
Abstract
Childhood sexual abuse (CSA) and intimate partner violence (IPV) have both been associated with numerous negative repercussions. The first aim of this study is to understand IPV perpetrated by men within a clinical population, by examining the effects of two potential predictors: CSA and dyadic empathy (cognitive and emotional). The second aim of this study is to explore whether dyadic empathy is an intermediary variable of the association between CSA and IPV. A sample of 198 men (aged 18–69 years old) who were seeking help for relationship problems, completed a set of self-administered questionnaires. While controlling for social desirability and family violence history, our findings outlined the mediating and moderating role of dyadic empathy in the link between CSA and perpetrated psychological, but not physical, IPV. Emotional empathy mediated and moderated the link between CSA and psychological IPV, whereas cognitive empathy only moderated this link. The examination of the direct links between the variables also revealed that CSA was related to lower emotional empathy and higher rates of both types of IPV. In addition, cognitive empathy was negatively associated with physical and psychological IPV, whereas emotional empathy was positively associated with psychological IPV. This study contributes to the literature by documenting some of the mechanisms that could explain the perpetration of IPV and highlights the importance of investigating CSA and empathy in men who are seeking help.
According to the World Health Organisation (WHO, 2019), up to one billion of children aged 2–17 years have experienced physical, sexual, or emotional violence or neglect in the past year. These childhood interpersonal traumas (CIT) can be defined as any negative interpersonal event that could affect one’s capacity to adequately assume adult roles in intimate relationships (Godbout, Dutton, et al., 2009). Because it is thought to alter the cognitive, emotional, and social development of children, CIT has been associated with lower self-esteem during adulthood (Wekerle & Wolfe, 2003), the development of traumatic, depressive or anxious symptoms (Paolucci et al., 2001; Turner et al., 2017), sexual problems (Bigras et al., 2021), interpersonal difficulties, (McCloskey & Stuewig, 2001), as well as the use of harmful parental behaviors (Dixon et al., 2005) and non-suicidal self-injury (Caron et al., 2018) (for a review, see Dugal et al., 2016). According to Vine et al. (2006), there are four forms of CIT: (1) neglect, which is the most prevalent form in Canada (46%), where this study was conducted; (2) physical violence (25%); (3) psychological violence, including witnessing parental violence (19%); and (4) childhood sexual abuse (CSA; 10%). Childhood sexual abuse can be defined as the use of a child for sexual purposes (Trocmé & Wolfe, 2001). Authors have argued that, although it is less prevalent, the negative psychological consequences of CSA could be more detrimental than those of physical violence (Fergusson et al., 2008; Turner et al., 2017), particularly among men (Briere et al., 1988). Therefore, focusing on the long-term consequences of this particular type of CIT in men is an important endeavor.
Although the majority of researchers have focused on women’s experiences of CIT, the few that have focused on men have found that 22.2%–82% of adult men would have witnessed or experienced physical violence during childhood (e.g., Rosenbaum & O'Leary, 1981; Briere & Elliott, 2003), and that 5.3%–21.6% would have experienced sexual abuse (e.g., Brassard et al., 2014; Turner et al., 2017; Vaillancourt-Morel et al., 2016). These prevalence rates may represent only a minority of men who are willing to disclose their experiences of abuse. It is therefore critical to further investigate the long-term correlates of CIT victimization among men in an effort to improve the preventive and clinical resources designed for men (Whitfield et al., 2003).
According to recent meta-analyses (Godbout et al., 2019; Li et al., 2020), there is a significant—albeit small—association between CIT victimization and intimate partner violence (IPV) perpetrated by men. This may include physical violence, referring to any brutal, excessive, or irrational behavior injuring physical and psychological integrity, or psychological violence, referring to any verbal and nonverbal behavior injuring or threatening others (Straus, 1979). Although not all men who have experienced CIT later use violence in their intimate relationships (Godbout et al., 2019; Li et al., 2020), this association warrants further investigation because IPV is a major public health issue generating serious repercussions for the victims and very high society costs (e.g., Black, 2011; Coker et al., 2002; Zhang et al., 2012). A recent report from WHO (2021) indicates that about one third of women have been victims of IPV from a male partner in their life, underlining the importance of addressing men’s perpetration of IPV and its correlates, including their history of CIT.
More precisely, sexual abuse victimization among men appears to be a particularly relevant type of CIT associated with the perpetration of psychological (e.g., Brassard et al., 2014) and physical violence (e.g., Fang & Corso, 2008) in adulthood, as highlighted by recent meta-analyses (Godbout et al., 2019; Li et al., 2020). According to the Model of intergenerational transmission of violence (e.g., Widom & Wilson, 2015), family violence (i.e. physical abuse or any act or omission by parents or guardians that caused or could have caused serious behavioral, cognitive, emotional, or mental disturbances, including witnessing parental violence) is also related to the perpetration of IPV in adulthood (Godbout et al., 2019; Li et al., 2020), this association being stronger among men (Li et al., 2020). To date, however, not all studies have found associations between these types of CIT and IPV (see Lavoie et al., 2002, for an exception), which suggest that other factors are needed to comprehend the context that would lead to IPV. Moreover, only a few studies have included the concomitant presence of family violence and CSA to understand IPV perpetrated by men (Dugal et al., 2021; Turner et al., 2017). As CSA is likely to occur concurrently with other forms of family violence (Finkelhor et al., 2007), the failure to consider these two CIT together limits our understanding of the adverse context in which CSA occurs.
Recent studies (e.g., Li et al., 2020) have urged researchers to identify the factors that could explain why and which adult CSA male survivors are more likely to use IPV towards their partner in adulthood, a critical need for the advancement of current clinical conceptualizations and treatment strategies designed for men who engage in violent behaviors. Growing empirical support suggest that CIT, and CSA in particular, can impair the development of empathy, by limiting the ability to experience or to regulate emotions (Brassard et al., 2014; Godbout et al., 2014; Locher et al., 2014). Empathy is defined as the set of processes (emotional, cognitive, and behavioral) generated in observers as a result of their response to the experience of another person (Davis, 1983, 1996). There are two key components of empathy: (1) perspective taking, the cognitive capacity to perceive the point of view of the other; and (2) empathic concern, the emotional response to the emotional experience of the other (Péloquin & Lafontaine, 2010).
A disruption in empathy may play a key role in explaining why and which CSA male survivors may perpetrate IPV in adulthood. Davis (1996) suggested that secure relationships with parents would contribute to developing a higher level of empathy, whereas trauma in childhood would disrupt the development of empathy. Yet, an early study (Walker, 1996) found no significant difference in the degree of emotional empathy of children with a history of CSA, compared to a non-representative comparison group of children without such experience. Another study found that children with a history of physical abuse who witnessed another child crying reacted with less helpful behaviors and more withdrawal, anger, and aggression than non-abused children, suggesting lower empathic abilities (Klimes-Dougan & Kistner, 1990). Among children, having sustained physical violence was related to a lower level of emotional empathy (Straker & Jacobson, 1981), whereas having sustained psychological violence was related to a lower level of general empathy (Hinchey & Gavelek, 1982). Adult survivors of CIT also demonstrated impaired cognitive and emotional empathy when compared to control (Locher et al., 2014), while incarcerated men who have experienced physical violence during childhood showed lower levels of cognitive empathy towards women in abusive situations than those who have not experienced such trauma (Simons et al., 2002).
In romantic relationships, a lack of empathy towards one’s partner—dyadic empathy—may result in this partner feeling misunderstood or invalidated (Péloquin & Lafontaine, 2010), potentially increasing the risk of conflict escalation. It is also more difficult to be empathetic when an individual is emotionally involved in a conflictual situation (Pistrang et al., 2001), which makes the study of dyadic empathy particularly relevant in the context of IPV. In previous studies, physical IPV has been associated with lower levels of global empathy (Clements et al., 2007), whereas psychological IPV has been associated with lower levels of cognitive empathy (Covell et al., 2007). Two studies have found that more cognitive dyadic empathy, but not emotional empathy, was related to the perpetration of less physical and psychological IPV by men from the general population (Lafontaine et al., 2016; Péloquin et al., 2011). More recently, Sun et al. (2020) found an indirect association between CIT and cyberbullying perpetration through lower cognitive empathy in college students, but a study examining the links between CIT, dyadic empathy, and IPV among men who are seeking services for IPV is still needed. Such research would be particularly relevant to inform and improve clinical services that specifically target the reduction of IPV in men (Chovanec, 2020; Mathews, 1996).
Addressing the limitations in past research, the first aim of the present study was to examine the potential roles of CSA and dyadic empathy for understanding IPV in a clinical sample of men seeking psychological services regarding their use of IPV, while controlling for early experiences of family violence. We expected that men with an experience of CSA would report lower levels of cognitive and emotional dyadic empathy (H1) and would use more IPV (physical and psychological) in adulthood (H2). We also hypothesized that men reporting higher levels of dyadic empathy would report lower levels of IPV (H3). The second aim of this study was to investigate whether dyadic empathy would play an intermediary role (mediator or moderator) in the association between CSA and IPV (Q1). In addition to family violence history, we opted to control for social desirability, an important bias in participants’ report of their IPV perpetration (Hamby, 2005).
Method
Procedure
The data collection was conducted as part of a larger study on IPV, in collaboration with a non-profit community organization (i.e., government-funded service) offering individual therapy for relationship difficulties and management of aggression. To participate in the study, men had to be at least 18 years old, be involved in a couple relationship in the last year, and agree to answer a series of self-administered questionnaires (duration: 50 minutes). A consent form informed them of their rights to refuse to participate or to withdraw, without affecting the services received. They were also informed that a summary of their responses would be transmitted to their individual therapists through an alphanumeric code.
Participants
The sample includes 198 men between the ages of 18 and 69 years (M = 34.18, SD = 10.38). They were mostly French-Canadians (91.9%), English-Canadians (2.5%), or were born in another country (5.6%). Participants reported a mean annual income of CAN$22,431(SD = 15,518). With respect to their occupations, 55.8% of the participants were employed, 33.5% were unemployed, 7.6% were full-time students, and 3% were retired. Most men (74.6%) had completed a high school education. The majority had been in a couple relationship for an average of 6 years (SD = 7.78), with 15.8% of them dating, 39.8% cohabiting, 10.2% married, and 34.2% who were single for less than a year. The main reasons for consultation were IPV (29.8%), generally violent behavior (23.7%), and anger management issues (17.7%). Participants were referred to the community organization by another professional (36.7%), the Court (13.3%), a youth center (10.7%) or a parent (17.9%), while 14.3% of men self-referred. About a quarter of the men (28.2%) reported taking medication (e.g., anxiolytics and anti-depressants) for a mental health problem (e.g., depression, bipolar disorder, anxiety, and attention deficit disorder), but no further details are reported here as medication was not a covariate in the main analyses.
Instruments
Childhood interpersonal trauma
As part of the demographic questionnaire, CIT experiences were evaluated using two dichotomous questions (Yes/No): (1) “Were you sexually abused during your childhood or adolescence?” (CSA) and (2) “Did you witness or sustain physical violence from your parents during your childhood or adolescence?” These items were chosen because, as Godbout, Sabourin, and Lussier (2009) have concluded, yes or no items provide as much information as a multi-item measure of CSA (i.e., assessing the frequency and the nature of the abusive acts to create an index of severity) when predicting relational variables, they are brief and are easy to understand by participants.
Dyadic empathy
The Interpersonal Reactivity Index for Couples (IRIC: Péloquin & Lafontaine, 2010), an adaptation of the Interpersonal Reactivity Index (IRI: Davis, 1980), assessed the degree of dyadic empathy based on 13 items rated on a 5-point Likert scale ranging from 0 “do not describe me well” to 4 “describe me well.” It contains two subscales: (1) perspective taking (tendency to spontaneously adopt the psychological point of view of the partner, e.g., “I sometimes try to understand my partner better by imagining how things look from his/her perspective”) and (2) empathic concern (other-oriented feelings of sympathy and concern for the partner, e.g., “I am often quite touched by things I see happen in my relationship”). A high score suggests a high degree of dyadic empathy. Internal consistency for the perspective taking and empathic concern dyadic empathy scales was satisfactory in this sample (α = .83 and .71, respectively).
Intimate partner violence
The Revised Conflict Tactics Scales (CTS2; Straus et al., 1996) assessed the perpetration of IPV during the last 12 months. The CTS2 contains 78 items rated on an 8-point scale (ranging from “this has never happened” to “more than 20 times”). Only two subscales were used in this study: (1) perpetrated physical violence (12 items, e.g., “I choke my partner”) and (2) perpetrated psychological violence (8 items, e.g., “I destroyed something belonging to my partner”). For each type of IPV, the number of times is summed to create a variable representing the number of behaviors that occurred in the last 12 months. In this sample, Cronbach’ alpha coefficients were adequate for both physical (α = .89) and psychological (α = .86) types of IPV.
Social desirability
A brief version (Frenette et al., 2000) of the Balanced Inventory of Social Desirability (BIDR, Paulhus, 1988) was used to assess social desirability, with 18 items rated on a 7-point scale (ranging from “not true” to “very true”). The BIDR assesses self-deception (e.g., “I never regret my decisions”) and impression management (e.g., “I have never dropped litter on the streets”). Items were averaged to create the scores; higher scores indicating a greater presence of social desirability. For this study, only the impression management scale was used (α = .71).
Results
Preliminary Analyses
Descriptive Statistics and Pearson Correlations among Childhood Trauma Indicators, Dyadic Empathy, Intimate Partner Violence, and Social Desirability.
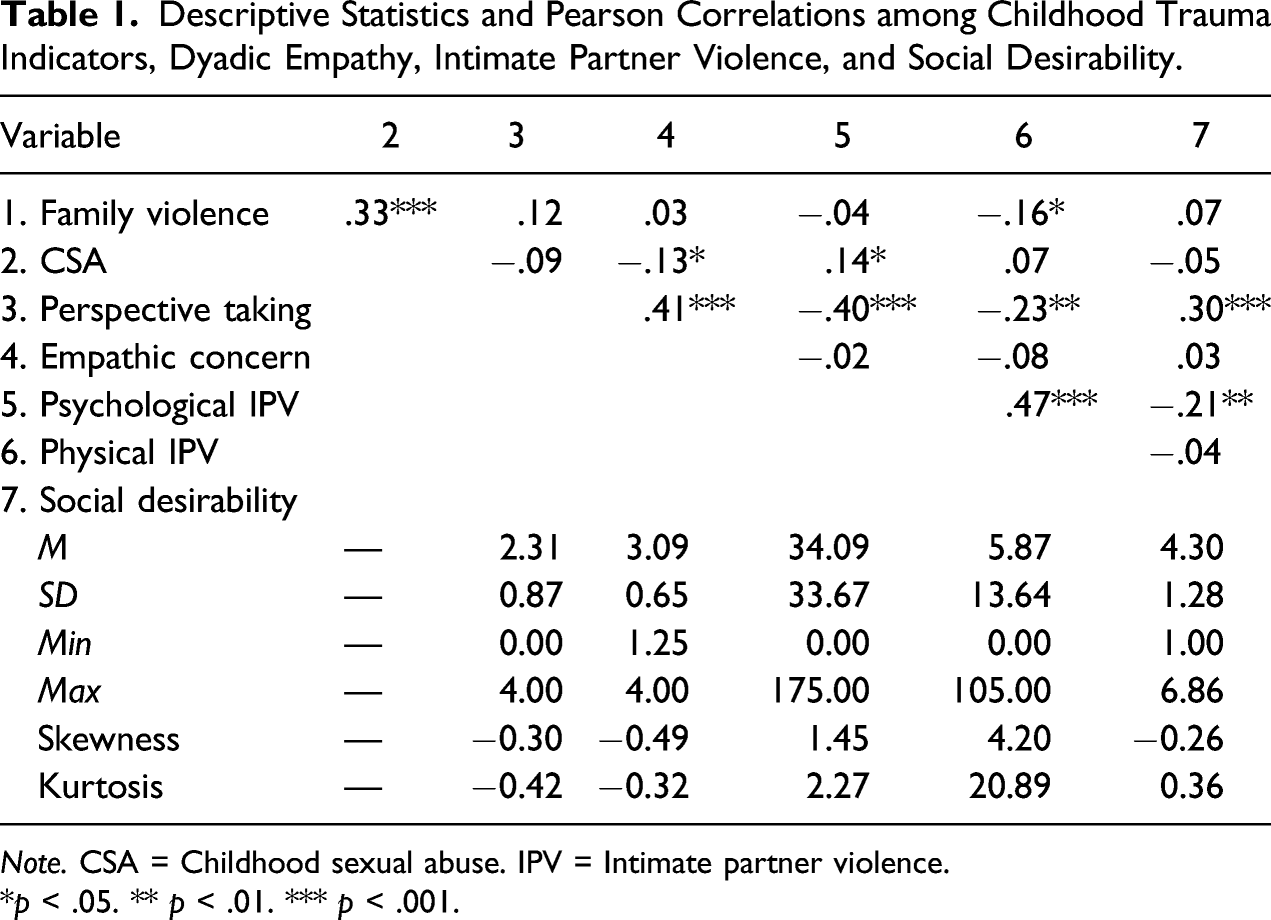
Note. CSA = Childhood sexual abuse. IPV = Intimate partner violence.
*p < .05. ** p < .01. *** p < .001.
Correlations, chi-square tests, and multivariate analyses of variance (MANOVAs) were conducted to examine the associations between demographic variables and the main variables. Pearson correlations did not show any significant correlations for age, annual income, and length of relationship. No significant differences were observed in the MANOVAS and chi-square tests conducted on categorical demographic variables (occupation, education, marital status, and medication), indicating that their statistical control in the main analyses was not justified.
Pearson correlations between the main variables (see Table 1) revealed that CSA was positively associated with the perpetration of psychological IPV, but negatively related to dyadic empathic concern. Perspective taking, but not empathic concern, was negatively associated with psychological and physical IPV. Since history of family violence and social desirability were related to the main measures, they were considered as covariates in the main analyses.
Main Analyses
Hypotheses were verified using hierarchical multiple regression or logistic regression (physical IPV) analyses. For each analysis, social desirability and family violence were entered in the first step as covariates, followed by predictors (step 2). When significant, the unique explained variance of predictors was calculated by the squared semi-partial correlation (sr 2 ). Assumptions of the regression analyses (e.g., normality, homoscedasticity and linearity of residuals, and absence of multivariate extreme values and multicolinearity) were verified.
Childhood sexual abuse and dyadic empathy
The first two hierarchical regression analyses aimed to test hypothesis 1, by predicting perspective taking and empathic concern, with social desirability and family violence as covariates (step 1), and CSA as a predictor (step 2). The regression model for perspective taking was significant, F (3, 186) = 6.070, p < .001, R 2 = .102. After controlling for social desirability, β = .273, p < .001, sr 2 = .07, and family violence, β = .127, p = .087, CSA was not related to perspective taking, β = −.111, p = .134. As for empathic concern, the regression model was not significant, F (3, 186) = 1.679, p = .173, but CSA was uniquely related to a lower level of empathic concern, β = −.164, p = .034, sr 2 = .02.
Childhood sexual abuse and IPV
A hierarchical multiple regression analysis was conducted on psychological IPV to test hypothesis 2, with social desirability and family violence as covariates and CSA as a predictor. The significant model, F (3, 186) = 3.943, p = .009, R 2 = .060, showed that beyond social desirability, β = −.176, p = .015, sr 2 = .031, and family violence, β = −.085, p = .263, CSA was positively related to the perpetration of psychological IPV, β = .158, p = .037, sr 2 = .023. A logistic regression was used to predict physical IPV with CSA, controlling for social desirability and family violence. Results indicated that when social desirability was taken into account, B = −.010, p = .930, family violence was related to a lower likelihood of perpetrating physical IPV, B = −.863, p = .008, while CSA was marginally related to a higher likelihood of perpetrating physical IPV, B = .736, p = .087.
Dyadic empathy and IPV
With regards to the third hypothesis, results from a hierarchical multiple regression analysis, F (3, 190) = 15.160, p < .001, R 2 = .193, suggested that beyond social desirability, β = −.078, p = .259, perspective taking was negatively related to psychological IPV, β = −.447, p < .001, sr 2 = .15, while empathic concern was positively related to psychological IPV, β = .158, p = .029, sr 2 = .02. Results from a logistic regression analysis showed that beyond social desirability, B = .059, p = .630, perspective taking was negatively related to physical IPV, B = −.608, p = .003, but not empathic concern, B = .011, p = .967.
Mediating role of dyadic empathy
To evaluate whether dyadic empathy is an intermediary variable in the associations between CSA and perpetrated IPV (psychological, physical), its mediating role was first examined. Following Preacher and Hayes (2008), a bootstrapping procedure with 5000 samples was used to calculate confidence intervals around the indirect effects of CSA on IPV through dyadic empathy.
Only one indirect effect was significant for the association between CSA and perpetrated psychological IPV through empathic concern, with social desirability, family violence, and perspective taking as covariates. Specifically, this result indicated that men who experienced CSA would perpetrate less psychological IPV through their lower level of empathic concern, B = −.135, SE = .100, 95% CI [-.409, −.003].
Moderating role of dyadic empathy
With regards to moderation, hierarchical regression with the bootstrapping procedure (5000 samples, Preacher & Hayes, 2008) was also used to assess whether dyadic empathy would moderate the associations between CSA and perpetrated IPV (psychological, physical), with social desirability and family violence as covariates. Two moderation effects were found.
A first moderation effect of empathic concern was found in the association between CSA and perpetrated psychological IPV, with social desirability, family violence, and perspective taking as covariates, F (5, 184) = 10.348, p < .001, R
2
= .213. The significant interaction effect of CSA X empathic concern, B = 1.707; SE = .667, p = .011, 95% CI [.391, 3.024], added 1.7% of the explained variance in perpetrated psychological IPV. Results from the simple slopes analyses revealed that when empathic concern was high (one SD above the mean), CSA was positively related to psychological IPV, B = 2.303, SE = .657, p = .001, 95% CI [1.007, 3.600], whereas when empathic concern was low (one SD below the mean) CSA did not predict psychological IPV, B = .106, SE = .618, p = .864, 95% CI [−1.114, 1.326]. As shown in Figure 1a, the experience of CSA in men was related to a higher number of psychological IPV acts, but only when they reported a high degree of empathic concern. The moderating role of (a) dyadic empathic concern and (b) dyadic perspective taking in the associations between childhood sexual abuse and perpetrated psychological intimate partner violence in men seeking help.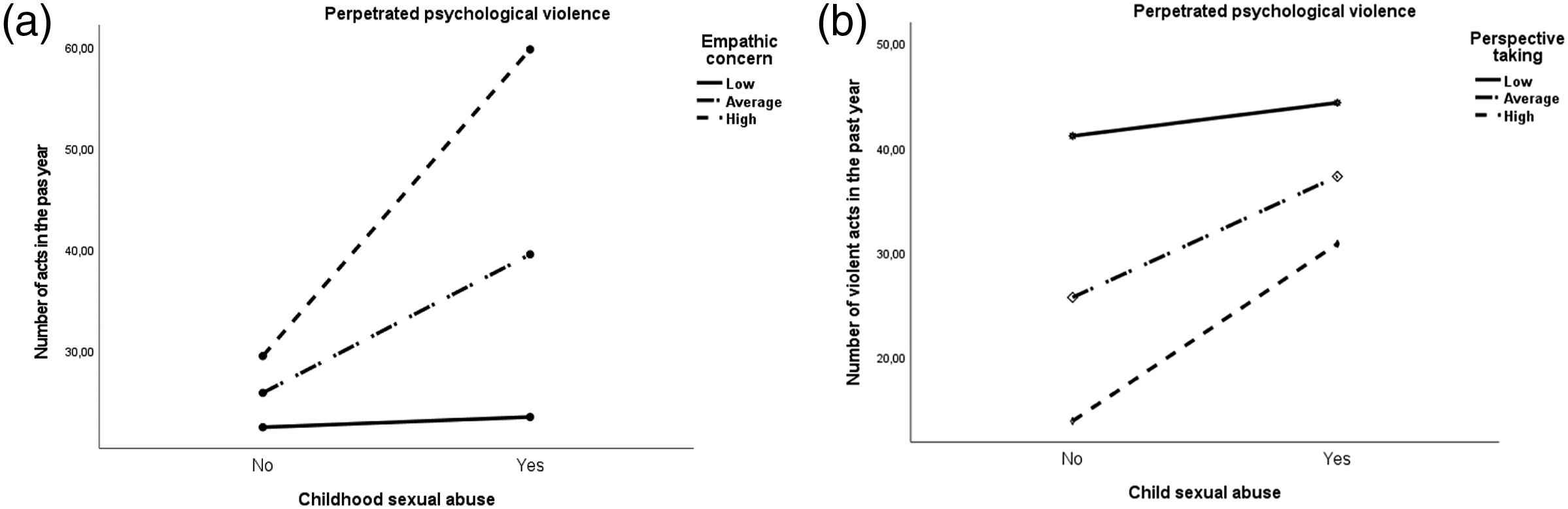
A second significant moderation effect of perspective taking was found in the association between CSA and perpetrated psychological IPV, with social desirability, family violence, and empathic concern as covariates, F (5, 184) = 9.291, p < .001, R 2 = .207. The significant interaction effect of CSA X Perspective taking, B = .919, SE = .454, p = .044, 95% CI [.024, 1.814], added 1.1% of the explained variance in perpetrated psychological IPV. Results from the simple slopes analyses indicated that when perspective taking was high (one SD above the mean), CSA was positively related to the perpetration of psychological IPV, B = 1.824, SE = .650, p = .006, 95% CI [.543, 3.106], whereas when perspective taking was low (one SD below the mean) CSA did not predict psychological IPV, B = .243, SE = .600, p = .686, 95% CI [-.941, 1.427]. That is, the experience of CSA in men was related to a higher number of psychological IPV acts, but only if they reported having a high degree of perspective taking (see Figure 1b). When men reported low levels of perspective taking, they perpetrated high levels of psychological IPV, whether they were sexually abused or not during childhood.
Discussion
Using a fairly large sample of men entering treatment for IPV, findings of this original study revealed the intermediary role of dyadic empathy as a key factor to understand the link between CSA and perpetrated psychological IPV. Precisely, our findings add to the literature by showing that male survivors of CSA generally report lower levels of empathic concerns, but not perspective taking, and higher levels of perpetrated psychological and physical IPV. As expected, higher dyadic perspective taking was related to lower reports of IPV (psychological, physical). In contrast, our results evidenced that higher levels of dyadic empathic concern in men—that is, being touched, concerned, or even disturb by one’s partner experience—were associated with their higher reports of psychological IPV perpetration.
Our preliminary results indicated that 16.5% of men reported being a victim of CSA, while 12.4% reported both CSA and having experienced or observed physical violence in their family, justifying the relevance of controlling for the latter in the explanatory models of IPV under study. These rates are similar to those documented in epidemiological studies. Participants also reported having perpetrated more psychological than physical IPV acts, which is consistent with data from the current literature. The condemnable social nature of physical aggression (Arias & Beach, 1987) and the general precedence of psychological violence on physical violence (Holtzworth-Munroe et al., 1997) could also explain this result.
When controlling for social desirability and history of family violence, results showed that CSA in men was related to a higher perpetration of psychological IPV, whereas only a marginal association was found between CSA and the perpetration of physical IPV. These results partially support our hypothesis and corroborate the findings of previous studies (e.g., Brassard et al., 2014; Cyr & Payer, 2011). Because we controlled for family violence history, it is possible that the unique contribution of sexual victimization was only marginal in explaining men’s perpetration of physical violence, as opposed to significant associations usually found in previous studies (Godbout et al., 2019). It may also be that, as stated by Li et al. (2020), the association between CSA and IPV is generally weak because other contextual factors—such as empathy—might be more decisive in IPV perpetration, a multi-determined and complex behavior.
Our findings revealed that male survivors of CSA reported lower levels of empathic concerns towards their romantic partners than men who did not experience CSA. Traditional masculinity norms (e.g., not sharing one’s emotions, not asking for help, being strong and capable of defending oneself) paired with the shame or guilt experienced my male victims might have lead them to isolate themselves rather than address their traumatic reactions (Easton et al., 2013), which could have disturbed the mature development emotional empathy. Contrasting with previous studies (e.g., Péloquin et al., 2011), however, higher empathic concerns in men was associated with a higher likelihood of perpetrating psychological IPV. In a marital conflict, empathic concerns towards a partner’s emotions may lead to the over-arousal of men and the inability to manage their own emotions in addition to the partner’s negative emotions, which could result in the use of violence. Ford (2002) also suggested that inadequate management of emotions limits awareness and may lead to violence. More recently, Dugal et al. (2021) found that affect dysregulation, the difficulty to control and tolerate strong negative affect, was related to the perpetration of psychological IPV in men and women. The perpetration of psychological IPV may thus result from a difficulty to manage emotional distress stemming from a higher emotional dyadic empathy (i.e., being overly concerned or disturb).
Furthermore, this study identified dyadic empathic concerns as a mediator and a moderator of the association between CSA and psychological IPV. In addition to the direct positive association between CSA and perpetrated IPV, a negative indirect link was observed through low empathic concerns (i.e., mediation). This indirect link means that male victims of CSA would generally use fewer psychological IPV through their lower empathic concerns, suggesting that their inhibited reaction to their partner’s distress could somehow limit their perpetration of violence. Briere et al. (2010) suggested that adults survivors of CIT may be more likely to avoid negative affects to limit their duration and impact. Although avoidance may interfere with the regulation of emotions (including empathy), this strategy would be favored over confrontation or aggression. However, a moderation effect revealed that when male survivors of CSA experienced high level of empathic concerns, they were more likely to perpetrate psychological IPV. Berthelot et al. (2014) have suggested that interpersonal trauma victims tend to use more violence during personal or relationship difficulties. It is plausible that when male survivors of CSA actually experience their partner’s distress during conflict, they feel overwhelmed or flooded by emotions—their own and their partner’s. The use of violence would be an inappropriate but temporarily effective means of dealing with this emotional overload by externalizing it. They could also use IPV as a harmful strategy to defend themselves from a partner’s blame or to counter-attack their partner during a conflict (Dugal et al., 2021).
Although not directly related to CSA, dyadic perspective taking was related to a lower perpetration of IPV, which corroborates past studies involving men from the community (Péloquin et al., 2011) and clinical settings (Covell et al., 2007). Davis (1996) explained that cognitive empathy limits the probability of violent acts by allowing the person to interpret a threat differently. Thus, in a couple conflict, a man presenting with higher perspective taking would better understand the context of his partner’s behaviors, rather than attributing them to personal characteristics, use blame, or use IPV to respond to behaviors he deems to be offensive (Epstein et al., 2008). Our results also evidenced a moderating role of dyadic perspective taking, whereby the positive link between CSA and psychological IPV was only significant when perspective taking was high. In other words, when men displayed weak perspective taking, they were more likely to perpetrate psychological violence, whether or not they experienced CSA. In the presence of high perspective taking, however, male victims of CSA were more likely to perpetrate psychological IPV than non-victimized men, suggesting that their early trauma could make it more difficult to abstain from saying hurtful words even if they could grasp their impact on their partners. Although this finding is quite unique in the literature, some authors have suggested that high social intelligence, which is closely linked to perspective taking, can play an important role in effective social manipulation leading to emotional abuse towards another person (Sutton et al., 1999; Yeo et al., 2011). Manipulating or hurting the partner could be a defensive response to a perceived threat, blame, or negative emotions in the partner, as a strategy to protect oneself. To understand this original result further, other relevant variables such as undesirable personality traits (e.g., psychopathy) and impulsivity (Dugal et al., 2021) should be studied.
Limitations
Several limitations of this study are worth mentioning. First, the cross-sectional retrospective design does not allow us to infer causality. Future research should use prospective longitudinal designs to assess the associations between a larger number of CIT, dyadic empathy, and IPV, while also considering the nature, duration, and severity of this victimization. Our dichotomous measure of CSA limited our understanding of the men’s experience and was also subject to underreporting bias, as men could have perceived an early sexual experience with an adult or older child as not abusive (Vaillancourt-Morel et al., 2016). Using a measure based on an objective definition of the behaviors that constitute CSA under the law without asking participants to label their experience as victims of CSA would limit this bias. Although the sample size is fairly large (N = 198) and diversified in terms of age (18–69), it lacks diversity concerning language (mostly French) and socioeconomic status (mostly low income). The sample was obtained from a single community organization helping men presenting with relationship difficulties or IPV, which limits the generalizability of our results. This clinical sample is not representative of the general population nor of the population of male victims of CSA. Generalization of the results is also limited in terms of gender, sexual, and cultural diversity, as most participants are Caucasian Canadian heterosexual cisgender men. Future research should recruit more diversified samples in terms of language, nationality, gender identity, and sexual orientation to increase the generalizability of the results and further document the underlying mechanisms linking CSA to IPV among more diverse samples.
In addition, while self-administered questionnaires facilitate access to intimate information such as CSA or IPV, they are limited by several biases (social desirability, lack of introspection, and recall bias). Indeed, participants tend to underreport their acts of violence (e.g., Hamby, 2005), which justified our decision to include social desirability as a covariate. Although we controlled for history of family violence, the question we used to assess this variable did not distinguish between witnessed parental violence and sustained physical violence. Dyadic studies are also needed to consider the perspective of both partners and document dynamics in which violence occurs. Finally, this study did not consider sexual coercion, cyberviolence, coercive control, and stalking as forms of violence, nor the severity or the context of the perpetrated acts, which could limit our comprehension of this phenomenon. Still, it is relevant to pursue the study of psychological IPV risk and protective factors (e.g., attachment, emotional regulation, and undesirable personality traits), because it is more common (Jose & O’Leary, 2009), but less studied than physical violence.
Clinical Implications
This study provides an original understanding of some of the mechanisms that modulate the perpetration of psychological (but not physical) IPV among a rather large sample of men within a clinical population. Our results highlight the importance of investigating experiences of CIT in men who are seeking help for relationship problems or IPV. By assessing the unique effects of these early traumas, therapists can develop personalized treatments that address the specific protection or survival mechanisms men have developed to survive CSA or other traumas, such as lower empathic concern. Indeed, many challenges have been identified by therapists regarding the regulation of emotions in CSA survivors, including emotional flooding, emotional numbing, dissociation, and a restricted range of affect (MacIntosh & Johnson, 2008). Our results thus emphasize the necessity of helping men learn to regulate the emotional flooding that may result from their emotional empathy (empathic concern) in conflict situations, as well as improving their ability to consider their partner’s point of view (perspective taking), while refraining from using this knowledge to hurt their partner. In addition to helping men regulate their negative emotions such as shame (MacIntosh & Johnson, 2008) and anger (Brassard et al., 2014), therapists can use interventions to help men improve their empathy and non-violent self-expression skills (e.g., Chovanec, 2020) as an alternative to psychological violence. Lastly, emotionally focused interventions could be used to progressively improve men’s emotion regulation and relational security, while being mindful that longer-term treatment is often needed among CSA survivors (e.g., MacIntosh & Johnson, 2008).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research authorship, and/or publication of this article: This research was supported in part by Université de Sherbrooke and Centre de Recherche Interdisciplinaire sur les Problèmes Conjugaux et les Agressions Sexuelles (CRIPCAS).