
Abstract
Despite an increase in research initiatives and prevention campaigns, intimate partner violence (IPV) remains a public health problem that affects many victims worldwide. The current study aims to examine whether psychological distress symptoms (anger, depression, and anxiety) are indirectly related to the perpetration of IPV (physical assault, psychological abuse, and coercive control) through affect dysregulation (AD) in men seeking help. Online questionnaires assessing psychological distress symptoms, AD, and violent behaviors were completed by 335 adult men entering treatment for IPV. A path analysis model revealed the indirect associations between psychological distress symptoms and higher IPV perpetration through higher AD. Symptoms of anger were indirectly related to the three forms of perpetrated IPV through higher AD. Symptoms of depression were, directly and indirectly, related to the three forms of perpetrated IPV through higher AD. Finally, symptoms of anxiety were directly related to lower physical assault perpetration, and indirectly related to higher physical assault and coercive control perpetration through higher AD. The final model explained 10% of the variance in perpetrated physical assault, 23% of the variance in perpetrated psychological abuse, and 13% of the variance in perpetrated coercive control. These results underline the necessity of assessing and addressing symptoms of psychological distress and AD among men perpetrators in the treatment of IPV.
Intimate partner violence (IPV) is the most common form of violence experienced by women (30%) within many socioeconomic and cultural groups across the world (World Health Organization [WHO], 2019). Recent literature also shows that gay men (43%), lesbian women (19%), bisexual people (10%), transgender people (10%), and queer people (9%) experience high rates of IPV (National Coalition of Anti-Violence Programs, 2016). This high occurrence is especially troublesome in view of its deleterious consequences, including psychological and physical distress among victims (Spencer et al., 2019), suffering in the families of the victims, and substantial costs for society (Peterson et al., 2018). These negative outcomes highlight the relevance of addressing the risk factors of IPV perpetration to understand its underlying mechanisms. One well-documented clinical risk factor of physical assault and psychological abuse perpetration is affect dysregulation (AD; Shorey et al., 2011). Yet, little is empirically known about AD reported by men seeking help for IPV perpetration since most studies have examined AD and IPV perpetration using community or criminal samples (Tager et al., 2010). Indeed, studies using samples of men seeking help for IPV are scarce and focus more on alcohol abuse than IPV perpetration treatment (Watkins et al., 2016). In addition, men who seek help for IPV-related difficulties are recognized to experience high psychological distress (Di Piazza et al., 2017), a known correlate of AD (Bradley et al., 2011; Velotti et al., 2017) and IPV perpetration (Oram et al., 2014). Yet, psychological distress in men with IPV-related difficulties is rarely considered in etiological models and is seldom acknowledged in awareness, prevention, and intervention programs (Bell & Naugle, 2008; Crane & Easton, 2017). For this reason, the development and empirical examination of etiological models of IPV perpetration that account for psychological distress and AD are needed.
Intimate Partner Violence
IPV refers to a pattern of behaviors perpetrated within a current or former romantic relationship and causing harm and suffering to an intimate partner (WHO, 2019). One of the most studied forms of IPV is physical assault (Romans et al., 2007), which is defined as physical acts of violence (e.g., hitting or grabbing) to harm the partner (Breiding et al., 2015). In a sample of men seeking treatment for IPV, 15% reported having perpetrated at least one act of physical assault in the last month (Strandmoen et al., 2016). Psychological abuse, the use of verbal (e.g., insulting and humiliating) and non-verbal (e.g., sulking) behaviors to harm the partner (Breiding et al., 2015), is even more frequent than physical assault among men seeking treatment for IPV (Chamberland et al., 2007), with a prevalence rate of 59% in the past month (Strandmoen et al., 2016). Coercive control draws parallels with psychological abuse, as it involves verbal and non-verbal behaviors such as intimidation, threats, and monitoring and/or limiting a partner’s whereabouts, finances, or communication with friends and family (Breiding et al., 2015; Kelly & Johnson, 2008). In a sample of men perpetrating IPV, 76% of them reported perpetrating a high level of coercive control (Johnson et al., 2014). Many authors have studied coercive control as part of psychological abuse, and not as a form of IPV on its own (Crossman & Hardesty, 2018). Yet, as put forward by Stark (2007), this form of IPV would differ from psychological abuse and physical assault, because of its underlying motive that is grounded in the need to control and entrap the partner.
In treatment efforts aimed at helping men reduce their use of IPV, distinctions based on the forms of IPV perpetrated are seldom included (Cunha & Gonçalves, 2013). Since men seeking help are often psychologically distressed and unable to regulate their emotions when entering treatment (Romero-Martínez et al., 2013), working on increasing affect regulation abilities is often put forward as an important part of treatment (Lee & DiGiuseppe, 2018; Palmstierna et al., 2012). However, to our knowledge, there is no empirical support regarding the joint roles of AD and psychological distress in explaining the use of varying IPV forms among men seeking help.
Psychological Distress
Psychological distress refers to the presence of symptoms associated with anger (i.e., feeling easily annoyed or irritated), depression (i.e., feeling lonely, bored, or hopeless), and anxiety (i.e., feeling nervous, tense, or fearful; Ilfeld, 1976). According to Di Piazza et al. (2017), 70% of men in IPV treatment report depression symptoms. In their systematic review, Spencer et al. (2019) found that depression and anxiety symptoms in men are related to increased use of physical assault. Anger and depression symptoms have also been associated with higher coercive control (Dahl et al., 2015; Diaz-Aguado & Martinez, 2015; Kelly & Johnson, 2008) as well as higher physical assault and psychological abuse perpetration (Redondo et al., 2019; Shorey et al., 2012). The associations between symptoms of anxiety and specific forms of IPV perpetration are, however, disputed. Ngo et al. (2018) have found a significant link between anxiety and higher physical assault perpetration, whereas Shorey et al. (2012) have not found significant associations between anxiety and physical assault or psychological abuse. In addition, no studies, to our knowledge, have examined the association between coercive control and anxiety.
Currently, it is thus unclear whether psychological distress alone can fully explain why men with depressive, anxious, or anger-related symptoms use more IPV. As such, perhaps the higher use of IPV in men who report psychological distress can be explained by a mechanism that is associated with both psychological distress and IPV perpetration, and that could be targeted in prevention and intervention programs. AD could represent such a mechanism.
Affect Dysregulation As an Underlying Mechanism
AD refers to the inability to manage and tolerate negative affects (Briere, 2000), which are externalized through inadequate and impulsive displays of anger and IPV perpetration (Briere & Runtz, 2002; Shorey et al., 2015). In the clinical and scientific literature, AD is recognized as an important risk factor for IPV perpetration, whether in men attending alcohol abuse (Watkins et al., 2016) or IPV perpetration treatment programs (Grigorian et al., 2020), or undergraduate male students (Shorey et al., 2015). Consequently, AD is a central aspect in the treatment of IPV (Lee & DiGiuseppe, 2018; Palmstierna et al., 2012). Individuals with affect regulation difficulties are indeed more likely to use harmful behaviors towards others as a result of a more intense experience of negative affect and the absence of effective regulation skills (Langer & Lawrence, 2010). Consistently, men in batterer intervention programs often explain their use of violence as being the result of their inability to regulate their negative emotions (Elmquist et al., 2014).
Yet, in recent years, clinicians and researchers have suggested that AD might not only act as a risk factor for IPV but also as an intermediate mechanism that can explain how other risk factors (e.g., the adherence to gender norms; Berke et al., 2019; childhood interpersonal trauma; Dugal et al., 2018) are related to IPV perpetration. As such, when a risk factor for IPV is also related to AD, its association with IPV perpetration may be partly explained by difficulties in affect regulation. Therefore, IPV treatments often target affect regulation skills as they can help reduce the risk of violence (Maldonado et al., 2015), even in the presence of other risk factors (Iverson et al., 2014). As such, those with higher psychological distress may be more likely to use violence as a way to diminish the negative affective experiences they are otherwise unable to regulate (Langer & Lawrence, 2010). However, to date, the intermediary role of AD in the associations between psychological distress symptoms and IPV perpetration has not been investigated.
The Current Study
This study investigated whether psychological distress symptoms (anger, depression, and anxiety) are directly and indirectly related to the perpetration of IPV (i.e., physical, psychological, and coercive control) through AD in men seeking help for IPV. In line with past literature, we expected that (H1) symptoms of anger would be directly and positively related to coercive control (Dahl et al., 2015), physical assault, and psychological abuse (Redondo et al., 2019), and that (H2) symptoms of depression would be directly and positively related to coercive control (Diaz-Aguado & Martinez, 2015; Kelly & Johnson, 2008), physical assault, and psychological abuse (Shorey et al., 2012). We also expected that (H3) symptoms of anger and depression would be indirectly associated with IPV perpetration through higher AD. Because of mixed results, no a priori hypotheses were put forward for the association between symptoms of anxiety and perpetrated IPV.
Method
Participants
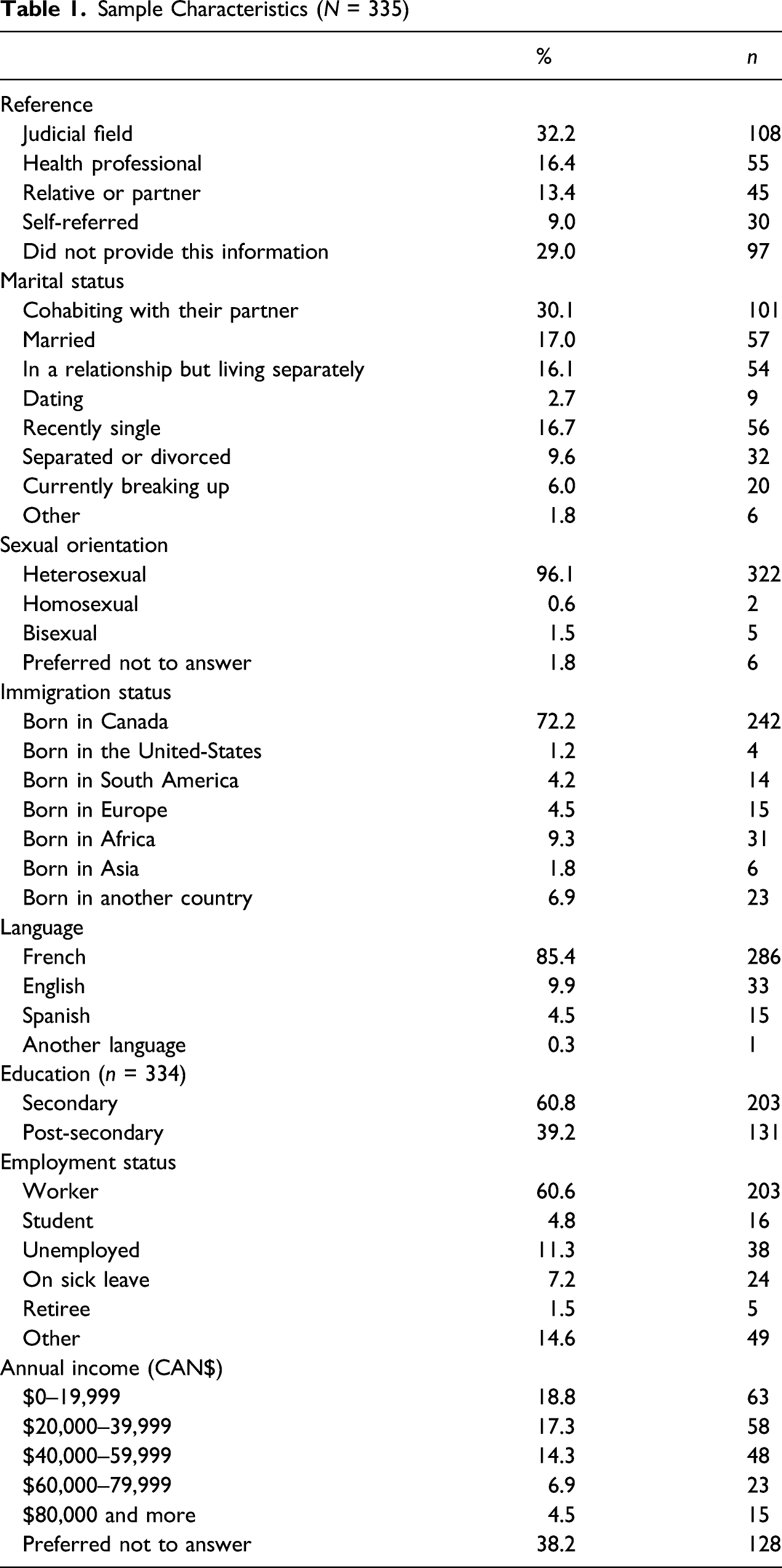
Sample Characteristics (N = 335)
Procedure
The current study is part of a larger ongoing research project involving nine community organizations offering group and/or individual treatment for men seeking help for IPV. Participants were recruited from these community organizations from the province of Quebec, Canada. Before entering treatment, men were asked to answer a series of online questionnaires (30–40 minutes) on the secure web platform Qualtrics, as part of the organizations’ standard assessment protocol. Although answering the questionnaires was mandatory, participants were free to consent to the use of their data for research purposes. Of a total of 410 participants who completed the questionnaires, 366 participants (participation rate: 89.3%) agreed to take part in the study. However, 31 participants were not retained in the final sample of 335 men, as they were not involved with a partner during the previous year and thus could not report their IPV perpetration. The ethics committee of the researchers’ institution approved the study procedures.
IPV treatment programs in Canada are regulated and offered by justice ministries, departments of health or social services, or by private agencies funded by the government (Department of Justice, 2017). Unlike the American justice system, the Criminal Code of the Canadian justice system does not include specific IPV offenses even though most acts of IPV are crimes in Canada (e.g., assault, uttering threats, and mischief). Thus, if a person pleads or is found guilty, the sentences can be a fine, probation, a jail sentence, or counseling depending on the nature of the offense and the aggravating or mitigating circumstances regarding the offender (Department of Justice, 2019).
Measures
Measures were chosen based on their satisfactory psychometric qualities, brevity, their availability in French, English, and Spanish, and the presence of a clinical cutoff. Participants were asked about their age, biological sex, gender identity, sexual orientation, relationship and work status, and judicial process.
Physical Assault and Psychological Abuse.
The short form of the revised Conflict Tactics Scales (CTS2-S; Straus & Douglas, 2004) was used to assess the participant’s perpetration of physical assault and psychological abuse in the past 12 months. Physical assault was assessed by the CTS2-S physical assault subscale (2 items, e.g., I pushed or shoved my partner) and psychological abuse by the CTS2-S psychological abuse subscale (2 items, e.g., I insulted or swore at my partner). Each item was rated by the participants on a scale from 0 (this never happened) to 6 (more than 20 times in the past year). As directed by Straus and Douglas (2004), scores were transformed into midpoints of the range mentioned (e.g., “3 to 5 times in the past year” was coded 4) and summed to create the participant’s scores for psychological abuse and physical assault. Higher scores on each subscale represent a greater annual frequency of physical assault and psychological abuse perpetration. The physical assault (α = .72) and psychological abuse (α = .77) subscales have demonstrated adequate internal reliability (Straus & Douglas, 2004). The validity of the CTS2-S is supported by correlations with the Revised Conflict Tactics Scales (CTS2).
Coercive Control.
Four items from the Coercive Control Scale (CCS; Johnson et al., 2014) were used to assess the participant’s perpetration of coercive control in the past 12 months (e.g., I tried to limit my partner’s contact with family and friends). Items were rated on a scale ranging from 0 (this never happened) to 6 (more than 20 times in the past year). Given that the authors of the Coercive Control Scale did not propose a specific guideline to assess the frequency of coercive control, the CTS2-S scales and midpoints were used to create the participant’s score, which also increases the interpretability of the data. Scores to each item were transformed into midpoints indicating the average frequency of each behavior, (e.g., “3 to 5 times in the past year” was coded 4) and were summed. Higher scores indicate a greater annual frequency of coercive control perpetration. The CCS has demonstrated adequate reliability among ex-husbands (α = .91) and current husbands (α = .75; Johnson et al., 2014). According to Johnson and colleagues (2014), many of the CCS items are similar to the items included in the Psychological Maltreatment of Women Survey (PMWS; Tolman, 1989), which validity was supported by correlations with other measures (Tolman, 1999).
Psychological Distress.
Descriptive Analysis, Cronbach’s Alpha Coefficients, and Pearson Correlations.
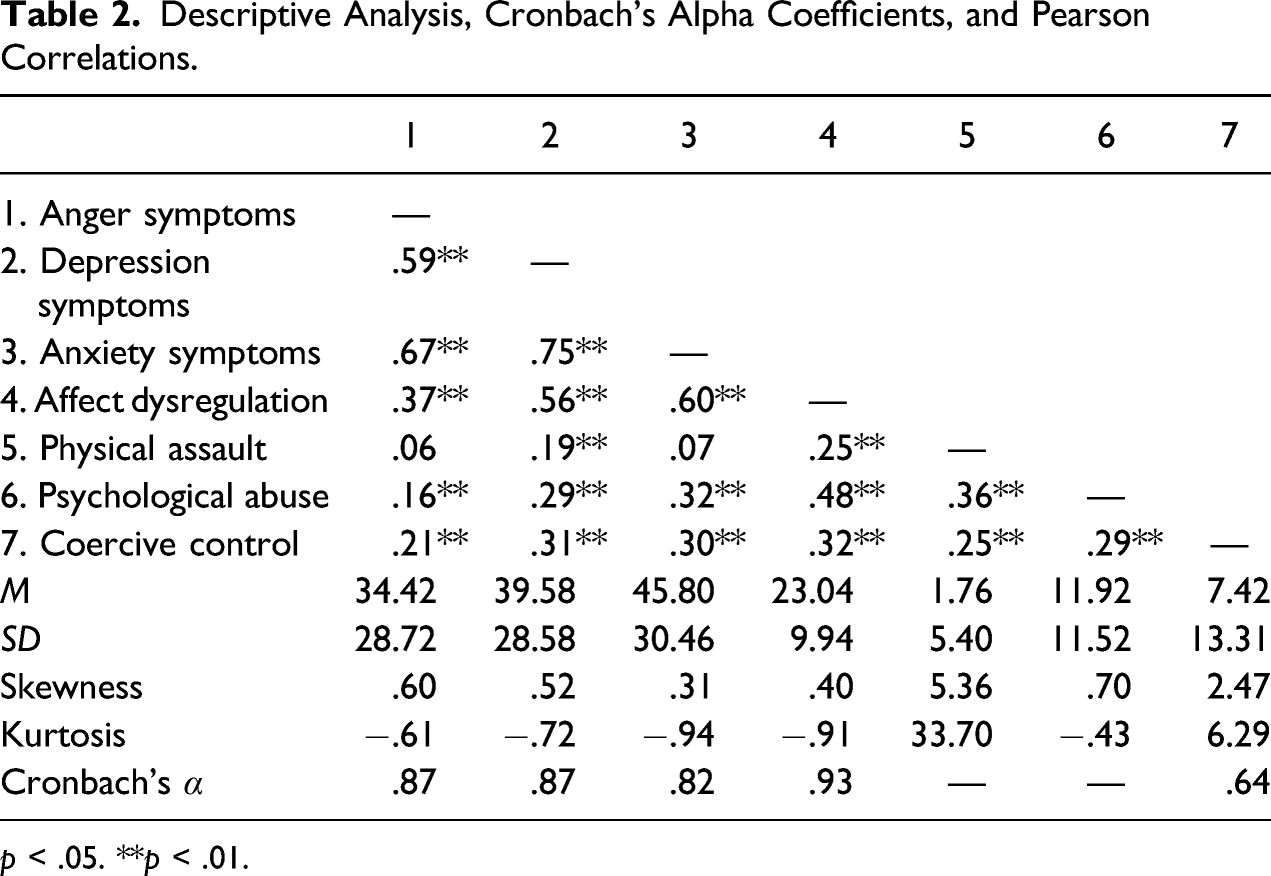
p < .05. **p < .01.
Affect Dysregulation.
The Inventory of Altered Self Capacities (IASC, Briere, 2000) was used to assess AD. The affect dysregulation subscale includes nine items (i.e., not being able to calm yourself down) assessing affect instability (i.e., mood swings and anger inhibition issues) and affect skills deficits (i.e., inability to regulate or tolerate distress). Participants indicated to what extent they agree with each item over the last 6 months, using a 5-point Likert-type scale ranging from 1 (never) to 5 (very often). Items were summed to obtain an overall score ranging from 9 to 45, in which higher scores reflect higher AD. Cronbach’s alpha coefficient for the affect dysregulation subscale (see Table 2) was similar to the original scale (α = .89). IASC scales correlated with other measures, which support their validity (Briere & Runtz, 2002).
Results
Preliminary Analyses
Descriptive analyses, Cronbach’s alpha coefficients, and Pearson correlations between the main variables are presented in Table 2. There were no missing values on the main variables. In the sample, 61.5% (n = 206) of the participants perpetrated at least one act of coercive control, 37.3% (n = 125) perpetrated at least one act of physical assault, and 81.8% (n = 274) perpetrated at least one act of psychological abuse in their intimate relationship in the last year. Moreover, most participants reported clinically significant symptoms of anger (51.6%, n = 173), depression (57.9%, n = 194), and anxiety (69%, n = 231). We found significant positive correlations between most study variables, except for the links between physical assault and anger and anxiety symptoms. Highly skewed distributions were found for physical assault and coercive control (as seen in Table 2), whereas the distribution for all other variables did not depart from normality. To address non-normality, a robust estimator was used in the main analysis.
Main Analysis
To investigate the direct and indirect associations between psychological distress symptoms (i.e., anger, depression, and anxiety) and IPV perpetration (i.e., physical, psychological, and coercive control) through AD, we conducted a path analysis model. This model (see Figure 1) was tested with the software Mplus 8.3 using the robust maximum likelihood estimator. Overall model fit was evaluated by examining the comparative fit index (CFI), the root means square error of approximation (RMSEA), and the chi-square statistic. A combination of a non-statistically significant chi-square value, a CFI value of .95 or higher, and a RMSEA value below .06 is thought to represent a good fit (Kline, 2011). To examine the significance of indirect paths, 95% confidence intervals (CI) were computed using 10,000 bootstrapping samples. Since we were interested in examining the indirect associations between psychological distress and IPV perpetration through AD (Hayes, 2009), and since the direct links between psychological distress and IPV perpetration had already been tested in previous research (Spencer et al., 2019), the direct and indirect associations between the study variables were all included in the model. Yet, to assess the model’s fit to the data, a non-saturated model must be tested. Because the link between depression symptoms and psychological abuse was the weakest of the observed associations ( Associations among psychological distress symptoms, affect dysregulation, and perpetrated intimate partner violence. Notes. Significant standardized path coefficients are shown. Dashed line represent marginally significant path. * p < .05. ** p < .01. *** p < .001.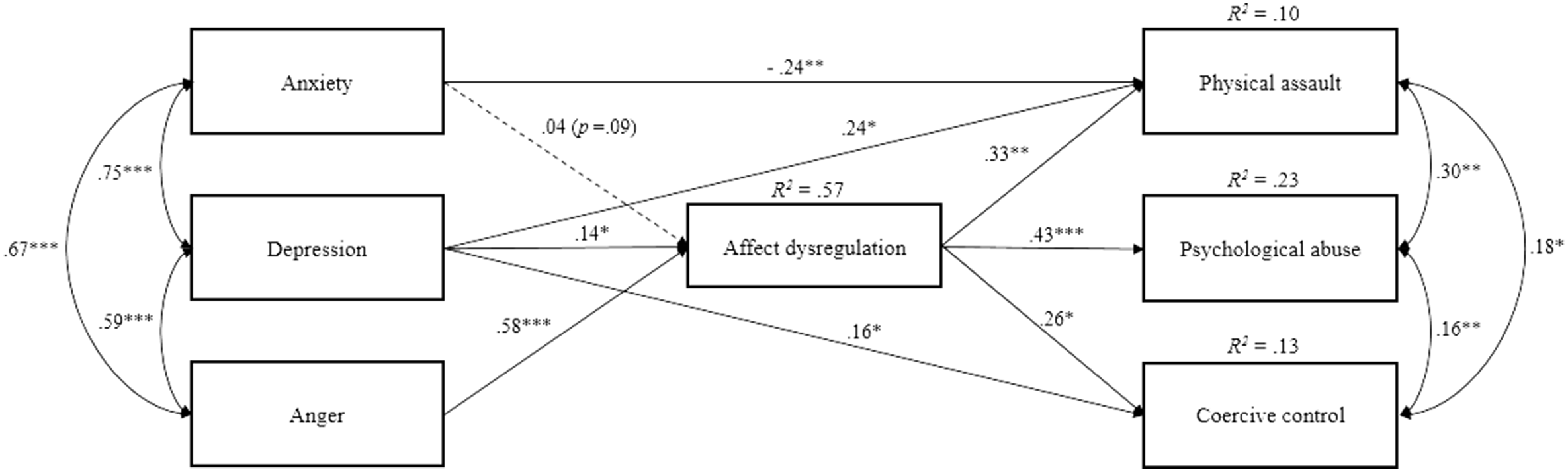
Indirect Effects of Psychological Distress Symptoms on Intimate Partner Violence via Affect Dysregulation.
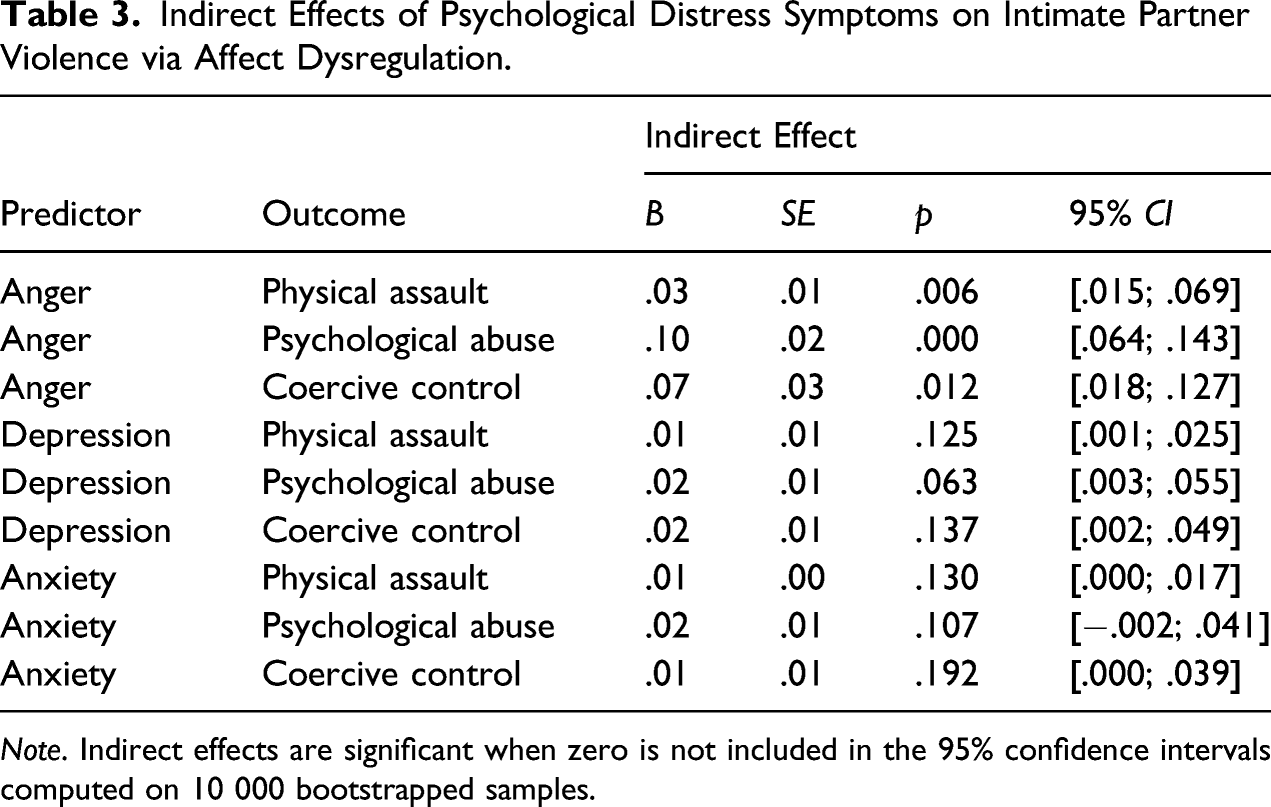
Note. Indirect effects are significant when zero is not included in the 95% confidence intervals computed on 10 000 bootstrapped samples.
Discussion
The purpose of this study was to explore the direct and indirect associations between psychological distress symptoms and IPV perpetration through AD among men seeking help for IPV. As expected, results revealed that psychological distress symptoms were directly and indirectly related to IPV perpetration through AD.
In line with our third hypothesis (but infirming H1), symptoms of anger are indirectly related to higher physical assault, psychological abuse, and coercive control through higher AD. When all variables are considered in a single model, anger is no longer directly linked to IPV; it is rather the indirect association through AD that explains the link between anger and IPV. That is, men with anger symptoms reported having greater difficulty regulating their affects, which contributed to their greater propensity to use IPV. These results corroborate and extend other studies showing that the intensity of anger is associated with AD (Velotti et al., 2017). Therefore, the more intensely these men experience anger, the less likely they are to regulate that anger, and the more they might use physical assault and psychological abuse as a dysfunctional communication channel to externalize their negative emotions (Garofalo et al., 2018; Velotti et al., 2017). Experts in the study of IPV have often argued that perpetrators of IPV can be distinguished according to the form of violence used and its underlying motivation. As such, they have suggested that some perpetrators might use psychological abuse or physical assault as a way to express unregulated anger, while others will use more coercive forms of aggression as a way to dominate or control their partner (Langhinrichsen-Rohling, 2010). Interestingly, our results suggest that anger and AD are similarly associated with coercive control and both physical assault and psychological abuse, which suggests that, perhaps, these forms of IPV might not be as different as we might expect them to be. Indeed, motivations for the use of these behaviors were not examined in this sample. Future studies are needed to better explore these associations.
The results partially supported our second and third hypotheses and suggest that symptoms of depression are directly and indirectly related to the use of physical assault, psychological abuse, and coercive control through higher AD. Indeed, although the associations between depressive symptoms and the three forms of IPV were partly explained by greater difficulties regulating negative affects, depressive symptoms also remained directly associated with physical assault and coercive control. These results indicate that negative mood, loneliness, or helplessness could contribute to men’s propensity to use physical assault and coercive control towards a romantic partner, beyond their association with AD. Previous studies have shown that men with depressive symptoms are more likely to report lower self-esteem, shame, and a negative image of themselves (Gaudet et al., 2016; Moritz & Roberts, 2018). As such, men with depressive symptoms and lower self-esteem might compensate their vulnerabilities and feelings of inadequacy by using externalizing behaviors (Imbach et al., 2013; Magovcevic & Addis, 2008), such as physical assault (Genuchi & Valdez, 2015), or they may try to control their partner to manage their vulnerabilities and regain power to fit traditional masculine roles of dominance by using coercive control (Diaz-Aguado & Martinez, 2015; Tager et al., 2010).
To a lesser extent, our results also suggest that symptoms of anxiety are indirectly associated with physical assault and coercive control through higher AD. That is, men with symptoms of anxiety seem to experience greater difficulty regulating their affects, which could contribute to the use of physical assault and coercive control in their romantic relationships. Perhaps, men who report being generally more nervous and agitated might experience couple’s conflicts as worrisome and distressing (Ilfeld, 1976; Ngo et al., 2018), which could hamper their capacity to regulate internal distress without exteriorizing it with physical assault or controlling behaviors. In response to internal distress, anxiousness, or physical agitation, some men might use coercive control in the attempt to regulate their distress by trying to control the situation or their partner (Bell & Naugle, 2008; Endler, 1997) or by exteriorizing their negative emotions using physical assault (Ngo et al., 2018). This association could also be explained by the fact that individuals with high anxiety are more likely to engage in indirect forms of aggression (Chung et al., 2019), such as passive aggression (i.e., hostile attitude, defiance, and passive resistance towards other’s demands; American Psychiatric Association, 2000). Individuals who use passive aggression often do so to make others do what they want (Hamel et al., 2015). As such, in a romantic relationship, these forms of indirect aggression could be associated with higher use of coercive control. Beyond these indirect links between anxiety and IPV through AD, a direct negative association between symptoms of anxiety and physical assault also emerged. It thus seems that, once one’s AD is accounted for, experiencing symptoms of anxiety is related to a lower use of physical assault in men. This result could be explained by the fact that physical assault is generally considered more socially undesirable than other forms of IPV (Arias & Beach, 1987), which are less noticeable and less emphasized in prevention and awareness campaigns. This result could also be explained by the specific nature of anxious symptoms which, unfortunately, were not assessed in the study. Indeed, perhaps men with a generalized anxiety disorder or social anxiety disorder are less likely to use physical assault compared, for instance, to men with anxious symptoms resulting from post-traumatic stress disorder (Spencer et al., 2019). Future research is needed to better understand these links.
Finally, the results showed that psychological distress and AD were differently related to the three forms of IPV perpetration assessed in this study. Based on the higher percentage of explained variance for psychological abuse, it seems that psychological distress and AD might explain a larger part of the occurrence of psychological abuse, compared to physical assault or coercive control. These findings suggest that some mechanisms behind the perpetration of physical assault and coercive control might be different, which is consistent with past literature on IPV perpetration. For instance, beliefs of male dominance, which were not examined in the current study, are more strongly associated with severe physical assault and coercive control compared to psychological abuse (Diaz-Aguado & Martinez, 2015; Whitaker, 2013). Moreover, when all the variables were measured in the same model, anger was more strongly related to the perpetration of IPV, which is consistent with past research (Redondo et al., 2019). As men who report depression or anxiety also tend to report more anger (Chung et al., 2019; Genuchi & Valdez, 2015), the variance in IPV perpetration that is uniquely explained by depression and anxiety symptoms is likely to be smaller.
Diversity
In the interest of respecting diversity, this study used inclusive measures to assess participants’ characteristics (i.e., gender identity, biological sex, sexual orientation, age, language, and country of birth). Although the study aims to consider the experiences of every man with IPV-related difficulties, the current sample represents primarily French-Canadian heterosexual males with lower education and income levels. Thus, this study seeks to add to the literature by providing greater insight on psychological distress in this specific diversity context. Future studies should aim to recruit a more diversified sample of participants.
Implications
The current study supports the relevance of focusing on the role of psychological distress symptoms and AD in the perpetration of IPV among men seeking help. The findings highlight the necessity of considering psychological distress symptoms in etiological models of IPV as men seeking help for IPV are often in psychological distress when entering treatment (Romero-Martínez et al., 2013). Developing prevention and intervention programs that acknowledge the psychological distress of men seeking help and that focus on their affect regulation abilities might help increase their awareness as well as understand and tolerate their negative emotions (Garofalo et al., 2020). As AD is one of IPV recidivism risk factors (Birkley & Eckhardt, 2015), it is essential to address affect regulation in IPV treatment, regardless of the treatment approach. Indeed, affect regulation abilities are often considered as an important part of IPV treatment (Lee & DiGiuseppe, 2018; Palmstierna et al., 2012). While targeting perpetrators’ affect regulation, the interventions also need to be adapted with the type of psychological distress symptoms experienced. Intervention should focus on improving anger management skills for perpetrators with anger, depression, and anxiety issues (Velotti et al., 2017). In addition, interventions aiming at enhancing men’s self-esteem and transforming their perceptions of masculine norms could be added for perpetrators with depression issues (Moritz & Roberts, 2018; Tager et al., 2010), and interventions aiming at increasing the abilities to accept and tolerate distress could be added for perpetrators with anxiety issues (Endler, 1997; Garofalo et al., 2018).
Limitations and Future Research
Finding should be considered in light of certain limitations. All questionnaires were self-reported measures, which can enhance social desirability biases, especially in the context of IPV, or recall difficulties among participants. Furthermore, the cross-sectional design of the study might limit the interpretation of the results. As such, it could also be that psychological distress symptoms are the result of poor affect regulation skills (Velotti et al., 2017) and thus contribute to the indirect association between AD and IPV perpetration. Adopting a longitudinal research design in future research could help further disentangling the links and direction in the proposed indirect associations. In addition, although psychological distress has been shown to remain generally stable across time (Welsh et al., 2020), the current study used an acute measure of psychological distress. This could potentially restrict the interpretation of its associations with AD and IPV, which were assessed on a longer time frame (e.g., in the past year). Also, the use of a subscale from the Altered Self-Capacities questionnaire could limit the result’s comparison to other studies as this measure is rarely used to assess AD in research on IPV. Finally, only men’s point of view has been considered in the study; therefore, it would be relevant to assess their partner’s point of view by recruiting both partners. Dyadic analyses could provide a more accurate understanding of the perpetration of violence in an intimate relationship and could help rescind some of the limitations of the use of self-report measures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a SSHRC Engage grant (# 892-2019-1049)