n subjects (n = the available sample size for the sociodemographic group). Each subject was randomly assigned a bullying exposure status (yes/no) and a spiritual health level (high/low). These assignments followed a Bernoulli distribution and were probability-weighted based on the exposure prevalence in a sociodemographic group (Freeman et al., 2016). The binary outcome for each subject was generated using a baseline risk of health complaints (Freeman et al., 2016), the RR of health complaints if the subject was exposed to bullying (Gini & Pozzoli, 2013), and the potential RRR if the subject was exposed and had high spiritual health. A Modified Poisson model analyzed the simulated data sets and the power for each RRR was calculated as the average number of datasets that rejected H0 at α = 0.05. Power curves plotted the available power for each RRR effect size. Based on our final unweighted analytic sample size (n = 12,593), the smallest RRR that could be identified for each spiritual health domain was a protective effect of 0.74 for younger boys, 0.70 for older boys, 0.52 for younger girls and 0.46 for older girls, at 80% power and α = 0.05.
Statistical Analysis
Analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC).
Descriptive objectives. The prevalence of key variables was examined, stratified by age group and gender. 95% confidence intervals that accounted for the nested and clustered nature of the sample were reported for each prevalence estimate. Estimated proportions were weighted using post-stratification weights to account for the disproportionate sampling of grades between provinces/territories and to ensure unbiased population estimates by grade (Bollen et al., 2016; West et al., 2016).
Analytical objectives. Generalized linear models were developed to estimate the strength of associations between bullying victimization and subjective health complaints, and to simultaneously determine if spiritual health domains act as effect modifiers in this relationship while controlling for other variables. Modified Poisson regression models with robust error variance estimation were used to generate prevalence proportion ratios as estimates of RR and their 95% confidence intervals. RR estimates for both adjusted models and unadjusted models were provided. Due to the clustered nature of our sampling, intraclass correlation coefficients (ICC) were produced from empty models to determine the variability of subjective health complaints at the school and classroom levels. Variations in this outcome were modest, that is, school ICC=0.045 and classroom ICC=0.006; we controlled for within-school correlation using a generalized estimating equation approach with an exchangeable correlation type. Survey weights were not employed in our analytical analysis, as our goal was to investigate exposure–outcome relationships rather than estimate population proportions.
A backwards elimination approach using a liberal p value (p = .20) was used to create a parsimonious model. The initial model included all potential confounders and their two-way interactions between gender and age. Wald (joint type 3) Chi-Squared tests were generated to examine the overall statistical significance of each parameter effect. Four 4-way interactions between our spiritual health domains, bullying victimization, gender and grade were forced into our models. RR estimates were generated for the effect of bullying victimization on high subjective health complaints between levels of spiritual health, and separately for boys and girls in different grades. Effect modification was evaluated by contrasting RR estimates between those with high vs. lower self-reported levels of connection within each domain for each sociodemographic group, with significance inferred by p < .05 and changes in the direction and strength of these relationships.
Results
Sample
Following the list-wise deletion of students with missing data, the sample was comprised of 12,593 students (12,907 weighted) from 286 schools across Canada (Table 1). We examined covariate distributions in the students that were excluded for missing data and found that excluded students were younger and had stronger connections to the transcendent domain. No other differences were observed between excluded and included students. Socioeconomic status, BMI, physical activity, race/ethnicity, immigration, screen time, learning exceptionalities and social support variables (excluding peer support) were all significantly (p < .05) related to the subjective health complaint outcome.
Prevalence of Victimization by Bullying
When asked about the frequency of any form of bullying victimization, approximately 21% [95% CI: 19%−23%] of students reported victimization. The proportion of bullied students was highest among younger students (26% girls, 20% boys), and decreased in older age groups (22% girls, 15% boys). Overall, more girls reported bullying victimization than boys (24% girls, 18% boys).
For subtypes of bullying victimization, 9% of students (11% girls, 7% boys) reported multiple forms of bullying victimization, followed by 5% (both genders) who only had exposure to direct forms of victimization, and 4% (5% girls, 3% boys) who experienced indirect forms alone. The reported prevalence of victimization by these subtypes was also higher in younger grades than older. Only 1% of all students were victimized by cyberbullying alone. We were unable to generate reliable associations for this exposure group due to this extremely low prevalence, and results for this exposure were suppressed.
Associations Between Bullying Victimization and Subjective Health Complaints, and the Modifying Effects of Spiritual Health Domains
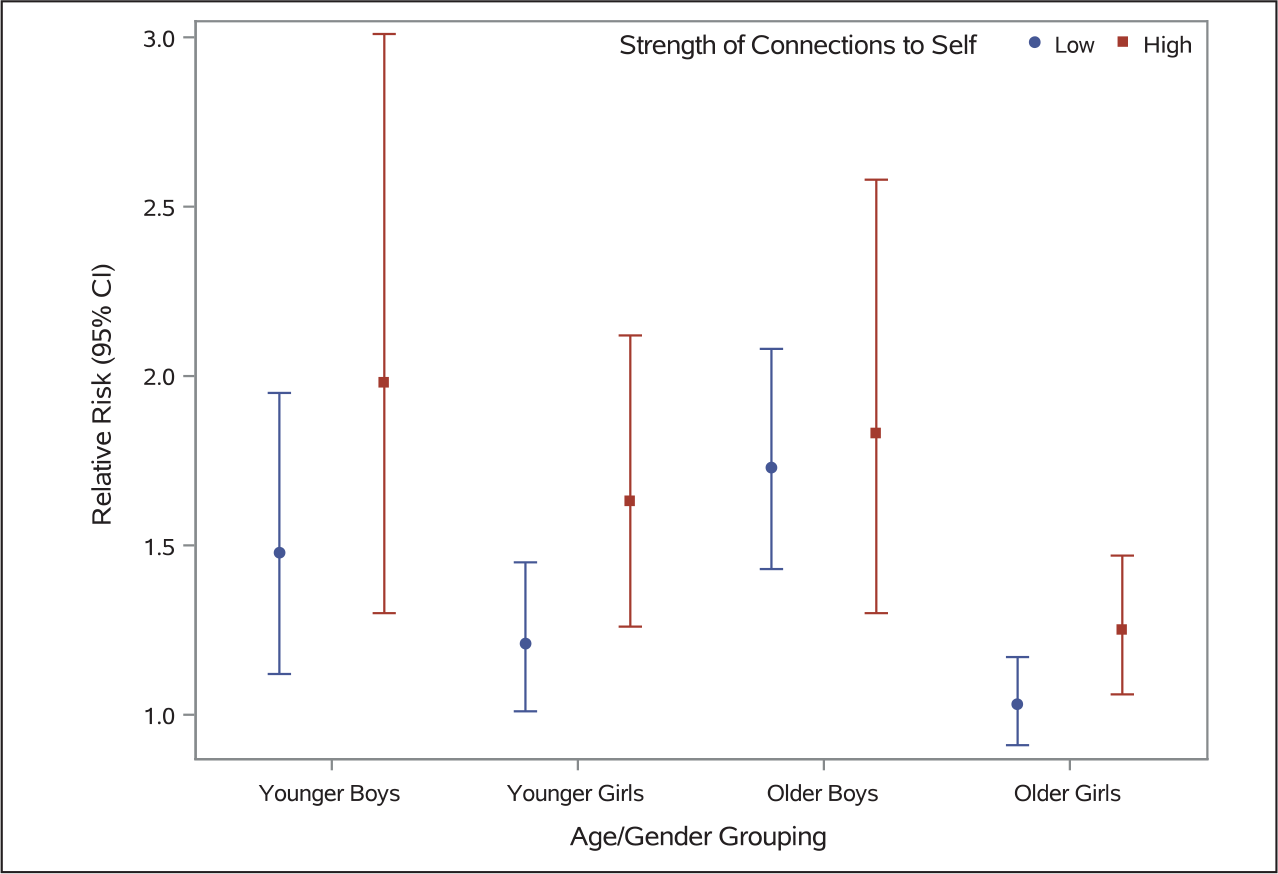
Among girls in all grades, we found a consistent modifying effect of connections to self on the association between bullying victimization and subjective health complaints in both adjusted and unadjusted models. The effect of bullying victimization on the risk of subjective health complaints appeared to be strongest for girls with high self-connections (younger girls RR = 1.63 [95% CI: 1.26–2.12]; older girls RR = 1.25 [95% CI: 1.06–1.47]; Table 2). This association was much weaker in strength for girls who did not have strong connections to self (younger girls RR = 1.21 [95% CI: 1.01–1.45]; older girls RR = 1.03 [95% CI: 0.91–1.17]; Figure 2).
No other clear patterns emerged among girls with respect to effect modification in terms of the other spiritual health domains.
Among boys, we failed to find effect modification by any spiritual health domain on the primary association of interest. However, the majority of RR point estimates were slightly stronger among boys with stronger spiritual health connections than those reporting weaker domain-specific spiritual health connections (Table 2).
Associations Between Subtypes of Bullying Victimization and Subjective Health Complaints, and the Modifying Effects of Spiritual Health Domains
We found evidence of effect modification by the “connections to self” domain in the association between exposure to multiple forms of victimization and subjective health complaints, among girls in all grades (Table 3). Consistent with the model measuring any form of victimization, associations were stronger among girls with strong connections to self (younger girls RR = 1.73 [95% CI: 1.33–2.26]; older girls RR = 1.48 [95% CI: 1.23–1.79], and weaker among those with weak connections (younger girls RR = 1.14 [95% CI: 0.95–1.38]; older girls RR = 1.11 [95% CI: 0.96–1.27]). The same direction of effect modification for self-connections was observed in the RR point estimates among boys, though this effect was not statistically significant.
Relative Risk (RR) Estimates for the Effect of Subtypes of Bullying Victimization on High Subjective Health Complaints, by Strength of Spiritual Health (SH) Connections, Gender, and Grade.
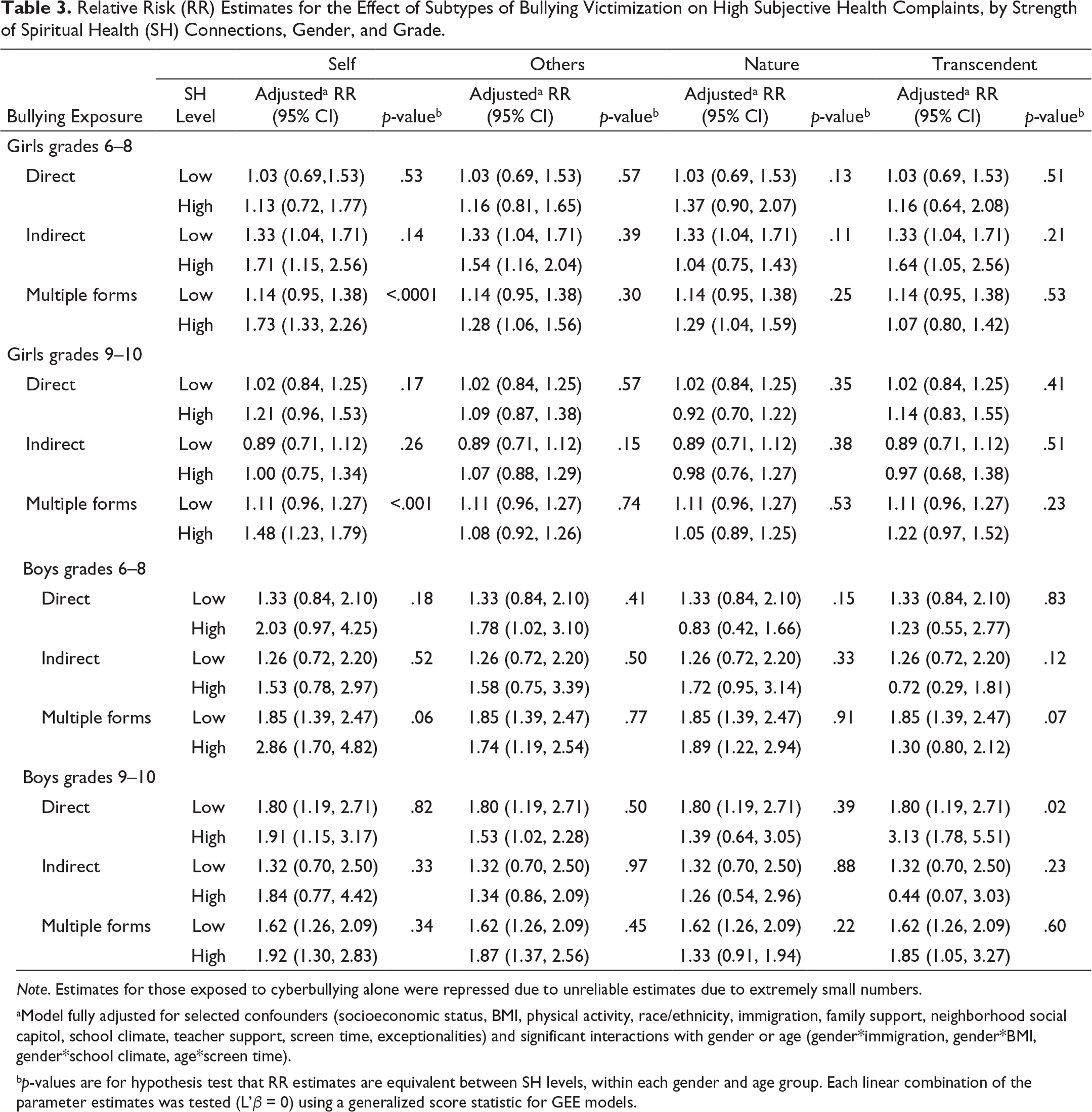
Note. Estimates for those exposed to cyberbullying alone were repressed due to unreliable estimates due to extremely small numbers.
aModel fully adjusted for selected confounders (socioeconomic status, BMI, physical activity, race/ethnicity, immigration, family support, neighborhood social capitol, school climate, teacher support, screen time, exceptionalities) and significant interactions with gender or age (gender*immigration, gender*BMI, gender*school climate, age*screen time).
bp-values are for hypothesis test that RR estimates are equivalent between SH levels, within each gender and age group. Each linear combination of the parameter estimates was tested (L’β = 0) using a generalized score statistic for GEE models.
The transcendent domain appeared to modify the association between exposure to direct bullying victimization and subjective health complaints in boys, but not in girls. Older boys with high connections to the transcendent had stronger associations between direct bullying victimization and subjective health complaints compared to boys with lower connections (strong connections RR = 3.13 [95% CI: 1.78 – 5.51]; weak connections RR = 1.80 [95% CI: 1.19 – 2.71], p = .02). We did not observe this effect modification among younger boys.
Discussion
In this study, we set out to determine if the connections afforded by strong spiritual health could modify or buffer some of the negative effects of bullying on the health and well-being of young people. The Canadian national data available to us included reports of being victimized by bullying, indicators of mental health status, and a simple scale that characterized connections inherent to spiritual health in four domains. Our primary finding was that relationships between being the victim of bullying and poor mental health status were evident in some population subgroups but were stronger among those who reported the highest levels of “connections to self.” Such relationships were weaker or nonexistent amongst those with lower perceived levels of self-connection.
Based on past theory this primary finding was unexpected. Past literature describing the importance of spiritual health in young people’s lives has shown that strong self-connections are linked to positive mental health status (Michaelson et al., 2019). Hence, a priori, we hypothesized that strong connections would act as substantial protective health assets in groups who are at particular risk of mental health consequences, such as bullied young people. Further, past psychological theory and associated empirical evidence support this view; psychological constructs that similarly emphasize meaning in life, such as a strong sense of coherence, are protective against psychosomatic complaints in bullied adolescents (García-Moya et al., 2014). Our findings, therefore, are provocative. Why might young people who report strong connections to self—indicative of experiencing joy or meaning in their inner world—be more vulnerable to the effects of bullying victimization?
One possible explanation for this unexpected finding is that some young people place particular importance on a high level of joy and happiness. Speculatively, such individuals may face a burdensome amount of stress when this state is disrupted by victimization. Philosophers and psychologists have long debated whether the pursuit of pleasurable experiences (hedonism) or the active pursuit of virtue and meaning (eudaimonism) leads to greater flourishing (Huta & Waterman, 2014). Consistent with a eudaimonic perspective, some research has recognized that psychological well-being is a multidimensional concept and has found that fostering the essential features of well-being is protective against the risk of disease (Ryff, 2014). Indeed, interventions that promote psychological well-being are protective against psychological distress in adolescents (Ruini et al., 2009; Shoshani & Steinmetz, 2014). However, some have also cautioned against the overpromotion of happiness as an explicit goal for children, and our data may bear this out in real-world experiences. Eaude contends that the promotion of resilience in children may enable a more long-term happiness or “flourishing,” rather than a focus on fostering immediate happiness or pleasure (Eaude, 2009). If children feel pressure to maintain happiness at all times, they could fail to learn how to process adversity; hence, they become more vulnerable to stress in the face of adversity (Eaude, 2009). Our findings are in keeping with such ideas.
The HBSC measure describing “connections to self” also focuses on the importance of meaning in life. Hence, it is also plausible that there are differential effects on mental health among young people whose meaning in life is especially affected by victimization. This hypothesis shares similarities with some cognitive models of trauma in the field of psychology. In her seminal Shattered Assumptions theory, Janoff-Bulman posits that victimization “shatters an individual’s assumption that the world is meaningful, controllable and benevolent.” Such broken assumptions lead to stress in victims. The ensuing mental health problems are the result of trauma challenging an individual’s fundamental conceptual systems (Janoff-Bulman & Frieze, 1983), that is, “[P]eople with more negative assumptions prior to victimization may not respond with as much psychological upheaval as a result of an extreme negative event” (Janoff-Bulman, 1989b, p. 166). As a consequence, adolescents who place strong importance on meaning and happiness are particularly affected by victimization, while those who do not possess these expectations are less distressed. While further research is needed to affirm the application of cognitive theories of trauma in this context and confirm our findings, our results may have implications for health promotion and intervention efforts (see Public Health Implications).
The existence of different findings by gender also warrants comment. Relationships between the importance of the “self” domain and mental health were stronger among girls than boys, suggestive of possible effect modification. Past analyses have shown that gender moderates the effect of self-connections on health, with girls reporting a stronger protective effect than boys (Brooks et al., 2018; Michaelson et al., 2019). Trauma theory supports the idea that gender plays a role in the effects of victimization on mental health (Janoff-Bulman, 1989a). Such patterns could relate to gendered socialization in the development of peer relationships. Early adolescence is a developmental period where such relations are of heightened importance (Noam, 1999). This is especially true for girls; relational-cultural theory posits that as girls develop, their sense of self is grounded in empathic connections with others (West, 2005). Rather than a separate sense of self, girls explore their identity in relation to others, and these relationships typically result in positive outcomes (West, 2005). When girls with a strong sense of self are victimized by their peers, it may create cognitive dissonance between their secure senses of self-worth and the positive, empathetic relationships that they pursue to develop identity. This may result in increased vulnerability in situations that involve bullying.
Beyond the overall findings, our bullying subtype analysis also yielded notable results. We observed a stronger association between being victimized by bullying directly and poorer self-perceptions of mental health among older boys who simultaneously reported strong connections to the transcendent. While the etiology of this finding remains uncertain, older boys with strong connections to the transcendent may have higher levels of “rejection sensitivity” (a disposition to overreact to social rejection), thus making them more sensitive to the potential negative effects of victimization (Downey et al., 1998). Religiosity has been associated with rejection sensitivity in cohorts of marginalized adults (Lassiter et al., 2017) and research shows that some children who feel rejected by their peers may turn to religion to cope (Aydin et al., 2010). Rejection sensitivity has also been shown to mediate the effect of bullying victimization on depressive symptoms (Nepon et al., 2021).
While intriguing, the current finding related to the transcendent domain is exploratory; more evidence is required to confirm why analogous effect modifications were not observed for the other subtypes of bullying. Additionally, because the transcendent domain describes connections “to something ultimate” that may be religious or fall outside the bounds of organized religion, it should be verified which of these aspects contributes to the observed effects of this domain.
Strengths and Limitations
Our article had several strengths. While unexpected, our findings contribute to an improved theoretical understanding of the value of spiritual health research in the public health domain and have practical implications for preventive interventions. Our research benefited from the use of theory-based modeling. Grounded in the theory of a four-domain model of spiritual health, we controlled for the individual effects of domains and examined each domain’s independent effect on mental well-being. Furthermore, our use of a large and robust national dataset allowed for a well-powered primary analysis and the estimation of effect modification by both gender and age. This enabled us to evaluate the consistency of the domain effects between demographic groups, as well as generate new etiological hypotheses.
Limitations of this study should also be noted. First, although student participation was high, there was a possibility of selection bias; school absenteeism is associated with both bullying victimization (Hutzell & Payne, 2012) and frequent health complaints among students (Havik et al., 2015). Additionally, due to sample restrictions, we were limited by our inability to include students who self-identify as a nonbinary gender due to privacy regulations for data presentation stipulated in our research ethics agreement. This is an obvious priority for future research. Another potential limitation is that we chose to use a moderation (i.e., “effect modification”) model in the study of spiritual health, based on our theoretical understanding of protective health assets. Future longitudinal research is required to investigate related mediation models to explore if bullying victimization could directly act on adolescent spiritual health. Our health complaints outcome also only captures one aspect of mental health and well-being. Frequent subjective health complaints may be a good indicator of internalizing problems but fail to capture other important dimensions of adolescent mental health, such as those characterized by externalizing behaviors. Another potential concern is that spiritual health is merely one component of mental health, rather than its own distinct factor, making any effect modification uninterpretable (Baron & Kenny, 1986). While the “connections to self” domain shares some similarities with mental health, prior research has contended that they are indeed discrete constructs with independent meaning and theoretical underpinnings (Michaelson, Brooks, et al., 2016; Michaelson et al., 2019). Finally, as with most cross-sectional designs, there is a lack of temporal data which limits our ability to draw causal inferences.
Public Health Implications
Practical implications of these findings warrant comment. We had initially hypothesized that spiritual health connections would particularly be beneficial to the mental health of students who experience bullying and theorized that our findings could inform secondary prevention strategies, in which interventions are targeted towards populations who are deemed “at-risk” (Kia-Keating et al., 2011). Such targeted school-based interventions may have involved strengthening spiritual health connections in bullied students to mitigate mental health consequences. However, our results suggest that those who are “highly self-connected” may face worse mental health outcomes when they are simultaneously victimized by bullying. Public health responses to these findings must be nuanced because it could be harmful to the well-being of students to explicitly discourage the fostering of resilience through connectedness in their lives. In light of these considerations, rather than attempting to minimize these connections to self in bullied youth, which could actually be detrimental, we propose that public health efforts may be better directed to preventing bullying perpetration in the general school population (a primary prevention approach) (Kia-Keating et al., 2011). Interventions that address the underlying issue of victimization might benefit the health and mental well-being of students with both higher and lower levels of connections to self. Many interventions for bullying exist with varying degrees of success. In a systematic review of reviews evaluating school-based interventions, the majority of high-quality studies found that multi-component interventions for violence yield the most consistently positive results (Shackleton et al., 2016). Thus, while high-quality RCT evidence is optimal to compare approaches, preventing victimization through a whole-school multi-component intervention may provide the greatest net benefit to student mental health.
Conclusion
To summarize, the present study finds that young people who report strong connections to self and who are simultaneously victimized by bullying, may face more severe mental health consequences. Although further research is required to expand our findings and confirm the causal links between spiritual health, violence, and mental health, there are implications for future health promotion and intervention efforts. While strong spiritual health connections are important to youth, a primary prevention method that addresses bullying perpetration in schools might provide the greatest contribution to the well-being of all students.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material for Do Spiritual Health Connections Protect Adolescents When They Are Bullied: A National Study of 12,593 Young Canadians by Nicole Shaver, Valerie Michaelson and William Pickett, in Journal of Interpersonal Violence
Footnotes
Acknowledgments
The HBSC study is conducted in Canada by the Social Program Evaluation Group at Queen’s University. We thank Dr Jo Inchley, international coordinator of the HBSC (University of Glasgow, Scotland) and Dr Oddrun Samdal international data coordinator (University of Bergen Norway). The Canadian principal investigators of the 2018 HBSC were Dr Wendy Craig and Dr William Pickett, of Queen’s University. The national coordinator was Matthew King.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Cycle 8 of the Health Behaviour in School-aged Children Survey in Canada was supported by a research contract from the Public Health Agency of Canada (6D016-123071/001/SS). This research was supported by the Canadian Institutes of Health Research through an operating grant to Drs. Pickett and Michaelson (MOP341188) and a Frederick Banting Masters Award (CGSM-CIHR) to Nicole Shaver. Ms. Shaver was also supported by the Ontario Graduate Scholarship program. Partial funding for this analysis was also provided via a contract from the Public Health Agency of Canada (contract 4500397002) which provided studentship funding to Ms. Shaver.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.