
Abstract
This study explored whether changes in risk and protective factors of intimate partner violence (IPV) can account for the noted reduction in 12-month IPV prevalence in New Zealand between 2003 and 2019. Changes in relational mobility over time were also explored. Data from two population-based surveys of 18-64 year-old ever-partnered women in New Zealand that were conducted according to identical procedures in 2003 (n=2764) and 2019 (n=944) were used. Changes in a variety of potential risk and protective factors over time and their possible contribution to IPV reduction were assessed. The findings indicated that there was no change in the prevalence of the strongest risk and protective factors of IPV victimisation and perpetration over time (e.g. partner concurrent relationship, previous exposure to violence for both respondent and partner, and partner’s problematic alcohol/drug use). However, a combination of factors including decline in women’s problematic alcohol or drug use, decline in the number of children within families, and increases in the proportion of women and partners with a qualification higher than secondary education are likely to be associated with the reduction in IPV prevalence. A greater degree of relational mobility, demonstrated through a greater proportion of women who left their abusive partner permanently and increased numbers of relationships that women had, was also observed between two study years. Overall, these results indicate that changes in 12-month IPV prevalence over time are likely to be linked with changes that increase women’s autonomy and ability to move out of violent relationships. To achieve sustained reductions in IPV, more comprehensive and planned efforts are needed to address other underlying and exacerbating causes, including problematic alcohol/drug use and previous exposure to violence during childhood and adulthood.
Keywords
Introduction
Intimate Partner Violence (IPV) against women is the most common form of gender-based violence and is widely recognised as a serious public health and human rights problem (World Health Organization, 2001). IPV can take a number of forms, including physical and sexual violence, as well as psychological abuse. It is now well-documented that IPV is associated with a wide range of deleterious consequences for women’s physical, mental, sexual, and reproductive health including fatal and non-fatal injuries, HIV and sexually transmitted infections, induced abortion, depression, anxiety and suicide (Sanz-Barbero et al., 2019; World Health Organization, 2013).
Given the adverse consequences of IPV for victims, it is important to investigate changes in IPV prevalence rates over time. Currently, there is limited consistent and reliable data available to monitor changes in the prevalence of IPV over time. New Zealand is one of a few high-income countries where more than one comprehensive population-based survey of violence against women has been conducted following identical procedures: the first survey was conducted in 2003, and the second survey in 2019. The analysis indicated that there was an approximately 50% reduction in the proportion of women who reported experiencing recent (12-month) physical and psychological IPV (for physical IPV from 5% in 2003 to 2.4% in 2019 and for psychological IPV from 8.4% in 2003 to 4.7% in 2019). Stable levels were found for lifetime prevalence of physical and psychological IPV (Fanslow, Hashemi, Malihi, Gulliver, & McIntosh, 2021 ).
Between the two surveys, a series of actions were taken to address family violence including legislation (e.g. amendments to family violence law and protection for victims act (Henaghan et al., 2020)) and prevention campaigns (e.g. the family violence: It is not ok national campaign (Roguski, 2015), and the Accident Compensation Corporation (ACC):funded mates and dates high schools programme on healthy relationships (Duncan & Kingi, 2015)). Many of these initiatives have focussed on increasing recognition of physical and sexual violence and taking action to reduce women’s exposure to violence after it has occurred, through steps such as encouraging women to leave abusive relationships.
In other countries, a decline in prevalence rates has also been reported. In Australia, the proportion of women reporting any physical or sexual violence during 12 months prior to the survey decreased from 7.1% to 5.8% between 1996 and 2005 (Australian Bureau of Statistics, 2005). A decline in prevalence of sexual IPV was also found in Finland between 1997 and 2005, using data from two national surveys on violence against women (Heiskanen & Piispa, 2008).
When changes in the prevalence of IPV are identified, providing information about potential explanations becomes the next important step, as understanding of explanatory factors may improve the tailoring of prevention efforts or guide appropriate targeting of services (Heise, 2011). Some studies have explored factors contributing to decline in intimate partner homicide (e.g. gender equality, relative employment, divorce rates, men’s education and exposure-reduction) (see Dawson et al., 2009), but few studies have explored potential explanations for changes in non-fatal forms of IPV (Farmer & Tiefenthaler, 2003).
The socio-ecological model is a widely used conceptual framework for understanding violence as a complex interplay between individual, relationship, social, cultural and environmental factors (Heise, 1998, 2011). This framework has been important in identifying risk and protective factors associated with violence occurrence, but also holds promise for prevention, as it carries the assumption that changes in contributing factors can potentially lead to changes in prevalence (Heise, 2011). These factors are worth exploring to ascertain the degree to which they contribute to violence exposure in different settings and over time. We summarise what is currently known about IPV risk and protective factors below.
At the individual level, decreased likelihood of recent experience of IPV has been found to be associated with socio-demographic characteristics of women and their partners, including older age, higher education, being employed and higher socio-economic status (such as living in areas with low deprivation level) (Abramsky et al., 2011; Fanslow & Gulliver, 2015; Yakubovich et al., 2018). Increased likelihood of IPV (victimisation and perpetration) is associated with previous exposure to different forms of violence (Abramsky et al., 2011), such as witnessing IPV during childhood, and experience of sexual abuse during childhood (Abramsky et al., 2011; Fanslow, Hashemi, Gulliver, & McIntosh, 2021; Speizer, 2010). Women’s exposure to physical and sexual violence by non-partners during adulthood has also been shown to be a risk factor for IPV (Abramsky et al., 2011).
At the relationship and behavioural level, increased likelihood of IPV experience is associated with problematic alcohol or drug use by both women and their partners, while perpetration of IPV is associated with men who use violence outside the home and who have concurrent sexual relationships (Abramsky et al., 2011; Fanslow & Gulliver, 2015; Fanslow, Gulliver, Hashemi, Malihi, & Mcintosh, 2021). In addition, having a greater number of children has also been found to increase risk of IPV (Peek-Asa et al., 2017).
However, the social context in which relationships occur also has bearing on the degree to which violence may occur or persist. For example, an increase in the recognition of violence and social messaging to encourage women to reduce violence exposure by leaving the relationship could result in a reduction of 12-month prevalence of violence. Concurrently, if these messages were successfully heard and actioned at the population level, we would expect to see an increase in the proportion of people who leave violent relationships, and an increase in the number of relationships that people have, as people are likely to re-partner.
However, these actions are only feasible in societies where the macrosocial factor of relational mobility exists. Relational mobility has been described as how much freedom and opportunity a society affords individuals to ‘choose and dispose of interpersonal relationships based on personal preference’ (Yuki & Schug, 2012). In societies with low relational mobility, interpersonal relationships are less flexible, more stable and guaranteed, but present fewer opportunities for people to find new relationships or leave unsatisfying ones (Brint, 2001; Caporael & Brewer, 1991). In contrast, societies with high relational mobility give people more choice and freedom to select or change interpersonal relationships, and to select partners based on self-interest (Chiang, 2010; Thomson et al., 2018). New Zealand has been identified as a society with high relational mobility (Chiang, 2010).
This paper investigates whether the observed reductions in IPV prevalence identified in two New Zealand surveys can be accounted for by changes in individual and behavioural level risk and protective factors previously identified in the literature. Additionally, to explore if relational mobility may have been used in the context of violent relationships, we examine whether there is a concurrent change in the proportion of women leaving violent relationships permanently, and in the number of relationships reported by women between the two study years.
Materials and Method
Procedure and Participants
Data were drawn from two cross-sectional studies on family violence conducted in New Zealand in 2003 and 2019. A comprehensive description of the methods used in the 2003 and 2019 surveys has been previously presented (Fanslow, Gulliver, Hashemi, Malihi, & Mcintosh, 2021). A brief description of the two surveys is presented here.
Sampling Strategy
The 2003 study was conducted in Auckland and Waikato regions. For the 2019 study, Northland was also included in the sampling. Together Auckland, Northland, and the Waikato regions of New Zealand account for approximately 40% of the New Zealand population with a diverse population of Māori, Pasifika, Asian and European New Zealanders.
Sampling strategies were similar in both surveys. A population-based cluster sampling scheme with a fixed number of dwellings per cluster was used for both studies. Primary sampling units (PSUs) were based on meshblock boundaries which contain between 50 and 100 dwellings. The starting point consisted of a randomly selected street and street number within each PSU. Interviewers made up to seven visits to each selected household to identify and recruit study participants. Non-residential, aged-care and short-term residential properties were excluded. Interviewer training and support procedures were comparable across survey waves.
Participants of the 2003 study were 2855 women aged 18–64 years. In 2019, the eligible population was expanded to include women aged 16 years and older. For the purpose of this paper, only ever-partnered women aged 18–64 years from each sample were included, equivalent to almost 94% of all women surveyed in both waves (2003, n= 2674; 2019, n=944).
In 2003, a household response rate of 88.3% was achieved and 75.8% eligible woman response rate was obtained, yielding an overall response rate of 66.9%. In 2019, a household response rate of 78% was achieved and 63.7% eligible woman response rate was obtained, yielding an overall response rate of 63.7%. Figure 1 demonstrates the number of people invited and those who were interviewed and included in the analyses for each survey year. Flow diagram of female participants in the 2003 and 2019 population-based studies on family violence in New Zealand. *Number of included women aged 18-64 from the 2019 survey.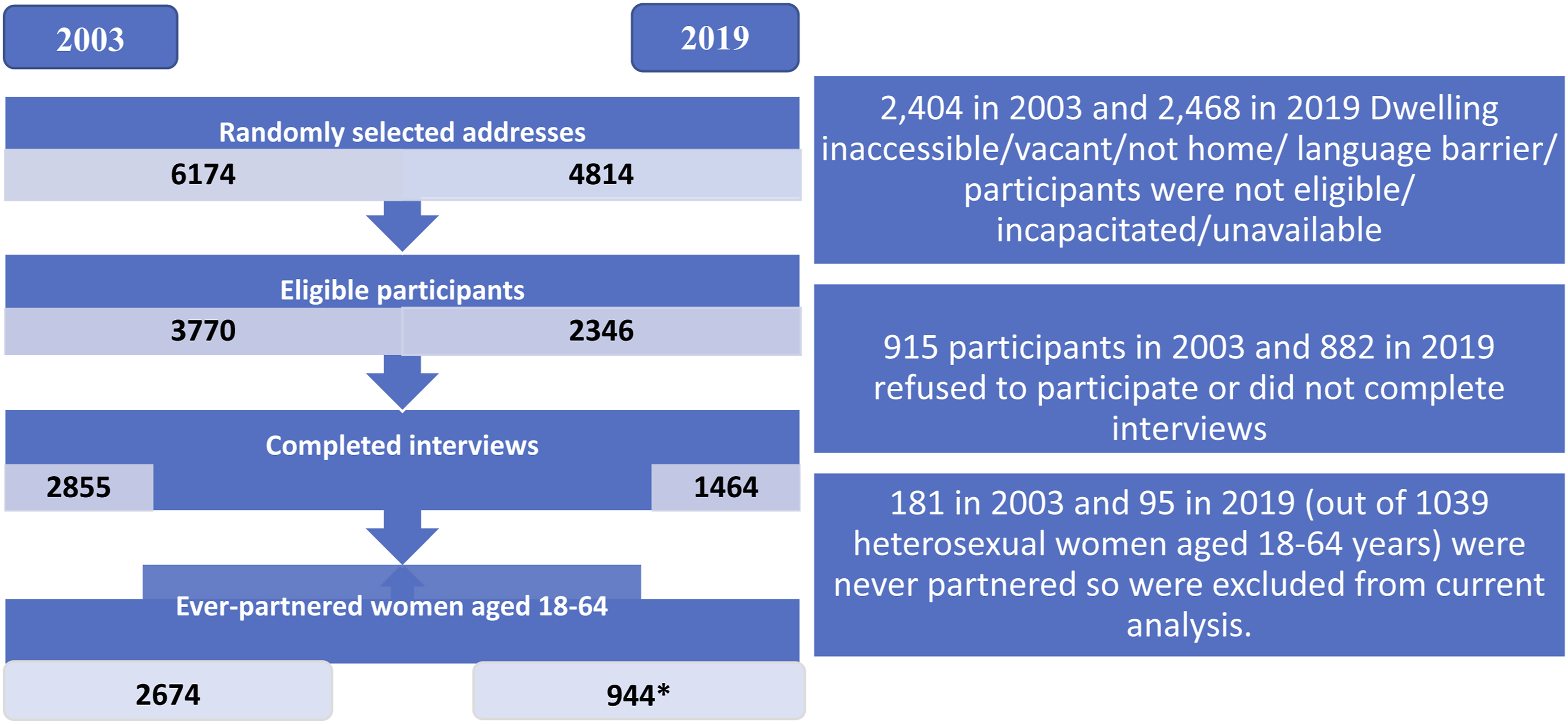
Demographic characteristics of ever-partnered women aged 18–64 years in 2003 and 2019 surveys.
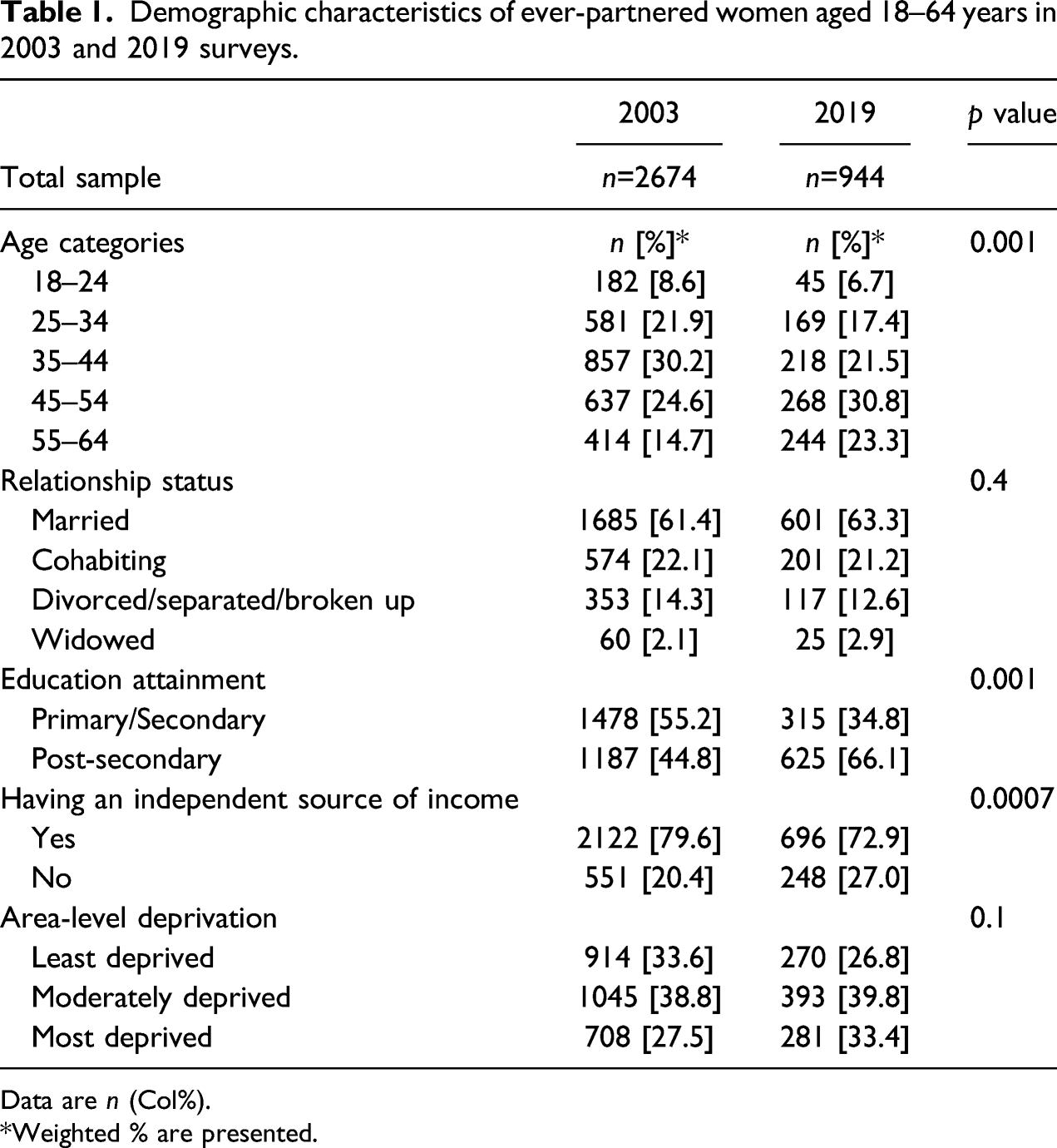
Data are n (Col%).
Weighted % are presented.
Safety and Ethics Considerations
Ethics and safety recommendations for research on violence against women were followed throughout the research (World Health Organization, 2001). One individual was randomly selected from each household for the interview. In households with more than one eligible resident, the participant was randomly selected. Interviews were conducted in privacy with no one over the age of 2 years present. At the completion of the interview, interviewers provided all respondents with a list of approved support agencies regardless of disclosure status. Written informed consent was obtained from all participants.
Ethics approval was granted through the University of Auckland human participants’ ethics committee (reference number 2002/199 for the 2003 study and 2015/018244 for the 2019 study).
Measures
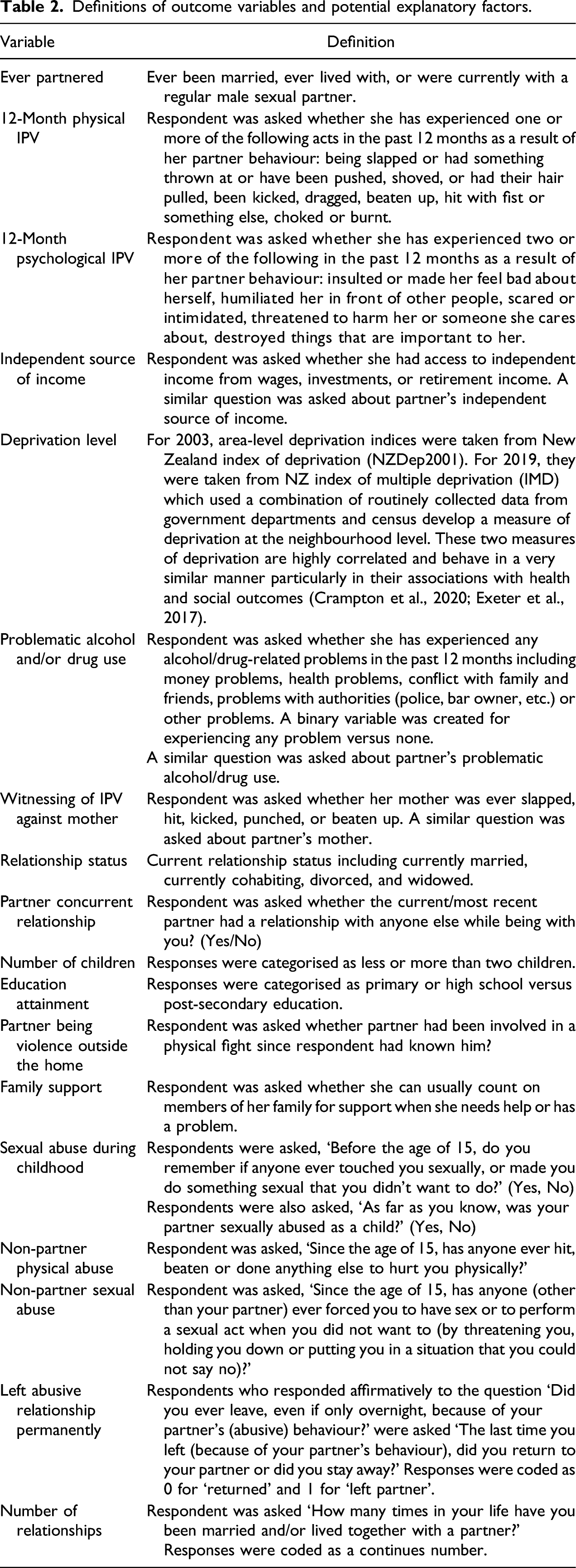
Definitions of outcome variables and potential explanatory factors.
Analytic Procedures
Analyses were performed to identify potential explanatory factors that might explain changes in 12-month IPV prevalence over time. Three criteria need to be fulfilled for a factor to be identified as contributing to the reduction in IPV prevalence.
Changes in potential factors for IPV victimisation 2013–2019.
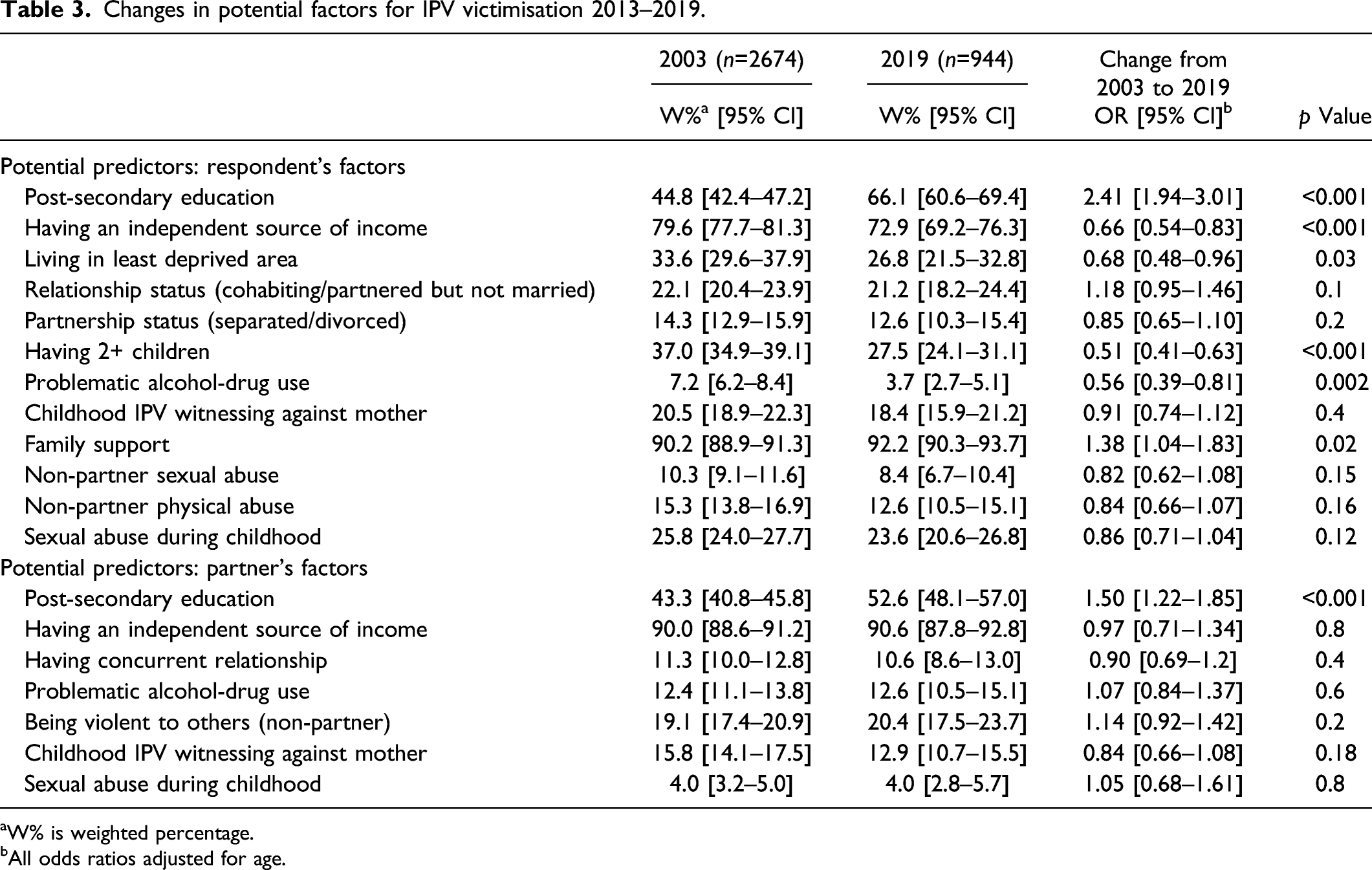
aW% is weighted percentage.
bAll odds ratios adjusted for age.
Association between IPV 12-month prevalence and all potential explanatory factors used (data from both years combined).
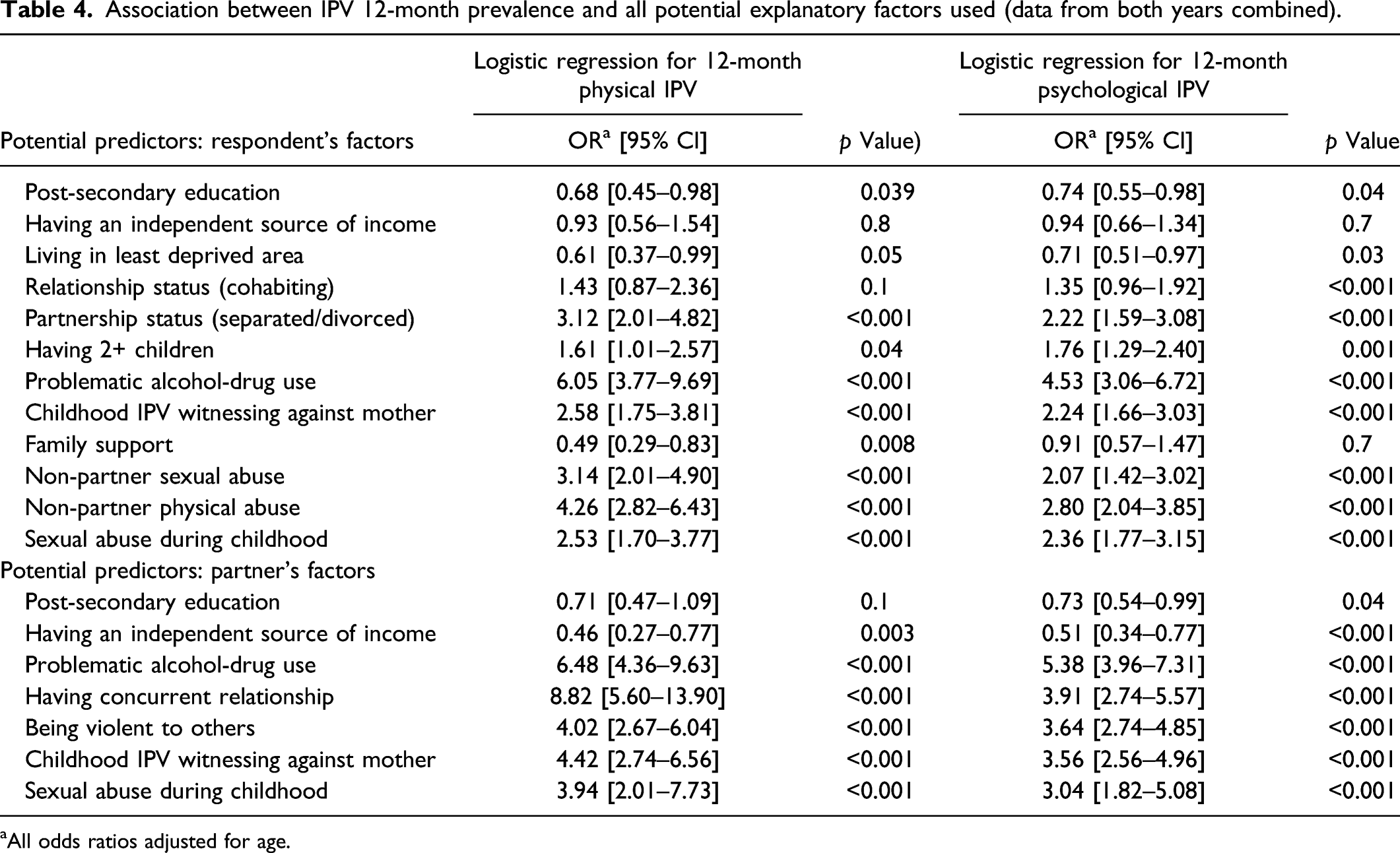
aAll odds ratios adjusted for age.
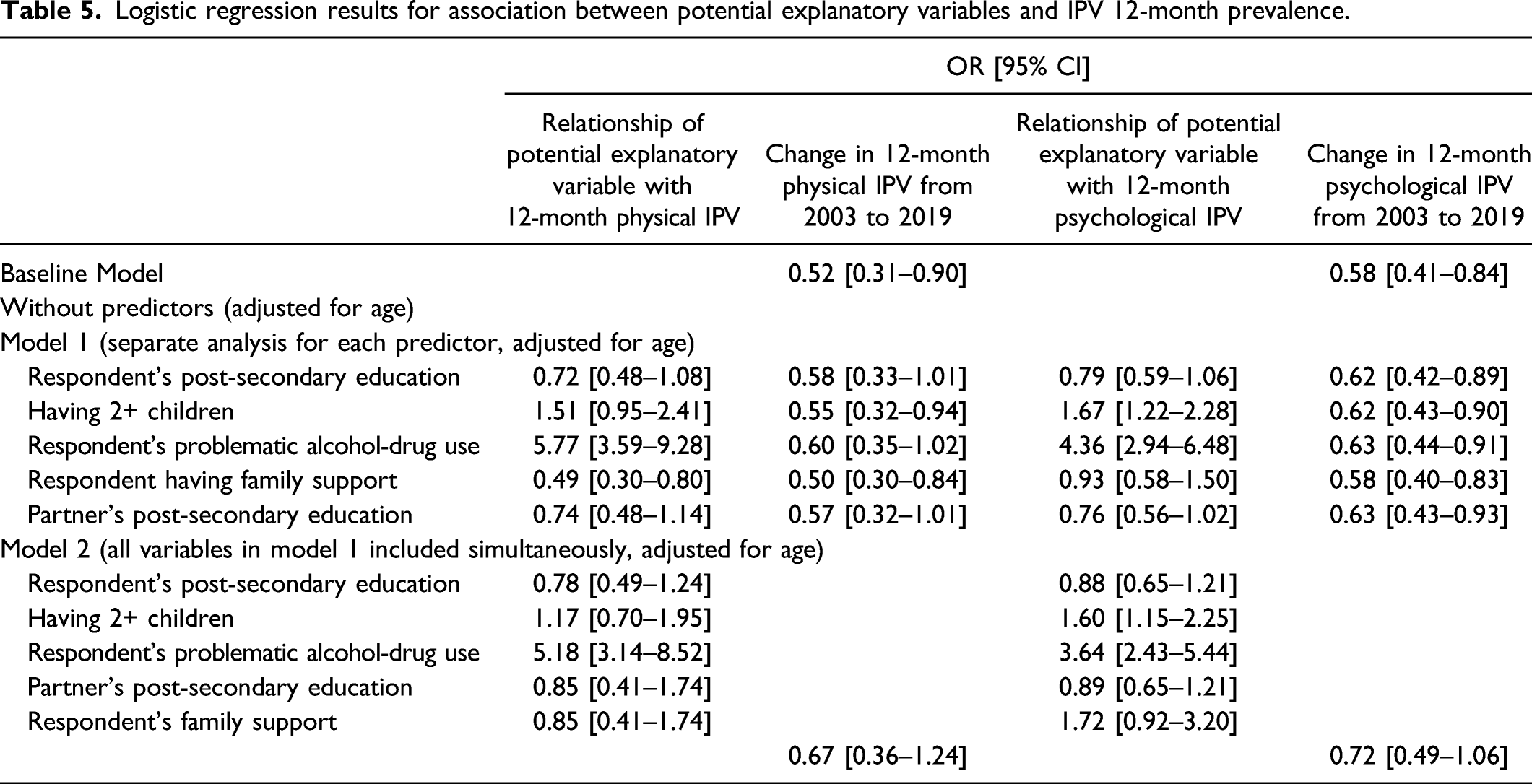
Logistic regression results for association between potential explanatory variables and IPV 12-month prevalence.
Age was entered as covariate in all analyses as the respondents from 2019 were older than respondents from 2003. Age was included as it is not a modifiable predictor.
To assess relational mobility, mean and SD of the number of relationships were calculated, and t-test was used to determine if there were significant differences between 2003 and 2019. The proportions of women who left an abusive partner permanently were reported as percentages with 95% CIs.
Missing data including do not know, do not remember, and no responses were excluded from all analyses. Missing data were less than 3% for all examined variables with the exception of variables related to the partner’s IPV witnessing (with 11% missing) and partner’s childhood sexual abuse (with 6% missing). This was due to relatively high number of participants who responded with ‘Do not Know’ to these questions about their partner’s experiences. All analyses were conducted using Stata/SE 15.1 (StataCorp, 2017). In all analyses, the complex sampling design has been allowed for by using the Survey Data Analysis programmes in Stata/SE, which allows for stratification by sample location (region), clustering by primary sampling units (PSU) and weighting of data to account for the number of eligible participants in each household.
Results
The 12-month prevalence of physical IPV decreased from 5% in 2003 to 2·4% in 2019 (OR = 0.52, 95% CI: 0.31–0.90). The 12-month prevalence of psychological IPV decreased from 8.4% in 2003 to 4.7% in 2019 (OR = 0.58, 95% CI: 0.41–0.84) (see Baseline Model, Table 5).
To determine if potential factors explained the observed reductions, the following three steps were taken.
Step 1. Exploring Changes in the Prevalence of Potential Factors Between the Two Survey Years
Changes in risk and protective factors between 2003 and 2019 that might have contributed to the observed decline in IPV prevalence over time were examined. The following statistically significant changes were noted. The proportion of respondents with post-secondary education increased significantly from 44.8% in 2003 to 66.1% in 2019. Similarly, there was a significant increase in the proportion of partners with post-secondary education from 43.3% in 2003 to 52.6% in 2019. A small but significant increase was observed in the proportion of women who reported that they could count on their family for support when needed (90.2% in 2003, 92.2% in 2019). Fewer respondents had two or more children in 2019 (37% in 2003, 27.5% in 2019). There was a decrease in the proportion of women who experienced any alcohol and or drug-related problems (7.2% in 2003, 3.7% in 2019) (Table 3). Changes in the above mentioned factors are plausibly associated with the reduction in IPV, as supported by previous literature.
There were no changes in the overall prevalence rates of the following factors between the two survey years: cohabiting and divorce rates; respondent’s and respondent’s partner’s childhood witnessing of IPV against their mother; respondent’s and partner’s exposure to childhood sexual abuse; and respondent’s exposure to physical or sexual non-partner violence. No other changes in the prevalence of other partner related factors were noted (Table 3).
In 2019, fewer women reported having an independent source of income (72.9 vs. 79.6% in 2003) and fewer reported living in areas with low deprivation (26.8 vs. 33.6% in 2003). These changes would usually be expected to be associated with an increase in IPV (Table 3).
Step 2. Testing Potential Factors for Association With Two Forms of IPV
Almost all potential factors were significantly associated with IPV prevalence. The only exception was respondent’s independent source of income which was not significantly associated with any form of IPV. However, partner having an independent source of income was negatively associated with both forms of IPV (Table 4).
Respondent’s and partner’s problematic alcohol/drug use was associated positively and most strongly with both forms of IPV, followed by respondent’s and partner’s previous exposure to violence (including respondent’s non-partner sexual abuse, respondent’s exposure to non-partner physical violence, respondent’s and partner’s exposure to sexual abuse as a child, and respondent’s and partner’s witnessing of IPV).
Partnership status (being divorced and cohabiting), partner having concurrent sexual relationships and partner being violent outside the home were positively associated with both forms of IPV (Table 4).
Step 3. Exploring the Role of Potential Factors in the Observed Reduction in IPV Prevalence
The Baseline Model, which demonstrates the reduction in IPV prevalence which was obtained when only survey year and age were included as predictors is shown in Table 5. To estimate each factor’s independent contribution to the observed reduction in IPV in the Baseline Model, factors that met Criteria 1 and 2 were entered one by one into logistic regression analyses along with a dummy variable representing survey year (Model 1). The factors entered were respondent’s and partner’s post-secondary education, having 2+ children, respondent’s problematic alcohol-drug use and respondent’s family support. To determine if individual factors contribute significantly to the observed reduction, the odds ratios of change in prevalence estimates of IPV obtained in Model 1 are compared with the Baseline Model (Table 5).
Inclusion of respondent’s and partner’s post-secondary education and respondent’s problematic alcohol-drug use attenuated the reduction in 12-month physical IPV to non-significance (compare ORs for Baseline Model in Table 5 with ORs for Model 1). Inclusion of respondent’s family support did not alter the observed reduction in any form of IPV prevalence over time, while the rest of included factors had minor influence.
Model 2 presents a multivariable logistic regression model where all the factors included in Model 1 were included simultaneously. Inclusion of these variables fully accounted for the observed reduction in 12-month physical and psychological IPV (Table 5).
Relational Mobility
There was a significant increase in the average number of intimate relationships that women reported, from less than 1.5 (SD = 0.76) relationships in 2003 to 2.5 (SD = 0.80) in 2019 (t-test = 36.67, p < 0.0001). There was also a significant increase in the proportion of women who reported that they permanently left an abusive partner (from 33.4% in 2003 to 40.3% in 2019).
Discussion
The overarching aim of the current study was to identify factors that may contribute to the observed reduction in IPV prevalence. Overall, findings indicate that a combination of factors were associated with the significant reduction in IPV prevalence. The contributing factors were decline in women’s problematic alcohol or drug use, decline in the number of children within families, and increase in the proportion of women and partners with a qualification higher than secondary education. While factors related to perceived family support in emergencies showed a small increase over time, this factor did not contribute to explaining the decline in IPV prevalence. Additionally, findings suggest that there might have been a greater degree of relational mobility in 2019 as evidenced by the increase in the proportion of women who permanently left violent relationships and in the increased number of total relationships women had.
While the observed reduction in IPV could be the result of changes in the association between risk and protective factors and IPV over time, and this study found that almost all examined factors retained a significant association with IPV in both 2003 and 2019. This suggests that these factors are still relevant as risk and protective factors for IPV (i.e. they did not change their relationship with IPV over time). The strongest risk and protective factors for IPV perpetration over time were partner’s problematic alcohol or drug use, partner having concurrent sexual relationships, partner being violent to others, and partner having previous exposure to violence as a child (witnessing IPV or being sexually abused). Risk of victimization was associated with women’s problematic alcohol-drug use, previous exposure to violence including non-partner’s physical or sexual abuse, and sexual abuse and/or exposure to IPV during childhood. Findings of the present study reinforce the need for policy initiatives to mitigate these IPV risks.
One of the most prominent factors that contributed to the decline in IPV prevalence was the reduction in respondent’s problematic alcohol or drug use. This is not surprising given the strong association between problematic alcohol or drug use and IPV experience in this study and in previous studies (Abramsky et al., 2011; Klostermann & Fals-Stewart, 2006). However, problematic alcohol-drug use may also be a consequence, rather than a cause, of IPV experience (Fanslow & Gulliver, 2015; Peters et al., 2012), so that no firm conclusions about the causality of this relationship can be inferred.
The increase in the proportion of women and their partners who had post-secondary education also contributed to the decline in IPV prevalence between 2003 and 2019, with a somewhat stronger relationship observed for increase in men’s education. This finding is consistent with previous studies reporting that men’s education has a negative association with IPV perpetration (Abramsky et al., 2011; Yakubovich et al., 2018). The increase in women’s education have also been reported to be associated with reductions in IPV experience (Abramsky et al., 2011; Farmer & Tiefenthaler, 2003; Yakubovich et al., 2018).
While women in the 2019 sample were exposed to lifetime IPV at a comparable rate with women from 2003 (Fanslow, Hashemi, Malihi, Gulliver, & McIntosh, 2021; Fanslow, Gulliver, Hashemi, Malihi, & Mcintosh, 2021), a higher number of women from the 2019 sample reported that they were able to leave their abusive partner. Leaving a violent relationship, in turn, could contribute to having a greater number of relationships, as people are likely to re-partner. Findings from the present study support this as women from the 2019 sample reported having a higher number of relationships than women from the 2003 sample. Collectively, these findings suggest that there was a greater degree of relational mobility in the 2019 sample compared with the 2003 sample which is consistent with the observed reduction in 12-month IPV prevalence.
Societal messaging may have contributed to increased relational mobility, through fostering growing recognition of the unacceptability of violence, and recommendations encouraging women to leave violent relationships. While leaving is not always successful at preventing further violence, other studies have reported that shorter duration of relationships with partners is associated with less violence exposure (Dawson et al., 2009; Kennedy et al., 2018). This study also found that there was a significant decrease in the number of children within families, and that this change was associated with the reduction in 12-month physical IPV prevalence. This could also be a factor associated with relational mobility, as women with fewer children may have fewer obstacles to leave a relationship if it turns violent. Others have found that increased number of children in the family is associated with partner violence (Peek-Asa et al., 2017).
This study provides evidence of positive changes in some of the underlying risk and protective factors that may underpin IPV. The significant changes identified are comprised of socio-demographic shifts (e.g. in education levels) and personal behaviours that may be largely undertaken by women (e.g. changes in the number of children and options to leave violent partners). To achieve sustainable reductions in IPV, more comprehensive and planned efforts are needed to address other underlying causes, such as exposure to violence in childhood (Fanslow, Gulliver, Hashemi, Malihi, & Mcintosh, 2021) through both prevention and provision of trauma-informed care for those already exposed; and efforts to address problematic alcohol use particularly among men. The consistency in the risk and protective factors that had the strongest association with IPV prevalence (e.g. partner infidelity, previous exposure to violence for both respondent and partner, and partner’s problematic alcohol use) still warrant attention and reinforce calls for provision of education around healthy relationships. These recommendations have also been endorsed by the World Health Organization and the World Bank, which have called for comprehensive public health strategies to address violence as population issue rather than a personal matter (Bott et al., 2005; Butchart et al., 2015).
Strengths
The present study is the first to examine how changes over time in the prevalence of physical and psychological IPV may be explained by concurrent changes in various risk and protective factors. Strengths include the use of large scale and representative samples, and the use of comparable methods and comparable questions across the two survey waves. This enabled us to test underlying factors that may have influenced the changes.
Limitations
The cross-sectional nature of the data does not provide information on causal order between IPV prevalence and risk and protective factors. Several of the variables included could be the result of changes in IPV victimization rather than the cause of it. For example, reduction in problematic alcohol or drug use could be the result of reduction in IPV and not vice versa. Additionally, while approximately 62% of eligible women were surveyed, it is still possible that the households and individuals most likely to be missed were those with greater levels of exposure to violence, as these individuals may have less capacity and willingness to participate in surveys. Consequently, rates of violence exposure noted in this study are likely to be underestimates of the true proportion of violence occurring in the population.
Collection of comparable data at different time points in the future would also be of benefit to determine if the observed reductions in IPV prevalence at these two time points are maintained and to allow additional exploration of factors that may underpin these changes. Future surveys should also collect data on the full spectrum of IPV types, as reductions in physical violence and psychological abuse are not always consistent with changes in economic abuse and controlling behaviours (Fanslow, Gulliver, Hashemi, Malihi, & Mcintosh, 2021)
There may also be unmeasured risk and protective factors particularly at the community and societal level that contribute to changes over time. As these factors can be linked with larger general societal initiatives (e.g. to close the gender pay gap (Willie & Kershaw, 2019)) or those that are directly targeted at changes that might influence IPV (e.g. public awareness campaigns to change attitudes and behaviours associated with IPV (Point Research Ltd, 2010)), these will be needed to be considered in future studies.
Conclusion and Implications
Despite a reduction in IPV prevalence between 2003 and 2019, work is still needed to address the substantial problem of IPV, as the strongest risk factors for IPV remained stable over the 15-year time interval (e.g. partner having concurrent sexual relationships, being violent to others, problematic alcohol-drug use or previous exposure to violence). The present study suggests that changes in IPV prevalence over time may be linked with changes that increase women’s autonomy (e.g. increase in education). Developing systems that enhance women’s relational mobility may also help reduce long-term exposure to IPV. Adequate structures and resources to support acute and long-term recovery for those exposed to violence remain important. Ultimately, prevention strategies that target perpetration of violence are needed.
Footnotes
Acknowledgements
We gratefully acknowledge participants, the interviewers, and the study project team, led by Patricia Meagher-Lundberg. We also acknowledge the representatives from the Ministry of Justice, the Accident Compensation Corporation, the New Zealand Police, and the Ministry of Education, who were part of the Governance Group for Family and Sexual Violence at the inception of the study.
Author’s Note
This study is based on the WHO Violence Against Women Instrument as developed for use in the WHO Multi-Country Study on Women’s Health and Domestic Violence and has been adapted from the version used in Asia and the Pacific by kNOwVAWdata Version 12.03. It adheres to the WHO ethical guidelines for the conduct of violence against women research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Research Council of New Zealand (grant number 02/207) for the 2003 study and the New Zealand Ministry of Business, Innovation and Employment (contract number CONT-42799-HASTR-UOA) for the 2019 study.